Embed Size (px)
Citation preview
MDS 3.0 Training: Day 2 5/31/2017
1
MDS 3.0 Training: Day 2
Case Mix TeamOffice of MaineCare Services
Updated June 2017
*Welcome and overviewReview and Questions from Day 1Case Mix ImplicationsChapter 3 – Multi-Disciplinary AreasRestorative NursingSections A, S, B, C, D, ESections F, K, Q, Z, V, XRAI Manual Chapters 4, 5, and 6Questions and Wrap-up
2
3
*
*Any questions, comments, need foradditional discussion related to anytopics discuss on Day 1?
MDS 3.0 Training: Day 2 5/31/2017
2
Case Mix Implicationsfor MDS 3.0
4
Case Mix Payment Items
Certain items coded asRUG III services,conditions, diagnosesand treatments on theMDS 3.0 assessmenthandout .
RUG IV refers topayment items for PPSservices.
5
*
Maine uses a modified RUG III Codefor Case Mix purposes.
PPS / Medicare uses RUG IV codes
Supporting Documentation forCase Mix payment items is
required
6
MDS 3.0 Training: Day 2 5/31/2017
3
*
*Resident interviews will be accepted as coded onthe MDS 3.0—NO additional supportingdocumentation is required.*Staff interviews must be documented in theresident’s record. If interviews are summarizedin a narrative note, the interviewer mustdocument the date of the interview, name ofstaff interviewed, and staff responses to scriptedquestions asked.*Follow all “Steps for Assessment” in the RAIManual, for the interview items.
7
Poor Documentation could mean…
Lower payment than the facility could bereceiving, OR
Overpayment which could lead to re-payment to the State (Sanctions). This isdue to either overstating the care aresident received or insufficientdocumentation to support the care thatwas coded.
8
9
Visit the portal at:www.Maine.gov/dhhs/dlrs/mds/training/index.shtml
MDS 3.0 Training: Day 2 5/31/2017
4
*Long Term Care Facility
Resident Assessment Instrument (RAI)
User’s Manual
Chapter 2Effective Oct 2016
10
*
*Initial and periodic assessments for alltheir residents residing in the facility for14 or more days.
*This includes hospice, respite, andspecial populations such as Pediatric andPsychiatric.
11
*
Federal regulatory requirements at42CFR483.20(d) requires NF to maintainall resident assessments completedwithin the previous 15 months in theresident’s active clinical record
12
MDS 3.0 Training: Day 2 5/31/2017
5
*
Nursing Homes may:
1. Use electronic signatures for the MDS
2. Maintain the MDS electronically
3. Maintain the MDS and Care Plans in a separatebinder in a location that is easily and readilyaccessible to staff, Surveyors, CMS etc.
13
*
OBRA = Omnibus Budget Reconciliation Act
PPS = Prospective Payment System
OMRA = Other Medicare RequiredAssessments (SOT, EOT, COT)
ARD = Assessment Reference Date
14
*Long Term Care Facility
Resident Assessment Instrument (RAI)
User’s Manual
Chapter 3Effective Oct 2016
15
MDS 3.0 Training: Day 2 5/31/2017
6
Nursing interventions that promotethe resident’s ability to adapt andadjust to living as independentlyand safely as possible.
Section ORestorative Nursing Programs
• Measureable objectives and interventions• Periodic evaluation by a licensed nurse• CNAs must be trained in the techniques• Does not require a physician’s order, but a
licensed nurse must supervise the activities
16
*Nursing staff are responsible forcoordination and supervision*Does not include groups with morethan 4 residents*Code number of days a residentreceived 15 minutes or more in eachcategory*Remember that persons with dementialearn skills best through repetition thatoccurs multiple times per day.
Section ORestorative Nursing Programs
17
* The following criteria must be met inorder to code O0500-Restorative Nursing
*Measureable Objectives and Interventions
*Must be documented in care plan and medical record
*It is appropriate to reassess progress, goals, frequency andduration as part of care planning process.
*Periodic evaluation by a licensed nurse must be documentedin the medical record
*Aides/assistants must be trained
*RN/LPN must supervise activities
18
MDS 3.0 Training: Day 2 5/31/2017
7
**he or she may be admitted to the facilitywith restorative needs, and is not acandidate for formalized rehabilitationtherapy
*when restorative needs arise during thecourse of a longer-term stay
* may be provided in conjunction withformalized rehabilitation therapy
*Generally initiated when the resident isdischarged from formalized. . .therapy
19
20
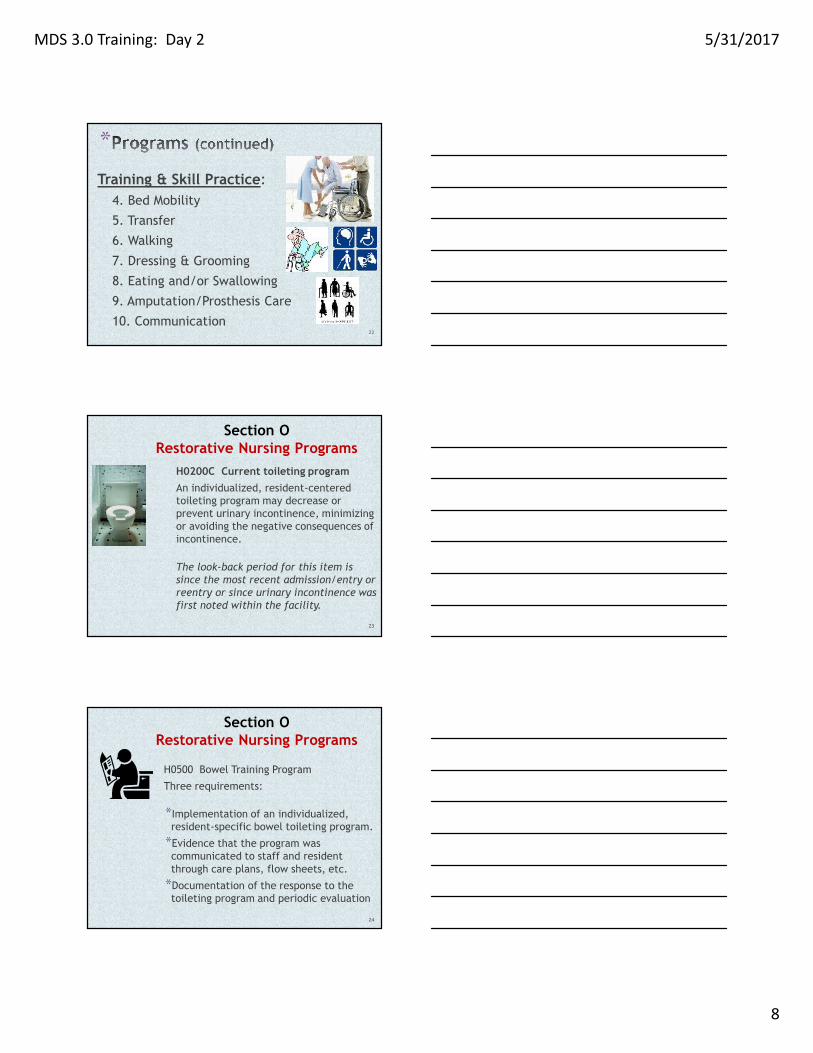
*Technique:Activities provided by restorative nursingstaff:
1. Passive range-of-motion
2. Active range-of-motion(staffdemonstrating / cueing /encouraging the resident)
3. Splint or Brace Assistance
-guidance/direction thatteaches the resident, or
-a program of applying &removing the splint or brace 21
MDS 3.0 Training: Day 2 5/31/2017
8
*Training & Skill Practice:
4. Bed Mobility
5. Transfer
6. Walking
7. Dressing & Grooming
8. Eating and/or Swallowing
9. Amputation/Prosthesis Care
10. Communication22
H0200C Current toileting programAn individualized, resident-centeredtoileting program may decrease orprevent urinary incontinence, minimizingor avoiding the negative consequences ofincontinence.
The look-back period for this item issince the most recent admission/entry orreentry or since urinary incontinence wasfirst noted within the facility.
Section ORestorative Nursing Programs
23
H0500 Bowel Training Program
Three requirements:
*Implementation of an individualized,resident-specific bowel toileting program.
*Evidence that the program wascommunicated to staff and residentthrough care plans, flow sheets, etc.
*Documentation of the response to thetoileting program and periodic evaluation
Section ORestorative Nursing Programs
24
MDS 3.0 Training: Day 2 5/31/2017
9
*RequirementsMeasureable objectives and interventions:
--Measureable: Be as precise as possible. Focus in on exactly what itis that the resident is no longer able to do, what he/she is still ableto do and how staff can work with the resident to improve that skill;thus working towards a goal.
--Functional:
Functional decline can lead to depression, withdrawal, socialisolation, and complications of immobility, such as incontinence andpressure ulcers.” Safety and prevention of complications arenecessary goals, but there must be at least one functional goal on“The Care Plan.”
(adjective) 1. of or having a special activity,purpose, or task; relating to the way in which somethingworks or operates.
25
* Examples of Measureable, Functional Goals
1. Resident will maintain ability toraise hands over head for donning& removing upper body clothing,BID.
2. Resident will improve ambulationfrom 100 feet, 3 times per day to200 feet, 3 times per day.
3. Resident will maintain ability totake food by mouth at all meal &snack times.
4. Resident will maintain ability tofeed self finger foods at all meal& snack times.
26
27
MDS 3.0 Training: Day 2 5/31/2017
10
28
29
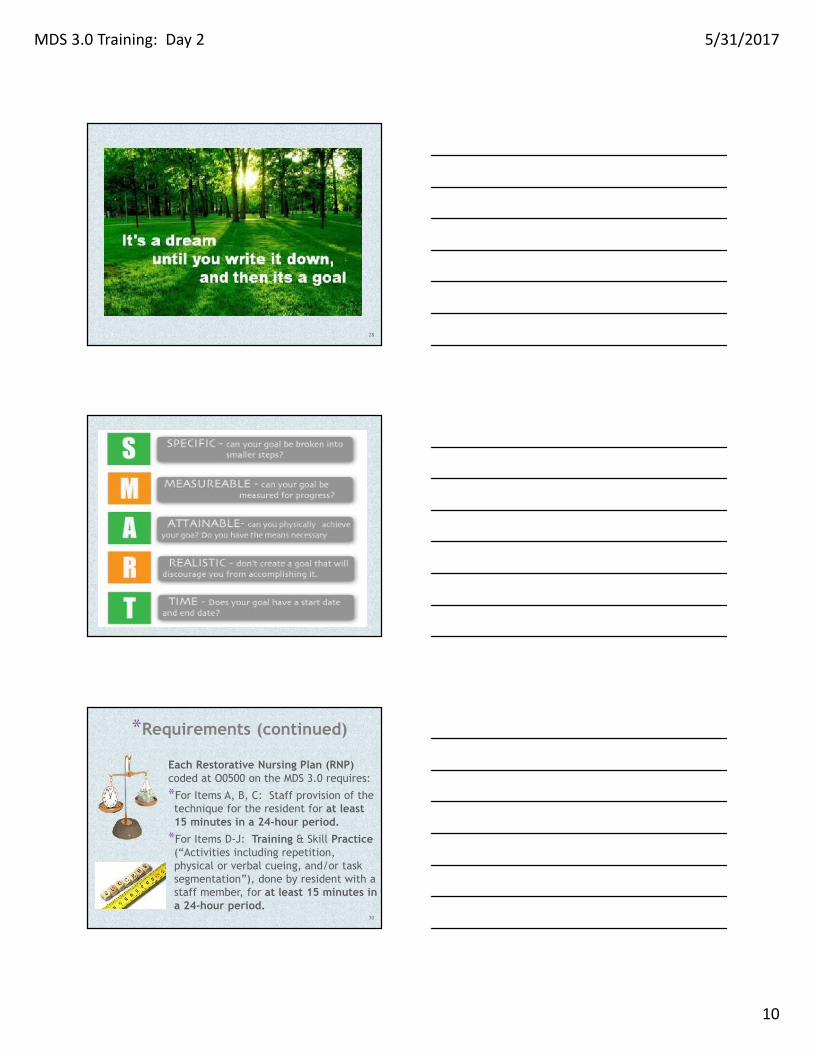
*Requirements (continued)
Each Restorative Nursing Plan (RNP)coded at O0500 on the MDS 3.0 requires:
*For Items A, B, C: Staff provision of thetechnique for the resident for at least15 minutes in a 24-hour period.*For Items D-J: Training & Skill Practice(“Activities including repetition,physical or verbal cueing, and/or tasksegmentation”), done by resident with astaff member, for at least 15 minutes ina 24-hour period.
30
MDS 3.0 Training: Day 2 5/31/2017
11
*Requirements (continued)Periodic Evaluation*“Evidence of periodic evaluation bya licensed nurse must be present inthe resident’s medical record. . .”*“. . .it is appropriate to reassessprogress, goals, and duration /frequency as part of the careplanning process.”*“Good clinical practice wouldindicate that the results of thisreassessment should be documentedin the resident’s medical record.”
31
Supporting documentation forAdmission Assessments
*The Care Plan provides guidance to staff as to thespecific needs and how to care for the Resident.
*If a Restorative Nursing Program (RNP) may be neededfor the resident, add those needs to the interim CarePlan with a measurable, functional Goal and measurableInterventions.
*Add the RNP to the documentation flow sheet, so staffare aware and documentation is completed.
*Evaluate the RNP’s at the time of the initialinterdisciplinary team (IDT) meeting. If not enoughinformation is available for accurate evaluation,document that the RNP’s will be continued for futureevaluation when more information is available.
32
Care Plan is not intended to be a “staticinstrument.” It will always be changing inresponse to the resident’s condition and needs(both long-term AND short term problems orimprovements).
33
MDS 3.0 Training: Day 2 5/31/2017
12
Case Mix cannot dictate what type of documentationtool a facility must use. However, documentation isrequired to support the coding on the MDS.
34
*Nursing must be “responsible for overallcoordination and supervision. . .”
*Programs must be on the Care Plan with ameasurable, functional goal & measurableinterventions (Approaches).
*For “AROM” & “training & skill practice,” residentmust be involved in the activity.
*There must be documentation that the programwas completed for at least 15 total minutes perday, for the number of days coded on the MDS.
*There must be a documented, periodic evaluationof decline, improvement or maintenance, by alicensed nurse.
35
*Intent: The intent of this section is to obtainkey information to uniquely identify eachresident, the home in which he or she resides,and the reasons for assessment.
36
MDS 3.0 Training: Day 2 5/31/2017
13
*
*Code 1 for a new record that has not beenpreviously submitted and accepted in the QIESASAP system
*Code 2 to modify the MDS items for a recordthat has been submitted and accepted in theQIES ASAP system
*Code 3 to inactivate a record that already hasbeen submitted and accepted in the QIES ASAPsystem
37
*
Documents the reason for completing theassessment
Identifies the required assessment contentinformation (determines item set)
There are several subsections to A0310
38
38
*
01. Admission
02. Quarterly
03. Annual
04. Significant change in status
05. Significant correction to priorcomprehensive
06. Significant correction to prior quarterly
99. Not OBRA required39
MDS 3.0 Training: Day 2 5/31/2017
14
*
40
** Electing or revoking the hospice benefit
requires a significant change in statusassessment
41
*
42
MDS 3.0 Training: Day 2 5/31/2017
15
*
43
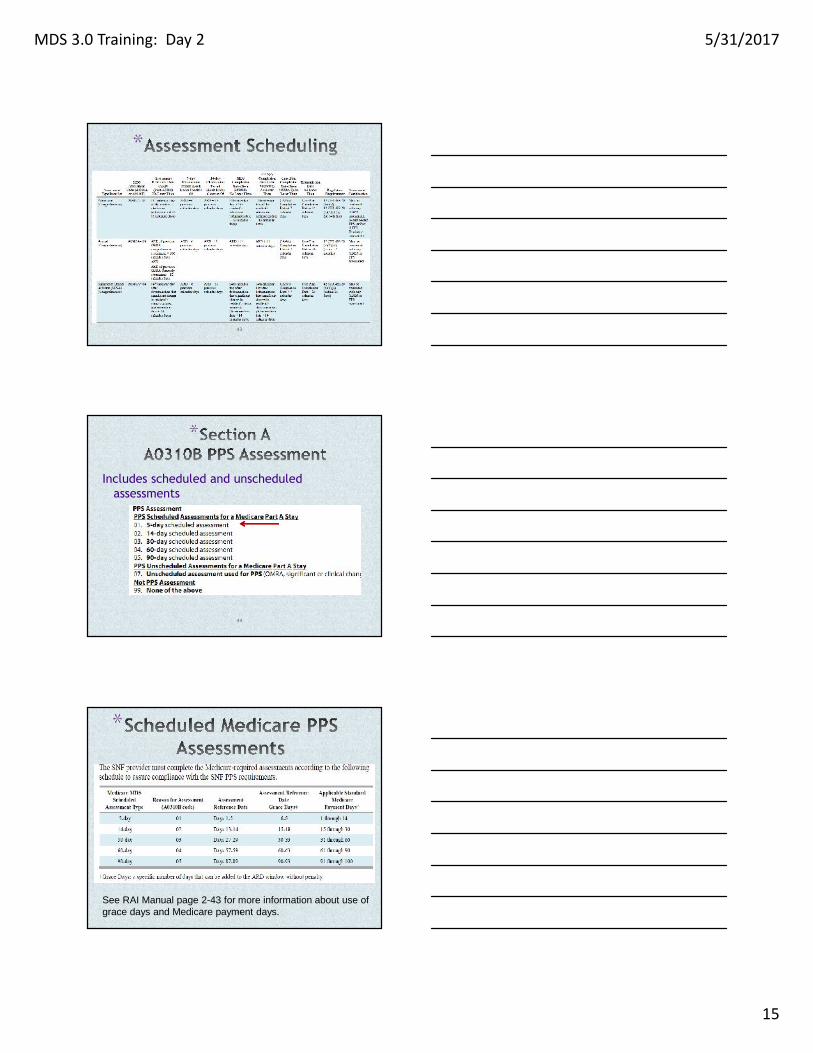
*
Includes scheduled and unscheduledassessments
44
45
*
See RAI Manual page 2-43 for more information about use ofgrace days and Medicare payment days.
MDS 3.0 Training: Day 2 5/31/2017
16
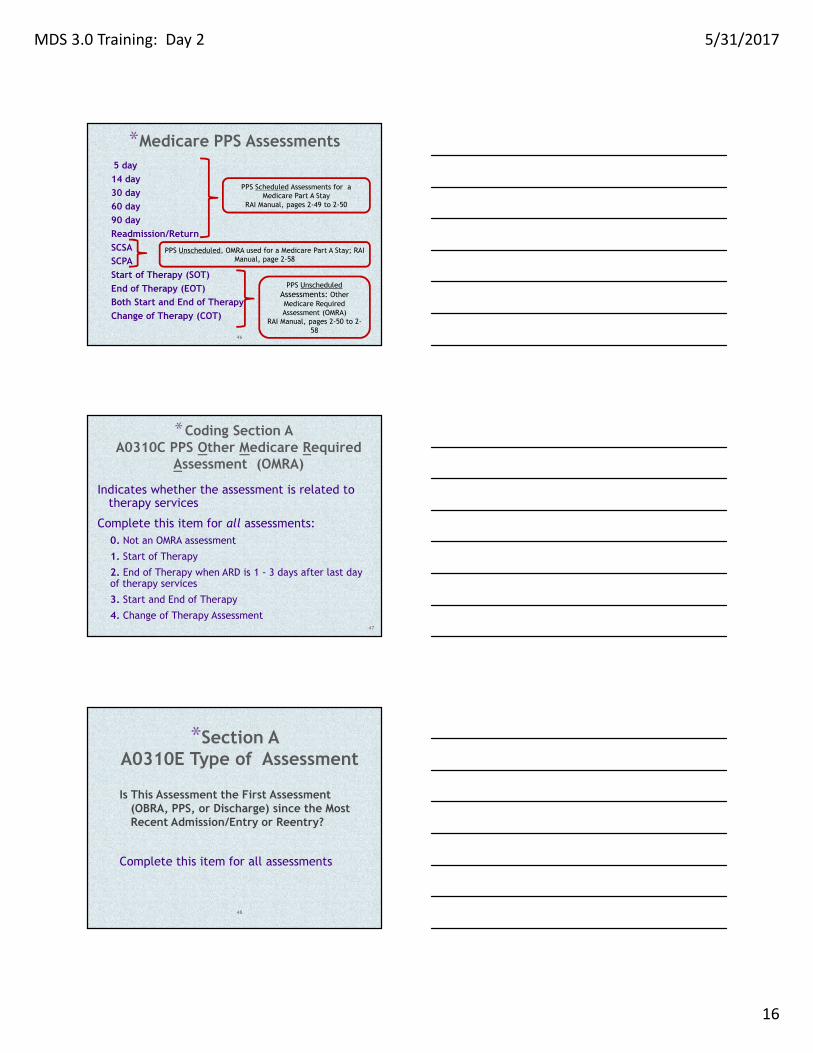
*Medicare PPS Assessments5 day14 day30 day60 day90 dayReadmission/ReturnSCSASCPAStart of Therapy (SOT)End of Therapy (EOT)Both Start and End of TherapyChange of Therapy (COT)
PPS Scheduled Assessments for aMedicare Part A Stay
RAI Manual, pages 2-49 to 2-50
PPS UnscheduledAssessments: OtherMedicare RequiredAssessment (OMRA)
RAI Manual, pages 2-50 to 2-58
PPS Unscheduled, OMRA used for a Medicare Part A Stay; RAIManual, page 2-58
46
*Coding Section AA0310C PPS Other Medicare Required
Assessment (OMRA)
Indicates whether the assessment is related totherapy services
Complete this item for all assessments:0. Not an OMRA assessment
1. Start of Therapy
2. End of Therapy when ARD is 1 - 3 days after last dayof therapy services
3. Start and End of Therapy
4. Change of Therapy Assessment47
*Section AA0310E Type of Assessment
Is This Assessment the First Assessment(OBRA, PPS, or Discharge) since the MostRecent Admission/Entry or Reentry?
Complete this item for all assessments
48
MDS 3.0 Training: Day 2 5/31/2017
17
*
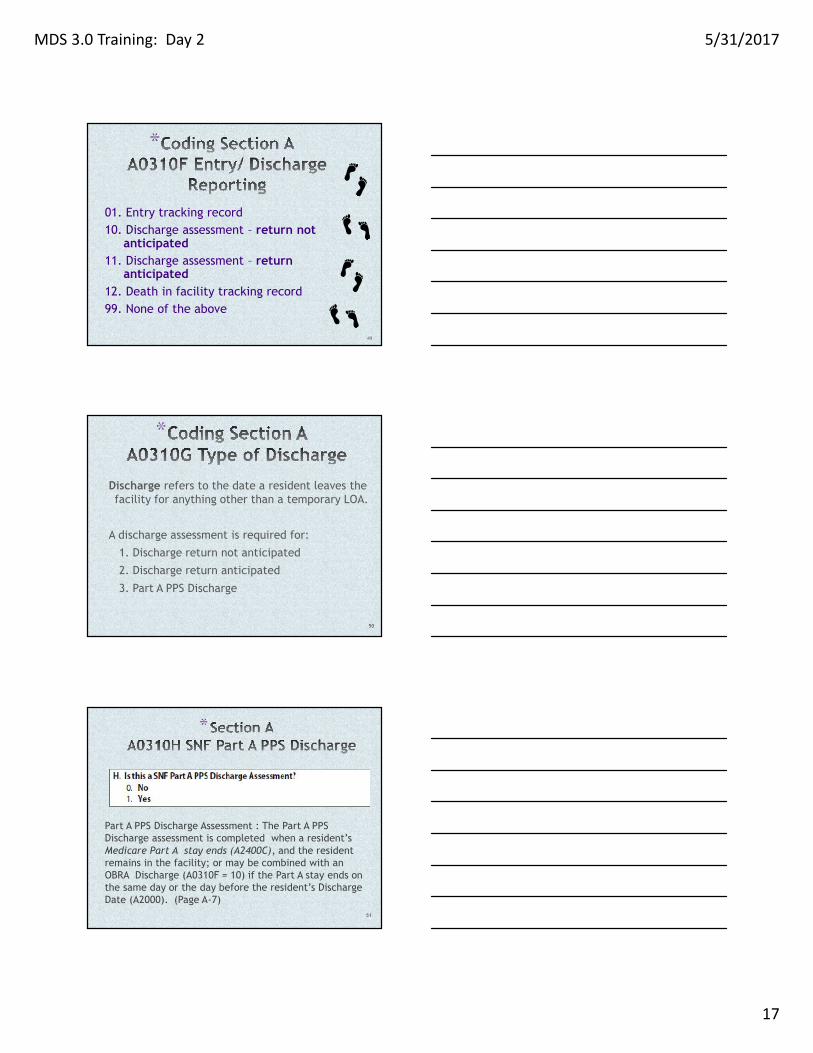
01. Entry tracking record10. Discharge assessment – return not
anticipated11. Discharge assessment – return
anticipated12. Death in facility tracking record99. None of the above
49
*
Discharge refers to the date a resident leaves thefacility for anything other than a temporary LOA.
A discharge assessment is required for:
1. Discharge return not anticipated
2. Discharge return anticipated
3. Part A PPS Discharge
50
*
Part A PPS Discharge Assessment : The Part A PPSDischarge assessment is completed when a resident’sMedicare Part A stay ends (A2400C), and the residentremains in the facility; or may be combined with anOBRA Discharge (A0310F = 10) if the Part A stay ends onthe same day or the day before the resident’s DischargeDate (A2000). (Page A-7)
51
MDS 3.0 Training: Day 2 5/31/2017
18
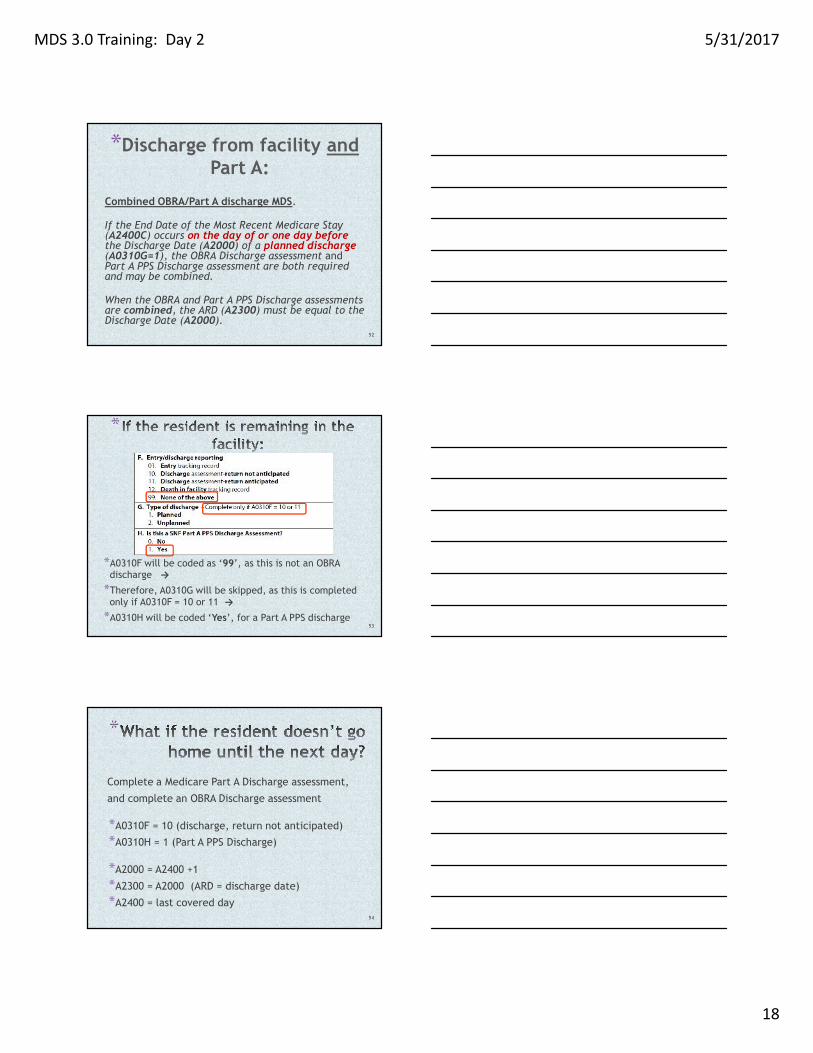
*Discharge from facility andPart A:
Combined OBRA/Part A discharge MDS.
If the End Date of the Most Recent Medicare Stay(A2400C) occurs on the day of or one day beforethe Discharge Date (A2000) of a planned discharge(A0310G=1), the OBRA Discharge assessment andPart A PPS Discharge assessment are both requiredand may be combined.
When the OBRA and Part A PPS Discharge assessmentsare combined, the ARD (A2300) must be equal to theDischarge Date (A2000).
52
*
*A0310F will be coded as ‘99’, as this is not an OBRAdischarge →*Therefore, A0310G will be skipped, as this is completedonly if A0310F = 10 or 11 →*A0310H will be coded ‘Yes’, for a Part A PPS discharge
53
*
Complete a Medicare Part A Discharge assessment,
and complete an OBRA Discharge assessment
*A0310F = 10 (discharge, return not anticipated)
*A0310H = 1 (Part A PPS Discharge)
*A2000 = A2400 +1
*A2300 = A2000 (ARD = discharge date)
*A2400 = last covered day54
MDS 3.0 Training: Day 2 5/31/2017
19
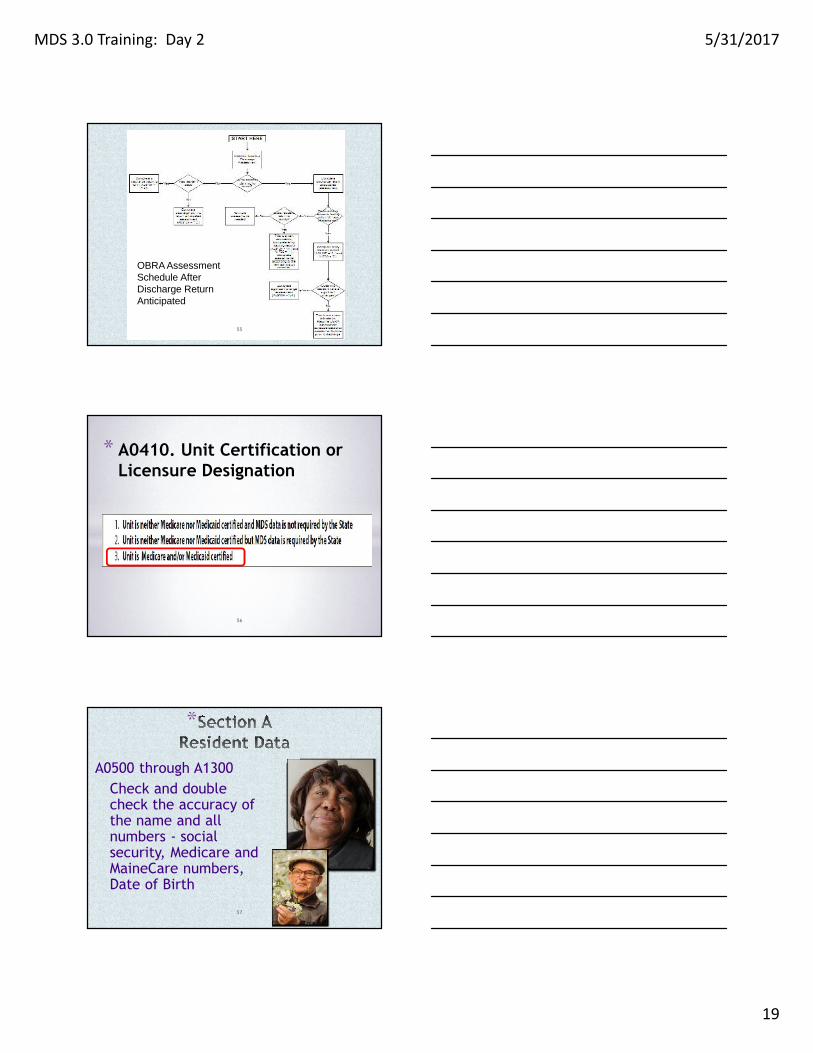
OBRA AssessmentSchedule AfterDischarge ReturnAnticipated
55
* A0410. Unit Certification orLicensure Designation
56
*
A0500 through A1300Check and doublecheck the accuracy ofthe name and allnumbers - socialsecurity, Medicare andMaineCare numbers,Date of Birth
57
MDS 3.0 Training: Day 2 5/31/2017
20
*
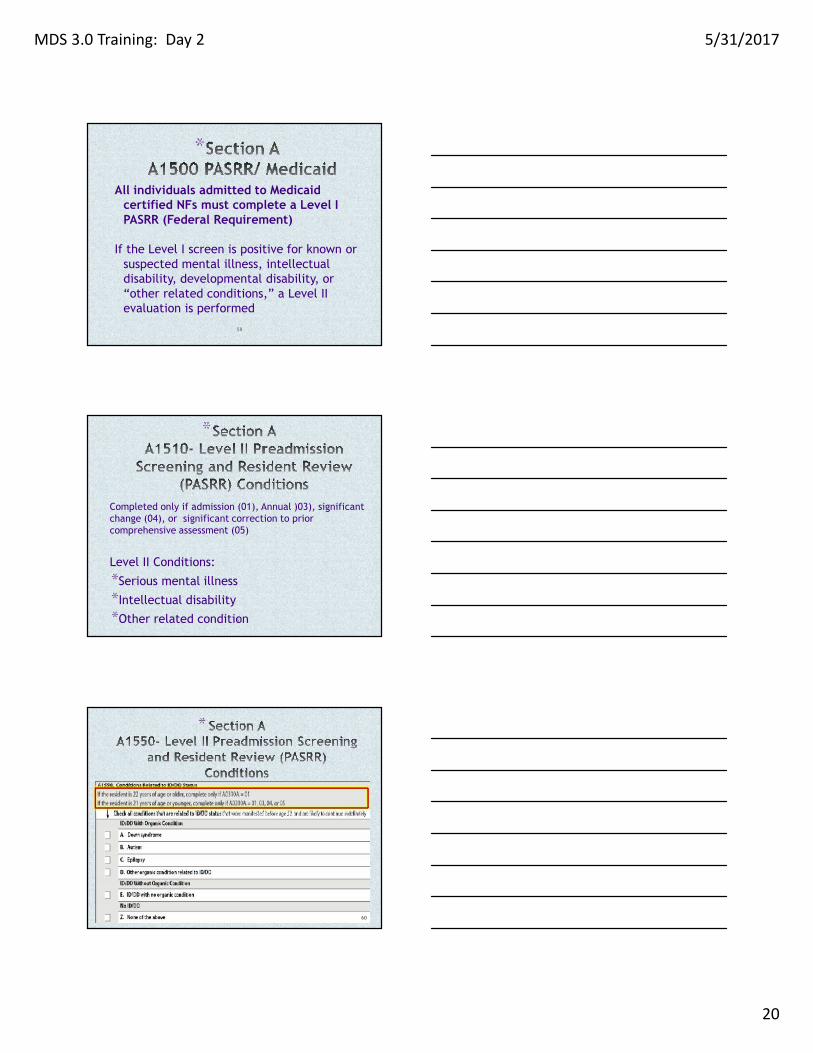
All individuals admitted to Medicaidcertified NFs must complete a Level IPASRR (Federal Requirement)
If the Level I screen is positive for known orsuspected mental illness, intellectualdisability, developmental disability, or“other related conditions,” a Level IIevaluation is performed
58
*
Completed only if admission (01), Annual )03), significantchange (04), or significant correction to priorcomprehensive assessment (05)
Level II Conditions:
*Serious mental illness
*Intellectual disability
*Other related condition59
*
60
MDS 3.0 Training: Day 2 5/31/2017
21
*http://assessmaine.com/
61
A1600-A1800 Most RecentAdmission/Entry or Reentry to thefacility
A1900 Admission Date
A2000 Discharge Date
A2100 Discharge Status62
*Section AA2300 Assessment Reference
Date (ARD)
*Designates the end of the look-back period sothat all assessment items refer to theresident’s status during the same period oftime.*Anything that happens after the ARD will notbe captured on that MDS.*The look-back period includes observations andevents through the end of the day (midnight) ofthe ARD.
63
MDS 3.0 Training: Day 2 5/31/2017
22
64
*
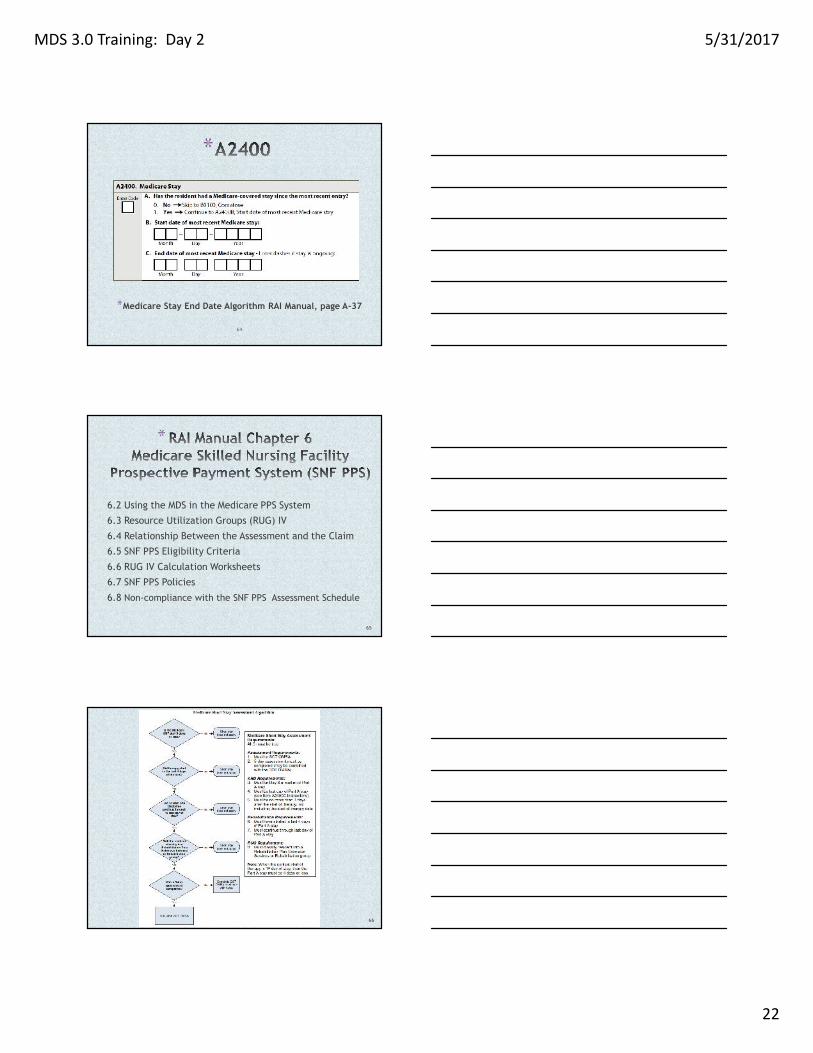
*Medicare Stay End Date Algorithm RAI Manual, page A-37
*
6.2 Using the MDS in the Medicare PPS System
6.3 Resource Utilization Groups (RUG) IV
6.4 Relationship Between the Assessment and the Claim
6.5 SNF PPS Eligibility Criteria
6.6 RUG IV Calculation Worksheets
6.7 SNF PPS Policies
6.8 Non-compliance with the SNF PPS Assessment Schedule
65
66
MDS 3.0 Training: Day 2 5/31/2017
23
Section SThis section is specific datarequirements for the State of Maineonly.
S0120 Residence Prior to AdmissionEnter the zip code of the
community address where theresident last resided prior to nursingfacility admission.
67
S0170. Advanced Directive
68
S0510. PASRR Level I Screening
Note the skip patterns
69
MDS 3.0 Training: Day 2 5/31/2017
24
S0511. PASRR Level I Date:(Complete only if S0510 = 1)
70
S0513. PASRR Level I ScreeningOutcome
71
S3300. Weight-based Equipment Need
72
MDS 3.0 Training: Day 2 5/31/2017
25
S3305. Requirements for Care,Specifically related to Weight
73
S6020. Specialized needs specificallyrelated to a resident’s need for aVentilator/Respirator
74
S6022. Direct care by a Licensed Nurse
Enter a response for A, B, and C to indicate the number of daysthe resident required direct care described
75
MDS 3.0 Training: Day 2 5/31/2017
26
S6023. Direct Care by a CNA
76
S6024. Direct Care by a Respiratory Therapist
77
Resident Stays Outside of the Facility:
S6200. Hospital StaysS6205. Observation StaysS6210. Emergency Room (ER) Visits
78
MDS 3.0 Training: Day 2 5/31/2017
27
Resident Stays
79
S8010 Payment Source – To determine paymentsource that covers the daily per diem orancillary services for the resident’s stay in thenursing facility, as of the ARD date.
• C3 – MaineCare per diem. Do not check ifMaineCare is pending
• G3 MaineCare pays Medicare or insuranceCo-pay
S8099 None of the above80
S8510. MaineCare TherapeuticLeave Days
81
MDS 3.0 Training: Day 2 5/31/2017
28
* Leave of Absence, or LOA,refers to:
• Temporary home visit• Temporary therapeutic leave• Hospital observation stay of less
than 24h where resident is notadmitted to hospital
82
S8512. MaineCare Hospital Bed-Hold Days
83
*
Intent: The intent of items in thissection is to document the resident’sability to hear (with assistive hearingdevices, if they are used), understand,and communicate with others andwhether the resident experiencesvisual limitations or difficultiesrelated to diseases common in agedpersons.
84
MDS 3.0 Training: Day 2 5/31/2017
29
*B0100: ComatoseB0200: Ability to Hear (with hearing aid if normally used)
B0300: Hearing Aid
B0600: Speech Clarity
B0700: Makes Self UnderstoodB0800: Ability to Understand Others
B1000: Vision (with adequate light)
B1200: Corrective Lenses
85
*
Intent: The items in this section are intendedto determine the resident’s attention,orientation and ability to register and recallnew information. These items are crucialfactors in many care-planning decisions.
86
*
Should the Brief Interview for Mental Status (BIMS) beconducted???
Code 0, no: if the interview should not be attemptedbecause the resident is rarely/never understood,cannot respond verbally or in writing, or an interpreteris needed but not available. Skip to C0700, StaffAssessment.
Code 1, yes: if the interview should be attemptedbecause the resident is at least sometimes understoodverbally or in writing, and if an interpreter is needed,one is available.
87
MDS 3.0 Training: Day 2 5/31/2017
30
*
C0200-C0500: BIMS resident interviewquestions (scripted interview)
88
*C0600: Should the staff assessment be conducted?
C0700-C1000 Staff assessment:C0700 Short-Term MemoryC0800 Long-Term MemoryC0900 Memory/Recall AbilityC1000 Cognitive Skills for Daily Decision Making
Documentation required to confirm responses
89
*C0200C0300 Resident Interview- BIMSC0400C0500ORB0700C0700 staff interviewC1000
To quality for the Impaired CognitionCategory, a resident must have a BIMSscore of 9 or less and an ADL score of 10or less.
90
MDS 3.0 Training: Day 2 5/31/2017
31
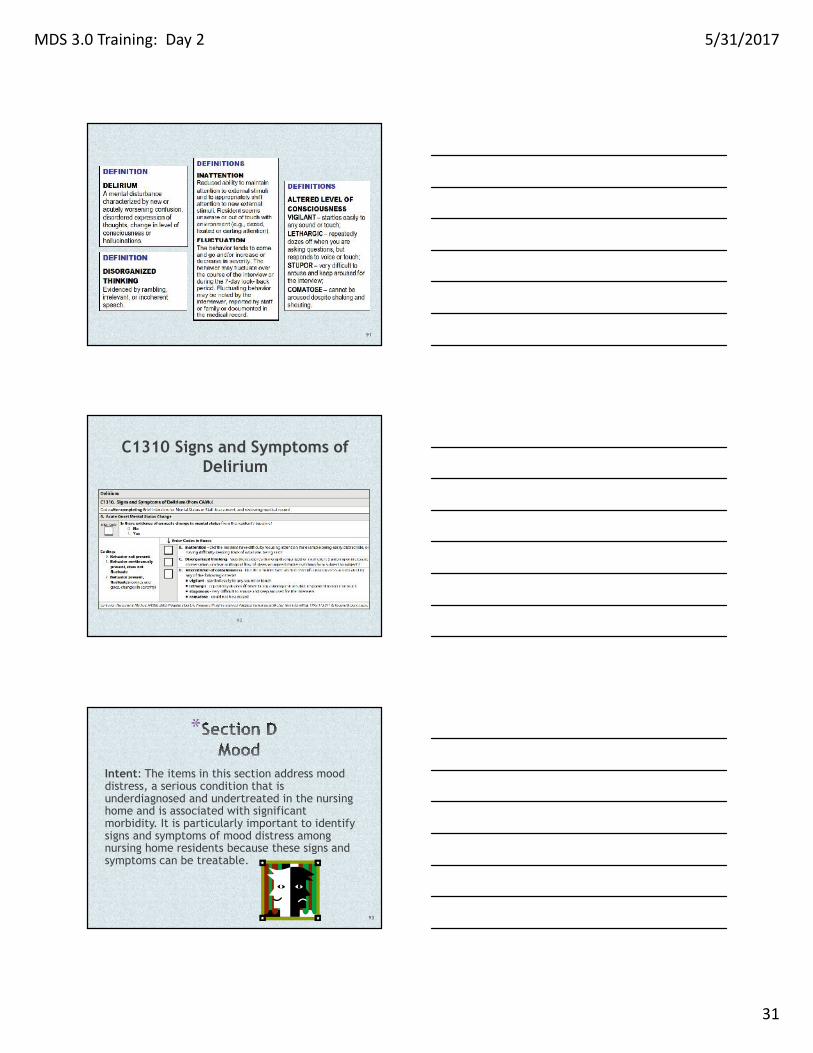
91
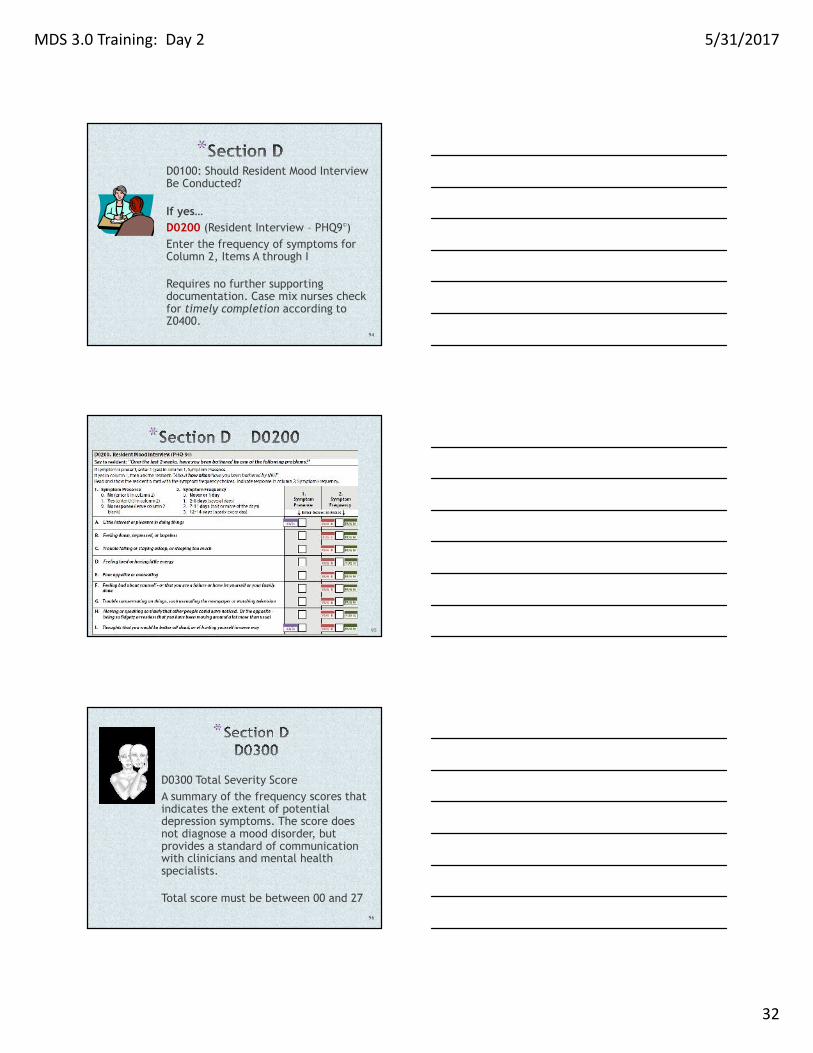
C1310 Signs and Symptoms ofDelirium
92
*
Intent: The items in this section address mooddistress, a serious condition that isunderdiagnosed and undertreated in the nursinghome and is associated with significantmorbidity. It is particularly important to identifysigns and symptoms of mood distress amongnursing home residents because these signs andsymptoms can be treatable.
93
MDS 3.0 Training: Day 2 5/31/2017
32
*D0100: Should Resident Mood InterviewBe Conducted?
If yes…D0200 (Resident Interview – PHQ9©)Enter the frequency of symptoms forColumn 2, Items A through I
Requires no further supportingdocumentation. Case mix nurses checkfor timely completion according toZ0400.
94
*
95
*
D0300 Total Severity ScoreA summary of the frequency scores thatindicates the extent of potentialdepression symptoms. The score doesnot diagnose a mood disorder, butprovides a standard of communicationwith clinicians and mental healthspecialists.
Total score must be between 00 and 27
96
MDS 3.0 Training: Day 2 5/31/2017
33
*
Staff Assessment of Resident MoodLook-back period for this item is 14days.
Interview staff from all shifts whoknow the resident best.
Supporting documentation isrequired
97
D0600 = Total Severity Score (Enter score of 00 to 30)
D0650 = safety notification if there is a possibility of residentself harm 98
*
Intent: The items in this section identifybehavioral symptoms in the last seven days thatmay cause distress to the resident, or may bedistressing or disruptive to facility residents,staff members or the care environment.
99
MDS 3.0 Training: Day 2 5/31/2017
34
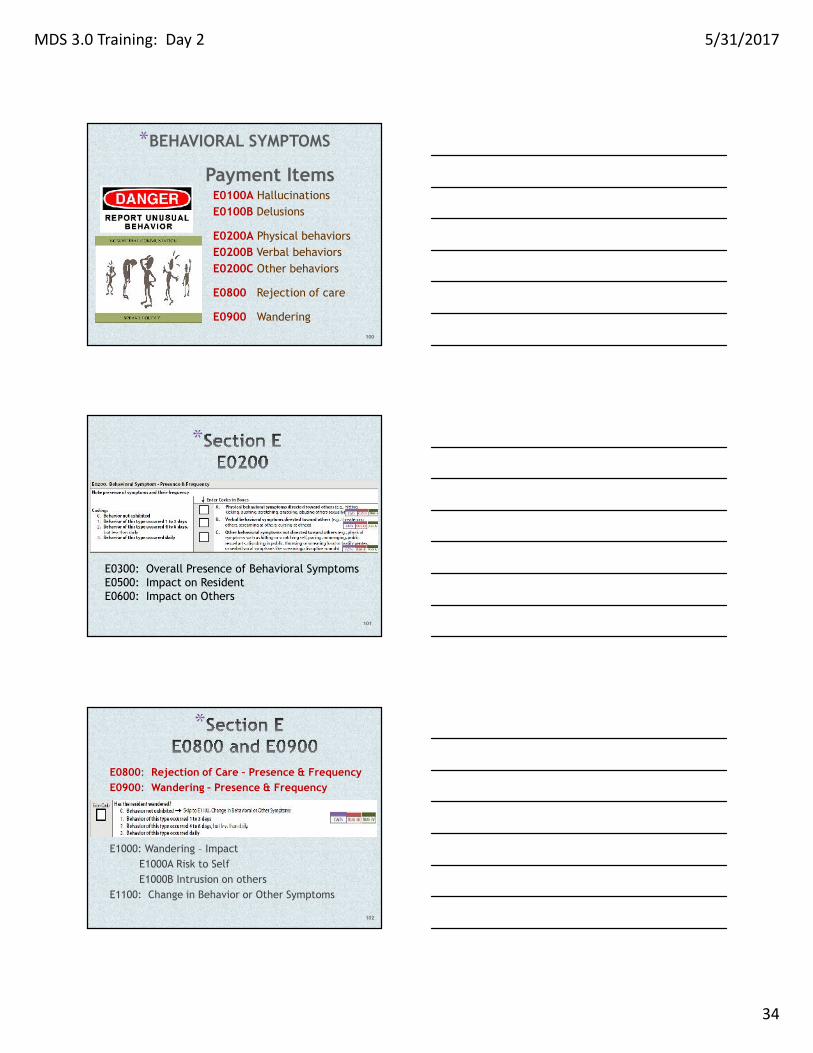
*BEHAVIORAL SYMPTOMS
Payment ItemsE0100A HallucinationsE0100B Delusions
E0200A Physical behaviorsE0200B Verbal behaviorsE0200C Other behaviors
E0800 Rejection of care
E0900 Wandering
100
*
E0300: Overall Presence of Behavioral SymptomsE0500: Impact on ResidentE0600: Impact on Others
101
*
E0800: Rejection of Care – Presence & FrequencyE0900: Wandering – Presence & Frequency
E1000: Wandering – ImpactE1000A Risk to SelfE1000B Intrusion on others
E1100: Change in Behavior or Other Symptoms
102
MDS 3.0 Training: Day 2 5/31/2017
35
*
Intent: The intent of items in this section is toobtain information regarding the resident’spreferences for his or her daily routine andactivities.
103
*1. Determine whether or not resident is rarely/never understoodand if family/significant other is available. If resident israrely/never understood and family is not available, skip to itemF0800, Staff Assessment of Daily and Activity Preferences.2. Conduct the interview during the observation period.3. Review Language item (A1100) to determine whether or notthe resident needs or wants an interpreter.• If the resident needs or wants an interpreter, complete theinterview with an interpreter.4. The resident interview should be conducted if the resident canrespond:• verbally,• by pointing to their answers on the cue card, OR• by writing out their answers.
104
*
Intent: The items in this section areintended to assess the many conditionsthat could affect the resident’s abilityto maintain adequate nutrition andhydration. This section coversswallowing disorders, height andweight, weight loss, and nutritionalapproaches. The assessor shouldcollaborate with the dietitian anddietary staff to ensure that items inthis section have been assessed andcalculated accurately.
105
MDS 3.0 Training: Day 2 5/31/2017
36
*
K0100: Swallowing disorder
K0200: Height and Weight
K0300: Weight LossK0310: Weight gain
106
*Section K - Nutritional ApproachesK0510: Approaches
A. Parenteral / IV Feeding
B. Feeding TubeC. Mechanically Altered Diet
D. Therapeutic Diet
Z. None of the above
107
*K0510 Assessment Guidelines
The following items are NOT coded inK0510A:
IV medications
IV fluids administered as a routine partof an operative or diagnostic procedureor recovery room stay
IV fluids administered solely as flushes
Parenteral/IV fluids administered inconjunction with chemotherapy ordialysis
RAI Manual pages K-10 through K-12108
MDS 3.0 Training: Day 2 5/31/2017
37
*
If the resident took no food or fluids by mouth (NPO) ortook just sips of fluid, stop here and code 3, 51% or more.
If the resident had more substantial oral intake than this,consult with the dietician.
109
K0710B.3 is apayment item
*K0710B Average Fluid Intake per Dayby IV or Tube Feeding
Code for the average number of cc perday of fluid the resident received via IVor tube feeding. Record what wasactually received by the resident, notwhat was ordered.
• Code 1: 500 cc/day or less• Code 2: 501 cc/day or more
110
K0710A and B (column 3) are payment items forResidents receiving nutrition via IV or Tube Feeding
* Section Q - Participation in Assessmentand Goal Setting
Intent: The items in this section areintended to record the participationand expectations of the resident,family members, or significant other(s)in the assessment, and to understandthe resident’s overall goals. Dischargeplanning follow-up is already aregulatory requirement (CFR 483.20(i)(3)). Interviewing the resident ordesignated individuals places theresident or their family at the center ofdecision-making.
111
MDS 3.0 Training: Day 2 5/31/2017
38
* Section Q - Participation inAssessment and Goal Setting
Q0100 Participation in Assessment:
Who participated??
Whenever possible, the resident should beactively involved-except in unusualcircumstances such as if the individual is unableto understand the proceedings or is comatose.
112
* Section Q - Participation inAssessment and Goal Setting
Q0300 Residents Overall Expectation*Overall expectations*Information source
Q0400 Discharge Plan
Q0490 Preference to Avoid Being AskedQuestion Q0500B
113
*
Q0500B Return to Community
The goal of follow-up action is to initiateand maintain collaboration between thenursing home and the local contact agencyto support the resident’s expressed interestin being transitioned to community living.
114
MDS 3.0 Training: Day 2 5/31/2017
39
* Section Q - Participation inAssessment and Goal Setting
Q0550A, Does the resident, (or family orsignificant other or guardian or legally authorizedrepresentative if resident is unable to respond)want to be asked about returning to thecommunity on all assessments? (Rather than onlyon comprehensive assessments.)
Q0550B, what is the source of the information?
115
* Section Q - Participation inAssessment and Goal Setting
Who is the Local Contact Agency for Maine?
Long Term Care Ombudsman Program
116
*Section ZAssessment Administration
Intent: The intent of the items in this sectionis to provide billing information andsignatures of persons completing theassessment.
117
MDS 3.0 Training: Day 2 5/31/2017
40
*Section ZAssessment Administration
The majority of this section is completed by yoursoftware.
Z0100 Medicare Part A Billing (RUG IV)Z0150 Medicare Part A Non-Therapy (RUG IV)Z0200 State Medicaid Billing (RUG III)Z0250 Alternate State Medicaid BillingZ0300 Insurance Billing
*****************************************************
To check your final validation report:https://sms.muskie.usm.maine.edu/
118
Z0400 Attestation Statement
Z0500 Signature of RN Assessment CoordinatorVerifying Assessment Completion
*
119
*
Z0400 Signature of Persons Completing theAssessment or Entry/Death Reporting.I certify that the accompanying information accurately reflects residentassessment information for this resident and that I collected orcoordinated collection of this information on the dates specified. To thebest of my knowledge, this information was collected in accordance withapplicable Medicare and Medicaid requirements. I understand that thisinformation is used as a basis for ensuring that residents receiveappropriate and quality care, and as a basis for payment from federalfunds. I further understand that payment of such federal funds andcontinued participation in the government-funded health careprograms is conditioned on the accuracy and truthfulness of thisinformation, and that I may be personally subject to or may subjectmy organization to substantial criminal, civil, and/or administrativepenalties for submitting false information. I also certify that I amauthorized to submit this information by this facility on its behalf.
120
MDS 3.0 Training: Day 2 5/31/2017
41
121
*Coding Instructions
• All staff who completed any part of the MDS must enter their signatures,titles, sections or portion(s) of section(s) they completed, and the datecompleted.
• If a staff member cannot sign Z0400 on the same day that he or shecompleted a section or portion of a section, when the staff member signs,use the date the item originally was completed.
• Read the Attestation Statement carefully. You are certifying that theinformation you entered on the MDS, to the best of your knowledge, mostaccurately reflects the resident’s status. Penalties may be applied forsubmitting false information.
FYI…
Chapter 110, Regulations Governing the Licensingand Function of Skilled Nursing Facilities andNursing Facilitieshttp://www.maine.gov/sos/cec/rules/10/ch110.htm
Chapter 2.B.1.b Comprehensive Assessment(page 2)b. Each individual who completes a portion of theassessment must sign and certify the accuracy ofthat portion of the assessment.
122
*
CAAs
Intent: The MDS does not constitute acomprehensive assessment. Rather, it is apreliminary assessment to identify potentialresident problems, strengths, and preferences.
and …
123
MDS 3.0 Training: Day 2 5/31/2017
42
124
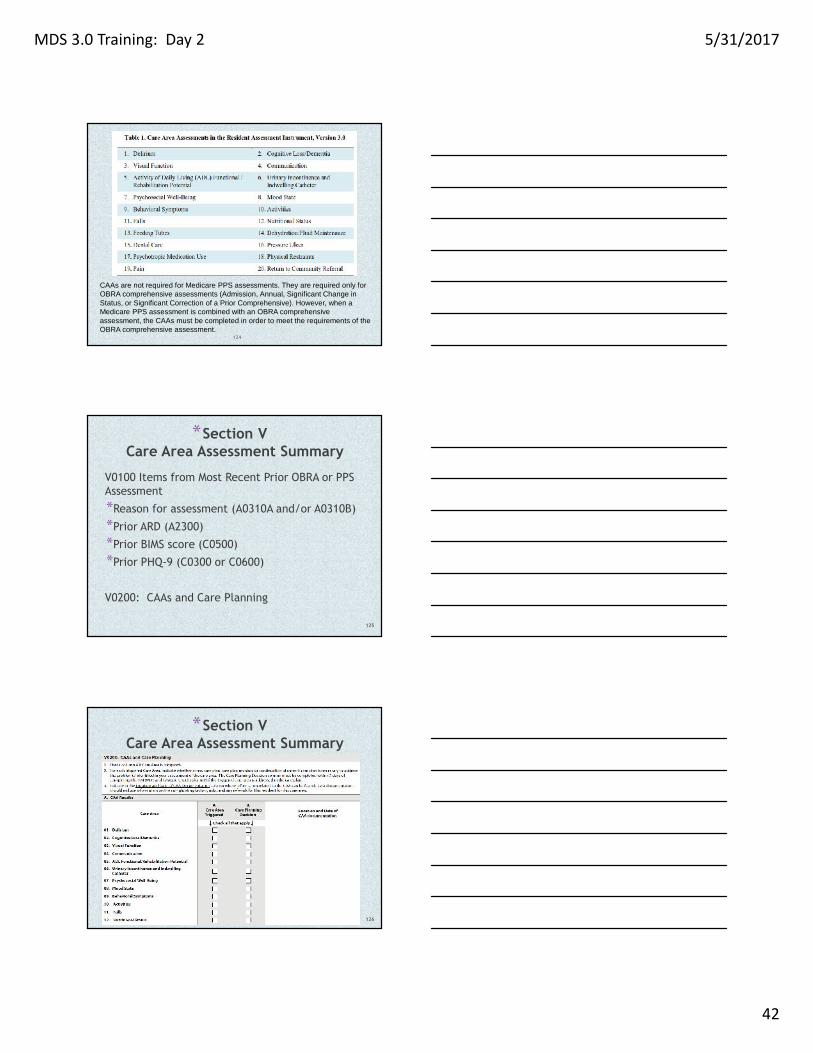
CAAs are not required for Medicare PPS assessments. They are required only forOBRA comprehensive assessments (Admission, Annual, Significant Change inStatus, or Significant Correction of a Prior Comprehensive). However, when aMedicare PPS assessment is combined with an OBRA comprehensiveassessment, the CAAs must be completed in order to meet the requirements of theOBRA comprehensive assessment.
*Section VCare Area Assessment Summary
V0100 Items from Most Recent Prior OBRA or PPSAssessment
*Reason for assessment (A0310A and/or A0310B)
*Prior ARD (A2300)
*Prior BIMS score (C0500)
*Prior PHQ-9 (C0300 or C0600)
V0200: CAAs and Care Planning
125
*Section VCare Area Assessment Summary
126
MDS 3.0 Training: Day 2 5/31/2017
43
127
*
This chapter provides information about the Care Area Assessments(CAAs), Care Area Triggers (CATs), and the process for care plandevelopment for nursing home residents.
Regulations require facilities to complete, at a minimum and atregular intervals, a comprehensive, standardized assessment ofeach resident’s functional capacity and needs, in relation to anumber of specified areas (e.g., customary routine, vision, andcontinence). The results of the assessment, which must accuratelyreflect the resident’s status and needs, are to be used to develop,review, and revise each resident’s comprehensive plan of care.
*
Intent: The purpose of Section X is to identify anMDS record to be modified or inactivated.Section X is only completed if Item A0050, Typeof Record, is coded a 2 (Modify existing record)or a 3 (Inactivate existing record).
In Section X, the facility must reproduce theinformation EXACTLY as it appeared on theexisting erroneous record, even if theinformation is incorrect. This information isnecessary to locate the existing record in theNational MDS Database.
128
*
A modification request is used to correct aQIES ASAP record containing incorrect MDSitem values due to:
• transcription errors,
• data entry errors,
• software product errors,
• item coding errors, and/or
• other error requiring modification
129
MDS 3.0 Training: Day 2 5/31/2017
44
*
An inactivation request is used to movean existing record in the QIES ASAPdatabase from the active file to anarchive (history file) so that it will notbe used for reporting purposes.
130
*
A Manual Deletion Request is required onlyin the following three cases:1. Item A0410 Submission Requirement is
incorrect.
2. Inappropriate submission of a testrecord as a production record.
3. Record was submitted for the wrongfacility.
131
*
X0150 Type of Provider
X0200 Name of Resident
X0300 Gender
X0400 Date of Birth
X0500 Social Security Number
X0600 Type of Assessment
X0700 Date on existing record
132
MDS 3.0 Training: Day 2 5/31/2017
45
*
X0800 Correction number
X0900 Reasons for Modification
X1050 Reasons for Inactivation
X1100 Name, Title, Signature,Attestation Date
133
*
5.1 Transmitting MDS Data:
The provider indicates the submission authorityfor a record in item A0410, SubmissionRequirement.
5.2 Timeliness Criteria
5.3 Validation Edits
5.4 Additional Medicare Submission Requirementsthat Impact Billing Under SNF PPS
134
*
6.2 Using the MDS in the Medicare PPS System6.3 Resource Utilization Groups (RUG) IV6.4 Relationship Between the Assessment and the Claim6.5 SNF PPS Eligibility Criteria6.6 RUG IV Calculation Worksheets6.7 SNF PPS Policies6.8 Non-compliance with the SNF PPS Assessment Schedule
135
MDS 3.0 Training: Day 2 5/31/2017
46
136
137
Forum call for Nursing Facilities
1st Thursday of the month, 1:00-2:00February, May, August and November
Call the MDS Help Desk to register!138
MDS 3.0 Training: Day 2 5/31/2017
47
139
*
Please complete your evaluations to help us tocontinually improve training to best meet yourneeds.
ASK questions!
ASK more questions!
Attend training as often as needed
Call the MDS help desk to inquire orregister for training.
**MDS Help Desk: 624-4019 or
toll-free: 1-844-288-1612
*Lois Bourque RN: 592-5909
*Darlene Scott-Rairdon RN: 215-4797
*Maxima Corriveau RN: 215-3589
*Sue Pinette RN: 287-3933 or 215-4504 (cell)
Training Portal: www.maine.gov/dhhs/dlrs/mds/training/140