Embed Size (px)
Citation preview

POSTGRAD. MED. J. (1965), 41, 418
IRON DEFICIENCY ANAEMIA IN ADULTS:PREVALENCE AND PREVENTION
A. JACOBS, M.D., M.C. Path.,Senior Lecturer in Hcematology.
G. S. KILPATRICK, M.D., M.R.C.P. (Ed.),Senior Lecturer in Medicine.
J. L. WITHEY, M.B., B.S., M.C. Path.,Lecturer in Hcematology.
Welsh National School of Medicine, Cardiff.
IRON deficiency anaemia is a common conditionin the United Kingdom. We propose to reviewthe evidence for this, to say something of thecause and to outline the possible ways by whichsuch anaemia might be prevented.
Prevalence StudiesBetween 1930 and 1940 Davidson and his
colleagues studied the prevalence of anaemiain Aberdeen. The subjects of this early workwere not random samples of the populationbut volunteers from the poorest classes in thecommunity. It is difficult to compare theirresults with those of later workers because ofselection and differences in methods ofhaemoglobinometry and in definition of anaemiabut they did demonstrate that iron deficiencyanaemia was common in adult women in thepoorer classes in North East Scotland(Davidson, Fullerton, Howie, Croll, Orr andGodden, 1933; Davidson and Fullerton, 1935).When anemia was defined as a hemoglobin ofless than 85% (Haldane) 16% of adolescentgirls and no less than 45% of adult womenwere found to be anaemic. Anaemia was rarein men and usually associated with organicdisease. Thus age and sex were clearly definedas important etiological factors. Davidson andFullerton (1938) concluded that poor dietaryintake of iron, together with the demands ofreproductive life, led to the high prevalenceof iron deficiency anaemia in the women theyinvestigated. A later study in Edinburgh gavesimilar results (Davidson, Donaldson, Lindsayand McSorley, 1943).
In 1943 the Medical Research Councilcarried out a detailed study of haemoglobinlevels in Great Britain (Medical ResearchCouncil, 1945). It was not possible to examinea true random sample of the population buttesting was planned to cover as many socialgroups as possible at all ages. Sixteen thousand
individuals were tested and detailed question-naires were completed providing data on health,diet, occupation, marital state and socialcondition. Haemoglobin levels as a whole wererather higher than the previous Aberdeenfigures, which may have been due to thedifferent methods of selection. It was concludedthat haemoglobin levels were low in a consider-able proportion of subjects, especially inchildren below the age of five years, pregnantwomen and persons at the lower economiclevels, and that this could be prevented byraising the dietary intake of iron.Apart from some studies in adolescents and
the elderly, few general surveys were done afterthe war until Kilpatrick and Hardisty (1961)studied a random sample of an industrialcommunity, the Rhondda Fach in South Wales.Their population included 300 miners andex-miners, 300 non-miners, aged between 35-64years, and 200 postmenopausal women between55-64 years. They found the mean haemoglobinconcentration of the men to be 14.9 g./100 ml.and that of the women to be 13.3 g./100 ml.Three per cent of the men, 18 in number, werefound to have a haemoglobin of 12.5 g./100 ml.or less, and of these 14 had a mean corpuscularhaemoglobin concentration (MCHC) of 31% orless. Fourteen per cent of the women, 25 innumber, had a haemoglobin concentration of12.0 g./100 ml. or less and 22 of them had anMCHC of 31% or below. Iron deficiency wasthus by far the commonest cause of anaemia inthis community. Although there was no clearfall in hmemoglobin concentration with age therewas a progressive fall of 'MCHC with age.Kilpatrick (1961) studied a sample of peopleover the age of 15 years living in Wensleydale,an agricultural area in the northern part ofYorkshire. The results of examining 182 menand 230 women in this district are summarisedin Table 1. The criteria of anaemia are thoseused in the Rhondda survey.
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from

July, 1965 JACOBS, KILPATRICK and WITHEY: Iron Deficiency Anaemia 419
TABLE 1PREVALENCE OF ANAEMIA IN WENSLEYDALE (182 men;
230 women)Incidence of Anaemia
Age Men Women15-24 3.4% 28.0%25-34 0.0 % 25.0 %35-44 2.9% 24.0%45-54 8.3% 12.0%55-64 8.0% 12.5%65-74 20.0% 21.0%75 25.0% 21.0%
Fry (1961) reported anaemia cases in hisgeneral practice in South London seen over afive-year period. His patients were investigatedonly if they presented clinical signs of anaemia.He found an annual incidence of 17.5 perthousand, but had he examined a sample ofhis practice this figure would undoubtedly havebeen higher. He confirmed that iron deficiencyanaemia was the commonest type.Of surveys of selected age-groups, there have
been several to determine the prevalence ofanaemia in young men. Leonard (1954) usingthe copper sulphate method for estimatinghaemoglobin concentration examined 4,221recruits aged 18 to 20 entering the Royal AirForce. Fifty were found to be undoubtedlyananmic as they had a haemoglobin concen-tration of less than 12.0 g./100 ml. Heexamined these 50 men thoroughly and foundthat 49 had iron deficiency anemia. In two ofthese men the anaemia was presumed to be dueto bleeding from the gastro-intestinal tract butin the remaining 47, no obvious cause for theanaemia was discovered and he regarded themas having idiopathic iron deficiency. Brumfitt(1960) examined 2,000 Royal Army MedicalCorps recruits aged 17 to 21 years and found1.1% to have a haemoglobin concentration ofless than 12.0 g./100 ml. He compared theserecruits with 1,000 trained men of an airbornedivision and in these found only 0.1% to havea hemoglobin concentration of less than 12.0g./100 ml. Elwood, Withey and Kilpatrick(1964), in a study of 505 boys and 621 girlsaged 14 years in 9 secondary modern schoolsin Cardiff, found that 12 boys (2.4%) and 25girls (4.0%) had haemoglobin concentrations of12.5 g./100 ml. or less and 12.0 g./100 ml. orless respectively. In children of this age inCardiff anemia was thus not a serious problem.So far as the elderly are concerned Hobsonand Blackburn (1953) took a 1 in 30 randomsample from the food office register inSheffield of men and women who had reachedpensionable age (65 for men and 60 for women).
Only those living alone or with their spouseswere selected. 'l1ere were 177 men aged be-tween 66 and 85 and 246 women aged between61 and 87; the mean haemoglobi concentra-tions of these two groups were 14.4 g./100 ml.and 13.8 g./100 ml. respectively. They con-sidered any person with a haemoglobin below11.7 g./100 ml. to be anaemic and they found9 men (5.1%) and 16 women (6.5%) who metthis criterion. Of these, 8 men and 13 womenwere iron deficient. If 12.3 g./100 ml. were tobe taken as the criterion then 23 men and 37women were anaemic. Parsons, Withey andKilpatrick (1965) examined a random sampleof elderly people in Swansea consisting of 208individuals over the age of 65. Ten men (12%)had a haemoglobin concentration less than 12.5g./100 ml. and 18 women (15.7%) less than12.0 g./100 ml. In 8 men and 13 women theMCHC was less than 31% indicating irondeficiency.Semmence examined 256 people in generalpractice (101 men and 155 women); of these,5 men (5%) and 20 women (13%) had
haemoglobin concentrations below 12.0 g./100ml. In all 5 men a cause was found; 2 hadcarcinoma, 1 leukaemia, 1 pernicious anaemiaand 1 bleeding duodenal ulcer. In the women apoor diet was considered to be an importantfactor. Women living alone had significantlylower haemoglobin concentrations than thosenot living alone, but this did not apply to themen. Hobson and Blackburn (1953), on theother hand, found the haemoglobin concen-tration to be lower in men living alone.
Iron MetabolismIn the normal non-anaemic adult about 3 g.of iron is present in the body as circulatinghaemoglobin. About 1 g. is present either ashaemosiderin or ferritin and this functions asan iron store which can be mobilised for haemsynthesis if necessary. Smaller amounts of ironare found in compounds serving specialisedfunctions such as myoglobin or tissue enzymes.The newborn baby derives about 300-400 mg.of iron from its mother by transfer across theplacenta, most of this taking place in the laterweeks of pregnancy. All the additional ironnecessary for the immense demands ofhaemopoiesis in infancy and childhood, togetherwith that necessary to build up adequatereserves for adult life, must be derived fromthe diet and it seems clear that the amountobtained in this way is not always adequate.Even when adolescence is reached withenough iron to maintain a normal haemoglobin
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
level, storage iron may be depleted. Themaintenance of a normal haemoglobin concen-tration in adult life depends on the adequacy ofthe total body iron pool and this in turndepends on a favourable balance between intakeand loss from the pool.Hypochromic anaemia in this country is
almost invariably due to iron deficiency. It ischaracterised by a reduction in the number ofcirculating red cells together with a reduction intheir haemoglobin content. In addition to ahaemoglobin concentration below normal theMCHC is decreased and the blood film showsthe presence of pale mis-shapen red cells. Fry(1961) found that the red cells in 84% ofanaemic men and 95% of anaemic women inhis Beckenham practice were hypochromic. Inthe Rhondda Fach survey carried out by Kil-patrick and Hardisty (1961) 18 anaemic menand 25 women were found of whom 14 menand 22 women had an MCHC of 31% or less.Serum iron concentration is low in iron-defic-iency anaemia and there is an increased amountof iron binding protein. The bone marrow isusually devoid of haemosiderin and thedeveloping red cells are poorly formed.The early stages of iron deficiency may not
show all these phenomena. Reduction of serumiron levels and a low saturation of the iron-binding protein may be found before thehaemoglobin level has fallen below acceptednormal limits and reduced marrow haemosiderinmay also be a feature of pre-anaemic irondeficiency. It has been suggested that thissideropenic state may, itself, give rise tosymptoms which can be corrected by theadministration of iron. The relationship of thesymptoms of anaemia to haemoglobin level hasnever been fully investigated and this we arenow attempting to do in a controlled mannerby means of a questionnaire administeredbefore and after treatment with iron. Reducedactivity of several iron-containing enzymes inthe tissues has been demonstrated in iron-deficient animals by Beutler and his co-workersand it appears that this may occur beforeanaemia is manifest (Beutler, 1964). The onlysimilar observation in man is a deficiency ofcytochrome oxidase activity in the buccalmucosa of some iron-deficient patients (Jacobs,1961). Whether the symptoms of the sidero-penic state are related to enzyme deficiencies isdebatable. Beutler, Larsh and Gurney (1960)carried out a well controlled double-blind trialof iron therapy in non-anaemic women sufferingfrom chronic fatigue and found that iron had asignificant effect in relieving symptoms in those
with evidence of sideropenia, such as a lowserum iron concentration or a reduction inmarrow haemosiderin.Anaemia develops when the amount of iron
available for haemoglobin in the bone marrowis inadequate and this only occurs when thestorage iron of the body has been depleted.There is some information on the iron balanceof normal subjects but a great deal more data isrequired. Excretion of non-haemoglobin ironfrom the body is small and loss from urine,faeces and skin has been estimated at about0.5 to 1 mg. per day (Moore, 1964). In womeniron loss through menstruation varies con-siderably between individuals but is about 10to 40 mg. per month. Iron intake depends onthe amount in the diet and the proportionabsorbed. The National Food Survey Com-mittee (1963) showed that the mean daily ironintake in persons from different types of house-hold varied from 11 to 18 mg. per day andindividual variations must presumably bemuch greater than this. The proportion of foodiron absorbed is 5 to 15% to normal subjects,the mean being 6.5% (Moore, 1964). Thesefigures indicate that about 0.5 to 2.7 mg. ironper day are being added to the body pool while0.5 to 1 mg. per day in men and 0.8 to 2.3 mg.per day in women is being lost. These approxi-mations only apply to normal persons in whomthere is no special demand for iron, eitherphysiological or pathological.Although theoretical considerations indicate
that the common iron-deficiency anaemia inadults must be due to inadequacy of ironstores resulting from a negative iron balancethe precise aetiology remains obscure. It isusually assumed that blood loss is an importantfactor causing iron depletion but the loss isoften difficult to measure or even to detect.Bannerman, Beveridge and Witts (1964) have,shown that even when occult bleeding fromthe gastrointestinal tract is detected it iscommon for no cause to be discovered. Fry(1961) could find no obvious reason for irondeficiency in 53% of men with anaemia andin 87% of anaemic women in his generalpractice. Only in 22% of anaemic men and,in 7% of anaemic women was there a clearsource of blood loss such as peptic ulcerationor carcinoma. Poor diet, excessive menstruationand repeated pregnancies are often suggestedas causes of iron deficiency in women butalthough these factors are undoubtedly import-ant precise data are not usually obtainablein individual cases.
420 July, 1965
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from

July, 1965 JACOBS, KILPATRICK and WITHEY: Iron Deficiency Anaemia 421
Information about iron in the diet is usuallyderived from questionnaire surveys rather thanby actual analyses, and the validity of suchsurveys has been criticised (Lambert, 1964).There is no certainty that the diets recordedby the National Food Survey (1963) in thiscountry represent the normal household dietwhen a survey is not being conducted; it iswell recognised that people are unreliable whenquestioned about their dietary habits. Despitethese qualifications some interesting factsemerge from the survey. The average con-sumption of iron per person per day in theUnited Kingdom is 14.2 mg. and this showslittle variation between geographical regions.Dietary iron intake is highest in childlesshouseholds but in households with childrenthe average intake falls as the number ofchildren increases. In families with four ormore children the average daily intake is only11.2 mg. This is found in all social classes.A number of factors influence the amount
of iron absorbed from the food. Studies offood containing radioactive iron show adifferent degree of availability from differentfoodstuffs (Moore, 1964). Absorption isdecreased when the meal has a large bulkor when phytates or phosphates are present inlarge quantities, and achlorhydria may have asignificant effect in reducing absorption (Gold-berg, lochhead and Daga. 1963). The propor-tion of iron absorbed from the intestine isincreased considerably in subjects with irondeficiency anaemia by a homeostatic mechanismthe nature of which is not fully understood.The evaluation of iron loss from the body
by menstruation is of use only if precisemeasurements are made. The subjectiveassessment of menstrual loss by women isnotoriously unreliable even when questioningis extended to the number of pads used,presence of clots etc. A recent survey ofsanitary towels (Consumer Association, 1964)showed that different brands vary in theirpower to absorb blood from 0.05 fl. oz.(1.4 ml.) to 2.5 fl. oz. (71 ml.) per towel.Thus estimation of the number used is oflittle value. In our hospital, patients referredto the gynaecology department because ofmenorrhagia have been found to lose as littleas 25 ml. of blood during a 'heavy' periodwhile some patients with severe iron deficiencyanaemia have lost up to 200 ml. of bloodduring a 'normal' period. Direct measurementof menstrual blood loss in 100 normal womenbv Barer and Fowler (1936) gave a range of6.5-179 ml. per period '(mean loss 50 ml.).
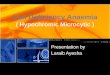
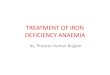
DAILY IRON REQUIREMENTS.50 16mg 21 27mg 33mg
*40 I 19 Ij2nuj30nuj
.30
20
IO'
blood 20 40 60 80 100 120 140 160 180Mge 8.6 17.2 258 34.4 43 51.6 602 68.8 77A
Monthl M.nstal Blood Loss
FIG. 1.-Menstrual blood loss in 151 normal women.Iron requirements show the amount needed inthe diet to balance losses.
Twenty one subjects who were members ofa hospital staff gave a range of 10-55 ml.(mean 25 ml.) (Baldwin, Whalley and Pritchard,1961). Our own measurements on 17 healthymembers of the hospital staff aged 21 to 40years gave a range of 4-87 ml. per period(mean 35 ml.).We have studied a number of women with
iron deficiency anaemia and excessive menstruallosses of as much as 600 ml. per periodhave been found in some of them. We havefound no case where menorrhagia has beenmaterially improved by treatment with iron,contrary to the findings of Taymor, Sturgisand Yahia, (1964) who suggest that menorrhagiamay be due specifically to iron deficiency.When menorrhagia with no obvious gynaeco-logical cause persists long-term treatment withiron may be necessary to maintain iron balanceand in extreme cases hysterectomy may beunavoidable.
Figure 1 shows the amount of blood lostduring menstruation by 151 normal women.The data have been derived from Barer andFowler, (1936); Millis, (1951); Baldwin andothers, (1961); and Jacobs (unpublished). Thefigures for daily iron requirements assume aloss of iron from the body of 1 mg. per day,apart from menstruation, and 10% iron absorp-tion from the diet. Thirty-eight per cent ofthese women have a menstrual loss of 40 ml.or more which is equivalent to 0.6 mg. ironper day. Most of them will develop iron de-ficiency with or without anaemia because only asmall number will have the required dietary ironintake of over 16 mg. per day. Some auto-
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from

422 POSTGRADUATE MEDICAL JOURNAL July, 1965
TABLE 2IRON BALANCE OF NORMAL PREGNANCY
Debit (mg.) Credit (mg.)To Foetus 300-500Placenta + cord 34-170Blood loss at delivery 100-2506 months lactation 100-18015 months amenorrhoea 135-585
Total 534-1100mg 135-585 mg.Net Loss 0-965 mg.
matic compensation will occur because anincreasing proportion of the dietary iron willbe absorbed from the gut as iron deficiencydevelops. Nevertheless, iron balance in thesewomen will be precarious and they will tendto be in a state of latent or overt iron deficiency.The intermittent removal of iron from the
body through the process of pregnancy tendsto reduce body stores. This is illustrated inTable 2. The iron conserved through amenor-rhoea does not usually compensate for theamount lost to the foetus while placentalblood together with bleeding during labouralso take their toll. The effect of this iscumulative with repeated pregnancies.
In an individual case of iron deficiencyanaemia it may not be clear, even after detailedinvestigations, why a patient is in negative ironbalance but it seems likely that both in-adequate intake and excessive loss areimportant factors. Unless a specific bleedinglesion is found there is little that can be doneto prevent the marginal,neeative balance foundso commonly in women. The rational measurewould be to increase iron intake by an appro-priate amount, but this would not, of course,be the same for each individual and could onlybe determined by a tedious process of trialand error in each case. A more practicableaporoach to the treatment of "idiopathic" irondeficiency in women is to provide all suchwomen with a regular supplement of iron thesize of which should enable most of them tomaintain a positive iron balance. A total dailyiron intake of 24 mg. would bring this aboutin all women whose menstrual loss is less than100 ml. per month (Fig. 1) and this could beachieved by a supplement of 10-15 mg. irondaily.Treatment
In men, iron deficiency anaemia is commonlyassociated with serious organic disease andtreatment with iron should not be started untila diagnosis has been made.
It is probably impracticable to submit allanamic women to detailed investigations; todo so would be to overload existing pathology
laboratories and radiology departments. Specificenquiries should be made regarding such thingsas weight loss, dyspepsia, colour of stools,aspirin consumption and blood loss other thanmenstruation. Information about menstrualblood loss should be criticially assessed witha view to detecting gynecological abnormalityrather than evaluating the amount of bloodlost. If the amount of blood lost seems grosslyexcessive then further investigation of this willbe necessary. In the great majority of casesthere will be no clue to abnormal blood lossand the anaemia should be treated with an oraliron preparation. The effectiveness of the treat-ment should be judged by periodic haemoglobinestimations and a final haemoglobin estimationshould be carried out four months afterthe cessation of treatment so that a relapsecan be detected.Those women who have an inadequate
response to oral iron or a relapse after fourmonths should be investigated more thoroughly.Occult intestinal bleeding, in particular, shouldbe looked for (Bedford and Wollner, 1958).The patient should not be discharged frommedical care until a satisfactory reason for theiron deficiency has been discovered and, ifpossible, treated.
PreventionThe occurrence of low haemoglobin levels in
the community presumably indicates a form ofpreventable ill-health. The form of this illhealth is, however, difficult to define. Thesymptoms of anaemia are vague and do notcorrelate well with hemoglobin levels. Thereis evidence that women with normal haemoglo-bin levels may benefit from an increased ironintake (Beutler and others, 1960). If this is sogeneral prophylactic measures would benefit agreater part of the population than merelythose with overt anaemia. In Cardiff an attemptis being made to measure the physical dis-ability caused by iron deficiency anaemia andto discover whether a similar disability occursin non-anaemic women.
There are a number of possible ways inwhich the incidence of iron deficiency couldbe reduced. Probably none is fully utilised atthe present time. The administration of med-icinal iron to especially vulnerable groups isone such measure. Most authorities agree thatbecause iron-deficiency anemia is so common'in pregnancy iron should be given to pregnantwomen as a routine procedure. This shouldbe carried out with the same enthusiasm asurine examinations, or blood pressure measure-
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from

JACOBS, KILPATRICK and WITHEY: Iron Deficiency Anaemia
ments, and continued throughout pregnancy.Iron should be given to all pregnant women,whether they appear anaemic or not. The satis-factory results of this have been well demonst-rated by Kerr and Davidson (1958). Otherspecial subjects likely to develop iron-deficiencyanaemia should also be given regular supple-ments of iron; patients who have undergonepartial gastrectomy for example form a part-icularly vulnerable group.The highest incidence of anaemia is found
in women during the reproductive period oflife. Studies of 14-year-old schoolgirls in Cardiffhave shown that there is very little anemia atthis age (Elwood and others, 1964) but sub-sequent work indicates that anaemia becomesa problem during adolescence. A prospectivestudy is being carried out to find the value ofregular iron supplements in preventing theanaemia of adolescence. A cohort of 14-year-old schoolgirls are all receiving a daily tabletand will be followed up for 5 years. Theyhave been randomly allocated to three groups.The first group receive 30 mg. iron daily, thesecond 10 mg. iron daily and the third aplacebo. Co-operation in actually taking thetablets is checked by administration of thecorrect number of tablets, by random homevisiting and urine testing for a riboflavintracer present in all tablets. The incidence ofanemia in the three groups will be measuredduring the investigation and at the end of fiveyears.A more satisfactory way of administering
prophylactic iron to a large population is byadding it, in adequate amounts, to a universallyconsumed food stuff. The most suitable foodfor this purpose is bread and existing legisla-tion does in fact specify that white flour mustcontain 1.65 mg. iron per 100 g. Flour isnormally fortified with ferrum redactum tomeet this legal requirement. An investigationcarried out by Elwood (1963) indicates that notonly does ferrum redactum appear to be poorlyabsorbed from bread but increasing the normalamount nearly forty-fold has little effect on itsefficiency. Present methods of fortification ofbread with iron seem to be of doubtful valueand further studies of iron-enriched bread arebeing carried out to determine what compoundsare most satisfactorily absorbed from the in-testine after being subjected to the bakingprocess.
If prevention of anemia is not always pos-sible the early recognition of cases is necessaryto prevent chronic ill-health. Clinical examina-
tion of patients is not enough to exclude thediagnosis of anaemia. There is a poor correla-tion between the doctors assessment of pallorand the actual hemoglobin level (McAlpine,Douglas and Robb, 1957). Many patients withchronic iron deficiency are called neurotic andtreated as such. The only satisfactory screen-ing test for anaemia is the haemoglobin estima-tion and the prevalence of anaemia at presentis so high that as large a population as possibleshould be screened. There are several meansof arranging this. Haemoglobin estimations couldbe carried out by the general practitionerwhen patients are seen in the surgery.In the past this has meant either thepossession of expensive equipment requiringcalibration and constant checking or theuse of cheaper but inaccurate devices forhaemoglobinometry. The present availability ofa simple battery-operated apparatus for accu-rate haemoglobin estimations using a drop ofwhole blood means that accurate results canbe obtained in any surroundings and without alaboratory. Failing this many pathology depart-ments have an "open door" policy with regardto blood tests requested by general practitioners.This should be fully utilised wherever it isavailable.There is evidence that mass screening for
anaemia reveals a substantial amount of un-suspected disease. Clinics for this purpose, orcombined with other screening procedures suchas urine testing, cervical cytology or audiometry,could well be established by local authorities.It is almost certain that a higher proportion ofpositive findings would emerge from such aclinic than in mass miniature radiographyunits at present. Multi-screening clinics includ-ing haemoglobin estimations have beenemployed recently in Middlesex, (Maddison,1962), land Rotherham, (Donaldson, 1965). Inthe former the clinic remained open all thetime but in the latter a concentrated publicitycampaign resulted in a large number of peoplebeing tested during one week.
It is important that case finding by haemo-globin estimation does not lead to theindiscriminate therapeutic use of iron withoutthe proper diagnosis and follow-up that hasalready been mentioned. The minimum evid-ence on which to base the diagnosis of irondeficiency anemia includes either a typicalblood film or a low MCHC. Other forms ofanaemia requiring urgent treatment, such aspernicious anamia, will be missed if the pre-liminary screening test is also used, by itself,for diagnosis.
July, 1965 423copyright.
on October 1, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.41.477.418 on 1 July 1965. Dow
nloaded from

424 POSTGRADUATE MEDICAL JOURNAL July, 1965
SummaryIron deficiency anaemia is common in Great
Britain. It is especially common in youngwomen and in most cases is due to an imbalancebetween iron intake and iron loss rather thanto any specific pathological lesion. The pre-valence of anemia could be reduced byprophylactic measures and active case finding.We are indebted to Professor H. Scarborough for
his valuable criticism.
REFERENCES
BALDWIN, R.M., WHALLEY, P. J., and PITCHARD, J. A.(1961): Measurements of Menstrual Blood Loss,Amer. J. Obstet. Gynec., 81, 739.
BANNER4MAN. R. M., BEVERIDGE, B. R., and WITrs,L. J. (1964): Anaemia Associated with UnexplainedOccult Blood Loss, Brit. med. J., i, 1417.
BARER, A. P., and FOWLER, W. M. (1936): The BloodLoss during Normal Menstruation, Amer. J. Obstet.Gynec., 31, 979.
BEDFORD, P. D., and WOLLNER, L. (1958): OccultIntestinal Bleeding as a Cause of Anaemia inElderly People, Lancet, i, 1144.
BEUTLER, E., LARSH, S. E., and GURNEY, C. W.(1960): Iron Therapy in Chronically FatiguedNonanaemic Women: a Double-blind Study, Ann.intern. Med., 52, 378.
BEUTLER, E. (1964): In 'Iron Metabolism'-An Inter-national Symposium. Berlin: Springer-Verlag.
BRUMFITr, W. (1960): Primary Iron-DeficiencyAnaemia in Young Men, Quart. J. Med, 29, 1.
CONSUMER ASSOCIATION (1964): Which, March Issue.DAVIDSON, L. S. P., FULLERTON, H. W., HOWIE, J. W.,
CROLL, J. M., ORR, J. B., and GODDEN, W. (1933):Observations on Nutrition in Relation to Anaemia,Brit. med. J., i, 685.
DAVIDSON, L. S. P., and FULLERTON, H. W. (1935)Nutritional Iron-deficiency Anaemia, Brit. med. J.,ii, 195.
DAVIDSON, L. S. P., and FULLERTON, H. W. (1938):Chronic Nutritional Hypochromic Anaemia, Edinb.med. J., 45, 1. 102, 193.
DAVIDSON, L. S. P., DONALDSON, G. M. M., LINDSAY,S. T., and MCSORLEY, J. G. (1943): NutritionalIron Deficiency Anaemia in Wartime, Brit. med. J.,ii, 95.
DONALDSON, R. J. (1965): Personal Communication.ELWOOD, P. C. (1963): A Clinical Trial of Iron-
fortified Bread, Brit. med. J., i, 224.
ELWOOD, P. C., WITHEY, J. L., and KILPATRICK, G. S.(1964): Distribution of Hemoglobin Levels in aGroup of School Children and its Relation toHeight, Weight and other Variables, Brit. J. prev.soc. Med., 18, 125.
FRY, J. (1961): Clinical Patterns and Course ofAnaemias in General Practice, Brit. med. J., ii,1732.
GOLDBERG, A., LOCHHEAD, A. C., and DAGG, J. H.(1963): Histamine-fast Achlorhydria and IronAbsorption, Lancet, i, 848.
HOBSON, W., and BLACKBURN, E. K. (1953): Haemo-globin Levels in a Group of Elderly PersonsLiving at Home Alone or with Spouse, Brit. med.J., i, 647.
JACOBS, A. (1961): Iron-containing Enzymes in theBuccal Epithelium, Lancet, ii, 1331.
KERR, D. N. S., and DAVIDSON, L. S. P. (1958): TheProphylaxis of Iron-deficiency Anaemia in Preg-nancy, Lancet, ii, 483.
KILPATRICK, G. S., and HARDISTY, R. M. (1961):The Prevalence of Anaemia in the Community,Brit. med. J., i, 778.
KILPATRICK, G. S. (1961): Prevalence of Anaemia inGenral Population, Brit. med. J., ii, 1736.
LAMBERT, R. (1964): Nutrition in Britain 1950-1960.Hitchin: Codicote Press.
LEONARD, B. J. (1954): Hypochromic Anaemia inR.A.F. Recruits, Lancet, i, 899.
MADDISON, J. (1962): Personal Communication.MCALPINE, S. G., DOUGLAS, A. S., and ROBB, R. A.
,(1957): Clinical Assessment of Haemoglobin Con-centration, Brit. med. J., ii, 983.
MEDICAL RESEARCH COUNCIL (1945): HaemoglobinLevels in Great Britain in 1943. Spec. Rep. Ser.med. Res. Coun. (Lond.) No. 252. London:H.M.S.O.
MILLIS, J. (1951): The Iron Losses of HealthyWomen during Consecutive Menstrual Cycles.Med. J. Aust., 2, 874.
MOORE, C. V. (1964): In 'Iron Metabolism'-anInternational Symposium. Berlin: Springer-Verlag.
NATIONAL FOOD SURVEY COMMITTEE (1963): DomesticFood Consumption and Expenditure. London:H.M.S.O.
PARSONS, P. L., WITHEY, J. L., and KILPATRICK, G. S.(1965): The Prevalence of Anaemia in the Elderly.Practitioner. (to be published).
SEMMENCE, A. (1959): Anemia in the Elderly, Brit.med. J., ii, 1153.
TAYLOR, H., STURGIS, S. H., and YAHIA, C. (1964):Thb Aetiological Role of Chronic Iron Deficiencyin Production of Menorrhagia, J. Amer. med. Ass.,187, 323.
copyright. on O
ctober 1, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.477.418 on 1 July 1965. D
ownloaded from