Embed Size (px)
Citation preview

medicaid
kaiser commiss ion o n
PO
L
I
C
Y
BR
I
E
F
a n d t h e uninsured
1 3 3 0 G S T R E E T N W , W A S H I N G T O N , D C 2 0 0 0 5
P H O N E : ( 2 0 2 ) 3 4 7 - 5 2 7 0 , F A X : ( 2 0 2 ) 3 4 7 - 5 2 7 4
W E B S I T E : W W W . K F F . O R G / K C M U
January 2013
Medicaid’s Role in Meeting the Long-Term Care Needs of America’s Seniors
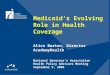
Medicaid plays a key role in the health and well-being of elderly Americans, particularly those with limited incomes. The nation’s elderly – 40.3 million individuals age 65 and older – account for 13 percent of the U.S. population, and the majority are women often living on constrained incomes (Figure 1). Over one-third (34%) of the elderly have household incomes below 200 percent of the poverty threshold ($20,916 for individuals and $26,388 for couples age 65 and older).1 More than 5 million elderly individuals require long-term care assistance to complete life’s daily activities due to decreasing mobility and/or cognitive functioning,2 and those with severely disabling chronic conditions often require more extensive acute care and long-term care services as they age.3 The 85 and over age cohort is at highest risk for needing long-term services and supports (LTSS),4 and the number of individuals in this age cohort is expected to increase by almost 70 percent over the next two decades (Table 1). Medicaid coverage of LTSS includes a wide array of medical and supportive services needed by individuals who cannot independently complete one or more activities of daily living (ADLs) and/or
instrumental activities of daily living (IADLs). About one-half of people with long-term care needs (defined here as individuals who have difficulty performing one or more ADL independently) are age 65 and over. Elderly individuals account for about 82 percent and 45 percent of the institution-based and community-based individuals requiring LTSS, respectively (Figure 2). These activities range from eating, bathing, and dressing to medication management and meal preparation. The need for assistance with ADLs and IADLs is a common
Source: Howden, L.M. and Meyer, J.A. (May 2011). Age and Sex Composition: 2010. U.S. Census Bureau. Available at: http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf.
Figure 1 Gender Distribution of Elderly Americans, by Age Group, 2010
12.4M 9.3M 7.3M 5.7M 3.6M 1.4M 0.4M 0.05M
Median Age = 74.1
49.8%
45.0%
8.4M 10.9M
1.6M 55.0% 18.2%
81.8%
45.0%
49.8%
Note: Data are from the 2007 American Community Survey (ACS). The ACS measure consists of one question about deficiencies in performing certain ADL tasks. Source: Kaye et al. (2010). Long-Term Care: Who Gets It, Who Provides It, Who Pays, And How Much? Health Affairs, 29:1, 11-21.
Figure 2
Seniors Account for Half of the Total Population with Long-Term Care Needs
49.2%
50.8%
10.0M
1.6M
8.4M
55.0%
45.0% 18.2%
81.8%

2 002 00
criterion for assessing functional eligibility for long-term care services. Other assessment criteria include the presence of certain medical conditions and evidence of cognitive impairment. Many seniors struggling with chronic disabling conditions, such as cancer, diabetes hypertension, stroke, Alzheimer’s disease and other dementias rely on friends and/or family for unpaid, informal caregiving, but as care needs mount, additional paid services are often required. Elderly individuals often need long-term services and supports as they age. For most elderly Americans Medicare is the primary payer for basic medical services such as hospital and physician visits, prescription drugs, skilled nursing and home health services, and other acute and post-acute services, but some critical services – LTSS, dental, and vision – are excluded or limited under Medicare. For some elderly individuals who require extensive care, nursing home care may be needed. Over 60 percent of nursing home residents rely on Medicaid for assistance.5 Other seniors may be able to “age in place” and receive services in their home or in a community-based setting (e.g. adult day care center, assisted living facility). Given the high cost of long-term care services, few elderly people can afford these services. For seniors with long-term care needs, Medicaid, as a complement to Medicare, serves as an essential safety net for institutional and community-based services not fully covered by Medicare or private insurance. Medicaid is the nation’s primary payer of long-term services and supports. Medicaid, administered by states and jointly financed by the state and federal governments, is the primary payer for long-term care services for individuals under age 65 with disabilities as well as many seniors who are low-income or who deplete their personal savings to pay for medical and long-term care. Paying for needed LTSS can be burdensome; nursing home care averages $83,585 per year, assisted living facility costs average $39,516 per year, and home health aide services average $21 per hour.6 Medicare provides limited post-acute care and few people can afford private long-term care insurance. In 2010, total long-term care spending in the U.S. was $342 billion with Medicaid’s share totaling 41 percent (Figure 3). State Medicaid programs provide a range of long-term care services. Medicaid medical and long-term care expenditures for the approximately 6 million elderly beneficiaries were almost $81 billion, or nearly a quarter (23%), of total Medicaid spending in 2009.7,8 In 2009, 32 percent of elderly Medicaid enrollees used long-term care services, but they accounted for 74 percent of all Medicaid spending on the elderly.9 Among the 2 million elderly Medicaid beneficiaries with long-term care use in 2009, per person total Medicaid spending averaged $34,579 in 2009 (Figure 4).10,11 For these long-term care beneficiaries, the bulk of Medicaid spending (88%) was for long-term care services as Medicare is the primary payer for acute care services. State Medicaid programs provide a wide range of LTSS in the nursing home and in the community including, but not limited to, home health, personal care, medical equipment, rehabilitative therapy, adult day care, targeted case management, home modifications, transportation, and respite care for caregivers. This array of services is key to enabling elderly individuals with long-term care needs to live as independently as possible in a range of settings.
Note: Total long-term care expenditures include spending on residential care facilities, nursing homes, home health services, personal care services, and home and community-based waiver services. Long-term care expenditures also include spending on ambulance providers. All home and community-based waiver services are attributed to Medicaid. Source: KCMU estimates based on CMS National Health Expenditure Accounts data, 2010.
Figure 3
Medicaid is the primary payer for long-term care services
Total in 2010 = $342 billion

States have considerable flexibility in designing their benefit package, but, as a requirement for participation in Medicaid, states must provide nursing home care and home health care to eligible beneficiaries age 21 and older. All other long-term care services are optional for states. States typically provide long-term care services to elderly people who qualify for Supplemental Security Income and may extend Medicaid benefits to elderly beneficiaries with relatively higher incomes who incur health care expenses and spend down to a state-set financial eligibility standard. After qualifying for Medicaid, often following a nursing home stay, seniors must put all income except for a small personal allowance toward the cost of health care services. Over half of seniors who rely on Medicaid for LTSS reside in nursing homes, while the remainder rely on the program primarily for assistance to help stay in the community.
Medicaid LTSS spending varies across states. The elderly are one of the two highest-cost populations in Medicaid on a per-enrollee basis, second only to individuals with disabilities. Per capita Medicaid spending for elderly long-term care users varies widely across states, from $13,504 (New Mexico) to $60,903 (Pennsylvania) (Figure 4 and Table 2). States have made considerable progress over the past 20 years in providing more LTSS in the community to help people avoid or delay nursing home admission. From 1999 to 2009, Medicaid home and community-based services (HCBS) expenditures increased by almost 200 percent.
12,13 Today, HCBS spending for elderly beneficiaries accounts for nearly one-fifth (19%) of total Medicaid long-term care expenditures the elderly, with state spending for these services as a share of total Medicaid long-term care expenditures for elderly ranging from 7 percent (Florida and Kentucky) to 58 percent (Alaska) (Figure 5 and Table 2).14 Recent state budget constraints have slowed states’ efforts to continue to expand coverage for HCBS; the use of waiting lists, service utilization caps, and cost containment tools can result in unmet need for services and possibly unnecessary institutionalization and/or poor health outcomes.
Note: *Spending per capita for Arizona is not shown because long-term users in Arizona are covered under the Arizona Long-Term Care System, which is a capitated program, and expenditures cannot be separated out by service type. However, the national average includes Arizona spending. Source: Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data for FFY 2009 MSIS, 2012. Because 2009 data were unavailable, 2008 MSIS was used for Pennsylvania, Utah, and Wisconsin.
National Average = $34,579
Figure 4
Per Capita Medicaid Spending for Elderly Beneficiaries with Long-Term Care Use Varies Across States
Figure 5 Medicaid HCBS Spending for the Elderly as a Share of Medicaid Long-Term Care
Expenditures for Elderly Beneficiaries Varies Across States
National Share = 19%
Note: *HCBS spending for Arizona is not shown because long-term users in Arizona are covered under the Arizona Long-Term Care System, which is a capitated program, and expenditures cannot be separated out by service type. Home and community-based services include § 1915(c) waiver services, home health services, and personal care services. Source: Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data for FFY 2009 MSIS, 2012. Because 2009 data were unavailable, 2008 MSIS was used for Pennsylvania, Utah, and Wisconsin.
AK
33

4 004 00
Looking Ahead: Medicaid will continue to play an important role in helping seniors obtain long-term care services. Medicaid spending continues to be a major focus of both state and federal budget deficit reduction policy discussions. The majority of adults (59%) deem Medicaid to be important for themselves and their family,15 and in the absence of other affordable long-term care options, Medicaid will continue to play a significant role, together with Medicare, in the providing care to elderly Americans as the 76 million “Baby Boomers” get older and develop conditions and impairments that require more extensive acute and long-term care services. Looking ahead, in addition to health care costs, population aging, preference for community-based long-term care options, and quality of care are likely to remain key concerns for Medicaid programs. The challenge to policymakers is to respond to the growing need for long-term care and assure adequate safeguards are in place to protect the most frail, long-term care beneficiaries across the various care settings. Budget constraints have limited states’ efforts to meet the growing demand for community-based care among the elderly, and cuts to federal Medicaid spending could jeopardize access to such care for high-cost, vulnerable populations including seniors.
This policy brief was prepared by Erica Reaves and Katherine Young of the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured.

500 500
Table 1: The Elderly Population by State, 2010
StateElderly (65+) Population,a
Elderly Population as a Percent of
State Populationa
Number of Individuals Age
85+a
85+ Population as a Percent of
State Populationa
85+ Population as a Percent
Change, 2012-2032b
Percent of Elderly with Any Disabilityc
Percent of Elderly with a Cognitive
Difficultyc
Percent of Elderly with a Self-Care
Difficultyc
Alabama 657,792 13.8% 75,684 1.6% + 74% 44.0% 13.0% 11.3%Alaska 54,938 7.7% 4,711 0.7% + 207% 39.0% 8.7% 8.3%Arizona 881,831 13.8% 103,400 1.6% + 105% 33.0% 7.8% 6.6%Arkansas 419,981 14.4% 51,402 1.8% + 65% 43.0% 11.1% 9.1%California 4,246,514 11.4% 600,968 1.6% + 78% 37.0% 10.6% 10.7%Colorado 549,625 10.9% 69,613 1.4% + 112% 35.0% 7.9% 7.1%Connecticut 506,559 14.2% 84,898 2.4% + 49% 33.0% 8.1% 7.5%Delaware 129,277 14.4% 15,744 1.8% + 91% 31.0% 8.0% 5.8%District of Columbia 68,809 11.4% 10,315 1.7% + 37% 34.0% 9.8% 8.7%Florida 3,259,602 17.3% 434,125 2.3% + 62% 34.0% 9.1% 8.0%Georgia 1,032,035 10.7% 113,823 1.2% + 121% 40.0% 11.1% 9.7%Hawaii 195,138 14.3% 30,238 2.2% + 59% 33.0% 9.9% 7.3%Idaho 194,688 12.4% 25,242 1.6% + 90% 38.0% 9.5% 7.6%Illinois 1,609,213 12.5% 234,912 1.8% + 51% 35.0% 8.0% 8.3%Indiana 841,108 13.0% 115,272 1.8% + 57% 37.0% 8.7% 7.9%Iowa 452,888 14.9% 74,658 2.5% + 28% 32.0% 6.6% 5.9%Kansas 376,116 13.2% 59,318 2.1% + 46% 38.0% 9.4% 7.8%Kentucky 578,227 13.3% 69,208 1.6% + 74% 42.0% 11.1% 10.2%Louisiana 557,857 12.3% 65,686 1.4% + 74% 43.0% 12.1% 10.8%Maine 211,080 15.9% 29,136 2.2% + 71% 38.0% 9.8% 6.7%Maryland 707,642 12.3% 98,126 1.7% + 92% 34.0% 8.4% 7.8%Massachusetts 902,724 13.8% 145,199 2.2% + 46% 33.0% 8.2% 7.7%Michigan 1,361,530 13.8% 191,881 1.9% + 58% 37.0% 9.7% 8.5%Minnesota 683,121 12.9% 106,664 2.0% + 55% 32.0% 6.6% 6.9%Mississippi 380,407 12.8% 44,359 1.5% + 67% 45.0% 13.9% 11.7%Missouri 838,294 14.0% 113,779 1.9% + 60% 39.0% 9.5% 8.4%Montana 146,742 14.8% 20,021 2.0% + 73% 37.0% 7.7% 6.6%Nebraska 246,677 13.5% 39,308 2.2% + 38% 36.0% 7.3% 6.8%Nevada 324,359 12.0% 30,187 1.1% + 184% 34.0% 7.8% 7.8%New Hampshire 178,268 13.5% 24,761 1.9% + 77% 32.0% 6.1% 5.9%New Jersey 1,185,993 13.5% 179,611 2.0% + 58% 33.0% 8.3% 8.3%New Mexico 272,255 13.2% 31,993 1.6% + 94% 41.0% 10.9% 9.6%New York 2,617,943 13.5% 390,874 2.0% + 46% 34.0% 9.0% 8.8%North Carolina 1,234,079 12.9% 147,461 1.5% + 97% 38.0% 10.4% 9.2%North Dakota 97,477 14.5% 16,688 2.5% + 17% 35.0% 6.5% 4.9%Ohio 1,622,015 14.1% 230,429 2.0% + 49% 36.0% 8.8% 7.9%Oklahoma 506,714 13.5% 61,912 1.7% + 70% 43.0% 10.3% 9.1%Oregon 533,533 13.9% 77,872 2.0% + 73% 38.0% 11.4% 9.4%Pennsylvania 1,959,307 15.4% 305,676 2.4% + 30% 36.0% 8.6% 7.9%Rhode Island 151,881 14.4% 26,750 2.5% + 37% 37.0% 7.9% 6.9%South Carolina 631,874 13.7% 70,717 1.5% + 101% 38.0% 11.0% 8.9%South Dakota 116,581 14.3% 19,226 2.4% + 39% 36.0% 7.4% 6.8%Tennessee 853,462 13.4% 99,917 1.6% + 91% 42.0% 11.9% 10.7%Texas 2,601,886 10.3% 305,179 1.2% + 100% 41.0% 10.8% 10.7%Utah 249,462 9.0% 30,991 1.1% + 94% 34.0% 8.2% 6.9%Vermont 91,078 14.6% 12,797 2.0% + 77% 34.0% 8.9% 6.9%Virginia 976,937 12.2% 122,403 1.5% + 101% 35.0% 8.7% 8.0%Washington 827,677 12.3% 117,271 1.7% + 90% 38.0% 10.0% 8.7%West Virginia 297,404 16.0% 35,921 1.9% + 55% 43.0% 11.6% 10.5%Wisconsin 777,314 13.7% 118,505 2.1% + 52% 33.0% 6.7% 6.6%Wyoming 70,090 12.4% 8,602 1.5% + 82% 37.0% 8.6% 4.9%United States 40,268,004 13.0% 5,493,433 1.8% + 69% 37.0% 9.5% 8.8%
Sources: a Howden, L.M. and Meyer, J.A. (May 2011). Age and Sex Composition: 2010. U.S. Census Bureau. Available at: http://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf. b AARP Public Policy Institute calculations from REMI 2012 baseline demographic projections. Houser, A., Fox-Grage, W., and Ujvari, K. (2012). Across the States 2012: Profiles of Long-Term Services and Supports. AARP Public Policy Institute. Available at: http://www.aarp.org/home-garden/livable-communities/info-09-2012/across-the-states-2012-profiles-of-long-term-services-supports-AARP-ppi-ltc.html. c AARP Public Policy Institute calculations using data from U.S. Bureau, American Community Survey 2010, Tables C18101, C18104, and C18106; and Houser, A., Fox-Grage, W., and Ujvari, K. (2012). Across the States 2012: Profiles of Long-Term Services and Supports. AARP Public Policy Institute. Available at: http://www.aarp.org/home-garden/livable-communities/info-09-2012/across-the-states-2012-profiles-of-long-term-services-supports-AARP-ppi-ltc.html.

6 006 00
Table 2: Medicaid Enrollment and Expenditures for Elderly Beneficiaries, FFY 2009
Nursing Home HCBS
Alabama 120,974 12.7% $1,000 26% $8,265 $864 $28,210 18,294 87% 11%Alaska 8,504 7.0% $181 17% $21,286 $147 $52,091 567 42% 58%Arizona 103,765 6.0% $979 12% $9,438 N/A N/A N/A N/A N/AArkansas 69,603 10.0% $875 27% $12,564 $617 $31,635 13,602 81% 19%California 998,482 9.1% $10,512 27% $10,528 $6,809 $24,859 78,152 51% 48%Colorado 49,781 8.1% $813 24% $16,332 $600 $32,226 10,436 74% 26%Connecticut 68,978 11.8% $1,708 30% $24,761 $1,555 $50,418 20,288 72% 20%Delaware 14,304 6.9% $205 17% $14,330 $168 $49,943 2,739 83% 13%District of Columbia 15,652 9.2% $346 22% $22,094 $204 $55,391 2,220 56% 41%Florida 445,500 13.0% $3,527 25% $7,917 $2,309 $37,624 49,444 91% 7%Georgia 170,538 9.4% $1,395 19% $8,183 $1,100 $34,311 26,401 88% 11%Hawaii 24,273 9.8% $315 25% $12,961 $103 $54,390 3,053 81% 18%Idaho 16,958 7.4% $217 17% $12,802 $185 $26,768 3,261 70% 29%Illinois 209,610 7.8% $2,118 17% $10,105 $1,469 $23,241 41,964 73% 23%Indiana 85,191 7.4% $1,240 21% $14,552 $1,036 $35,333 26,305 85% 11%Iowa 42,978 8.2% $611 21% $14,207 $540 $21,286 13,783 70% 27%Kansas 36,396 9.8% $537 23% $14,761 $450 $26,146 10,813 72% 26%Kentucky 95,686 10.8% $934 18% $9,759 $773 $33,678 18,645 92% 7%Louisiana 112,361 9.8% $960 17% $8,548 $777 $29,972 18,882 68% 27%Maine 60,768 17.0% $562 23% $9,242 $342 $50,337 6,673 88% 9%Maryland 73,239 8.5% $1,326 21% $18,106 $1,074 $51,034 15,406 81% 18%Massachusetts 170,036 10.5% $3,110 25% $18,288 $1,958 $49,831 34,384 84% 11%Michigan 137,892 6.8% $2,088 21% $15,139 $1,768 $33,798 30,679 89% 11%Minnesota 96,039 10.9% $1,644 23% $17,119 $927 $36,430 19,708 80% 18%Mississippi 88,741 11.8% $867 24% $9,775 $691 $34,352 14,022 87% 9%Missouri 94,318 8.9% $1,318 19% $13,971 $881 $26,171 25,490 82% 17%Montana 10,603 9.2% $242 29% $22,824 $220 $43,938 3,607 80% 18%Nebraska 23,929 9.4% $367 24% $15,344 $300 $29,695 7,561 79% 18%Nevada 25,841 8.9% $210 17% $8,117 $164 $27,862 2,957 74% 26%New Hampshire 15,464 9.7% $303 27% $19,616 $279 $37,887 5,431 80% 19%New Jersey 148,457 14.7% $2,628 31% $17,705 $2,042 $40,987 29,865 76% 19%New Mexico 36,133 6.6% $190 6% $5,247 $117 $13,504 3,111 42% 56%New York 591,892 11.4% $13,314 29% $22,494 $10,069 $55,793 105,111 57% 39%North Carolina 182,522 10.1% $1,946 18% $10,664 $1,646 $24,569 30,391 65% 32%North Dakota 9,179 12.2% $191 33% $20,763 $178 $37,479 3,699 87% 9%Ohio 176,456 8.1% $3,335 25% $18,900 $2,766 $35,432 54,576 77% 19%Oklahoma 66,263 8.3% $693 18% $10,464 $564 $22,466 13,910 73% 25%Oregon 55,714 9.9% $927 26% $16,646 $809 $39,355 5,879 53% 46%Pennsylvania 235,668 10.7% $5,012 31% $21,268 $4,548 $60,903 58,416 88% 9%Rhode Island 28,103 13.7% $427 24% $15,211 $343 $44,120 6,386 92% 8%South Carolina 83,323 9.3% $911 20% $10,936 $716 $35,096 12,193 77% 17%South Dakota 12,548 9.8% $149 21% $11,874 $128 $25,097 4,207 87% 11%Tennessee 149,440 9.9% $1,118 16% $7,484 $886 $34,007 23,283 84% 13%Texas 439,643 9.8% $3,872 18% $8,808 $2,520 $20,157 63,678 68% 28%Utah 15,419 5.2% $186 12% $12,088 $131 $36,413 3,239 87% 9%Vermont 20,158 11.1% $222 23% $11,018 $173 $39,483 2,739 77% 23%Virginia 105,853 11.2% $1,114 20% $10,522 $901 $31,301 18,695 71% 22%Washington 87,797 7.6% $1,275 21% $14,519 $1,059 $30,768 12,528 43% 57%West Virginia 41,741 10.0% $535 22% $12,820 $483 $37,362 8,113 83% 16%Wisconsin 146,292 14.2% $1,868 28% $12,766 $1,020 $35,958 23,711 80% 18%Wyoming 5,736 7.0% $112 21% $19,518 $85 $37,009 1,835 81% 17%United States 6,124,741 9.8% $80,536 23% $13,149 $59,525 $34,579 1,011,054 72% 19%
Total Medicaid Long-Term Care Expenditures,
Elderly (in millions)
Total Medicaid Expenditures Per Long-Term Care
User, Elderly
Total Nursing Home
Enrollment, Elderly
Distribution of Medicaid Long-Term Care Expenditures for Elderly Enrollees
State
Total Medicaid
Enrollment, Elderly
Elderly Medicaid Enrollment as a
Percent of Medicaid
Enrollment
Total Medicaid Expenditures,
Elderly (in millions)
Total Medicaid Expenditures for Elderly Enrollees
as Percent of Total Medicaid
Expenditures
Total Medicaid
Expenditures Per Enrollee,
Elderly
Notes: Arizona’s long-term care users are covered under the Arizona Long-Term Care System, a capitated program. As a result, nursing home enrollment and long-term care spending cannot be separated out by service type. However, the national totals include Arizona spending.
Total Medicaid expenditures per elderly enrollee do not include Medicaid payments for Medicare premiums.
A long-term care user is defined as an enrollee who spent more than the 10th percentile in their state on community-based care, or more than the 10th percentile in their state in nursing homes, Intermediate Care Facilities for Individuals with Intellectual Disabilities, mental health facilities for the elderly, or psychiatric long-term care facilities for those under 21. Long-term care expenditures do not include Medicaid payments for Medicare premiums.
HCBS expenditures include § 1915(c) waiver services, home health services, and personal care services.
Source: Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data for FFY 2009 MSIS, 2012.Because 2009 data were unavailable, 2008 MSIS was used for Pennsylvania, Utah, and Wisconsin.

700 700
Endnotes
1 DeNavas-Walt et al. (September 2012). Income, Poverty, and Health Insurance Coverage in the United States: 2011. U.S. Census Bureau, Current Population Reports, P60-243. At http://www.census.gov/hhes/www/poverty/data/incpovhlth/2011/index.html. 2 Kaye et al. (January 2010). Long-Term Care: Who Gets It, Who Provides It, Who Pays, and How Much. Health Affairs, 29:1, 11-21. 3 Kaiser Commission on Medicaid and the Uninsured, “Medicaid and Long-Term Care Services and Supports,” February 2009. Available at: http://www.kff.org/medicaid/upload/2186_06.pdf. 4 Houser, A., Fox-Grage, W., and Ujvari, K. (2012). Across the States 2012: Profiles of Long-Term Services and Supports. AARP Public Policy Institute. Available at: http://www.aarp.org/home-garden/livable-communities/info-09-2012/across-the-states-2012-profiles-of-long-term-services-supports-AARP-ppi-ltc.html. 5 Harrington et al. (2011). Nursing, Facilities, Staffing, Residents, and Facility Deficiencies, 2005 Through 2010. University of California, San Francisco. At http://www.pascenter.org. 6 MetLife Market Institute. (October 2010). Market Survey of Long-Term Care Costs: The 2010 MetLife Market Survey of Nursing Home, Assisted Living, Adult Day Services, and Home Care Costs. At: http://www.metlife.com/assets/cao/mmi/publications/studies/2010/mmi-2010-market-survey-long-term-care-costs.pdf 7 This figure does not include Medicaid payments for Medicare premiums. 8 Kaiser Commission on Medicaid and the Uninsured (KCMU) and Urban Institute estimates based on data from FFY 2009 MSIS and CMS-64 reports, 2012. Because 2009 data was unavailable, 2008 MSIS data was used for Pennsylvania, Utah, and Wisconsin. 9 Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data from FFY 2009 MSIS and CMS-64 reports, 2012. 10 A long-term care user is defined as an enrollee who spent more than the 10th percentile in their state on community-based care, or more than the 10th percentile in their state in nursing homes, Intermediate Care Facilities for the Individuals with Disabilities, or mental health facilities for individuals age 65 and older. 11 KCMU and Urban Institute estimates based on data for FFY 2009 MSIS, 2012. Because 2009 data was unavailable, 2008 MSIS was used for Pennsylvania, Utah, and Wisconsin. 12 Home and community-based services include § 1915(c) waiver services, home health services, and personal care services. 13 KCMU and UCSF analysis of CMS Form 372 data and program surveys. 14 Kaiser Commission on Medicaid and the Uninsured (KCMU) and Urban Institute estimates based on data from FFY 2009 MSIS and CMS-64 reports, 2012. Because 2009 data was unavailable, 2008 MSIS data was used for Pennsylvania, Utah, and Wisconsin. Spending for these states was then adjusted to 2009 CMS-64 spending levels. Spending for Arizona is not shown because long-term users in Arizona are covered under the Arizona Long-Term Care System, which is a capitated program, and expenditures cannot be separated out by service type. 15 Kaiser Family Foundation/Harvard School of Public Health. (January 2011). The Public’s Health Care Agenda for the 112th Congress. At http://www.kff.org/kaiserpolls/upload/8134-C.pdf.

1 3 3 0 G S T R E E T N W , W A S H I N G T O N , D C 2 0 0 0 5
P H O N E : ( 2 0 2 ) 3 4 7 - 5 2 7 0 , F A X : ( 2 0 2 ) 3 4 7 - 5 2 7 4
W E B S I T E : W W W . K F F . O R G / K C M U
A d d i t i o n a l c o p i e s o f t h i s r e p o r t ( # 0000 ) a r e a v a i l a b l e o n t h e K a i s e r F a m i l y F o u n d a t i o n ’ s w e b s i t e a t w w w . k f f . o r g .
The Kaiser Commission on Medicaid a nd the Uninsured provides information a nd a nalys is on health care coverage
a nd access for the low-income populat ion, with a specia l focus on Medicaid's role a nd coverage of the uninsured.
Begun in 1991 a nd based in the Kaiser Family Foundation's Washington, DC off ice , the Commission is the largest
operat ing program of the Foundation . The Commission’s work is conducted by Foundation sta f f under the guida nce
of a bi-part isa n group of nat ional leaders a nd experts in health care a nd publ ic pol icy .
This report (#8403) is available on the Kaiser Family Foundation’s website at www.kff.org.