Embed Size (px)
Citation preview

1
Changing representations of mosquito borne disease risk in Réunion.
by
Philip Weinstein
MB BS, PhD, FAFPHM
This thesis is presented for the degree of Master of Arts
of the University of Western Australia
School of Humanities
French Studies
2008

2
Declaration
This thesis contains no material which has been accepted for any award of any other degree
or diploma in any university, and, to the best of my knowledge and belief, it contains no
material previously published or written by another person, except where due reference is
made in the text of the thesis.
…………………………….
Philip Weinstein
Publications arising from thesis
This thesis contains work accepted for publication and work submitted for publication,
which has been co-authored. The bibliographical details of the work and where it appears
in the thesis are outlined below.
1. Weinstein P. and Ravi, S. (In press) The failure of colonial „distancing‟: changing
representations of the 2005-6 Chikungunya virus epidemic in Réunion. Singapore Journal
of Tropical Geography. Accepted 29/3/2007 (Chapter 3)
2. Weinstein P. and Ravi, S. (In review) Intersecting discourses on tropicality and disease
causation: representations of Réunion‟s mosquito borne epidemics in the scientific
literature. Asian Journal of Social Science. Accepted subject to revisions 22/5/08
(Chapter 2)
3. Weinstein P. and Ravi, S. (In review) Print media representations of an unusual health
event: Chikungunya virus, risk and identity on Réunion Island. Journal of Asian and
African Studies. Submitted 7/3/2008 (Chapter 4)
In recognition of her assistance with contextualising, motivating, and overseeing my work,
I have included my supervisor, Dr Srilata Ravi, as a co-author on each of the above papers
arising from the thesis. However, all of the work remains my own, except where
specifically acknowledged in the papers. I have the permission of Dr Ravi to include these
papers in my thesis.
……………………………. …………………………….
Philip Weinstein Srilata Ravi

3
“They will be so entranced by the beauty you have created that they’ll forget their
sustenance depends on the work of their hands. Watch while I arrange for men of the
future to remember the need for constant movement”, she said, and opened her hand to
release an enormous sandfly.
Hine-nui-te-po (Godess of Death) to Tu-te-rangi-whanoa (Creator of the South
Island), Maori creation myth, New Zealand (Reed 1977, p.6).

4
Abstract
In March 2005, the Indian Ocean island of Réunion, a former colony and now overseas
department of France, saw the first cases of what was to become a massive epidemic of the
mosquito borne viral infection Chikungunya. More than 250,000 people, one third of the
Island‟s population, were subject to high fevers, rash, and joint and muscle pains over the
next 18 months, yet the public health authorities in metropolitan France were arguably slow
to take the epidemic seriously. The research presented here explores attitudes underlying
the management of the epidemic by examining both metropolitan and local representations
of mosquito borne disease from historical, epidemiological and media perspectives.
The research seeks to answer the general question Does colonial history continue to
influence the representation and management of mosquito borne disease in Réunion?
Three parallel approaches are taken to answering this question, using a common framework
of tropicality (a Western discourse that exalts the temperate world over its tropical
counterpart, and overlaps with colonialism and orientalism). These three approaches are:
An exploration of the relationship between discourses of tropicality and paradigm shifts in
Western thinking about medicine, as represented in the contemporaneous scientific
literature; an examination of the extent to which discourses on tropicality and colonial
distancing can explain the slow reaction to the epidemic, as represented in the official
bulletins of the Institut National de Veillance Sanitaire (INVS); and an analysis of the
possible influences of colonialism and island identities on differences in print media
representations of the risk posed by the virus both in metropolitan France and in Réunion.
In the historical scientific literature, a transition is evident in the dominant scientific
understanding of disease causation from miasma theory (epidemics caused by unhealthy
air) to microbial theory (epidemics caused by transmission of microbes). In pre-microbial
representations, the unhealthy tropical environments thought to be responsible for
miasmatic disease transmission are associated predominantly with the non-white
population; in microbial representations non-whites are directly blamed for the spread of

5
tropical infections. These findings suggest that tropicalist thinking persisted through a
major paradigm shift in the Western understanding of disease causation, and supports
Said‟s contention that “Othering” is a generalisable ahistorical phenomenon.
In the official bulletins of the INVS, representations of the Chikungunya epidemic are
initially consistent with a centred tropicality: There is no perceived risk to metropolitan
France because of its non-tropical climate; there is no justification for costly control
measures for a disease that is inevitable in the tropics; and the symptoms of residents of the
tropics can be described in detached terms so as to generate knowledge about the disease.
However, when the perceived risk to metropolitan France increases, representations
become more consistent with a decentred tropicality: The concept of a protective
metropolitan French climate is abandoned; the need for whole-of-society involvement in
control measures is accepted; and symptoms are described using more inclusive language.
In the newspaper articles on Chikungunya, a considerable lag is evident between reporting
and the real-time evolution of the epidemic. In the Reunionese representations
(Témoignages and Clicanoo), there is a suggestion of passive denial of the public health
risk posed by the virus in the early stages of the epidemic, followed by acceptance with
blame attributed to the French metropolitan government. In the French metropolitan
representations (Le Figaro and Le Monde), an even greater delay may reflect the influence
of residual colonialist thinking on the priority placed on reporting on an epidemic in a
remote tropical location: Once a risk to metropolitan France is identified, reporting
intensifies considerably.
Thus each of the three approaches revealed representations (and changes in representations
with time) that were influenced by tropicalism and colonialism. Taken together, these three
pieces of converging and corroborative evidence provide strong support for answering the
research question in the affirmative: Colonial history does continue to influence the
representation and management of mosquito borne disease in Réunion. It appears likely
that these tropicalist attitudes contributed to the suboptimal management of the epidemic,
resulting in considerable preventable morbidity and mortality in the Reunionese population.

6
Several factors are likely to have contributed to the persistence of tropicality in public
health practice in Réunion: Othering as a universal phenomenon; the cost of administering
interventions to combat tropical diseases in the remote environments of French overseas
departments and territories; the denial of a serious public health risk as a cultural trait in
Réunion; and the significant rôle of the colonies in forming and maintaining the French
national identity. It has to be acknowledged that historically, tropicalism does appear to
have played one positive role in the management of mosquito borne disease: „Top-down‟
public health campaigns successfully eradicated malaria and dengue fever in Réunion.
However, the public health response to the Chikungunya epidemic was not as successful,
and led to an exacerbation of Reunionese feelings of resentment towards the metropolitan
French government.
This study is original in so far as it is multidisciplinary, drawing on discourses on
tropicality, public health, risk perception, and postcolonialism to interpret the findings. The
approach has provided insights that might not otherwise have come to light, highlighting
the value of the contribution that textual analysis can make to our understanding of public
health – particularly in providing information on what constitutes culturally appropriate
advice and acceptable forms of public health intervention. Regardless of our understanding
of the mechanisms of disease transmission in the physical space of tropical epidemics,
affected populations will continue to suffer a preventable disease burden until such a time
as the conceptual space of tropical Otherness is changed. Ongoing research collaboration
between the Humanites and Health Sciences can only help to bring such a time closer.

7
Table of contents
Declaration and Publications arising from thesis p. 2
Abstract p. 4
Table of Contents p. 7
Acknowledgements p. 8
1.0 Chapter 1 Introduction 1.1 Introduction p. 10
1.2 Approach p. 11
1.3 Historical and cultural context of representations p. 13
2.0 Chapter 2 Intersecting discourses on tropicality Intersecting discourses on tropicality and disease causation: representations
of Réunion‟s mosquito borne epidemics in the scientific literature. p. 16
3.0 Chapter 3 The failure of colonial ‘distancing’
The failure of colonial „distancing‟: changing representations of the 2005-6
Chikungunya virus epidemic in Réunion. p. 39
4.0 Chapter 4 Chikungunya virus, risk and identity
Print media representations of an unusual health event: Chikungunya virus,
risk and identity on Réunion Island. p. 64
5.0 Chapter 5 General discussion 5.1 The rôle of 'tropicality' in public health practice in p. 82
postcolonial societies.
5.2 Recommendations for further research. p. 85
6.0 Bibliography p. 88

8
Acknowledgements
Foremost I wish to thank my supervisor, Dr Srilata Ravi, whose particular ability to
imperceptibly train the student towards the goal whilst still capitalising on the student‟s
own ideas, is the main reason that this thesis has been completed in a timely and enjoyable
fashion. Other members of the School of Humanities have also contributed to making my
learning experience in this field a real pleasure; Gareth Griffiths, Andrew Hunwick, Hélène
Jaccomard, Tristan Kewe, John Kinder, Peter Morgan, and Rob Stuart. Thanks also to my
fellow students for their good humour and innumerable coffees, particularly Bénédicte
André, Chandra Eastwell and Lovisa Rosnäs. Additional acknowledgements for specific
assistance are included in the individual chapters.

9
Chapter 1
Introduction

10
1.1 Introduction
In March 2005, the Indian Ocean island of Réunion, an overseas department of France, saw
the first cases of what was to become a massive epidemic of the mosquito borne viral
infection Chikungunya - a name meaning “stooped over” in Swahili that reflects the
debilitating joint pains experienced by sufferers. More than 250,000 people, one third of
the Island‟s population, were subject to high fevers, rash, and joint and muscle pains over
the next 18 months, yet the public health authorities in metropolitan France were arguably
slow to take the epidemic seriously. My research explores attitudes underlying the
management of the epidemic by examining both metropolitan and local representations of
mosquito borne disease from historical, epidemiological and media perspectives.
The research seeks to answer the general question:
Does colonial history continue to influence the representation and management
of mosquito borne disease in Réunion?
Specifically, I ask:
1. Were discourses of tropicality affected by paradigm shifts in Western thinking about
medicine, and are any such effects reflected in representations of mosquito borne epidemics
in the contemporaneous scientific literature about Réunion?
2. Can discourses on tropicality and colonial distancing explain the slow reaction to the
2005-6 Chikungunya epidemic, as represented in the official bulletins of the Institut
National de Veillance Sanitaire (INVS)?
3. To what extent can residual colonialism and island identities influence differences in
print media representations of the risk posed by the virus, when comparing the content of
articles about Chikungunya from Reunionese newspapers with those from metropolitan
France?

11
1.2 Approach
To answer these questions, I analyse historical, epidemiological, and print media
documents. The study integrates a scientific context (allowing an evaluation of the
representation and management of the Chikungunya epidemic from the perspective of best
public health practice), within an historical, geographical and social context (allowing an
evaluation of the representation and management of the Chikungunya epidemic from the
perspective of tropicality and colonial discourse). This approach is original in so far as it is
multidisciplinary, drawing on discourses on tropicality, public health, risk perception, and
postcolonialism to interpret the findings.
Following the present Introduction (Chapter 1), the research findings are given as three
separate papers each addressing one of the specific research questions above:
Chapter 2: Intersecting discourses on tropicality and disease causation:
representations of Réunion’s mosquito borne epidemics in the scientific literature.
This chapter explores whether or not persistent tropicalism is evident in representations in
the scientific literature on mosquito borne disease epidemics that occurred on the island
before, during and after a paradigm shift in Western thinking about disease causation. I
argue that any persistence of tropicalist thinking through a major paradigm shift in the
Western understanding of disease causation would supports Said‟s (1979) contention that
“Othering” is a generalisable ahistorical phenomenon.
The chapter was submitted as a paper to the Asian Journal of Social Science, and at the
time of thesis submission had been accepted subject to revisions.
Chapter 3: The failure of colonial ‘distancing’: changing representations of the 2005-6
Chikungunya virus epidemic in Réunion.
This chapter analyses official reports on the epidemic from the bulletins of the Institut
National de Veillance Sanitaire (INVS), seeking evidence for any change in representations
during the course of the epidemic. I examine changes in representations from the

12
perspective of the risk posed by Chikungunya to metropolitan France; from the perspective
of the emphasis on control measures for the epidemic; and from the perspective of
descriptions of Chikungunya case symptomatologies, compared to parallel representations
of another epidemic, flu, already well known in metropolitan France.
The chapter was submitted as a paper to the Singapore Journal of Tropical Geography,
and at the time of thesis submission was in press.
Chapter 4: Print media representations of an unusual health event: Chikungunya
virus, risk and identity on Réunion Island.
This chapter explores possible reasons for the delay in reporting on the epidemic in the
print media. I analyse articles about Chikungunya from two Reunionese newspapers
(Témoignages and Clicanoo) and two newspapers from metropolitan France (Le Figaro and
Le Monde), comparing representations of the perceived risks posed by the virus in the
different articles.
The chapter was submitted as a paper to the Journal of Asian and African Studies, and at
the time of thesis submission was in review.
Following these three chapters, I provide a General Discussion (Chapter 5) that integrates
the findings from Chapters 2, 3 and 4 to draw conclusions about the rôle of 'tropicality'
in public health practice in postcolonial societies. Recommendations for further research
are included.
A full Bibliography of the references cited is provided at the end of the thesis.
The thesis covers representations of the epidemic in Réunion up to the end of 2006 when
the last local cases were reported. Subsequently the virus spread to Italy, confirming the
threat to metropolitan France discussed in Chapters 3 and 4 (ECDC/WHO 2007), and to
India, where at the time of thesis submission at least 1.4 million people had been infected
and more than 300 had died (Parmar and Ramani 2008). Chikungunya is now considered
an “emerging infectious disease” at the global scale (Charrel et al. 2007), precipitating
intense and ongoing research activity internationally.

13
1.3 Historical and cultural context of representations
La Réunion is a full (overseas) department of France, of which it has been an integral part
with the same administrative status as a Départment in metropolitan France since 1946. It
does considerably better economically than is average for France, with an economic growth
rate of 4.9% compared to 1.2% (2005 data; INSEE 2006, p.9). Expectations are therefore
that the minimum wage, social security payments, and availability of education and health
care in Réunion match the standards set by metropolitan France. These expectations have
partly been met: The minimum wage was brought to the same level as for metropolitan
France in 1996, but welfare payments are still 20% lower; literacy is at 89% compared to
99% in France; and the infant mortality rate of 7.63/1000 is much lower than that of
neighbouring Mauritius (14.59), but is still nearly double the rate in metropolitan France
(4.21) (CIA 2006). Although much improved over the historical situation, these figures do
suggest ongoing inequity – perhaps best illustrated by the unemployment rate, which at
over 30% in Réunion remains more than three times the rate in metropolitan France, and
the highest of any overseas department of France (INSEE 2006, p.125). The relationship
between the Reunionese, the majority of whom are of mixed race, and their fellow French
citizens in metropolitan France therefore might hide more persistent issues of
discrimination and dependence than is at first obvious. As with many „colonised‟
populations, discrimination against Créole Reunionese can persist either overtly or covertly,
fuelled by the vicious cycle of lack of educational opportunity and socio-economic
deprivation. To understand the evolution of this situation, it is important to appreciate the
colonial history of the island, of which a short summary therefore follows.
When first discovered by Malay and Arab mariners in the Indian Ocean in the 15th century,
Réunion was uninhabited, and they left it thus. The European discovery by the Portuguese
captain Pedro de Mascarenhas in 1512 also did not lead to settlement, and it was over a
century before the first human inhabitants actually took up residence - a dozen Frenchmen
of dubious reputation, living in a cave. Thus there were no inhabitants when the French
settled, no resistance to settlement, and no dispossessed and oppressed indigenous
population following „colonisation‟ (“l‟île vierge”, Vaxelaire 2002). African and Malagasy

14
slaves, imported to support the growth of the coffee industry from 1715, certainly were
oppressed, but not in any way that was different from the oppression of slaves elsewhere:
They could in fact be considered to have been (relatively) fortunate to have benefited from
the (relatively) benevolent rule of Mahé de la Bourdonnais, whose labour-saving
management enabled many slaves to move away from hard labour and into artisanry
(Combeau and Maestri 2002). These slaves provided the basis of the island‟s Créole
community, later to be joined by large numbers of indentured labourers for the island‟s
sugar cane industry, chiefly from India and China, following the abolition of slavery in
1848. A brief period of economic prosperity ensued, with standards of living improving
and the construction of roads and ports facilitating transport and communication. Later in
the 19th century the sugar crisis drove many small white landholders to retreat to the
mountains to engage in small-scale subsistence farming, along side freed slaves who had
now already adopted such a lifestyle. The resultant communities provided even greater
opportunities for ethnic mixing than already existed on the island, thereby further effacing
any historical „racial‟ boundaries. This socioculturally and ethnically diverse population
was then subject to successive crises – a series of serious epidemics including malaria and
cholera, and two world wars during which the isolation of the island was felt acutely.
Although living through these times together in many ways helped to unify the population
and develop a Reunionese identity, departmentalisation in 1946 was not uniformly
supported: A pro-independence movement has seen fluctuating popularity on the island,
unfortunately epitomised by anti-government demonstrations in 1991 that left 10 people
dead.
With this historical background, and despite the lack of an indigenous population per se,
the Créole community in Réunion has been and remains subject to the imposition of a
dominant French culture in a situation analogous to that of colonial occupation. Discourses
on tropicality and colonialism therefore provide useful frameworks within which to
contextualise and examine the changing representations of mosquito borne disease risk on
the island.

15
Chapter 2
Intersecting discourses on tropicality and disease causation:
representations of Réunion’s mosquito borne epidemics in the
scientific literature.
This chapter was submitted as a paper to the Asian Journal of Social Science, and at the
time of thesis submission had been accepted subject to revisions.

16
2. 0 Intersecting discourses on tropicality and disease causation:
representations of Réunion’s mosquito borne epidemics in the scientific
literature.
Abstract
In this paper we examine whether discourses of tropicality were affected by paradigm shifts
in Western thinking about medicine. If tropicalist thinking reflects latent Western
assumptions about the „Other‟, tropicalism should persist through major shifts in Western
thought. Here we explore whether or not such persistence is evident in representations in
the scientific literature of mosquito borne disesae on the Indian Ocean island of Réunion,
where discrete epidemics occurred before, during and after a paradigm shift in Western
thinking about disease causation.
Late in the 19th
century, miasma theory (epidemics caused by unhealthy air) was replaced
by microbial theory (epidemics caused by transmission of microbes) as the dominant
scientific understanding of disease causation. We analyse representations of mosquito
borne epidemics in the contemporaneous scientific literature about Réunion for evidence of
both tropicalism and a shift in scientific paradigm. In pre-microbial representations, the
unhealthy tropical environments thought to be responsible for miasmatic disease
transmission are associated predominantly with the non-white population; in microbial
representations non-whites are directly blamed for the spread of tropical infections.
The paper argues that the persistence of tropicalist thinking through a major paradigm shift
in the Western understanding of disease causation supports Said‟s (1979) contention that
“Othering” is a generalisable ahistorical phenomenon, and discusses issues of economic
exigency that may have supported an ongoing tropicalist influence on public health practice
in French overseas departments.

17
Introduction
Tropicality is a Western discourse that “exalts the temperate world over its tropical
counterpart” (Bowd & Clayton, 2005: 297). It has clear overlaps and synergies with
colonialism and orientalism, parallel discourses that provide what McLeod (2000: 37)
succinctly summarises as a justification for “the possession and continuing occupation of
other people‟s lands”. Tropicality supports Western temperate countries‟ assertions of
superiority over their tropical (often developing) counterparts, and reinforces the
representation of the tropical world as the negative “Other” – a concept crystalised by Said
(1979) which refers to an identity constructed out of those projected negative aspects of a
society from which that society wishes to disassociate or distance itself (Mills, 1997: 106;
Edgar & Sedgwick, 1999: 266). Thus Western societies tend to distance themselves from
ignorance, weakness, and, importantly for this paper, epidemic disease. Arguably the
major criticism of Orientalism (and implicitly therefore also of Tropicalism) as conceived
by Said (1979) is that it provides an ahistorical interpretation of representations drawn from
a vast range of temporally (and geographically) disparate sources. It could be seen as
unreasonable to expect that such a massive archive of materials could be readily
homogenised, attending “little to individual historical moments, their anomalies and
specifics” (McLeod 2000, p. 47, emphasis in original). One such “individual historical
moment” is the late 19th
century transition from the then dominant miasma theory of
disease causation to a theory of contagion to explain the occurrence of epidemics. If Said is
right, then representations of epidemic tropical disease should reflect similar latent western
assumptions about the tropical „Other‟, regardless of the perceived scientific cause of such
disease. By contrast, if individual historical moments do change western assumptions
about the „Other‟, one might expect representations of epidemic tropical disease in the
historical scientific literature to undergo a significant transformation when contagion theory
gains supremacy over miasma theory late in the 19th
century. In this paper, we look for
possible changes in the representation of mosquito borne disease on Réunion Island, where
discrete epidemics occurred before, during, and after the transition in medical thinking. We
examine representations in the contemporaneous scientific literature corresponding to the
emergence of each of four mosquito borne diseases on the island, from the first paper on

18
filariasis in 1756, to publications available on chikungunya at the end of that epidemic in
late 2006.
Based on a distillation of older concepts, two main theories of epidemic disease causation
were current in the early 19th
century: the miasma theory, and the theory of contagion. The
miasma theory held that „bad air‟ – mala aria to the Romans – was responsible for both
causing and maintaining high disease rates in particular locations at particular times.
Strongly supportive evidence came in the form of correlations observed between sewage,
swamps and other unsanitary conditions and a high prevalence of dysentery, malaria and
other diseases. The Romans had noted such a correlation two millennia earlier, leading
them to found their capital on two of seven „healthy‟ hills with plenty of fresh air, and
leaving the swampy and malaria-ridden Tiber valley below to those less fortunate (Sallares
2002). The theory of contagion, by contrast, held that epidemics resulted from the spread of
specific, living, but invisible (to the naked eye) organisms, or contagions – microbes now
recognised as viruses, bacteria, protozoa, and other pathogens. It was as a result of
contagionist thinking that John Snow famously had the pump handle removed from the
Broad Street pump in London during the 1854 cholera epidemic: By completing some of
the earliest epidemiological investigations, Snow had concluded that cholera was caused by
a water borne contagion, and, brilliantly for his time, devised this appropriate public health
intervention without the benefit of laboratory backup (Kiple 1997). That backup became
available over the next few decades however, and the meticulous experimental approach
developed by Louis Pasteur and others ensured that by the 1870s, the understanding of the
relationship between specific contagia and disease epidemics was past the point of no
return: The theory of contagion gained the upper hand over miasma theory, with the latter
virtually disappearing from the western scientific scene by early in the 20th
century.
In examining representations of epidemics before, during, and after this “scientific
revolution” (Kuhn, 1962), it is important to remember that discourses on disease causation
were not informed by scientific evidence alone. The standpoint taken was strongly
influenced by political, economic and social factors. Contagionism “found its concrete
expression in the institution of quarantine and its officialdom” (Rosen 1993 p. 266), and

19
was unpopular with merchants and industrialists because it limited business opportunities
(1). Thus “an attack against contagionism was a blow against bureaucracy and for
freedom” (ibid.), and many liberal reformers (especially middle class physicians) were
therefore anti-contagionists. The imposition of quarantine can affect island communities
particularly severely because they are vulnerable in terms of their dependence on external
supplies, and non-scientific factors are therefore likely to have influenced especially the
public health practitioners dealing with epidemics in islands like Réunion. Many of these
doctors were particularly fearful of epidemics because of the immediate suspension of
access that they entailed; not only to Réunion but between the extensive network of French
Indian Ocean Territories at that time (Lougnon 1944, p.19).
Of particular interest in this paper is the effect of the change in paradigm of disease
causation, as an “individual historical moment”, on discourses on tropicality: The scientific
literature on mosquito borne disease epidemics in Réunion allows us to look for such a
relationship because of the fortuitous historical timing of different epidemics. A
description of this historical context follows, and we then go on to analyse the
representations of mosquito-borne disease epidemics in chronological order from pre-
contagionist to contagionist. We finish by integrating our findings in terms of the possible
persistence of tropicality in Western thought.
Historical context of representations of Réunion epidemics
When first discovered by Malay and Arab mariners in the 15th
century, the Indian Ocean
island of Réunion was uninhabited, and they left it thus. The European discovery by the
Portuguese captain Pedro de Mascarenhas in 1512 also did not lead to settlement, and it
was over a century before the first human inhabitants actually took up residence - a dozen
Frenchmen of dubious reputation, living in a cave. Thus there were no inhabitants when
the French settled, no resistance to settlement, and no dispossessed and oppressed
indigenous population following „colonisation‟. African and Malagasy slaves, imported to

20
support the growth of the coffee industry from 1715, certainly were oppressed, but not in
any way that was different from the oppression of slaves elsewhere: They could in fact be
considered to have been (relatively) fortunate to have benefited from the (relatively)
benevolent rule of Mahé de la Bourdonnais, whose labour-saving management enabled
many slaves to move away from hard labour and into artisanry (Combeau and Maestri
2002). These slaves provided the basis of the island‟s créole community (3), later to be
joined by large numbers of indentured labourers for the island‟s sugar cane industry, chiefly
from India and China, following the abolition of slavery in 1848. The Créole community
was (and arguably remains) subject to the imposition of a dominant French culture in a
situation analogous to that of colonial occupation, and discourses on tropicality can
therefore provide the context for our examination of representations of mosquito borne
epidemics in the scientific literature.
As with many „colonised‟ populations, discrimination against Créole Reunionese persists
either overtly or covertly, and is fuelled by the vicious cycle of lack of educational
opportunity and socio-economic deprivation. Not surprisingly then, the créole population
of Réunion has also suffered a disproportionate share of the disease burden, including that
from mosquito borne epidemics. Since settlement in 1646, the Reunionese were subject to
four mosquito borne diseases that appeared epidemically: Lymphatic filariasis, malaria,
dengue, and chikungunya. A review of the progressive introduction of the first three of
these diseases into Réunion is provided by Julvez et al. (1998), and a brief description of
each follows below. The transmission of all four diseases depends upon humans being
infected with microorganisms from a mosquito upon being bitten, these microorganisms
having completed part of their lifecycle in that mosquito:
• Filariasis, an infection with parasitic nematodes of the genus Wuchereria. Blockage of the
lymphatics can result in classical elephantiasis with swollen limbs. The disease is likely to
have been introduced with the first sailors and settlers, from 1646.
• Malaria, an infection with parasitic protozoa of the genus Plasmodium. The presence of
Plasmodia in the bloodstream results in classical cyclical fevers. The first Réunion
epidemic occurred in 1869.

21
• Dengue fever, an infection with a virus of the family Flaviviridae. High fever and severe
pain has resulted in the name “break-bone” fever for this disease. The first Réunion
epidemic occurred in1873.
• Chikungunya, an infection with a virus of the family Alphaviridae. The name means
“bent over” in Swahili, referring to the posture adopted by sufferers in order to minimise
the severe joint pains. The first Réunion epidemic occurred in 2005.
These dates of first appearance are listed in Table 1 to facilitate a comparison of the timing
of epidemics with key developments in Western scientific thinking about mosquito borne
disease. As can be seen, the chronological sequence of first appearances of the four
diseases in Réunion provides natural examples of mosquito-borne epidemics before, during,
and after the transition in scientific thinking from miasma theory to contagionism at the end
of the 19th
century. Miasma theory was dominant for over 200 years of the island‟s early
history of mosquito borne disease, with the first important turning point provided by the
discoveries of Alphonse Laveran, then a surgeon with the French armed forces serving in
Algeria. He discovered the malarian parasite in human blood in 1880, but its mode of
transmission remained unsubstantiated. Building on the views of several prominent 19th
century researchers who had suggested a role for mosquitoes in the transmission of malaria
(including Laveran himself, the German bacteriologist Robert Koch, and others), Patrick
Manson clearly articulated a mosquito-borne hypothesis for malaria in 1894. The then
London-based Manson (now considered the „Father of Tropical Medicine‟ (3)), inspired
Ronald Ross to test his hypothesis. Ross was also a surgeon with the armed forces, but
serving with the British in India. His breakthrough came in 1897 when he demonstrated
the (Plasmodium) parasite in the gut wall of the (Anopheles) vector mosquito, cementing its
role as a vector and providing an important victory for the theory of contagion (4). We now
proceed to summarise relevant extracts from the contemporaneous scientific literature
published before this victory (pre-contagionist) and after (contagionist); transitional period
is inevitable between these two groupings, neither of which is of course absolute.

22
Pre-contagionist representations of tropicality
The earliest documentation of (what is now known to be) mosquito borne disease in
Réunion is that of Couzier (1757) who mentions lymphatic filariasis (éléphantiafis [sic] p.
408). In his description the symptoms of syphilis are not clearly differentiated from those
of filariasis (and possibly also leprosy), but two general themes nevertheless show through
about his general construction of disease aetiology: The lifestyle of the African créoles as
well as the (tropical and volcanic) environment in which they live are both largely to blame.
Intemperance, excessive coffee consumption and the culture-specific purification rituals are
variously mentioned as contributing to disease causation, and although only by implication,
these habits are assumed to differ sufficiently from those in metropolitan France that a
different (tropical) disease pattern results. Unlike subsequent authors (below), Couzier is
not derogatory about the local inhabitants, but his blaming of disease on the behaviour and
practices of those affected is consistent with what in modern public health terms could be
described as victim blaming: A construction of disease causation that places responsibility
for the disease or condition on the sufferer rather than on the society in which the situation,
for example drug addiction, has arisen. Such victim blaming can be seen as a form of
„Othering‟, and is therefore consistent with tropicalist thinking, especially as it is being
applied to a population demonstrating a different disease pattern on a tropical island.
Barat (1869), writing about the island‟s first malaria epidemic, reports that despite excellent
distribution programmes for the anti-malarial quinine as well as of fortifying staple foods
(p.436), these interventions were ultimately doomed because of poor uptake by the non-
white population and because the convalescent continued to live in the unhealthy
atmosphere of their tropical swamps (pp.436-7). Although Barat is not here overtly
judgemental, there is an implicit element of blaming the non-white population for not
conforming to the best-practice Western medical intervention made available, and for
possibly perpetuating the epidemic cycle by maintaining the unhealthy human-environment
link upon which the spread of the disease depends. His writing here highlights the effect of
miasma theory on representations of the local population. Consistent with thinking at the
time he does blame environmental change and climate for the disease (“…un marécage

23
dont l‟existence suffit pour expliquer les manifestations de la fièvre…”; p. 426), but he
makes clear the observation that general health (including nutritional status) affects
susceptibility to the disease. He therefore includes a consideration of socio-economic
status in his discussion, and identifies as particularly vulnerable those [non-white] Créoles
that have been dispossessed of land, and affected by economic downturns in the sugar
industry as well as crop failure (“… la plus affreuse misère…”; p 427). He also describes
the serious impact of the disease at the community level, where whole families are rendered
helpless once the chief bread winner is struck down. Again there is no blame, and indeed he
is empathetic in his observations that these unfortunates (“malheureux”) are stoical in the
face of such a predicament (“…attendaient patiemment une solution par la mort ou la
guérison.”; p 432). Nevertheless, his statements about [non-white] Créoles not accepting
„Western‟ quinine, preferring instead their own herbal remedies like Madagascar
Periwinkle (Vinca rosea) (“...inspirait une grande confiance aux créoles”), reflect the
prevailing understanding of Western science and medicine as superior to the „primitive‟
healing practices of the „indigenous‟ population.
Showing somewhat less empathy for the affected population is Cotholendy (1873), writing
only four years later about the island‟s first epidemic of dengue fever. He explains that if
the disease had arisen spontaneously in situ (from bad air, consistent with miasma theory),
then that would not be surprising because dengue does this in India, and migration from
India is moulding the Réunion environment in its own image (“…l‟immigration est en train
de façonner à l‟image de la mère patrie”; p 192) – that is, replicating the unsanitary
environment in which miasmata arise. He goes on to clarify that such change is the result
of the lack of basic hygiene amongst the Indian migrants (“..cette race qui paraît rebelle aux
préscriptions les plus élémentaires de l‟hygiène…”; ibid), and leans towards a conclusion
that the disease was in fact imported either from Mauritius or India (more consistent with
germ theory) (p.192). Here, a shift in thinking about disease causation has facilitated a
change in representation of indentured labourers, who are increasingly implicated in disease
spread and blamed for the importation. Writing only shortly after Barat, it is obviously
possible that these differences in representation are simply a result of individual differences
between the two authors – but regardless, there is at this time a clearly tropicalist element to

24
the perception of the causation of epidemics: Even if Mauritians and Indians were not to
blame for the importation (contagionist), non-whites are still represented as either
modifying or maintaining the local environment in such a way as to enhance the spread of
disease (miasma theory).
The papers above, and others on mosquito borne disease in Réunion from the same time
period, all reflect authors with a solid grounding in pre-contagionist theories of disease
causation and epidemic spread, but slowly starting to incorporate elements of contagionism.
Couzier‟s (1757) paper was written about a century before Pasteur, and as expected his
aetiological descriptions reflect, above all, a belief in miasmata. He attributes a variety of
acute ailments (including dysentery) to the permanent presence of volcanic fumes (p. 402),
and suggests that the hot climate is contributory. He does mention theoretical “germs”
(“germe”, p. 408) and contagion, but given that these concepts first appeared in antiquity,
their mention does not conflict with the dominance of miasma theory. The later writing of
Trelat (1864), also discussing lymphatic filariasis (then “tumeurs lymphatiques”), still
shows a clear Pre-contagionist mark: He compares the high frequency of cases in Réunion
(5) to the rarity of cases in France, and concludes that location and climate are the primary
aetiological agents in the development of the disease (“…prouve bien en faveur des
conditions étiologiques de pays et de climat”) (p.309). Interestingly, Trelat‟s conclusions
can also be interpreted as reflecting climatic determinism, which despite a paradigm shift in
the understanding of disease causation, persists into the mid-20th
century where it forms a
cornerstone of the French school of tropical geography (see for example Gourou, 1947).
Trelat is in part correct of course, in so far as tropical conditions do favour mosquito borne
disease transmission. However, the apparently spontaneous demise of filariasis in Réunion
demonstrates that living standards, not climate, are the over-riding aetiological determinant
of the prevalence of filariasis; without any specific control campaign against filariasis in
Réunion, the disease changes from being highly prevalent (up to 10% of the population
infected) in 1892, to being virtually completely absent a century later (Brygoo et Brunhes
1971).

25
During the transitional period in the late 1800s, miasma theory and contagion theory were
not seen as mutually exclusive, nor was either theory inconsistent (obviously) with
empirical observations. Thus, Barat‟s description of the 1869 malaria epidemic as being
centred on a pond and spreading throughout the lowlands (“...avait son principal foyer à
l‟étang …; s‟irradiait dans toute l‟étendue des terrains plats...”; Barat 1869 p.422) is
consistent both with the then prevalent miasma theory and with our current scientific
understanding of mosquito-borne disease: In the former case unhealthy atmospheres would
generally be associated with stagnant waters in ponds and swamps, dispersing with the
wind in all directions (but not up to higher ground); in the latter case stagnant waters would
permit a build-up of mosquito numbers to a point where epidemic malaria transmission was
possible once the Plasmodium parasite was introduced into the island.
As an interesting and important aside, Barat (ibid.) makes insightful suggestions for
environmental management of malaria on Réunion that are well ahead of his time. The
future, he suggests, lies in rehabilitating the environment to remove the disease-causing
swamps (p.438) – and he identifies here a story that is all too familiar in environmental
health circles nearly 150 years later: In the rush for more agricultural land on which to grow
high profit crops, the island‟s slopes were denuded of their forests with no consideration for
the future (“… sans la moindre inquietude pour l‟avenir”; p. 438). The ensuing soil erosion
clogged and diverted water courses to create vast swamps, spoiling what was once an island
so „healthy‟ that it was used as a malaria-free recuperation stop by mariners and troops that
had been afflicted with the disease in Africa or Madagascar (6). From this perspective, it
could be argued that miasma theory was (although for the wrong reason) more consistent
with sustainable ecosystem management than is the „technological fix‟ approach to
mosquito borne disease developed as a result of the identification of Plasmodium in malaria
sufferers and later in mosquitoes (Laveran and Ross respectively, See Table 1) (7). For
Réunion, these later interventions are elegantly summarised by Hamon and Dufour (1954),
and focus principally on cure (quinine) to eradicate the parasite from the human population,
and insecticidal (DDT) eradication of the vector – both chemical rather than environmental
interventions.

26
Cotholendy (1873) is another author who attributes epidemics to environmental conditions,
but he does favour the hypothesis that the first dengue epidemic was caused by imported
germs; he explains that this could be possible because such germs can remain viable for
months or even years (“…la propriété qu‟ont les germes contagieux de conserver leur
puissance d‟action pendant des mois et même des années.”; p.194). In an elegant
compromise, imported germs are seen as being potentially spread by unhealthy climatic
conditions (not mosquitoes).
Contagionist representations of tropicality
We have seen above that in pre-contagionist representations of what we now know to be
mosquito borne disease epidemics, the tropical environment is seen as largely responsible
for disease transmission, with an element of blaming certain (predominantly non-white)
populations for modifying that environment to render it more susceptible to disease. We
now go on to explore similar representations in the contagionist literature that follows the
paradigm shift in Western scientific thinking about disease causation.
Writing in 1944, well into the microbial era but long before the eradication of malaria in
Réunion (refer Table 1), Lougnon provides an ethnographic component in his summary of
diseases in Réunion. He highlights not only he importance of understanding the island‟s
racial groupings, but the relevance of their countries of origin. Chinese are for example
described as having a total lack of hygiene, and Indians are given first place as drivers of
disease on the island: They are “dirty and ignorant of even the most basic rules of hygiene”
(sales, ignorant les lois les plus élémentaires de l’hygiène, p.11), and are also responsible
for importing the worst epidemics. By way of comparison to the Comores, other (then)
French Indian Ocean islands that at the time of colonisation were inhabited by an
indigenous Black African population, the indentured labourers on Réunion are actually let
off lightly: Raynal (1928) writes about the indigenous Comorians during their first
outbreak of Malaria, describing them as thieving sloths with deplorable hygiene and an
unintelligent approach to Islam (“...très voleur, indolent et paresseux; ...hygiène

27
détestable…”; p. 37) (8). Based on such a scathing representation of „colonised‟
populations during mosquito borne disease epidemics, it would appear that the dramatic
advances in discourses on disease causation that characterise the turn of the 19th
century are
not matched by similar advances in colonialist and tropicalist thinking; rather, tropicalism
appears to have been strengthened by the advent of germ theory, with a growing element of
victim blaming whereby the sufferers are held responsible for their own predicament.
Some positivity does return when DDT becomes available to eradicate malaria after WWII,
and Hamon and Dufour‟s (1954) description of the malaria control is noticeably more
objective than the scientific papers cited above. However, the contagionist victim blaming
is still prominent in their writing, and they attribute the primary cause for the high malaria
mortality in Réunion to the population‟s generally poor sanitation and ignorance of the
mode of transmission (p.537). It is interesting to ponder the degree (or lack) of penetration
of germ theory into the island‟s non-European communities in this context; although
contagionism has by this time been universally adopted in European-educated circles,
alternative belief systems of mosquito borne disease causation were obviously still
prevalent in non-European communities at this time, and may remain as high as two-thirds
of the population today (Gaüzère and Aubry (2006), p. 25) (9).
Moving now to the present day outbreak of Chikungunya virus, Gaüzère and Aubry‟s
(2006) book Le chik, le choc, le cheque is probably the most comprehensive publication
produced about a mosquito borne epidemic on the island, and was written in response to a
need for information about the 2005-6 outbreak. Although directed more at the educated
public than a scientific readership, the book nevertheless provides some valuable
representations of the epidemic to inform our analysis. The jacket summary states that the
outbreak of this virus with a “cannibal name” (nom cannibale) has forced the European
outpost of Réunion to reconnect with its tropical roots, and highlights the possible threat
posed to Europe should the virus be inadvertently transported there. In the introduction (p.
12), the epidemic is described as exotic, unknown and from terra incognita (tierra
incognita [sic]), and as an ancestral secret of a distant black people (secret ancestral de
peuplade cafre si lointaine). People opposed to insecticidal spraying of mosquitoes are

28
described as recalcitrants and rebels (p.67), and there is also little toleration of „alternative
medicine‟ approaches to treatment: Although the possible value of some herbal remedies is
acknowledged (Morinda sp., p.58), other clearly local practices (bracelets, earrings,
piercing) are mentioned only dismissively in passing (p.88).
In the official epidemiological reports on the Chikungunya epidemic produced by the INVS
(Institut National de Veillance Sanitaire), it has already been shown that tropicalism and
colonial distancing persist in representations of risk posed by Chikungunya to metropolitan
France; in the emphasis on control measures for the epidemic; and in descriptions of
Chikungunya case symptomatologies (Weinstein and Ravi, in press).
All of these authors are writing in what is unquestionably the microbial era: The parasites
and viruses responsible for the epidemics are named, the mosquito and its control are
integral to every paper, and a Western pharmacotherapeutic approach is adopted. In
Gaüzère and Aubry‟s (2006) book the scientific content per se is state-of-the-art, drawing
on modern virology, serology, epidemiology and vector ecology. From a public health
perspective, it is fascinating to see such rapid development in representations of scientific
fact without a parallel attenuation of tropicalism. Rather, once mosquitoes have been
established as disease vectors, „tropical‟ people can be seen as a disease reservoir that can
be directly blamed for transmission, an Other which threatens the healthy identity of the
metropolitan Self. The final picture is therefore one of tropicalist thinking persisting well
beyond the “individual historical moment” of a paradigm shift in theories of disease
causation, and into the present day of emerging infectious diseases like Chikungunya.

29
Persistence of Tropicalism
The pre-contagionist representations discussed in this paper attribute the epidemics of
filariasis, malaria and dengue on Réunion to the tropical nature of the country, climate, and
people, and are consistent with tropicalism in “Othering” such diseases from temperate,
metropolitan France: Tropicalism, like colonialism, distances Western societies from the
implicit ignorance and weakness associated with „tropical‟ diseases amoungst the „natives‟.
The contagionist representations that followed appear to build on this theme, adding an
element of directly blaming (non-white) tropical people for transmitting the infections –
focussing attention “more on the native subject as disease carrier than on the tropics as a
pathological site” (Edmond, 2005, p. 181) (10). A disease-based scientific rationale was
now available for racial segregation, and tropicality thus uses contagionist theory to
reinforce racism (11). Our analysis clearly demonstrates the persistence, indeed growth, of
tropicalist thinking through a major paradigm shift in the Western understanding of disease
causation. This finding suggests that tropicalism, like orientalism, reflects latent Western
assumptions about the „Other‟ and supports Said‟s (1979) contention that “Othering” is a
generalisable ahistorical phenomenon.
Apart from the need to reinforce dominance and superiority over the Other as above, the
strength and persistence of tropicalist (and colonial) thinking in French society can possibly
be partly explained by the economic challenge of maintaining tropical departments and
territories overseas. Departmentalisation of Réunion has come at a great expense to France
because of the need to match the minimum wage, social security payments, and availability
of education and health care to the same standard as is available in metropolitan France.
This financial challenge also proves to be an important determinant of attitudes and
approaches to public health management: If tropicalist public health attitudes were formed
by a need to create an inferior, ignorant and diseased “Other”, then they were maintained
by a need to restrict public health expenditure in widely dispersed, costly environments
(12). Medical expenditure in British Asia was for example originally outlaid only to

30
protect the health of civilian and military members of the colonial administration, and the
high cost of genuine public health programmes targeting the entire population were only
seen as justifiable once it became important to protect the labour market in the late 1800‟s
(Sinha, 2004 p.202). Despite the inhabitants of DOMs theoretically being full and equal
citizens of France (13), public health expenditure was never equal to that in metropolitan
France. A well-funded and successful malaria eradication campaign in France in the
middle of the 20th
century was less adequately replicated in Réunion. Although also
ultimately successful, the Government-funded campaign in Réunion in the 1950‟s suffered
serious constraints that are clear from contemporaneous writing: Budgeting constraints
hampered progress through staffing restrictions, and the programme was not coordinated by
an (expensive) medical specialist as was the case in (closer to home) Corsica; no dedicated
laboratory support was funded (Hamon and Dufour 1954 p.531); and field operations were
often of less than ideal duration because of the limited means at the disposal of control
teams (“…en raison du peu de moyens dont nous disposions”, ibid. p538). More recently,
in 2006, Chikungunya virus was added to the notifiable disease list (14) for Metropolitan
France, Corsica and the French Antilles, but was not included on the list for Réunion where
the outbreak occurred (INVS 2006a, 2006b)! The only possible reason for this apparent
paradox is that the large number of cases in Réunion would necessitate the employment of
additional local epidemiology and laboratory staff to confirm and follow up cases. It is fair
to note however that this is not a uniquely „colonial‟ phenomenon, in so far as many
western countries do not include influenza on their notifiable disease lists for the same
reason – the sheer number of cases would swamp limited State epidemiology services.
Nevertheless, colonialist and tropicalist thinking have continued to influence public health
expenditure and management in DOMs (Weinstein and Ravi 2007), and local populations
are therefore still more likely than their fellow metropolitan citizens to be subject to a
preventable disease burden as a result of limited public health expenditure.
The persistence of tropicalism is such that it has survived the inevitable demise of the
French colonial empire – an end that has always been accepted as inevitable in France, but
vaguely placed so far into the future as to be indeterminate (Girardet 1972 p.298). It was to
be considered only once the colonised peoples had “matured” (“…auraient atteint leur

31
« maturité »...”) and once the gap between the colonies and metropolitan France had been
closed (“…lorsque serait effacé le décalage qui les séparait de la métropole…”) (ibid.
p.298). This is perhaps tropicalist and colonial thinking at its best, providing clear
justification for the “possession and continuing occupation of other people‟s lands”
(McLeod 2000: 37). But implicit in these statements is therefore also a responsibility on
the part of the colonising power to protect, educate and promote „their‟ colonial subjects –
Girardet‟s (1972 p.344) “devoir de protection”. Soustelle (head of the colonial government
in Algeria in the 1950‟s) expressed this French colonial „responsibility‟ in terms of an
unbearable shame that would result from “abandoning” the colonised people prematurely
because of their cost [both figurative and literal] to France (“… la honte insoutenable que
signifierait pour notre pays l‟abandon des musulmans d‟Algérie parce qu‟ils nous coûtent
cher”; cited in Girardet 1972, p.345). Such a perceived responsibility extends easily to a
duty of care from a public health perspective and therefore also entails considerable
expenditure on public health infrastructure. Despite being in direct conflict with the
tropicalist tendency to victim-blame, the expectation of expenditure on tropical public
health interventions is thus ingrained ideologically in France – even if it is somewhat more
difficult to translate into practice.
We have shown that tropicalist thinking persists through a paradigm shift in theories of
disease causation, and it is therefore of interest to further discuss the intersections and
mutual influences between these discourses. Discourses on disease causation were
themselves affected by tropicalist thinking in so far as indentured labourers being blamed
for importing epidemics as part of the unhealthy Other also supported a contagionist
approach. Labourers were therefore often quarantined on arrival, whereas crews were
admitted directly to Réunion (Lougnon, 1944 p.18) – a discriminatory practice and
ineffective form of quarantine in the context of our current understanding of microbial
transmission, but nevertheless a significant step away from miasma theory. Here societal
factors can be seen to be influencing scientific thinking in favour of contagion theory,
whereas an earlier example of liberal reformers demonstrated societal factors influencing
scientific thinking in favour of miasma theory. Societal influences on scientific thinking
were thus not unidirectional, and can be construed as reciprocating the influence of shifting

32
scientific paradigms of disease causation on the broad realms of politics, economics, and
sociology. An example of disease causation theory affecting tropicalist thinking is afforded
by the successes of Laveran, Ross, and others at generating knowledge about tropical
diseases, which served to cement the perceived superiority of Western scientific rationalism
over indigenous belief systems. The military medical services of both the French (Laveran)
and English (Ross) were instrumental in such „progress‟, thereby also rationalising an
ongoing military presence to help colonial powers „civilise‟ the diseased citizens of their
tropical colonies. Discourses on tropicality and disease causation were thus intersecting and
mutually influenced.
In this paper, we have focused on the scientific literature contemporaneous to the various
epidemics, because it is in this writing that the paradigm shift in disease causation is likely
to be most clearly represented. The presence of tropicalist representations in the more
„objective‟ scientific papers studied here is therefore all the more significant in that it offers
a reliable window on society more generally; we can be confident that if tropicalist
representations persist through a scientific revolution in the writings of scientists, then such
representations are likely to accurately reflect persistent tropicalist thinking in wider
western society. Further, because the writers are trained in objective observation, and
because, having experienced life on the island first hand, they are writing in the literary
genre “Littérature des colons” their representations are relatively free from the exotic
fantasies of travel writers. These latter non-scientific writers do reflect miasma theory in
their writing about the health benefits of the Réunionese environment (…“bonnes
exhalaisens qui sortent continuellement de la terre et des plantes..”; cited in Joubert 1991,
13.1), but the overlay of „rediscovered Eden‟ and similar elements of the authors‟ mental
landscape makes a parallel analysis of literary sources a task beyond the scope of the
present paper.
The final word should perhaps go to Arnold (1996), who observes that despite a scientific
revolution that led physicians to “eschew climate and topography in favour of bacilli and
protozoa, there remained a sense in which the physical and social peculiarities of Africa,
Asia and the central regions of the Americas, continued to inform the medical discourse

33
and praxis” (p.10). Tropicalism seems destined to remain part of Western medical thinking
until such a time as the conceptual space of tropical Otherness is changed, regardless of our
understanding of the mechanisms of disease transmission in the physical space of tropical
epidemics.
ENDNOTES
(1) Cotholendy (1873) describes the 10-day quarantine imposed on ships arriving from
Mauritius to prevent the importation of dengue: He complains that cargoes are not
quarantined for longer or fumigated, given that germs are thought to remain viable for
much longer than the quarantine period (pp. 194, 208), suggesting the power of commercial
interest over scientific logic.
(2) In the late 1700‟s, slaves escaped in significant numbers to settle in the rugged interior,
electing their own chiefs to head their villages (“les marrons”). The hunting down of these
chiefs by bounty hunters caused a deep resentment of the French authorities by the créole
community, and it could be argued that these communities had been „translated‟ into the
equivalent of an indigenous population, fighting to reclaim „their‟ land and their autonomy.
Young (2003) describes the process of creolisation as a two-way translation involving an
evolution away from an original identity, and a cultural interaction that leads to both
cultures taking on elements of the other (p. 142). Therefore, we are seeing here not only
the birth of a Reunionese Créole culture, but also an incremental differentiation between
Reunionese French and Metropolitan French.
(3) In an interesting twist of fate, Patrick Manson rose to fame as the leading exponent of
tropical medicine of his time only after his financial situation prevented him from retiring:
He practiced tropical medicine in China for 20 years in relative obscurity, but rose to fame
after reluctantly setting up a practice in London rather than retiring to Scotland (Arnold
2003).

34
(4) A detailed historical review of the people, geopolitics, and science involved is provided
by Gordon Harrison in Mosquitoes, Malaria, and Man: A History of the Hostilities Since
1880, EP Dutton, New York, 1978.
(5) Trelat uses the name Ile Bourbon. The island was known initially as Mascarin, was
renamed Ile Bourbon after being officially claimed by France in 1649, then renamed
Réunion after the French Revolution but for a brief period was also known as Ile
Bonaparte. The modern name Réunion is used here throughout in the interest of simplicity.
(6) Such a recuperation stop allowed malarious sailors to recover in a disease-free
environment, but obviously in so doing exposed local mosquito populations to the
Plasmodium in the sailors‟ blood streams, creating the risk of seeding a local epidemic.
The approach is fundamentally different from quarantine, where diseased crews are kept on
board ship well off shore specifically to prevent epidemics from spreading to the population
in the receiving port.
(7) For an example and for a simple summary of the importance of an ecological approach
to managing mosquito borne disease epidemics, see Weinstein (1997) and Weinstein (2005)
respectively.
(8) Raynal (1928) is writing about the first epidemic of malaria in the Comores in 1923-5.
Whereas Barat (1869, discussed earlier) attributed the poor nutritional state of many [non-
white] Créoles to crop failures and market forces, Raynal puts the blame squarely on the
locals because they plant vanilla rather than food crops, and in any case can‟t be bothered
processing their rice (“…ne voudrait pas se donner la peine de pilonner son riz; p.37). He
also blames them for causing the mosquito problem by unthinkingly building a
proliferation of water-holding cisterns that allow the vector mosquitoes to multiply; for
hampering control operations; and finally for their religion: Islam is blamed for leaving the
locals too nutritionally deficient to fight malaria following the fast of Ramadan, and the

35
cooling effect of ritual bathing in the sea each morning is seen as very bad for a febrile
patient (Raynal 1928: 135,136).
(9) The nature and extent of alternative belief systems of disease causation in non-European
communities in Réunion appears to be poorly documented, but is likely to be closely tied to
the diversity of religious beliefs on the island. The interaction between religion and
constructions of health risk is the subject of further study by the authors, but its discussion
lies beyond the scope of the present paper.
(10) The idea of „blaming‟ others for epidemic disease is of course not new and features
strongly throughout European history. Generally minority groups were incriminated (for
example Jews, Saracens or Gypsies causing „black death‟ or plague), but „foreigners‟ were
also popular targets right into the 1900s. Blakely (2003) describes how the naming of
epidemics reflects an “indirect blaming device using racial stereotypes” (p. 893), citing
several flu epidemics labelled variously as German, Spanish, and Asian.
(11) From 1901 the British used malaria prevention as a rationale for racial residential
segregation in their tropical colonies: for example, tropical “native peoples” in Sierra Leone
were separated from their rulers by a distance believed to be greater than that which could
be covered by a mosquito (Frenkel & Western 1988), and the Hill Station retreats from
diseased locals (and mosquitoes) in India were similarly construed (Kenny 1995).
(12) The pattern is similar to the perceived need in metropolitan French to restrict
expenditure on the social security payments to Réunion, and is also reflected in the level of
local minimum wages, which were only brought (almost) into line with metropolitan rates
in the late 1990‟s. The unemployment rate in Réunion is generally over 30%, more than
three times the rate in metropolitan France (Mouazé c.2003). This overseas department of
just under 750,000 people therefore uses French social security resources at an equivalent
rate to about 3 million metropolitan residents.

36
(13) As a Département d‟Outre Mer (DOM), Réunion was accorded the same
administrative status as a Départment in Mainland France. Following the Constitutional
reforms of 2003 it was officially redesignated a DROM (Départment et Région d‟Outre
Mer), meaning simply that it was a Région of one single Départment. It thus has only one
prefect, but both a general and a regional assembly
(http://www.tlfq.ulaval.ca/AXL/francophonie/dom-tom.htm. Accessed 10/8/06).
(14) A notifiable disease list is a communicable disease control tool specifying those
diseases for which case data are to be collected through a notification system and subjected
to epidemiological analysis. Real-time trends are thereby identified that permit control and
education campaigns to be targeted in the right geographical area in a timely manner. To
ensure that such routine surveillance and control occurs for serious diseases, the
notification of cases by treating physicians (and sometimes diagnostic laboratories) is a
legislative requirement in most countries. France (and therefore Réunion) has a list of 30
such notifiable diseases that provides the foundations for communicable disease control in
metropolitan France as well as DOMs (INVS, 2006a). However, until July 2006, this list
did not contain either Chikungunya or dengue fever (INVS, 2006b).

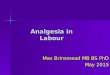
Table 1. Chronology of mosquito borne disease epidemics in Réunion in relation to advances in scientific thought and practice.
Year Disease emergence in Réunion Ascent of contagion theory Reference
1646 First human settlement
1646+ Filariasis introduced Brygoo & Brunhes 1971
1850s Pasteur discovers microbial cause of fermentation Rosen 1993
1854 Snow closes Broad Street Pump during cholera epidemic Kiple 1997
1869 First malaria epidemic Julvez & Mouchet 1994
1870s Contagion theory becomes dominant Rosen 1993
1873 First dengue epidemic Cotholendy 1873
1880 Laveran discovers Plasmodium in human malaria case Harrison 1978
1897 Ross demonstrates mosquito borne transmission of malaria Harrison 1978
1900 First antimosquito measures introduced in Réunion (1) Julvez et al. 1990
1949 DDT becomes available Julvez et al. 1998
1952 Endemic dengue eradicated (2) Salaun & Julvez 1981
1973 Endemic malaria eradicated (3) Julvez et al. 1990
2005 First chikungunya epidemic INVS 2005
(1) Quinine (both therapeutic and prophylactic), bednets, and source reduction (removal or poisoning of standing water as larval
habitats). Personal repellents (chemical) and adulticiding (aerial insecticide fogging) and are later additions.
(2) Introduced cases continue to occur, and can seed further epidemics. In the (southern) summer of October 1977 - April 1978, a
massive epidemic of dengue broke out in Réunion, infecting one third of the population (Julvez et al. 1998), and there were dengue
outbreaks in 2004 as well as concurrently with the 2005-6 Chikungunya epidemic.
(3) Introduced cases continue to occur, as do rare cases of secondary transmission, but the disease has never re-established itself. By
contrast, Mauritius was declared malaria free in 1973 but the disease re-established itself following the cyclone Gervaise: Local
malaria transmission there peaked in 1982 (Julvez et al. 1990), but has again been eradicated.
Miasma-inspired representations of tropical mosquito borne disease likely to dominate
Contagion-inspired representations of tropical mosquito borne disease likely to dominate

38
Chapter 3
The failure of colonial ‘distancing’: changing representations of
the 2005-6 Chikungunya virus epidemic in Réunion.
This chapter was submitted as a paper to the Singapore Journal of Tropical Geography,
and at the time of thesis submission was in press.

39
3.0 The failure of colonial ‘distancing’: changing representations of the
2005-6 Chikungunya virus epidemic in Réunion.
ABSTRACT
In 2005-6, the Indian Ocean island of Réunion experienced a massive epidemic of the
mosquito borne viral infection Chikungunya. Public health authorities in metropolitan
France were arguably slow to react, and we explore their representations and management
of the epidemic in the context of tropicality and colonial discourse. We analyse official
reports on the epidemic from the bulletins of the Institut de Veillance Sanitaire, seeking
evidence for any change in (1) representations of risk posed by Chikungunya to
metropolitan France; (2) the emphasis on control measures for the epidemic, (3)
descriptions of Chikungunya case symptomatologies, and (4) parallel representations of
another epidemic, flu, already known in metropolitan France. At the beginning of the
Chikungunya epidemic, our findings are consistent with a centred tropicality: There is no
perceived risk to metropolitan France because of its non-tropical climate; there is no
justification for costly control measures for a disease that is inevitable in the tropics; and
the symptoms of residents of the tropics can be described in detached terms so as to
generate knowledge about the disease. However, this „distancing‟ from a tropical problem
fails when the perceived risk to metropolitan France increases, so that towards the end of
the epidemic in late 2006, representations are more consistent with a decentred tropicality:
The concept of a protective metropolitan French climate is abandoned; the need for whole-
of-society involvement in control measures is accepted; and symptoms are described using
more inclusive language. Similar changes are not found in official reports on the flu
epidemic.

40
Introduction
In April 2005, the Indian Ocean island of Réunion, an overseas department of France, saw
the first cases of what was to become a massive epidemic of the mosquito borne viral
infection Chikungunya. More than 250,000 people, one third of the Island‟s population,
were subject to high fevers, rash, and debilitating joint pains over the next 18 months, yet
the public health authorities in metropolitan France were arguably slow to take the
epidemic seriously. Drawing on discourses on tropicality, we explore attitudes underlying
the metropolitan response by examining representations of the disease in official reports on
the epidemic. We suggest that tropicalism and colonial „distancing‟ continue to influence
public health policy and practice in France‟s overseas departments, and present evidence
that policies so influenced were revised only when the epidemic was perceived as a threat
to metropolitan France.
Tropicality is a Western discourse that “exalts the temperate world over its tropical
counterpart” (Bowd & Clayton, 2005: 297). It has clear overlaps and synergies with
colonialism and orientalism, parallel discourses that provide what McLeod (2000: 37)
succinctly summarises as a justification for “the possession and continuing occupation of
other people‟s lands”. Tropicality supports Western temperate countries‟ assertions of
superiority over their tropical (often developing) counterparts, and reinforces the
representation of the tropical world as the negative “Other” – a concept crystalised by Said
(1979) which refers to an identity constructed out of those projected negative aspects of a
society from which that society wishes to disassociate or distance itself (Mills, 1997: 106;
Edgar & Sedgwick, 1999: 266). Thus Western societies tend to distance themselves from
ignorance, weakness, and, importantly for this paper, epidemic disease. The attitudes and
reasons underlying such distancing are here referred to as resulting from tropicalism, which
has permeated knowledge production in many disciplinary areas. Best documented of these
is perhaps geography, which developed the distinct subdiscipline of tropical geography
with the publication of Gourou‟s (1947) landmark tome Les pays tropicaux (Claval, 2005).
Here we focus predominantly on the impact of tropicalism on selected and geographically

41
relevant aspects of public health practice, and it is within this context that we examine
representations of the 2005-6 Chikungunya epidemic in Réunion.
Tropicalism has long influenced the approach that Western powers have taken to
administering public health in countries where their Western medical paradigm is not
prevalent. „Tropical diseases‟ like cholera and malaria were initially perceived as a threat
only to the civilian and military personnel of the colonial administration. However, when it
became important to safeguard the labour market in the late 1800s, the perceived risk to
local people grew and it became justifiable to incur the high costs of protecting against
„tropical disease‟ at the population level (Sinha, 2004: 202). The reluctance to take
responsibility for „tropical diseases‟ nevertheless remained, as reflected in this name itself:
There was for example nothing „tropical‟ about cholera at this time, with the epidemic in
London in 1854 providing one of the formative moments in „modern‟ public health practice
(1). Much thought went into naming the discipline of „tropical medicine‟, and the “rhetoric
of colonialism further presented the colonies as uninhabitable for the European races”
because of the presence of these diseases (Sinha, 2004: 200). There were many reasons for
colonial powers to maintain this „distance‟ from the colonies and their diseases, not least of
which was the provision of a rationale for perpetuating a position of dominance and
superiority over lesser and sickly peoples.
Particularly pertinent is the phenomenon of colonial powers and colonists „distancing‟
themselves both physically and mentally from tropical mosquito borne diseases. The
British used malaria prevention as a rationale for racial residential segregation in their
tropical colonies from 1901, resulting for example in the distancing of “native peoples”
from their colonial rulers in Sierra Leone by a distance believed to be greater that which
could be covered by a mosquito (Frenkel & Western 1988). It is clear, however, that policy
on such preventive measures was influenced by more than just the biomechanics of
mosquito borne disease transmission: Such segregation was “conditioned by the pervasive
racial thinking of the time” (Frenkel & Western 1988: 211). In discussing the Hill Stations
used as climatic (mosquito) retreats in India, Kenny (1995: 695) suggests that they
“reflected and reinforced assumptions of social and racial difference”. Said (1979: 55)

42
explains that such distancing helps the colonial mind to “intensify its own sense of itself by
dramatising the distance and difference between what is close and what is far away”, and
„distancing‟ was firmly entrenched in the colonial mindset. It is therefore reasonable to
suggest that residual tropicalism in the administration of French public health infrastructure
might have led to a „distancing‟ of metropolitan France from the tropical, mosquito borne
disease problems of French overseas departments. In this paper we are looking specifically
at the official reporting of Chikungunya for the French overseas Department of Réunion.
We argue that distancing became increasingly difficult to maintain as the direct threat to
metropolitan France was perceived to increase with the progression of the epidemic. The
ultimate failure of public health authorities to distance themselves from the problem is
reflected in the rhetoric of the official reports on the epidemic from the Institut de Veillance
Sanitaire (INVS; Institute of Health Surveillance), which we examine here from a broad
perspective: Not within a scientific context (allowing an evaluation of the representation
and management of the Chikungunya epidemic from the perspective of best public health
practice), but from the perspective of tropicality and colonial discourse.
The metropolitan France (Saint-Maurice)-based INVS is the national coordinating body for
communicable disease surveillance and control, and has responsibility for reporting on
epidemics for all departments of France, including overseas departments (Departments et
Regions d‟Outre-Mer [DROMs]: La Réunion, Martinique, Guadaloupe and Guyane)
(INVS, 2006). All departments provide surveillance data to the INVS, where data are
analysed centrally and the results published in INVS bulletins. Epidemiological
information is therefore produced centrally for distribution to all departments (including
DROMs), and there is no regional production of official reports on epidemics. INVS
bulletins are disseminated to health care workers and are available to journalists and other
interested parties on the web, with a readership that is both local (Réunion) and central
(metropolitan France). Different regional interpretations of these reports are likely to be
reflected in the respective mass media; a complimentary study to the present paper aims to
examine the regional variation in such media representations, but lies beyond the scope of
the present study of official discourse on the Chikungunya epidemic.

43
To differentiate between changes in disease representation that might result from
tropicalism as opposed to simply reflecting the increasing severity of the epidemic, we also
examined official discourses on a different epidemic: Flu. This viral infection was selected
because of its similarity to Chikungunya both clinically (sore joints and muscles, limited
associated mortality) and epidemiologically (rapid rise in case numbers, recent outbreak).
Flu epidemics are also officially reported in INVS bulletins, and the representations of flu
therein therefore provide unbiased comparative material for analysis in so far as both flu
and Chikungunya data are analysed and reported on by similar staff working in a similar
environment. In addition, the flu outbreak in early 2007 affected both metropolitan France
and Martinique (another of France‟s overseas departments), providing an ideal opportunity
for comparison with Chikungunya which affected only an overseas department.
A description of several of the key elements of the Chikungunya epidemic is necessary to
provide a framework for our reading of “tropicality” in the INVS bulletins and is presented
here in three sections for clarity: A. Symptoms; B. Transmission and vectors; and C.
Disease control measures.
A. Symptoms
The Chikungunya virus is a member of the group of viruses called alphaviruses (Family
Togaviridae), which cause a complex of diseases classified under the general heading
“Athropod-borne viral arthritis and rash” (Chin, 2000). Infection with Chikungunya virus
is generally self-limiting, with fever, joint pains and rash that resolve over a few weeks.
The fever has a sudden onset and is followed by intense joint pains and headaches. A
spotty (maculopapular) rash is often present, and children may experience minor nose and
gum bleeding. Infection without any clinical disease (asymptomatic) is common, and
complications are rare: Most often, there are no residual effects at all, but occasional
individuals have lingering symptoms for many months and may develop a type of “post
viral syndrome” with ongoing lethargy and impaired social functioning. Severe
complications like brain involvement (meningoencephalitis) and death were unknown

44
before the Réunion outbreak, and remain rare. There is no treatment available for
Chikungunya infection other than supporting the patient (analgesics, non-steroidal anti-
inflammatories, and fluids) until the disease resolves.
B. Transmission and vectors
Chikungunya is a virus transmitted by mosquitoes (arthropod borne virus, or arbovirus). A
mosquito becomes infected by biting a person with Chikungunya virus circulating in their
blood stream (viraemic), and after some time (extrinsic incubation period) the virus has
multiplied sufficiently in the mosquito to render it infectious when biting its next victim. If
that victim has not had the infection before (ie. is non-immune), the viral particles can
again multiply and after another delay (intrinsic incubation period), this person in turn
becomes viraemic and may develop clinical symptoms. The incubation periods are very
important in understanding the epidemiology of the disease, particularly in an island
context like Réunion: The length of the extrinsic incubation period is very environmentally
dependent, particularly on temperature (because the virus can replicate faster at higher
temperatures); this explains why arbovirus epidemics are more common in the hotter
months, regardless of when the wettest months occur. The worst epidemics, like
Chikungunya in Réunion, occur when water availability for mosquitoes and high
temperatures coincide. The length of the intrinsic incubation period determines if a person
has the opportunity to disseminate the virus (eg. by travelling and being bitten by local
mosquitoes elsewhere) before he/she realises that he/she is infected. It is likely that
Chikungunya (and dengue virus) was introduced to Réunion by this mechanism, and could
be introduced to metropolitan France in the same way. A mosquito capable of transmitting
a disease is known as a “competent vector”, and for Chikungunya on Réunion this is the
Asian tiger mosquito Aedes albopictus. The species is native to the jungles of SE Asia and
is believed to have been inadvertently introduced to the Indian Ocean Islands by early
contact with Malayan seafarers, possibly over 500 years ago. It readily lays its eggs
(oviposits) in hollowed coconut husks and shells, and since coconuts would have been

45
staple food stores on voyages from Asia at that time, eggs or larvae could easily have been
brought to the islands (Juvez et al., 1998). Particular biological adaptations of Aedes
mosquitoes makes such a scenario likely (2), and explains the probable presence of this
vector in Réunion before first European contact.
C. Disease Control Measures
The mainstay of controlling an epidemic of arboviral disease lies in preventing mosquitoes
from coming into contact with people – both by reducing the number of mosquitoes, and by
use of personal mosquito protection. Because Aedes albopictus is a peri-urban container
breeder, two approaches are possible to reducing mosquito numbers; urban insecticide
application (targeting either adults or larvae), and source reduction (removing water-
holding larval habitats such as garbage, saucers, pot plants, tyres, blocked gutters, potholes,
drains, etc). For Aedes albopictus source reduction is by far the more effective approach,
but is dependent on community participation. The population-level effectiveness of
personal mosquito protection is also dependent on community participation, and involves
all individuals applying personal insect repellents; using mosquito screens, bed nets and
knockdown sprays indoors; limiting outdoor activities at dawn and dusk (the main biting
times); and wearing long, loose sleeves and trousers (Bailey et al., 2004). Personal
mosquito protection not only reduces the chances of being bitten by an infected mosquito,
but also decreases the accessibility of viraemic individuals to vectors (thereby reducing the
proportion of mosquitoes that are infected). Community participation is therefore critical to
the control of arboviral epidemics – an important point to which we will return.
In our reading of the official INVS bulletins (INVS 2005-6a, b, 2006a, b, c), we look at
how the risk posed to metropolitan France by imported cases is represented, what disease
control measures are recommended by the INVS for application in Réunion, how case
symptomatologies are described, and for comparative purposes, a similar analysis of flu.
The temporal changes in representations of the Chikungunya-related material can be

46
considered relative to the course of the epidemic by reference to Table 1., which provides
monthly figures for the number of cases in Réunion, the number of deaths, and the number
of cases imported into metropolitan France (please see last page of this chapter).
The table covers the period between April 2005 when the first cases occurred, and August
2006 when the epidemic abated – a total of over one quarter of a million cases (INVS,
2005-6b). It shows the peak of the epidemic occurring early in 2006 almost a year after the
first cases, and a Chikungunya-associated mortality coinciding with this peak. Imported
cases are reported from the earliest stages of the epidemic, but show a surge in early 2006
that also coincides with the epidemic peak. By August 2006 the epidemic has subsided and
this forms the end of our study period. (Additional data available at the time of going to
press have been added for completeness and to confirm this subsidence).
We now go on to analyse reports from the bulletins of the INVS, presenting our findings in
four sections: 1. Representations of risk to metropolitan France; 2. Control measures; 3.
Representations of symptoms; and 4. Chikungunya reporting relative to reporting of flu.
1. Representations of risk to metropolitan France
The French notifiable disease list has always been based very much on Metropolian
communicable disease control, with little regard for the tropical arboviral infections of
French overseas departments, despite their status as integral parts of France. In 1946, La
Réunion was accorded the same administrative status as a Départment in metropolitan
France. This status is still maintained (as a DROM), and Réunion has thus been an integral
part of France proper for 60 years. Expectations are therefore that the minimum wage,
social security payments, and availability of education and health care in Réunion match
the standards set by metropolitan France. These expectations have very nearly been met:
The minimum wage was brought to the same level as for metropolitan France in 1996, and
welfare payments to within 20%; literacy is at 89% and the infant mortality rate much
closer to that of metropolitan France than to that of Mauritius (3). An important component

47
of health care provision is communicable disease control, the mainstay of which is a
disease surveillance system linked to specific interventions. The stated aim of
communicable disease surveillance, in France as elsewhere, is the early detection of cases
to allow a timely deployment of public health interventions, thus minimising the spread of
the disease as well as its resultant morbidity and mortality. In the specific case of outbreaks
of non-endemic arboviral disease, it is a particularly important function of surveillance to:
(a) detect imported cases so as to limit the opportunities for transmission (by reducing the
viraemic individual‟s exposure to local mosquitoes), (b) detect any local transmission of the
disease and use this information to direct the timing and location of mosquito control
measures, and (c) follow any trends apparent in the epidemic (MSS, 2006: 2).
A historical example is appropriate to contextualise the longstanding need for arboviral
infections to be included on the French notifiable disease list that forms the basis of such
surveillance (4). Réunion experienced its first recorded epidemic of dengue, a very
common and serious arboviral infection, as early as 1873 (Cotholendy, 1873). Dengue then
became endemic in Réunion, with occasional epidemics such as those associated with the
troop movements of WWII. By 1952 it was nevertheless considered eliminated (Salaun &
Julvez, 1981), possibly as a side effect of malaria control activities. The main vector in
Réunion, Aedes albopictus, nevertheless remained. It was therefore no surprise that another
major epidemic of dengue occurred on the island in 1977-8, with a full one third of the
population suffering clinically significant infection (Julvez et al., 1998). Despite over 100
years of dengue on the island, the disease was still not on the French notifiable disease list,
and the local response in Réunion to this lack of surveillance was to set up a limited local
surveillance system independent of the notifiable disease list. The system consisted of a
network of doctors and laboratories on the island notifying dengue on a voluntary basis to
local health authorities, with use of the Institut Pasteur in Madagascar as a reference
laboratory (Lassalle et al., 1998). The need to implement a local surveillance system
independent of a centralised metropolitan one still did not appear to be sufficiently
influential to warrant the inclusion of the disease in the official notifiable disease
surveillance system. Similarly, the epidemic of Chikungunya that gripped Réunion in
2005-6 also affected about one third of the Island‟s population, and was also not notifiable

48
as part of the routine health surveillance system. It was only following the importation of
cases of Chikungunya to metropolitan France, in the presence of Aedes albopictus
mosquitoes newly established there, that arboviral disease prevention was deemed relevant
and important enough by the INVS to include dengue and Chikungunya in the official
notifiable disease surveillance system.
The large numbers of people infected (one third of the population) is of particular relevance
in an island context: A severe public health impact from both dengue and Chikungunya lies
in the cumulative disease burden (morbidity) at the population level. In non-immune
populations particularly (no previous exposure to the virus), the whole of the population is
susceptible and in small unexposed communities such as isolated villages or islands,
epidemics can therefore be devastating, with a significant proportion of key service
providers ill at any one time. By not having dengue or Chikungunya on the notifiable
disease list, Reunionese were deprived of the surveillance functions designed to minimise
such impacts, and they are therefore likely to have suffered considerable preventable
morbidity and mortality as a result. In other DROMs where arboviral infections occur, the
population is therefore also likely to have suffered a large preventable arboviral disease
burden, particularly Guadaloupe, Martinique, and Guiana, where dengue is rampant.
In May 2005, at an early stage of the Chikungunya epidemic before the occurrence of the
majority of the infections and deaths (see Table 1.), the risk of Chikungunya being
transmitted in metropolitan France was deemed very unlikely (très improbable) in the first
Point de situation on the epidemic issued by the INVS (INVS 2005-6a: Point au 3 mai).
That issue also mentions the several imported cases already recorded at that time in
Marseilles, in travellers returning to the large Comorian community there. It was therefore
already known that the virus had been imported in viraemic travellers, and was thus
available to mosquitoes in metropolitan France. Further along the Mediterranean coast in
the area of Nice, the vector Aedes albopictus was known to be established (5), and May in
southern France is heading towards temperatures high enough to allow the extrinsic
incubation period to be completed well within the lifetime of a mosquito: The prerequisites

49
for an outbreak of arboviral disease in metropolitan France could thus be considered to
have been fulfilled.
It is therefore not surprising that the statement of “very unlikely” had been toned down in
the next issue (19 May 2005) to “no current risk of secondary transmission in metropolitan
France” (Il n’y a pas, à l’heure actuelle, de risque…) (INVS, 2005-6a: Point de situation au
19 mai). This statement of perceived risk remains unchanged in the next 5 issues (6 and 21
June, 6 July, 12 August and 7 September 2005), but it makes its last appearance in the 7
September issue. Interestingly, any comment about the risk to metropolitan France is then
totally lacking not just from the INVS‟s Points de situation, but from all INVS bulletins
about the epidemic until March 2006. The removal of this information may simply reflect
the reduced risk during September to March, which are the colder months in France with
dramatically reduced mosquito numbers. However, it could also be interpreted as a
realisation that the risk was greater than had been stated, and that such a controversial item
was therefore removed until better risk communication strategies had been considered.
This latter interpretation would be supported if the changes made were part of a trend to
reduce metropolitan „distancing‟ from the epidemic, and this is in fact the case. In March
2006 the first issue of an entirely new Series of INVS bulletins appears, entitled Cas de
chikungunya importés en métropole (INVS, 2006a). In the March issue (6), the presence of
both imported viraemic cases and the vector mosquito Aedes albopictus is acknowledged,
but climatic conditions are proffered as protective against local transmission of the virus
(“…en raison des conditions climatiques…”). This statement is consistent with what might
have been expected based on the virtues of a temperate climate, as exalted by discourses in
tropicality. However, in the next edition (3rd
April, 2006) even this climate reference has
been removed, apparently acknowledging that there may, in fact, be a risk, and that
temperate France is perhaps not that different from tropical Réunion after all. The
statements of (no) risk that appeared in the early editions of the Points de situation have
been supplanted in this new bulletin by a justification of imported case-counting as a
separate mechanism of evaluating the risk of local transmission (“évaluation de risque
potentiel de transmission autochtone en métropole”) (INVS, 2006a). Case-counting is later
made a legislative requirement in France by placing Chikungunya (and dengue) on the

50
French notifiable disease list for the first time, in July 2006 (INVS 2006b), but the lateness
of this addition is damning because of the neglected opportunities to reduce disease burdens
in those French overseas departments with arboviral disease epidemics. The inclusive
nature of the complete list of notifiable diseases can nevertheless be seen as a final
acknowledgement that the Chikungunya epidemic is not an exclusively „tropical‟ public
health problem.
In considering the changing nature of the way that this public health risk is represented in
the INVS bulletins, it is important to remember that the scientific evidence about the risk of
transmission does not change with time: Imported cases were present from the start, the
vector distribution is unaltered, and seasonal climate change is broadly predictable. One
can therefore only conclude that the changing rhetoric reflects a change in the way that the
risk is being perceived by the public health authorities, and that this perception has moved
from one of being at a safe distance from a tropical problem, to being on the verge of a
possible metropolitan outbreak. The “self” and “Other” barrier has therefore arguably been
eroded, with the metropolitan public health mindset no longer “intensifying its own sense
of itself” (Said, 1979: 55) by distancing.
2. Control measures
The importance of community participation in controlling mosquito borne disease
epidemics has already been highlighted. However, the necessary community participation
is often difficult to achieve (particularly in hot climates where outdoor living is de rigueur),
and it is therefore critical to target publicity campaigns optimally in both time and place.
To achieve optimal targeting, public health agencies involved in communicable disease
control again depend on surveillance systems, which are health data collecting mechanisms
with a built-in interpretative or “intelligence” function that leads directly to an action plan
for public health intervention (Cameron, 2004). In the case of arboviral disease control,
case data are collected through the notification system to identify real-time trends that
permit both mosquito control and education campaigns to be targeted in the right

51
geographical area at an appropriate time. The desired outcome then is community
participation to facilitate source reduction and to decrease human contact with mosquitoes,
as has been discussed above. Surprisingly then, in the first 7 issues of Points d’actualité
générales (3 May – 7 September 2005; INVS, 2005-6a), there is no mention of community
participation or other control measures; it is as if the central authorities need not concern
themselves about controlling the epidemic, because they are sufficiently „distanced‟ from
the problem that the implementation and targeting of control measures can be left to local
authorities in Réunion. A mention of control measures first appears in the 21 November
issue, about 6 months after the Indian Ocean epidemic took hold (see Table 1.). The
interventions described include the standard armamentarium of anti-mosquito measures:
individual protection (repellents, netting), community intervention (source reduction
[emptying potential breeding sites around the house like saucers and water holding
rubbish]), and mosquito control (insecticide application, both for larvae and adults).
Community intervention (“lutte communautaire”) is now mentioned once, but it is
mentioned 3 times some 2 months later in the 12 January 2006 issue, demonstrating an
increased awareness of the need to engage the community in a whole-of-society approach
to controlling the epidemic. By the 18th
August issue, community intervention has become
paramount and “the whole of the community needs to be involved in daily source
reduction” (INVS, 2005-6a: Point de situation au 18 août 2006). Note that, as in the
previous section on risk representation, there was no change in scientific knowledge about
appropriate public health interventions during the course of the epidemic: Mosquito borne
disease outbreaks have been controlled by well integrated individual-community-health
authority approaches for decades, with community involvement in source reduction always
a critical link in the control of urban epidemics. The role of the community was
nevertheless not reflected in the official bulletins until very late, arguably only once the
extent of the epidemic had been acknowledged as large enough to possibly impact on
metropolitan France. Once it was obvious that „distancing‟ could not absolve metropolitan
French public health authorities from the responsibility of controlling the outbreak in the
tropics, it became appropriate to share the burden of that responsibility with the
community. Thus, if secondary transmission in metropolitan France were detected, it
would not be the fault of the authorities (who arguably intervened too late), but a shared

52
responsibility between individuals, communities and authorities together - both from
Réunion and from metropolitan France. Any „distancing‟ that might have influenced
French public health thinking early in the epidemic, weather subliminal or otherwise, was
thereby effectively annulled, and in the end, metropolitan public health writers cease to
conceptualise themselves as being distant and different from the people at risk in Réunion.
3. Representations of symptoms
The third strand of evidence for the failure of „distancing‟ comes from the descriptions of
the symptoms experienced by sufferers of Chikungunya infection. In the INVS‟s first issue
of Points de situation génerale (3 May 2005), the symptoms described include: Intense
arthralgia; maculopapular rash; and benign haemorrhages in kids. Some 15 months later
(18 August 2006) after the peak of the epidemic has passed (see Table 1.), the same
descriptions of symptoms have, respectively, changed to: Serious joint and muscle pain;
skin rash; and examples of benign haemorrhages have been added (bleeding noses and
gums). These changes reflect a shift to more user-friendly medical language rather than a
change in the natural history of the disease; less technical language is used and more details
are provided. The description of symptoms is thus made more tangible to the reader by de-
jargonising and by the inclusion of examples of symptoms that are more accessible,
supporting a shift away from „distancing‟.
Interestingly, there is a concurrent increase in the number of possible complications of the
disease that are described, but these do in fact reflect a change in the natural history of the
disease during the Réunion epidemic. An early statement (3 May 2005) that asymptomatic
infections are common is removed, and the previously unrecorded complications of
meningoencephalitis and maternal-neonatal infection appear (21 November 2005), and later
also death (6 February 2006) under a new subheading “Formes graves et atypiques”. The
emergence of such severe complications for what was historically a more benign viral
infection has been the subject of much scientific attention, but that discussion lies beyond
the scope of the present paper. The rhetoric used to report deaths is nevertheless relevant,

53
in so far as it appears to follow the same trend of initial detachment to later acceptance.
The official stance reported on 27 January 2006 was that there had been no deaths directly
attributable to Chikungunya, implying that it may nevertheless have been a contributing
factor to death in some cases. The latter suggestion is formalised from 6 February 2006,
with a listing of the number of death certificates that mention Chikungunya as contributory.
Finally, a new subheading “Décès” appears from 24 February 2006. Previous to this
acceptance that deaths do occur, the change in reporting of the absence of deaths in the
Points de situation generales (INVS 2005-6a) is interesting in its own right, and again
follows the same trend towards acceptance: It moves from a succinct statement that no
death has (ever) been reported from Chikungunya infection (“Aucun cas mortel d‟infection
à Chikungunya n‟a été rapporté ”, 3 May 05), to progressively longer statements with
further qualifications (“Aucun cas mortel d‟infection à Chikungunya n‟a été rapporté à ce
jour ”, 22 Dec 05; “Aucun cas mortel d‟infection à Chikungunya n‟a été rapporté lors des
épidémies précédents ”, 27 Jan 06). On 18 May 06 the final modification has no deaths
occurring from Chikungunya previous to the current epidemic (“Aucun cas mortel
d‟infection à Chikungunya n‟a été rapporté lors des épidémies précédant celle de la
Réunion ”). Because the first three of these statements pre-date the recording of any deaths
from Chikungunya (see Table 1.), their modification does not reflect a change in the natural
history of disease progression. Rather, the modifications suggest an increasing acceptance
by health authorities that they can no longer „distance‟ themselves from the epidemic based
on historical precedent.
4. Chikungunya reporting relative to reporting of flu
In contrast to the changing representations of Chikungunya outlined above, representations
of flu in INVS bulletins are remarkably constant. Take for example the most recent
epidemic in early 2007, which shows rapidly increasing notification rates and large
numbers of cases, including deaths (INVS 2006-7). This epidemic affected metropolitan
France as well as the French overseas department of Martinique, which, like Réunion, is
subject to the same public health legislation and notifiable disease surveillance as

54
metropolitan France. Cases are notified based on clinical diagnosis (flu like symptoms
including a temperature above 39C and a sudden onset of myalgia and respiratory
symptoms), and are collated with hospitalization and mortality data for publication in the
INVS bulletins. Winter epidemics are expected both in metropolitan France and in French
overseas departments, and weekly bulletins are produced from October to April regardless
of the number of cases occurring.
In 2007 the number of notified cases in metropolitan France first approaches the epidemic
threshold level in the second week of January (8-14 January) (“…au niveau du seuil
épidémique…”; INVS 2006-7, Semaine 2). This fact is simply and objectively reported, as
is the hospitalisation rate (<1%) and mortality since October (8 deaths) (“…décès lies à une
grippe clinique…”). A similar straightforward pattern is followed in subsequent weeks,
with the increasing number of cases being described as above the epidemic threshold value
in week 3, as constituting a confirmed epidemic in week 4, and as continuing to increase in
weeks 5 and 6. Once the existence of an epidemic has been confirmed in week 4 by case
numbers exceeding the threshold value in two consecutive weeks, a prediction is included
that the epidemic peak will be passed within three weeks. The cumulative number of
deaths is also reported each week using the same standard phrase (“…décès lies à une
grippe clinique…”), being 8, 11, 14, 14 and 17 deaths up to week 6. The notification rate is
increasing dramatically during this same period (from 136 to 990 cases per 100,000
population), but there is no apparent change in the approach to or tone of the case reporting
in these INVS bulletins (“…l‟incidence [ ] continue à augmenter…”, INVS 2006-7,
Semaine 6).
Importantly, Martinique is included in these reports before the number of cases reaches the
epidemic threshold in metropolitan France. In the last two weeks of 2006 the number of
cases in Martinique is reported as stable, but they show a 45% increase in the first week of
2007, and a further 33% increase in the following week. The same simple and objective
language used to describe the epidemic in metropolitan France is also apparent here; the
intensification of epidemic activity (“…le nombre [ ] a augmenté de x%...”), and the
number of cases stated to have exceeded the epidemic threshold in Week 2 (“… a dépassé

55
le seuil épidémique…”; INVS 2006-7, Semaine 5). There is no apparent change with time
in the relative importance placed on reporting on the epidemic in metropolitan France
compared to French overseas departments; as cases accumulate a graph of the epidemic in
Martinique is included and the number of doctors contributing to the surveillance system
there is corrected from “about 50” (une cinquantaine; week 2) to “59” (week 4), but there is
no indication that perceptions of the disease are changing.
There are may reasons that may explain why flu should demonstrate such a constancy in its
reporting compared to Chikungunya: The timeframe is shorter (perhaps not allowing slow
changes in perception and representation of the disease), and there is historical precedent to
the approach to reporting based on previous flu epidemics; but the most likely explanation
is that flu is accepted and familiar as a common winter epidemic in temperate metropolitan
France, and representations of it are therefore not influenced by tropicalism. The latter
interpretation is supported by the fact that flu in Martinique is represented in an identical
fashion to flu in metropolitan France, since there is no opportunity to “distance”
metropolitan France from the disease. In this situation, Martinique is therefore treated as an
integral part of France and included in the INVS bulletins on an equal footing.
Conclusion
We have observed firstly a change in the representation of risk posed by Chikungunya to
metropolitan France, from dismissal early in the epidemic to acceptance later; secondly a
change in emphasis for control measures for the epidemic, with an increasing
acknowledgement of the importance of community involvement and shared responsibility;
thirdly a change in the descriptions of Chikungunya case symptomatologies, moving from
technical terms to more people-oriented language later in the epidemic; and finally a lack of
change in the representation of a comparison epidemic, flu, which unlike Chikungunya was
accepted as part of the expected disease burden in metropolitan France.

56
When taken together, the first three of these trends provide a strong suggestion that the
initial attitude of public health authorities in metropolitan France to the epidemic was
coloured by tropicalism and colonial attitudes towards Réunion and the Reunionese. This
interpretation is supported by the remarkable constancy of the representations of flu,
already endemic in temperate, metropolitan France. Whereas Chikungunya in Réunion was
arguably not taken as seriously as it might have been until it posed a threat to metropolitan
France, flu in Martinique was treated on an equal basis to flu in metropolitan France
because the disease was already taken seriously in metropolitan France. It could be argued
that this difference is also due in part to the novelty and unfamiliarity of Chikungunya, but
such an argument reinforces rather than detracts from our conclusions about tropicalist
thinking in French public health policy: Chikungunya, and dengue, are familiar enough to
local public health practitioners in the African region that only failure to consult with the
latter could have led to these diseases being passed over for inclusion on the list of
notifiable diseases in France and her overseas departments.
Because Réunion was an uninhabited island until settled by the French, one might question
the relevance of an analytic framework based on tropicalism and colonial discourses, since
these presuppose the possession and continuing occupation of other people‟s lands.
However, these discourses apply equally to “members of the European communities who
had settled overseas and no longer wished to defer power and authority to the imperial
motherland” (McLeod, 2000: 8). Also, and perhaps more importantly, the island acquired
significant populations of Malagasy, African, Indian, and Chinese origin, as a result of both
slave trade and the importation of indentured labour. By the time mosquito borne disease
control first features as a public health issue in Réunion in the early 20th
century, the
makeup of the affected population and its relationship with metropolitan France is therefore
such that tropicalism does provide a useful analytic framework within which to look at
representations of the Chikungunya epidemic; the population of the island provides a
“diseased native” element against which metropolitan health authorities could, as Said
would argue, intensify their own sense of worth and control. The “diseased native” as a
concept has been engrained in European thinking since the advent of germ theory in the late
1800s, when microbially infected indigenous communities became synonymous with “sites

57
of disease” (Kenny, 1995: 711). It is therefore not surprising to find indications of a
residue of this colonial attitude in France today, an attitude that is arguably perpetuated
because of the peculiar postcolonial relationship that France maintains with its former
colonies, particularly in Africa. Staniland (1987: 61) argues that French-African relations
cannot be understood in terms of the normal “conventions of analysis and practice in
international affairs” because of the breadth of cultural and economic relationships that
remain. In some instances, former colonies (and/or DROMs) stand to benefit from these
relationships, and there is a clear advantage for most Reunionese in being part of France
and therefore heavily financially subsidised. In other cases, unfortunately, the relationship
hides ongoing inequity, dependence and exploitation (Staniland, 1987: 53), and it is likely
that these more negative aspects of French colonial relations are those that underlie the
initial „distancing‟ of metropolitan health authorities from the 2005-6 public health
emergency in the Indian Ocean.
In attempting to summarise our findings in the context of tropicalism and colonial
discourse, it seems clear that the representation of tropical disease as distant and affecting
lesser peoples provides a rationale for temperate France to maintain a position of
dominance and superiority over its tropical departments. In practical terms, it also provides
a rationale for public health inaction: The cost of administering interventions to combat
tropical diseases at the population level have long held back colonial public health
initiatives (Sinha, 2004: 202). The omission of Chikungunya from the French notifiable
disease list until 2006 can therefore be construed in these terms, illustrating a central tenet
of colonial discourse which holds that there is an “important mutually supportive
relationship between the material practices of colonialism and the representations it
fashions in order for it to work” (McLeod, 2000:38, emphasis in original). The distancing
from tropical diseases and the cost saving associated with not putting them under
surveillance thus go hand in hand. Nevertheless, it is reassuring to see that „distancing‟,
and hopefully the tropicalist attitudes underlying it, were replaced by a more accepting and
inclusive approach to public health policy not much more that a year after the first
appearance of Chikungunya virus in Réunion.

58
To finish, we would like to draw on the work of Bruneau (2005), whose terms “centred
tropicality” and “decentered tropicality” are directly applicable to our analysis. Bruneau
describes centred tropicality as a system of (geographical) knowledge based on French
colonialism and holding as a key tenet that the natural tropical environment directly
influences and constrains local populations in a deterministic way. In disease epidemic
terms, the tropical environment could be seen to provide the appropriate and irreversible
conditions required for mosquito breeding and (Chikungunya) virus transmission; tropical
disease risk is thus fixed in a deterministic way by the environment, and there is
justification for metropolitan health planners to accept this inevitability and do nothing in
the face of a tropical disease epidemic. The representations and management of the
Chikungunya epidemic as we have described them are thus consistent, at the beginning of
the outbreak, with centred tropicality: There is no perceived risk to metropolitan France
because of its non-tropical climate; there is no justification for costly control measures for a
disease that is inevitable in the tropics; and the symptoms of residents of the tropics can be
described in detached terms so as to generate knowledge about the disease. Bruneau (ibid.)
goes on to describe how this centred tropicality evolved historically into a decentered
tropicality, the latter rejecting environmental determinism and integrating more broadly
with the social sciences. The parallels with our analysis of the Chikungunya epidemic are
to be found during the later stages of the epidemic: The concept of a protective French
climate is abandoned; the need for whole-of-society involvement in control measures is
accepted; and symptoms are described using more inclusive language that is arguably more
akin to how the people affected by the disease would describe it themselves. It is thus
possible to conceptualise the changing representations of the 2005-6 Chikungunya
epidemic in Réunion in terms of an initially centred tropicality in which public health
authorities distanced themselves from the problem, followed by a later decentered
tropicality in which the thinking of public health authorities became more integrated with
that of the regional communities affected. We therefore conclude that tropicalism and
colonial distancing continue to influence public health policy and practice in France‟s
overseas departments, but that public health authorities demonstrate a positive capacity for
rapid evolution towards more inclusive approaches.

59
ENDNOTES
(1) Dr John Snow, suspecting that the disease was water borne, had the city authorities
remove the handle from the Broad Street pump, thereby curtailing the epidemic. This was
the first time that „modern‟ epidemiology had resulted directly in a public health
intervention.
(2) Two special features of Aedes mosquito biology favour their facilitated dispersal by
humans. Firstly, eggs are desiccation-resistant, and are laid in containers on the surface
above the water line (not in the water, like Culex or Anopheles mosquitoes). If rainfall is
favourable, the eggs will be submerged by the rising water level in the container, and the
larvae (wrigglers) hatch to complete their development in the water. If rainfall is
unfavourable and the eggs stay dry, they can remain dormant for many months until
submerged subsequently. Secondly, Aedes mosquitoes demonstrate staggered hatching: a
proportion of the eggs only hatch after a second (or even third) immersion. This guarantees
the survival of at least some individuals in ephemeral conditions, such as those experienced
in coconut shells (or other water receptacles) on Malay boats, where light rain might
inundate the eggs without providing sufficient water for them to complete their
development before it evaporates.
(3) Infant mortality rates per 1000 population for metropolitan France, Réunion, and
Mauritius are, respectively, 4.21, 7.63, and 14.59. World Fact Book, CIA,
http://sportsforum.ws/sd/factbook/index.html. Accessed 4/6/06.
(4) To ensure that routine surveillance occurs for serious diseases, the notification of cases
by treating physicians (and sometimes diagnostic laboratories) is a legislative requirement
in most countries. France (and therefore Réunion) has a list of 30 such notifiable diseases
that provides the foundations for communicable disease control in metropolitan France as
well as DROMs (INVS, 2006c).

60
(5) In a modern day equivalent of the desiccated-eggs-in-coconuts scenario described for
the arrival of Aedes albopictus in Réunion, these mosquitoes have been transported globally
with the international trade in used tyres (artificial containers). A population is now
established and spreading in the USA (since 1985), Italy (1990), and most recently France
(for a review, see Juliano & Lunibos, 2005). It was first detected in metropolitan France in
1999 in used tyre storage centres in Normandy (Schaffner & Karch, 2000), and is now also
spreading along the Mediterranean coast. It is likely that Aedes albopictus is in France to
stay, because eggs are able to overwinter (diapause) during the colder months. Thus,
France now has an established population of vectors capable of transmitting Chikungunya,
dengue, or other arboviruses.
(6) The first issue is not actually dated, but contains a reference to another publication from
March 2nd. The second issue is dated 3 April, so it can be concluded that the first issue is
from sometime between these two dates.
ACKNOWLEDGEMENTS
Thanks to Fiona Maley for assistance with references, Agnes Weinstein for typing the
manuscript, and two anonymous referees for helping to improve the paper.

61
Table 1. The progression of the 2005-6 Chikungunya epidemic illustrated as case numbers
by month for Réunion and for Metropolitan France. Based on INVS data available at
http://www.invs.sante.fr/surveillance/chikungunya/default.htm (accessed 18/2/07).
Month
Confirmed cases in
Réunion1
Estimated cases in
Réunion2
Monthly mortality in
Réunion3
Confirmed imported
cases4
Jan 2005
Feb
March 24
April 281 25
May 1486 15
June 1234 15
July 449 15
August 410 7
Sept 458 3
Oct 616 2
Nov 967 7
Dec 951 6667 0 15
Jan 2006 54136 17 72
Feb 127073 76 151
March 45202 88 176
April 14667 32 115
May 5267 19 88
June 343 2700 7 47
July 141 4 24
August 90 3 15
Sept 57 3 19
Oct 57 3 25
Nov 32 0 25
1. Confirmed cases are individuals who have sought medical attention and have had a
diagnosis of Chikungunya virus infection confirmed by subsequent laboratory testing
(serology). The actual number of people infected is likely to be larger, and this differential
increases with the severity of the epidemic (see 2.).
2. The estimated number of cases is derived from surveillance data that include medical
contacts without laboratory confirmation. During a severe epidemic, laboratory

62
confirmation of cases becomes both unnecessary and logistically impossible through sheer
pressure of numbers, and is either abandoned or becomes meaningless.
3. Based on the number of death certificates that mention Chikungunya, but not necessarily
as the primary cause of death; the numbers therefore overestimate the number of deaths
directly attributable to Chikungunya.
4. Numbers represent individuals who have sought medical attention in Metropolitan
France and have had a diagnosis of Chikungunya virus infection confirmed by laboratory
testing. All have a history of travel to Chikungunya affected areas, but not exclusively to
Réunion; for example, many of the 2005 cases were traced to the Comores (Mayotte).

63
Chapter 4
Print media representations of an unusual health event:
Chikungunya virus, risk and identity on Réunion Island.
This chapter was submitted as a paper to the Journal of Asian and African Studies, and at
the time of thesis submission was in review.

64
4.0 Print media representations of an unusual health event:
Chikungunya virus, risk and identity on Réunion Island.
ABSTRACT
In 2005-6, the French Indian Ocean island of Réunion experienced a massive epidemic of
the mosquito borne viral infection Chikungunya. Reporting on the epidemic in the print
media demonstrates a considerable lag compared to the real-time evolution of the epidemic,
and this paper explores possible reasons for that delay. We analyse the content of print
media articles about Chikungunya from two Reunionese newspapers (Témoignages and
Clicanoo) and two newspapers from metropolitan France (Le Figaro and Le Monde). In
the Réunionnnais newspapers, the delay in acknowledging the public health risk posed by
the virus suggests passive denial in the early stages of the epidemic, followed by
acceptance with blame attributed to the French metropolitan government – reflecting the
uneasy historical relationship between the Reunionese and the government. In the French
metropolitan newspapers, the delay is even greater and may reflect the influence of residual
colonialist thinking on the priority placed on reporting on an epidemic in a remote tropical
location: Once a risk to metropolitan France is identified, reporting intensifies considerably.
The media representations also highlight the importance of belief systems as modulators of
people‟s risk perception and their subsequent health protective behaviour. We suggest that
a better understanding of these relationships in multicultural societies may provide
important opportunities to reduce the community burden of disease.
Introduction
In 2005-6, the Indian Ocean island of Réunion, a French overseas department since 1946,
experienced a massive epidemic of the mosquito borne viral infection Chikungunya – an
“emerging infectious disease” (1) never before seen in the Indian Ocean. More than

65
250,000 people, one third of the Island‟s population, were subject to a sudden onset of high
fevers, rash, and debilitating joint pains, but the media both on Réunion and in metropolitan
France were slow to pick up on the epidemic. There is no mention of chikungunya in the
Reunionese print media until April 2005, by which time the INVS (2) had already recorded
24 cases for March, and over 300 to date; and there is no mention of the epidemic in the
metropolitan French print media until January 2006, almost a year after the first cases.
Media reporting therefore demonstrates a considerable lag compared to the real-time
evolution of the epidemic, and this paper explores possible reasons for that delay. We
analyse the content of print media articles about Chikungunya from two Reunionese
newspapers (Témoignages and Clicanoo) and two newspapers from metropolitan France
(Le Figaro and Le Monde). These were selected on the basis of representativeness of a
broad cross section of readership in both places: Témoignages has a distinctive Créole
flavour (as evidenced for example by numerous interjections in the Créole language), and
Clicanoo appeals to a broader Reunionese readership including French expatriates
(Zoreilles); Le Figaro is widely acknowledged as having a right-wing agenda in
metropolitan France (Moores 2006), and Le Monde is more broadly representative of public
opinion, with its editorialists seen as “independent and committed intellectuals in the
French tradition” (Le 2004, p. 687). Our study covers all articles in these newspapers from
their first mention of Chikungunya, to the end of the epidemic in November 2006. The
apparent reluctance of the media to prioritise their reporting on the epidemic is interpreted
with reference to discourses on island identities as well as theories of risk perception that
relate to unusual health events.
Reunionese print media: Témoignages and Clicanoo
The first articles to mention chikungunya appear on 20/4/2005 in both newspapers, but only
as a passing comment about the chikungunya epidemic in the Comores. The Clicanoo
article is much longer than its Témoignages counterpart, and is more detailed and more
practical in so far as it offers advice on mosquito eradication and limiting the disease risk.
This difference already sets the trend for the main divergence between the two newspapers,

66
but they are similar in their reporting delays. The first article to report cases in Réunion
appears in Témoignages on 2/5/2005 reporting 4 cases, and the second article appears two
days later reporting 150 cases – on pages 6 and 9 respectively, almost as general interest
articles on health rather than as news items reflecting the appearance of a new virus with
dramatic increases in case numbers. In Clicanoo, the first article to report cases in Réunion
does not appear until a week later (11/5/2005), but articles are thereafter more frequent than
in Témoignages; Table 1 shows the numbers of articles published by each newspaper in
each month of the epidemic, highlighting this difference as well as showing the significant
delay between the obvious increase in case numbers reported to the INVS and the priority
given to print media reporting on the chikungunya outbreak. These delays continue to be
reflected in subsequent articles: The third and fourth articles in Témoignages appear 6 days
later (20/5/2005 and 21/5/2005), and the fifth article a full 2 weeks later when case numbers
have escalated to over 1000 cases. These articles are on pages 10, 6 and 8 respectively, still
away from the front pages where apparently more newsworthy items are placed. The
Clicanoo articles appear with greater frequency, rarely exceeding a week between articles,
but also not showing any increase in frequency that might parallel the rapidly rising case
numbers (See Table 1). The case numbers are readily available but a delay of many weeks
is evident in their use: during this time, an astute investigative journalist could easily have
become aware of the risk posed by the epidemic and would have been well positioned to
produce headlines stories therewith.
Another aspect of these early reports is that they describe the epidemic in terms that appear
to be the antithesis of sensationalism. The 14/5/2005 Témoignages article reports the
disease as new (“touche pour la première fois l‟océan Indien”), large (“épidémie de grand
ampleur”), widespread (“présent dans tous les pays”), rapidly progressive (case numbers
increasing as above), and serious (“symptômes graves”) – enough to ring alarm bells with
people with no public health training whatsoever. Yet these terms are spread factually and
dilutingly through the text, and are moderated by reassurances about official action, a
paucity of hospitalised cases, the fact that people are not contagious, and the not-fatal
nature of the virus. Overall, the risk of the epidemic is very understated in these early
reports; the short, late, and infrequent articles convey an impression of a mild disease which

67
is preventable and being dealt with effectively by the authorities. Clicanoo, with a slightly
more populist reporting style that includes many anecdotal personal statements, goes so far
as to suggest that Chikungunya is so trendy that one might almost want to catch it (“C‟est la
maladie à la mode […] qu‟avec ce nom un brin exotique, on aurait presque envie de
contracter la chikungunya”; Clicanoo, 25/5/2005). The epidemic is presented as a trivial
addition to the other „tropical‟ mosquito borne diseases, dengue and malaria, that are
already familiar to the Réunionnese (3). The Témoignage reports are dealing with the
epidemic as a non-event, a minor public health incident that does not constitute a
significant risk on an island that is perceived as modern with a solid public health
infrastructure (“Une cellule de veille des services de l‟État [DRASS] a été mise en
place….”, Témoignages 12/5/05). Clicanoo presents a clearer rôle for community
involvement in combating the disease (“une lutte communautaire”, 14/5/2005), but is no
better in these early articles at conveying a sense of urgency.
There is no significant change in this delayed and downbeat reporting over the next few
months; an incredible 6 weeks elapse between Témoignages articles 6 and 7 (15/6/2005 and
22/7/2005) despite a corresponding jump in case numbers from 1678 to 2724 – and this
during the southern winter/dry season when no vector borne disease transmission would be
expected (because of fewer mosquitoes), a point that most health reporters would seize on
fast and hard. Témoignages articles 7 to 10 are very short (< 200 words) but do add an
invitation for new cases to contact the DRASS (Direction Regionale d‟Affaires Sociales et
Sanitaires) to help target mosquito control efforts. In the same period Clicanoo publishes
23 articles specifically on Chikungunya, and also mentions the disease in other articles on
for example football (which players are struck down, 18/6/2005) and teaching (what newly
arriving teachers from France can expect, 23/8/2005). More so than Témoignages, but still
without sensationalism, there are suggestions here that people are being affected in more
than a trivial way. Then, in late September/early October 2005, there is a dramatic change
in media representations – the existence of an „unusual health event‟ is finally
acknowledged, and the government is blamed for it. For the first time, Clicanoo highlights
the DRASS‟s failure to control the epidemic: The outbreak is now acknowledged to have
never abated despite the southern winter, and government incompetence is cited as the

68
cause (“defaut d‟organisation”, Clicanoo 12/9/2005). Later, but more vehemently,
Témoignages follows suit on 13/10/2005 with an article that is suddenly much longer (>800
words) and highlights both the severity and potential for recrudescence of the epidemic
with the onset of the southern summer. Articles become more frequent (in the order of
days, then moving to sometimes two articles per day), and fundamentally different in
content. During the 2 months‟ interval between the 10th
Témoignages article and the 11th
,
the existence of an „unusual health event‟ has finally been accepted: It is reported that the
southern winter has not interrupted transmission, that there have now been over 4000
notified cases, that serious complications have arisen including fetal infections and
meningitis, and, importantly, that a whole-of-community approach is necessary to combat
the epidemic (“L‟État seul ne pourra pas éradiquer le virus”; Témoignages 13/10/2005).
This weight of evidence has made it impossible to deny the severity of the epidemic any
longer.
Accepting that the epidemic was worse than thought and that a recrudescence in the
oncoming summer would seem inevitable, the government is firmly blamed for failing to
control the situation. The issue is quickly politicised, and questions are asked in both
newspapers about the adequacy of the evaluation of the epidemic, the appropriateness of
the public health response, and the apparent tendency of the government to avoid blame by
transferring the responsibility for controlling the epidemic to families and local
communities (4). Although individual and community involvement in source reduction
(removal of potential breeding sites) is essential in urban mosquito borne disease control,
the spraying of insecticides at a broad scale by competent operators is obviously beyond the
capability of local communities (“…n‟est pas possible [..] aux agents d‟une commune
d‟appliquer un tel traitement.”, Témoignages 14/110/05). In an angry letter signed by 32
local general medical practitioners and reproduced in Témoignages 18/1/06, a major point
is made of the inappropriateness of blaming the Reunionese for allowing the virus to
spread, when mosquito control at a departmental scale needs to led by the government.
More generally the government is accused of failing to protect the public health (“Les
services de l‟État ont failli à leur mission de protection de la santé publique”, Témoignages
14/10/2005), despite having had a warning from the World Health Organization several

69
years earlier that the virus was serious enough to be considered as a potential agent of
bioterrorism (WHO 2002) (5). This latter argument finally demonstrates the type of
sensationalism one might have expected when faced with an „unusual health event‟, and the
emotive term “bioterrorism” now appears in the title of an article promoted to page 3 (“Le
bioterrorisme peut utiliser le Chikungunya”, Témoignages 17/10/2005). A barrage of
interventions that could have or should have been implemented are identified in subsequent
articles: Why was WHO assistance not requested from the beginning as it was in Comores
during the same outbreak? Why is there no attempt to devise a specific treatment or
antidote? Why is the disease burden underestimated and trivialised when an equivalent
problem in metropolitan France would have precipitated a massive response? For each of
these questions, the responsibilities and failures are projected onto the (French
Metropolitan) government, allowing the island and its inhabitants to assume the role of
victims.
In the subsequent months, new themes are introduced and additional issues raised in
relation to the epidemic, including control campaigns, loss of tourism income, and
environmental concern about insecticides; but the undercurrent of public outrage remains
consistently represented and firmly anti-government – if control campaigns are
unsuccessful, if tourist income is lost, and if local ecosystems are poisoned, these effects
remain squarely a result of governmental mismanagement. In so far as these media
representations can be assumed to reflect public opinion, their consistency illustrates the
fact that perceived health risks and the trust of public health organizations are mental
constructs that are very difficult to shift once formed (Finucane 2004). One does however
have to admire the creativity of the Reunionese, examples of which include blaming Al-
Quaïda (Clicanoo, 14/2/06) and issuing an album of Séga, the local dance music, with a
Chikungunya theme (Clicanoo, 15/6/06); but the shift from passive denial to acceptance
with active government denunciation is the only significant transition in representation
evident in Témoignages and Clicanoo up to the end of the period studied (end of epidemic,
November 2006).

70
French metropolitan print media: Le Figaro and Le Monde
The first mention of Chikungunya in the metropolitan print media studied is in Le Monde
on 16/12/2005: A technically detailed and politically neutral article reports on the disease
and its presence in Réunion, including the control efforts being implemented. The article is
an outlier in so far as the next mention does not occur for another 5 weeks, but the fact that
this information is available and has appeared without being followed up is an indication of
the low priority placed on reporting on such a „tropical‟ health issue – at least until a
„mediagenic‟ controversy is later identified. In Le Figaro (21/1/2006) the first article
appears almost a full year after the first cases were registered by the INVS; and it is not so
much about the epidemic per se, but about the conflict (“polémique”) between the island‟s
general medical practitioners and the government public health services. In a letter by local
general practitioners, the government is accused of underestimating the extent of the
epidemic, of not taking appropriate action, and of inappropriately blaming the islanders for
allowing the virus to spread (see also above, Témoignages 18/1/06). This attack on French
metropolitan government health services and representatives remains the theme for the next
four articles in Le Figaro: Case numbers are presented in support of the general
practitioner‟s claim, but official rebuttals are also documented and include statements of the
massive commitment of personnel to mosquito control (Figaro 28/1/2006), the
implementation of a surveillance system by the INVS (Figaro 30/1/2006), and official
confirmation that the situation is under control (“Le probleme est réglé”, Figaro
30/1/2006).
Le Monde is initially less focused on this controversy and again provides articles that
appear to be richer in factual detail, explaining the need for mosquito control and the
appearance of severe complications not previously recorded (29/1/2006, 4/2/2006).
However, a very metro-centric interest is apparent even from the early articles: The
emphasis is on the metropolitan public health officials‟ thoughts on the epidemics, the
metropolitan mosquito controllers being sent to Réunion, and the economic consequences
for the tourism industry. The Director General of Health is quoted as explaining that the
unusual circumstances arise because a developing world epidemic has established itself in

71
the developed world (“...une épidémie de pays en voie de développement qui survivent [sic]
dans un pays dévelopé”, Le Monde 4/2/2006). The controversy is picked up more on
8/2/2006, highlighting the rapid spread of the epidemic despite the surfeit of government
driven interventions. Le Figaro has in the interim picked up on the inundation of the
island‟s hospitals reaching crisis point (“tous les hôpitaux de l‟île [vivent] en état de crise”,
Le Figaro 6/2/2006), with the theme of controversy still remaining dominant: The
Reunionese are reported as feeling abandoned and panicked despite many personnel, much
financial support, and free anti-mosquito kits being provided by the government (ibid). The
statement “They had forgotten that they were an Indian Ocean island” (“La Réunion a
oublié qu‟elle était une île de l‟ océan Indian”, ibid.) indicates that the islanders should not
be so surprised by an epidemic of tropical disease since their island is, after all, in tropics.
In Le Figaro, the epidemic per se (disease burden, spread) only becomes the dominant
theme when it is realised that the vector mosquito, Aedes albopictus, also occurs in
metropolitan France - and that and importation risk for Chikungunya may therefore exist
(Le Figaro 9/2/2006, 25/2/2006). From this point on, the polemical differences of opinion
between islanders and officials take a back seat, and information about the epidemic is
presented in three major areas that are presumably of direct interest to the metropolitan
readership: The seriousness of the disease once contracted, the latest research findings, and
the appropriateness of the public health response. Severity of infection: Although
originally thought to be benign, the severe complications that can arise are now highlighted
(Le Figaro 18/2/2006), particularly neonatal meningoencephalitis (Le Figaro 27/2/2006),
and Chikungunya-associated mortality which has never before been recorded (“Premier
décès attribué au chikungunya”; Figaro 6/3/2006). The seriousness of the disease becomes
a major tourist deterrent (Figaro 23/2/2006, 1/3/2006). Research findings: Knowledge
generation about the „tropical disease‟ becomes a priority, and is coordinated by a newly
formed national research centre with over 9 million euros of funding (Le Figaro 22/2/2006,
27/2/2006). The aim is to establish why severe symptoms never before recorded (above)
have appeared in this epidemic. A major launch of research on the island is highlighted at
the end of February (Le Figaro 28/2/2006). Appropriateness of response: The official
management of the epidemic is now described as possibly negligent (Le Figaro 22/2/2006)

72
bordering on a total stuff-up (“gabegie totale”; Le Figaro 23/2/2006), and emphasising that
virtually nothing was done in terms of health promotion (community education about
control and avoidance measures). Some 76 million euros are invested to provide free
medication and repellents to the needy, to step up mosquito control, to fund research
(above), and to revitalise the devastated tourist industry (Le Figaro 27/2/2006).
No similar change is reflected in Le Monde, where the importation risk is not highlighted
and the emphasis continues to remain on other metropolitan issues (the travels to the island
of the President and Ministers [24/2/2006 et seq], and the arrangements for tourists to
rebook their flights for later travel without penalty [16/2/2006]). The islanders are
nevertheless afforded an intermittent voice, and here too the feeling of abandonment comes
through strongly - particularly when the attention paid to their epidemic is compared to the
far greater interest shown in bird flu (“Les poulets sont plus importants que les
Réunionnais”, Le Monde 22/2/2006) (6).
From March 2006, a significant decrease in the number of cases is reported (“épidémie en
repli”, Le Monde 14/3/06; “décru spectaculaire”; Le Figaro 30/3/2006), and subsequent
articles on the Réunion epidemic are limited to reporting on this continuing downward
trend in both numbers of cases and in impact. Some selected research findings are
discussed intermittently, and there is then an ever decreasing interest shown (which reflects
in both the number and content of articles), until the end of the epidemic and study period
(November 2006).
Discussion
A key finding in analysing these media reports is the significant delay in reporting on the
epidemic: Firstly in the Réunionnnais newspapers, suggesting passive denial in the early
stages of the epidemic; and secondly in the French metropolitan newspapers, suggesting
that residual colonialist thinking may be influencing the priority placed on reporting on
such an epidemic in a remote tropical location. It is possible that a contributing factor to

73
the delays is also a failure of public health officials to adequately communicate the
potential gravity of the situation to the media and public; Watin (in press) highlights the
apparent disinterest of public health authorities in the early stages of the epidemic, and we
have previously shown (Weinstein and Ravi, 2008) that the rhetoric of the official INVS
bulletins on the epidemic reflected an underestimate of the potential public health risk
posed by Chikungunya. However, regular INVS bulletins giving case numbers were
readily available to journalists from the first month of the epidemic (see Table 1.), so we
argue here that the delays were more likely to result from a reluctance on the part of the
media to prioritise their reporting on the epidemic for either or both of the above reasons:
early denial and postcolonialist trivialisation of the public health risk posed by the virus.
The manner in which public health risk is constructed is a result of risk perception - a social
construct in which health hazards are mentally „scaled‟ from negligible to catastrophic
based on characteristics of the hazard itself as well as on attributes of individuals in the
population of interest. To better understand such „scaling‟, the relevant characteristics of
hazards have been construed in terms of „personalities‟ defined predominantly by “dread
risk” and “unknown risk” (Slovic 1997, 1998; Finucane 2004). Dread risk is the extent to
which the hazard is dreaded by the community, with strong elements of lack of control,
being involuntary, inequitable, and potentially fatal or catastrophic: For example, nuclear
reactor accidents are perceived as posing a greater risk to health than does smoking.
Unknown risk is the extent to which the risk is unfamiliar to the community, with strong
elements of unobservability, lack of understanding, and delayed consequences: For
example, pesticides and asbestos are perceived as posing a greater risk to health than do car
accidents. The „personality‟ of a hazard is the mix of dread risk and unknown risk that it
presents, and at the media and community level is obviously strongly influenced by the
perceivers‟ particular mix of age, gender, ethnicity, education, sociopolitical attitudes, and
belief systems (including religion). In the specific case of the Réunion Chikungunya
epidemic, different Reunionese therefore perceived the risk from mosquitoes differently:
For example, residents of European origin were very concerned about being bitten by these
(unknown, tropical) insects, as reflected in the media by their complaints about the
inadequacy of mosquito control efforts. Their feelings of lack of control were exacerbated

74
by feelings of abandonment (inequity), leading to hightened perceptions of “dread” risk.
The non-white Créole community on the other hand perceive the (known, local) mosquitoes
only as a nuisance, against which herbal repellents provide adequate protection (above; Le
Monde, 23/2/06); they thus have control, and in any case often do not believe that
mosquitoes cause the disease.
In the metropolitan newspapers, the perception of the severity of the public health risk
posed by the disease, and the need to understand (research) and control it, take on new
significance after the realisation that the epidemic could pose a threat to residents of
metropolitan France (above; Le Figaro 9/2/2206, and “Plus proche que l‟on ne croit”,
25/2/2006). While the disease was seen as a purely tropical phenomenon, the central
government could afford to relax (“Le fait qu‟il s‟agisse d‟un départment d‟outre-mer a
sans doute conduit le pouvoir central à une certaine négligence”; Figaro 22/2/2006). With
the possible threat to metropolitan France identified, the rhetoric of the newspaper articles
changes to one of a more inclusive approach to „health for all‟, with suggestions such as the
modification of national surveillance systems to better deal with emerging infectious
diseases (Le Figaro, 2/2/2006) (see also (4)). There is a realisation that to decrease the
public health risk to their own populations, Western countries need to invest in protecting
the health of more vulnerable populations in developing and tropical countries that can act
as sources of emerging infectious diseases (Le Figaro, 3/3/2006). Such an approach is
consistent with recent developments in international public health policy (WHO 2000), but
where better for France to start reducing this international risk of emerging infectious
diseases than in one of its own overseas departments?
There are representations in the French metropolitan print media that clearly indicate a
persistence of colonialist thinking in officialdom: Two examples have been cited; the
explanation of a third world disease impinging on the developed world, and the lack of
surprise that might have been anticipated when a tropical disease occured on a tropical
island (above; Le Monde, 4/2/2006; Le Figaro 6/2/2006). The emphasis on research
provides another such example: Although not apparent until more than a year after the
onset of the epidemic, the new research emphasis can be interpreted as a scholarisation of

75
the problem. A clinical approach to knowledge generation allows metropolitan public
health officials and politicians to distance themselves from the very real suffering,
including deaths, to which over 250,000 people - one third of the island‟s population - were
subject. This process of distancing from the epidemic is similar to one evident in the INVS
reports on Chikungunya, which represent the epidemic in tropicalist terms with a degree of
unempathetic „othering‟ of Indian Ocean health events (for detailed discussion, see
Weinstein and Ravi 2008). The effects of these colonialist representations are to contribute
both directly and indirectly to the perceived risk posed by Chikungunya: Directly because
they allow officialdom to distance itself from the risk by „othering‟ the disease to the
remote tropics, and therefore perceiving no risk to metropolitan France; and indirectly
because such representation influence the formation of risk perceptions by the
(metropolitan) readership.
The Reunionese newspapers, by contrast, contain few representations of the nature of the
risk, but focus strongly on the attribution of blame for the risk; after an initial period of
apparent denial of the presence of a potential public health hazard, the presence of such a
hazard is accepted and blamed firmly on the government. Poumandère (2007) describes
this transition as reflecting the change from social attenuation to social amplification of the
constructed risk (passage de l’atténuation à l’amplification sociales de ce risque, p.340) -
and there is clearly also an element of reciprocity here in so far as the media itself
influenced public perceptions of risk posed by the epidemic (Idelson 2007). From a certain
perspective, this dichotomous representation of the epidemic - with passive denial on one
hand and acceptance with active government denunciation on the other - reflect the
dichotomous aspects of Reunionese identity. Denial “haunts the contemporary Reunionese
discourse” (Vergès 2003, p. 162), with a violent history of slavery, indentured labour and
colonialism still not being adequately acknowledged (7). In such an historical environment,
Glissant (1981, p. 101) interprets passive denial as a cultural trait that results from that
environment itself; only physically strong but passive slaves survived. And there was
suffering. Suffering “turns into lament, lament into anger, anger into violence [ ] against
France” (Vergès 2003, p. 162), providing an undercurrent that persists through two
centuries of slavery and one century of colonialism right up to the present day. Thus, once

76
the scale and extent of suffering from Chikungunya infection became undeniable, the
suffering turned to anger against the „French‟ government, with representations in the
media reflecting this by means of fervent denunciations. “Que font les élus?” (What are the
elected representatives doing?) is often heard in relation to any discontent on Réunion
(Vergès 2003, p.165), and in a sense is „othering‟ the problems of the island onto
metropolitan France. This is a direct reversal of the metropolitan „othering‟ of tropical
diseases that is evident as „distancing‟ (discussed above), and can be interpreted as a form
of “writing back” (Ashcroft et al. 1989).
An interesting debate is that surrounding the extent and appropriateness of involvement of
Reunionese in mosquito control to combat the epidemic. Complaints about the lack of
health promotion activities and community involvement have been presented above (Le
Figaro, 23/2/2006), and are reinforced by descriptions of hundreds of mosquito controllers
being deployed from metropolitan France, rather than enlisting local Reunionese (Le
Monde, 22/2/2006). However, it could be argued that placing more emphasis on enlisting
locals in mosquito control operations could have jeopardised such operations: A full two
thirds of Reunionese do not believe that the disease is mosquito borne (Gaüzère and Aubry
2006, p. 25), and are therefore unlikely to have embraced the campaign efficiently and
effectively. Some insight into the local belief systems that result in this situation is
provided in the form of a report about a lady who has used citronella (a herbal mosquito
repellent) for the last 40 years, and has always been alright so does not believe that the ill
could originate from the insects (Le Monde, 23/2/2007). Such a belief is reinforced by the
observation that the mosquitoes are being killed, but that the epidemic is worsening. A
hospital psychologist explains that in times of crisis old beliefs and superstitions resurface
(ibid), and Réunion is well known for a preponderance of such beliefs (8). Thus an
exploration of local belief systems would appear integral, even critical, to managing an
„unusual health event‟ in the multicultural environment of Réunion, particularly with
respect to informing health education and public health practice about what approaches
might be most culturally appropriate on the island.

77
Belief systems are fundamental modulators of people‟s risk perception and their subsequent
health protective behaviour (Douglas and Wildavski 1982), yet consideration of these
cultural aspects may have been overlooked in the top-down management of the
Chikungunya epidemic by the French metropolitan government. Religion in particular
stands out as a determinant of perceived risk, and forms the subject of another discussion
which is beyond the scope of the present paper. Perceptions of risk are rapidly formed and
difficult to alter, making it imperative to explore the potential influence of different belief
systems before an understanding of them becomes critical to the management of an
„unusual health event‟. Armed with this knowledge, public health practitioners could have
a more powerful opportunity to reduce the community burden of disease, because they are
then in a position of influencing the early formation of different community perceptions of
risk, and thus also the translation of those perceived risks into public health practice. We
have shown here that such an approach could be particularly valuable in a multicultural
society where community perceptions of risk may be different from those predicted in a
Western paradigm.
Endnotes
(1) An “emerging infectious disease” is defined as an infectious disease which is rapidly
increasing in one or more of: the numbers of cases occurring, the geographic distribution of
cases, or severity of symptoms. Prominent example include the recent pandemic of human
HIV infections and the appearance of SARS.
(2) The INVS (Institut National de Veillance Sanitaire (National Institute of Health
Surveillance) is the national coordinating body for communicable disease surveillance and
control, and has responsibility for reporting on epidemics for all departments of France,
including the overseas departments of La Réunion, Martinique, Guadaloupe and Guyane).
All departments provide disease surveillance data to the INVS, where data are analysed
centrally and the results published in INVS bulletins.

78
(3) Malaria first appeared in Réunion in 1869, was declared eradicated in 1973, and now
only imported cases continue to occur. Dengue first appeared in 1873, and although also at
one stage eradicated (1952), introduced cases seeded further epidemics in 1977-78, 2004,
as well as concurrently with the 2005-6 Chikungunya epidemic.
(4) In urban environments, vector borne disease control depends on top-down and bottom-
up management approaches working synergistically. Ultimately only individual
householders can eliminate all the containers of standing water that might provide suitable
environments for mosquito larvae (garbage, pot plants, blocked gutters, old tyres, etc.); but
only governments can coordinate the large scale spraying of insecticides required to kill
larvae in larger water bodies, or to „knock-down‟ adult mosquitoes during an epidemic.
(5) This WHO report summarises the requirements for minimising the potential impact of
microbial pathogens used as agents of bioterrorism. It lists the agents of potential concern
(which include Chikungunya virus), and outlines global surveillance and response needs to
limit the spread of epidemics. The recommended strengthening of surveillance systems
would equally improve countries‟ ability to respond effectively to “emerging infectious
diseases” as defined in Endnote (1)
(6) Although „Bird Flu‟ virus is closely related to human influenza virus and can infect
people, without a significant mutation it cannot be transmitted from person to person.
Because Bird Flu was and (at the time of writing) remains epizootic (epidemic in animals)
on a global scale, and because the possibility of mutation to cause a human flu pandemic
remains, there is a global „hysteria‟ to prepare for the worst. It is understandable that a
population experiencing an actual epidemic of Chikungunya should be cynical about the
disproportionate amount of time, energy and funding being spent on a potential epidemic of
flu.
(7) The European discovery of Réunion was by the Portuguese in 1512, with the French
being the first to settle the uninhabited island over a century later. From 1715 they
imported African and Malagasy slaves to support the growth of the coffee industry,
providing the basis of the island‟s Créole community. Following the abolition of slavery in

79
1848 they were joined by large numbers of indentured labourers for the island‟s sugar cane
industry, chiefly from India and China. The Créole community was (and arguably remains)
subject to the imposition of a dominant French culture in a situation analogous to that of
colonial occupation.
(8) As a result of the varied ethnic makeup of the Reunionese (see Endnote 7), a great
variety of belief systems coexist and mingle on the island, ranging from animist magic of
Malagasy origin, through Hindu, Buddhist and Islamic beliefs, to Roman Catholicism. An
example of the interesting interactions between these religions is afforded by the grave of
the late 19th
century sorcerer and bandit Le Sitarane in St-Pierre: Black magic rites are
practiced at his grave in a Catholic cemetery – the latter incidentally also providing a
variety of water holding containers for both flowers and mosquito larvae.
Acknowledgements
We thank Dr Gilbert Potier, Mme Ségolène Bernard, Dr Karin LeRoux, Prof Alain
Michault and Mlle Bénédicte André for insightful discussions about the epidemic and for
their hospitality whilst in Réunion. Lovisa Rosnäs assisted with the compilation of media
reports, and Agnes Weinstein with typing the manuscript. The research was funded, in
part, by the Graduate Research School at the University of Western Australia.

80
Table 1. The number of cases of Chikungunya by month and the corresponding numbers
of print media reports mentioning Chikungunya. A considerable delay is evident between
the first occurrence of cases and the first articles in the Reunionese newspapers
Témoignages and Clicanoo; a further delay is evident before the appearance of articles in
the metropolitan French newspapers Le Figaro and Le Monde.
Month Number Number of articles
of cases* Témoig. Clicanoo+
Le Figaro Le Monde
February 05 0 0 0 0 0
March 24 0 0 0 0
April 281 1 1 0 0
May 1486 4 10 0 0
June 1234 2 9 0 0
July 449 1 3 0 0
August 410 3 5 0 0
Sept 458 0 7 0 0
Oct 616 11 15 0 0
Nov 967 9 24 0 0
Dec 6667 20 19 0 1
January 06 54136 77 146 6 2
Feb 127073 169 482 41 34
March 45202 70 319 29 13
April 14667 31 116 11 7
May 5267 20 91 10 11
June 2700 17 65 1 2
July 141 20 48 2 1
August 90 12 45 3 1
Sept 57 10 67 6 1
Oct 57 9 56 4 3
Nov 32 6 40 2 2
* Based both on notifications (before Dec 05 and after June 06) and estimates (Dec 05
to June 06 inclusive) from the INVS (2005-6).
+
Includes letters to the Editor.

81
Chapter 5
General Discussion

82
5.0 General Discussion
It was the aim of this thesis to explore attitudes underlying the management of the 2005-6
Chikungunya epidemic in Réunion by examining representations of mosquito borne disease
from historical, epidemiological and media perspectives. I sought to answer the question
“Does colonial history continue to influence the representation and management of
mosquito borne disease in Réunion?”, and used three different sources to do so: the
scientific literature on mosquito borne disease epidemics that occurred on the island before,
during and after a paradigm shift in Western thinking about disease causation; the official
reports on the Chikungunya epidemic in the bulletins of the Institut National de Veillance
Sanitaire (INVS) from the beginning to the end of the epidemic; and newspaper articles
about Chikungunya from two Reunionese newspapers (Témoignages and Clicanoo) and
two newspapers from metropolitan France (Le Figaro and Le Monde). In each of these
print media it was clear that the representations (and the changes in representations with
time) were influenced by tropicalism and colonialism: In the historical scientific literature,
tropicalism persisted through a major shift in Western thought; in the INVS bulletins,
„distancing‟ from a tropical problem failed when the perceived risk to metropolitan France
increased; and in the newspaper articles, a considerable reporting lag reflected residual
colonialist thinking in not prioritising reporting on the epidemic. Taken together, these
three pieces of converging and corroborative evidence provide strong support for Said‟s
(1979) contention that „Othering‟ is a generalisable ahistorical phenomenon. In the case of
the 2005-6 Réunion Chikungunya epidemic, it is likely that „othering‟ contributed to the
suboptimal management of the epidemic, resulting in considerable preventable morbidity
and mortality in the Reunionese population.
5.1 The rôle of tropicality in public health practice in postcolonial societies
Othering may provide the ultimate driver for the persistence of tropicality in public health
practice in Réunion, but other more proximate drivers are likely to also play significant

83
rôles. I have discussed how the cost of administering interventions to combat tropical
diseases at the population level have historically held back colonial public health initiatives
(Chapter 3); if tropicalist attitudes to public health provision were formed by a need to
create an inferior, ignorant and diseased “Other”, then they were maintained by a need to
restrict public health expenditure in the widely dispersed, costly environments of French
overseas departments and territories. I have also discussed how the power relationships on
the island could have led to the denial of a serious public health risk (Chapter 4); with a
violent history of slavery, indentured labour and colonialism still not being adequately
acknowledged, denial has become a cultural trait in Réunion. One further potential driver
is worthy of consideration here, and that is the significant rôle of the colonies in forming
and maintaining the French national identity.
Girardet (1972) attributes to the French territories the very makings of France as a great
nation (“ce sont ses territories d‟Outre-Mer qui confèrent à la France son rang de grande
puissance”; p.288). Perhaps importantly for a nation that was itself „colonised‟ by
Germany during WWII, France utilised its government-in-exile and unconquered Africa
possessions as launching-pads for the re-conquest, thereby conceiving a national identity of
an unconquered and united empire, despite the temporary occupation of one part thereof
(ibid p.281). Following decolonisation, these former colonies and overseas territories
continued to play an equally important role in affirming France as a world power:
Financially unable to compete with the economic and military domination that allowed the
USA to become a global political power, France nevertheless retained the ability to „punch
above its weight‟ in international politics because of the special relationship it retained with
francophone countries on every continent – and most importantly Africa. Without the
resources of a superpower but with the political will to retain major-power status
internationally, France has concentrated its foreign policy and trade on this continent which
is within its means (Staniland 1987 p.56). Cultural and linguistic links are strong,
persistent and politically influential and to some extent provide an alternate approach to
economic and military neo-colonialism. Although the approach has been partly successful
in asserting the international importance of France, it has also led to its own problems,
particularly where former territories have been integrated into France proper as DOMs
(Départment Français d‟Outre Mer). After Réunion became a DOM in 1946, the slowness

84
of departmentalisation in practice led many Reunionese to feel abandoned (Combeau and
Maestri 2002, p.120) – the same feeling recently voiced in relation to the Chikungunya
epidemic (“Nous nous sentons abandonnés”; Clicanoo 26/1/06). In some sections of the
metropolitan population, it is in fact felt that this abandonment should be intensified,
because of the disproportionately large slice of the French social security budget that is
dedicated to supporting the 30% of Reunionese who are unemployed – an ironic twist for
the tropical peoples whose exploitation once filled the coffers of the French Government.
This discussion would be incomplete without mention of the one arguably positive role that
tropicalism has played in the management of mosquito borne disease (although apparently
not in the Réunion Chikungunya epidemic), regardless of the appropriateness or otherwise
of the underlying ideology. Tropicalism carries with it an element of climatic determinism
(Chapter 2), with man seen as dominated by a hostile environment. However, it is in the
Judaeo-Christian mindset to conquer, dominate and exploit such hostile environments, to
pursue the God-given right of dominion over the earth – and this latter approach became a
possibility with the advent of the contagionist approach to managing tropical mosquito
borne diseases. Large-scale, military-style campaigns to eradicate mosquitoes and the
diseases they carried were introduced (Harrison 1978), all as part of the colonial duty to
improve the health of the helpless and uncivilised natives with Western knowledge and
technology not otherwise available to them. Together with improvements in the standard of
living, these assaults often succeeded in dominating the tropical environment, as evidenced
by the eradication of both endemic dengue fever and endemic malaria from Réunion by
1952 and 1973 respectively (see Chapter 3, Table 1). Veterans of these eradication
campaigns might argue that ‟greener‟ thinking – a more sustainable co-existence with
nature, an avoidance of toxic insecticides, and the incorporation of indigenous knowledge –
has contributed to the re-emergence of mosquito borne disease as a significant public health
problem globally: The emergence of Chikungunya in Réunion in 2005 would support this
argument, as would the current global resurgence of malaria (with case numbers at an all
time historical high). Thus, despite negative cultural implications, a tropicalist approach to
controlling epidemics of mosquito borne disease did deliver a historically successful public
health programme in Réunion.

85
The apparent paradox of a tropicalist approach to public health practice being beneficial in
some situations (dengue, malaria) and detrimental in others (Chikungunya) can perhaps be
resolved by considering health from a broader holistic perspective: The advantages in
mosquito control to be gained from a tropicalist approach are arguably offset by the disease
burden that results from cultural domination and financial and educational disadvantage.
Conversely, the health gains associated with self determination may be offset by a loss of
critical mass of rapidly deployable pubic health infrastructure. It is apparent from this case
study of mosquito borne disease in Réunion that an optimal balance of these factors is not
easily achievable; added to the uncertainties and variability of global changes in climate,
travel, and trade that all affect mosquito borne disease ecology, it is likely that these
diseases will remain a permanent thorn in the side of public health practice.
5.2 Recommendations for further research
This study is original in so far as it is multidisciplinary, drawing on discourses on
tropicality, public health, risk perception, and postcolonialism to interpret the findings. The
approach has provided insights that might not otherwise have come to light; foremost
amongst these is the value that textual analysis can add to our understanding of public
health, and therefore also to the management of „unusual health events‟ to minimise the
community disease burden.
One significant aspect of the contribution of textual analysis to public health practice that
was identified but not pursued in this thesis, is an exploration of the relationship between
belief systems and health practice in multicultural societies. We saw, based on an analysis
of print media reports, that belief systems modulate people‟s risk perception and therefore
their subsequent health protective behaviour. An understanding of these relationships is
critical to the management of „unusual health events‟, and textual analysis provides one
useful approach to discovering the most relevant aspects of such complex interactions.
Armed with information so derived, public health practitioners would be well positioned to

86
reduce the community burden of disease by providing more culturally appropriate advice
and implementing more acceptable public health interventions.
In addition, I hope that the present study has added to the evidence supporting the value of
multidisciplinary research. If „othering‟ contributed to the suboptimal management of the
Chikungunya epidemic and thus also to a considerable preventable disease burden, then
tropicalism seems likely to continue to influence public health practice adversely for the
foreseeable future: Regardless of our understanding of the mechanisms of disease
transmission in the physical space of tropical epidemics, affected populations will continue
to suffer a preventable disease burden until such a time as the conceptual space of tropical
Otherness is changed. Ongoing research collaboration between the Humanites and Health
Sciences can only help to bring such a time closer.

87
Bibliography

88
6.0 Bibliography
Arnold, D. (1996) Warm Climates and Western Medicine. Amsterdam, Rodopi.
Arnold, D. (2003) Imperial medicine: Patrick Manson and the conquest of tropical disease.
Victorian Studies 45: 733-735.
Ashcroft, B., Griffiths, G. and Tiffin, H. (1989) The Empire Writes Back: Theory and
Practice on Post-Colonial Literatures. London: Routledge.
Bailey, P., Hopkins, D. and Weinstein P. (2004) Pests and Pest Control, In: Cromar N,
Cameron S, and Fallowfield H, Environmental Health in Australia and New Zealand,
Melbourne: Oxford University Press, Ch. 24, pp.395-409.
Barat [no initial] (1869) Étude sur la fievre épidémique qui a régné en 1869 a l‟ile de la
Réunion. Archives de Médécine Navale 12: 422-440.
Blakely, D.E. (2003) Social construction of three influenza pandemics in the New York
Times. Journalism and Mass Communication Quarterly 80: 884-902
Bowd, G. and Clayton, D. (2005) Tropicality, orientalism and French colonialism in
Indochina: The work of Pierre Gourou, 1927-1982. French Historical Studies 28: 297-327.
Bruneau, M. (2005) From a centred to a decentred tropicality: Francophone colonial and
postcolonial geography in Monsoon Asia. Singapore Journal of Tropical Geography 26:
304-322
Brygoo, E.R. and Brunhes, J. (1971) Historique de la filariose lymphatique a l‟ile de la
Réunion. Arch Inst Pasteur Madagascar 40: 47-56.

89
Cameron, S. (2004) Communicable Disease Control, In: Cromar N, Cameron S, and
Fallowfield H, Environmental Health in Australia and New Zealand, Melbourne: Oxford
University Press, Ch. 13, pp. 198-212.
Charrel, R.N., de Lamballerie, X. and Raoult, D. (2007) Chikungunya outbreaks – the
globalisation of vectorborne diseases. New England Journal of Medicine 356:769-71
Chin, J. (2000) Control of Communicable Disease Manual, 17th edition, Washington:
American Public Health Association.
CIA (Central Intelligence Bureau) (2006) World Fact Book,
http://sportsforum.ws/sd/factbook/index.html. Accessed 4/6/06.
Claval, P. (2005) Colonial experience and the development of tropical geography in France.
Singapore Journal of Tropical Geography 26: 289-303.
Clicanoo. All articles containing the search term “Chikungunya”, 2005 and 2006.
http://www.clicanoo.com/, accessed November 2006.
Combeau, Y. and Maestri, E. (2002) Histoire de La Réunion, Nathan, Paris
Cotholendy [no initial] (1873) Relation de l‟épidémie de dengue qui a régné a Saint-Denis
(Réunion) pedant les mois de février, mars, avril et mai 1873. Archives de Médécine
Navale 20: 190-209.
Douglas, M. and Wildavsky, A. (1982) Risk and culture: An essay on the selection of
technical and environmental dangers. Berkley: University of California Press.
ECDC/WHO (European Centre for Disease Prevention and Control/ World Health
Organisation) (2007) Mission Report, Chikungunya in Italy: Joint visit for a European Risk
Assessment 17-21 September 2007. ECDC/WHO.

90
Edgar, A. and Sedgwick, P. (eds) (1999) Cultural Theory, The Key Concepts. London:
Routledge.
Edmond, R. (2005) Returning fears: Tropical disease and the metropolis. In: Driver F and
Martins L (eds) Tropical visions in the age of empire. Chicago, University of Chicago
Press, Ch.10 pp. 175-94.
Finucane, M.L. (2004) The psychology of risk judgements and decisions. In: Cromar N,
Cameron S and Fallowfield H (eds) Environmental Health. South Melbourne: Oxford
University Press, Ch 9 pp 142-55.
Frenkel, S. and Western, J. (1988) Pretext or Prophylaxis? Racial Segregation and Malaria
Mosquitoes in a British Tropical Colony: Sierra Leone. Annals of the Association of
American Geographers 78 (2) 211-28.
Gaüzère, B.-A. and Aubry, P. (2006) Le chik, le choc, le cheque. Sainte-Marie (Réunion):
Azalées Éditions.
Girardet, R. (1972) L‟idée coloniale en France de 1871 à 1962. La Table Ronde, Livre de
Poche.
Glissant, E. (1981) Le Discours antillais. Paris: Seuil.
Gourou, P. (1947) Les pays tropicaux: Principes d‟une géographie humaine et économique.
Paris: Presses Universitaires de France.
Hamon, J. and Dufour, G. (1954) La lutte antipaludique à la Réunion. Bull Org Mond Santé
11: 525-556

91
Harrison, G. (1978) Mosquitoes, malaria and man: A history of the hostilities since 1880.
EP Dutton, New York.
Idelson, B. (2007) L‟épidémie de Chikungunya à la Réunion, medias, opinion publique et
pouvoirs publiques dans la crise. In: Abstracts, Chikungunya et autres arboviroses
émergentes en milieu tropical (CRVOI and INVS, 3-4 December 2007, Saint-Pierre, La
Réunion): 339.
INSEE (Institut National de la Statistique et des Études Économiques) (2006) Tableau
économique de la Réunion. St-Denis: INSEE.
INVS (2005-6a) Points de situation générale sur l‟epidémie de chikungunya à La Réunion/
Océan Indien. http://www.invs.sante.fr/surveillance/chikungunya/actu.htm. Accessed
22/8/06.
INVS (2005-6b) Points epidémiologiques hebdomedaires sur l‟épidémie de chikungunya à
La Réunion, http://www.invs.sante.fr/surveillance/chikungunya/actu.htm. Accessed
10/12/06.
INVS (2006) National Institute for Public Health Surveillance: “monitor, alert, prevent”.
http://www.invs.sante.fr/presentations/default.htm. Accessed 8/5/06.
INVS (2006a) Cas de chikungunya importés en métropole.
http://www.invs.sante.fr/surveillance/chikungunya/actu.htm. Accessed 10/8/06.
INVS (2006b) Maladies à déclaration obligatoire.
http://www.invs.sante.fr/surveillance/chikungunya/actu.htm. Accessed 10/8/06
INVS (2006c) Maladies à déclaration obligatoire.
http://www.invs.sante.fr/surveillance/mdo/declaration.htm. Accessed 23/9/06.

92
INVS (2006-7) Bulletin hebdomadaire de surveillance de la grippe saisonnière, Saison
2006/2007 (Surveillance de la grippe, semaine 40. 13 octobre 2006 to Surveillance de la
grippe, semaine 06. 16 février 2007)
http://www.invs.sante.fr/surveillance/grippe/default.htm. Accessed 18/2/07.
Juliano, S. A. and Lounibos, P.L. (2005) Ecology of invasive mosquitoes: effects on
resident species and on human health. Ecology Letters 8 (5), 558-574
Julvez, J., Ragavoodoo, C., Gopaul, A.R. and Mouchet, J. (1998) Maladies humaines
transmises par les culicides dans les Îles du sud-ouest de l‟Océan Indien. Bulletin de la
Société de Pathologie Exotique 91 (1) 99-103
Kenny, J.T. (1995) Climate, Race, and Imperial Authority: The Symbolic Landscape of the
British Hill Station in India. Annals of the Association of American Geographers 85(4):
694-714.
Kiple, K.F. (1997) Plague, Pox and Pestilence. London: Phoenix Illustrated.
Kuhn, T.S. (1962) The Structure of Scientific Revolutions. Chicago: University of Chicago
Press
Lassalle, C., Grizeau, P., Isautier, H., Bagnis, O., Michault, A. and Zeller, H. (1998)
Epidemiological surveillance of grippe and dengue, Réunion, 1996. Bulletin de la Société
de Pathologie Exotique 91 (1): 61-3
Le, E. (2004) Active participation within written argumentation: metadiscourse and
editorialist's authority. Journal of Pragmatics 36: 687-714.
Le Figaro. All articles containing the search term “Chikungunya”, 2005 and 2006.
http://www.lefigaro.fr/, accessed November 2006.

93
Le Monde. All articles containing the search term “Chikungunya”, 2005 and 2006.
http://www.lemonde.fr/, accessed November 2006.
Lougnon, P. (1944) Essai sur l‟ethnologie et la pathologie de l‟Île de la Réunion. Thèse
Médicale, Montpellier.
McLeod, J. (2000) Beginning Postcolonialism. Manchester: Manchester University Press.
Mills, S. (1997) Discourse. London: Routledge.
Moores, P. (2006) Media demonisation, „la fabrique de la haine‟ and Le Figaro.
http://wjfms.ncl.ac.uk/MooresWJ.htm, Accessed 28/1/08.
Mouazé, F. (c.2003) Clin d‟Oeuil de la Réunion. Île de la Réunion, Editions Clin d‟Oeuil.
MSS (Ministère de la Santé et des Solidarités) (2006) Circulaire NoDGS/SD5C/2006/310
du 10 juillet 2006, République Française: Ministère de la Santé et des Solidarités.
Parmar, J. and Ramani, K.V. (2008) Increased mortality rate associated with chikungunya
epidemic, Ahmedabad, India. Emerging Infectious Diseases
http://www.cdc.gov/EID/content/14/3/412.htm. Accessed 21/3/08
Poumadère, B. (2007) Le Chikungunya à la Réunion: entre atténuation et amplification
sociales du risque. In: Abstracts, Chikungunya et autres arboviroses émergentes en milieu
tropical (CRVOI and INVS, 3-4 December 2007, Saint-Pierre, La Réunion): 339-40.
Raynal, J. (1928) Enquête sanitaire à la Grande Comore en 1925: Observation de paludisme
à forme épidémique. Bull Soc Path Ex 21: 35-54 & 132-141
Reed, A.W. (1977) Treasury of Maori Exploration. AH & AW Reed, Wellington.

94
Rosen, G. ([1958]1993) A history of Public Health, Expanded Edition. Johns Hopkins
University Press, Baltimore.
Said, E. (1979) Orientalism. New York: Vintage Books.
Sallares, R. (2002) Malaria and Rome: A History of Malaria in Ancient Italy. Oxford,
Oxford University Press.
Salaun, H. and Julvez, J. (1981) La dengue à La Réunion. Communication séminaire, La
Réunion: OMS inter-îles Océan Indien.
Slovic, P. (1998) The risk game. Reliability Engineering and Systems Safety 59: 73-7
Slovic, P., Malmfors, T., Mertz, C.K., Neil, N. and Purchase, I.F.H. (1997) Evaluating
chemical risks: Results of a survey of the British Toxicology Society. Human and
Experimental Toxicology 16: 289-304.
Schaffner, F. and Karch, S. (2000) Première observation d‟Aedes albopictus (Skuse 1894)
en France métropolitaine. Comptes Rendus de l‟Academie des Sciences, Paris (Sciences de
la vie) 323: 373-5
Sinha, V. (2004) British colonial rhetoric on „modern medicine‟ and „health at home‟:
Realities of health conditions in 19th century Britain. In: Ravi S, Rutten M and Goh BL
(eds), Asia in Europe, Europe in Asia, The Netherlands: International Institute for Asian
Studies.
Staniland, M. (1987) Francophone Africa: the Enduring French Connection. Annals of the
American Academy of Political and Social Science, 489: 51-62.
Témoignages. All articles containing the search term “Chikungunya”, 2005 and 2006.
http://www.temoignages.re/, accessed November 2006.

95
Trelat, U. (1864) Tumeurs lymphatiques. Bull Soc Chir (Paris 2e S.), 5: 306-312
Vaxelaire, D. (2002) Portraits d‟une île. Ste-Marie (Réunion): Azalées Éditions.
Vergès, F. (2003) The Island of Wandering Souls. In: Edmond R and Smith V (eds)
Islands in History and Representation. London: Routlege Research in Postcolonial
Literatures, Ch 10 pp 162-76.
Watin, M. (in press) Polémique, rumeur et tension: Aspects de la « crise » du chikungunya
dans l‟espace publique médiatique Réunionnais. In: Chronique d‟une crise sanitaire,
économique et sociale: L‟île de La Réunion face au Chikungunya. Paris, UMR Prodig,
Infogéo.
Weinstein, P. (1997) An ecological approach to public health intervention: Ross River virus
in Australia. Environmental Health Perspectives 105: 364-6
Weinstein, P. (2005) Human health is harmed by ecosystem degradation, but does
intervention improve it? A research challenge from the Millennium Ecosystem
Assessment. EcoHealth 2: 1-3.
Weinstein, P. and Ravi, S. (2008) The failure of colonial „distancing‟: changing
representations of the 2005-6 Chikungunya virus epidemic in Réunion. Singapore Journal
of Tropical Geography (in press).
WHO (World Health Organization) (2000) Consensus meeting on surveillance of infectious
diseases: Report on a WHO meeting, Grottaferrata, Italy 4-7 April 2000. Regional Office
for Europe: World Health Organization.

96
WHO (World Health Organization) (2002) Se préparer pour faire face à l'usage délibéré
d'agents biologiques: Pour une approche rationelle face à l'impensable. Geneva: World
Health Organization.
Young, R.J.C. (2003) Postcolonialism: A Very Short Introduction. Oxford University
Press, Oxford.