Embed Size (px)
Citation preview

Herz 2011 · 36:296–305DOI 10.1007/s00059-011-3470-3Published online: 9 June 2011© Urban & Vogel 2011
Y. Shi1 · M. Moon1 · S. Dawood2 · B. McManus3 · P.P. Liu1
1 Division of Cardiology, Heart and Stroke/Richard Lewar Centre of Excellence, University Health Network, University of Toronto, Toronto General Hospital, Toronto
2 Department of Medicine, Saint John Hospital & Medical Center, Detroit3 Institute for HEART+LUNG Health, UBC James Hogg Research
Centre, and NCE CECR PROOF Centre of Excellence, St. Paul’s Hospital, University of British Columbia, Vancouver
Mechanisms and management of doxorubicin cardiotoxicity
Main topic/CME
Introduction
Doxorubicin (Dox; trade name, Adriam-ycin) is an anthracycline antibiotic used in cancer chemotherapy. It is effective in a wide range of cancers, including both he-matological and solid tumors. The thera-peutic activity of doxorubicin is achieved through the processes of intercalating in-to DNA, inhibiting topoisomerase II, and preventing DNA and RNA synthesis [1]. Acute adverse effects of doxorubicin oc-curring during and within 2–3 days of ad-ministration can include nausea, vomit-ing, neutropenia, alopecia, and arrhyth-mias. The incidence of acute cardiotox-icity is approximately 11% [2]. A chron-ic side effect of doxorubicin is its dose-dependent cardiotoxicity. As the lifetime accumulative dose approaches 500 mg/m2 and beyond, iatrogenic life-threaten-ing cardiomyopathy becomes more like-ly, which can lead to dilated cardiomy-opathy (DCM) and congestive heart fail-ure (CHF) in up to 20% of cases [2]. This chronic cardiotoxicity is likely related to iron oxidation and oxygen free radical for-mation, rather than the drug’s anti-tumor mechanisms, since cardiomyocytes are minimally replicating cells. Other mecha-nisms may include abnormal protein pro-cessing, hyper-activated innate immune responses, doxorubicin-induced gene al-terations, inhibition of survival and/or growth factors, impaired progenitor cell
renewal/cardiac repair, and decreased vas-culogenesis. This review focuses on the new mechanisms of doxorubicin toxicity and potential clinical approaches to mini-mize toxicity and maximize patients’ qual-ity of life and survival.
Metabolic and pharmacokinetic features of doxorubicin
The anthracycline antibiotic family com-prises hundreds of analogues, but only a few are in actual clinical use. The best known and most widely used is doxoru-bicin. Anthracyclines are metabolized by reducing a ketone group to a hydrox-yl group, which are less active than the parent compound. Pharmacokinetic fea-tures include a rapid distribution phase and a slow elimination phase, with the half-lives of doxorubicin and its stron-ger metabolites in plasma being approx-imately 5 min, 1 h, and 30 h, respectively. Since these are mainly excreted through bile, special care must be taken in patients with hepatic dysfunction [3]. The newer anthracyclines, such as epirubicin, ida-rubicin, or liposomal preparations, have higher lipophilicity and putatively greater safety. However, the risk of inducing car-diomyopathy is not abated, and there is al-ways concern regarding tumoricidal effi-cacy [4, 5].
Doxorubicin has been detected immu-nohistochemically directly in cardiomyo-
cytes and in kidney, pancreas, hair follicle, and stomach cells [6]. In cardiomyocytes, these drugs trigger reactive oxygen species (ROS) production and are in turn inacti-vated as a result of ROS production [7, 8].
Pathology and physiology of doxorubicin-induced congestive heart failure
Doxorubicin typically induces dilated car-diomyopathy, demonstrating microscop-ic features including myofibrillar loss, cy-toplasmic vacuolization, apoptosis, inter-stitial edema, and fibroplasia [2]. Cardiac fiber loss contributes to the transforma-tion of ventricular dilatation into a glob-ular geometry accompanied by increased wall stress, impaired relaxation, and im-paired contractility, all of which contrib-ute to the development of CHF [9]. Clin-ical biomarkers, such as the natriuretic peptides (BNP or proBNP) and troponins, may increase and serve as important ear-ly predictors of the preclinical phase of the cardiotoxic effect of anthracyclines [10].
Mechanisms of doxorubicin cardiotoxicity
The mechanisms of doxorubicin cardio-toxicity have recently been elucidated in more detail. Some of these are discussed below (. Fig. 1).
296 | Herz 4 · 2011

Doxorubicin-related iron and redox injury
Studies have shown that doxorubicin can directly increase the labile intracellular iron pool, which generally represents <5% of total cellular iron [11]. Cellular iron ho-meostasis is regulated by the transferrin receptor (TfR) and storage regulator ferri-tin. The former controls iron uptake by in-ternalizing iron-laden transferrin; the lat-ter stores iron in excess of the metabolic requirements of the cell. Both TfR and fer-ritin are mainly regulated at a post-tran-scriptional level involving interactions of iron regulatory protein (IRP)-1 with specific motifs in so-called iron-respon-sive elements (IREs) in target genes [12]. Doxorubicin and its metabolites can dis-rupt the Fe-S cluster of cytoplasmic acon-itase and inhibit IRP-1, whose role it is to adapt the levels of cellular iron appropri-ate to the metabolic needs of the cell. It has been suggested that doxorubicin-mediat-ed intracellular iron accumulation causing increased oxidative stress is a major as-pect of doxorubicin toxicity and that iron chelators are highly effective in reducing doxorubicin-induced cardiotoxicity [13, 14]. Interestingly, patients harboring gene mutations in hereditary hemochromato-sis (HH) show increased susceptibility to doxorubicin cardiotoxicity and exacerbat-ed iron metabolism [15].
Increased oxidative stress due to doxo-rubicin metabolism has also been consid-ered as the classical mechanism of cardio-toxicity. Reduced doxorubicin results in the formation of a semiquinone free rad-ical, which regenerates its parent quinone by reducing molecular oxygen to super-oxide anion (O2
–) and hydrogen perox-ide (H2O2), potent members of cardiotox-ic ROS [16].
Despite the widely accepted theory of ROS and iron as the primary mechanism of doxorubicin toxicity, the use of antioxi-dants has failed to date to alleviate anthra-cycline cardiotoxicity in clinically relevant animal models and clinical trials. In ad-dition, studies with potent and selective chelators for iron have also yielded nega-tive or mixed results, likely suggesting that mechanisms other than ROS and iron are involved in doxorubicin-induced cardio-toxicity [17].
Abstract · Zusammenfassung
Herz 2011 · 36:296–305 DOI 10.1007/s00059-011-3470-3© Urban & Vogel 2011
Y. Shi · M. Moon · S. Dawood · B. McManus · P.P. Liu
Mechanisms and management of doxorubicin cardiotoxicity
AbstractDoxorubicin is an effective anti-tumor agent with a cumulative dose-dependent car-diotoxicity. In addition to its principal tox-ic mechanisms involving iron and redox re-actions, recent studies have described new mechanisms of doxorubicin-induced cell death, including abnormal protein process-ing, hyper-activated innate immune re-sponses, inhibition of neuregulin-1 (NRG1)/ErbB(HER) signalling, impaired progenitor cell renewal/cardiac repair, and decreased vas-culogenesis. Although multiple mechanisms involved in doxorubicin cardiotoxicity have been studied, there is presently no clinical-
ly proven treatment established for doxorubi-cin cardiomyopathy. Iron chelator dexrazox-ane, angiotensin converting enzyme (ACE) in-hibitors, and β-blockade have been proposed as potential preventive strategies for doxoru-bicin cardiotoxicity. Novel approaches such as anti-miR-146 or recombinant NRG1 to in-crease cardiomyocyte resistance to toxicity may be of interest in the future.
KeywordsChemotherapy · Doxorubicin · Cardiotoxicity · Cardiomyopathy · Iron
Mechanismen und Management der Doxorubicinkardiotoxiztät
ZusammenfassungDoxorubicin ist eine hochwirksame antineo-plastische Substanz mit einer von der kumu-lativen Dosis abhängigen Kardiotoxizität. Ne-ben den hauptsächlichen toxischen Mecha-nismen mit Eisen und Redoxreaktionen wur-den in letzter Zeit neue Ursachen für den do-xorubicininduzierten Zelltod beschrieben, u. a. eine pathologische Eiweißprozessierung, eine überproportionale Stimulation des an-geborenen Immunsystems, die Inhibition der Neuregulin-1(NRG1)-ErB(HER)-Signalkas-kade, eine gestörte Erneuerung der kardia-len Progenitorzellen und Reparaturmecha-nismen und eine verminderte Vaskulogene-se. Obwohl verschiedene Mechanismen der Doxorubicinkardiotoxizität bisher untersucht
wurden, fehlt es bislang an einer klinisch ef-fektiven und etablierten Behandlung der Do-xorubicinkardiomyopathie. Der Eisenchelat-bildner Dexrazoxan, ACE-Hemmer und Beta-blocker wurden als eine mögliche präventive Behandlung diskutiert. Neue Therapieansätze stützen sich auf Anti-MiR-146 oder rekombi-nantes NRG1 zur Verbesserung der Resistenz der Kardiomyozyten gegen die toxische Ne-benwirkung und könnten zukünftig von be-sonderem Interesse sein.
SchlüsselwörterChemotherapie · Doxorubicin · Kardiotoxizität · Kardiomyopathie · Eisen
297Herz 4 · 2011 |

Doxorubicin-induced cell death
In addition to the traditionally empha-sized “ROS and iron” hypothesis involved in cell death, evidence has emerged that doxorubicin could directly interact with cell death triggers [18]. There are general-ly three forms of cell death: necrosis, apop-tosis, and autophagy. Necrosis is charac-terized by extensive and uncontrolled cell death with inflammatory cell infiltration. Apoptosis is a programmed process with no rupture of the plasma membrane and characteristic morphological changes in-
cluding cell shrinkage, chromatin conden-sation, and nuclear fragmentation. Au-tophagy occurs locally within a cell and is a catabolic process involving the deg-radation of a cell’s own intracellular com-ponents through the lysosomal machin-ery. Doxorubicin induces mitochondri-al DNA damage, mitochondrial mem-brane disruption, mitochondrial dysfunc-tion, and ATP depletion, all of which con-tribute to necrosis [19, 20, 21, 22, 23, 24]. Numerous studies have shown that doxo-rubicin induces apoptosis of cardiomy-ocytes through the activation of p53 [25,
26], down-regulation of GATA-4 [27, 28, 29], and degradation of p300 (. Fig. 1, [30, 31]). Transcription factor GATA-4 is a survival factor for differentiated, post-na-tal cardiomyocytes and an upstream acti-vator of the anti-apoptotic gene Bcl-X [27]. Anthracycline-induced downregulation of GATA-4 is mediated by the inhibition of GATA-4 gene transcription involving the p53-dependent inhibition of CBF/NF-Y binding to the CCAAT box within the GATA-4 promoter [29]. The transcription-al co-activator p300 is generally implicat-ed in different cellular processes, includ-
DOX
TLR2 ↑TLR4 ↑TIR ↑
NFKB ↑GATA4 ↓
In�ammation ↑
Necrosis ↑
Apoptosis ↑
Cardiomyopathy
Atrogin-1 ↑MuRF ↑
Ubiquitin ↑
Proteosome ↑
MAPK ↑p38 ↑JNK ↑
Cardiomyopathy
Apoptosis ↑
DOX-proteosomecomplex
UPS ↑
DOX-DNAcomplex
Caspase 9 ↑
Bax ↑Bcl2 ↓p300 ↓
NFAT -5 ↓TauT ↓
Pro-apoptotic factors ↑
Anti-apoptotic factors ↓ Myo�lament
proteins ↓
Myo�brillarproteins ↓
β-catenin ↓ARC ↓
NRG1 ↓ErB4 ↓
Akt ↓Erk ↓
Caspase 3 ↑
ROS ↑
Mitochondrial damage ↑ Labile
intracellular iron pool ↑
IRP -1Ferritin ↓
Intracellular Ca2+ ↑
Autophagy ↑
Iron Rich LysosomeRupture ↑
Necrosis ↑
Cardiomyopathy
Apoptosis ↑
Cardiomyopathy
CPCBMPC
EC
Cardiac repair ↓
Cardiomyopathy
P300 ↓
p38 ↑
CARP ↑H-FABP ↑OCTN2 ↑
Troponin c ↓ANF ↓
CD95 ↑
Apoptosis ↑
p53 ↑
CBF/NF-Y ↓
GATA4 ↓
Bcl-X ↓
Telomerase ↓
Senescence ↑
Cardiomyopathy
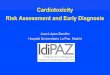
Fig. 1 8 A summary of potential mechanisms involved in doxorubicin (Dox)-induced cardiomyopathy as described in the text. The major mechanisms involve ROS and iron (red). Meanwhile, Dox-induced cell death (necrosis, apoptosis, and autoph-agy) and activation of innate immunity (brown), gene changes that reduce cardiac-specific gene expression or trigger apop-tosis, induction of cardiac premature senescence in cardiomyocytes (yellow), activation of the ubiquitin-proteasome system (UPS) causing the balance of the protein system to shift toward pro-apoptosis, downregulation of prosurvival gene (NRG1 and ErB4) expression (blue), and impaired cardiac repair by inhibiting bone marrow, cardiac progenitor cell, and/or endothe-lial cell function (green) all emerge as potential mechanisms contributing to Dox cardiotoxicity. ROS reactive oxygen species, IRP iron regulatory protein, TLR toll-like receptor, TIR toll-interleukin-1 receptor, CARP cardiac Adriamycin-responsive protein, H-FABP heart fatty acid binding protein, OCTN organic cation/carnitine transporter, ARC apoptosis repressor with caspase re-cruitment domain, NFAT nuclear factors of activated T-cell, TauT taurine transporter, NRG neuregulin, ErbB epidermal growth factor receptor B, BMPC bone marrow cardiac progenitor cell, CPC cardiac progenitor cell, EC endothelial cell, arrows pointing up or down (inside text boxes) indicate increases or decreases in function or expression, horizontal arrows indicate positive re-gulatory sequence, blocks represent inhibition
298 | Herz 4 · 2011
Main topic/CME

ing regulation of the cell cycle, differentia-tion, tumorigenesis, and apoptosis [32, 33]. Doxorubicin-activated p38 kinases alpha and beta are associated with phosphoryla-tion of p300 and are implicated in the deg-radation of p300, which parallels the apop-tosis of primary neonatal cardiomyocytes observed in response to doxorubicin [31]. Pharmacological blockade of p38 prevents p300 degradation. Restoration of GATA4 [34] and p300 [30] inhibits doxorubicin-induced cardiomyocyte death.
Autophagy, an intralysosomal degra-dation of a cell’s own constituents, plays an important role in the renewal of cardi-ac myocytes that are represented by long-lived post-mitotic cells [35]. Autophagy re-cycles cellular constituents and is substan-tially enhanced under pathological condi-tions, including cardiac hypertrophy, dil-atation, cardiomyopathy, and heart fail-ure. Studies have indicated that autopha-gy may have dual effects in the heart un-der stress: removing protein aggregates and damaged organelles as a pro-surviv-al pathway maintaining energy homeo-stasis, while excessive levels of autoph-agy can lead to cell death [18]. Excessive levels of autophagy in response to cell re-pair, starvation, or various stressors (e.g., ROS, ionizing radiation, hypoxia, etc.) re-sult in the rupture of autophagolysosomes with the release of lysosomal hydrolases and ensuing apoptosis [36]. The mecha-nism behind rupture of this kind may be that the lysosomal compartment is greatly enriched with labile iron when substantial parts of it have been subjected to autoph-agy, e.g., as a result of the degradation of mitochondria containing metalloproteins such as cytochrome c. The increase in in-tracellular calcium mediated by ROS not only induces apoptosis and necrosis, but also activates calmodulin-dependent ki-nase and AMP-activated protein kinase [37, 38, 39]. ROS production can also rup-ture iron-rich lysosomes, while the deg-radation of iron-saturated ferritin in lyso-somes mediates myocardial injury in he-mochromatosis, an acquired or hereditary disease associated with iron overload [36]. Therefore, doxorubicin affects the signal-ing process to enhance autophagy in the heart through both iron and ROS mecha-nisms in order to mediate lysosomal deg-radation.
In summary, all three types of cell death can be directly induced by doxoru-bicin, converging in the myocardium and eventually leading to cardiomyopathy. Therapeutic opportunities may include the inhibition of apoptotic pathways with caspase inhibitors and overexpression of Bcl-2 and Akt [41].
Doxorubicin-induced cardiotoxicity is associated with cardiac inflammation mediated by activation of the innate immune system
The innate immune system has long been regarded as the first line of defense against foreign pathogens [40]. Doxoru-bicin stimulates cytokine production, aug-ments natural killer (NK) cell activity [41], stimulates cytotoxic T-lymphocyte (CTL) responses [42], and augments differentia-tion of macrophages [43], all of which are important components of both innate and adaptive immune responses, leading to di-rect cardiac damage.
Toll-like receptors (TLRs) are part of the innate immune system and are germ-line-encoded receptors involved in the car-diac stress reaction. They are key compo-nents of innate immunity and are acti-vated in response to pathogens as well as non-pathogenic components of damaged tissue. A growing body of evidence indi-cates a causal link between TLRs and the development of heart failure [44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55]. Among the TLR family, TLR2 and TLR4 are the most extensively studied in terms of the patho-genesis of cardiomyopathy. TLR2 is in-volved in the oxidative stress-induced ac-tivation of NF-κB in neonatal rat cardio-myocytes, which is necessary for cardio-myocyte apoptosis [56, 57]. In TLR2-de-ficient mice, the activation of NF-κB was suppressed following exposure to doxoru-bicin, and there were fewer TUNEL-posi-tive nuclei and less caspase-3 activity than in WT mice (. Fig. 1, [50]). TLR4 acti-vation not only triggers an inflammatory response but also results in extracellular matrix degradation, causing a vicious cy-cle, the outcome of which is cardiomyop-athy [58]. TLR4 deficiency is able to atten-uate the generation of oxidative stress in the heart and prevent GATA-4 downreg-
ulation [51]. TLRs together with interleu-kin-1 receptors form a receptor superfam-ily with shared TIR (Toll-IL-1 receptor) do-mains [59]. Recombinant human interleu-kin-1 receptor antagonist (rhIL-1Ra) pre-vented doxorubicin cardiomyopathy by di-minishing microstructural damages [55].
Taken together, doxorubicin cardiotox-icity broadly involves the activation of in-nate immunity and its downstream effects.
Doxorubicin alters cardiac- specific gene expression and interferes with the cardiac stress response
Recent studies have shown that doxorubi-cin has a wide range of effects on cardiac-specific gene expression, including struc-tural, metabolic, and enzyme activities.
In a chronic doxorubicin-exposure mouse model, cDNA microarray identi-fied dysregulated genes that implicate spe-cific mechanisms of cardiac toxicity, in-cluding STARS, a hypertrophy-responsive gene; SNF1-kinase, a potential modulator of ATP levels; and AXUD1, a downstream target of the proapoptotic regulator AX-IN1 [9]. Additional gene candidates affect-ed mitochondrial function, glycolysis, and fatty acid metabolism [60].
Alterations in contractile proteins have also been found in doxorubicin-treated animals [10]. Natriuretic peptide, cardiac troponin (cTnI or cTnT), and beta-myo-sin heavy chain expression progressively increased with escalating doxorubicin ex-posure [61, 62]. Constitutively expressed, cardiac Adriamycin-responsive protein (CARP) mRNA is exquisitely sensitive to doxorubicin [63]. Overexpression of CARP in cardiomyocytes suppressed car-diac troponin C and atrial natriuretic fac-tor transcription [63].
Acute doxorubicin (i.p. 15 mg/kg) tox-icity in rats increases the expression of several cytochrome P450 (CYP) enzymes with a consequent alteration in arachidon-ic acid metabolism, causing progressive cardiotoxicity [64]. Heart fatty acid bind-ing protein (H-FABP) and organic cation/carnitine transporter (OCTN2) are criti-cal for lipid metabolism and energy gen-eration. Chronic treatment with doxorubi-cin in Wistar rats decreased H-FABP and OCTN2 genes in cardiac tissue, while in-
299Herz 4 · 2011 |

creasing expression of apoptotic genes p53 and CD95 (. Fig. 1, [65]).
Doxorubicin also directly affects the cardiac-specific gene expression of regu-lators of energy and calcium metabolism [66, 67, 68, 69]. In an animal study [66], doxorubicin had a pronounced effect on electron transport chain activity, which led to the loss of ATP, increased AMPK expression, mitochondrial genome am-plification, and caspase 3 activation. Tran-scripts of important enzymes critical for energy production, such as ADP/ATP translocase, Rieske iron-sulphur protein, and phosphofructokinase, are rapidly de-graded as early as 2 h after doxorubicin ad-ministration [68]. The expression of gene-encoding proteins that affect calcium ion homeostasis was also altered in the hearts of rabbits chronically treated with doxoru-bicin, including significantly diminished ryanodine receptor-2, sarcoplasmic retic-ulum Ca2+-ATPase, phospholamban, and cardiac calsequestrin [69].
In addition to the aforementioned mechanisms underlying doxorubicin car-diotoxicity, the induction of premature se-nescence in cardiomyocytes is a recently recognized mechanism [70]. The age-re-lated alterations in cardiac myocytes in-clude structural and functional changes in mitochondria and lysosomes associat-ed with oxidative stress [71]. The most re-liable marker of cellular senescence is the modification of the telomere-telomerase axis, together with the expression of the cell cycle inhibitors p16INK4a and p53 [71, 72]. Doxorubicin-treated neonatal cardio-myocytes showed significantly increased positive staining for senescence-associated cdk-I expression, decreased cardiac tropo-nin I phosphorylation, decreased telomer-ase activity, and promyelocytic leukemia-related p53 acetylation [70].
Doxorubicin-induced UPS activity leads to cardiac toxicity
The ubiquitin-proteasome systemThe UPS is a proteolytic system medi-ating important degradation and post-translational modifications of proteins in the cell [73, 74]. The UPS system, which consists of two main processes, ubiqui-tination and proteasome-mediated deg-radation, is important for maintaining
protein function and quality control [30, 73, 74, 75, 76].
Ubiquitination is a process of attach-ing ubiquitin molecules to proteins by means of ATP-dependent enzymatic re-actions involving the ubiquitin-activat-ing enzyme (E1), the ubiquitin-conjugat-ing enzyme (E2), the ubiquitin ligase (E3), and the ubiquitin chain elongation fac-tor (E4) [74, 77]. Ubiquitination of a pro-tein can change its activity or degrade the protein [30, 73, 74, 75]. Polyubiquitinated proteins are degraded predominantly by the 26S proteasome [30, 73, 74, 75]. Pro-teasomes are able to activate the signaling pathway proteins by cleaving the protein into an active form [73, 75]. Degradation and cleavage of proteins can also be per-formed by proteasomes in ubiquitin-inde-pendent manners [78, 79].
Doxorubicin-induced UPS activityA therapeutic dose of doxorubicin acti-vates UPS-mediated proteolysis by acting on both the ubiquitination apparatus and proteasomes [80]. Although a few stud-ies determined that doxorubicin-prote-asome complex formation effectively in-hibits proteasome activity, the majority of studies indicated that doxorubicin induc-es proteasome-mediated degradation of proteins in cardiomyocytes by increasing the expression of ubiquitin E3 ligase and other proteases (. Fig. 1, [74]).
By increasing ubiquitin E3 ligase ex-pression [81, 82], doxorubicin enhanc-es UPS-mediated degradation of essen-tial proteins including structural proteins (e.g., myofibrillar proteins, β-catenin) [83, 84, 85], survival factors (ARC, apoptosis repressor with caspase recruitment do-main, and Bcl2), and transcription fac-tors (e.g., p300) [86]. These degradations can directly cause cardiomyocyte apop-tosis and impair cardiomyocyte function [74]. Doxorubicin can also induce UPS-mediated degradation of IκB, an inhibitor of nuclear transcription factor κB (NFκB; pro-apoptotic in cardiomyocytes) [57, 87].
Doxorubicin activates mitogen-acti-vated protein kinases (MAPKs), p38 and JNK [88, 89], and increases cardiomyo-cyte apoptosis by decreasing the expres-sion levels of anti-apoptotic proteins like Bcl-2 and increasing the expression lev-els of pro-apoptotic proteins like Bax,
cleaved caspase-9, and cleaved caspase-3 [2, 25].
Atrogin-1 is a striated muscle-specif-ic E3 ligase promoting the degradation of muscle proteins [90, 91]. Doxorubicin in-duces atrogin-1 and MuRFs (muscle-spe-cific RING finger proteins), which are as-sociated with myopathic alterations [92, 93]. The atrogin-1 induced by doxorubi-cin can activate MAPK p38 and induce cardiomyocyte atrophy, muscle wasting, and ventricular dilatation [88, 94, 95, 96].
Doxorubicin-induced increases in ROS and mitochondrial-mediated calcium re-lease can increase the amount of mis-fold-ed proteins [80] and activate the nuclear factors of activated T-cell (NFAT) 4 in a calcium/calcineurin-dependent manner and cause cardiomyocyte apoptosis [97]. Doxorubicin causes proteasome-mediat-ed degradation of NFAT-5, which results in cell injury and cell death [98], and a decrease in the taurine transporter gene (TauT), which reduces the ability of car-diomyocytes to absorb taurine (a potent cardioprotective antioxidant amino ac-id) [99].
In summary, a doxorubicin-induced increase in ubiquitin E3 ligases and other proteases can cause myofibrillar loss, de-creased cardioprotective/cardiomyocytes survival factors, increased pro-apoptot-ic factors, and impaired sarcomeric struc-ture. Clinical studies are currently ongoing to evaluate the protective effects of protea-some inhibitors such as bortezomib [100].
Doxorubicin inhibits neuregulin/ErbB signalling
Neuregulins are proteins belonging to the epidermal growth factor (EGF) protein family [101, 102]. There are four neureg-ulin proteins: neuregulin-1 to -4 (NRG1–4). These proteins have a high number of isoforms with different functions resulting from alternative splicing [103].
ErbBs are receptor tyrosine kinases of the epidermal growth factor receptor (EGFR) protein family [104, 105]. Simi-larly, there are four ErbBs: ErbB1/HER1, ErbB2/HER2, ErbB3/HER3, and ErbB4/HER4 [105]. ErbB2 and ErbB4 are ex-pressed in differentiated cardiomyocytes [106]. With the exception of ErbB2, which has no ligand, other ErbBs are activated
300 | Herz 4 · 2011
Main topic/CME

by ligand binding [105, 107]. ErbBs can then homodimerize or heterodimerize to activate downstream signalling pathways [108], such as Akt pathways [109, 110]. NRG1 is known to bind ErbB3 and ErbB4 [111]. In cardiomyocytes, NRG1 binds to ErbB4, causing ErbB4 to homodimerize or heterodimerize with ErbB2 [112] so as to have cardioprotective effects via the Akt and Erk pathways [109, 110].
Studies have shown that dilated cardio-myopathy can develop in ErbB2-deficient conditional mutant mice [113, 114], as well as ErbB1/ErbB2-tyrosine kinase inhibitor (PKI166)-mediated myofibrillar structural damage and decreased p-Erk1/2 [115, 116].
Clinically, trastuzumab [117, 118, 119, 120] (or Herceptin [99]; antibodies against ErbB2), which is used to treat patients with breast cancer and positive receptor status, can directly cause cardiotoxicity and par-ticularly enhance the toxicity in patients with prior anthracycline exposure.
Doxorubicin significantly reduces the protein expression of NRG1 and ErbB4 in the heart, but not ErbB2 [105]. In the het-erozygous knockout of NRG1 mice, doxo-rubicin induced more severe cardiac inju-ry, higher mortality, and worse left ven-tricular dysfunction compared to wild type mice [121]. Recombinant NRG1 sig-nificantly improved survival and cardiac function in doxorubicin-treated mice by inhibiting proteasome-mediated degra-dation of troponin proteins and reducing caspase activation via ErbB2-PI3K-Akt pathways [110, 115, 121, 122]. New thera-peutic strategies such as NRG1 adminis-tration can protect the heart from doxo-rubicin cardiotoxicity.
Doxorubicin inhibits cardiac cell renewal and vasculogenesis
Despite wide acceptance that the heart is a terminally differentiated organ, limited repair after injury or stress through bone marrow progenitor cells (BMPCs) or car-diac progenitor cells (CPCs) has been re-ported [123, 124]. However, a few studies have shown an intrinsic relationship be-tween doxorubicin exposure and CPC dynamics [125, 126]. In one study [107], doxorubicin decreased the viability of clo-nogenic c-kit positive CPCs in vitro with reduced CPC viability. In vivo studies
show significant increases in CPC apop-tosis and a decrease in functional CPCs in the myocardium, along with a signifi-cant decrease in the rate of myocyte for-mation evidenced by a dramatic reduc-tion in the numbers of doxorubicin-treat-ed CPCs expressing Ki67. Using a cumula-tive dose that did not induce acute cardio-toxicity in young mice [126], the mice de-veloped abnormal vascular architecture in the adult hearts, with less branching and decreased capillary density. When sub-jected to myocardial infarction, the mice developed rapid heart failure, which cor-related with a failure to increase capillary density in the injured area and fewer pro-genitor cells in the infarct border zone. Doxorubicin treatment reduced prolifera-tion and differentiation of progenitor cells into cardiac lineage cells [126].
Doxorubicin can also block endotheli-al progenitor cell-induced repair [127] and induce cell death in human umbilical vein endothelial cells [128]. Although infusion of cardiac progenitor cells after anthracy-cline exposure provides some degree of cardiac rescue [81], this approach may al-so prevent some of the beneficial effects of these chemotherapeutics on their targeted malignancies.
Management of doxorubicin-induced cardiotoxicity
Risk evaluation
Given the lethal nature of doxorubicin cardiotoxicity, the risk evaluation of pa-tients prior to chemotherapy and close monitoring of patients post treatment are necessary [129, 130]. Risk factors include prior mediastinal irradiation, concurrent cyclophosphamide therapy, advanced age, and pre-existing heart disease. Children tend to develop delayed clinical symptoms with their cardiac toxicity in that doxoru-bicin-induced cardiomyopathy impairs cardiac remodeling with thinning of ven-tricular walls, with no fall in ejection frac-tion for some time [131].
Monitoring
Initial management with doxorubicin re-quires the observation of patients and
periodic monitoring of complete blood counts, liver function tests, ECG, B-type natriuretic peptide and troponins (I and T), echocardiogram, as well as radionu-clide left ventricular ejection fraction. In adults, a 10% decline in LVEF to below the lower limit of normal or an absolute LVEF of 45%, or a 20% decline in LVEF at any level is indicative of deterioration in car-diac function. In children, deterioration in cardiac function during or after the com-pletion of doxorubicin therapy is indicat-ed by a drop in fractional shortening (FS) or a decrease in LV wall thickness.
Treatment
In the case of established doxorubicin-in-duced CHF, treatment to relieve symp-toms includes diuretics, low salt diet, as well as β-blockers [132, 133, 134] and an-giotensin converting enzyme (ACE) in-hibitors [130, 135, 136] titrated to improve the functional status of the patient.
Prevention
To date, strategies using pharmaceutical agents to prevent or reduce doxorubicin cardiotoxicity have been sought and test-ed in many animal models and some clin-ical studies. The only compound current-ly approved to protect against doxorubi-cin cardiotoxicity is dexrazoxane [137]. Of note, dexrazoxane appears to provide long-term cardioprotection without com-promising oncological efficacy in doxo-rubicin-treated children [138]. The un-derlying mechanisms include iron chela-tion [11, 14, 139], protecting the heart from acute doxorubicin-induced QT prolonga-tion via I(Ks) [13], and upregulation of Akt and Erk phosphorylation pathways [14].
In addition to the treatment of estab-lished CHF, ACE inhibitors [140] and β-blockers [141] have been shown to have preventive effects against doxorubicin-in-duced cardiotoxicity in randomized clin-ical trials. Pretreatment with ACE inhib-itors improves doxorubicin-induced car-diomyopathy by preserving mitochon-drial function [135]. Both zofenopril and lisinopril prevented electrocardiographic alteration induced by chronic doxorubi-cin administration in the rat [136]. Carve-dilol partially inhibited the doxorubicin-
301Herz 4 · 2011 |

induced activation of caspase-3 to prevent doxorubicin cardiotoxicity [132]. Since mechanisms of doxorubicin cardiotoxic-ity also involve over-activated UPS, using a proteasome inhibitor like bortezomib, which is on clinical trial, may be anoth-er potential approach to prevent doxoru-bicin cardiotoxicity [100].
Other promising pharmaceutical ap-proaches have been tested in animal or in vitro studies, potentially opening the way to clinical prevention of doxorubicin car-diomyopathy in the future [18, 129, 137, 142]. Antioxidants, such as N-acetylcys-teine [143], probucol [144], taurine [145], and vitamin E [146], have been found to be protective in laboratory models. Phen-ylbutyrate, a histone deacetylase inhibi-tor, protects against Adriamycin-induced cardiac injury by increasing cardiac man-ganese superoxide dismutase (MnSOD) protein and activity [147]. Zinc inhib-its the doxorubicin-activated calcineurin signal transduction pathway in H9c2 em-bryonic rat cardiac cells [148]. Vinca al-kaloid vincristine is able to prevent doxo-rubicin-induced cardiomyocyte death by activating the prosurvival signal Akt and diminishing cytochrome C release [149]. Neuregulin/ErbB is known for its indis-pensable role during cardiac and neuro-nal development [109]. Cardiac inactiva-tion of Neu/ErbB leads to cardiomyop-athy [109, 114] and is one of the mecha-nisms of cardiotoxicity caused by anthra-cyclines and/or the tyrosine kinase inhib-itor trastuzumab [105, 122]. The introduc-tion of NRG1 [122], or selective-targeting miR-146a [105], provides a protective ef-fect in doxorubicin cardiotoxicity. Adi-ponectin protects against doxorubicin-induced cardiomyopathy by anti-apop-totic effects through AMPK upregula-tion [150]. Overexpression of p300 pro-tects cardiac myocytes from doxorubi-cin-induced apoptosis by increasing the cardiac level of bcl-2 and mdm-2 [30]. L-carnitine reduces doxorubicin-induced apoptosis through a prostacyclin-medi-ated pathway in neonatal rat cardiomyo-cytes [151]. Nuclear calcium/calmodulin-dependent protein kinase IIdeltaB (CaM-KIIdeltaB) is required for GATA-4-medi-ated co-activation and binding to the Bcl-2 promoter. Overexpression of CaMKI-IdeltaB in primary cardiac cells inhibits
doxorubicin-mediated apoptosis and pre-vents the loss of the anti-apoptotic protein Bcl-2, suggesting that selective targeting of CaMKII in the nuclear compartment might represent a strategy to regulate car-diac apoptosis and reduce doxorubicin-mediated cardiotoxicity [152]. Phospho-diesterase-5 (PDE-5) inhibitors, including sildenafil, have been shown to have a pow-erful cardioprotective effect against inju-ries under a variety of experimental con-ditions, including ischemia/reperfusion injury, myocardial infarction, and doxo-rubicin -induced cardiomyopathy [153].
Conclusions and future directions
Although doxorubicin remains one of the most effective chemotherapy agents, its cardiotoxicity is becoming a major is-sue as more patients survive their cancer and chemotherapy. Multiple mechanisms have been implicated (. Fig. 1), of which the “ROS and iron” hypothesis still domi-nates. Subsequent gene expression chang-es and activation of the ubiquitin-protea-some system, cell death, as well as innate immunity activation all contribute to tox-icity. The intrinsic cardiac repair mecha-nism is also impaired as doxorubicin may inhibit local cell renewal and bone mar-row cell mobilization. Clinically, no sin-gle drug has hitherto been able to com-pletely prevent doxorubicin cardiotoxici-ty. More clinical studies are needed to val-idate its essential mechanisms and devel-op preventive strategies.
Corresponding addressP.P. LiuDivision of Cardiology, Heart and Stroke/Richard Lewar Centre of Excellence, University Health Network, University of Toronto, Toronto General Hospital200 Elizabeth Street, M5G 2C4 [email protected]
Acknowledgements. Supported in part by grants from the Heart and Stroke Foundation (HSF) of Ontario and the Canadian Institutes of Health Research (CIHR).
Conflict of interest. The authors declare that there are no conflicts of interest.
References
1. Pommier Y, Leo E, Zhang H, Marchand C (2010) DNA topoisomerases and their poisoning by anticancer and antibacterial drugs. Chem Biol 17:421–433
2. Chatterjee K, Zhang J, Honbo N, Karliner JS (2010) Doxo-rubicin cardiomyopathy. Cardiology 115:155–162
3. Robert J, Gianni L (1993) Pharmacokinetics and metabo-lism of anthracyclines. Cancer Surv 17:219–252
4. Cartoni A, Menna P, Salvatorelli E et al (2004) Oxidative degradation of cardiotoxic anticancer anthracyclines to phthalic acids. Novel function or ferrylmyoglobin. J Biol Chem 279:5088–5099
5. Minotti G, Menna P, Salvatorelli E et al (2004) Anthracy-clines: molecular advances and pharmacologic develop-ments in antitumor activity and cardiotoxicity. Pharma-col Rev 56:185–229
6. Shin M, Matsunaga H, Fujiwara K (2010) Differences in accumulation of anthracyclines daunorubicin, doxorubi-cin and epirubicin in rat tissues revealed by immunocy-tochemistry. Histochem Cell Biol 133:677–682
7. Menna P, Salvatorelli E, Minotti G (2010) Anthracycline degradation in cardiomyocytes: a journey to oxidative survival. Chem Res Toxicol 23:6–10
8. Menna P, Salvatorelli E, Minotti G (2007) Doxorubicin degradation in cardiomyocytes. J Pharmacol Exp Ther 322:408–419
9. Yi X, Bekeredjian R, De Filippis NJ et al (2006) Transcrip-tional analysis of doxorubicin-induced cardiotoxicity. Am J Physiol Heart Circ Physiol 290:H1098–H1102
10. Umlauf J, Horky M (2002) Molecular biology of doxoru-bicin-induced cardiomyopathy. Exp Clin Cardiol 7:35–39
11. Xu X, Persson HL, Richardson DR (2005) Molecular phar-macology of the interaction of anthracyclines with iron. Mol Pharmacol 68:261–271
12. Minotti G, Ronchi R, Salvatorelli E et al (2001) Doxoru-bicin irreversibly inactivates iron regulatory proteins 1 and 2 in cardiomyocytes: evidence for distinct metabolic pathways and implications for iron-mediated cardiotox-icity of antitumor therapy. Cancer Res 61:8422–8428
13. Ducroq J, Moha ou Maati H, Guilbot S et al (2010) Dexra-zoxane protects the heart from acute doxorubicin-in-duced QT prolongation: a key role for I(Ks). Br J Pharma-col 159:93–101
14. Xiang P, Deng HY, Li K et al (2009) Dexrazoxane protects against doxorubicin-induced cardiomyopathy: upreg-ulation of Akt and Erk phosphorylation in a rat model. Cancer Chemother Pharmacol 63:343–349
15. Miranda CJ, Makui H, Soares RJ et al (2003) Hfe deficien-cy increases susceptibility to cardiotoxicity and exacer-bates changes in iron metabolism induced by doxorubi-cin. Blood 102:2574–2580
16. Menna P, Salvatorelli E, Minotti G (2008) Cardiotoxicity of antitumor drugs. Chem Res Toxicol 21:978–989
17. Simunek T, Sterba M, Popelova O et al (2009) Anthracy-cline-induced cardiotoxicity: overview of studies exam-ining the roles of oxidative stress and free cellular iron. Pharmacol Rep 61:154–171
18. Zhang YW, Shi J, Li YJ, Wei L (2009) Cardiomyocyte death in doxorubicin-induced cardiotoxicity. Arch Immunol Ther Exp (Warsz) 57:435–445
19. Lebrecht D, Walker UA (2007) Role of mtDNA lesions in an-thracycline cardiotoxicity. Cardiovasc Toxicol 7:108–113
20. L’Ecuyer T, Sanjeev S, Thomas R et al (2006) DNA damage is an early event in doxorubicin-induced cardiac myocyte death. Am J Physiol Heart Circ Physiol 291:H1273–H1280
21. Solem LE, Heller LJ, Wallace KB (1996) Dose-dependent increase in sensitivity to calcium-induced mitochondrial dysfunction and cardiomyocyte cell injury by doxorubi-cin. J Mol Cell Cardiol 28:1023–1032
22. Wallace KB (2003) Doxorubicin-induced cardiac mitochon-drionopathy. J Pharmacol Toxicol Methods 93:105–115
23. Wallace KB (2007) Adriamycin-induced interference with cardiac mitochondrial calcium homeostasis. Cardiovasc Toxicol 7:101–107
24. Zhou S, Starkov A, Froberg MK et al (2001) Cumulative and irreversible cardiac mitochondrial dysfunction in-duced by doxorubicin. Cancer Res 61:771–777
302 | Herz 4 · 2011
Main topic/CME

25. Liu X, Chua CC, Gao J et al (2004) Pifithrin-alpha pro-tects against doxorubicin-induced apoptosis and acute cardiotoxicity in mice. Am J Physiol Heart Circ Physiol 286:H933–H939
26. Liu J, Mao W, Ding B, Liang CS (2008) ERKs/p53 sig-nal transduction pathway is involved in doxorubicin-in-duced apoptosis in H9c2 cells and cardiomyocytes. Am J Physiol Heart Circ Physiol 295:H1956–H1965
27. Aries A, Paradis P, Lefebvre C et al (2004) Essential role of GATA-4 in cell survival and drug-induced cardiotoxicity. Proc Natl Acad Sci U S A 101:6975–6980
28. Kim Y, Ma AG, Kitta K et al (2003) Anthracycline-induced suppression of GATA-4 transcription factor: implica-tion in the regulation of cardiac myocyte apoptosis. Mol Pharmacol 63:368–377
29. Park AM, Nagase H, Liu L et al (2010) Mechanism of an-thracycline-mediated down-regulation of GATA4 in the heart. Cardiovasc Res 90:97–104
30. Kawamura T, Hasegawa K, Morimoto T et al (2004) Ex-pression of p300 protects cardiac myocytes from apop-tosis in vivo. Biochem Biophys Res Commun 315:733–738
31. Poizat C, Puri PL, Bai Y, Kedes L (2005) Phosphorylation-dependent degradation of p300 by doxorubicin-activat-ed p38 mitogen-activated protein kinase in cardiac cells. Mol Cell Biol 25:2673–2687
32. Vo N, Goodman RH (2001) CREB-binding protein and p300 in transcriptional regulation. J Biol Chem 276:13505–13508
33. Yuan ZM, Huang Y, Ishiko T et al (1999) Function for p300 and not CBP in the apoptotic response to DNA damage. Oncogene 18:5714–5717
34. Kobayashi S, Volden P, Timm D et al (2010) Transcription factor GATA4 inhibits doxorubicin-induced autophagy and cardiomyocyte death. J Biol Chem 285:793–804
35. Terman A, Brunk UT (2005) Autophagy in cardiac myo-cyte homeostasis, aging, and pathology. Cardiovasc Res 68:355–365
36. Terman A, Kurz T, Gustafsson B, Brunk UT (2008) The in-volvement of lysosomes in myocardial aging and dis-ease. Curr Cardiol Rev 4:107–115
37. Hoyer-Hansen M, Bastholm L, Szyniarowski P et al (2007) Control of macroautophagy by calcium, calmodulin-de-pendent kinase kinase-beta, and Bcl-2. Mol Cell 25:193–205
38. Hoyer-Hansen M, Jaattela M (2007) Connecting endoplas-mic reticulum stress to autophagy by unfolded protein re-sponse and calcium. Cell Death Differ 14:1576–1582
39. Kumar D, Lou H, Singal PK (2002) Oxidative stress and apoptosis in heart dysfunction. Herz 27:662–668
40. Janeway CA Jr, Medzhitov R (2002) Innate immune rec-ognition. Annu Rev Immunol 20:197–216
41. Ehrke MJ, Ryoyama K, Cohen SA (1984) Cellular basis for adriamycin-induced augmentation of cell-mediated cy-totoxicity in culture. Cancer Res 44:2497–2504
42. Maccubbin DL, Wing KR, Mace KF et al (1992) Adriamy-cin-induced modulation of host defenses in tumor-bear-ing mice. Cancer Res 52:3572–3576
43. Haskill JS (1981) Adriamycin-activated macrophages as tumor growth inhibitors. Cancer Res 41:3852–3856
44. Methe H, Kim JO, Kofler S et al (2005) Statins decrease toll-like receptor 4 expression and downstream signal-ing in human CD14+ monocytes. Arterioscler Thromb Vasc Biol 25:1439–1445
45. Mann DL, Topkara VK, Evans S, Barger PM (2010) Innate immunity in the adult mammalian heart: for whom the cell tolls. Trans Am Clin Climatol Assoc 121:34–50; dis-cussion 50–31
46. Apetoh L, Ghiringhelli F, Tesniere A et al (2007) Toll-like receptor 4-dependent contribution of the immune sys-tem to anticancer chemotherapy and radiotherapy. Nat Med 13:1050–1059
47. Apetoh L, Tesniere A, Ghiringhelli F et al (2008) Molec-ular interactions between dying tumor cells and the in-nate immune system determine the efficacy of conven-tional anticancer therapies. Cancer Res 68:4026–4030
48. Kast RE, Foley KF, Focosi D (2007) Doxorubicin cardiomy-opathy via TLR-2 stimulation: potential for prevention using current anti-retroviral inhibitors such as ritonavir and nelfinavir. Hematol Oncol 25:96–97
49. Methe H, Kim JO, Kofler S et al (2005) Expansion of circulat-ing Toll-like receptor 4-positive monocytes in patients with acute coronary syndrome. Circulation 111:2654–2661
50. Nozaki N, Shishido T, Takeishi Y, Kubota I (2004) Modula-tion of doxorubicin-induced cardiac dysfunction in toll-like receptor-2-knockout mice. Circulation 110:2869–2874
51. Riad A, Bien S, Gratz M et al (2008) Toll-like receptor-4 deficiency attenuates doxorubicin-induced cardiomyop-athy in mice. Eur J Heart Fail 10:233–243
52. Sakata Y, Dong JW, Vallejo JG et al (2007) Toll-like recep-tor 2 modulates left ventricular function following isch-emia-reperfusion injury. Am J Physiol Heart Circ Physiol 292:H503–H509
53. Shishido T, Nozaki N, Yamaguchi S et al (2003) Toll-like re-ceptor-2 modulates ventricular remodeling after myo-cardial infarction. Circulation 108:2905–2910
54. Fairweather D, Frisancho-Kiss S, Rose NR (2005) Viruses as adjuvants for autoimmunity: evidence from Coxsacki-evirus-induced myocarditis. Rev Med Virol 15:17–27
55. Zhu J, Zhang J, Xiang D et al (2010) Recombinant human interleukin-1 receptor antagonist protects mice against acute doxorubicin-induced cardiotoxicity. Eur J Pharma-col 643:247–253
56. Frantz S, Kelly RA, Bourcier T (2001) Role of TLR-2 in the activation of nuclear factor kappaB by oxidative stress in cardiac myocytes. J Biol Chem 276:5197–5203
57. Wang S, Kotamraju S, Konorev E et al (2002) Activation of nuclear factor-kappaB during doxorubicin-induced apop-tosis in endothelial cells and myocytes is pro-apoptotic: the role of hydrogen peroxide. Biochem J 367:729–740
58. Timmers L, Sluijter JP, Keulen JK van et al (2008) Toll-like receptor 4 mediates maladaptive left ventricular remod-eling and impairs cardiac function after myocardial in-farction. Circ Res 102:257–264
59. Dunne A, O’Neill LA (2003) The interleukin-1 receptor/toll-like receptor superfamily: signal transduction during inflammation and host defense. Sci STKE 2003:re3
60. Berthiaume JM, Wallace KB (2007) Persistent alterations to the gene expression profile of the heart subsequent to chronic Doxorubicin treatment. Cardiovasc Toxicol 7:178–191
61. Herman EH, Lipshultz SE, Rifai N et al (1998) Use of car-diac troponin T levels as an indicator of doxorubicin-in-duced cardiotoxicity. Cancer Res 58:195–197
62. Saadane N, Alpert L, Chalifour LE (1999) TAFII250, egr-1, and D-type cyclin expression in mice and neonatal rat cardiomyocytes treated with doxorubicin. Am J Physiol 276:H803–H814
63. Jeyaseelan R, Poizat C, Baker RK et al (1997) A novel car-diac-restricted target for doxorubicin. CARP, a nucle-ar modulator of gene expression in cardiac progenitor cells and cardiomyocytes. J Biol Chem 272:22800–22808
64. Zordoky BN, Anwar-Mohamed A, Aboutabl ME, El-Kadi AO (2010) Acute doxorubicin cardiotoxicity alters cardiac cytochrome P450 expression and arachidonic acid me-tabolism in rats. Toxicol Appl Pharmacol 242:38–46
65. Sayed-Ahmed MM, Al-Shabanah OA, Hafez MM et al (2010) Inhibition of gene expression of heart fatty acid binding protein and organic cation/carnitine transport-er in doxorubicin cardiomyopathic rat model. Eur J Phar-macol 640:143–149
66. Pointon AV, Walker TM, Phillips KM et al (2010) Doxoru-bicin in vivo rapidly alters expression and translation of myocardial electron transport chain genes, leads to ATP loss and caspase 3 activation. PLoS One 5:e12733
67. Maeda A, Honda M, Kuramochi T, Takabatake T (1998) Doxorubicin cardiotoxicity: diastolic cardiac myocyte dysfunction as a result of impaired calcium handling in isolated cardiac myocytes. Jpn Circ J 62:505–511
68. Jeyaseelan R, Poizat C, Wu HY, Kedes L (1997) Molecular mechanisms of doxorubicin-induced cardiomyopathy. Selective suppression of reiske iron-sulfur protein, ADP/ATP translocase, and phosphofructokinase genes is as-sociated with ATP depletion in rat cardiomyocytes. J Biol Chem 272:5828–5832
69. Arai M, Tomaru K, Takizawa T et al (1998) Sarcoplasmic reticulum genes are selectively down-regulated in car-diomyopathy produced by doxorubicin in rabbits. J Mol Cell Cardiol 30:243–254
70. Maejima Y, Adachi S, Ito H et al (2008) Induction of pre-mature senescence in cardiomyocytes by doxorubicin as a novel mechanism of myocardial damage. Aging Cell 7:125–136
71. Kajstura J, Rota M, Urbanek K et al (2006) The telomere-telomerase axis and the heart. Antioxid Redox Signal 8:2125–2141
72. Bernhard D, Laufer G (2008) The aging cardiomyocyte: a mini-review. Gerontology 54:24–31
73. Wang X, Su H, Ranek MJ (2008) Protein quality control and degradation in cardiomyocytes. J Mol Cell Cardiol 45:11–27
74. Ranek MJ, Wang X (2009) Activation of the ubiquitin-proteasome system in doxorubicin cardiomyopathy. Curr Hypertens Rep 11:389–395
75. Wang X, Robbins J (2006) Heart failure and protein qual-ity control. Circ Res 99:1315–1328
76. Patterson C, Ike C, Willis PWT et al (2007) The bitter end: the ubiquitin-proteasome system and cardiac dysfunc-tion. Circulation 115:1456–1463
77. Tu D, Li W, Ye Y, Brunger AT (2007) Structure and function of the yeast U-box-containing ubiquitin ligase Ufd2p. Proc Natl Acad Sci U S A 104:15599–15606
78. Powell SR (2006) The ubiquitin-proteasome system in cardiac physiology and pathology. Am J Physiol Heart Circ Physiol 291:H1–H19
79. Davies KJ (2001) Degradation of oxidized proteins by the 20S proteasome. Biochimie 83:301–310
80. Liu J, Zheng H, Tang M et al (2008) A therapeutic dose of doxorubicin activates ubiquitin-proteasome system-mediated proteolysis by acting on both the ubiquitina-tion apparatus and proteasome. Am J Physiol Heart Circ Physiol 295:H2541–2550
81. Li YZ, Lu DY, Tan WQ et al (2008) p53 initiates apoptosis by transcriptionally targeting the antiapoptotic protein ARC. Mol Cell Biol 28:564–574
82. Nam YJ, Mani K, Wu L et al (2007) The apoptosis inhibitor ARC undergoes ubiquitin-proteasomal-mediated degra-dation in response to death stimuli: identification of a deg-radation-resistant mutant. J Biol Chem 282:5522–5528
83. Fukuda N, Sasaki D, Ishiwata S, Kurihara S (2001) Length dependence of tension generation in rat skinned cardiac muscle: role of titin in the frank-starling mechanism of the heart. Circulation 104:1639–1645
84. Lim CC, Zuppinger C, Guo X et al (2004) Anthracyclines induce calpain-dependent titin proteolysis and necrosis in cardiomyocytes. J Biol Chem 279:8290–8299
85. Haq S, Michael A, Andreucci M et al (2003) Stabilization of beta-catenin by a wnt-independent mechanism reg-ulates cardiomyocyte growth. Proc Natl Acad Sci U S A 100:4610–4615
86. Poizat C, Sartorelli V, Chung G et al (2000) Proteasome-mediated degradation of the coactivator p300 impairs cardiac transcription. Mol Cell Biol 20:8643–8654
87. Li Q, Sanlioglu S, Li S et al (2001) GPx-1 gene delivery modulates NFkappaB activation following diverse envi-ronmental injuries through a specific subunit of the IKK complex. Antioxid Redox Signal 3:415–432
88. Yamamoto Y, Hoshino Y, Ito T et al (2008) Atrogin-1 ubiq-uitin ligase is upregulated by doxorubicin via p38-MAP kinase in cardiac myocytes. Cardiovasc Res 79:89–96
89. Xie P, Guo S, Fan Y et al (2009) Atrogin-1/MAFbx enhanc-es simulated ischemia/reperfusion-induced apoptosis in cardiomyocytes through degradation of MAPK phos-phatase-1 and sustained JNK activation. J Biol Chem 284:5488–5496
90. Gomes MD, Lecker SH, Jagoe RT et al (2001) Atrogin-1, a muscle-specific F-box protein highly expressed during muscle atrophy. Proc Natl Acad Sci U S A 98:14440–14445
91. Stitt TN, Drujan D, Clarke BA et al (2004) The IGF-1/PI3 K/Akt pathway prevents expression of muscle atrophy-in-duced ubiquitin ligases by inhibiting FOXO transcription factors. Mol Cell 14:395–403
92. Razeghi P, Baskin KK, Sharma S et al (2006) Atrophy, hy-pertrophy, and hypoxemia induce transcriptional reg-ulators of the ubiquitin proteasome system in the rat heart. Biochem Biophys Res Commun 342:361–364
303Herz 4 · 2011 |

93. Razeghi P, Taegtmeyer H (2006) Hypertrophy and atro-phy of the heart: the other side of remodeling. Ann N Y Acad Sci 1080:110–119
94. Li HH, Kedar V, Zhang C et al (2004) Atrogin-1/muscle at-rophy F-box inhibits calcineurin-dependent cardiac hy-pertrophy by participating in an SCF ubiquitin ligase complex. J Clin Invest 114:1058–1071
95. Bodine SC, Latres E, Baumhueter S et al (2001) Identifica-tion of ubiquitin ligases required for skeletal muscle at-rophy. Science 294:1704–1708
96. Murton AJ, Constantin D, Greenhaff PL (2008) The in-volvement of the ubiquitin proteasome system in hu-man skeletal muscle remodelling and atrophy. Biochim Biophys Acta 1782:730–743
97. Kalivendi SV, Konorev EA, Cunningham S et al (2005) Doxorubicin activates nuclear factor of activated T-lym-phocytes and fas ligand transcription: role of mitochon-drial reactive oxygen species and calcium. Biochem J 389:527–539
98. Ito T, Fujio Y, Takahashi K, Azuma J (2007) Degradation of NFAT5, a transcriptional regulator of osmotic stress-relat-ed genes, is a critical event for doxorubicin-induced cyto-toxicity in cardiac myocytes. J Biol Chem 282:1152–1160
99. Ito T, Fujio Y, Schaffer SW, Azuma J (2009) Involvement of transcriptional factor TonEBP in the regulation of the taurine transporter in the cardiomyocyte. Adv Exp Med Biol 643:523–532
100. LoConte NK, Thomas JP, Alberti D et al (2008) A phase I pharmacodynamic trial of bortezomib in combination with doxorubicin in patients with advanced cancer. Can-cer Chemother Pharmacol 63:109–115
101. Burden S, Yarden Y (1997) Neuregulins and their recep-tors: a versatile signaling module in organogenesis and oncogenesis. Neuron 18:847–855
102. Li JY, Wang H, May S et al (2008) Constitutive activa-tion of c-jun N-terminal kinase correlates with histolog-ic grade and EGFR expression in diffuse gliomas. J Neu-rooncol 88:11–17
103. Steinthorsdottir V, Stefansson H, Ghosh S et al (2004) Multiple novel transcription initiation sites for NRG1. Gene 342:97–105
104. Bublil EM, Yarden Y (2007) The EGF receptor family: spearheading a merger of signaling and therapeutics. Curr Opin Cell Biol 19:124–134
105. Horie T, Ono K, Nishi H et al (2010) Acute doxorubicin cardiotoxicity is associated with miR-146a-induced inhi-bition of the neuregulin-ErbB pathway. Cardiovasc Res 87:656–664
106. Zhao YY, Sawyer DR, Baliga RR et al (1998) Neuregulins promote survival and growth of cardiac myocytes. Per-sistence of ErbB2 and ErbB4 expression in neonatal and adult ventricular myocytes. J Biol Chem 273:10261–10269
107. Spector NL, Blackwell KL (2009) Understanding the mechanisms behind trastuzumab therapy for human epidermal growth factor receptor 2-positive breast can-cer. J Clin Oncol 27:5838–5847
108. Garrett TP, McKern NM, Lou M et al (2002) Crystal struc-ture of a truncated epidermal growth factor receptor ex-tracellular domain bound to transforming growth factor alpha. Cell 110:763–773
109. Lemmens K, Doggen K, De Keulenaer GW (2007) Role of neuregulin-1/ErbB signaling in cardiovascular physiolo-gy and disease: implications for therapy of heart failure. Circulation 116:954–960
110. Engelman JA, Zejnullahu K, Mitsudomi T et al (2007) MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science 316:1039–1043
111. Linggi B, Carpenter G (2006) ErbB receptors: new in-sights on mechanisms and biology. Trends Cell Biol 16:649–656
112. Yarden Y, Sliwkowski MX (2001) Untangling the ErbB sig-nalling network. Nat Rev Mol Cell Biol 2:127–137
113. Ozcelik C, Erdmann B, Pilz B et al (2002) Conditional mu-tation of the ErbB2 (HER2) receptor in cardiomyocytes leads to dilated cardiomyopathy. Proc Natl Acad Sci U S A 99:8880–8885
114. Crone SA, Zhao YY, Fan L et al (2002) ErbB2 is essential in the prevention of dilated cardiomyopathy. Nat Med 8:459–465
115. Sawyer DB, Zuppinger C, Miller TA et al (2002) Modu-lation of anthracycline-induced myofibrillar disarray in rat ventricular myocytes by neuregulin-1beta and anti-erbB2: potential mechanism for trastuzumab-induced cardiotoxicity. Circulation 105:1551–1554
116. Pentassuglia L, Graf M, Lane H et al (2009) Inhibition of ErbB2 by receptor tyrosine kinase inhibitors causes myo-fibrillar structural damage without cell death in adult rat cardiomyocytes. Exp Cell Res 315:1302–1312
117. Slamon DJ, Leyland-Jones B, Shak S et al (2001) Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 344:783–792
118. Christodoulou C, Kostopoulos I, Kalofonos HP et al (2009) Trastuzumab combined with pegylated liposo-mal doxorubicin in patients with metastatic breast can-cer. phase II Study of the Hellenic Cooperative Oncology Group (HeCOG) with biomarker evaluation. the Interna-tional Society for Cellular 76:275–285
119. Rayson D, Richel D, Chia S et al (2008) Anthracycline-trastuzumab regimens for HER2/neu-overexpressing breast cancer: current experience and future strategies. Ann Oncol 19:1530–1539
120. Ewer MS, Vooletich MT, Durand JB et al (2005) Reversibil-ity of trastuzumab-related cardiotoxicity: new insights based on clinical course and response to medical treat-ment. J Clin Oncol 23:7820–7826
121. Liu FF, Stone JR, Schuldt AJ et al (2005) Heterozygous knockout of neuregulin-1 gene in mice exacerbates doxorubicin-induced heart failure. Am J Physiol Heart Circ Physiol 289:H660–H666
122. Bian Y, Sun M, Silver M et al (2009) Neuregulin-1 attenu-ated doxorubicin-induced decrease in cardiac troponins. Am J Physiol Heart Circ Physiol 297:H1974–H1983
123. Hosoda T, Kajstura J, Leri A, Anversa P (2010) Mecha-nisms of myocardial regeneration. Circ J 74:13–17
124. Di Nardo P, Forte G, Ahluwalia A, Minieri M (2010) Car-diac progenitor cells: potency and control. J Cell Physiol 224:590–600
125. De Angelis A, Piegari E, Cappetta D et al (2010) Anthra-cycline cardiomyopathy is mediated by depletion of the cardiac stem cell pool and is rescued by restoration of progenitor cell function. Circulation 121:276–292
126. Huang C, Zhang X, Ramil JM et al (2010) Juvenile expo-sure to anthracyclines impairs cardiac progenitor cell function and vascularization resulting in greater suscep-tibility to stress-induced myocardial injury in adult mice. Circulation 121:675–683
127. Yasuda K, Park HC, Ratliff B et al (2010) Adriamycin ne-phropathy: a failure of endothelial progenitor cell-in-duced repair. Am J Pathol 176:1685–1695
128. Yin D, Li C, Kao RL et al (2004) Angiopoietin-1 inhibits doxorubicin-induced human umbilical vein endotheli-al cell death by modulating fas expression and via the PI3 K/Akt pathway. Endothelium 11:247–252
129. Ewer MS, Ewer SM (2010) Cardiotoxicity of anticancer treatments: what the cardiologist needs to know. Nat Rev Cardiol 7:564–575
130. Takemura G, Fujiwara H (2007) Doxorubicin-induced car-diomyopathy from the cardiotoxic mechanisms to man-agement. Prog Cardiovasc Dis 49:330–352
131. Lipshultz SE, Alvarez JA, Scully RE (2008) Anthracycline associated cardiotoxicity in survivors of childhood can-cer. Heart 94:525–533
132. Spallarossa P, Garibaldi S, Altieri P et al (2004) Carvedilol prevents doxorubicin-induced free radical release and apoptosis in cardiomyocytes in vitro. J Mol Cell Cardiol 37:837–846
133. Malcom J, Arnold O, Howlett JG et al (2008) Canadian Cardiovascular Society Consensus Conference guide-lines on heart failure–2008 update: best practices for the transition of care of heart failure patients, and the recog-nition, investigation and treatment of cardiomyopathies. Can J Cardiol 24:21–40
134. Shaddy RE, Olsen SL, Bristow MR et al (1995) Efficacy and safety of metoprolol in the treatment of doxorubicin-in-duced cardiomyopathy in pediatric patients. Am Heart J 129:197–199
135. Hiona A, Lee AS, Nagendran J et al (2010) Pretreatment with angiotensin-converting enzyme inhibitor improves doxorubicin-induced cardiomyopathy via preservation of mitochondrial function. J Thorac Cardiovasc Surg
136. Sacco G, Mario B, Lopez G et al (2009) ACE inhibition and protection from doxorubicin-induced cardiotoxicity in the rat. Vascul Pharmacol 50:166–170
137. Hensley ML, Hagerty KL, Kewalramani T et al (2009) American Society of Clinical Oncology 2008 clinical prac-tice guideline update: use of chemotherapy and radia-tion therapy protectants. J Clin Oncol 27:127–145
138. Lipshultz SE, Scully RE, Lipsitz SR et al (2010) Assess-ment of dexrazoxane as a cardioprotectant in doxoru-bicin-treated children with high-risk acute lymphoblas-tic leukaemia: long-term follow-up of a prospective, ran-domised, multicentre trial. Lancet Oncol 11:950–961
139. Lebrecht D, Geist A, Ketelsen UP et al (2007) Dexrazox-ane prevents doxorubicin-induced long-term cardiotox-icity and protects myocardial mitochondria from genetic and functional lesions in rats. Br J Pharmacol 151:771–778
140. Cardinale D, Colombo A, Sandri MT et al (2006) Preven-tion of high-dose chemotherapy-induced cardiotoxicity in high-risk patients by angiotensin-converting enzyme inhibition. Circulation 114:2474–2481
141. Kalay N, Basar E, Ozdogru I et al (2006) Protective effects of carvedilol against anthracycline-induced cardiomyop-athy. J Am Coll Cardiol 48:2258–2262
142. Sawyer DB, Peng X, Chen B et al (2010) Mechanisms of anthracycline cardiac injury: can we identify strategies for cardioprotection? Prog Cardiovasc Dis 53:105–113
143. Shi R, Huang CC, Aronstam RS et al (2009) N-acetylcyste-ine amide decreases oxidative stress but not cell death induced by doxorubicin in H9c2 cardiomyocytes. BMC Pharmacol 9:7
144. Lou H, Danelisen I, Singal PK (2005) Involvement of mitogen-activated protein kinases in adriamycin-in-duced cardiomyopathy. Am J Physiol Heart Circ Physiol 288:H1925–H1930
145. Ito T, Muraoka S, Takahashi K et al (2009) Beneficial effect of taurine treatment against doxorubicin-induced car-diotoxicity in mice. Adv Exp Med Biol 643:65–74
146. Berthiaume JM, Oliveira PJ, Fariss MW, Wallace KB (2005) Dietary vitamin E decreases doxorubicin-induced oxida-tive stress without preventing mitochondrial dysfunc-tion. Cardiovasc Toxicol 5:257–267
147. Daosukho C, Chen Y, Noel T et al (2007) Phenylbutyr-ate, a histone deacetylase inhibitor, protects against Adriamycin-induced cardiac injury. Free Radic Biol Med 42:1818–1825
148. Merten KE, Jiang Y, Kang YJ (2007) Zinc inhibits doxoru-bicin-activated calcineurin signal transduction pathway in H9c2 embryonic rat cardiac cells. Exp Biol Med (May-wood) 232:682–689
149. Chatterjee K, Zhang J, Tao R et al (2008) Vincristine atten-uates doxorubicin cardiotoxicity. Biochem Biophys Res Commun 373:555–560
150. Konishi M, Haraguchi G, Ohigashi H et al (2011) Adipo-nectin protects against doxorubicin-induced cardiomy-opathy by anti-apoptotic effects through AMPK up-reg-ulation. Cardiovasc Res 89:309–319
151. Chao HH, Liu JC, Hong HJ et al (2011) L-carnitine reduces doxorubicin-induced apoptosis through a prostacyclin-mediated pathway in neonatal rat cardiomyocytes. Int J Cardiol 146:145–152
152. Little GH, Saw A, Bai Y et al (2009) Critical role of nucle-ar calcium/calmodulin-dependent protein kinase IIdel-taB in cardiomyocyte survival in cardiomyopathy. J Biol Chem 284:24857–24868
153. Koka S, Das A, Zhu SG et al (2010) Long-acting phospho-diesterase-5 inhibitor tadalafil attenuates doxorubicin-in-duced cardiomyopathy without interfering with chemo-therapeutic effect. J Pharmacol Exp Ther 334:1023–1030
304 | Herz 4 · 2011
Main topic/CME