Embed Size (px)
Citation preview

4/1/2016
1
Metacognitive Strategy Training for Breast Cancer Survivors with Chemobrain: Translating Research into Clinical Practice
Meghan Doherty, MSOT, OTR/L, OTD/S Timothy Wolf, OTD, OTR/L, MSCI, FAOTA
Describe the outcomes of a metacognitive strategy training pilot intervention on client occupational performance
Explain components of a metacognitive strategy training program for use with women with CRCI.
List outcome measures to assess participation and cognition in breast cancer survivors in the clinic.
Objectives
THE EFFECT OF METACOGNITIVE STRATEGY TRAINING (MCST) ON CHEMOTHERAPY-INDUCED COGNITIVE IMPAIRMENT (CICI)
Timothy J. Wolf, OTD, MSCI, OTR/L, Principal Investigator Jay F. Piccirillo, MD, FACS, CPI, Sub-Investigator, Professor Otolaryngology - Head and
Neck Surgery Bradley Schlaggar MD, PhD, Sub-Investigator, Associate Professor Radiology, Anatomy
& Neurobiology & Pediatrics Joshua S. Shimony MD, PhD, Sub-Investigator, Assistant Professor Radiology Cynthia X. Ma, MD, PhD, Sub-Investigator, Associate Professor-Medicine, Division of
Oncology, Section of Medical Oncology Carolyn Baum, PhD, OTR/L, FAOTA, Sub-Investigator, Elias Michael Executive Director,
Program in Occupational Therapy, Professor of Occupational Therapy, Neurology, and Social Work
Joyce E. Nicklaus, RN, BSN, CCRC, Clinical Research Nurse Coordinator, Otolaryngology
Meghan Doherty, MSOT, OTR/L, Research Coordinator, Occupational Therapy Caroline Bumb, MS, CCRP, Division of Oncology, Medicine Rebecca Coalson, BS, Department of Neurology
MCST‐CICI
2013 - funded by the McDonnell Center for Systems Neuroscience, Washington University Institute of Clinical and Translational Sciences grant UL1 TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH), Mallinckrodt Institute of Radiology at the Washington University School of Medicine
MCST‐CICI
Epidemiology Breast cancer is the most common malignancy
(28%) in females in the United States
The use of chemotherapy has led to dramatic improvements in survival in breast cancer patients and is now considered standard of care
Population & Background
Chemotherapy and Cognitive Deficits Recent findings of decreased productivity, impaired
community involvement, and poor role-functioning resulting from cognitive dysfunctions after chemotherapy
Studies in BRCA survivors have shown deficits in the domains of attention, learning, working memory, motor speed, visuo-spatial skills, executive function(planning, problem solving, multitasking), and information processing after chemo
These are referred to as chemotherapy-induced cognitive impairments (CICI) or “chemobrain”
The rate of CICI in the literature ranges from 16% to 50%
Population & Background

4/1/2016
2
Wide range in published rates of CICI is largely due to methodological issues related to assessment of cognitive function Tools
Timing
Follow-up period
Functional neuroimaging being used in research Resting-state functional MRI (rs-fcMRI)
Our research group found differences in the frontal-parietal cognitive control regions in those who self-report CICI vs. those who do not
Moment-to-moment control of cognitive function
Cognitive flexibility
Background‐CICI Assessment
Left Right
Dorsal
Traditionally rehab for BRCA survivors post-chemotherapy has focused on exercise programs management of edema psychosocial adjustment arm range of motion ADLs
However, cognitive dysfunction is having the greatest negative impact on return to complex everyday life activities such as work/productivity and community living
Background‐Intervention
Past studies addressing CICI in BRCA and other cancers
have focused on specific cognitive impairment reduction
which has had little impact on everyday life performance
Little work has looked at the use of metacognitive strategy training which targets the mechanisms associated with the frontal-parietal network Cognitive-Orientation to daily Occupational Performance
(CO-OP) approach
Background‐Intervention
Specific Aim 1: To assess the effect of metacognitive strategy training on self-reported cognitive performance in a sample of breast cancer survivors with self-reported CICI.
Hypothesis: Metacognitive strategy training will improve self-reported cognitive performance in patients with self-reported CICI.
Study Aims
Specific Aim 2: To assess the effect of metacognitive strategy training brain networks as defined by rs-fcMRIin a sample of breast cancer survivors with self-reported CICI.
Hypothesis: Metacognitive strategy training will improve functional connectivity characterized by rs-fcMRI-in patients with self-reported CICI in the two connections in the frontal-parietal network found to be negatively impacts with CICI.
Study Aims

4/1/2016
3
Single group, pre/post pilot study
Obtained approval from WU Human Research Protection Office and Protocol Review Monitoring Committee
Participants recruited from Siteman cancer center
N=14
Study Design
Inclusion criteria : Females 35-70 years old
Self-reported CICI (Global Rating of Cognition dysfunction as “Moderately” “Strongly “or “Extremely” and a Cognitive Failures Questionnaire score >30)
Completed adjuvant (or neoadjuvant) chemotherapy at least 6 months prior to participation
Able to read, write, and speak English fluently
Able to provide valid informed consent
Have a life expectancy >6 months at time of enrollment
Diagnosed with BRCA (invasive ductal or lobular Stages I, II, or III)
and completed chemotherapy within the preceding 2 years
On stable doses (i.e., no changes in past 90 days) of medication
that impact cognitive function (i.e., anti-depressants).
Inclusion & Exclusion Criteria
Exclusion criteria: Prior CA diagnoses of other sites with evidence of active disease within 1 yr
Active dx of any acute or chronic brain-related neurological conditions that can alter normal brain anatomy or function (e.g., Parkinson’s disease, dementia, cerebral infarcts)
Severe depressive symptoms (Personal Health Questionnaire score of ≥21)
History of traumatic brain injury
Weigh over 350 pounds (limit of MRI machine)
Received skull-based radiation treatment within the past year for any reason
Implanted metal objects not compatible with MRI
History of claustrophobia or inability to lie flat that will preclude undergoing MRI
Any medical condition which would render the study unsafe or not in
the best interest of the participant
Inclusion & Exclusion Criteria
Potential participants completed a screening survey with medical background questions and two cognitive screens: Cognitive Failures Questionnaire (CFQ) & the Global Rating of Cognition (GRC)
Face to Face assessment: consent, baseline assessment battery, and neuroimaging
12 sessions of CO-OP metacognitive strategy training with an occupational therapist
Discharge assessment battery and MRI
Methods
What is CO‐OP?
Treatment Approach Client-centered Performance-based Problem solving
Enables skill acquisition
Strategy use
Guided discovery
Focuses on occupational performance
Haskins, E. (2012). Rehabilitation for Impairments of Executive Functions. In L. Trexler (Primary Ed) Cognitive Rehabilitation Manual (pg. 12). Reston, VA: American Congress of Rehabilitation MedicineReproduced from ACRM Publishing, 2012, by permission

4/1/2016
4
Other Metacognitive Strategy approaches
WSTC – What should I be doing? (Lawson & Rice, 1989)
PST – problem-solving training (von Cramon, Matthes-von Cramon, & Mai, 1991)
GMT – Goal management training (Levine et al., 2000)
STP – Self-talk Procedure (Cicerone & Wood, 1987; Ciccerone and Giacino, 1992).
Why was CO‐OP developed?
Basic premise: engagement in activity is necessary for healthy development
Developed as an alternative to motor interventions that focused on remediation of deficits Bottom-up approach—remediation of deficits should result in
improved performance (limited evidence) Bottom-up interventions = intensive Current motor theory shifted to focus more on task-oriented Needed an intervention that focused on performance
Solution Combine contemporary task-oriented motor theory with learning theory
Bottom‐up approaches
Improved
Improved Cognition
Cognitive Exercises
•Memory
•Problem solving
•memory
•attention
Activity Participation
Top‐Down Approaches
Improved Cognition ?
Metacognitive Strategy TrainingDirect Skill Training
Improved Activity Participation
Uses Health & Disability Model of ICF
Focus not at disability & impairment
Focus on discovering strategies to eliminate barriers & create supports that enable activity & participation
Mandich & Polatajko, 2005
Goals of CO‐OP
Skill acquisition
Cognitive strategy use
Generalization of learning
Transfer of learning
Activity Performance
Global Strategy Training
Client‐chosen goals
Self evaluation
Guided Discovery

4/1/2016
5
Why CO-OP is Valuable
It meets the demands of three key players:
Therapists – it is client-centered and performance based
Administrators – it is cost-effective, efficient, and evidence based
Clients and caregivers – it is effective in helping adults and children succeed
Polatajko and Mandich, 2004
CO-OP Prerequisites
language skills to respond to Canadian Occupational Performance Measure (COPM)
ID 3+ occupational goals
Respond and attend to therapist
Have potential to perform task
Have motivation to learn 3 skills
Awareness Polatajko, 2006
CO-OP Key Features
Mandich & Polatajko, 2005
Client Chosen Goals
Daily logs
Activity Card Sort
Canadian Occupational Performance Measure Guided process
Measureable goals
Can be used as an outcome
measure
VIDEO
CO-OP Key Features
Mandich & Polatajko, 2005
Dynamic Performance Analysis
Observe performance
Identify breakdown, test potential strategies
Correct problem, not underlying skill
TASK ANALYSIS!

4/1/2016
6
CO-OP Key Features
Mandich & Polatajko, 2005
Cognitive Strategies
Global
Domain-specific
Global Strategy: Goal, Plan, Do, Check
GOAL: What do I want to do?
PLAN: How am I going to do it?
DO: Do it!
CHECK: How well did my plan work?
Domain‐Specific Strategies Body position
Attention to task
Task specification/modification
Supplementing task knowledge
Feeling the movement
Verbal mnemonic
Verbal script
Mental imagery
Relaxation techniques
CO-OP Key Features
Mandich & Polatajko, 2005
Guided Discovery
Just Listen! I will tell you what to do!
Try to figure it out on your own, but I will help you if
you get stuck.
Low: Discovery Learning
Mid: Guided Discovery
High: Explicit Instruction
Trial and Error Learning: Figure it out on your own!

4/1/2016
7
Guided Discovery
Posing questions to the client that focus on factors that are relevant and irrelevant to help client identify relevant cues
Similar to scaffolding
Process questions
Guided Discovery
One thing at a timeAsk, don’t tell (verbal)Coach, don’t adjust (physical)Make it obviousVideo
This is how we should be cuing
CO-OP Key Features
Mandich & Polatajko, 2005
Enabling Principles
Make it fun
Promote learning Progress through stages
Small steps
Support, feedback, practice, and review
Motivation
Behavioral strategies (e.g., reinforcement, shaping)
Work toward independence
Promote generalization and transfer
Significant Other Involvement
Primary role
Support in skill acquisition
Help facilitate transfer/generalization
Therapist shares info so that success can be celebrated & new skills supported
Caregiver change their perspective on the client - See lack of success as failure of the PLAN, not personal failure

4/1/2016
8
CO-OP Key Features
Mandich & Polatajko, 2005
Intervention Format
10-12 Sessions Phase I-Preparation
Establishing the goals COPM
Phase II-Acquisition Typically 10 sessions Start: introduce GPDC Work through GPDC for all 3 goals (plan, do, check)
Phase III-Verification Progress reviewed COPM re-rated
Mistakes are OKAY!
Strategy Training > Direct Skill Training Generalization Learning can be inhibited when we prevent patients
from discovering their own solutions
Learning may be best when: Patients overcome their difficulty challenges (with
guidance from therapist)
Patients develop their own reasoning and problem-solving skills
Goal – Plan – Do – Check
Goal is achieved
GOALWhat do I want to
do?
GOALWhat do I want to
do?
GOALWhat do I want to
do?
PLAN
How ?When ?
Where ?
CHECKDid I do my plan?
Did it work?
CHECKDid I do my plan?
Did it work?
CHECKDid I do my plan?
Did it work?
DOThe plan
DOThe plan
DOThe plan
Putting it all Together
Activity Performance
Global Strategy Training
Client‐chosen goals
Self evaluation
Guided Discovery
Behavioral Data Distribution of scores described using median
and range
Change scores calculated
Median difference and 95% CI calculated
Wilcoxon signed rank test
Non-parametric effect size r
Data Analysis

4/1/2016
9
Neuroimaging Data Timecourses calculated for each subject an each scan for
two frontoparietal control regions Fisher z-transformed Pearson correlation coefficients
calculated between two frontal-parietal region’s timecourses(functional connectivity)
Functional connectivity changes across the brain compared using Object Oriented Data Analysis (OODA) Iterative approach using Gibb’s distribution
Pearson correlations to evaluate relationship between changes in connectivity and behavioral outcomes
Analysis Results
Variable Median (Min‐Max) or %
Age (Years) 50.50 (36 to 65)
Time since completion of chemotherapy
(months)
9.5 (7 to 34)
Race n (%)
Caucasian 12 (86%)
African American 1 (7%)
Asian 1 (7%)
Highest level of education
High School or Associate Degree 2 (14%)
Bachelor’s Degree 3 (21%)
Master’s or Doctoral Degree 9 (65%)
Work Status
Full‐time 12 (86%)
Part‐time 1 (7%)
Retired 1 (7%)
Table 2: Study sample characteristics (n = 14)
Results‐Behavioral
Assessment Pre‐Score
Median
(Min‐Max)
Post‐Score
Median (Min‐
Max)
Median of
difference (pre‐
post) (95%CI)
Effect
size (r)bInterpretation
Cognitive Failures
Questionnaire
50 (39‐68) 36 (15‐49) 15 (8.9 to 25.2)a ‐.85 Significant decrease in
subjective cognitive
symptoms
DKEFS Trail Making 12 (1‐13) 12 (7‐14) ‐1 (‐2.1 to 0)a ‐.50 Sig improvement in
objective EF (cog flexibility)
Dysexecutive
Questionnaire
23 (3‐39) 11 (0‐33) 9 (4 to 16)a ‐.75 Sig improvement in
subjective EF
Montreal Cognitive
Assessment
28 (21‐30) 28 (21‐30) 0(‐1.05 to 0.05) ‐.28 Stable general cognitive
function
The Canadian
Occupational
Performance
Measure
4.8 (2.6‐7.3) 7.7 (5.8‐9.7) ‐3 (‐3.3 to ‐1.6)a ‐.88 Sig improvement in self‐rated
performance of activities
2.8 (1.4‐5.5) 8.0 (3.5‐10.0) ‐4.5 (‐5.3 to ‐3.3)a ‐.88 Sig improvement in self‐rated
satisfaction with performance
of activities
PHQ‐9 ‐ Depression 6.5 (1‐13) 4.5 (0‐11.0) 1.5 (0.9 ‐ 4.1) ‐.53 Decrease in depressive
symptoms approaching sig
Table 3: Behavioral Outcomes
10 subjects had enough data for analysis The amount of data kept did not differ between two
scans (p = .59)
Using object oriented data analysis (OODA) A one-tailed, paired t-test on the connection
between the two frontal parietal control regions previously described showed trend level significance (p=.054)
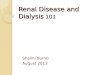
Increase in functional connectivity strength after treatment in 6 of the 10 subjects
Results‐Neuroimaging
The change in Personal Health Questionnaire (PHQ-9) explained 35% of the difference in connection strength (p=0.057)
The change in the Trailmaking subtest of the Delis-Kaplan Executive Function System (DKEFS), a measure of EF explained 26% of the change in connection strength (p=0.108)
Results‐Neuroimaging
-0.2
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5 6 7 8 9 10
z tr
ansf
orm
ed C
orre
latio
n C
oeffi
cien
t
Subject
Before Treatment
After Treatment

4/1/2016
10
-5
0
5
10
15
20
25
30
35
CF
Q S
core
Cha
nge
Individual Participants
No control group
Small sample
Heterogeneity in terms of age, time since chemo, and response to intervention
Study Limitations
CO-OP is a feasible intervention for BRCA survivors
CO-OP has a positive effect on: subjective cognitive performance objective cognitive performance Activity performance Quality of life
CO-OP showed a positive change in functional connectivity in one brain network
Conclusions & Clinical Implications
Translation into clinical program
Future research projects
Next Steps
How can a research-based protocol be adapted for clinical use? Is it feasible?
How will it be assessed?
How can we track outcomes to add strength to the evidence base?
Who will benefit?
Community‐based OT services for Survivors
“Evaluating the individual’s physical, emotional, and cognitive abilities in order to make appropriate recommendations…”
“Identifying specific cognitive deficits affecting occupational roles, and providing compensatory training to successfully complete activities….”
AOTA Guidelines for cancer
Deluliis ED, Hughes JK. Occupational Therapy's Role in Breast Cancer Rehabilitation 2012; http://www.aota.org/‐/media/Corporate/Files/AboutOT/Professionals/WhatIsOT/HW/Facts/Breast‐cancer.pdf, 2015.

4/1/2016
11
Survivors of all types experience challenges with returning to work, work performance, and 1 in 10 never returns to work.
Cognitive dysfunction is well recognized among patients with non-central nervous system cancers14 and cognitive symptoms related to cancer treatment are a major contributor to difficulty with return to work and other productive roles.
Difficulty with prolonged mental concentration; with analyzing data; and with learning new things.
While definitions of cognitive impairment vary from study to study, the literature demonstrates cognitive impairment both during chemotherapy and longitudinally after treatment.
Other cancers with similar problems
The research design of MCST-CICI was purposely set up to be clinically feasible
It included clinical cognitive and participation measures that showed good effect sizes post-study
Cancers of all types can cause treatment-related cognitive impairment
Expansion to term CRCI – Cancer-related Cognitive Impairment
Clinic clients may have non-cognitive therapy concerns as well
Transitioning research into practice
Create a logic model
Develop treatment protocol and assessment battery
Build relationships
Marketing
IRB approval
Creating a clinical program Logic Model
Logic Model –Assumptions
• Cancer survivors are individuals w/ a cancer diagnosis• Many survivors have cognitive deficits resulting from cancer
or cancer treatments that impact daily life participation.• Cancer survivors in the St. Louis metro region have limited
access to community-based outpatient therapy services to address their cognitive concerns.
• Rehabilitation services for survivors will help prevent or treat side-effects of cancer or its treatment and decrease healthcare costs (i.e. time lost from work, caregiving & hospital readmissions).
• Metacognitive Strategy Training (MCST) improves occupational performance and self-management skills in neurological populations.
• Occupational Therapists are uniquely capable of addressing the cognitive, physical, and psychosocial limitations of survivors that limit their independence in daily activities.
• Interdisciplinary community partnerships will improve health-related quality of life (HRQOL) for cancer survivors.
Logic Model – Assumptions

4/1/2016
12
Logic Model
Cancer survivors
WUOT Therapists experienced in MCST
Cancer health care providers
Payers (insurance, out of pocket pay)
Students
Logic Model – Inputs
Logic Model
Administer focus groups and surveys for therapists involved in cancer care
Develop assessment battery including web-based data management to measure program outcomes.
Build relationships with Siteman Cancer Center staff who provide referrals
Instruct therapists in metacognitive strategy training approach and assessment tools
Market program including print and web materials
Deliver program to survivors
Logic Model – Activities
N=61 therapists, 28 PTs and 33 Ots In response to questions regarding OT’s expertise in
helping address symptoms/side effects in adult cancer survivors, OT and PT responses significantly differed in the following areas: fatigue/energy conservation management, gait/postural issues/balance issues, and equipment needs.
PT viewed OT as having less expertise than OT’s viewed themselves as having.
Survey Completed by Jenna Rebhun, OTD/S
The large majority of respondents from both professions (n=60) believe OT has the expertise in helping address cognitive deficits with cancer survivors (96%)
52% of respondents believe all therapists should receive advanced specialty training before working with cancer survivors.
Of 58 respondents, 69% believe oncologists do not understand the difference between OT and PT
Biggest barrier to expanding OT practice: Lack of recognition and understanding of OT role in cancer survivorship (63%)
Survey of Therapists

4/1/2016
13
Logic Model
Increased referrals of cancer survivors to WUOT
Refined assessment battery Measurable change of occupational
performance Comprehensive approach to
individualized rehabilitation
Logic Model ‐ Outputs
Logic Model
Cancer survivors report high satisfaction with program and staff on patient satisfaction surveys
Survivors promote the program’s value to the cancer community
Increased referrals translate into profits for WUOT clinic
Survivors report improved self-management skills and psychosocial health
Logic Model – Outcomes
Logic Model
Improved health related quality of life of cancer survivors
Decreased overall healthcare costs due to greater use of primary care and better return to work outcomes.
Comprehensive, integrated health care delivery system
Logic Model – Impacts

4/1/2016
14
Goal: skill acquisition and skill improvement
12 60-minute sessions: Session 1-2 Preparation
Sessions 3-11 Treatment
Session 12 Review and Re-evaluation
Develop Treatment Protocol Assessment Battery
Measure Description Method & Time Administered
Cognitive Failures Questionnaire (CFQ)
24
CFQ measures lapses in motor function memory, and perception. This questionnaire contains 25 items and scores range from 0 to 100.
Redcap Pre and Post
Montreal Cognitive Assessment (MOCA) 25
The MOCA is a publically‐available cognitive screening tool validated to distinguish normal from those with mild cognitive impairments.
Face to Face Session 1
Personal Health Questionnaire (PHQ‐9)‐Depression 26
The PHQ‐9 is a quick screening tool for depression that has been used in research and clinical settings to screen for depressive symptoms.
Face to Face Session 1 Session 12
The Weekly Calendar Planning Activity (WCPA)
27
The WCPA is used as a screen for difficulties in executive functioning across a variety of populations to understand the underlying nature of performance problems.
Face to Face Session 2 Session 12
The Behavioural Assessment of Dysexecutive Syndrome (BADS)
28
The Behavior Assessment of Dysexecutive Syndrome contains 7 tests to evaluate planning, organization, problem solving, and attention. We will use the Zoo Map Test of planning.
Face to Face Session 1 Session 12
Develop Assessment battery
Measure Description Method & Time Administered
Assessments to be completed as Needed Upper Extremity Screen
Range of Motion, Strength, and somatosensation screening tests
Face to Face
Whisper Test29 Audition screening measure to detect hearing impairment for further referral.
Face to Face
Tinetti Performance Oriented Mobility Assessment (POMA‐1)30
The POMA‐I is a task‐oriented test that measures adult gait and balance with an ordinal scale from 0 (most impairment) to 2 (independence).
Face to Face
With regional cancer center, Siteman WU Physicians
Nurses coordinators and navigators
Resource center staff
WU Physical Therapy
Ethics board staff
Support groups
Build Relationships
Development of materials Print
Web
Patient-centered
Physician-centered
Sharing of materials throughout regional cancer center satellites
Marketing

4/1/2016
15
Required navigation of the Protocol Review and Monitoring Committee (PRMC) AND Human Research Protection Office at WU
Needed to collect patient outcomes for dissemination and program improvement
IRB Approval
Utilizing REDCap online data collection tool as well as EMR and paper assessments
Will streamline assessment battery
Will measure client change on activity participation and subjective and objective cognitive performance
Will measure client satisfaction with the program through client satisfaction surveys
Tracking Outcomes
Our intervention (CO-OP) is a feasible intervention for BRCA survivors in clinical trials and in an outpatient community-based clinic
“If you build it, they will come” = WRONG
Conclusions Questions?
Meghan Doherty
Washington University School of Medicine
Program in Occupational Therapy
Timothy Wolf
Department of Occupational Therapy
University of Missouri
Contact Information