Embed Size (px)
Citation preview
MDG related to Maternal and Child Health Status in Lebanon: an update
Presented by Dr Alissar Rady
NPO,WHO BeirutNCPNN meeting, 21/11/ 2008

2000
MillenniumSummit
MillenniumDeclaration
UNGARoad Map
8 Goals
Poverty
Education
Genderequality
Child mortality
Maternalmortality
HIV/AIDS,malaria &
other diseases
Environment
Globalpartnership
Where do Millennium Development Goals come from?

How do the MDGs link with the global health agenda?
18 Health Related Indicators
48 Indicators9 Health-Related
Targets
16 Targets
3 Health Goals
8 Goals
WHO reports on 17 out of 18 MDG health indicators
Broad
Specific

MDG related to Maternal and Child Health
1.Eradicate extreme poverty and hunger2.Achieve Universal primary education3. Promote gender equality and empower women4. Reduce Child Mortality5. Improve maternal health6.Combat HIV/AIDS, Malaria and other diseases7.Ensure Environment sustainability8.Develop global partnership for health

MDGS health and health related indicators:
• 8 out of 18 Indicators are for mother and Child health, related to mortality, nutrition, pregnancy and reproductive health including STDs
• 12 out of 18 indicators are directly related to health interventions
• 5 out of 18 indicators relate to control of communicable diseases( Malaria, TB, HIV and Measles)

SIS
Vital registrationHealth purchasing
agencies
Stewardship agencies Research and studies
Households
Health facilities
Patients registriesand surveillance
Types of sources

These estimates :• Are indicative of orders of magnitude • Are not intended to serve as precise estimates. • Help to stimulate greater awareness of and attention to
the challenge of measuring maternal and child mortality. • Help to assess the completeness and adequacy of the
vital registration and health information systems. • Can be used to highlight the potential pitfalls associated
with indirect measurement techniques such as sisterhood studies.

Tracking progress and measuring achievements• WHO at global level:
– further development of measurement instruments and estimation methods for the 17 health indicators
– improve access to country health information• WHO at country level:
– build capacities to generate information and use it for assessing national policies towards achieving the MDGs
GOAL 4 – Reduce Child Mortality
• Global Target 5: Reduce by two-thirds, between 1990 and 2015, the under-five child mortality rate
• Lebanon Transitory Targets: as per 2003 MDGR:
-Reduce infant mortality rate to 22 per thousand by 2006
-Reduce under-five child mortality rate to 27 per thousand by 2006
-Maintain 90 percent of children immunized against MMR
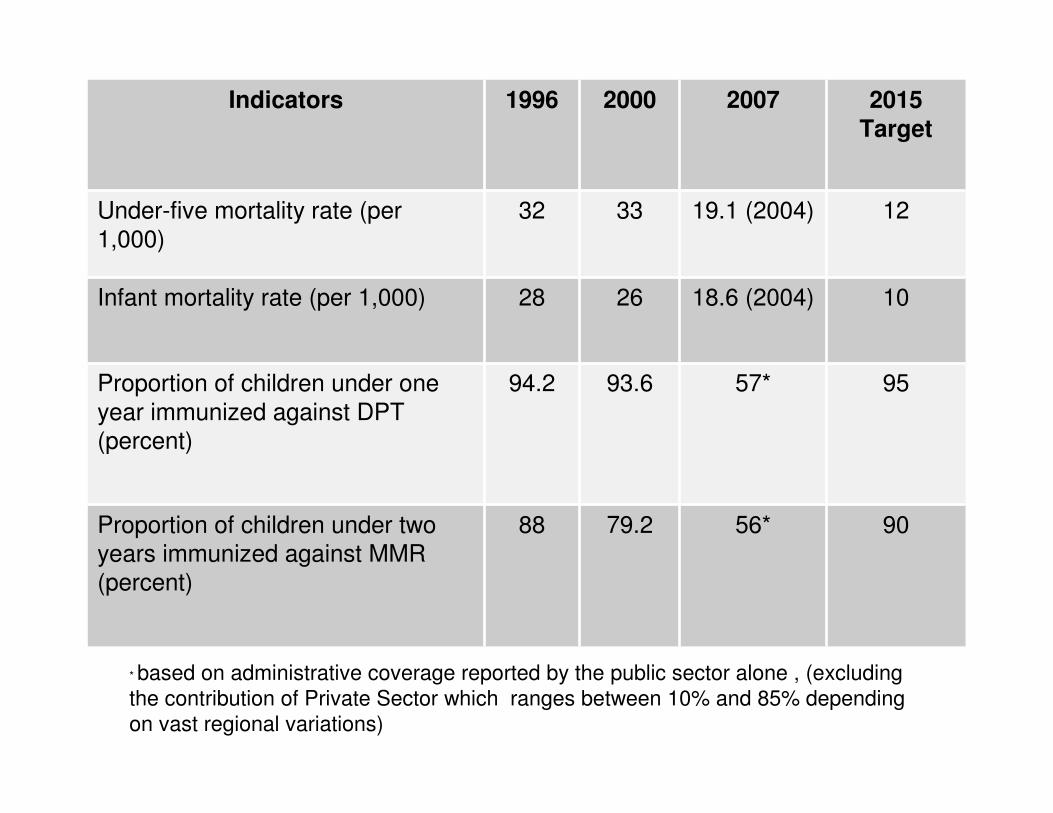
Indicators 1996 2000 2007 2015 Target
Under-five mortality rate (per 1,000)
32 33 19.1 (2004) 12
Infant mortality rate (per 1,000) 28 26 18.6 (2004) 10
Proportion of children under one year immunized against DPT (percent)
94.2 93.6 57* 95
Proportion of children under two years immunized against MMR (percent)
88 79.2 56* 90
* based on administrative coverage reported by the public sector alone , (excluding the contribution of Private Sector which ranges between 10% and 85% depending on vast regional variations)

Goal 5: Improve Maternal Health
• Global Target 6: Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio and achieve by 2015 universal access to reproductive health

Indicators 1990 1996 2000 2004Maternal Mortality Ratio (per 100,000 live births)
140(in 1993)
107 --- 86.3
Proportion of births attended by skilled health personnel (%)
N/A N/A 96 98
Contraceptive Prevalence Rate Modern & Traditional (%)
53(1987-1994)
61 63 74.2
Adolescent Birth Rate
Antenatal Care coverage (at least one visit) (%)
87.1 87 93.9 95.6
Unmet need for Family Planning
Challenges (1)
– Ministry of Public Health (MoPH) institutional weaknesses and the government’s difficulty in enforcing all existent regulations.
– Regional disparities in quality and accessibility to health services, especially in under-served areas of the country.
– thriving high cost poorly regulated private sector
Challenges (2)
– demographic and epidemiological transition .– primary prevention and health promotion are
relatively weak, as compared to highly specialized and costly care services.
– Different studies and different sources, in the absence of a clear denominator, often generate different indicators and results

Challenges (3)
• Poorly adapted health services to Youth/adolescent needs, particularly in relation to RH
• Absence of comprehensive referral system between the primary and secondary health care systems
• Inadequate attention to gender related issues as determinants of health

Strengths(1)
– Political commitment to fulfil the goals of the World Summit for Children, and the International Conference on Population and Development (ICPD) plan of action
– The MOPH reform scheme, including reinforcing the PHC, and its possible financing modalities.
– The continued resource allocation from national budget towards implementing RH and EPI and MCH programmes

Strengths(2)
– The multiplicity of partners in health services. – The active role of NGOs in raising awareness
about child mortality– The contribution of the media in raising public
opinion and disseminating information to the public.
- High level of education among women and men- The establishment of a Inter Ministerial
Committee for Social Issues

Recommendations(1)• Fully integrate the immunization and maternal and child
health interventions in the primary health care system, • Improve outreach interventions aiming at increasing
access for children to immunization ((RED) approach)• Strengthen private-public partnership in health system. • Develop and implement policy and strategy on neonatal
care and child survival, treatment protocols and standard operating procedures in maternities, neonatal and paediatric wards.
• Training/rehabilitation of all concerned personnel.
Recommendations(2)• Improve child nutrition through promotion of breast-
feeding, proper use of supplementary foods, and protection against iron and iodine deficiency.
• Ensure that all pregnant and breast-feeding mothers do not suffer from anaemia and are provided with adequate nutrition and vitamins to prevent malnutrition and iron and folic acid deficiency.
• Improve the health care seeking behaviour at the community level through the implementation of behavioural change communication strategy on maternal and child health.
Recommendations(3)
• Improving national capacity to regularly gather, analyze, update, and utilize high quality data on child health.
• Establish a maternal and child/neonatal death audit.
• Provide programs with early interventions with children with disability

Recommendations (4)
• Enhance comprehensive emergency obstetric care provided by the public sector and NGOs, particularly in under-served regions.
• Increase awareness and outreach programs to men and women on reproductive health rights and choices.

Selected Child Health Indicators
Country New born > 2.5kg Acceptable wt for age
Region average 80% 78%Yemen 79% 54%Iraq 94% 90%Lebanon 93% 98%Jordan 90% 96%Morocco 97% 90%Saudi Arabia 95% 93%Syria 93% 94%UAE 95% 86%

EMR Antenatal Coverage (%)
Bahrein 97Iraq 78Jordan NAKuweit 95Lebanon 87Oman 96Morocco 85 ( local health services)
Saudi Arabia 90Syria 51United Arab Emirates 97Yemen 34


Thank you




![Untitled-1 [planipolis.iiep.unesco.org]...MDG Report, years 2006-2010) UNDAF Ill Alignment to Nigeria Vision 20:2020 UN DAF Ill Results Frame".vork Overview Indicative Financial Resources](https://img.pdfslide.net/doc/110x75/5f42f381f45c564961781d80/untitled-1-mdg-report-years-2006-2010-undaf-ill-alignment-to-nigeria-vision.jpg)