Embed Size (px)
Citation preview

Disclaimer
Privileged & Confidential This document is covered under the attorney-client privilege. This document is also part of the quality assessment and peer review activities of CCHMC and, as such, is a confidential document not subject to discovery pursuant to Ohio Revised Code (ORC) Sections 2305.24, 2305.25, and 2305.252. All committees involved in the review of this document, as well as those individuals preparing and submitting information to such committees, claim all privileges and protection afforded by ORC Sections 2305.24, 2305.25, 2305.251, and 2305.252 and any subsequent legislation. The information contained is solely for the use of the individual or entity intended. If you are not the intended recipient, be aware that any disclosure, copying, distribution, or use of the contents of this document is prohibited.

16 year old
male
1 day history of black stools and bright red bloody emesis
Initial hemoglobin 9.4 pRBC transfusion Administered PPI Yes NG - In place upon arrival
PICU X4 days + floor 6 days Shock-AKI with large volume resuscitation (pRBC, plts and cryo)
EGD - several varices and 1 gastric varix + mild portal HTN

Upper GI BleedsMedical Video Review

Learning Objectives Etiology and recognition of the upper GI tract as the source of bleeding
Management of Upper GI bleeding with hemorrhagic shock in the STS

16 year old
male
17 year old
male
4 year old female
15 year old
male

17 year old
male
A few hours of nausea and dark coffee colored emesis
Initial hemoglobin 10.2 pRBC transfusion Administered PPI Yes NG - No
PICU x 3 days + floor 7 days Shock, intubation and continued hematemesis, epi drip
EGD - large esophageal and gastric varices with large clot in obstructing part of the gastric wall

16 year old
male
17 year old
male
4 year old female
15 year old
male
4 year old female
Dark stool for 1 day and coffee ground emesis
Initial hemoglobin 7 pRBC transfusion Administered PPI yes NG - No
Floor x 7 days, Abd U/S: Cavernous transformation of the portal vein, Cirrhosis, splenomegaly, enlarged gall bladder and ascites Hep C AB+, Hep A IgG+, Hep Bs+
EGD - Esophageal varices with banding

16 year old
male
17 year old
male
4 year old female
15 year old
male

15 year old
male
1.5 weeks of melena and 1 day of coffee ground emesis, syncope
Initial hemoglobin 3.9 pRBC transfusion Administered PPI yes NG - In place upon arrival
Floor x 24 hours
EGD - multiple gastric ulcers

Etiology and recognition of the upper GI tract as the source of bleeding

Severe UGI bleeds are rare
We saw 8 in the STS in the past year

20% of GI bleeds in pediatric patients are upper

Cochran, Crit Care Med ,1992
Prospective cohort of 208 ICU patients
25% had upper GI bleeding
No association between upper GI bleeding and age, weight, race, or sex
Independent association w/ circulatory shock, an operative procedure and trauma

Lacroix, Crit Care Med,1992
Prospective study of >900 patients
<7% UGI bleed
Multivariate analysi
Risk factors high Pediatric Risk of Mortality score, coagulopathy, pneumonia, and multitrauma

Pant, Curr Med Res Opin, 2014
23,383 pediatric discharges with a diagnosis of GI bleeding (0.5%)
More likely to be male (54.5% vs. 45.8%)
Older (children ≥11 years; 50.8% vs. 38.7%)
Lower GI bleeding more common (17.6 per 10,000 discharges) followed by hematemesis (11.2 per 10,000 discharges)
Highest mortality rates w/ GI bleeding intestinal (8.7%) and esophageal perforation (8.4%)

Unsurprisingly most patients with hematemesis are not seen in the bay
The most common cause of serious UGI bleeds in children >2 is a variceal bleed

Neonates
Swallowed maternal blood
Vitamin K deficient bleeding (Hemorrhagic disease of the newborn)
Stress gastritis or ulcers in shock/critical illness
NEC
Intestinal duplications or vascular anomalies
Coagulopathy
Milk protein intolerance (lower GI bleeding is more common)

Mallory-Weiss tear
Ulcers and gastritis - NSAIDs
Esophagitis
GERD is #1 in this age range, recurrent emesis, or caustic ingestion/foreign body
Variceal bleeding
More likely in children with portal hypertension
Hemangioma, Vascular malformation, HHT, Kasabach-Merritt syndrome
AV fistula
Infants/Toddlers

Mallory-Weiss tears
Peptic ulcers and gastritis
Pill esophagitis
Varices (#1 cause of severe UGI bleeding in children)
Older Children

IVC
Hepatic ve
ins
Portal vein
Esophageal vein
Gastric
vein
Intrahepatic Cirrhosis
Biliary atresia Cystic fibrosis TPN-induced liver disease
Intrahepatic scarring1
Portal vein resistance2
Pressure increase3
Portal Hypertension

Direct injuryOmphalitis Umbilical catheterization Neonatal peritonitis Abdominal trauma Cysts and tumors at the porta hepatis
Portal vein abnormalitiesStenosis/atresia/agenesis
Indirect factorsSepsis Dehydration Multiple exchange transfusions Hypercoagulable states
IVC
Hepatic ve
ins
Portal vein
Esophageal vein
Gastric
vein
Prehepatic Portal vein thrombosis or narrowing
Portal vein obstruction1
Splenomegaly + thrombocytopenia2
Portal Hypertension
IVC
Hepatic ve
ins
Portal vein
Esophageal vein
Gastric
vein
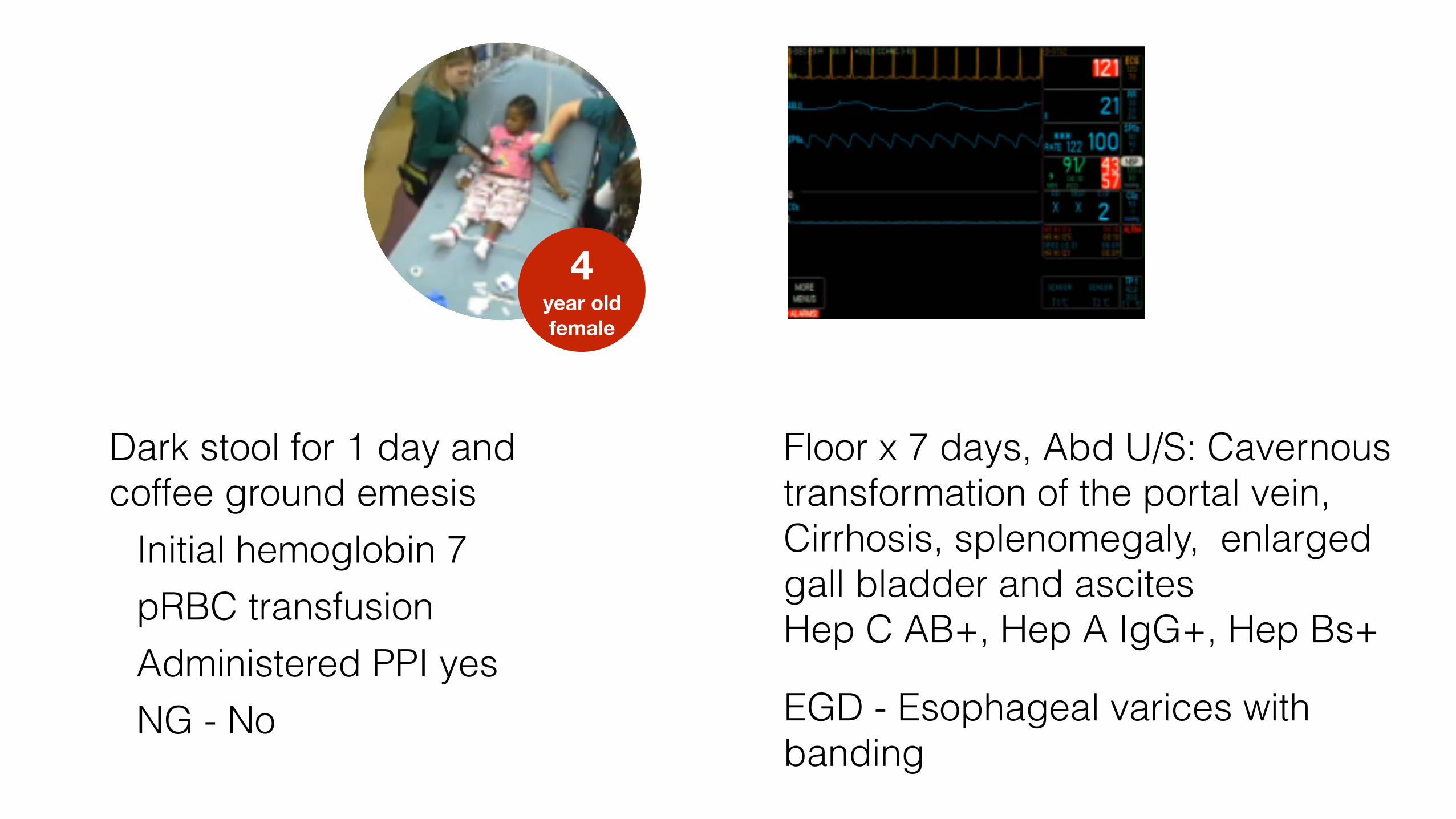
Suprahepatic Post-sinusoidal portal hypertension
Budd Chiari CHF Veno-occlusive disease
Suprahepatic resistance1
Pressure increase2
Portal Hypertension

Peptic ulcer (35-50%)
Esophagitis (20-30%)
Duodenitis/gastritis/erosions (10-20%)
Varices (5-12%)
Mallory-Weiss tears (2-5%)
Tumour (2-5%)
Angiodysplasia (2-3%)
Aorto-enteric fistula (<1%)
Adults
Not the GI tract Epistaxis is far and away #1
Pulmonary hemorrhage
Friable tonsils, hemorrhagic pharyngitis
Injury
Post T&A bleeding

Not actually blood Red food (drinks, candy, beets)
Hint: do a guaiac test
Management of Upper GI bleeding with hemorrhagic shock in the STS

ABCs (Recognition of shock state)
Access x2
Determination of hemoglobin early
Anticipate need for blood

Focused history
NSAID use
Family history of H. pylori
Relevant comorbidities (including psych re caustic ingestion)
Pain
Fever
Diarrhea
Previous hemoglobin

Blood Products
O Negative Blood was given emergently in STS 12 times over the past year (medical and trauma)
To obtain blood emergently for medical patients: Call 636-4508 Name, gender and MRN Number of units Send a transporter

Blood Products
Type & Cross
When potential for blood transfusion need is high
ABO/Rh blood type and antibody screen
In the crossmatch, the patient's blood and donor blood are tested for compatibility
Turn around time is approx. 35-45 min once blood arrives in the lab
Type and screen
ABO/Rh blood type is determined, and an antibody screen is done
No blood is crossmatched

Blood Products
One unit of blood is 280-320 mL (average 300mL)
Blood is good for 4 hours once the bag is spiked
You may want to consider premedication with Tylenol and Benadryl

Blood Products
Consent for blood is not covered under the general ED consent for treatment
Under emergent conditions consent for blood must be obtained within 24 hours
Includes O- not just type specific
Usually obtained by the admitting service
Under less emergent conditions obtain consent upon ordering blood
Hard copies located in “STS Forms” binder on WOW or on Centerlink

Blood Products
Alaris
Can not warmed (consider hot line )
Two Units can be given before filter change
Use a Large Standard Blood filter 170-260 micron, then attach Alaris tubing.
Belmont
Gives rapidly and warms – no special filters needed
Filter does not need to be changed, can give approx. 70 units
Push/pull
Use with the hotline to warm blood

FFPpRBC Platelets
Shock +/- Acute ↓ Hb ≤ 7.0 INR >1.5 <50 x 109/L
Blood Products
Medical Management
Proton Pump Inhibitor In adults 80 mg IV loading dose and 8 mg/hr for 72 hours Reduces high-risk stigmata and need for endoscopic therapy if given pre-endoscopy (OR 0.67) Reduces risk of rebleeding, surgery and death in high-risk patients if given after endoscopy (RR 0.4 / 0.43 / 0.41 respectively)
H2 blocker Cheap + safe but poor ability to consistently maintain a high intragastric pH >6 No evidence for effect in acute bleeding

Octreotide Somatostatin analog that reduces portal venous inflow and intravariceal pressure
Considered if the patient is unstable due to volume loss and there is going to be some delay in getting to the PICU or OR
Reduce the risk of rebleeding in adult patients with variceal hemorrhage
Also may reduce the risk of bleeding due to nonvariceal causes
Initial bolus of 1 µg/kg (max 100 µg), followed by 1 µg/kg/hr continuous IV infusion
Medical Management
Vasopressin/Terlipressin Used in a similar fashion to octreotide
Beta Blockers In adults reduces risk of recurrent variceal bleedTitrate to 25% of resting HR reduction
Prokinetics (Erythromycin, Metclopramide)May improve visualization if given prior to endoscopy
Tranxemic Acidantifibrinolytic, may reduce mortality
AntibioticsIn adults with cirrhosis 20% have infections upon presentation with UGI50% develop one while hospitalized
Medical Management

Patients with airway compromise
Ongoing bleeding
Large bore tube for suctioning and decompression
NGTube

Per Fleisher
“All patients with a significant bleeding episode should have a nasogastric tube
placed for a diagnostic saline lavage”
Clinically significant = more than a teaspoon EBL
NG/OG lavage to confirm if ongoing bleeding
NGTube

If the lavage returns fresh blood or coffee grounds UGI or nasopharyngeal bleed
Red flecks or coffee grounds – LOW rate of bleeding
Bright red blood – FAST rate of bleeding
Lavage may not be positive if the bleeding has ceased or arises beyond a closed pylorus
Bilious fluid + no blood pylorus is open and no active UGI bleeding
NGTube
Specific technique of Saline lavage
Volume of saline
50 mL infants
100-200 mL older children
You really don’t need to perform lavage for greater than 10 min
Afterwards leave the tube to low wall suction
NGTube
Ice water lavage (an older practice) does not slow bleeding & may induce iatrogenic hypothermia

Do you think that we should perform saline lavage on upper GI bleeds?

NGTube
Recommendations from GI Faculty
NG recommended on a per-patient basis, not everyone
The result of gastric lavage doesn’t dissuade them from EGD when the blood has only been present as melena
Neurologically compromised + vomiting should get a large NG for suctioning/decompression of the stomach to limit potential for aspiration
28-36 French tube to evacuate
10-16 French salem sumps get clogged
Hard to gauge rate of bleeding

Diagnostic modality of choice for UGI bleeding
Determines source of bleeding for 90%
Goal within 24-48 of severe/acute bleeds
Safe in children
Endoscopy

Source Identification
RiskStratification
Therapeutic Intervention

Technique is lesion dependent
Diffuse mucosal disease = medical management
Focal source (ulcer, visible vessel)
Focal coagulation
Tamponade vessel (clip or band)
Endoscopy

The therapy applied depends on being able to find, see, and approach the lesion, the size of
the lesion and the size of the child - which determines which scope will fit and which
instruments will go through it.

Immediate control of hemorrhage with injection of epinephrine followed by a
coagulative or tamponading intervention (in adults, at least) limits the potential for rebleeding under most circumstances.
- Philip Putnam, Gastroenterology

Endoscopy
Balloon tamponade with a Sengstaken-Blakemore or Minnesota tube is 80% successful but has a higher rate of rebleeding and pressure necrosis
Sclerotherapy with sodium morrhuate is 90-95% successful and is often repeated q2-4 weeks
Variceal banding is comparable to sclerotherapy but is more difficult to perform in children because of the smaller esophagus

Endoscopy
When conservative management fails (multiple transfusions + meds + endoscopy) surgery is indicated
TIPS for intrahepatic portal hypertension to provide temporary decompression of the intrahepatic portal vein into the hepatic veins
Surgical portosystemic or portoportal shunts for refractory cases and/when liver transplantation is not an option
Sugiura procedure is rarely performed - removal of vessels of upper stomach and esophagus + splenectomy

Other studies
If endoscopy fails to identify bleeding source = arteriography
Can detect bleeding at a rate of 0.5 mL/min per minute
Allows for embolization and and intra-arterial administration of vasoconstrictors

Take Home Points

Most serious bleeds are variceal

NG Lavage is generally not necessary

Administer IV PPI early
Endoscopy is safe and effective

The End