Embed Size (px)
Citation preview

Medical Care Utilization and theTranscendental Meditation Program
DAVID ORME-JOHNSON, PHD
This field study compared 5 years of medical insurance utilization statistics of approximately2000 regular participants in the Transcendental Meditation (TM) program with a normativedata base of approximately 600,000 members of the same insurance carrier. The benefits, de-ductible, coinsurance terms, and distribution by gender of the TM group were very similar tothe norm, yet the TM group had lower medical utilization rates in all categories. Inpatient daysper 1000 by age category were 50.2% fewer than the norm for children (0-18), 50.1% fewer foryoung adults (19-39), and 69.4% fewer for older adults (40 + ). Outpatient visits per 1000 forthe same age categories were, respectively, 46.8%, 54.7%, and 73.7% fewer. When comparedwith five other health insurance groups of similar size and professional membership, the TMgroup had 53.3% fewer inpatient admissions per 1000 and 44.4% fewer outpatient visits per1000. Admissions per 1000 were lower for the TM group than the norm for all of 17 majormedical treatment categories, including -55.4% for benign and malignant tumors, -87.3% forheart disease, - 30.4% for all infectious diseases, - 30.6% for all mental disorders, and - 87.3%for diseases of the nervous system. However, the TM group's admissions rates for childbirthwere similar to the norm. The issue of self-selection is addressed in terms of previous medicalresearch in this area.
The U.S. Public Health Service's Cen-ters for Disease Control estimates that halfof the mortalities from the ten leadingcauses of death can be linked to behaviorand life-style (1). A review of 25 studiesconcludes that treatment for alcohol abuse,drug abuse, or mental treatment (ADM im-pact) generally reduces medical care uti-lization [2). Although none of these stud-ies used randomized clinical trials, 13studies did use a comparison group, in-dicating reduced medical care utilizationby about 20% in the treatment group com-pared to. controls. These studies focused
From the Department of Psychology, Maharishi In-ternational University.
Address reprint requests to: David Orme-Johnson,Ph.D., Chairman, Department of Psychology, Mahar-ishi International University, Fairfield, IA 52556.
Received for publication December 15, 1986; re-vision received March 10, 1987.
primarily on outpatient psychotherapy,mostly in organized health maintenanceorganizations (HMOs) or in alcoholismtreatment provided for employees or pro-vided by HMOs.
A more recent review of 58 studies foundreductions in use of medical services as-sociated with inpatient rather than out-patient mental health care, particularly forpersons over 55 years of age (3). Twenty-two random assignment studies reviewedindicated a 10.4% mean reduction in in-patient hospitalization compared with33.1% mean reduction in 26 time seriesstudies in which patients had self-selectedpsychotherapy treatment. Both changeswere statistically significant, indicating thatself-selection studies yield reliable infor-mation, albeit a larger effect size. A meta-analysis of 49 experiments on the effectsof psychoeducational interventions withsurgical patients indicated that method ofsubject assignment was not systematically
Psychosomatic Medicine 49:493-507 (1987)
Copyright © 1987 by the American Psychosomatic Society, InPublished by Elscvier Science Publishing Co , Inc52 Vanderbilt Avenue, New York, NY 10017
493
0033-3174/87/S3 50

D. ORME-JOHNSON
related to effect size, i.e., the outcomes weresimilar for random assignment and self-selection studies (4).
The present study analyzes 5 years ofmedical care utilization statistics from amajor health insurance carrier on a self-selected group of approximately 2000 par-ticipants in the Transcendental Medita-tion (TM) program of Maharishi MaheshYogi (5). There are about two million TMmeditators worldwide and the TM tech-nique is not a therapeutic modality per sebut is offered to the general public as ameans of self-actualization (5). It is taughtin seven systematic steps, which includeintroductory and preparatory lectures,personal interview and personal instruc-tion, and verification and validation of ex-periences of the first 3 days of meditation(6, p. 6). The technique is taught by qual-ified teachers trained by Maharishi and itis described as "an effortless procedure forallowing the excitations of the mind grad-ually to settle down until a least excitedstate of mind is reached" (6, p. 123).
The TM program consists of the regularpractice of the TM technique 15-20 mintwice a day. It is practiced at home, in theoffice, or wherever is convenient. It doesnot require any special treatment setting,and although a quiet place is best, it canalso be practiced successfully in noisy en-vironments such as a bus, commuter train,or airplane.
Physiologic research shows that the TMtechnique produces a state of "restfulalertness" (7, 8). Rest is indicated by re-duced minute ventilation, respiration rate,plasma lactate levels, and spontaneous skinresistance responses and increased basalskin resistance relative to eyes-closed restin nonmeditating control subjects (7-9).Alertness or inner awareness is indicatedby increased alpha band EEG power (7, 8)and coherence (10). Subjective experi-
ences of a "least excited state of mind,"also referred to as transcendental con-sciousness, are highly correlated withslowing of respiration and increased EEGcoherence over all frequencies and deri-vations (11, 12).
It has been proposed that the state ofrestful alertness gained during the TMtechnique optimizes the efficiency of theinnumerable intrinsic self-repair mecha-nisms of the body (9). Subsequent nor-malization of accumulated physiologic in-balances through the technique could thusbe expected to help maintain good health.A number of experiments using randomassignment as well as other research de-signs have demonstrated that the TM pro-gram does have an impact on alcohol use(13-15), drug abuse (13, 14, 16, 17), andcigarette smoking (13, 14, 18), as well ason mental health (17, 19, 20).
For example, Brooks and Scanaro (19)randomly assigned 18 Vietnam veteransseeking treatment for post-Vietnam ad-justment symptoms to either the TM pro-gram or psychotherapy. After 3 months theTM group showed significant improve-ments relative to the psychotherapy group,as indicated by reductions in emotionalnumbness, alcohol abuse, insomnia,depression, anxiety, and severity of de-layed stress syndrome, and improved em-ployment status. In addition, habituationof the skin resistance response to a loudtone (a physiologic measure of stress reac-tivity) was faster in the TM group on post-test relative to pretest, whereas no changewas observed in the psychotherapy group,indicating more rapid recovery from stressin the meditators.
A meta-analysis of 66 longitudinal andcross-sectional studies on anxiety and otheraffective outcomes, controlling for popu-lation, experimental design, duration oftreatment, demand characteristics, pay-
494 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
ment of fees, experimenter attitude, typeof publication, and attrition, found that theTM program had twice the effect size asother meditation or relaxation techniques,whether or not the studies were matchedon possible confounding variables (20).
"Sense of coherence" is a personalityfactor that has been found to have an im-pact on health. It is defined as the abilityto make cognitive sense of stimuli, to per-ceive resources as adequate and to makeemotional sense of the environment (21).Several studies indicate that the TM pro-gram increases these factors. One studyrandomly assigned 60 high school stu-dents to either the TM technique or theTM technique plus SCI (Science of Crea-tive Intelligence, a course on the displayof intelligence in nature), or SCI alone, andanother 20 subjects served as a no-treat-ment control group (22). After a 14-weekexperimental period those participating inthe TM technique (with or without SCI)showed a significant improvement relativeto SCI alone or the no-treatment controlgroup on intelligence (Raven ProgressiveMatrices), creativity, ability to work withcomplex and abstract situations, energylevel, innovation, self-esteem, tolerance,and anxiety.
One measure of perceptual and cogni-tive coherence is field independence, theability to disembed target stimuli from high"noise" backgrounds. In one study, 40 sub-jects were randomly assigned to either theTM program or a control group. After a 3-month experimental period the TM groupsignificantly improved on three indices offield independence, indicating increasedperceptual and cognitive structuring abil-ity (23).
Another study demonstrating increased"sense of coherence" found support for thehypothesis that the TM technique reduceshabitual patterns of perceptual activation,
resulting in 1) more effective applicationof schemata to new information and 2) lessdistracting mental activity during perfor-mance (24). Signal detection analysis in-dicated that in contrast to two control con-ditions (ordinary relaxation or reading) theTM technique had immediate and longi-tudinal effects of improving detection ofnovel stimuli that could not be attributedto response bias.
These studies demonstrating ADM im-pact and increased sense of coherence sug-gest that the TM program might engendersuccessful aging, which is perhaps the ul-timate test of well-being. A cross-sectionalstudy (25) showed a lower level of biologicaging in TM participants (n = 84, meanage 53 years) relative to controls as mea-sured by systolic blood pressure, auditorythreshold, and near point vision. Anotherstudy (26) extended this finding by ran-domly assigning 73 residents of homes forthe elderly to either a no-treatment con-dition, or to one of three treatments de-signed to be equivalent in external struc-ture and expectation-fostering features—the TM program, an active thinking pro-cedure, and a relaxation program. After a3-month experimental period the TM grouphad significantly improved in comparisonto one or more treatment conditions onthree measures of cognitive flexibility, onword fluency, systolic blood pressure, self-report measures of behavioral flexibility,aging, and in nurse's rating of mental health(the last after 18 months). The most strik-ing finding is that all members of the TMgroup were still alive 3 years after the pro-gram began, in contrast to other groupsand to the 62.5% survival rate for the re-maining population in the homes for theelderly.
Other medical research indicating thatthe TM program improves health has showndecreased bronchial asthma (27), de-
Psychosomatic Medicine 49:493-507 (1987) 495

D. ORME-JOHNSON
creased blood pressure in hypertensivesubjects (28-30), decreased serum choles-terol levels in normal and hypercholester-olaemic patients (31), and reduced insom-nia (32).
The present study complements thisprevious laboratory research by being thefirst large-scale field study of the effects ofthe TM program on general health.
METHODS
This study examined the medical care utilizationstatistics over a 5-year period for the SCI InsuranceGroup, which is based in Fairfield, Iowa, but whosemembership is 80% out of state, distributed through-out the United States. The only requirement for mem-bership in the SCI health insurance group is that theindividual (and all family members of age 10 andolder] have practiced the Transcendental Mediata-tion technique regularly for at least 6 months priorto enrollment. In order to remain eligible for partic-ipation in the health insurance plan and its benefits,SCI members are required to continue to regularlypractice the TM technique. Participation in the TMprogram in no way biased the availability of any typesof medical treatment; it was only the criterion ofmembership in the SCI health insurance group.
SCI is one of many health insurance groups be-longing to a major health insurance carrier of Iowahereafter referred to as "MIC."1 MIC's total member-ship numbered from 600,000 to 700,000 during theperiod of the experiment. MIC is not an HMO, but ahealth insurance carrier whose member companies,such as SCI, offer prepaid health insurance plans forthe usual medical, surgical, and obstetric services.Sixty percent of the health insurance policies offeredby the different groups with MIC have a $100 to $200deductible, and 80% of MIC's business is with an 80/20 coinsurance plan.
Semiannually the MIC actuarial services send eachgroup in its membership a standard report on ac-
'More detailed information about the SCI healthinsurance group and MIC can be obtained from DickAlexander, President, SCI Insurance Group, 2nd andBroadway, Fairfield, IA 52556.
count-specific utilization and charge indicators forthat group compared to all other groups with MIC.The statistics reported in this article were taken fromthe MIC's standard reports sent to the SCI healthinsurance group from 1981 to 1985. In these reports,SCI's medical utilization rates in different categorieswere compared with the mean of all other groups.These normative data for all other groups is basedon MIC's 600,000 plus membership and is referredto as Group Business. In addition, MIC's actuarialservices provided statistics comparing the SCI groupwith five other health insurance groups specificallyselected to be of similar size and professional mem-bership as SCI.
SCI's membership enrollments were 694, 1123,1395, 2119, and 2011 for 1981 to 1985, respectively.The terms of SCI's insurance policy were typical orbetter than the other groups represented by GroupBusiness. For the majority of the study, SCI membershad a $100 deductible with a 80/20 coinsurance levelin force. The lowest deductible range offered by MICis $100 to $200. SCI does screen potential applicantsfor current major illnesses, but this is also implicitlydone by almost all medical insurance groups eitherthrough their not enrolling high health risk individ-uals or through a waiting period (SCI does not havea waiting period).
SCI and Group Business were compared on stan-dard medical care and charge indicators, includinghospital inpatient, outpatient, inpatient procedures(medical, surgical, and obstetric procedures per-formed by the physician, and x-ray and laboratoryprocedures) and outpatient procedures (physician'sprocedures performed at the office, emergency room,outpatient department, ambulatory surgery center, athome, and ambulance trips and independent labs).
As a control for age, and to see whether the TMprogram has a differential impact on different agegroups. MIC of Iowa actuarial services kindly pro-vided utilization statistics comparing SCI and GroupBusiness in three age categories (0-18,19-39, 40 + ).Because of small numbers, the utilization indicatorsfor SCI were derived as averages over 2 years(1982-1983) and relatively broad age categories hadto be used. For the SCI group there were 80, 975, and218 in the 0-18, 19-39, and 40+ categories, respec-tively.
Since these age categories are broad, it was of in-terest to compare the distributions by decades thatfall within the broader age categories. For the oldestdecade (60-69), which would be expected to havethe highest medical utilization, SCI and Group Busi-ness had similar percentages (18.47% and 17.8%, re-
496 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
spectively). However, in the next oldest decade(50-59), the SCI group had 12% fewer and they had11.3% more in the 40-49 decade.
For the 19-39 age group, SCI members tended tobe older than Group Business, with 87.4% in the30-39 decade compared to 49.8% in the 30-39 dec-ade for Group Business. In the 0-18 bracket, SCI hadproportionally fewer school age children from 5-18than Group Business (53.9% vs. 73.2%).
The distribution of gender by age was found to bevery similar for SCI and Group Business, with 46.5%males in the SCI group in 1982 and 1983 combined,compared with 47% males in Group Business.
The medical and surgical hospital admission per1000 were also compared for SCI and Group Businessfor 18 standard treatment categories. The categories,ordered by frequency of admissions for the normativedata (Group Business) are
1. Pregnancy and childbirth—including shortlybefore and after childbirth
2. Intestinal diseases—ulcers and disorders of thestomach, hernia, functional digestive disor-ders, chronic liver disease, gastroenteritis/co-litis, appendicitis, and gallbladder disorders
3. Nose, throat, and lung—tonsils, adenoids,bronchitis, emphysema, pneumonia, andasthma
4. Heart and blood vessels—hypertensive dis-ease, ischemic heart disease, hemorrhoids, an-gina, atherosclerosis, congestive heart failure
5. Genital and urinary—kidney/urinary tractstones, hyperplasia of prostate, benign mam-mary displasia
6. Injuries and poisoning—accidents, wounds,burns, fractures, internal head injuries
7. Benign and malignant tumors—malignancy ofthe oral cavity/stomach, colon/rectum/anus,throat/lung, skin, female breast, cervix/ovary/uterus, prostate, thyroid, benign tumors of var-ious sites, carcinoma of breast/genitourinaryand leukemia
8. Bones and muscles—intervertebral disc dis-orders, bone infections, arthritis
9. Ill defined condition—convulsions, chest pain,abdominal pain
10. All mental disorders—psychoses/neuroses,drug/mental disorders, alcohol/mental disor-ders, other mental disorders
11. Nervous system—migraine, glaucoma and cat-aract, disorders of ear
12. Irregularities of metabolism—thyroid disor-der, diabetes mellitus, pituitary/adrenal glandailment, nutritional deficiencies, obesity
13. All infectious diseases14. Other15. Medical carveout—services covered by Med-
icare16. Skin17. Congenital18. Blood
Data aggregated into this system of treatment cat-egories could be calculated from the available infor-mation for 3 years (1983-1985) for Group Businessand for 5 years (1981-1985) for SCI. The means ofthree years for Group Business and 5 years for SCIare reported. The following formulas were used tocalculate this data from the available information:
SCI hospital admissions/1000 =number of admissionsin a treatment category x ——'for SCI in that category
where N = group membership of SCI that year.
Group Business % chargedhospital admissions = for that/1000 in a treat- categoryment category
total charges charges per (2)x /1000 for - admission in
that category that category1000
N
The accuracy of these values was checked byshowing that the sum of the admissions per 1000calculated for the 18 categories equalled the totaladmissions per 1000 given in the MIC report.
Other Accounts
As a control for profession, MIC actuarial servicesselected five other insurance accounts with compa-rable policies that were of similar size and profes-sional membership as SCI for utilization indicatorsfor 1982 incurred. None of the Other Accounts se-
Psychosomatic Medicine 49:493-507 (1987) 497

TABLE 1.
SCI
Uti
liz
ati
on
Rate
s C
om
pa
red
wit
h O
ther
Acc
ou
nts
of S
imil
ar
Pro
fess
ion
al
Me
mb
ers
hip
"
Oth
er
Acc
ounts
R
ange
P
P
S
CI v
s.
SC
I vs.
A
vera
ge
Hig
h
(ID
) Low
(I
D)
SC
I A
vera
ge
Low
Adm
issi
ons
per
1000 m
embe
rs
Me
d~
ca
l S
urgi
cal
Obst
etr
ic
Tota
l
Pat
ient
day
s pe
r 1000 m
embe
rs
Medic
al
Sur
gica
l O
bst
etr
ic
Tota
l
Ave
rage
length
of
stay
M
ed
~c
al
Sur
gica
l O
bst
etr
ic
Tota
l
Outp
atie
nt
wit
s p
er
1000 m
embe
rs
Medic
al
Sur
gica
l O
bst
etr
ic
Tota
l ID
Num
ber
Typ
e o
f A
ccount
1,2
Banki
ng In
dust
ry
3 S
choo
l Sys
tem
4
Com
pute
r F
irm
(H
~g
h Tec
h)
5 C
itylG
ove
rnm
ent U
nit
T
ota
l
a198
2 In
curr
ed,
Pai
d th
rough M
arc
h 3
1,
1983
b
T~
e: 2,
3,4
& 5
5

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
MEDICRL
81 82 83 84 85
Inpatient
SURGICRL
Illl81 82 83 84 85
Year
OBSTETRICRL
81 82 83 84 85
I Group Bu3ine33 0 SCI
ooX.w
160
140
120
100 •
80
60
20
MEDICRL
m
• 1 1IIIIII1 1 1ililiL1 milIII
1
31 82 83 84 85
160
140
120
100
80
60
40
20
OutpatientSURGICRL
• • • 1 1
81 82 83 84 85
Year
160
140
120
100
80
60
40
20
OBSTETRICRL
81 82 83 84 85
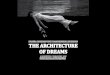
Fig. 1. Levels of inpatient and outpatient medical care utilization in major treatment categories over 5 yearsfor SCI (TM group) and Group Business (normative data).
lected for the comparison with SCI exactly matchesthe SCI group, which was difficult to match becauseits membership is not based on a common profession,although most of its membership can be character-ized as "white collar" and many are teachers. TheOther Accounts do, however, cover a variety ofprofessions typical of the SCI members, includingtwo banking groups, a school system (teachers andadminstrators), a computer firm (high technology),and a city government unit (see bottom of Table 1for N for each of these groups). The terms of thehealth insurance policies of the Other Accounts werecomparable to SCI's.
Statistical Analysis
The hypothesis that the medical utilization indi-cators for SCI and Group Business were significantlydifferent over the 5 years was tested using the chi-
Psychosomatic Medicine 49:493-507 (1987)
square statistic for a 2 x 5 table representing the twogroups (SCI and Group Business) for the 5 years (1981-1985). The utilization rates for the normative data(Group Business) were used as the expected valuesand the rates for SCI were the observed values. Aseparate chi square was calculated for each indica-tor—inpatient admissions per 1000, inpatient daysper 1000, outpatient visits per 1000, inpatient pro-cedures (e.g., x-rays etc.) per 1000, outpatient pro-cedures per 1000, and total health charges.
The data on the different age categories were ana-lyzed by calculating a 2 x 3 chi square table repre-senting the two groups (SCI and Group Business) andthe three different age categories, testing the hypoth-esis that the two groups were different over the agecategories. This was done for hospital inpatient daysper 1000 and outpatient visits/1000 (p values fromthese analyses are shown in Figure 2).
The critical ratio test (33) was used to compare SCIand Other Accounts (data presented in Table 1). This
499

D. ORME-JOHNSON
V.inz(Daca
« _ i
030 .
in
in
ca>
CDCL
=1a
inL.
Earooo
inL.0)
£
Cooo
1200
1000
800
600
400
200
0
250
200
150
100
50
0
GroupBusiness
0 - 1 8
GroupBusiness
• •^^•sci
0 - 1 8
Inpatient
p<0001
Group
B||S
^^H cri
19-39Age
Outpatientp<0001
Group
Business
^̂ H :1 9 - 3 9
Age
Group
•••̂•sci
40+
GroupBusiness
•̂H sci
» ^
40+
Fig. 2. Levels of inpatient and outpatient medical care utilization by age categories for SCI and GroupBusiness.
tests the hypothesis that the observed proportion ofthe statistic in question (admissions per 1000, patientdays per 1000, average length of stay, or outpatientdays per 1000 for SCI members (Psci) was signifi-cantly lower than the expected proportion (P) of ad-missions for Other Accounts. The standard deviationin proportion units is V(PQ)/N, where Q = (1 - P)and N = sample size of the SCI group. Thus,z = (Psci - P)/V(PQ)/N (33, p. 50). As a test for nor-mality, NP and NQ must exceed 5, and the data mustbe corrected for continuity if either product is be-tween 5 and 10 (30, p. 51). This would be the test ofchoice for the 18 treatment categories as well, butdue to very small proportions the data were too skewedand nonnormal to justify the use of the test. Instead,the sign test was used as an overall test of the dif-ference between SCI and Group Business on the 17pathologic treatment categories taken together (omit-ting pregnancy and childbirth).
RESULTS
Figure 1 shows that for every year from1981 to 1985, SCI's utilization rates wereconsistently lower than Group Business formedical and surgical inpatient and out-patient medical care. It is interesting tonote in Figure 1 that over the 5 years, GroupBusiness decreased on inpatient medicaland surgical utilization while its outpa-tient utilization increased.
The 5-year means showed that SCI's ad-missions per 1000 compared to GroupBusiness's were 63% fewer for inpatientmedical, 71.5% fewer for inpatient surgi-cal, 58.8% fewer for outpatient medical,
500 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
Group Business
Childbirth Intestinal Nosejhroat Heart Genital & Injuries& Lung Urinary
Tumors Bones &. Ill-Defined All Mental Nervous MetabolisMuscle Condition Dtsorders System
Treatment Category
Fig. 3. Levels of medical care utilization in 18 treatment categories for SCI and Group Business.
and 56.0% fewer for outpatient surgical(ps < 0.0001]. SCI's obstetric admissionwere 5.6% higher than Group Business overthe 5-year period, a nonsignificant differ-ence.
All other utilization indicators—patientdays per 1000, inpatient and outpatientprocedures—showed results that weresimilar to admissions per 1000(ps < 0.0001).
Figure 2 shows that SCI had lower med-ical utilization rates than Group Businessin all age categories. Inpatient days per1000 were 50.2% fewer for SCI children
(0-18), 50.1% fewer for SCI young adults(19-39), and 68.4% fewer for SCI olderadults (40 + ), p < 0.0001. Outpatient vis-its per 1000 were 46.8% fewer for SCI chil-dren, 54.7% fewer for SCI young adults,and 73.7% fewer for SCI older adults,p < 0.0001.
Figure 3 shows that SCI had lower ad-missions per 1000 than Group Business inall 18 treatment categories except obstet-rics. For the other 17 categories, SCI hadlower admissions rates: intestinal, -49%;nose, throat, and lung, -73.0%; heart,-87.3%; genital and urinary, - 37.0%; in-
Psychosomatic Medicine 49:493-507 (1987) 501

D. ORME-JOHNSON
juries, -63.2%; tumors, - 55.4%; bone andmuscle, -67.6%; ill-defined conditions,-76.0%; all mental disorders, -30.6%;nervous system, -87.2%; metabolism,-65.4%; infectious diseases, -30.4%;other, - 91.2%; medical carveout (servicescovered by Medicare), -100%; congeni-tal, -50.6%; and blood, -32.8%. Theprobability of SCI being lower than GroupBusiness in the 17 medical treatment cat-egories is 0.517 = 7.63 x 10"6, a highlysignificant result. The N of the SCI groupwas not large enough for a finer breakdowninto subcategories.
Table 1 shows that SCI had significantlyfewer hospital admissions than the meanof Other Accounts of similar professionalmembership for medical and surgical ad-missions per 1000 and patient days per1000 (ps < 0.0001), but a comparable av-erage length of stay. However, the averagelength of stay in the hospital for child de-livery for the meditating mothers was 3days, compared with an average of 4.1 daysfor Other Accounts and the obstetrics pa-tient days per 1000 were 62 for SCI com-pared to 88 for Other Accounts(p = 0.0021). It is noteworthy that SCI waslower than the lowest of the five OtherAccounts for medical, surgical, total ad-missions per 1000, and patient days per1000.
Cost Benefit
SCI's combined cost of inpatient andoutpatient treatment per 1000 memberspaid out by the insurance carrier was 26.5%to 67.4% less than Group Business for dif-ferent years, which amounted to $623,571per 1000 less over the 5-year period. Theaverage one-time cost to learn the TM tech-nique per person is approximately $300,or $300,000 per 1000. Therefore, afterteaching a group of people the TM tech-
nique, one would still save an estimatedthird of a million dollars per 1000 over afive-year period, a considerable reductionof health care costs if extended nation-wide.
DISCUSSION
Regular practice of the TM technique15-20 min twice a day was the only ex-plicit defining characteristic of the SCIgroup. It is reasonable to believe that SCImembers actually did meditate regularlybecause members sign a legal agreementto continue to regularly practice the pro-gram as a condition of eligibility for theinsurance benefits, and because they areperiodically required to participate instandard checking of the practice offeredby TM centers. The specific criteria of cor-rect meditation used by the TM teacher arethat the practice is effortless and relaxingand produces cumulative benefits inactivity.
However, the SCI group (as well as allthe comparison groups) were self-selected,which raises the question of causality. Doesthe requirement for 6 months of partici-pation in the TM program bias this groupin relation to the nonmeditator enrolleesin the other insurance groups? One pos-sible explanation for the data is that peo-ple who learn and continue to participatein the TM program tend to have morehealth-promoting life-styles anyway. Thisappears to be unlikely, however, becausemany people come to learn the techniquebecause they are having problems, and re-search using random assignment and otherexperimental designs have shown that thetechnique has beneficial effects on peoplewho begin even with serious problems (e.g.,19, 20). In addition, it seems unlikely thatthe meditators could significantly change
502 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
their life-styles merely on the basis of anintellectual or emotional commitment tosome ideal of behavior; indeed, no changein belief system or life-style is suggestedor required for participation in the pro-gram.
In addition, there does not appear to beanything in the terms of the SCI insurancepolicy that would tend to reduce its uti-lization relative to the comparison groups.The SCI insurance policy had a low de-ductible and a coinsurance plan typical ofthe normative data (Group Business) andOther Accounts of similar professionalmembership. SCI does exclude prospec-tive members who have a current majorillness, but so do most group insuranceplans represented in the comparisongroups, either through not enrolling highhealth-risk individuals in their health in-surance plan or by having a waiting period(SCI had no waiting period). The distri-bution of gender was the same for the SCIand Group Business so this was not afactor.
With regard to age, the SCI group hadlower medical utilization rates in all agecategories. The categories were broad inorder to maintain a substantial N in each,but there was little in the distributionswithin the categories to explain the re-sults. For example, in the high-risk 60-69decade the SCI group actually had a slightlyhigher percentage of members than GroupBusiness, although they did have 12% fewermembers in the 50-59 decade and pro-portionally more in the 40-49 decade.Within the 19-39 bracket, SCI memberswere actually more distributed towards theolder 30-39 decade, so younger age couldnot account for their lower medical utili-zation rates. For the 0-18 group, SCI had19.3% more preschoolers, which mighthave resulted in less disease because of notbeing exposed at school. However, it is
unlikely that this 19.3% discrepancy couldhave accounted for all of the approxi-mately 50% reduction in hospitalizationand doctor visits observed for the SCI chil-dren.
An interesting note on age is that thecontrast between the SCI group and GroupBusiness increased with age. Whereashealth care utilization was approximately50% less for SCI in the 0-18 and 19-39age brackets, for the 40 + group it was 68.4%less for inpatient and 73.7% less for out-patient utilization. This result supportsprevious research (25, 26) demonstratingthe cumulative preventative benefits of theTM program for aging.
Inpatient vs. Outpatient Treatment
SCI's reduced medical care utilizationcannot be attributed to a shift from inpa-tient to outpatient care, because SCI hadlower inpatient and outpatient rates rela-tive to both Group Business and Other Ac-counts. The normal obstetric admissionrates for SCI further indicate normal med-ical utilization for nonpathologic use, i.e.,child delivery. This pattern of results sug-gests that the reduction in SCI's utilizationrates was not due to a life-style preference,such as a tendency to deliver babies at homerather than in the hospital or a preferencefor outpatient rather than inpatient treat-ment. In addition, the finding that the SCIgroup had lower incidences of major con-ditions such as heart disease and cancershows that their utilization levels were notrestricted to the less serious medical cat-egories.
The SCI mothers did spend somewhatfewer days (3.0) in the hospital than didOther Accounts mothers (4.1). This mayhave been because of a preference to leavethe hospital earlier or because of betterhealth. The latter interpretation is con-
Psychosomatic Medicine 49:493-507 (1987) 503

D. ORME-JOHNSON
sistent with previous medical research onover 100 mothers showing better health formother and child during pregnancy andchildbirth, shorter duration of labor, andlower frequency of operative interventionduring labor (34) and research showingmore time in the quiet alert state in neo-nates of meditating mothers (35).
The explanation for the data that is mostconsistent with the previous research takenas a whole (7-20, 22-32, 34-37) is that theregular experience of the physiologic stateof restful alertness produced by the TMtechnique influences health both directlyand indirectly. Direct effects would occurthrough preventing the accumulation ofphysiologic stress. Indirect effects wouldoccur through improved life-style due tobecoming a "better chooser" on the basisof stabler, more balanced physiologicfunctioning, which increases one's senseof coherence. Decreasing the physiologicmanifestations of stress could be expectedto decrease internal "noise," thus increas-ing the signal-to-noise ratio, which wouldallow one to attend to the subtle cues com-ing from within the body and environmentso that one would spontaneously makemore health-supporting choices with re-gard to diet, smoking, seat belts, etc.
The research showing that TM medita-tors reduce their intake of alcohol, drugs,and tobacco (13-19, 36) can be interpretedas indicating their growing ability to makebetter choices. One study (37) found thatthe principal reason given by TM partic-ipants for reducing their intake of thesesubstances is increased sensitivity to thenegative consequences of the substanceson their physiology. Increased sensitivityto the physiologic effects of food mightalso result in dietary changes. Diet influ-ences health (38), but unfortunately infor-mation on the dietary and exercise habitsof the SCI group was not available. Al-
though there is no published research onthe TM program and diet, personal obser-vation suggests that a tendency towardsvegetarianism develops gradually over amatter of years in some but not all medi-tators. However, in their study of biologicaging, Wallace et al. (25) controlled for bothdiet and exercise and found that the TMprogram had an independent effect on re-ducing biologic age relative to chronologicage.
More random assignment studies areneeded to further clarify the relationshipbetween the TM program, health-promot-ing behavior, and health. However, large-scale studies of this type are difficult to dofor a number of practical reasons; randomassignment experiments were nonexistentin one review of ADM impact (2) and thosethat did exist on the effects of mental healthtreatment on medical utilization weresmall, with a median N = 22 (3). The pre-sent study had a larger N than all but 1 of25 studies cited in the first review (2) anda larger N than all 58 studies cited in thesecond review (3). The present study alsohad a longer treatment duration than allbut 3 of the 25 studies in the first review(2).
A New Theoretical Perspectiveon Health
A recent overview of health-enhancingstrategies stated that "we need to be openat this point to a broad spectrum of con-ceptual models of health and ways to en-hance it" (39). Most health-enhancementstrategies follow a two-step process of 1)identifying specific behavioral factors thatinfluence health and 2) finding techniquesthat modify behavior to promote health.The list of health-related behaviors in-cludes cigarette smoking, physical exer-cise, the use of seat belts, and chronic stress
504 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
(40). Techniques for changing health-re-lated behaviors have been termed partic-ipant modeling (41) and include variousprocedures that have been classified ascorrective action, direct feedback, and so-cial modeling (39).
The TM program differs fundamentallyfrom these health-enhancement strategiesin that it does not involve attempting toidentify or directly modify specific targetbehaviors. Recently, however, Maharishihas made available a comprehensive pre-vention program called Maharishi's Ayur-veda, which, in addition to the TM tech-nique, includes programs on diet, herbalsupplements, exercise, behavioral pat-terns, and prevention techniques for dif-ferent physiologic types, seasons, and cli-mates (42, 43). However, the majority ofthe present study occurred before theseother programs were available and it onlyinvolves the TM program itself, which doesnot require or even recommend changesin life-style. Yet without specifically at-tempting to change behavior, the TM pro-gram has been shown to have a wide-rang-ing impact on ADM (13-20, 36, 37), senseof coherence (22-24), and health (25-32).The generality of the TM program's effectsis also illustrated in the present study bythe low utilization rates of the SCI groupin virtually all medical treatments cate-gories.
The holistic effects indicated by the pre-sent and previous research have prompteda new theoretical approach to health thatdraws upon unified field theory of modernphysics (42-44). Hagelin (44) and othertheoretical physicists have noted theemergence at nature's fundamental scalesof measurement of characteristically sub-jective qualities, such as dynamism, in-telligence, and attributes of self-aware-ness, suggesting that consciousness mayrequire a more fundamental position in our
conception of nature. Hagelin (44) hasdemonstrated that there are close struc-tural parallels between the technical prop-erties of the unified field of quantum fieldtheory and the descriptions by both an-cient and modern meditators of the fieldof pure consciousness experienced whenconscious awareness settles into its "leastexcited state" (6). Chopra (42) points outthat the Vedic tradition that Maharishirepresents, as well as the roots of mostcultures of the world, identify the unifiedfield of natural law with a field of pureconsciousness, which can be directly ex-perienced by the human nervous systemto achieve higher levels of health and wellbeing. Wallace (43) has reviewed experi-mental evidence on the TM program sup-porting the theory that the direct experi-ence of the unified field as pureconsciousness produces an optimally bal-anced state in the neurochemical environ-ment of the body that maximizes the ef-ficient use of the information in DNA toinduce self-repair, holistic growth, and,hence, a higher level of health.
Based on previous research, some phy-sicians prescribe the TM program for stressmanagement, and there are two organiza-tions that serve the over 6000 physicianswho have learned the TM technique andmany more who recommend it.2 Futurelarge-scale research in business, industry,military, governmental, or educational set-tings would further clarify the ability ofthis promising technology of health en-hancement to prevent disease and to re-duce medical care costs.
2World Medical Association for Perfect Health-U.S.A. and American Association for AyurvedicMedicine c/o Dr. Barry Charles, Vice-President, 500014th Street NW, Washington, DC 20011.
Psychosomatic Medicine 49:493-507 (1987) 505

D. ORME-JOHNSON
REFERENCES
1. Matarazzo JD, Weiss SM, Herd JA, Miller NE. Weiss SM (eds), Behavioral Health: A Handbook of HealthEnhancement and Disease Prevention. New York, Wiley, 1984
2. Jones KR, Vischi TR: Impact of alcohol, drug abuse and mental health treatment on medical careutilization. Med Care 17 (Suppl 12), 1979
3. Mumford E, Schlesinger HJ, Glass GV, Patrick C, Cuerdon T: A new look at evidence about reducedcost of medical utilization following mental health treatment. Am J Psychiatry 141:10, 1984
4. Devine EC, Cook TD: A meta-analytic analysis of effects of psychoeducational interventions on lengthof postsurgical hospital stay. Nurs Res 32(5):267-274, 1983
5. Maharishi Mahesh Yogi: On the Bhagavad Gita. Baltimore, Penguin, 19696. Maharishi Mahesh Yogi: Creating an ideal society. West Germany, MERU Press, 19777. Wallace RK, Benson H, Wilson AF: A wakeful hypometabolic physiologic state. Am J Physiology
221:795-799, 19718. Wallace RK, Benson H: The physiology of meditation. Sci Am 226:84-90, 19729. Orme-Johnson DW, Dillbeck MC: Meta-analysis and theoretical framework of physiological research
on the Transcendental Meditation technique. Submitted for publication.10. Levine PH: The coherence spectral array (COSPAR) and its application to the study of spatial ordering
in the EEG. Proc San Diego Biomed Symp 25:237-247, 197611. Farrow JT, Hebert RJ: Breath suspension during the Transcendental Meditation technique. Psychosom
Med 44:133-153, 198212. Badawi K, Wallace RK, Orme-Johnson DW, Rouzerre AM: Electrophysiologic characteristics of respi-
ratory suspension periods occurring during the practice of the Transcendental Meditation program.Psychosom Med 46:267-276, 1984
13. Monahan RJ: Secondary prevention of drug dependency through the Transcendental Meditation pro-gram in metropolitan Philadelphia. Int J Addiction 12:729-754, 1977
14. Benson H, Wallace RK: Decreased drug abuse with Transcendental Meditation: A study of 1,862 subjects.In Zarafonetis C (ed), Drug Abuse: Proceedings of the International Conference. Philadelphia, Lea &Febiger, 1975, pp 239-252
15. Shafi M, Lavely RA, JaffeRD: Meditation and the prevention of alcohol abuse. Am J Psychiatry 132:924-945, 1975
16. Shafi M, Lavely RA, Jaffe RD: Meditation and marijuana. Am J Psychiatry 131:60-63, 197417. Bielefeld M: Transcendental Meditation: A stress reducing self-help support system. Paper presented
at the American Psychological Association, Los Angeles, CA, August 24,1981. In Chalmers RA, ClementsG, Schenkluhn H, Weinless M (eds), Scientific Research on the Transcendental Meditation and TM-Sidhi program: Collected Papers, West Germany, MERU Press, vol 3, in press
18. Ottens AJ: The effect of Transcendental Meditation upon modifying the cigarette smoking habit. J SchoolHealth 45:577-583, 1975
19. Brooks JS, Scanaro T: Transcendental Meditation in the treatment of post-Vietnam adjustment. J Counsel.Dev, 64(3):212-215, 1985
20. Epply K, Abrams A, Shear J: Factors influencing the effectiveness of meditation and relaxation tech-niques. Paper presented at the annual convention of the American Psychological Association, Toronto,August 1984
21. Antonousky A: The sense of coherence as a determinant of health. In Matarazzo JD, Weiss SM, HerdJA, Miller NE, Weiss SM (eds), Behavioral Health: A Handbook of Health Enhancement and DiseasePrevention. New York, Wiley, 1984
22. Shecter H: The Transcendental Meditation program in the classroom. In Orme Johnson DW, Farrow JT(eds), Scientific Research on the Transcendental Meditation: Collected Papers. Livingston Manner, NY,MIU Press, 1977, vol 1, pp 403-409
23. Pelletier KR: Influence of Transcendental Meditation upon autokinetic perception. Percep Mot Skills39:1031-1034, 1974
24. Dillbeck MC: Meditation and flexibility of visual perception and verbal problem solving. Memory Cogn10(3):207-215, 1982
506 Psychosomatic Medicine 49:493-507 (1987)

MEDICAL CARE AND TRANSCENDENTAL MEDITATION
25. Wallace RK, Dillbeck MC, Jacobe E, Harrington B: The effects of the Transcendental Meditation andTM-Sidhi program on the aging process. Int J Neurosci 16:53-58, 1983
26. Alexander CN, Langer EJ, Davies JL, Newman R, Chandler H: Enhancing health and longevity: The TMprogram, mindfulness, and the elderly. Paper presented at the 36th Annual Council on the Aging,Washington D.C., April 11, 1986
27. Wilson AF, Honsberger RW, Chiu JT, Novey HS: Transcendental Meditation and asthma. Respiration32:74-80, 1975
28. Benson H, Wallace RK: Decreased blood pressure in hypertensive subjects who practiced meditation.Circulation 45/46 (Suppl II): 516, 1972
29. Blackwell B, Hanenson IB, Bloomfield SS, Magenheim HG, Nidich SI, Gartside P: Effect of Transcen-dental Meditation on blood pressure: A controlled pilot study. Psychosom Med 37:86, 1975
30. Wallace RK, Silver J, Mills P, Dillbeck MC, Wagoner DE: Systolic blood pressure and long-term practiceof the Transcendental Meditation and TM-Sidhi program: Effects of TM on systolic blood pressure.Psychosom Med 45:41^6, 1983
31. Cooper MJ, Aygen MM: A relaxation technique in the management of hypercholesterolemia. ) HumStress 5(4):24-27, 1979
32. Fuson JW: The effect of Transcendental Meditation on sleeping and dreaming patterns. Doctoral dis-sertation, Yale Medical School, 1976. Reprinted (abbr.) in Scientific Research on the TranscendentalMeditation: Collected Papers, Vol 2, in press.
33. McNemar Q: Psychological Statistics. New York, Wiley, 1982, p 20934. Heidelberg R: Transzendentale Meditation in der geburtshilflichen Psychoprophylaxe. Doctoral thesis
(abbr.), Medical Faculty, Free University of Berlin, West Berlin, W. Germany, 1979. In Chalmers RA,Clements G, Schenkluhn H, Weinless M (eds), Scientific Research on the Transcendental Meditationand TM-Sidhi Program: Collected Papers. West Germany, MERU Press, in press.
35. Doan MJ: TM program as a prenatal factor in the quiet alert state in normal newborns. MA thesispresented to the faculty of San Diego State University, California, 1985
36. Brautigam E: Effects of the Transcendental Meditation program on drug abusers: A prospective study.In Orme Johnson DW, Farrow JT (eds), Scientific research on the Transcendental Meditation: CollectedPapers, Livingston Manner, NY, MIU Press, 1977, vol 1, pp 506-514
37. Aron A, Aron E: The Transcendental Meditation program's effect on addictive behavior. Addict Behav5:3-12, 1980
38. Rodin J: Overview: Healthful diet. In Matarazzo JD, Weiss SM, Herd JA, Miller NE, Weiss SM (eds),Behavioral Health: A Handbook of Health Enhancement and Disease Prevention. New York, Wiley,1984, pp 549-551
39. Thoresen CE: Strategies for health enhancement: Overview. In Matarazzo JD, Weiss SM, Herd JA, MillerNE, Weiss SM (eds), Behavioral Health: A Handbook of Health Enhancement and Disease Prevention.New York, Wiley, 1984
40. Matarazzo JD: Behavioral Health: A 1990 challenge for the health services professions. In MatarazzoJD, Weiss SM, Herd JA, Miller NE, Weiss SM (eds), Behavior Health: A Handbook of Health Enhancementand Disease Prevention. New York, Wiley, 1984
41. Bandura A: Social Learning Theory. Englewood Cliffs, NJ, Prentice-Hall, 197742. Chopra D: Creating Health: The Psychophysiological Connection. New York, Vantage, 198543. Wallace RK: Maharishi Technology of the Unified Field: Neurophysiology of Enlightenment. Fairfield,
IA, MIU Neuroscience Press, 198644. Hagelin JS: Is consciousness the unified field? A field theorist's perspective. Mod Sci Vedic Sci 1(1):28-
87, 1987
Psychosomatic Medicine 49:493-507 (1987) 507