Embed Size (px)
Citation preview
![Page 1: Mecillinam in patients on haemodialysis [letter]](https://reader042.pdfslide.net/reader042/viewer/2022020612/575086b11a28abf34fc45cb6/html5/page/1.jpg)
Br. J. clin. Pharmac. (1980), 10 LETTERS TO THE EDITORS 177
activity and erythrocyte folate was a weak one andcould be due to two distinct actions of phenytoin andphenobarbitone rather than an effect of folate onNa+K+-ATPase or vice versa.
Measurement of erythrocyte ATPase activitiescannot be considered as a satisfactory guide to dosageof anticonvulsant drugs in relation to the control ofseizures in patients with grand mal epilepsy becauseof the almost complete inhibition ofNa+K' -ATPaseeven at subtherapeutic drug concentrations.
A.K. SCOTT, J.C. GILBERT1 & J. WEBSTER
Department of Therapeutics and ClinicalPharmacology, University of Aberdeen, AB9 2ZD and'Section of Pharmacology, Heriot-Watt University,Edinburgh EHI 2HJ
Received January 11, 1980
References
GILBERT, J.C. & WYLLIE, M.G. (1975). Synaptic vesiclemagnesium-adenosine triphosphatase as a possible site ofaction of anticonvulsant drugs. Br. J. Pharmac., 55,252P.
GILBERT, J.C. & WYLLIE, M.G. (1976). Effects ofanticonvulsant and convulsant drugs on the ATPaseactivities of synaptosomes and their components. Br. J.Pharmac., 56, 49-57.
LOWRY, O.H., ROSEBROUGH, N., FARR, A.L. & RANDALL,
R.J. (1951). Protein measurement with the Folin phenolreagent. J. biol. Chem., 193, 265-275.
MAXWELL, J.D., HUNTER, J., STEWART, D.A., ARDEMAN,S. & WILLIAMS, R. (1972). Folate deficiency afteranticonvulsant drugs: an effect of hepatic enzymeinduction? Br. med. J., 1, 297-299.
SCHWOCH, G. & PASSOW, H. (1973). Preparation andproperties of human erythrocyte ghosts. Mol. Cell.Biochem., 2, 197-218.
MECILLINAM IN PATIENTS ON HAEMODIALYSIS
Because of its low toxicity particularly towards thekidneys, mecillinam is a suitable antibiotic with whichto treat patients with renal impairment. However,haemodialysis may reduce serum and tissueconcentrations of antibiotics and other drugs to sub-therapeutic levels. The effect varies within the'penicillin' group. Ampicillin (Jusko, Lewis &Schmitt, 1973), penicillin (Schreiner & Teehan, 1972:Bryan & Stone, 1975), and carbenicillin (Hoffman,Cestero & Bullock, 1970) are removed byhaemodialysis while the blood levels of isoxazolylpenicillins (oxacillin, cloxacillin, dicloxacillin) are notsignificantly altered (Nauta, Maltie & Goslings, 1973:Nauta & Maltie, 1975).The present trial was undertaken to determine
whether haemodialysis significantly increased theclearances of mecillinam, the first of the amidino-penicillins in patients with end stage renal diseasemaintained on regular intermittent haemodialysis.
Details of the ten patients who agreed toparticipate in the trial are given in Table 1. All hadbeen on twice or thrice weekly haemodialysis forbetween 2 months and 6 years, and all had creatinineclearances of less than 0.2 1/h (3 ml/min). Three(patients 5, 8 and 9) were anuric and the remaindereach passed less than 1 litre of urine per 24 h. Dialysiswas carried out for between 4 and 6 h using single
pass dialysis and Cordis Dow 1.3 square metrehollow fibre artificial kidneys, except for one patient(no. 3) who used a Hemaflow 1.3 square metre. Ablood flow rate of 9 1/h (150 ml/min) was maintainedduring dialysis in all cases.
:~10EE
0EE
Cn 2
1 2 3 4 5
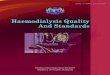
Time after dose (h)Figure 1 Consolidated concentration-time curve frompatients on dialysis after 200 mg mecillinam i.v.
![Page 2: Mecillinam in patients on haemodialysis [letter]](https://reader042.pdfslide.net/reader042/viewer/2022020612/575086b11a28abf34fc45cb6/html5/page/2.jpg)
178 LETTERS TO THE EDITORS
Table 1 Details of patients and data obtained while on dialysis
Age WeightPatient (years) (kg)
DialysateCause of flow rate
renalfailure (I/h)
Creatininelevel
pre-dialysis(Pmol/l)
Eliminationstage half-
life (h)
Area underthe curve Clearance(mg 1- 1 h) (I/h)
1 78 50 Post-operativerenal failure
2 46 43.5 Polycystickidneys
3 41 42 Chronic pyelo-nephritis
4 63 72 Polycystickidneys
Horseshoe5 27 53 kidney pyelo-
nephritis6 64 46.5 Polycystic
kidneys7 53 58 Chronic glome-
rula disease8 42 50 Nephrectomy
hypertension9 27 44 Glomerulo-
nephritis10 58 63 Post-operative
renal failure
30
30
36
294 2.06 18.95 10.50
947 1.90 30.37 6.54
591
30 1002
36 1070
36
36
36
36
1.13 19.57 10.20
2.33 22.92 8.70
1.88 34.03 5.88
734 2.02
899
756
37.75 5.28
1.97 18.79 10.62
1.63 28.06 7.14
834 1.57 28.73 6.96
30
A single intravenous dose of 200 mg mecillinamwas given at the start of dialysis and blood sampleswere taken approximately 15 and 40 min afterinjection and thereafter at hourly intervals. Sampleswere stored on ice until separated. Three of the tenpatients also received a single intravenous dose of200 mg mecillinam on a day when dialysis was nottaking place and samples were taken and stored asabove.
Samples were assayed on the day of collectionusing the agar plate diffusion method (Williams,Andrews, Mitchard & Kendall, 1976) with the Leo
1.83 22.68 8.82
HA strain of E. coli. Standards, prepared inphosphate buffered saline pH 7.0 from mecillinamhydrochloride dihydrate powder on the day on whichthey were used, gave a linear response when thediameters of zones of inhibition were plotted semi-logarithmically against concentration over the range1 jg/ml to 30 tg/ml (regression coefficient (r) 0.994,standard error of estimate (SEE) 0.39). Assays wereperformed in triplicate and the plates were incubatedat 37°C overnight. The results are expressed asmilligrams of mecillinam per litre of serum.The serum concentrations in specimens taken from
Patient 4
A
1 2 3 4 5
Patient 8
1 2 3 4 5
Time after dose (h)
Patient 10
1 2
1 2 3 4 5
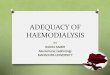
Figure 2 Concentration-time curves on patients when on dialysis (0-*) and when not on dialysis (A-A) after200 mg mecillinam i.v.
0,EEX 10
cJ0)EE2 2a)en)
Br. J. clin. Pharmac. (1980), 10
![Page 3: Mecillinam in patients on haemodialysis [letter]](https://reader042.pdfslide.net/reader042/viewer/2022020612/575086b11a28abf34fc45cb6/html5/page/3.jpg)
Br. J. clin. Pharmac. (1980), 10 LETTERS TO THE EDITORS 179
Table 2 Data on patients obtained while not on dialysis
Creatinine Area under % increaseWeight level Half-life the curve Clearance in clearance
Patient (kg) (1imol/t) (h) (mg 1- 1 h) (I/h) during dialysis
4 69 789 3.05 42.01 4.76 838 52 956 4.22 65.06 3.07 132
10 60 3.01 45.79 4.36 102
patients on haemodialysis plotted against time afterinjection, are presented in Figure 1. Each point is themean of the concentrations in ten patients and thebars represent the range.The curve was biphasic; the mean ,B or elimination
half-life was 1.83 h (s.d. 0.33) and mean clearance8.06 1/h (s.d. 1.97). Values for individual half-lives,areas under the serum concentration-time curves(AUC), and clearances are shown in Table 1. Thetotal body clearance of mecillinam was calculated bydividing the intravenous dose by the area under theserum conentration-time curve (AUC) (Greenblatt& Koch-Weser, 1975).
In the three patients who received mecillinam on anon-dialysis day results were plotted together withthose obtained during dialysis (Figure 2). The mean /Bphase half-life was 3.43 h (s.d. 0.69) and the meanclearance 4.06 1/h (s.d. 0.88), (Table 2). The averageincrease of clearance of mecillinam during dialysiswas 106%.The biphasic distribution curves obtained during
haemodialysis correspond with those of Mitchard,Andrews & Kendall (1977) who demonstrated a mean,B phase half-life of 0.814 (±0.16) h in six normalsubjects given 200 mg of mecillinam intravenously.Roholt (1977) using the same dose studied ninenormal subjects and calculated an average AUCvalue of 9.9+1.5 h mg I-', from which we haveinterpreted a clearance of 20.2 1/h. In our patientswhen unaided by dialysis the clearance of creatinine( < 0.2 1/h) was significantly less than that formecillinam ( - 4 1/h), and it is clear that mechanismsother than renal filtration are involved in theelimination of the drug. Urinary mecillinam levelswere not measured however and it was not possible todetermine whether active renal secretion took place.Our findings demonstrate that the serum half-life isprolonged and the clearance of mecillinam reduced in
end stage renal disease, and that some removal of thedrug takes place during dialysis. This was to beexpected for a drug with low protein binding andsmall volume of distribution similar to ampicillin andbenzylpenicillin; in contrast the isoxazolyl penicillinsare not removed by dialysis due to high proteinbinding ( - 90%). However, the rate of removal issuch that, where standard doses are given, levelsshould remain in the therapeutic range during theprocedure and alterations in the regime areunnecessary either during or after the period ofdialysis. Where higher levels are to be maintained,e.g. with partially resistant organisms, a booster doseshould be given at end of dialysis and intervalsbetween doses prolonged to avoid possibleneurotoxicity.While it should be noted that our
recommendations are based upon single doseintravenous studies, Ekberg, Denneberg, Larsson &Juhlin (1978) using the oral preparationpivmecillinam came to similar conclusions in dialysispatients undergoing treatment for urinary tractinfections.
We acknowledge gratefully the technical assistanceof Mrs J. Gawler, AIMLSO, and the co-operation ofthe staff of the Renal Unit of the Royal Devon &Exeter Hospital. Leo Laboratories kindly providedcomputer facilities.
KATHRYN BAILEY, J.G. CRUICKSHANK, P.G.BISSON & B.L. RADFORDRoyal Devon and Exeter Hospital, Wonford, Exeter,Devon
Received January 24, 1980
References
BRYAN, C.S. & STONE, W.J. (1975). 'Comparably massive'penicillin G therapy in renal failure. Ann. intern. Med.,82, 189-195.
EKBERG, M., DENNEBERG, T., LARSSON, S. & JUHLIN, I.(1978). Pharmacokinetic and therapeutic studies on
pivmecillinam in patients with normal and impairedrenal function. Scand. J. inf. Dis., 10, 127-133.
GREENBLATT, D.J. & KOCH-WESER, J. (1975). Clinicalpharmacokinetics. New Engi. J. Med., 293, 702-705.
HOFFMANN, T.A., CESTERO, R. & BULLOCK, W.E. (1970).
![Page 4: Mecillinam in patients on haemodialysis [letter]](https://reader042.pdfslide.net/reader042/viewer/2022020612/575086b11a28abf34fc45cb6/html5/page/4.jpg)
180 LETTERS TO THE EDITORS Br. J. clin. Pharmac. (1980), 10
Pharmacodynamics of carbenicillin in hepatic and renalfailure. Ann. intern. Med., 73, 173-178.
JUSKO, W.J., LEWIS, G.P. & SCHMITT, G.W. (1973).Ampicillin and hetacillin pharmacokinetics in normaland anephric subjects. Clin. Pharmac. Ther., 14, 90-99.
MITCHARD, M., ANDREWS, J., KENDALL, M.J. & WISE, R.(1977). Mecillinam levels following intravenousinjection: a comparison with pivmecillinam. J.Antimicrob. Chemother., 3, Suppl. B, 83-88.
NAUTA, E. & MALTIE, H. (1975). Pharmacokinetics offlucloxacillin in healthy subjects on chronic intermittenthaemodialysis. Br. J. clin. Pharmac., 2, 111-121.
NAUTA, E., MALTIE, H. & GOSLINGS, W. (1973).
Pharmacokinetics of cloxacillin in patients on chronicdialysis. Chemotherapy, 19, 261-271.
ROHOLT, K. (1977). Pharmacokinetic studies withmecillinam and pivmecillinam. J. Antimicrob.Chemother., 3, Suppl. B, 71-81.
SCHREINER, G.E. & TEEHAN, B.P. (1972). Dialysis ofpoisons and drugs. Trans. Am. Soc. Art. Org., 18,563-580.
WILLIAMS, J.D., ANDREWS, J., MITCHARD, M. &KENDALL, M.J. (1976). Bacteriology andpharmacokinetics of the new amidino penicillin-mecillinam. J. Antimicrob. Chemother., 2, 61-69.
NALOXONE MODULATES THEPERCEPTION OF ITCH IN MAN
Naloxone, a pure opiate antagonist, can alter thesubjective assessment of pain, thus providingevidence that endorphins may modulate pain in man(Lasagna, 1965; Buchsbaum, Davis & Bunney, 1977;Levine, Gordon, Jones & Fields, 1978; Levine,Gordon & Fields, 1978a; Levine, Gordon & Fields,1979). The hyperalgesia caused by naloxone inpatients with dental pain appears to be due entirely tothe abolition of the placebo response (Levine et al.,1978a). The present study was designed to assess theeffect of naloxone on the related sensation, itch. Bothitch and pain are transmitted to the dorsal horns ofthe spinal cord by small diameter (c) fibres(Zotterman, 1939), and are probably integrated at acommon site at each spinal segment (Graham,Goodell & Wolff, 1951). Furthermore, there isevidence that pain may be modulated by anenkephalin system in the interneurones of thesubstantia gelatinosa in each dorsal horn (Hokfelt,Ljungdahl, Terenius, Elde & Nilsson, 1977; Jessell &Iversen, 1977). In these experiments the effect ofnaloxone on nocturnal itch was studied in patientswith cholestatic liver disease who had severeprotracted itching.Twenty patients with cholestatic liver disease were
studied (age range 29 to 71 years). Thirteen werefemale. The diagnosis was established by com-patible biochemical tests, liver biopsy and/orcholangiography. They had been itching for between 1month and 17 years (mean 3.2 years). The itch wasconstantly present although six patients volunteeredthat it was worse at night. Patients with mild itchingwere excluded from the trial. Three patients, who hadreceived cholestyramine continuously for between 4months and 3 years, and four patients who tookregular night sedation (diazepam or nitrazepam),continued to receive therapy. D-penicillamine
treatment was continued in six patients with primarybiliary cirrhosis. The study was approved by thehospital ethical practices committee and informedconsent was obtained from each patient. The patientswere told they would receive an agent that reduceditch in a proportion of patients (placebo) and a drugwhose effect was being evaluated (naloxone). Arandomized double-blind placebo controlled designwas used. The code was not broken during anyexperiment. Drugs were administered intravenouslyat 18.00 h in equal volumes (5 ml) of either naloxone(2 mg) or saline (0.9% w/v). The injections wereindistinguishable colourless liquids and produced noimmediate effect that could be identified. All thepatients completed the study. The experiments wereperformed between May and September 1979.Nocturnal itching was assessed on 4 consecutivenights. Night 1 and night 3 were control nights. Onnight 2 and night 4 patients received either placebo ornaloxone. The last eight patients also received aplacebo on night 1 to access the reproducibility ofthe placebo response. Itching was assessed at 9.00 hthe following morning by the visual analogue scalevalidated for the assessment of pain (Joyce, Zutshi,Hrubes & Mason, 1975; Scott & Huskisson, 1976).This was a 10 cm horizontal line on a white cardmarked at the left end 'none' and at the right end'unbearable'. The patient assessed the previousnight's itching by marking a point along this line. Thevisual analogue scales were later estimated to within 1mm. Patients could not refer to earlier assessments.The results were expressed as the change in itch scorebetween the treatment night and the previous night.Nocturnal scratch was estimated in the first 12patients on nights 2, 3 and 4. Electronic movementmeters were attached to each arm on retiring to sleepand removed on waking. In previous experiments this