Embed Size (px)
DESCRIPTION
medq
Citation preview
Page 1 of 7
Group 12: Cabuguason, Cabungcal (09228966531), Caldozo, Calingo, Calma, Calubayen
Dr. Samuel Vincent Yrastorza | March 13, 2014
SURGERY 3.5 Advances and Diagnostics in Surgery 2013-2014 2nd
OUTLINE I. Introduction II. Diagnostic and Surgical Advances
A. CT Scan B. Non-Invasive Surgeries C. Surgical Advances D. Robootic Advances
III. Education and Training A. Telementoring B. Telesurgery
IV. Stem Cell Therapy V. Tissue Engineering
References: Dr. Yrastorza’s lecture recording and ppt
I. INTRODUCTION
How do Filipino physicians measure up to physicians in the first world countries?
In symptomatic diseases, history and physical exam alone can give a 80-90% chance of obtaining a correct diagnosis and lead to the subsequent treatment of the patient. Ancillary procedures are supposed to be there only to give additional boosts to your primary diagnosis.
In asymptomatic diseases, screening procedures can help detect diseases, such as cancer, much earlier.
Nowadays, however, especially in the first world countries, screening exams have become the primary means of obtaining diagnoses, and this approach is also now becoming more prevalent in the Philippines.
Becoming more common in the metropolis and urban centers like in Metro Manila.
The art of medicine might get lost in future, but may not be true for the Philippines since many cannot afford healthcare.
Thus, our emphasis in the basic science of history taking and physical exam boosts our clinical eye, and gives us an advantage to healthcare of the first world.
II. DIAGNOSTIC AND SURGICAL ADVANCES Before, only patients presenting with signs and symptoms can
be diagnosed. Now, even asymptomatic patients who are simply undergoing their annual diagnostic screening can be diagnosed.
There has been great leaps and bounds for diagnostic advances in the past years, especially in the field of gastroenterology. Modalities such as CT Scan have been fundamental in the diagnosis and detection of many conditions such as the presence tumors.
A. CT Scan
With the advent of 3D-CT Scan/virtual colonoscopy, we are able to see inside a human person using non-invasive means, thus causing no need for anesthesia and no discomfort during patient screening. Some disadvantages, however, is that these non-invasive
procedures will not allow you to obtain a tissue biopsy.Thus, you would still need to do a colonosopy especially for those indicated for a biopsy, doubling the amount of procedures the patient has to undertake and pay for.
But how many of these patients undergoing screening exams have tumors/polyps/etc and need tissue biopsy? Very few. This is the beauty of using CT Scan, because if not indicated, can provide non-invasive screening for those patients who do not need it.
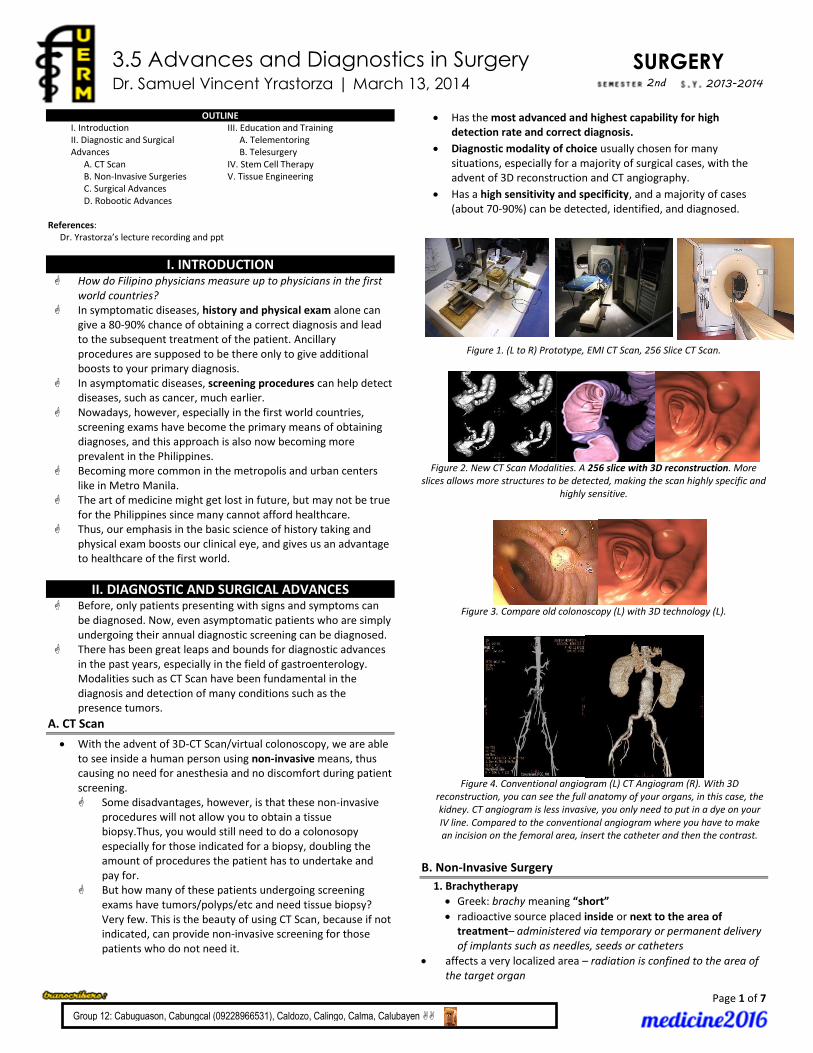
Has the most advanced and highest capability for high detection rate and correct diagnosis.
Diagnostic modality of choice usually chosen for many situations, especially for a majority of surgical cases, with the advent of 3D reconstruction and CT angiography.
Has a high sensitivity and specificity, and a majority of cases (about 70-90%) can be detected, identified, and diagnosed.
Figure 1. (L to R) Prototype, EMI CT Scan, 256 Slice CT Scan.
Figure 2. New CT Scan Modalities. A 256 slice with 3D reconstruction. More
slices allows more structures to be detected, making the scan highly specific and highly sensitive.
Figure 3. Compare old colonoscopy (L) with 3D technology (L).
Figure 4. Conventional angiogram (L) CT Angiogram (R). With 3D
reconstruction, you can see the full anatomy of your organs, in this case, the kidney. CT angiogram is less invasive, you only need to put in a dye on your IV line. Compared to the conventional angiogram where you have to make an incision on the femoral area, insert the catheter and then the contrast.
B. Non-Invasive Surgery
1. Brachytherapy
Greek: brachy meaning “short”
radioactive source placed inside or next to the area of treatment– administered via temporary or permanent delivery of implants such as needles, seeds or catheters
affects a very localized area – radiation is confined to the area of the target organ
Page 2 of 7
SURGERY3.5
less exposure to surrounding normal tissue → less complications
not just for adjunctive therapy or palliation
as first line treatment for various forms of cancer o for cancer of the prostate, cervix, head and neck
Radioactive Sources: o strontium plaque o iridium wires o iodine 125 seeds
Brachytherapy vs External Beam Radiotherapy
Brachytherapy External Beam Radiotherapy Radiation source is in contact
with the tissue being irradiated.
Radiation source is inside the body.
An external source of radiation is pointed at a particular part of the body.
Both are localized forms of radiotherapy
Figure 5. External Beam Radiotherapy
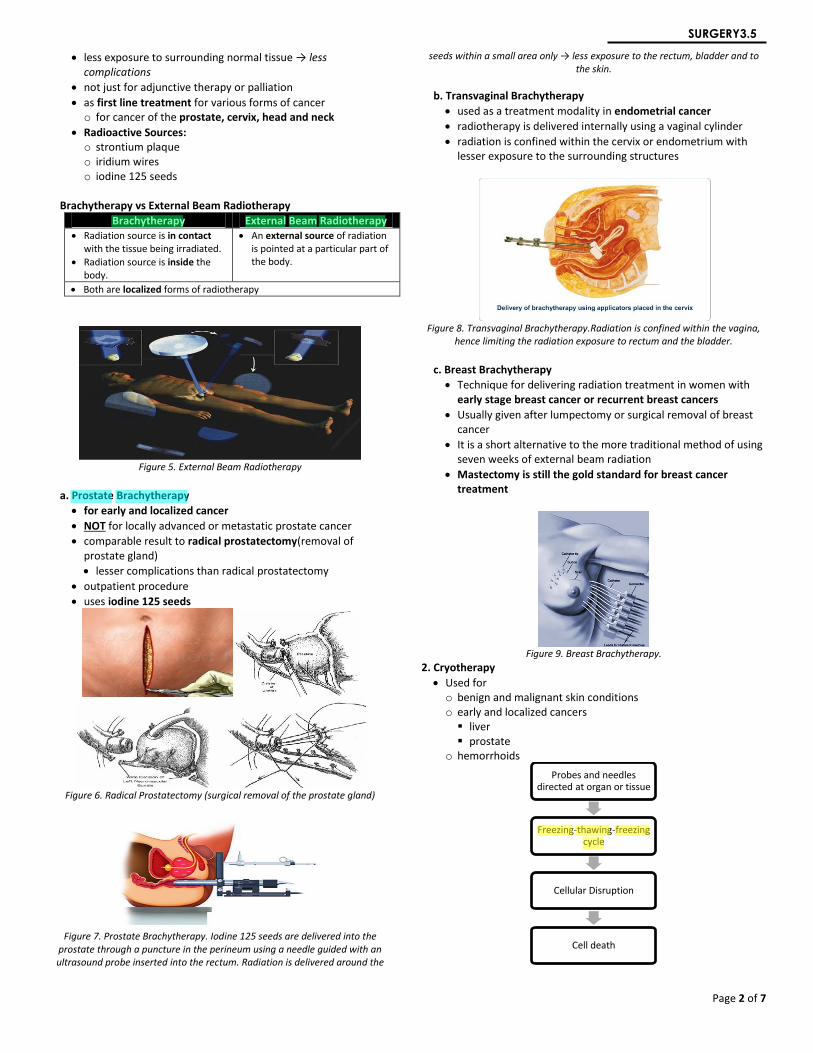
a. Prostate Brachytherapy
for early and localized cancer
NOT for locally advanced or metastatic prostate cancer
comparable result to radical prostatectomy(removal of prostate gland)
lesser complications than radical prostatectomy
outpatient procedure
uses iodine 125 seeds
Figure 6. Radical Prostatectomy (surgical removal of the prostate gland)
Figure 7. Prostate Brachytherapy. Iodine 125 seeds are delivered into the
prostate through a puncture in the perineum using a needle guided with an ultrasound probe inserted into the rectum. Radiation is delivered around the
seeds within a small area only → less exposure to the rectum, bladder and to the skin.
b. Transvaginal Brachytherapy
used as a treatment modality in endometrial cancer
radiotherapy is delivered internally using a vaginal cylinder
radiation is confined within the cervix or endometrium with lesser exposure to the surrounding structures
Figure 8. Transvaginal Brachytherapy.Radiation is confined within the vagina,
hence limiting the radiation exposure to rectum and the bladder.
c. Breast Brachytherapy
Technique for delivering radiation treatment in women with early stage breast cancer or recurrent breast cancers
Usually given after lumpectomy or surgical removal of breast cancer
It is a short alternative to the more traditional method of using seven weeks of external beam radiation
Mastectomy is still the gold standard for breast cancer treatment
Figure 9. Breast Brachytherapy.
2. Cryotherapy
Used for o benign and malignant skin conditions o early and localized cancers liver prostate
o hemorrhoids
Probes and needles directed at organ or tissue
Freezing-thawing-freezing cycle
Cellular Disruption
Cell death
Page 3 of 7
SURGERY3.5
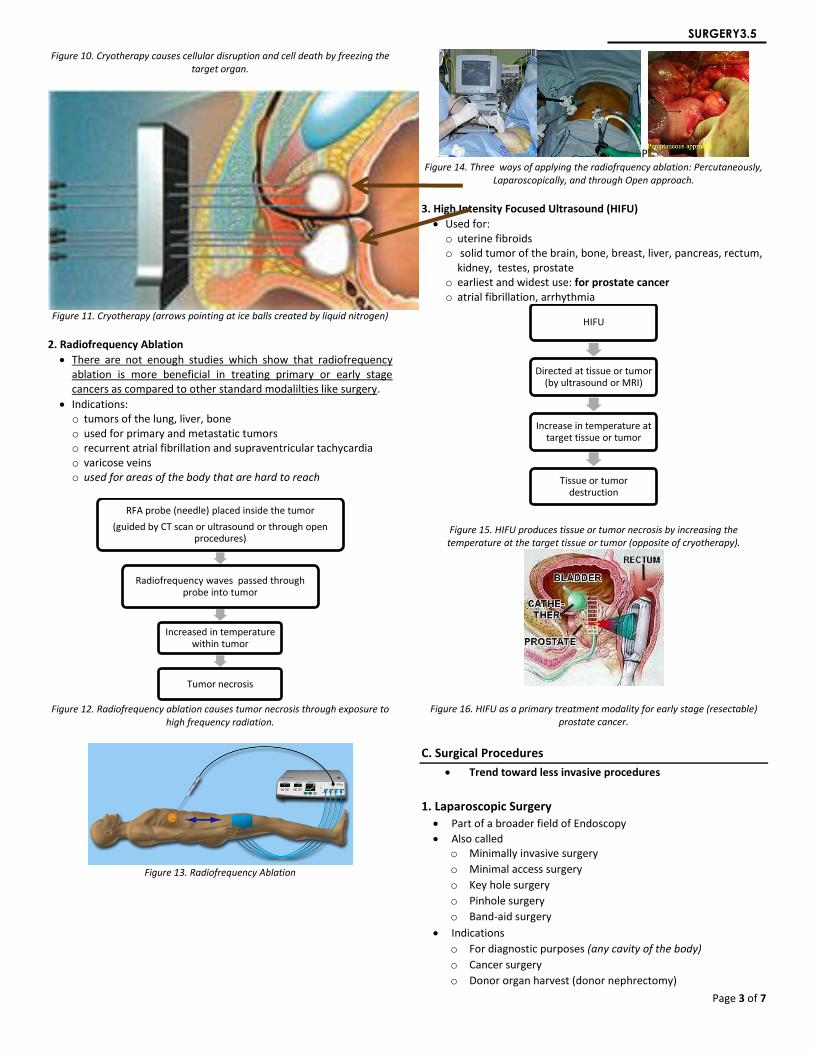
Figure 10. Cryotherapy causes cellular disruption and cell death by freezing the target organ.
Figure 11. Cryotherapy (arrows pointing at ice balls created by liquid nitrogen)
2. Radiofrequency Ablation
There are not enough studies which show that radiofrequency ablation is more beneficial in treating primary or early stage cancers as compared to other standard modalilties like surgery.
Indications: o tumors of the lung, liver, bone o used for primary and metastatic tumors o recurrent atrial fibrillation and supraventricular tachycardia o varicose veins o used for areas of the body that are hard to reach
Figure 12. Radiofrequency ablation causes tumor necrosis through exposure to
high frequency radiation.
Figure 13. Radiofrequency Ablation
P Figure 14. Three ways of applying the radiofrquency ablation: Percutaneously,
Laparoscopically, and through Open approach.
3. High Intensity Focused Ultrasound (HIFU)
Used for: o uterine fibroids o solid tumor of the brain, bone, breast, liver, pancreas, rectum,
kidney, testes, prostate o earliest and widest use: for prostate cancer o atrial fibrillation, arrhythmia
Figure 15. HIFU produces tissue or tumor necrosis by increasing the temperature at the target tissue or tumor (opposite of cryotherapy).
Figure 16. HIFU as a primary treatment modality for early stage (resectable) prostate cancer.
C. Surgical Procedures
Trend toward less invasive procedures
1. Laparoscopic Surgery
Part of a broader field of Endoscopy
Also called o Minimally invasive surgery
o Minimal access surgery
o Key hole surgery
o Pinhole surgery
o Band-aid surgery
Indications
o For diagnostic purposes (any cavity of the body)
o Cancer surgery
o Donor organ harvest (donor nephrectomy)
RFA probe (needle) placed inside the tumor
(guided by CT scan or ultrasound or through open procedures)
Radiofrequency waves passed through probe into tumor
Increased in temperature within tumor
Tumor necrosis
HIFU
Directed at tissue or tumor (by ultrasound or MRI)
Increase in temperature at target tissue or tumor
Tissue or tumor destruction
Page 4 of 7
SURGERY3.5
o Vascular surgeries
o Any abdominal surgery
Advantages
o Better visualization of abdominal structures: because of the camera system (most important)
o Smaller incisions smaller scars (aesthetic reason)
o Fast recovery short hospital stay
Disadvantages
o More expensive
o Requires expertise
o Steep learning curve
“see one, do one” does not apply here, they say that you have to do at least 100 procedures to be really adept in laparoscopy
o Longer operating time (gap is slowly closing with that of open surgery)
Instruments
o Trocars
o Lens or telescope/camera
o Hand instruments
2. Retroperitoneoscopy
Figure 17. Retroperitoneoscopy
Endoscopy in the retropertoneum (any area of the body where there’s space, you can do endoscopy!)
Dilate area with a balloon and then expand it with carbon dioxide, so that you don’t have to pass through the abdominal cavity to take out masses
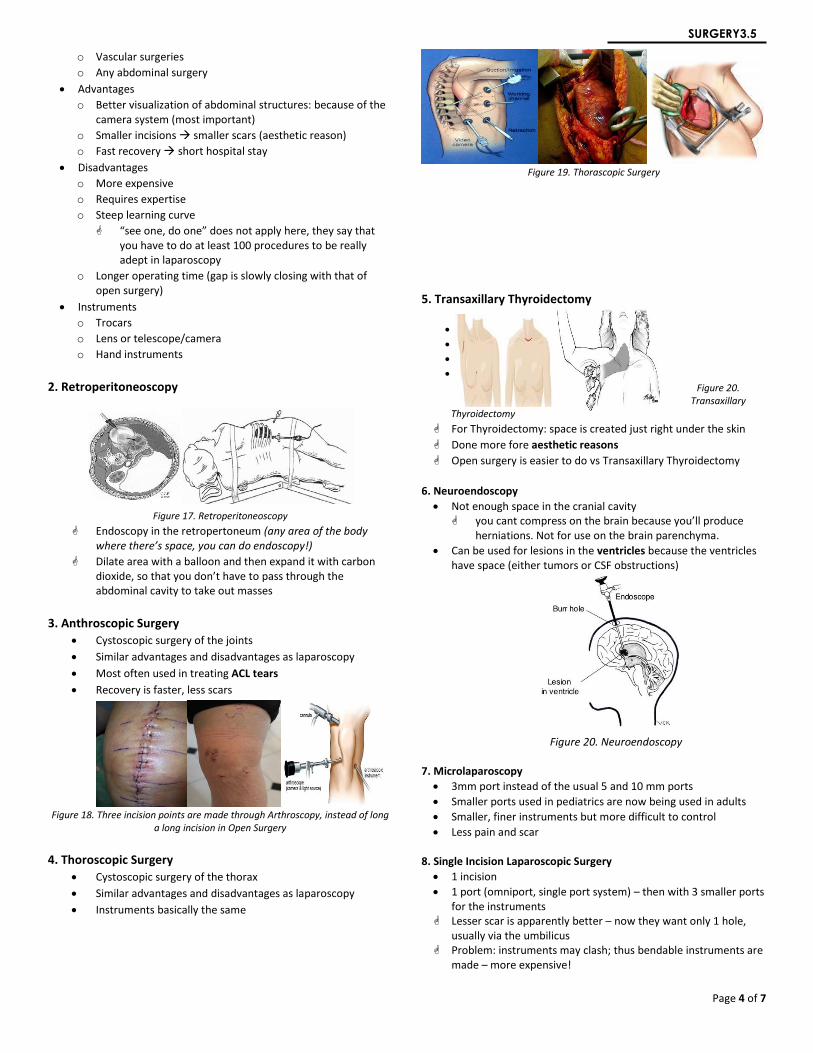
3. Anthroscopic Surgery
Cystoscopic surgery of the joints
Similar advantages and disadvantages as laparoscopy
Most often used in treating ACL tears
Recovery is faster, less scars
Figure 18. Three incision points are made through Arthroscopy, instead of long
a long incision in Open Surgery
4. Thoroscopic Surgery
Cystoscopic surgery of the thorax
Similar advantages and disadvantages as laparoscopy
Instruments basically the same
Figure 19. Thorascopic Surgery
5. Transaxillary Thyroidectomy
Figure 20. Transaxillary
Thyroidectomy
For Thyroidectomy: space is created just right under the skin
Done more fore aesthetic reasons
Open surgery is easier to do vs Transaxillary Thyroidectomy
6. Neuroendoscopy
Not enough space in the cranial cavity you cant compress on the brain because you’ll produce
herniations. Not for use on the brain parenchyma.
Can be used for lesions in the ventricles because the ventricles have space (either tumors or CSF obstructions)
Figure 20. Neuroendoscopy
7. Microlaparoscopy
3mm port instead of the usual 5 and 10 mm ports
Smaller ports used in pediatrics are now being used in adults
Smaller, finer instruments but more difficult to control
Less pain and scar 8. Single Incision Laparoscopic Surgery
1 incision
1 port (omniport, single port system) – then with 3 smaller ports for the instruments
Lesser scar is apparently better – now they want only 1 hole, usually via the umbilicus
Problem: instruments may clash; thus bendable instruments are made – more expensive!
Page 5 of 7
SURGERY3.5
Figure 21. Single incision laparoscopic surgery
9. Natural Orifice Surgery
Natural Orifice Transluminal Endoscopic Surgery (NOTES)
No incision
Use natural openings in the body (mouth, anus, vagina)
Cholecystectomy via mouth/vagina
Nephrectomy via vagina
Rectal surgery via anus
Figure 22. No Incision Surgery
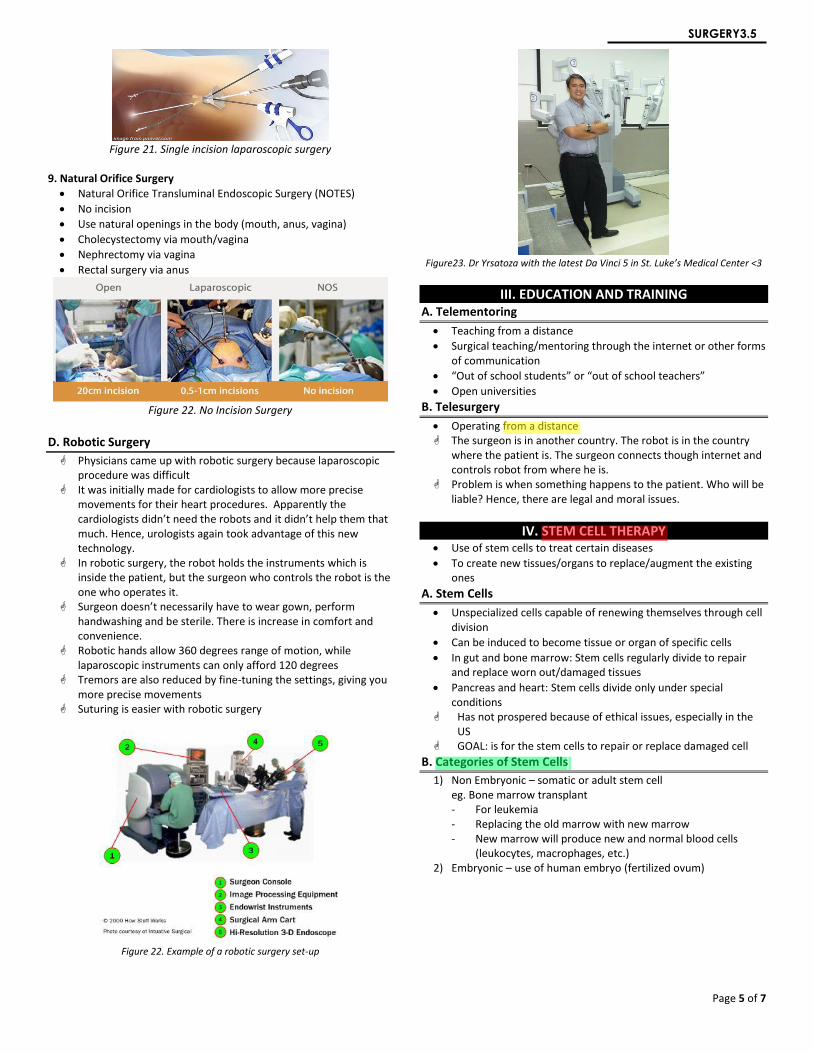
D. Robotic Surgery
Physicians came up with robotic surgery because laparoscopic procedure was difficult
It was initially made for cardiologists to allow more precise movements for their heart procedures. Apparently the cardiologists didn’t need the robots and it didn’t help them that much. Hence, urologists again took advantage of this new technology.
In robotic surgery, the robot holds the instruments which is inside the patient, but the surgeon who controls the robot is the one who operates it.
Surgeon doesn’t necessarily have to wear gown, perform handwashing and be sterile. There is increase in comfort and convenience.
Robotic hands allow 360 degrees range of motion, while laparoscopic instruments can only afford 120 degrees
Tremors are also reduced by fine-tuning the settings, giving you more precise movements
Suturing is easier with robotic surgery
Figure 22. Example of a robotic surgery set-up
Figure23. Dr Yrsatoza with the latest Da Vinci 5 in St. Luke’s Medical Center <3
III. EDUCATION AND TRAINING A. Telementoring
Teaching from a distance
Surgical teaching/mentoring through the internet or other forms of communication
“Out of school students” or “out of school teachers”
Open universities
B. Telesurgery
Operating from a distance The surgeon is in another country. The robot is in the country
where the patient is. The surgeon connects though internet and controls robot from where he is.
Problem is when something happens to the patient. Who will be liable? Hence, there are legal and moral issues.
IV. STEM CELL THERAPY Use of stem cells to treat certain diseases
To create new tissues/organs to replace/augment the existing ones
A. Stem Cells
Unspecialized cells capable of renewing themselves through cell division
Can be induced to become tissue or organ of specific cells
In gut and bone marrow: Stem cells regularly divide to repair and replace worn out/damaged tissues
Pancreas and heart: Stem cells divide only under special conditions
Has not prospered because of ethical issues, especially in the US
GOAL: is for the stem cells to repair or replace damaged cell
B. Categories of Stem Cells
1) Non Embryonic – somatic or adult stem cell eg. Bone marrow transplant - For leukemia - Replacing the old marrow with new marrow - New marrow will produce new and normal blood cells
(leukocytes, macrophages, etc.) 2) Embryonic – use of human embryo (fertilized ovum)
Page 6 of 7
SURGERY3.5
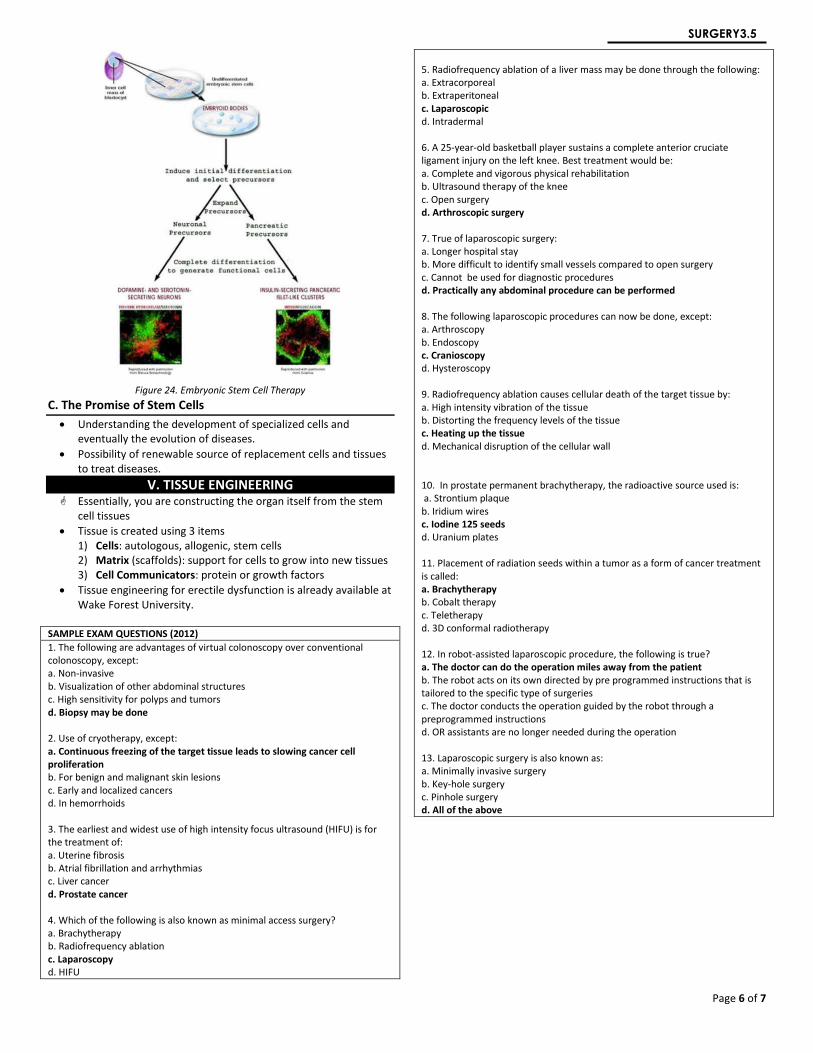
Figure 24. Embryonic Stem Cell Therapy
C. The Promise of Stem Cells
Understanding the development of specialized cells and eventually the evolution of diseases.
Possibility of renewable source of replacement cells and tissues to treat diseases.
V. TISSUE ENGINEERING Essentially, you are constructing the organ itself from the stem
cell tissues
Tissue is created using 3 items 1) Cells: autologous, allogenic, stem cells 2) Matrix (scaffolds): support for cells to grow into new tissues 3) Cell Communicators: protein or growth factors
Tissue engineering for erectile dysfunction is already available at Wake Forest University.
SAMPLE EXAM QUESTIONS (2012)
1. The following are advantages of virtual colonoscopy over conventional colonoscopy, except: a. Non-invasive b. Visualization of other abdominal structures c. High sensitivity for polyps and tumors d. Biopsy may be done 2. Use of cryotherapy, except: a. Continuous freezing of the target tissue leads to slowing cancer cell proliferation b. For benign and malignant skin lesions c. Early and localized cancers d. In hemorrhoids 3. The earliest and widest use of high intensity focus ultrasound (HIFU) is for the treatment of: a. Uterine fibrosis b. Atrial fibrillation and arrhythmias c. Liver cancer d. Prostate cancer 4. Which of the following is also known as minimal access surgery? a. Brachytherapy b. Radiofrequency ablation c. Laparoscopy d. HIFU
5. Radiofrequency ablation of a liver mass may be done through the following: a. Extracorporeal b. Extraperitoneal c. Laparoscopic d. Intradermal 6. A 25-year-old basketball player sustains a complete anterior cruciate ligament injury on the left knee. Best treatment would be: a. Complete and vigorous physical rehabilitation b. Ultrasound therapy of the knee c. Open surgery d. Arthroscopic surgery 7. True of laparoscopic surgery: a. Longer hospital stay b. More difficult to identify small vessels compared to open surgery c. Cannot be used for diagnostic procedures d. Practically any abdominal procedure can be performed 8. The following laparoscopic procedures can now be done, except: a. Arthroscopy b. Endoscopy c. Cranioscopy d. Hysteroscopy 9. Radiofrequency ablation causes cellular death of the target tissue by: a. High intensity vibration of the tissue b. Distorting the frequency levels of the tissue c. Heating up the tissue d. Mechanical disruption of the cellular wall 10. In prostate permanent brachytherapy, the radioactive source used is: a. Strontium plaque b. Iridium wires c. Iodine 125 seeds d. Uranium plates 11. Placement of radiation seeds within a tumor as a form of cancer treatment is called: a. Brachytherapy b. Cobalt therapy c. Teletherapy d. 3D conformal radiotherapy 12. In robot-assisted laparoscopic procedure, the following is true? a. The doctor can do the operation miles away from the patient b. The robot acts on its own directed by pre programmed instructions that is tailored to the specific type of surgeries c. The doctor conducts the operation guided by the robot through a preprogrammed instructions d. OR assistants are no longer needed during the operation 13. Laparoscopic surgery is also known as: a. Minimally invasive surgery b. Key-hole surgery c. Pinhole surgery d. All of the above

Page 7 of 7
SURGERY3.5









![MD Journal - Material Designmaterialdesign.it/media/formato2/allegati_6014.pdf · 2017. 2. 2. · MD ournal 2 2016 7 MD ournal 2] 2016 EDITORIALE MD Journal, con il suo secondo numero,](https://img.pdfslide.net/doc/110x75/6125fb5e30630d7bf91c20cf/md-journal-material-2017-2-2-md-ournal-2-2016-7-md-ournal-2-2016-editoriale.jpg)



















