Embed Size (px)
Citation preview

Medicaid Redesign
Consumer Concernsby Quela Robinson
Staff Attorney New Mexico Center on Law and Poverty
December 7, 2011
NM center on law and poverty
Who does Medicaid serve?
Over 550,000 people (or 25% of the New Mexico population)
Being low income is not enough to qualify for Medicaid. You must also fit into specific eligibility categories.
This means you must also be…

A senior citizen
A person with a disability
A pregnant woman or a child
A low income family

Or fit another specific category
Women needing family planning services, or treatment for breast or cervical cancer.
People living in institutions (nursing homes)
“Waiver” programs for certain adults: SCI for adults up to 200% FPL ($1815/month for 1 person) Home and Community Based Services for disabled and seniors
at risk of institutionalization whose income is higher than traditional Medicaid (DD waiver, D&E waivers)
Budget cuts have frozen these programs, resulting in waitlists of tens of thousands
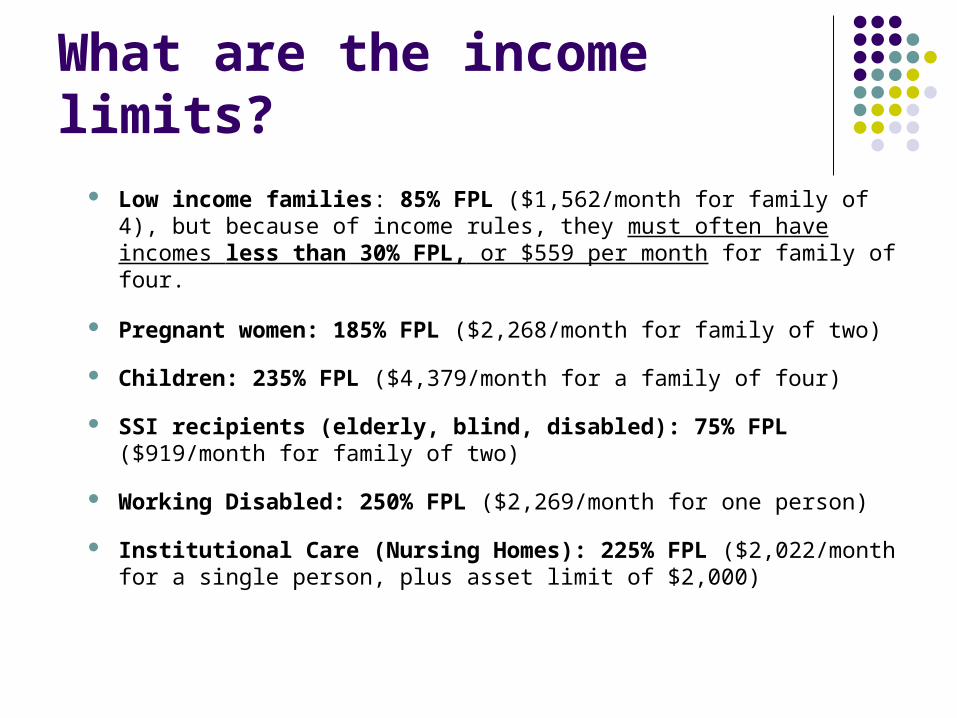
What are the income limits? Low income families: 85% FPL ($1,562/month for family of 4),
but because of income rules, they must often have incomes less than 30% FPL, or $559 per month for family of four.
Pregnant women: 185% FPL ($2,268/month for family of two)
Children: 235% FPL ($4,379/month for a family of four)
SSI recipients (elderly, blind, disabled): 75% FPL ($919/month for family of two)
Working Disabled: 250% FPL ($2,269/month for one person)
Institutional Care (Nursing Homes): 225% FPL ($2,022/month for a single person, plus asset limit of $2,000)

Why is all of this important? Over 200,000 more New Mexicans will become eligible
for Medicaid in 2014 (healthcare reform expands Medicaid to everyone up to 138% FPL).
The federal government will pay 100% of the cost of the expansion for the first three years.
Over 50,000 children currently eligible for Medicaid are not enrolled, and must be by 2014. The state must pay its regular share to cover these children.
The State wants to “redesign” Medicaid to save money. We must make sure that the redesign does not negatively affect access or needed services.

The public has spoken out:
New Mexico has a severe provider shortage
Additional co-payments are unaffordable
Home and community based services cuts devastate seniors and people with disabilities
End the waiting lists for waiver programs for people with disabilities, and for SCI
Managed care has too much red tape
HSD’s Redesign Proposals
1. “Personal Responsibility” (premiums, additional co-pays, deductibles, fees for ER in non-emergency)
2. Global Waiver
3. Care Coordination
4. Pay for Performance

1. What’s wrong with co-pays?
A. 35 years of research shows that fees and co-pays prevent low income people from getting both medically necessary and “unnecessary” care
Their conditions worsen, and they need emergency or more intensive care, driving up costs
Providers and hospitals lose money (can’t collect debt) Co-pays hit seniors, people with disabilities, and those
with chronic conditions the hardest Co-pays are a hidden tax on the poor, who already spend
more of their income on food, housing, and transportation
What’s wrong with co-pays?
B. The state will not save money
The state does not receive federal matching funds for money collected through fees and co-pays
Many states have rejected additional cost sharing because the administrative cost of collection is greater than what is taken in
When people lose Medicaid coverage because they can’t afford premiums, they become uninsured, increasing the cost to local taxpayers to support charity care programs, and increasing the costs of private health insurance.
MCO’s and providers are burdened with collecting the debt

What’s wrong with co-pays?
C. There are few alternatives to the ER in NM
The Medicaid Act requires that “actually available and accessible” ER alternatives exist before charging co-pays
32 of 33 NM counties are federally designated as Health Professions Shortage Areas, Medically Underserved (NM Health Policy Commission, Jan. 2011)
HSD reports the majority of non-emergency use of the ER occurs in rural and frontier areas on evening and weekend hours when there is no alternative
Fees punish sick people for the lack of primary care in NM

What’s wrong with co-pays?
D. Rather than impose fees, there are better alternatives:
Incentives to providers for offering off-hour access and 24 hour nurse help lines.
Better funding for community health programs Diversion programs that screens patients who do
not have emergencies and schedules them for clinic appointments instead (ex: Presbyterian)

2. Global Waiver
12 existing waivers will be combined into 2 or 3
The state must show the federal government that more federal funds will not be required to do this
Many states prove this by cutting services
Current Medicaid waiting lists of people with critical needs are likely to grow
Over 20,000 seniors & people w/ disabilities are on waitlist Over 40,000 working adults are on waitlist

3. Care Coordination
Patients benefit from personal contact (care coordinator, community worker, or navigator)
New technology can efficiently deliver services and saves
administrative costs to providers and the state
Create relevant and public reporting standards so that issues with access and outcomes can be quickly identified
HSD proposal is to reduce Medicaid MCO’s from 7 to 4 – we don’t know how this will affect recipients

4. Pay for Performance
Punitive pay for performance initiatives can exacerbate health disparities by driving out already-scarce providers
Incentives should be positive: higher payments to providers for expanded hours, encourage telemedicine and community health workers that improve health outcomes and save money
Tools for assessing health outcomes must be relevant and transparent.
In conclusion…
Successful Medicaid redesign must be patient-centered - focused on healthcare access and better outcomes. Support at the community level works!
Imposing fees on low-income recipients, especially in a bad economy, does not.
Most Medicaid members responsibly take an active role in managing their own care, but the system could supply more tools to do so.

Contact Me
Quela Robinson
Staff AttorneyNM Center on Law and Poverty
720 Vassar Dr NE, Albuquerque NM(505) 255-2840
NM center on law and poverty




























![Magazine [redesign]](https://img.pdfslide.net/doc/110x75/557c8689d8b42a9f578b4f3c/magazine-redesign.jpg)