Embed Size (px)
Citation preview

Validation of the Medical Battalion Enhancement Initiative using NHRC Tools in Support of the Marine Corps
2007-03-22 MBCE Med BN Validation Study
Med BN Validation Study• Purpose, Objectives, and Approach• CONOPS• Baseline Case and Excursions• Assumptions• Scenario Description
– Med Bn Capability– Casualty Stream
• Results

2006-09-07 ERSS Validation Study 2
Purpose, Objectives, and Approach• Purpose: Provide information for the Medical Battalion Capability Enhancement WIPT
and decision makers on the HS OAG COA to restructure the Medical Battalion (MedBn)
• Objectives- Determine if the OAG COA to restructure the MedBn has the capability and capacity to support a
“MEF in the assault” in a MCO Defense Planning Scenario.
- Compare patient outcomes between the OAG COA and the current MedBn in the MCO DPS
- Determine the impact of limiting tactical evacuation on patient outcomes
- Perform other excursions as directed
• Approach- Describe the USMC casualty flow from the MCO DPS
- Provide a descriptive analysis and assessment of the OAG COA and current MedBn in terms of:• Casualty survival rates and patient outcomes (mortality, return to duty) • Define health services laydown (resources for Direct Support, General Support, and patient movement) • Define initial metrics• Define assumptions, base case, excursions
- Iterative Process• Investigate the 1 RCT case to understand issues, then complete 3 RCT case and excursions.• Model base case and excursions in TML+ (Tactical Medical Logistics Planning Tool)• Analyze results using the mean and 95th percentile of multiple TML+ runs• Revise as necessary

2006-09-07 ERSS Validation Study 3
CONOPS• Scenario Development
– MCO 30 days high intensity combat operations ashore– 15 days prior to casualty peak, 15 days after– Focused on 3 RCTs conducting operations ashore
GroundCASEVAC
1 hr
30 min
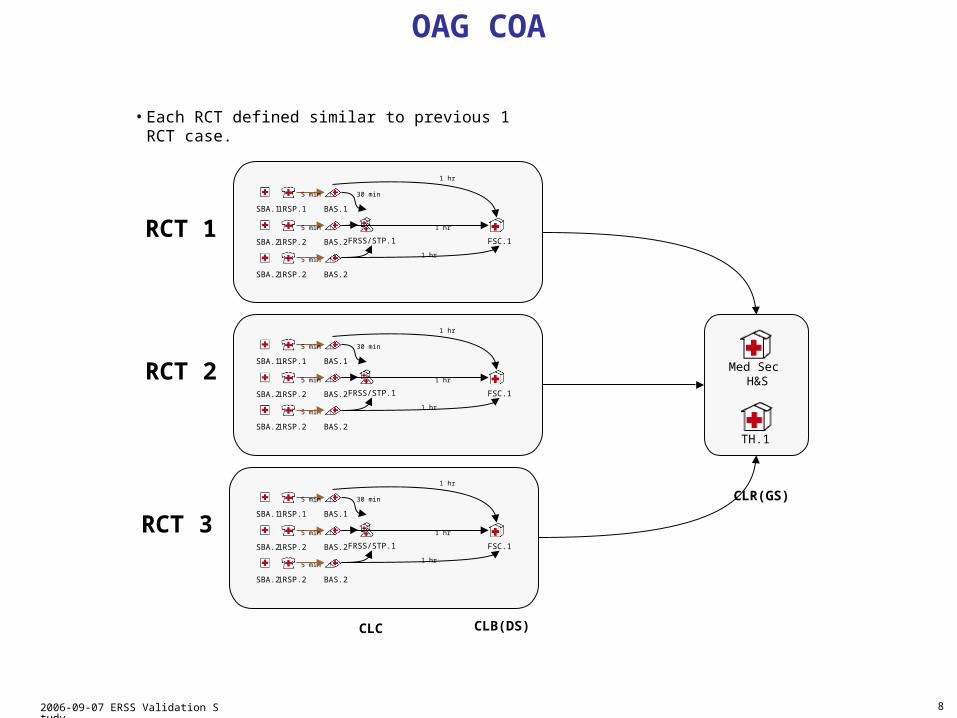
HSS laydown applies to RCT 1, RCT 2, RCT 3
FRSS/STP
BAS FSC TheaterHospital
ERCS
ERCS
1 hr
1.5 hrs
Air CASEVAC
AirCASEVAC
2 hrsAir CASEVAC
5 min
POI
RCT 1RCT 2RCT 3
FRSS/STP from FSC deployed fwd to support RCT.
Baseline
CLR(GS)
Med Sec (H&S)
2 hrs
Air CASEVAC
Mental Health
RTDs/DNBI
1 hrSur
gica
l
FRSS/STP located with the Battalion HQ
FSC with the Regimental HQ
CLB(DS)
POI: Point of Injury
FRSS/STP: Forward Resuscitative Surgical System (FRSS)/Shock Trauma Platoon (STP)
ERCS: Enroute Care System
FSC: Forward Surgical Company
RTD: Return to Duty
DNBI: Disease/Non-Battle Injury
CLC: Combat Logistics Company
CLB(DS): Combat Logistics Battalion (Direct Support)
CLR (GS): Combat Logistics Regiment (General Support)
CLC

2006-09-07 ERSS Validation Study 4
• There was no draft CONOPs provided by CD&I describing how the restructured MedBn would support a “MEF in the assault”.
• The CONOPs used for the TML+ modeling was based on:– 1st MedBn’s experience in OIF 1 supporting a “MEF in the assault”– Employment of the MedBn’s capability sets consistent with other
pertinent studies and MAAs— No USMC doctrine on use of the FRSS or ERCS
– Conceptual employment of the CLC, CLB(DS) and CLR(GS)– Employment of a Theater Hospital co-located with the CLR(GS)
based on our OIF1 experience
• What are the casualty survival rates and patient outcomes (mortality, return to duty) for the OAG COA and the current MedBn?
• Are the quantity of capability sets (FRSS, STP, ERCS, Wards, etc.) adequate?
• What are the impacts of decreasing holding capacity on patient outcomes?
Medical Planning Issues

2006-09-07 ERSS Validation Study 5
Baseline Case and Excursions
Analyze baseline.Compare baseline with the current Med Bn capability.Investigate excursions.
Cases Name Description
Baseline OAG COA
The OAG COA provides a proposal to restructure the MEDBN to support the new MLG construct and make it more “mobile, scalable, and tailorable”.
Comparison Current Med BnThe "As Is" COA supports the new MLG construct without reorganizing the Med Bn.
Excursions
OAG COA with Nighttime Air Evac
Baseline OAG COA with all air evacuations occurring at night (1800 to 0600).
OAG COA with BAS/STP/FRSS
Baseline OAG COA with STP/FRSS colocated with each BAS.

2006-09-07 ERSS Validation Study 6
AssumptionsCONOPS Assumptions• Rapid evacuation under ideal conditions• USMC Patient Evacuation Team (PET) is coordinating tactical helicopter evacuation • Resuscitative surgery should be available within 60 minutes from the BAS• The Forward Surgical Company will relocate with the Regimental HQ and CLB(DS)• The FRSS/STP will relocate with the Battalion HQ and CLC.• The "Medical Section, H&S Company, MedBn", and the Theater Hospital will not relocate
TML+ Modeling Assumptions• BASs are able to handle the casualty stream
– Use 3 BASs per 1 RCT• Tactical evacuation assets are always available when needed
– Unlimited tactical evacuation assets available to evacuate patients from the FRSS and FSC.• If a patient requires an ERCS team, a designated helicopter will be available.• Theater hospital will have sufficient resuscitative surgical capability, holding, and diagnostic capacity to handle the casualty stream.

2006-09-07 ERSS Validation Study 7
OAG COA – A Regimental Combat Team (RCT)
SBA.1 1RSP.1 BAS.1
Medical Capability• Med Sec (H&S) provides:
– Surge capacity – If FRSS is closed, evac to FSC.– Treatment of mental health patients – If FSC is closed, evac to theater
hospital.– Temporary holding for RTD and DNBIs
Evacuation• Evacuate patients requiring specialty care (neuro need, etc) to theater hospital.• Evacuate moderate to severe mental health patients from BASs to Med Sec (H&S).• Far-forward evacuation assets will include 2 dedicated CH-53s and 2 dedicated MV-22s per RCT.
– Based at FSC.1 (Co-locate these dedicated evacuation assets with the RCT)– Increase this number as needed to avoid shortfalls in tactical evacuation
• Sufficient ground vehicles to handle all requests from 1RSP to BAS.• Sufficient helos to handle all requests from FRSS and FSC to theater hospital
Maneuver• The FRSS will maneuver with the supported RCT, and will always be within 30 minutes flying time
from the RCT. Two maneuvers will occur. Both during a lull in operations.
FRSS/STP.1 FSC.1SBA.2 1RSP.2 BAS.2
SBA.3 1RSP.3 BAS.3
TH.1
5 min
5 min
Sufficient ground vehicles to handle all requests from 1RSP to BAS.
30 min
Sufficient helos to handle all requests from FRSS and FSC to theater hospital.
1 hr
1 hr
1 hr
1 hr
ERCS
2 hr
2 hr
2x MV-22 2x CH-53
MV-22Speed: 275 mphCapacity (amb, litter): 24 or 12 maxLoad (amb, litter): 2 & 3 minUnload (amb, litter): 2 & 3 minPre-Mission: 30 minPost-Mission: 30 minWait Time: 0 min
CH-53ESpeed: 170 mphCapacity (amb, litter): 19 & 8 combinedLoad (amb, litter): 2 & 3 minUnload (amb, litter): 2 & 3 minPre-Mission: 30 minPost-Mission: 30 minWait Time: 0 min
Route LegendAir CASEVACERCS
Med Sec H&S2 hr
2 hr
30 min
2 hr
2 hr
5 min
5 min
10 min
1 hr
MV-22
Sufficient helos to handle all requests, if necessary.
CLC CLB(DS) CLR(GS)
2006-09-07 ERSS Validation Study 8
OAG COA
RCT 1SBA.11RSP.1 BAS.1
5 min
FRSS/STP.1 FSC.1SBA.21RSP.2 BAS.2
SBA.21RSP.2 BAS.2
5 min
5 min 30 min
1 hr
1 hr
1 hr
RCT 2
RCT 3
• Each RCT defined similar to previous 1 RCT case.
SBA.11RSP.1 BAS.1
5 min
FRSS/STP.1 FSC.1SBA.21RSP.2 BAS.2
SBA.21RSP.2 BAS.2
5 min
5 min 30 min
1 hr
1 hr
1 hr
SBA.11RSP.1 BAS.1
5 min
FRSS/STP.1 FSC.1SBA.21RSP.2 BAS.2
SBA.21RSP.2 BAS.2
5 min
5 min 30 min
1 hr
1 hr
1 hr
Med Sec H&S
TH.1
CLC CLB(DS)
CLR(GS)
2006-09-07 ERSS Validation Study 9
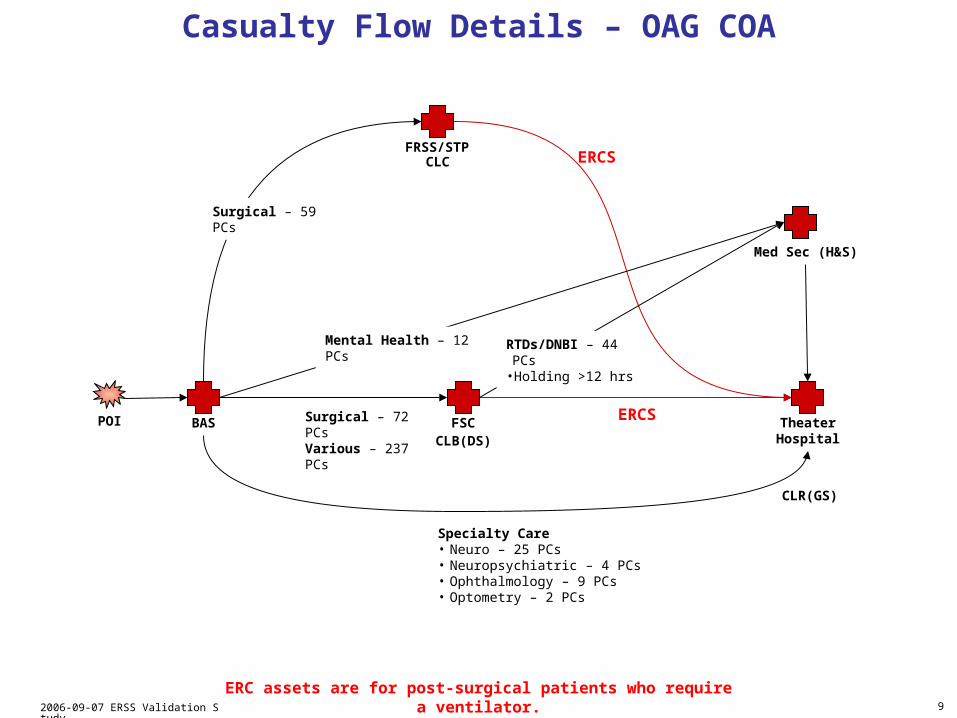
Casualty Flow Details – OAG COA
FRSS/STP
BAS FSC TheaterHospital
POI
Med Sec (H&S)
Specialty Care• Neuro – 25 PCs• Neuropsychiatric – 4 PCs • Ophthalmology – 9 PCs• Optometry – 2 PCs
Surgical – 59 PCs
Mental Health – 12 PCs RTDs/DNBI – 44 PCs •Holding >12 hrs
Surgical – 72 PCsVarious – 237 PCs
ERCS
ERCS
ERC assets are for post-surgical patients who require a ventilator.
CLC
CLB(DS)
CLR(GS)

2006-09-07 ERSS Validation Study 10
Current Med Bn – 1 RCT
SBA.1 1RSP.1 BAS.1
Medical Capability• SC- provides:
– More holding (40 beds)– Combat Stress Platoon available– Ancillary support
Evacuation• If SC- “closed” and patient WIA, then evac to theater hospital.• If SC- “closed” and patient DNBI, then evac to Surgical Co in CLR(GS).• Evacuate patients requiring specialty care (neuro need, etc) to theater hospital.• Evacuate moderate to severe mental health patients from BASs to Surgical Co in CLR(GS).• Far-forward evacuation assets will include 2 dedicated CH-53s and 2 dedicated MV-22s per RCT.
– Based at SC-.1 (Co-locate these dedicated evacuation assets with the RCT)– Increase this number as needed to avoid shortfalls in tactical evacuation
• Sufficient ground vehicles to handle all requests from 1RSP to BAS.• Sufficient helos to handle all requests from FRSS and FSC
Maneuver• The FRSS will maneuver with the supported RCT, and will always be within 30 minutes flying time
from the RCT. Two maneuvers will occur. Both during a lull in operations.
FRSS/STP.2 SC-.2SBA.2 1RSP.2 BAS.2
SBA.3 1RSP.3 BAS.3
TH.1
5 min
5 min
Sufficient ground vehicles to handle all requests from 1RSP to BAS.
30 min
Sufficient helos to handle all requests from FRSS and FSC to theater hospital.
1 hr
1 hr
1 hr
1 hr
ERCS
2 hr
2 hr
2x MV-22 2x CH-53
MV-22Speed: 275 mphCapacity (amb, litter): 24 or 12 maxLoad (amb, litter): 2 & 3 minUnload (amb, litter): 2 & 3 minPre-Mission: 30 minPost-Mission: 30 minWait Time: 0 min
CH-53ESpeed: 170 mphCapacity (amb, litter): 19 & 8 combinedLoad (amb, litter): 2 & 3 minUnload (amb, litter): 2 & 3 minPre-Mission: 30 minPost-Mission: 30 minWait Time: 0 min
Route LegendAir CASEVACERCS
SCCLR (GS)
30 min
2 hr
5 min
5 min
Sufficient helos to handle all requests, if necessary.
MV-22
• CLR (GS) provides: – Surge capacity
1 hr
CLC CLB(DS) CLR(GS)

2006-09-07 ERSS Validation Study 11
Casualty Flow Details – Current Med Bn
FRSS/STP
BAS SC- TheaterHospital
POI
SCCLR (GS)
Specialty Care• Neuro – 25 PCs• Neuropsychiatric – 4 PCs • Ophthalmology – 9 PCs• Optometry – 2 PCs
Surgical – 59 PCs
DNBIs when SC- busy
Surgical – 72 PCsMental Health – 12 PCsVarious – 237 PCs
ERCS
ERCSWIAs when SC- busy
CLB(DS)
CLC
ERC assets are for post-surgical patients who require a ventilator.

2006-09-07 ERSS Validation Study 12
OAG COA with BAS to STP/FRSS – 1 RCT
SBA.1 1RSP.1 BAS.1
FRSS/STP.2SBA.2 1RSP.2 BAS.2
SBA.3 1RSP.3 BAS.3
TH.1
5 min
5 min
Sufficient ground vehicles to handle all requests from 1RSP to BAS.
Sufficient helos to handle all requests from FRSS to theater hospital.
ERCS
Route LegendAir CASEVAC
Med Sec H&S2 hr
2 hr
2 hr
5 min
5 min
10 min
5 min
5 min
FRSS/STP.1
FRSS/STP.3
Medical Capability• Theater Hospital provides:
– Surge capacity– Post surgical support
Evacuation• Evacuate post surgical patients to theater hospital.• Sufficient ground vehicles to handle all requests from 1RSP to BAS to FRSS/STP.• Sufficient helos to handle all requests from FRSS/STP to theater hospital
Maneuver• The FRSS will maneuver with the supported RCT, and will always be within 30 minutes flying time
from the RCT.
• H&S Medical Section : – Full medical capability
CLC CLR(GS)
Post-Surgery to TH
2 hr
2 hr
2 hr

2006-09-07 ERSS Validation Study 13
Casualty Flow Details – OAG COA with BAS to STP/FRSS
FRSS
BAS
TheaterHospital
POI
Med Sec (H&S)
Surgical – 59 PCs
STP
All other PCs
Post-Surgical – 59 PCs
All other PCs
Specialty Care• Neuro – 25 PCs• Neuropsychiatric – 4 PCs • Ophthalmology – 9 PCs• Optometry – 2 PCs
CLR(GS)
CLC
ERC assets are for post-surgical patients who require a ventilator.

2006-09-07 ERSS Validation Study 14
Proposed OAG COA Med Bn
Medical Battalion760 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Headquarters & Service Company
352 PAX
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 80 BEDS / 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
HSS OAG COA 1 Nov.ppt and MBCE HSS COA T_O_Revised.xls

2006-09-07 ERSS Validation Study 15
Proposed OAG COA Med BnForward Surgical Company (FSC)
FRSS #18 PAX
FRSS #28 PAX
FRSS #38 PAX
STP #118 PAX
STP #218 PAX
STP #318 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
Ancillary ServicesPlatoon
X-Ray #16 PAX
AmbulancePlatoon
AMB #13 PAX
ERCS #12 PAX
ERCS #22 PAX
ERCS #32 PAX
ERCSPlatoon
HeadquartersPlatoon26 PAX
DentalSection17 PAX
HSS OAG COA 1 Nov.ppt and MBCE HSS COA T_O_Revised.xls
FSC
Navy Personnel Only.
Medical Battalion760 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Headquarters & Service Company
352 PAX
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 80 BEDS / 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS

2006-09-07 ERSS Validation Study 16
Ward-411 PAX
Ward-311 PAX
Proposed OAG COA Med Bn – H&S CompanyMedical Battalion
760 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Headquarters & Service Company
352 PAX
H&S Med Section MEU CLB DETS
H&S Company Section
2 PAX
S-1Section
7 PAX
S-2/S-3Section
9 PAX
Patient Evac Team7 PAX
S-4Section
7 PAX
HeadquartersSection
5 PAX
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 80 BEDS / 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
Prev MedSection31 PAX
ChaplainSection
2 PAX
MEU CLB Dets-120 PAX
MEU CLB Dets-220 PAX
MEU CLB Dets-320 PAX
FRSS-18 PAX
FRSS-28 PAX
FRSS-38 PAX
STP-118 PAX
STP-218 PAX
STP-318 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
Ancillary ServicesPlatoon
ERCS-12 PAX
ERCS-22 PAX
ERCS-32 PAX
ERCSPlatoon
DentalSection
6 PAX
Combat StressPlatoon
Stress-16 PAX
Stress-26 PAX
Stress-36 PAX
Lab-16 PAX
Xray-23 PAX
Xray-13 PAX
Lab-26 PAX
Lab-46 PAX
Lab-36 PAX
HSS OAG COA 1 Nov.ppt and MBCE HSS COA T_O_Revised.xls
H&S Company
Ward-211 PAX
Ward-111 PAX
Ward-810 PAX
Ward-710 PAX
Ward-610 PAX
Ward-510 PAX
Navy Personnel Only.

2006-09-07 ERSS Validation Study 17
TML+ Modeled Med Bn Capabilities
FSC
FRSS #18 PAX
FRSS #28 PAX
STP #118 PAX
STP #218 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
Ancillary ServicesPlatoon
X-Ray #16 PAX
AmbulancePlatoon
AMB #13 PAX
ERCS #12 PAX
ERCS #22 PAX
ERCSPlatoon
HeadquartersPlatoon26 PAX
2 STPs / 2 FRSS 2 OR Tables8 Temporary Holding Beds20 COTS2 ERCS
FSC
DentalSection17 PAX
Medical Battalion760 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Headquarters & Service Company
352 PAX
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 80 BEDS / 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
FRSS #38 PAX
STP #318 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
ERCS #32 PAX
ERCSPlatoon
FRSS/STP
FRSS/STP
1 STP / 1 FRSS 1 OR Table4 Temporary Holding Beds10 COTS1 ERCS

2006-09-07 ERSS Validation Study 18
TML+ Modeled Med Bn Capabilities (continued)
H&S Med Section
H&S Med Section
FRSS-18 PAX
FRSS-28 PAX
STP-118 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
Ancillary ServicesPlatoon
ERCS-12 PAX
ERCS-22 PAX
ERCS-32 PAX
ERCSPlatoon
Combat StressPlatoon
Stress-16 PAX
Stress-26 PAX
Stress-36 PAX
Lab-16 PAX
Xray-23 PAX
Xray-13 PAX
Lab-26 PAX
Lab-46 PAX
Lab-36 PAX
Ward-810 PAX
Ward-710 PAX
Ward-610 PAX
Ward-510 PAX
1 STPs / 2 FRSS 2 OR Tables8 Temporary Holding Beds40 Beds / 10 COTS3 ERCS
DentalSection
6 PAX
Unused Capability Sets
-1 FRSS
-2 STPs (Total: 20 COTS)
-4 Wards (Total: 40 Beds)
Medical Battalion760 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Forward Surgical Company
136 PAX
Headquarters & Service Company
352 PAX
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 30 COTS3 ERCS
3 STPs / 3 FRSS 80 BEDS / 30 COTS3 ERCS
2006-09-07 ERSS Validation Study 19
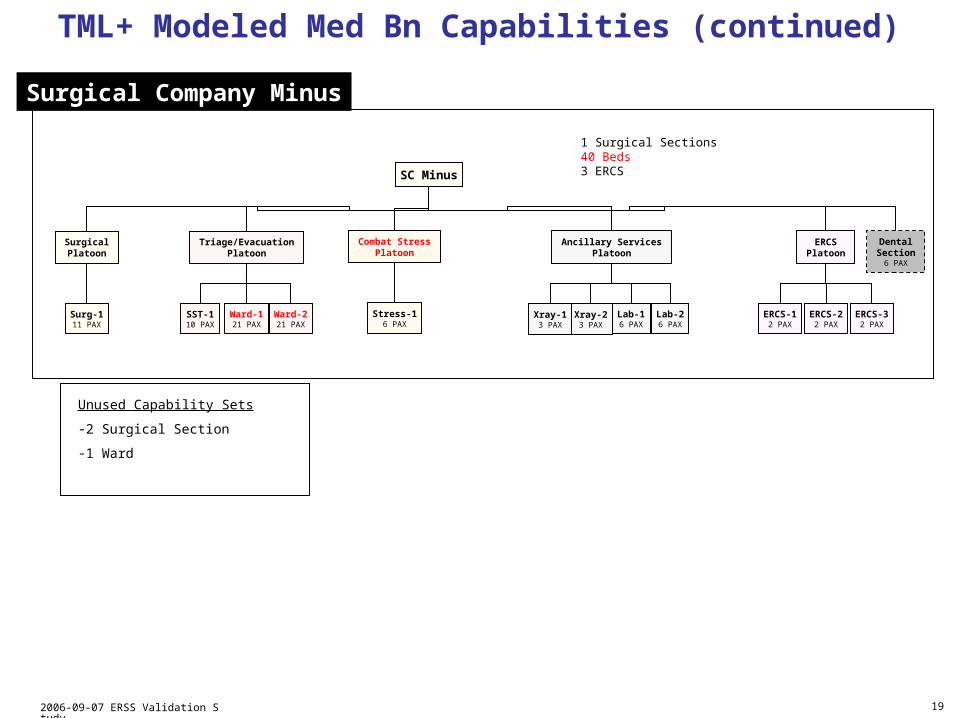
TML+ Modeled Med Bn Capabilities (continued)
Surgical Company Minus
SC Minus
Surg-111 PAX
SST-110 PAX
SurgicalPlatoon
Triage/EvacuationPlatoon
Ancillary ServicesPlatoon
ERCS-12 PAX
ERCS-22 PAX
ERCS-32 PAX
ERCSPlatoon
Lab-16 PAX
Xray-23 PAX
Xray-13 PAX
Lab-26 PAX
Ward-221 PAX
Ward-121 PAX
1 Surgical Sections 40 Beds3 ERCS
Combat StressPlatoon
Stress-16 PAX
Unused Capability Sets
-2 Surgical Section
-1 Ward
DentalSection
6 PAX

2006-09-07 ERSS Validation Study 20
MCO Casualty Stream

2006-09-07 ERSS Validation Study 21
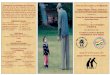
MCO Casualty Stream• Casualty Stream from OSD’s Medical Readiness Review (MRR)
– Based on Medical Analysis Tool (MAT) modeling of Level III requirements for each Service in a 2012 MCO DPS– Represents USMC Level III Admissions for 5 RCTs in high intensity combat in MCO DPS
– Focused on 3 RCTs conducting operations ashore– First 180 days of MCO
Admissions at Level III
0
50
100
150
200
250
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 160 170Day
Nu
mb
er
Total
WIA
DNBI
WIAs 1249DNBIs 4020Total 5269
Represents 5 RCTs• 3 Ashore
Our focus was on the 30 days of combat operations ashore (15 days prior to casualty peak and 15 days after)

2006-09-07 ERSS Validation Study 22
Casualty Occurrence at Level I (3 RCTs)
0
50
100
150
200
250
76 78 80 82 84 86 88 90 92 94 96 98 100 102 104 106
Day
Nu
mb
er
Total
WIA
DNBI
Admissions at Level III (3 RCTs)
0
50
100
150
200
250
76 78 80 82 84 86 88 90 92 94 96 98 100 102 104 106
Day
Nu
mb
er
Total
WIA
DNBI
Med Bn Validation Casualty Stream• MedBn Validation Casualty Stream
– Based on MBCE Casualty Stream from Medical Readiness Review (MRR)– MCO 30 days (15 days prior to casualty peak, 15 days after)– Casualties evenly distributed across areas of operations– Conversion formulas from admissions to casualty occurrences at Level 1 based on OIF-1 data
—Total WIAs = 1.4 * Level 3 WIAs—Total DNBI = 1.7 * Level 3 DNBIs
– MRR DNBI count split 53% Disease, 35% NBI, and 12% Battle Fatigue
* Level I is First Responder
WIAs 737DNBIs 634Total 1371
WIAs 1032DNBIs 1056Total 2088
15 days prior 15 days after
91
15 days prior 15 days after
91

2006-09-07 ERSS Validation Study 23
Trauma Category WWII Korea VietnamDesert Storm
USMCOIF-1
USMCOIF-2
Amputations 1.8% 1.4% 1.9% 1.5% 3.4% 3.6%
Burns 1.0% 1.0% 1.4% 3.7% 3.0% 4.6%
Intracranial injuries 1.4% 2.3% 1.3% 1.5% 2.6% 3.3%
Crush injuries 0.0% 0.0% 0.0% 3.0% 1.6% 1.0%
Dislocation 0.1% 0.1% 0.5% 0.0% 2.6% 0.8%
Fractures 21.8% 23.0% 16.3% 17.8% 22.1% 33.0%
Sprains/strains 3.1% 2.8% 1.4% 6.7% 3.8% 1.7%
All wounds/single/multiple 63.7% 67.9% 76.5% 56.3% 54.0% 41.8%
Other 7.1% 1.5% 0.7% 9.6% 6.9% 10.1%
Total 100.0% 100.0% 100.00% 100.0% 100.0% 100.0%
Distribution Among WIA Casualties from Major Combat Operations
Will use USMC OIF-1 distribution to determine Patient Condition Codes (PCCs).
Sources: OIF-1 (19 Mar 03 – 30 Apr 03) data are from Surgical Companies, Personnel Casualty Reports, TRAC2ES data.OIF-2 (1 Mar 04 – 30 Apr 05) data are from Joint Patient Tracking Application.

2006-09-07 ERSS Validation Study 24
Distribution Among NBI Casualties from Major Combat Operations
Trauma Category WWII Korea VietnamDesert Storm
USMC OIF-1
USMC OIF-2
Amputations 0.8% 1.0% 1.4% 0.0% 1.2% 0.3%
Burns 6.4% 6.8% 6.0% 5.2% 1.1% 6.0%
Concussions 2.1% 0.9% 2.1% 0.0% 3.0% 1.0%
Crushing/contusions 0.5% 11.8% 4.6% n/a 4.1% 1.4%
Dislocations 2.4% n/a 5.1% 8.6% 11.1% 9.0%
Effects of cold 4.8% 15.8% 3.3% n/a 0.0% 0.0
Effects of heat 1.2% 0.9% 7.4% n/a 1.0% 2.3%
Fractures 19.6% 18.2% 20.1% 33.1% 37.2% 45.5%
Sprains/strains 20.3% 17.0% 13.8% 24.3% 26.2% 17.9%
Wounds all types 34.4% 18.3% 29.8% 18.2% 14.1% 12.3%
Other 7.5% 9.3% 6.2% 10.0% 1.0% 4.3%
Total 100.0% 100.0% 100.00% 100.0% 100.0% 100.0%
Will use USMC OIF-1 distribution to determine Patient Condition Codes (PCCs).
Sources: OIF-1 (19 Mar 03 – 30 Apr 03) data are from Surgical Companies, Personnel Casualty Reports, TRAC2ES data.OIF-2 (1 Mar 04 – 30 Apr 05) data are from Joint Patient Tracking Application.

2006-09-07 ERSS Validation Study 25
Distribution Among DIS Casualties from Major Combat Operations
ICD Category Korea VietnamDesert Storm
USMC OIF-1
USMC OIF-2
Infectious/Parasitic 12.2% 29.2% 5.1% 1.0% 2.8%
Neoplasm 1.6% 1.7% 0.4% 0.0% 1.9%
Endocrine 2.2% 0.8% 1.2% 4.9% 2.1%
Mental Disorders 8.0% 6.9% 5.6% 7.8% 9.4%
Nervous System 8.7% 6.0% 6.2% 6.8% 12.8%
Circulatory 3.4% 2.4% 5.9% 7.8% 3.6%
Respiratory 23.7% 6.3% 8.2% 3.9% 2.8%
Digestive 9.5% 8.4% 15.1% 24.3% 16.2%
Genitourinary 5.5% 3.8% 7.5% 12.6% 7.7%
Skin/Subcutaneous 9.2% 11.6% 10.1% 6.8% 6.2%
Musculoskeletal 4.5% 5.1% 23.1% 12.6% 20.7%
Symptoms/ill-defined conditions 11.1% 17.2% 11.5% 11.7% 13.9%
Total 100.0% 100.00% 100.0% 100.0% 100.0%
Will use USMC OIF-1 distribution to determine Patient Condition Codes (PCCs).
Sources: OIF-1 (19 Mar 03 – 30 Apr 03) data are from Surgical Companies, Personnel Casualty Reports, TRAC2ES data.OIF-2 (1 Mar 04 – 30 Apr 05) data are from Joint Patient Tracking Application.
2006-09-07 ERSS Validation Study 26
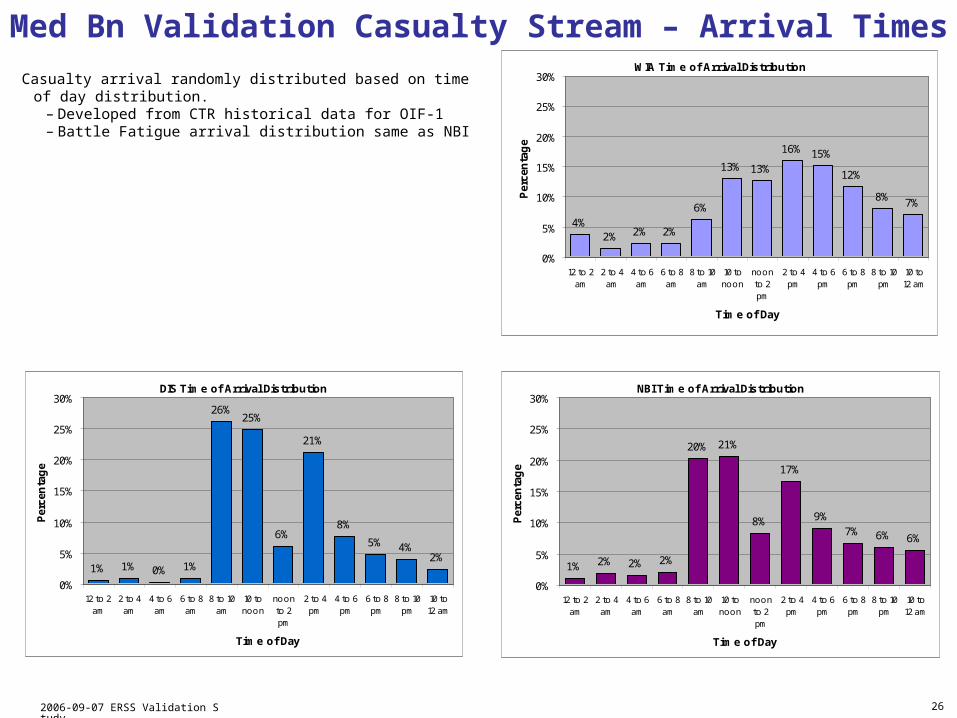
Med Bn Validation Casualty Stream – Arrival Times
Casualty arrival randomly distributed based on time of day distribution.– Developed from CTR historical data for OIF-1– Battle Fatigue arrival distribution same as NBI
WIA Time of Arrival Distribution
4%2% 2% 2%
6%
13% 13%
16% 15%
12%
8% 7%
0%
5%
10%
15%
20%
25%
30%
12 to 2am
2 to 4am
4 to 6am
6 to 8am
8 to 10am
10 tonoon
noonto 2pm
2 to 4pm
4 to 6pm
6 to 8pm
8 to 10pm
10 to12 am
Time of Day
Per
cen
tag
e
DIS Time of Arrival Distribution
1% 1% 0% 1%
26%25%
6%
21%
8%
5% 4%2%
0%
5%
10%
15%
20%
25%
30%
12 to 2am
2 to 4am
4 to 6am
6 to 8am
8 to 10am
10 tonoon
noonto 2pm
2 to 4pm
4 to 6pm
6 to 8pm
8 to 10pm
10 to12 am
Time of Day
Per
cen
tag
e
NBI Time of Arrival Distribution
1% 2% 2% 2%
20% 21%
8%
17%
9%7% 6% 6%
0%
5%
10%
15%
20%
25%
30%
12 to 2am
2 to 4am
4 to 6am
6 to 8am
8 to 10am
10 tonoon
noonto 2pm
2 to 4pm
4 to 6pm
6 to 8pm
8 to 10pm
10 to12 am
Time of Day
Per
cen
tag
e

2006-09-07 ERSS Validation Study 27
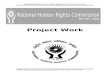
TML+ Estimated Casualty Stream
49%
27%
18%
6%
WIA
DIS
NBI
BF
10%
19%
71%
High
Medium
Low
Percentage of Casualties by Type
Casualties by Mortality Risk
219.965.3
35.8
1883.3
0
400
800
1200
1600
2000
Non-Life Threatening Life Threatening
Num
ber
NLT
High
Medium
Low
87%
13%
Percentage of Life Threatening Casualties
Sources: Modeling Dynamic Casualty Mortality Curves in the TML+ planning tool. NHRC Technical Report 04-31.Simulating Dynamic Mortality within the military medical chain of evacuation and treatment. Proceedings of SCS Spring Sim 2006.
50 Replications
50 Replications
50 Replications
Casualty Type
% Mean95th
Percentile Min Max
WIA 49% 1010.8 1065.1 902 1095
DIS 27% 557.5 592.0 504 599
NBI 18% 369.6 394.6 335 398
BF 6% 126.7 142.3 108 149
Total 100% 2088.9 2173.5 1979 2214
Mortality Risk
% Mean95th
Percentile Min Max
NLT 87% 1808.5 1883.3 1715 1915
LT 13% 280.4 307.1 238 317
Total 100% 2088.9 2173.5 1979 2214
NLT Non-Life ThreateningLT Life Threatening
High Probability LT patient dies in 1st hour without any treatment (>=2/3)Medium Probability LT patient dies in 1st hour without any treatment (>=1/3 and < 2/3)Low Probability LT patient dies in 1st hour without any treatment (<1/3)
Mortality Risk
% Mean95th
Percentile Min Max
High 10% 27.7 35.8 18 39
Medium 19% 54.1 65.3 37 71
Low 71% 198.6 219.9 170 221
Total 100% 280.4 307.1 238 317

2006-09-07 ERSS Validation Study 28
17.5%
9.1%7.7% 7.0%
4.7% 4.4%2.7% 2.3% 2.2% 2.0% 1.8% 1.7% 1.7% 1.4% 1.4% 1.3% 1.2% 0.7% 0.4% 0.2% 0.2%
28.2%
0%
5%
10%
15%
20%
25%
30%O
pe
nW
ou
nd
s
Fra
ctu
res
Sp
rain
s &
Str
ain
s
Me
nta
lD
iso
rde
rs
Dig
est
ive
Ge
nito
uri
na
ry
Cir
cula
tory
Ski
n
Dis
loca
tion
s
Am
pu
tatio
ns
Infe
ctio
us
Mis
c
Bu
rns
Re
spir
ato
ry
Cru
shIn
juri
es
Intr
acr
an
ial
Inju
rie
s MIW
He
ari
ng
Ne
op
lasm
Vis
ua
l
Bite
s &
Stin
gs
He
at
PC Category
Pe
rce
nta
ge
TML+ Estimated Casualty Stream (continued)
Top 10 Categories
Percentage of Casualties by PC Category
Category % Mean95th
Percentile Min Max
Open Wounds 28.2% 589.0 627.4 541 657Fractures 17.5% 365.8 399.3 313 411Sprains & Strains 9.1% 190.5 213.1 162 218Mental Disorders 7.7% 159.9 179.2 137 191Digestive 7.0% 146.7 166.2 118 167Genitourinary 4.7% 99.0 111.8 85 118Circulatory 4.4% 92.9 109.1 76 119Skin 2.7% 57.3 72.9 41 84Dislocations 2.3% 48.8 59.8 37 65Amputations 2.2% 46.8 59.3 34 65
… … … … … …Total 100% 2173.5 1979 2214
50 Replications
Categories based on ICD-9 classifications and sub-classifications

2006-09-07 ERSS Validation Study 29
Results
• Mortality• Casualty Flow Statistics
Summary from Casualty Stream Slides
• Number of casualties from the MCO DPS
• Calculation of Level 1 occurrences from OIF1 data
• Patient condition code distribution from OIF1 data
• Casualty arrival times from OIF1 data

2006-09-07 ERSS Validation Study 30
Medical System Effectiveness – Mortality
The OAG COA and Current Med Bn are statistically equivalent for mortality. Deploying the FRSSs with the BAS saves 6% more lives.
Metrics
MCO WIAs
OAG COA Current Med BnOAG COA
Night Air Evac
OAG COABAS to STP/FRSS
DOWPercent (Mean / 95th) 4.6% / 5.9% 4.6% / 5.8% 5.9% / 7.4% 4.4% / 5.4%
Values (Mean / 95th) 47 / 60 47 / 59 60 / 75 44 / 55
Total WIAs Values (Mean / 95th) 1008 / 1066 1008 / 1066 1004 / 1065 1012 / 1067
Metrics
MCO Casualties
OAG COA Current Med BnOAG COA
Night Air Evac
OAG COABAS to STP/FRSS
% DOW Percent (Mean / 95th) 2.4% / 3.0% 2.4% / 3.0% 3.1% / 3.9% 2.3% / 2.8%
Total Casualties
Values (Mean / 95th) 2086 / 2165 2086 / 2165 2083 / 2158 2089 / 2174
The 95th percentile provides the decision maker an extra measure of risk mitigation.
50 Replications
50 Replications
2006-09-07 ERSS Validation Study 31
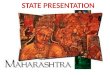
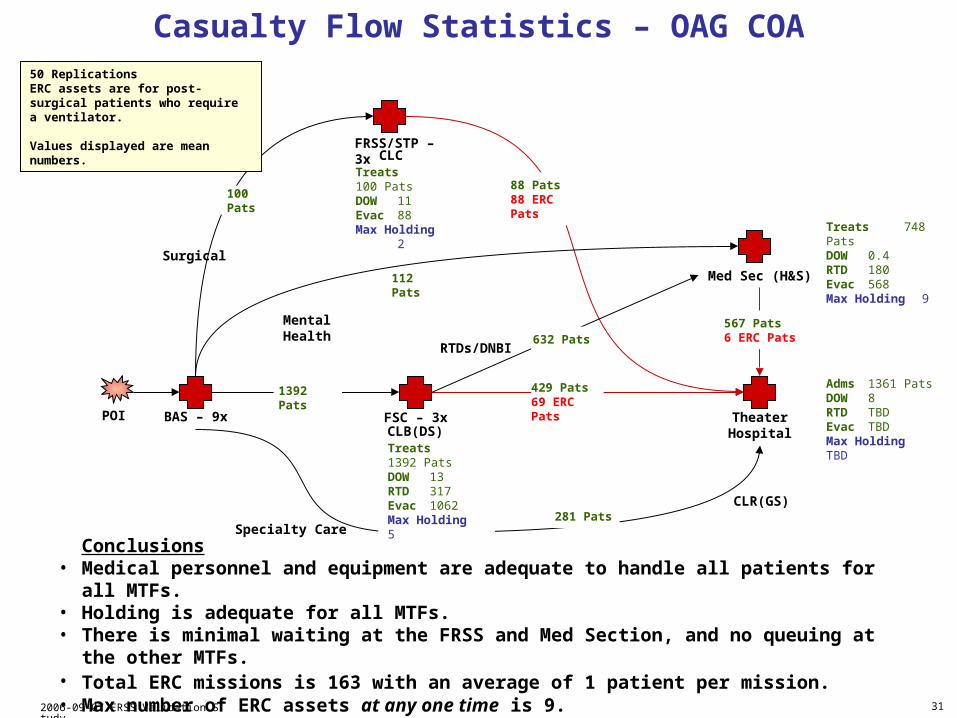
RTDs/DNBI
Casualty Flow Statistics – OAG COA
TheaterHospital
POI
Med Sec (H&S)
88 Pats88 ERC Pats100 Pats
1392 Pats
Treats 748 PatsDOW 0.4RTD 180Evac 568Max Holding 9
632 Pats
Specialty Care
Surgical
Mental Health
Conclusions• Medical personnel and equipment are adequate to handle all patients for all MTFs.• Holding is adequate for all MTFs. • There is minimal waiting at the FRSS and Med Section, and no queuing at the other MTFs. • Total ERC missions is 163 with an average of 1 patient per mission. • Max number of ERC assets at any one time is 9.• Maximum number of ERC assets required in a 24 hr period is 9 at one peak day.
Adms 1361 PatsDOW 8RTD TBDEvac TBDMax Holding TBD
Treats 100 PatsDOW 11Evac 88Max Holding 2
Treats 1392 PatsDOW 13RTD 317Evac 1062Max Holding 5
112 Pats
281 Pats
429 Pats69 ERC Pats
567 Pats6 ERC Pats
50 ReplicationsERC assets are for post-surgical patients who require a ventilator.
Values displayed are mean numbers.
CLB(DS)
CLR(GS)
CLC
BAS – 9x
FRSS/STP – 3x
FSC – 3x

2006-09-07 ERSS Validation Study 32
Conclusion
• Given the assumptions, the OAG COA to restructure the MedBn has the medical capability and capacity to support a “MEF in the assault” in the most demanding DPS MCO scenario.
• The OAG COA to restructure the MedBn provides a decrease in the DOWs (6%) compared to the current MedBn in the DPS MCO scenario.
• With tactical evacuation limited to 12 hours per day, the OAG COA has the medical capability and capacity to support a “MEF in the assault” in the most demanding DPS MCO scenario.
• The OAG COA to restructure the MedBn provides increased flexibility to task organize the direct support and general support capability sets.
• Since the TML+ modeling was based on a DPS MCO future scenario, you cannot conclude the restructured MedBn has the medical capability or capacity to support a “MEF in the assault” in the current MCO OPLANs
• Since the TML+ modeling was based on a MCO scenario, you cannot conclude the restructured MedBn has the medical capability or capacity to support other types of operations across the range of military operations