Embed Size (px)
Citation preview

Median arcuate ligament: significance in pancreaticoduodenectomy
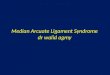
A 50-year-old man was referred to our unit with a history of painlessobstructive jaundice. On investigation with a multiphase abdominalcomputed tomogram, he was found to have a 4-cm mass within thehead of the pancreas. He was also found to have a stenosis at theorigin of the coeliac artery (Fig. 1) and the presence of an accessoryright hepatic artery (RHA) arising from the superior mesentericartery (SMA). After further assessment the patient was organized toundergo pancreaticoduodenectomy (PD).
Intraoperatively, the aetiology of the coeliac artery stenosis (CAS)was found to be due to compression by the median arcuate ligament(MAL). The MAL is a fibrous arch that unites the diaphragmaticcrura on either side of the aortic hiatus and while it normally passescranial to the origin of the coeliac axis, in 10–24% patients it maypass at the level of the origin of the coeliac axis, leading to com-pression of the coeliac artery.1 Prior to formal ligation of thegastroduodenal artery (GDA), the effect on arterial inflow by theMAL was assessed by the GDA occlusion test. After occludingthe GDA, the adequacy of the blood supply was assessed by digitalpalpation and using a Doppler probe on the common hepatic artery(CHA). In our case, it was noted there was both a reduced pulsationand Doppler signal in the CHA following clamping of the GDA. TheMAL was divided and this led to an immediate release of the com-pressed coeliac artery. As expected, there was improved arterialpulsation and Doppler signal of the CHA despite clamping of theGDA. To add further anatomical complexity, the patient was foundto have an accessory right hepatic artery originating from the SMA(Fig. 2). The incidence of this finding is 0.8–8%.2 In our case, wewere able to preserve the accessory right hepatic artery during resec-tion, which likely represented an important collateral pathway forblood supply.
Vascular anomalies in the peripancreatic region add to the surgicalchallenge in PD by not only altering the resection but also recon-struction of the pancreatic remnant. Variations can be classified asoriginating from: (i) coeliac artery; (ii) hepatic artery – either right orleft which can be either replaced or accessory; and (iii) SMA.2 In thiscase, the first two types are seen.
CAS is reported to be present in 2–7.6% of patients undergoingPD.3 In this condition, the blood flow at the origin of the coeliacartery is reduced due to either extrinsic stenosis from compressionby the MAL, intrinsic stenosis because of atherosclerosis or by othercauses such as neoplasia and inflammation.4 The resultant reductionin blood flow results in the development of a number of majorcollateral pathways. Firstly are the pancreaticoduodenal arcadesoriginating from the coeliac artery and SMA. In the presence of CASthese vessels are dilated and dominant flow occurs retrograde into anenlarged GDA. Secondly, the dorsal pancreatic artery acts as animportant collateral circulation point between coeliac artery and
SMA. Thirdly, persistence of an embryological communicationbetween the coeliac axis and SMA exists as the Arc of Buhler, whichalso provides collateral flow.4 The variability of collateralvascularization makes it difficult to predict if residual collateralsupply after GDA ligation and resection of the head of the pancreaswill be adequate in any individual patients.4 Ligation of the GDA canpotentially lead to ischaemia of the liver, stomach and spleen inaddition to an increased risk of post-PD morbidity due to vascularcompromise of the choledochojejunal and gastrojejunal anastomo-ses.5 Once CAS is diagnosed, therapeutic options include preopera-tive endovascular stenting, division of MAL when present,preservation of known collateral blood supply such as a replacedright hepatic artery and operative revascularization such as bypassor arterial implantation.4
The importance of the accessory RHA in this patient is related tothe diagnosis of CAS. Blood supply to the proximal biliary ductdepends exclusively on the right hepatic artery after dividing the bileduct in PD.6 If arterial inflow following division of MAL remainedpoor, right hepatic arterial inflow would be dependent on supply viathe accessory RHA, and thus the integrity and attendant risk of leakof the choledochojejunal anastomosis. If preservation of the acces-sory RHA was not possible and coeliac inflow remained poor, otheroptions of operative revascularization as mentioned earlier wouldhave had to be considered.
Arterial anomalies during PD increase operative complexity.Increased awareness of the vascular anatomy will decreaseintraoperative vascular injury and consequent post-operative
Fig. 1. Contrast enhanced computed tomogram in sagittal view. Thecoeliac artery is compressed just distal to its origin from the aorta (redarrow).
IMAGES FOR SURGEONSANZJSurg.com
© 2013 Royal Australasian College of SurgeonsANZ J Surg 83 (2013) 686–687

complications. Routine preoperative computerized tomographyangiography helps to identify the hepatic vascular anatomy andthereby prepares the surgeon to better deal with vascular anomalies.
References1. Lindner HH, Kemprud E. A clinicoanatomical study of the arcuate liga-
ment of the diaphragm. Arch. Surg. 1971; 103: 600–5.2. Shukla PJ, Barreto SG, Kulkarni A, Nagarajan G, Fingerhut A. Vascular
anomalies encountered during pancreatoduodenectomy: do they influenceoutcomes? Ann. Surg. Oncol. 2010; 17: 186–93.
3. Pfeiffenberger J, Adam U, Drognitz O et al. Celiac axis stenosis in pan-creatic head resection for chronic pancreatitis. Langenbecks Arch. Surg.2002; 387: 210–5.
4. Sakorafas GH, Sarr MG, Peros G. Celiac artery stenosis: anunderappreciated and unpleasant surprise in patients undergoingpancreaticoduodenectomy. J. Am. Coll. Surg. 2008; 206: 349–56.
5. Bong JJ, Karanjia ND, Menezes N, Worthington TR, Lightwood RG.Total gastric necrosis due to aberrant arterial anatomy and retrogradeblood flow in the gastroduodenal artery: a complication followingpancreaticoduodenectomy. HPB (Oxford) 2007; 9: 466–9.
6. Yang F, Long J, Fu DL et al. Aberrant hepatic artery in patients under-going pancreaticoduodenectomy. Pancreatology 2008; 8: 50–4.
Shahrir Kabir, MBBS, FRACSJaswinder Samra, FRCS (Eng and Ed), FRACS
Royal North Shore Hospital, Upper Gastrointestinal SurgicalUnit, University of Sydney, St Leonards, New South Wales,
Australia
doi: 10.1111/ans.12218
(a) (b)Fig. 2. The right hepatic artery (bluearrow) is seen originating from thecoeliac artery and an accessory righthepatic artery (green arrow) is seenoriginating from the superiormesenteric artery. (a) Coronal view and(b) axial view.
Images for surgeons 687
© 2013 Royal Australasian College of Surgeons