Embed Size (px)
Citation preview
Sze ’ JVIR872 ’ Commentary: Measuring Cellular Immune Activation
cachectic cancer patients with an ongoing acute-phase response. Ann
Surg 1998; 227:249–254.
30. Padillo FJ, Muntane J, Montero JL, et al. Effect of internal
biliary drainage on plasma levels of endotoxin, cytokines, and C-
reactive protein in patients with obstructive jaundice. World J Surg
2002; 26:1328–1332.
31. Chen T, Zamora R, Zuckerbraun B, Billiar TR. Role of nitric oxide in liver
injury. Curr Mol Med 2003; 3:519–526.
& SIR, 2013
J Vasc Interv Radiol 2013; 24:872–873
http://dx.doi.org/10.1016/j.jvir.2013.03.007
Division of Interventional Radiology, Stanford University School of Medicine,
300 Pasteur Drive, H-3646, Stanford, CA 94305-5642. Received March 7,
2013. Address correspondence to D.Y.S.; E-mail: [email protected]
32. Ding JW, Andersson R, Stenram U. Effect of biliary decompression on
reticuloendothelial function in jaundiced rats. Br J Surg 1992; 79:648–652.
33. Welsh FKS, Ramsden CW, MacLennan K, et al. Increased intestinal
permeability and altered mucosal immunity in cholestatic jaundice. Ann
Surg 1998; 227:205–212.
34. Vane DW, Redlich P, Weber T, Leapman S, Siddiqui AR, Grosfeld
JL. Impaired immune functions in obstructive jaundice. J Surg Res
1998; 45:287–293.
INVITED COMMENTARY
Measuring (and Manipulating) Cellular ImmuneActivation
Daniel Y. Sze, MD, PhD
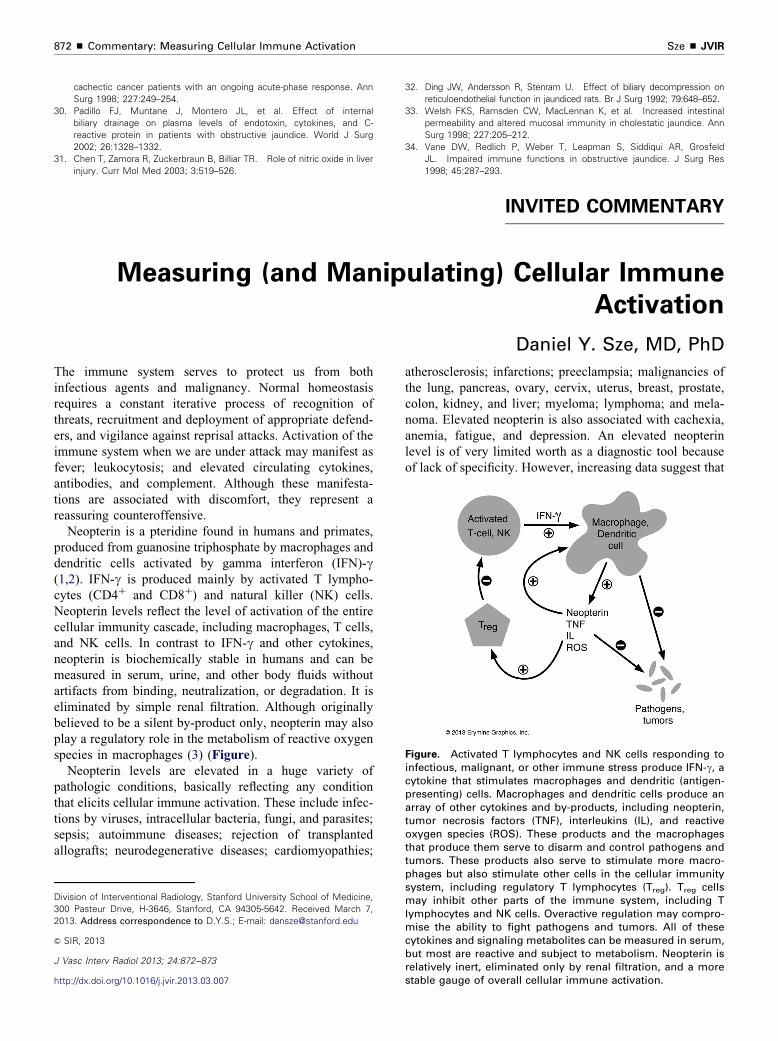
Figure. Activated T lymphocytes and NK cells responding toinfectious, malignant, or other immune stress produce IFN-g, acytokine that stimulates macrophages and dendritic (antigen-presenting) cells. Macrophages and dendritic cells produce anarray of other cytokines and by-products, including neopterin,tumor necrosis factors (TNF), interleukins (IL), and reactiveoxygen species (ROS). These products and the macrophagesthat produce them serve to disarm and control pathogens and
The immune system serves to protect us from both
infectious agents and malignancy. Normal homeostasis
requires a constant iterative process of recognition of
threats, recruitment and deployment of appropriate defend-
ers, and vigilance against reprisal attacks. Activation of the
immune system when we are under attack may manifest as
fever; leukocytosis; and elevated circulating cytokines,
antibodies, and complement. Although these manifesta-
tions are associated with discomfort, they represent a
reassuring counteroffensive.
Neopterin is a pteridine found in humans and primates,
produced from guanosine triphosphate by macrophages and
dendritic cells activated by gamma interferon (IFN)-g(1,2). IFN-g is produced mainly by activated T lympho-
cytes (CD4þ and CD8þ) and natural killer (NK) cells.
Neopterin levels reflect the level of activation of the entire
cellular immunity cascade, including macrophages, T cells,
and NK cells. In contrast to IFN-g and other cytokines,
neopterin is biochemically stable in humans and can be
measured in serum, urine, and other body fluids without
artifacts from binding, neutralization, or degradation. It is
eliminated by simple renal filtration. Although originally
believed to be a silent by-product only, neopterin may also
play a regulatory role in the metabolism of reactive oxygen
species in macrophages (3) (Figure).
Neopterin levels are elevated in a huge variety of
pathologic conditions, basically reflecting any condition
that elicits cellular immune activation. These include infec-
tions by viruses, intracellular bacteria, fungi, and parasites;
sepsis; autoimmune diseases; rejection of transplanted
allografts; neurodegenerative diseases; cardiomyopathies;
atherosclerosis; infarctions; preeclampsia; malignancies of
the lung, pancreas, ovary, cervix, uterus, breast, prostate,
colon, kidney, and liver; myeloma; lymphoma; and mela-
noma. Elevated neopterin is also associated with cachexia,
anemia, fatigue, and depression. An elevated neopterin
level is of very limited worth as a diagnostic tool because
of lack of specificity. However, increasing data suggest that
tumors. These products also serve to stimulate more macro-phages but also stimulate other cells in the cellular immunitysystem, including regulatory T lymphocytes (Treg). Treg cellsmay inhibit other parts of the immune system, including Tlymphocytes and NK cells. Overactive regulation may compro-mise the ability to fight pathogens and tumors. All of thesecytokines and signaling metabolites can be measured in serum,but most are reactive and subject to metabolism. Neopterin isrelatively inert, eliminated only by renal filtration, and a morestable gauge of overall cellular immune activation.

Volume 24 ’ Number 6 ’ June ’ 2013 873
it can be useful for prognostication and may exceed the
utility of other nonspecific tests of immune activation, such
as C-reactive protein and erythrocyte sedimentation rate.
However, measurement of neopterin is not offered in most
clinical laboratories and requires timely centrifugation and
freezing of serum and radioimmunoassay.
If immune activation represents our counteroffensive
against infectious or malignant threats, it seems that an
elevation of neopterin level should be an encouraging sign.
In their article in this issue, Yilmaz et al (4) describe the
opposite prognosis—pronounced elevation of the serum
neopterin level was associated with a poor outcome in
patients undergoing percutaneous drainage of malignant
biliary obstruction from a variety of different cell types.
This finding confirms what has been found in nearly every
other study on neopterin in malignancy or infection,
showing correlation of neopterin elevation with tumor
aggressiveness and poor patient survival. Are we to
conclude that cellular immune activation is harmful in
patients with cancer or infection? No. A moderate eleva-
tion in neopterin, similar to a moderate fever or moderate
leukocytosis, probably represents the immune system
getting the job done. An extreme elevation of neopterin,
such as a fever of 431C with a heart rate of 150 beats/min,
represents the desperate last paroxysms of an overwhelmed
and defeated immune system.
If extreme elevation of neopterin level is a death knell,
how can it be useful in clinical practice? Frequently, there
are other signs of impending demise that may be quicker
and cheaper to measure and to interpret. What remains
under investigation is whether the cellular immune system
gone awry can be effectively modulated to improve its
function and whether this function can be monitored using
neopterin as a metabolomic gauge. Immunomodulation,
specifically immunosuppression in circumstances of infec-
tious, inflammatory, or malignant stress, is not an alien
concept; for instance, corticosteroids have been shown to
improve the outcome in severe sepsis, when intuitively,
immunosuppression could worsen the infection and the
outcome (5). Yilmaz et al (4) have described a model in
which immunomodulation may potentially be attempted in
an identified patient population carrying an extremely
grave prognosis.
REFERENCES
1. Sucher R, Schroecksnadel K, Weiss G, Margreiter R, Fuchs D,
Brandacher G. Neopterin, a prognostic marker in human malignancies.
Cancer Lett 2010; 287:13–22.
2. neopterin_e.pdf. Available at: http://www.neopterin.net. Accessed March
4, 2013.
3. Murr C, Widner B, Wirleitner B, Fuchs D. Neopterin as a marker for
immune system activation. Curr Drug Metab 2002; 3:175–187.
4. Yilmaz B, Parildar Z, Bozkaya H, et al. Prognostic utility of serum
neopterin in obstructive jaundice secondary to malignant lesions treated
by percutaneous transhepatic biliary drainage. J Vasc Interv Radiol 2013;
24:865–871.
5. Skrupky LP, Kerby PW, Hotchkiss RS. Advances in the management of
sepsis and the understanding of key immunologic defects. Anesthesiol-
ogy 2011; 115:1349–1362.





























