Embed Size (px)
Citation preview
MATERNAL MENTAL HEALTH AND INFANT HEALTH
Sarah Nagle-Yang MD 12/6/16
GOALS
Motherhood and mental health in the context of trauma •Mental health implications •Obstetrical implications •Parenting implications •What can we do to help?
WHY TRAUMA?
Trauma is common
Trauma informs one’s mental health and worldview
Trauma in mothers has the potential to impact their children in multiple dimensions In utero environment Attachment patterns Parenting practices
WHAT IS TRAUMA: DSM DSM V: “Exposure to actual or threatened death, serious injury, or sexual violence.”
•Combat
•Natural Disaster
•Act of Terrorism
•Assault
•Childhood abuse
•Childhood molestation
•Childhood Neglect
•Prolonged IPV
Circumscribed Prolonged
WHAT IS TRAUMA: TRAUMATIC STRESS
3 Types of stress response Positive Brief, mild-moderate
Available caring adult
Growth promoting
Tolerable More severe in magnitude
Available caring adult facilitates adaptive coping
Toxic Strong, frequent or prolonged
Absence of buffering effect of supportive adult Shonkoff 2012
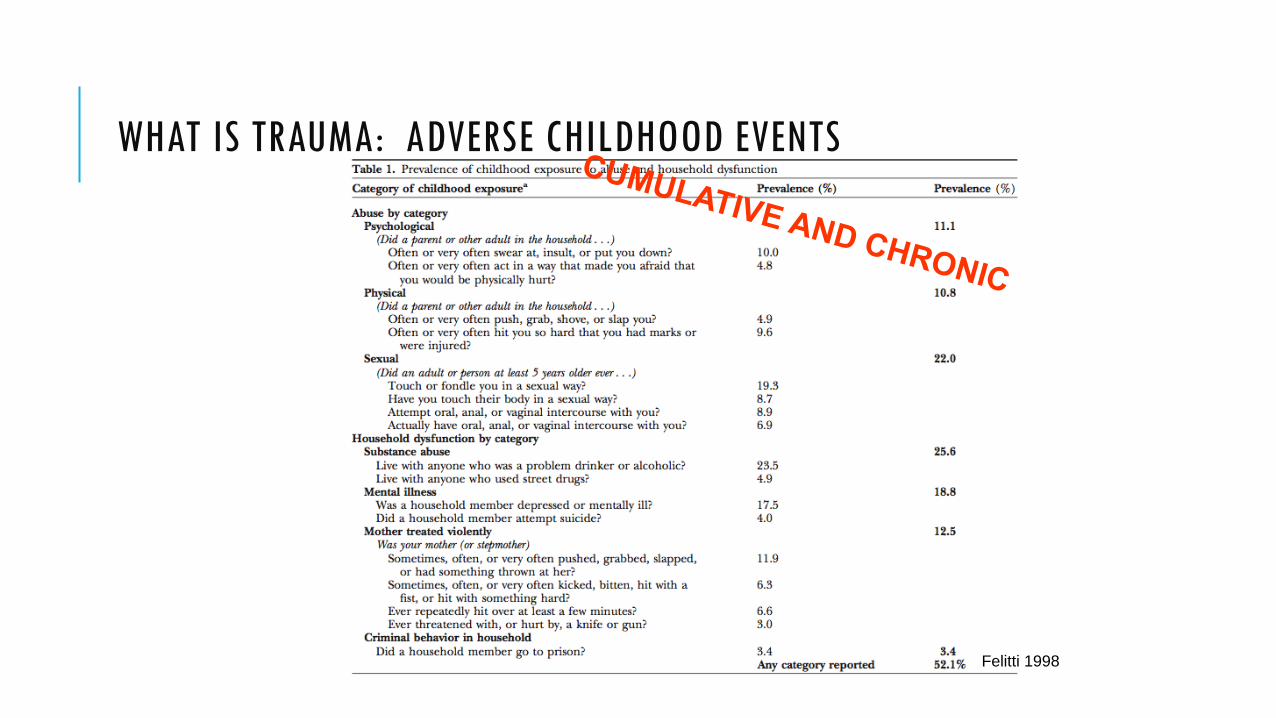
WHAT IS TRAUMA: ADVERSE CHILDHOOD EVENTS
Felitti 1998

Felitti 1998
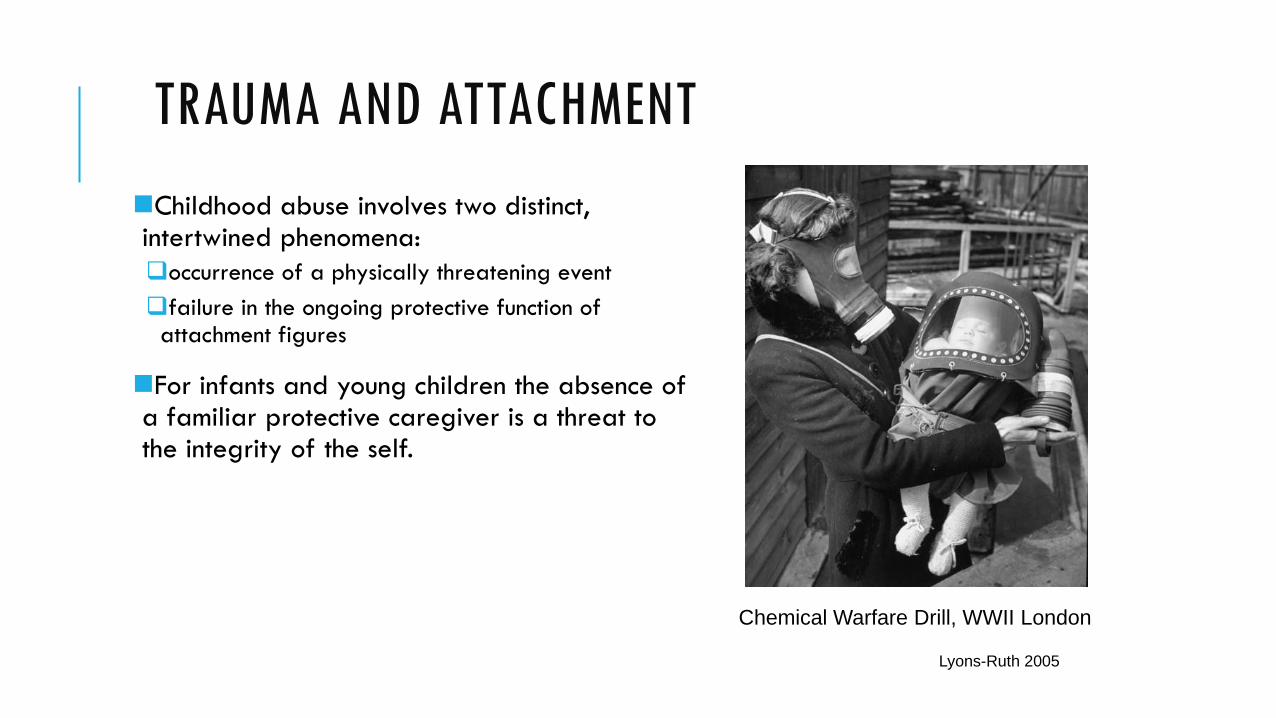
TRAUMA AND ATTACHMENT Childhood abuse involves two distinct, intertwined phenomena: occurrence of a physically threatening event failure in the ongoing protective function of
attachment figures
For infants and young children the absence of a familiar protective caregiver is a threat to the integrity of the self.
Lyons-Ruth 2005
Chemical Warfare Drill, WWII London
DIAGNOSES: COMPLEX PTSD
Proposed by Judith Herman in 1992 to describe a syndrome observed in survivors of prolonged, repeated trauma
PTSD field trial for the DSM-IV tested cPTSD as Disorders of Extreme Stress, Not Otherwise Specified (DESNOS) Much overlap with PTSD, so symptoms of DESNOS were listed as associated features of PTSD
Critical evaluation by DSM-V committee
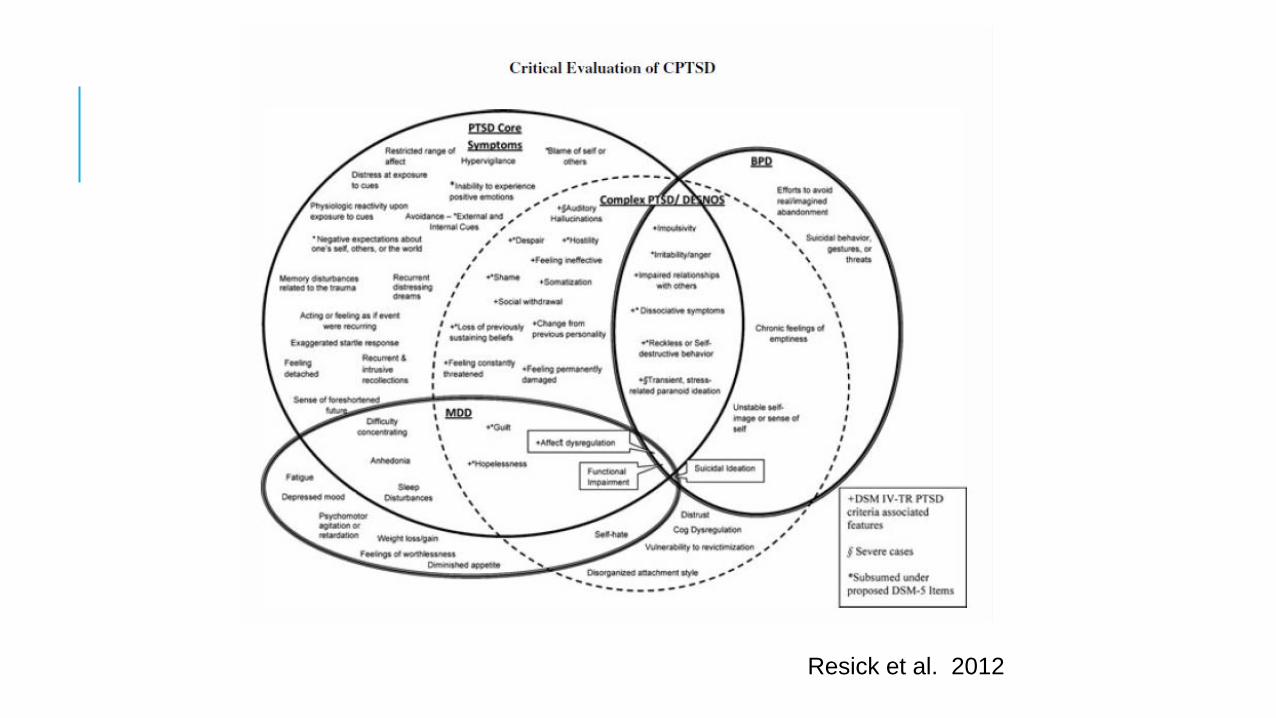
Resick et al. 2012
DIAGNOSTIC PRESENTATION OF CHILDHOOD TRAUMA MDD
PTSD
Borderline Personality Disorder
Dissociative Disorder
Chemical Dependency
Developmental crisis which impacts the formation of self-definition and self-regulation
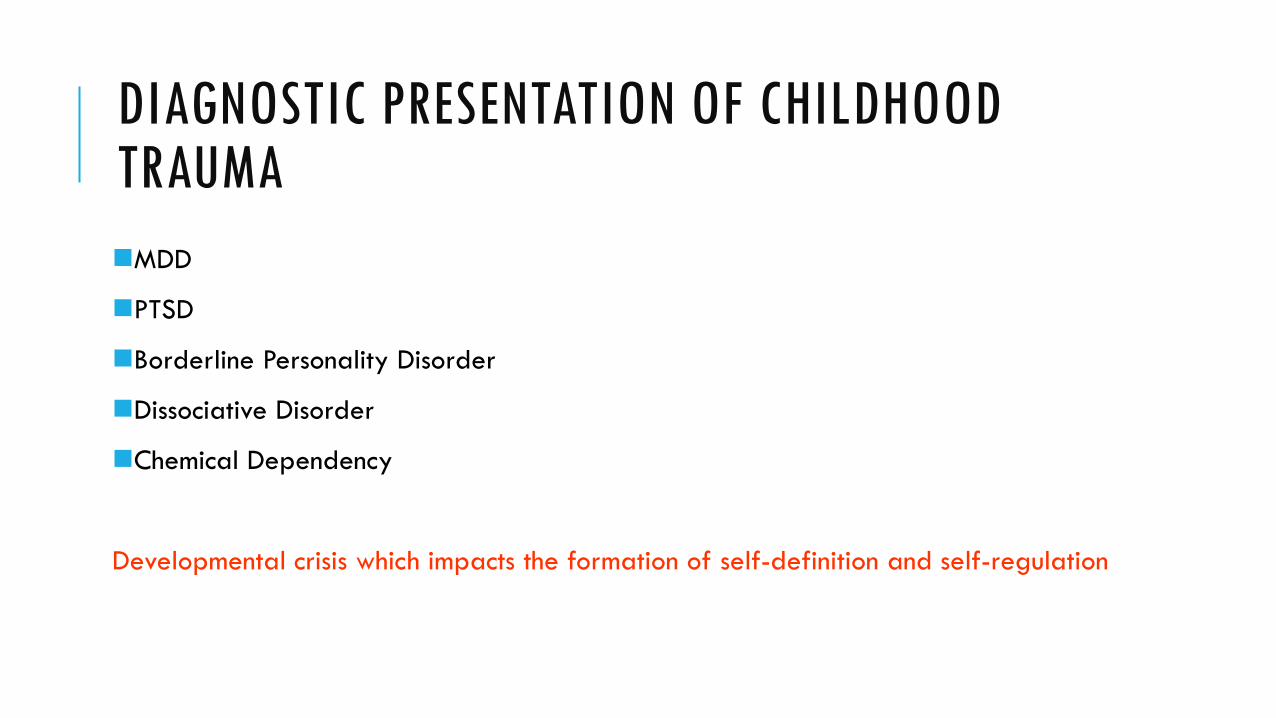
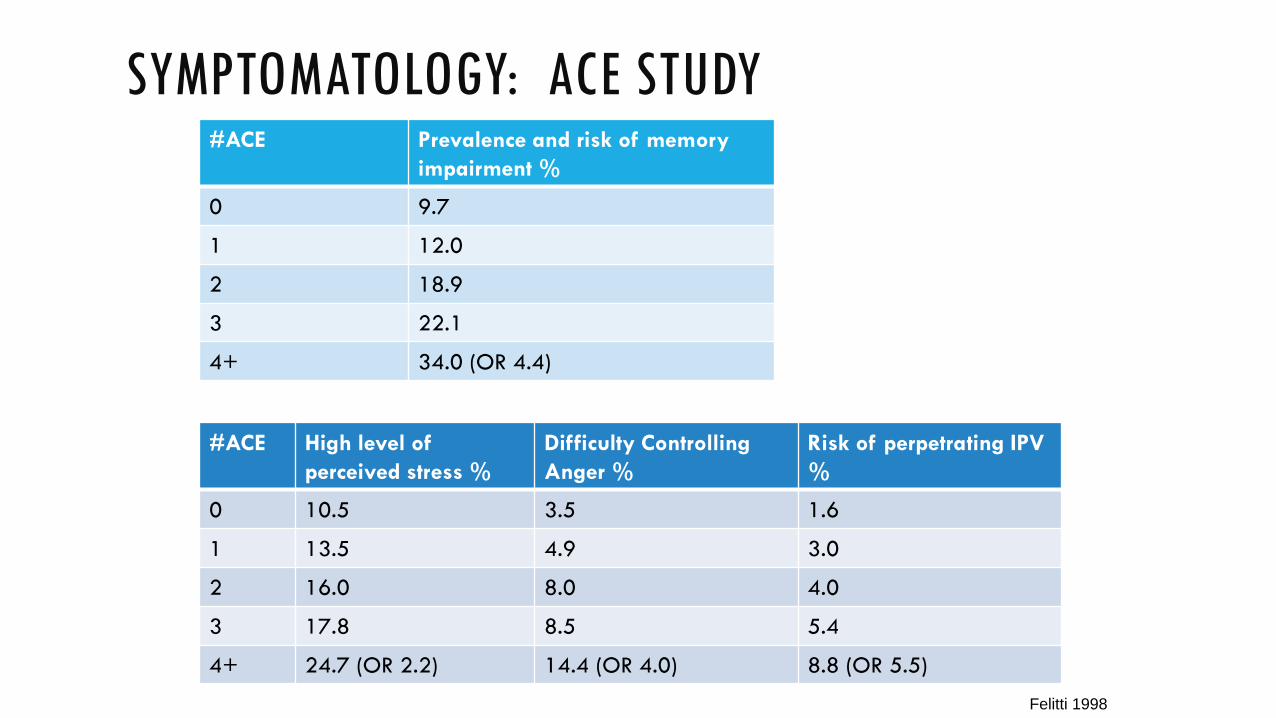
SYMPTOMATOLOGY: ACE STUDY #ACE Panic Reaction
% Depressed Affect %
Anxiety % Hallucinations %
0 8.3 18.4 7.8 1.3
1 10.9 25.2 9.1 1.5
2 13.6 34.1 12.4 2.3
3 16.8 38.8 14.1 2.9
4+ 20.9 (OR 2.5) 49.0 (3.6) 19.0 (2.4) 4.0 (2.7)
#ACE Sleep Disturbance % Severe Obesity % Mult Somatic Sx %
0 36.3 5.6 5.1
1 41.6 7.4 6.4
2 47.5 8.3 8.6
3 51.1 8.8 8.1
4+ 56.1 (OR 2.1) 11.9 (OR 1.9) 13.9 (OR 2.7) Felitti 1998
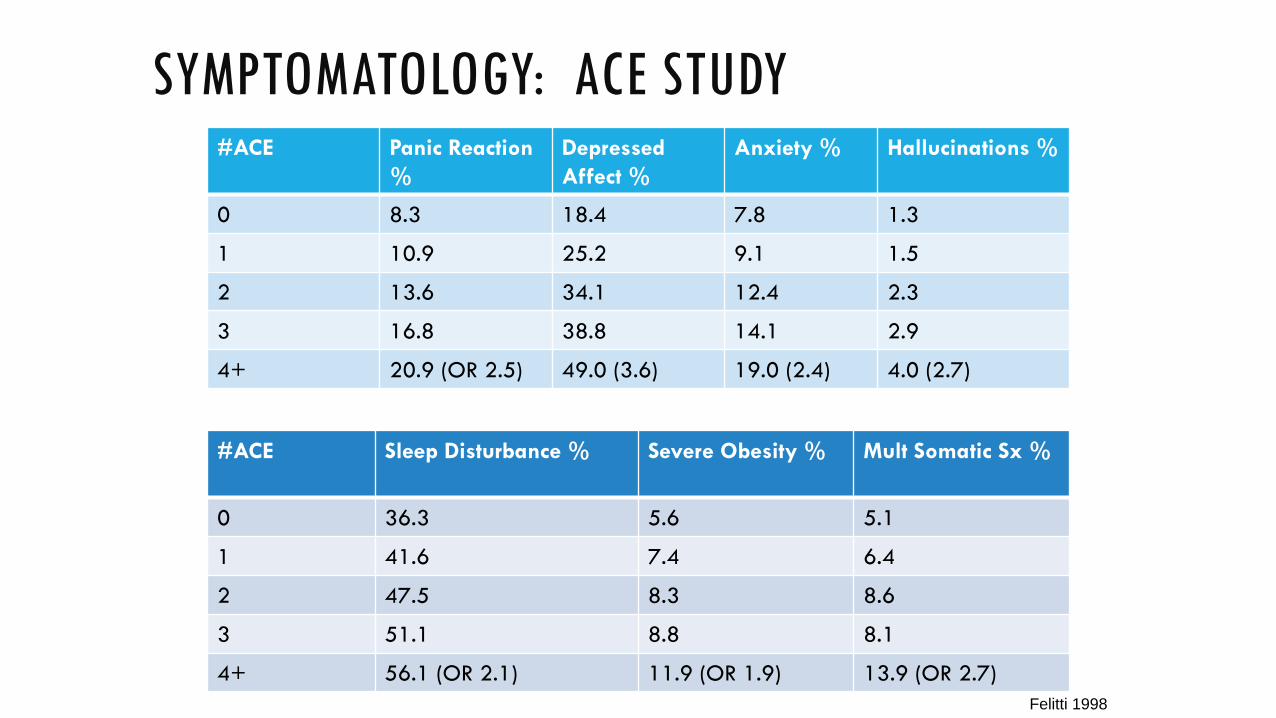
SYMPTOMATOLOGY: ACE STUDY #ACE Prevalence and risk of memory
impairment %
0 9.7
1 12.0
2 18.9
3 22.1
4+ 34.0 (OR 4.4)
#ACE High level of perceived stress %
Difficulty Controlling Anger %
Risk of perpetrating IPV %
0 10.5 3.5 1.6
1 13.5 4.9 3.0
2 16.0 8.0 4.0
3 17.8 8.5 5.4
4+ 24.7 (OR 2.2) 14.4 (OR 4.0) 8.8 (OR 5.5)
Felitti 1998

COMORBIDITY: ACE STUDY #ACE Smoking % Alcoholism % Illicit Drug Use % Injected Drug Use
%
0 6.5 2.5 7.9 0.2
1 7.6 5.1 13.8 0.6
2 9.3 7.4 20.0 1.4
3 11.9 10.5 24.9 1.6
4+ 14.5 (OR 1.8) 15.3 (OR 7.2) 35.2 (OR 4.5) 3.7 (OR 11.1)
#ACE Early Intercourse % Promiscuity >30 partners %
0 2.3 3.9 1 5.1 5.2 2 6.6 7.4 3 8.5 8.7 4+ 14.2 (OR 6.6) 10.8 (OR 3.6) Felitti 1998

COMORBIDITY: ACE STUDY #ACE Current Severe
Family Problems % Current Severe Job Problems %
Current Severe Financial Problems %
0 8 4 7
1-2 12 7 13
3-4 16 12 20
5+ 24 (OR 3.3) 16 (OR 2.9) 23 (OR 2.4)
Felitti 1998
impulsivity
Unstable relationships
Illicit drug use
Decreased concentration
smoking
shame
irritability
anger
Self-hate
Preconception promiscuity
Financial stress
alcoholism depression
anxiety

TRAUMA AND PREGNANCY
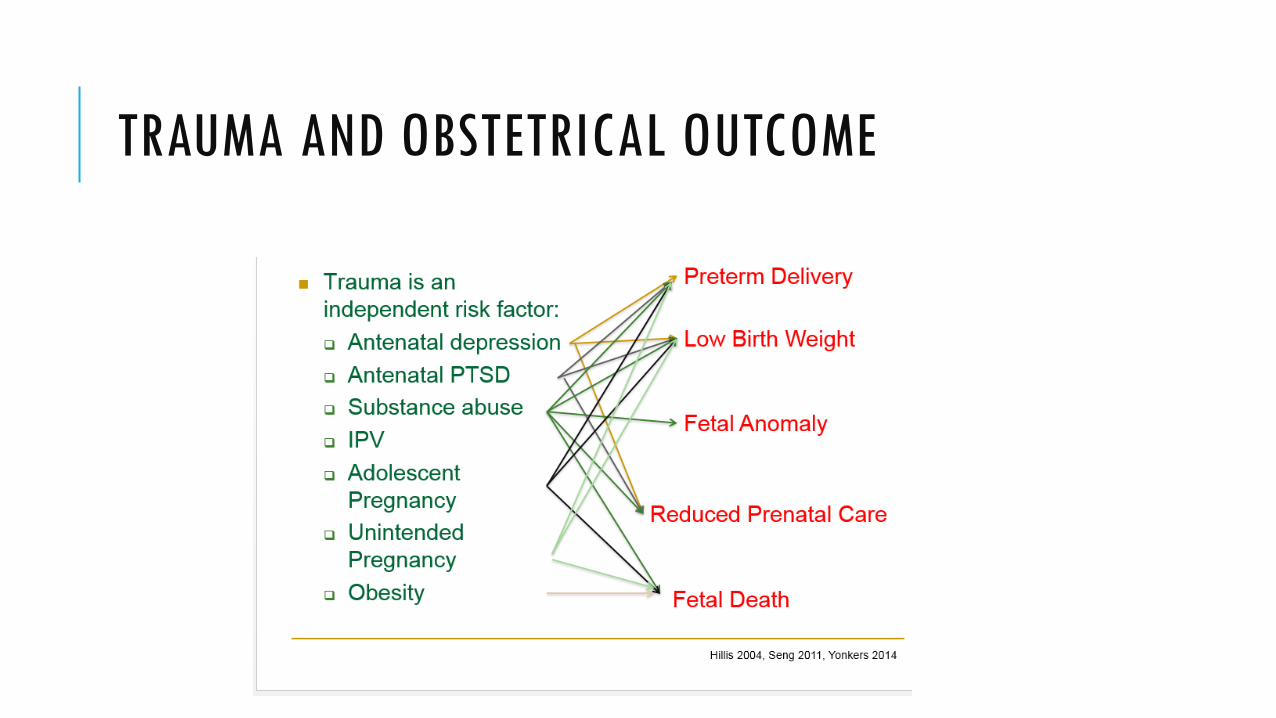
TRAUMA AND OBSTETRICAL OUTCOME
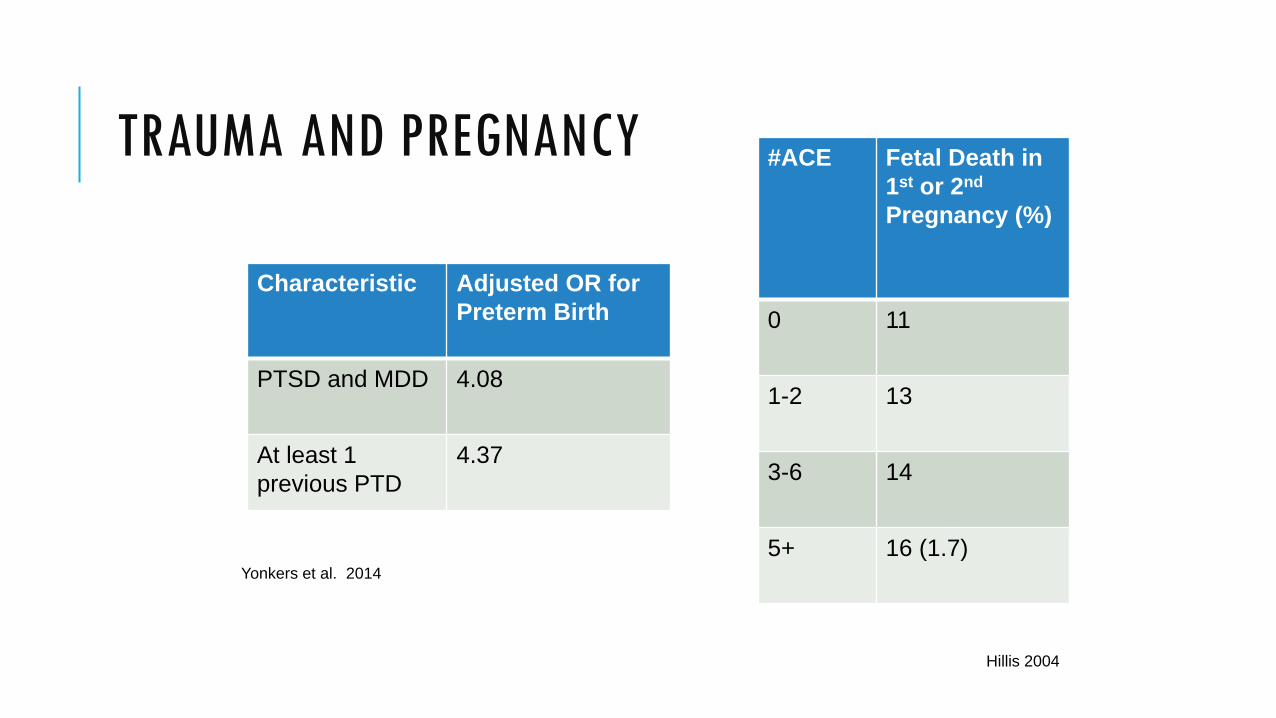
TRAUMA AND PREGNANCY #ACE Fetal Death in 1st or 2nd Pregnancy (%)
0 11
1-2 13
3-6 14
5+ 16 (1.7)
Characteristic Adjusted OR for Preterm Birth
PTSD and MDD 4.08
At least 1 previous PTD
4.37
Yonkers et al. 2014
Hillis 2004
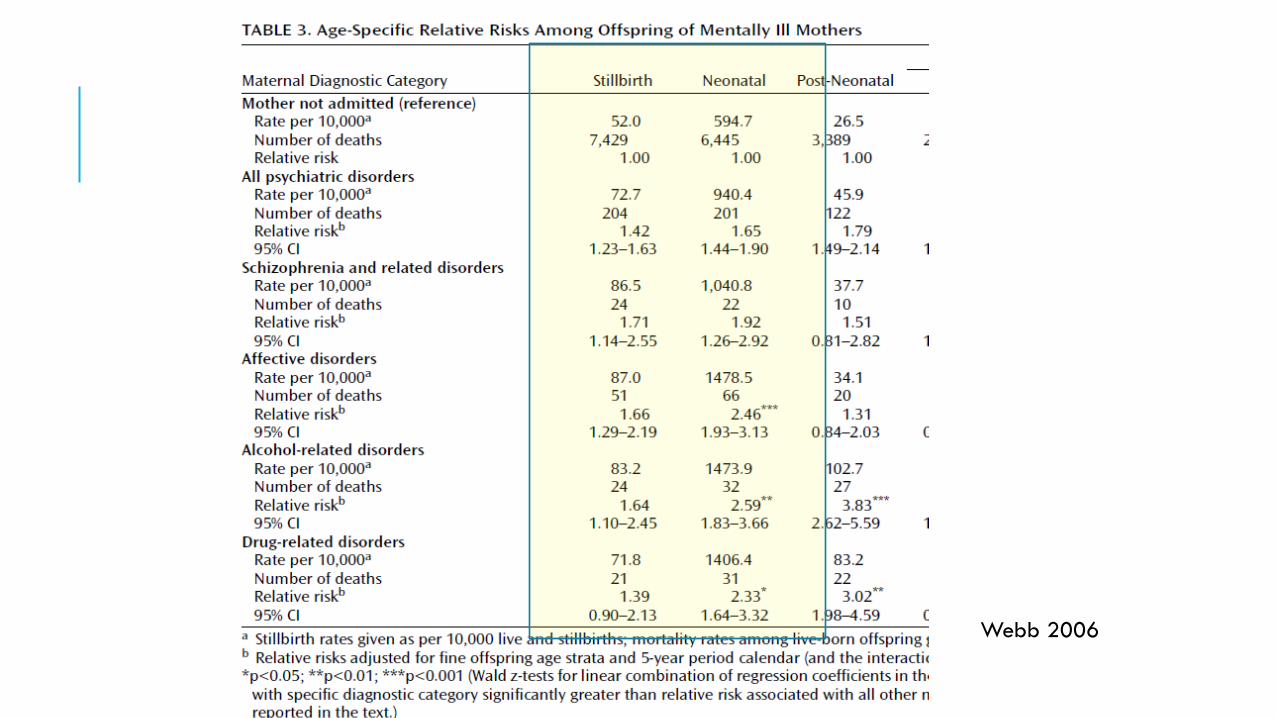
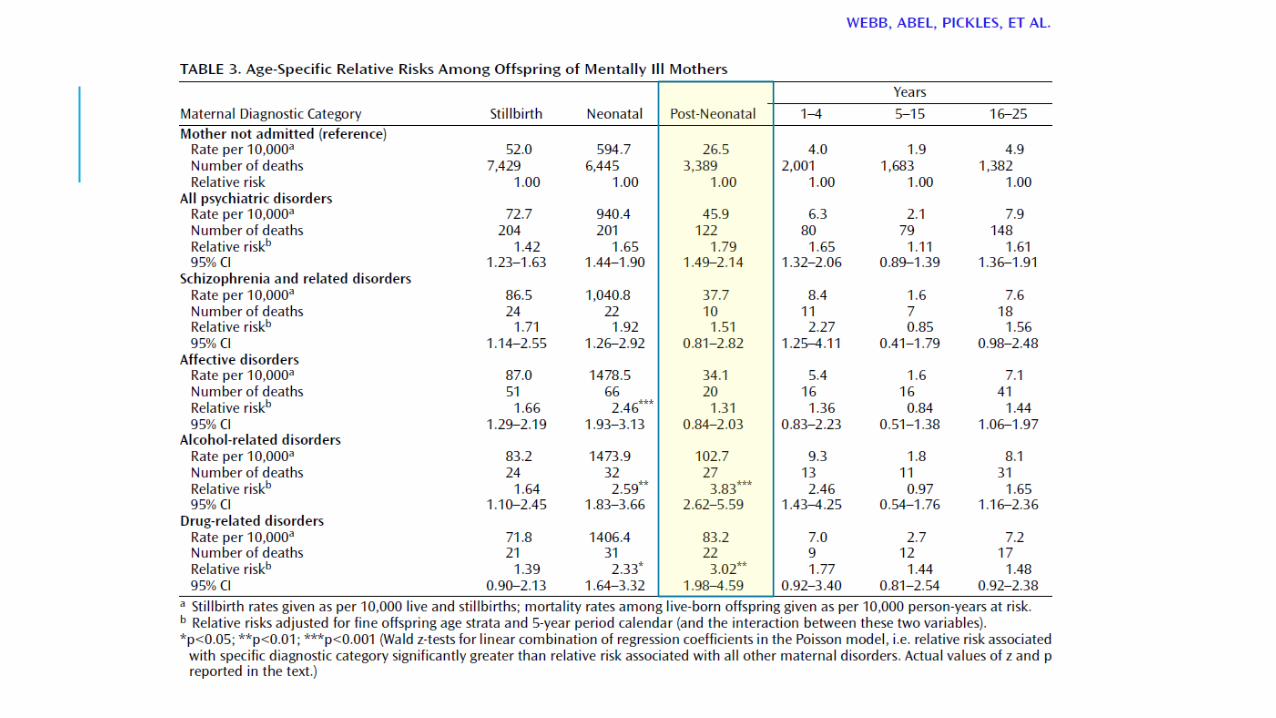
Webb 2006
PRENATAL STRESS: CHILDHOOD DEVELOPMENTAL/
BEHAVIORAL OUTCOMES
ADHD
Anxiety
Cognitive delays
Language delays Kinsella 2009

FETAL NEUROBEHAVIOR Indices of emerging differences in stress-related neurodevelopment Fetal Heart Rate Variability
Reactivity to a stimulus
Fetal Activity Coupling
Fetuses with abnormal neurobehavior are more likely to be come fussy infants at 6 weeks of age
DiPietro 2008, Kinsella 2009
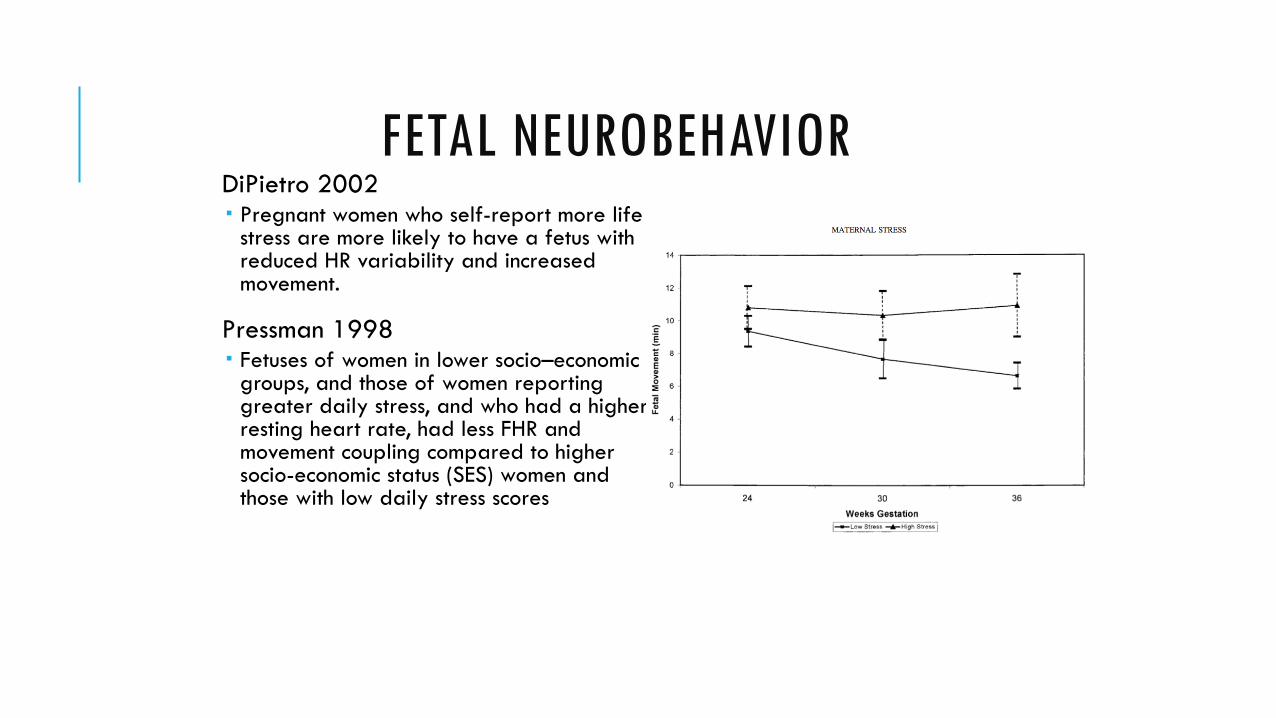
FETAL NEUROBEHAVIOR DiPietro 2002 Pregnant women who self-report more life
stress are more likely to have a fetus with reduced HR variability and increased movement.
Pressman 1998 Fetuses of women in lower socio–economic
groups, and those of women reporting greater daily stress, and who had a higher resting heart rate, had less FHR and movement coupling compared to higher socio-economic status (SES) women and those with low daily stress scores
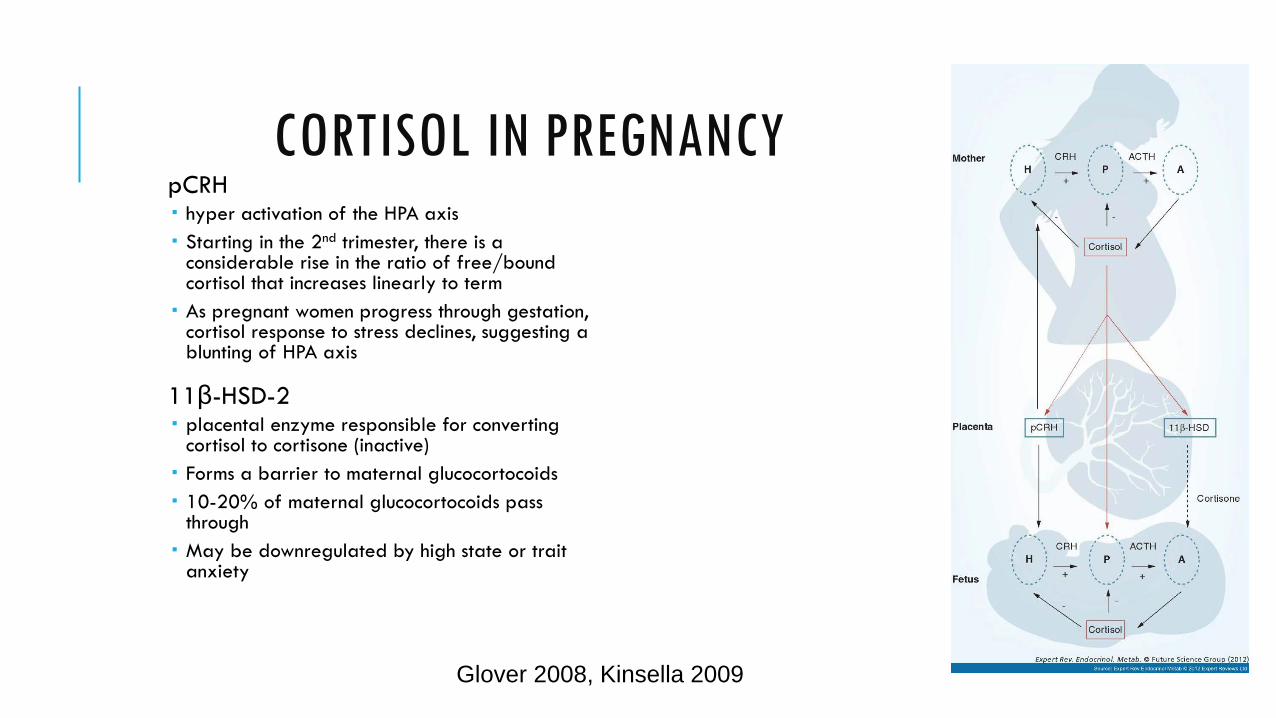
CORTISOL IN PREGNANCY pCRH hyper activation of the HPA axis Starting in the 2nd trimester, there is a
considerable rise in the ratio of free/bound cortisol that increases linearly to term As pregnant women progress through gestation,
cortisol response to stress declines, suggesting a blunting of HPA axis
11β-HSD-2 placental enzyme responsible for converting
cortisol to cortisone (inactive) Forms a barrier to maternal glucocortocoids 10-20% of maternal glucocortocoids pass
through May be downregulated by high state or trait
anxiety
Glover 2008, Kinsella 2009
PRENATAL STRESS AND NEONATAL Lundy 1999 Depressed women had higher cortisol and
norepinephrine levels and lower dopamine levels. Their newborns also had higher cortisol and
norepinephrine levels and lower dopamine levels, thus mimicking their mothers’ biochemical profile. The neonates of depressed mothers also showed
inferior performance on the orientation, reflex, excitability, and withdrawal clusters of the Brazelton scale.
FETAL PROGRAMMING Fetal, infant and early childhood brain plasticity makes it particularly sensitive to chemical influences
Evolutionary advantage?
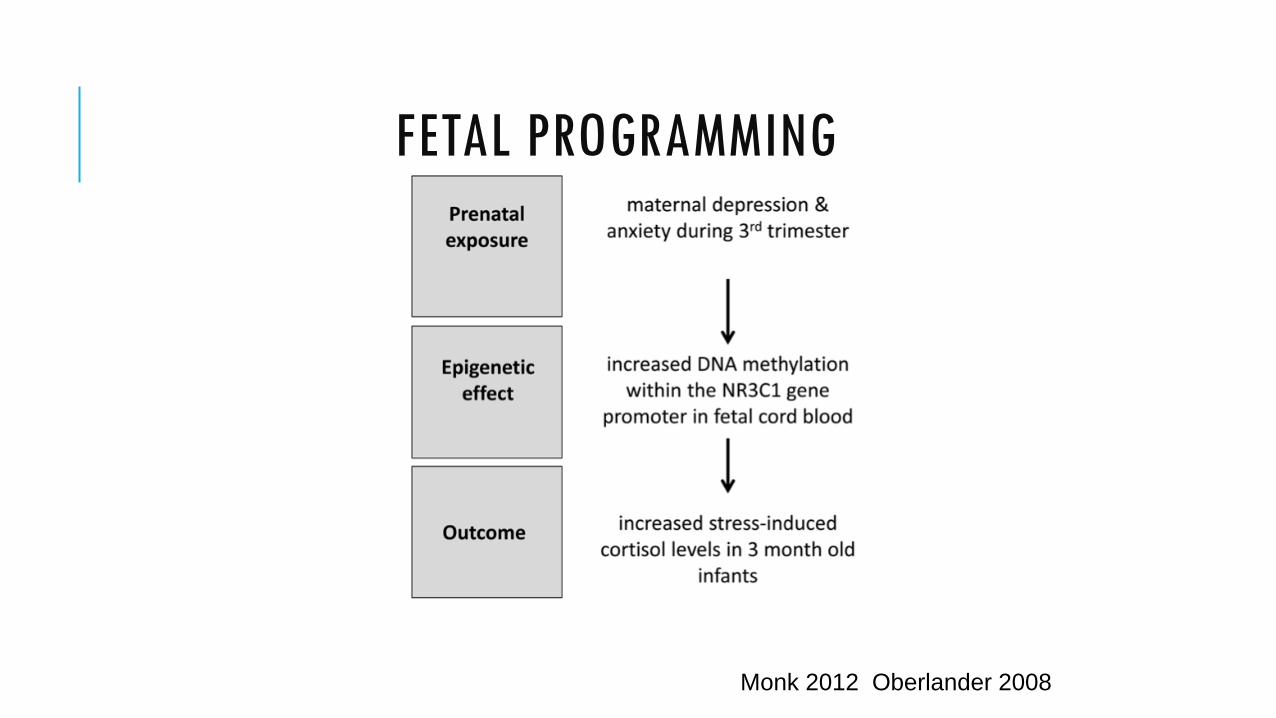
FETAL PROGRAMMING
Monk 2012 Oberlander 2008
FETAL PROGRAMMING
Microarray analysis of fetal brain cells: increased cortisol exposure affects the expression of over a thousand genes
Salaria 2006
impulsivity
Unstable relationships
Illicit drug use
Decreased concentration
smoking
shame
irritability
anger
Self-hate
Postnatal Environment promiscuity
Financial stress
alcoholism
anxiety
depression
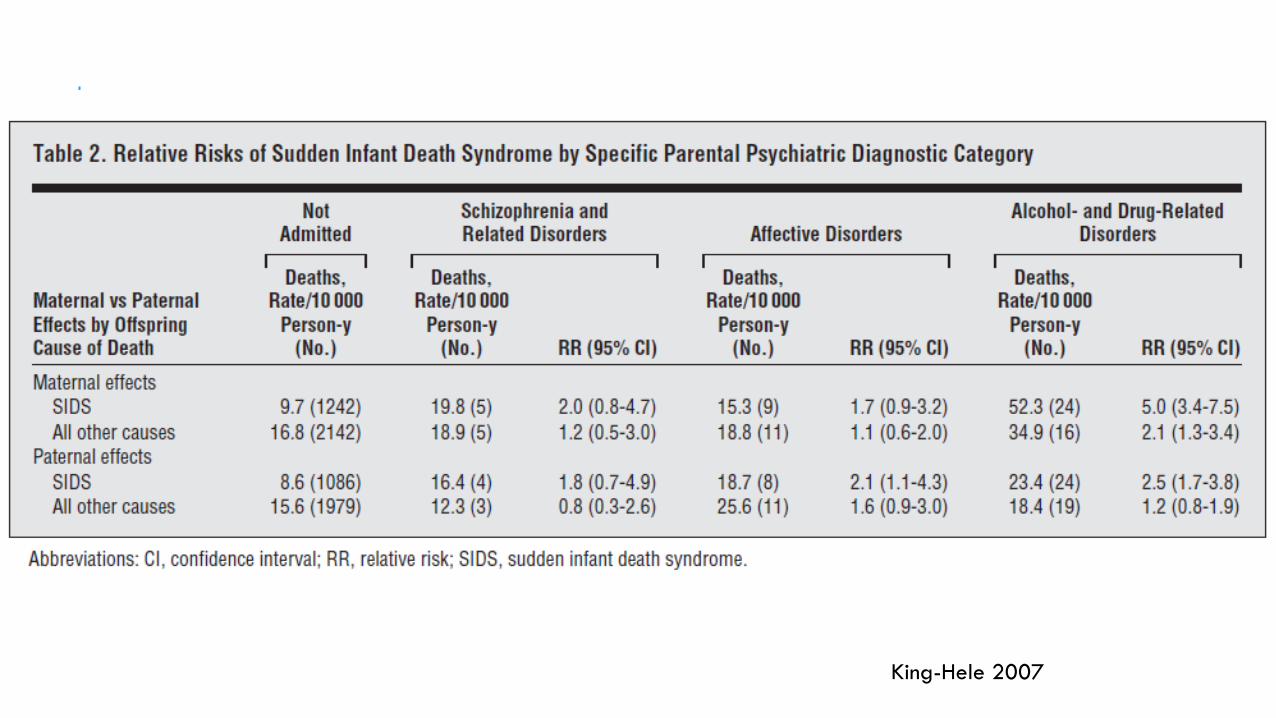
King-Hele 2007

TRAUMA AND MOTHERHOOD
Reduced parenting confidence
More malevolent attributions
Boundary distortion
Role reversal
Authoritarian/ Hostile parenting
Permissive/ Helpless style
Increased psychological aggression
Increased use of physical punishment
Alexander 2000, Banyard 2003, Lyons-Ruth 2005, Noll 2009
TRAUMA AND MOTHERHOOD
Disrupted infant attachment
Diminished parenting support
Child Protective Services involvement
Banyard 2003, Noll 2009
MATERNAL DEPRESSION
Depressed moms at 2 to 4 months postpartum report less: Breastfeeding Use of healthy child development
practices (eg: showing books to, playing with or talking to their infant) Routines
Depressed moms at 30 to 33 months postpartum report: More use of harsh discipline (spanking
and slapping) Fewer limits on toddler TV time Fewer safety measures (outlet covers,
safety latches) Less of a daily routine
McLearn 2006
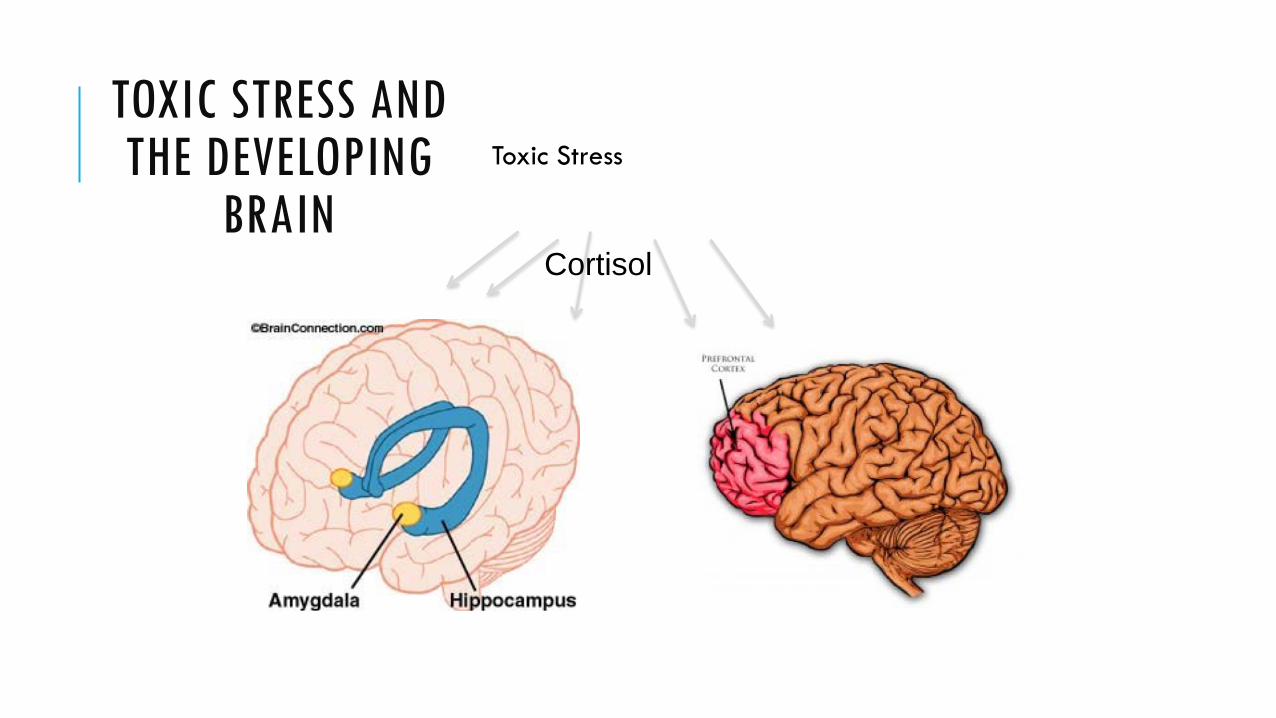
TOXIC STRESS AND THE DEVELOPING
BRAIN Toxic Stress
Cortisol
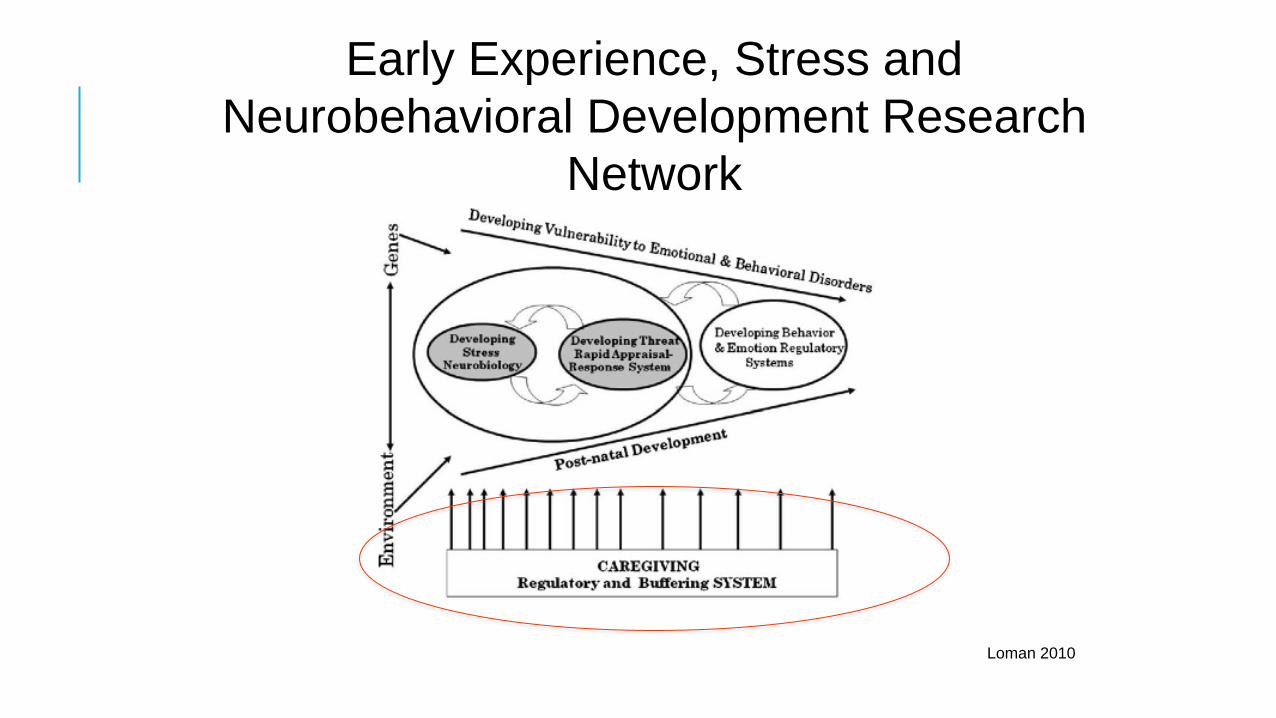
Loman 2010
Early Experience, Stress and Neurobehavioral Development Research
Network

MARY AINSWORTH: MATERNAL SENSITIVITY Described the mother of a securely attached child as being “capable of perceiving things from {the child’s} point of view” and being able to regard her child “as a separate person; she also respects his activity-in-progress and thus avoids interrupting him.”
Meins 2001
MATERNAL SENSITIVITY: AINSWORTH
1. Sensitivity to baby’s signals ability to perceive and to interpret
accurately the communications implicit in her infant's behavior, and given this understanding, to respond to them appropriately and promptly
2. Cooperation with Baby’s ongoing behavior
3. Physical and Psychological Availability
4. Acceptance of the Baby's Needs
Meins 2001
ATTACHMENT AND SELF-REGULATION
A mother’s capacity to regulate her infant’s fear and distress is crucial to that child’s ultimate feeling of security.
Secure attachment is the direct outcome of successful containment, namely the parent’s capacity to both reflect the infant’s internal state, as well as represent that state for the infant as a manageable experience.
The mutual regulatory processes of early childhood gradually allow for an increase in the child’s ability to self-regulate
Meins 2001
In order to respond sensitively, a parent needs to be able to make sense of her own and her child’s mental states.
TRAUMA AND MOTHERHOOD
Reduced parenting confidence
More malevolent attributions
Boundary distortion
Role reversal
Authoritarian/ Hostile parenting
Permissive/ Helpless style
Increased psychological aggression
Increased use of physical punishment
Alexander 2000, Banyard 2003, Lyons-Ruth 2005, Noll 2009
INTERGENERATIONAL TRANSMISSION OF ATTACHMENT
HOWEVER, a h/o trauma does not necessarily dictate a specific pattern of parenting
Van IJzendoorn 1992: Metanalysis We tend to repeat the automatic attachment and
parenting interactions we experienced However, the intergenerational transmission of
parenting in situations of trauma is more related to the caregiver’s state of mind regarding the trauma than the trauma itself
Van IJzendoorn 1992
WHAT IS MATERNAL REFLECTIVE FUNCTIONING?
A mother’s capacity step back from her own affective experience in order to reflect upon her child’s uniquely subjective intentions during moments of stress or conflict
Painful affect (in either the caregiver or the child) becomes manageable because the caregiver can see painful feelings, or disturbing thoughts, as merely mental states, rather than concrete realities, thus opening the possibility for modulation and change over time.
It is this capacity, in turn, that allows the caregiver, time after time, to remain both emotionally engaged and sufficiently in control, so that she can contain the infant’s distress and transform it into a tolerable experience over which the child can begin to develop a sense of mastery.
Grienenberger 2005
MATERNAL REFLECTIVE FUNCTIONING Negatively correlated with dysfunctional maternal behavior
Grienenberger 2005
Positively correlated with infant attachment security Parents with high RF are more likely to be classified
as autonomous on AAI and to have children who are themselves securely attached
Fonagy 1991
MATERNAL REFLECTIVE FUNCTIONING
High RF in adoptive mothers= lower child externalizing
Higher mind-mindedness Behavioral sensitivity Interactive synchrony
Lundy 2003, Priel 2000
Higher RF in a sample of mothers with significant trauma history was significantly associated with an balanced internal representations of her child
Schechter 2005

WHAT CAN WE DO?
•Recognize maternal mental health disorders as a risk factor for infant morbidity and mortality.
•Prioritize the mental health and wellness of mothers by • destigmatizing mental health treatment, • increasing access to mental health treatment for mothers • increasing parenting supports for women with mental health disorders
WHAT CAN WE DO?
•Educate colleagues and clients about the RISKS of mental health and substance abuse disorders that occur during and after pregnancy.
•If you work in obstetrics or pediatrics, inquire about SCREENING for trauma, mental health and substance use disorders in your practice
•Know about your local MENTAL HEALTH RESOURCES, particularly those that are targeted towards pregnant or postpartum women
•Address the stigma of mental health treatment. Let mothers you work with know that these are COMMON and TREATABLE conditions.
•If you have the opportunity to work directly with a mother-child pair, let that mother know that you VALUE her and are there as a support to HER. Validate that parenthood is hard, and important.

EXAMPLES OF TARGETED INTERVENTIONS Mother-infant Therapy Group for Postpartum Depression Roseanne Clark, U of Wisconsin CBT-based depression group for moms, dyadic
group focused on reflective functioning
Mothers and Toddlers Program Nancy Suchman, Yale Individual therapy program targeting
parenting difficulties among substance abusing mothers Aim to build healthier maternal representation
of their children and higher reflective functioning Results show participants show greater
maternal sensitivity
EXAMPLES OF TARGETED INTERVENTIONS
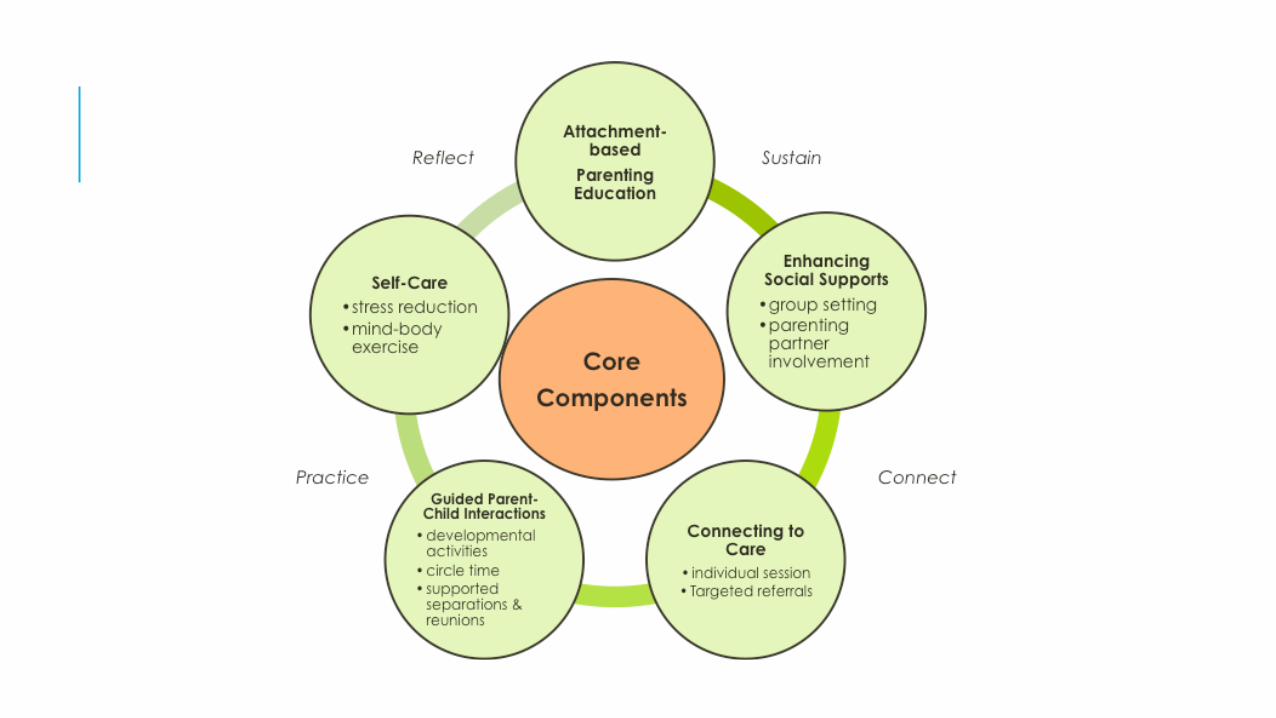
MOM Power Maria Muzik, U of Michigan 13-week manualized group psychoeducational program for trauma-exposed mothers of young
children ages 0-6 Topics include: Understanding your child’s attachment needs
Restoring your emotional balance
Impact of trauma on one’s own parenting experience
Building a parenting support system
Questions?





























