Embed Size (px)
Citation preview
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #Sat 04/24/2010 Healthfirst visit
MVA - rolled car 4/8/10Cervical strain resolved. Given workrelease.
MVA rollover4/8/10. Cervicalstrain resolved in 2wks then wasreleased to work.
Healthfirst 0018
Mon 10/24/2011 Healthfirst - MVA previous thursday,10/20, when he rearended an 18 wheeler.Complaint - Lower back pain - "has backproblems already" per office note. Nodiagnostics are documented fromHealthfirst.
MVA - Lower backpain. Notesalready had backproblems.
Healthfirst 0016
Thu 04/12/2012 Date of injuryWas driving a dump truck down a narrowroad while on the job. 2 other dump truckswere also coming down the road, failed toyield so he moved over to make room andhis wheel slipped off the pavement. Histruck was loaded with gravel and it rolledover onto its side into ditch. He hit his headseveral times. They did a drug test on him.His employer was angry and he wasultimately fired from his job.
Rolled truck - hithead several times
Erwin C, MD0035
Thu 04/12/2012 Followup Robert R, MD
CHIEF COMPLAINT: Right shoulder pain.
HISTORY OF PRESENT ILLNESS: Thecortisone shot did give some relief. Today'spain is still 8/10. Cortisone tends to makehim swell. His pain is worse at night whensleeping. He is still having his closed headinjury evaluated. The patient has afull-thickness right shoulder rotator cufftear.
PLAN: The patient still has to do somemore things with lawyers, hearings, and aclosed head injury evaluation before I willsee him again in about 4 weeks. In thefuture, he will require a right shoulder openrotator cuff repair.
Dr. R00008-00009
Tue 05/15/2012 Seen at Healthfirst NW approx 1 mo postMVA
Complaints: dizziness, sensation ofmovement, loss of balance,nausea/vomiting
History: "No known event that precededsymptom onset" then contradicted andstates "had a concussion that started all
Phone call toHealthfirstComplains ofworsening vertigoand severeheadache, passingout, left armnumbness,nausea/vomiting,ringing in ears,
Healthfirst 0034
Page 1 of 52
Medical Chronology James S
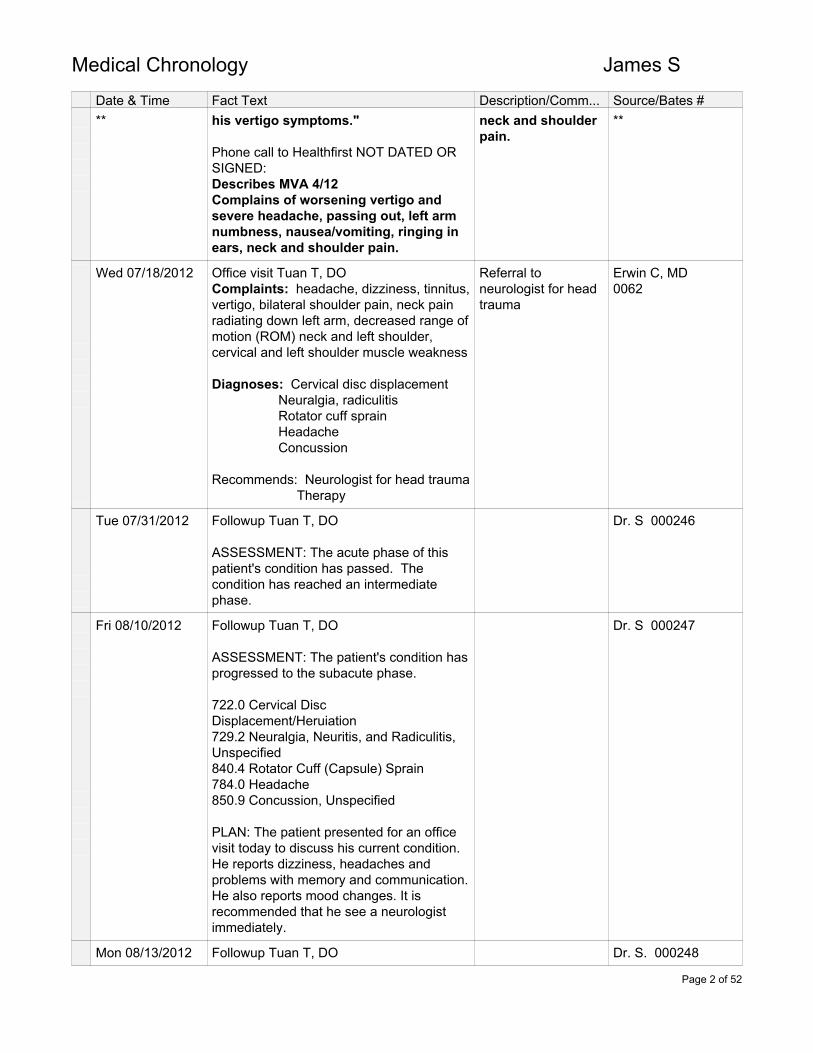
Date & Time Fact Text Description/Comm... Source/Bates #** his vertigo symptoms."
Phone call to Healthfirst NOT DATED ORSIGNED:Describes MVA 4/12Complains of worsening vertigo andsevere headache, passing out, left armnumbness, nausea/vomiting, ringing inears, neck and shoulder pain.
neck and shoulderpain.
**
Wed 07/18/2012 Office visit Tuan T, DOComplaints: headache, dizziness, tinnitus,vertigo, bilateral shoulder pain, neck painradiating down left arm, decreased range ofmotion (ROM) neck and left shoulder,cervical and left shoulder muscle weakness
Diagnoses: Cervical disc displacement Neuralgia, radiculitis Rotator cuff sprain Headache Concussion
Recommends: Neurologist for head trauma Therapy
Referral toneurologist for headtrauma
Erwin C, MD0062
Tue 07/31/2012 Followup Tuan T, DO
ASSESSMENT: The acute phase of thispatient's condition has passed. Thecondition has reached an intermediatephase.
Dr. S 000246
Fri 08/10/2012 Followup Tuan T, DO
ASSESSMENT: The patient's condition hasprogressed to the subacute phase.
722.0 Cervical DiscDisplacement/Heruiation729.2 Neuralgia, Neuritis, and Radiculitis,Unspecified840.4 Rotator Cuff (Capsule) Sprain784.0 Headache850.9 Concussion, Unspecified
PLAN: The patient presented for an officevisit today to discuss his current condition.He reports dizziness, headaches andproblems with memory and communication.He also reports mood changes. It isrecommended that he see a neurologistimmediately.
Dr. S 000247
Mon 08/13/2012 Followup Tuan T, DO Dr. S. 000248
Page 2 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #**
No changes. Manual therapy given.** **
Wed 08/22/2012 Followup Tuan T, DO
No change. Manual therapy given
Dr. S 000251
Fri 08/24/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000252
Mon 08/27/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000253
Wed 08/29/2012 Neuro consult - Erwin C, MDSymptoms/complaints: short-term memoryloss, stuttering, expressive aphasia,dizziness, vertigo, loss of balance,nausea/vomiting.
Impression: Closed head injury withconcussionPost traumatic vestibulopathyPost trauma episodic confusion (r/o partialseizures)
Recommends: Video ENG Vestibular exercises Brain MRI Ambulatory EEG
Diagnoses: Closedhead injury withconcussionPost traumavestibulopathyPost trauma episodicconfusion
Erwin C, MD0011
Wed 08/29/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000255
Fri 08/31/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000256
Wed 09/05/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000257
Fri 09/07/2012 Office visit Neil A, DOInitial pain evaluation.
Chief complaint of chronic, persistent neckpain associated with daily headaches,shoulder and upper back pain as well aspanicky feelings associated with memoryloss, both short-term and long-term,difficulty concentrating, and sleep loss.DIAGNOSIS:1. Chronic neck pain syndrome followingtraumatic work
Injury One 00772
Page 3 of 52
Medical Chronology James S
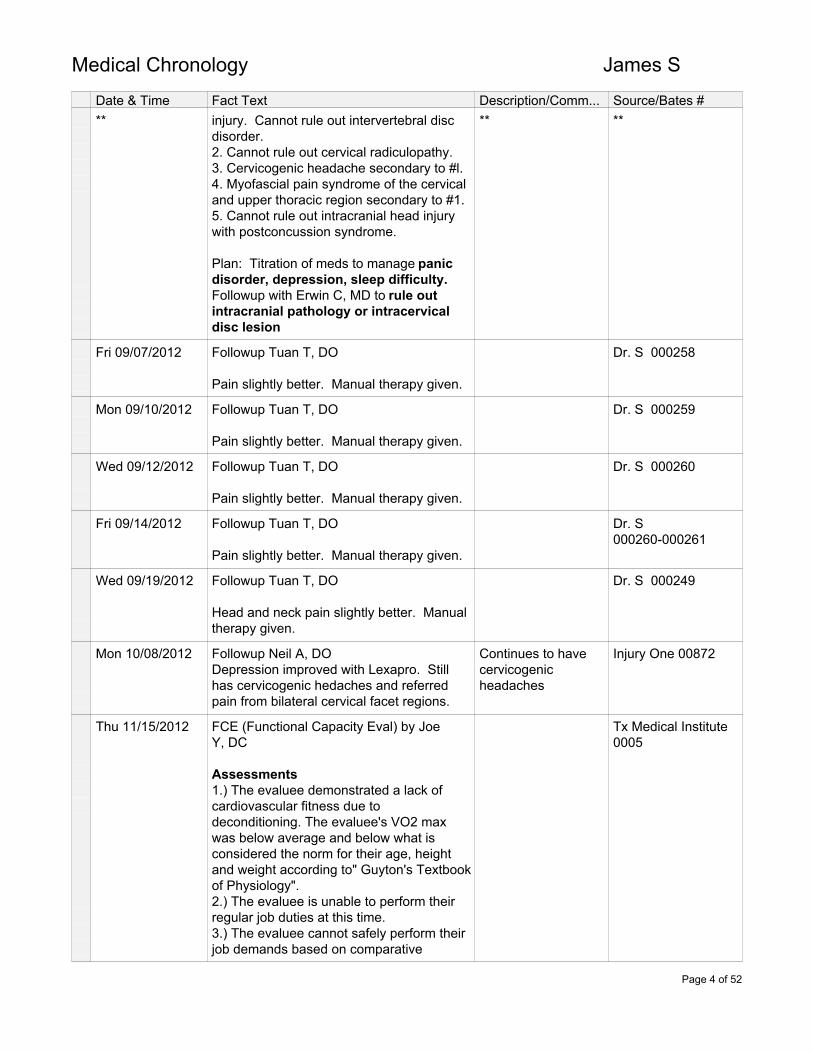
Date & Time Fact Text Description/Comm... Source/Bates #** injury. Cannot rule out intervertebral disc
disorder.2. Cannot rule out cervical radiculopathy.3. Cervicogenic headache secondary to #l.4. Myofascial pain syndrome of the cervicaland upper thoracic region secondary to #1.5. Cannot rule out intracranial head injurywith postconcussion syndrome.
Plan: Titration of meds to manage panicdisorder, depression, sleep difficulty.Followup with Erwin C, MD to rule outintracranial pathology or intracervicaldisc lesion
** **
Fri 09/07/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000258
Mon 09/10/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000259
Wed 09/12/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S 000260
Fri 09/14/2012 Followup Tuan T, DO
Pain slightly better. Manual therapy given.
Dr. S000260-000261
Wed 09/19/2012 Followup Tuan T, DO
Head and neck pain slightly better. Manualtherapy given.
Dr. S 000249
Mon 10/08/2012 Followup Neil A, DODepression improved with Lexapro. Stillhas cervicogenic hedaches and referredpain from bilateral cervical facet regions.
Continues to havecervicogenicheadaches
Injury One 00872
Thu 11/15/2012 FCE (Functional Capacity Eval) by JoeY, DC
Assessments1.) The evaluee demonstrated a lack ofcardiovascular fitness due todeconditioning. The evaluee's VO2 maxwas below average and below what isconsidered the norm for their age, heightand weight according to" Guyton's Textbookof Physiology".2.) The evaluee is unable to perform theirregular job duties at this time.3.) The evaluee cannot safely perform theirjob demands based on comparative
Tx Medical Institute0005
Page 4 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** analysis between their required job
demands and their current evaluationoutcomes.
** **
Thu 01/31/2013 Followup Neil A, DO
Chronic neck and head pain associatedwith postconcussion injury, cannot rule outintervertebral disk disorder andradiculopathy.
There is a vacuum affect in his neck andshoulder. He has marked decreased neckROM. He has trigger point tenderness inthe trapezius interscapular region.
Recommends brain MRI, epidural block
Erwin C, MD0049Injury One 00871
Mon 02/04/2013 Followup Tuan T, DO
Worsening of neck pain, headaches andright shoulder pain. Recommends cervicalMRI. Manual therapy given
Dr. S 000262
Thu 02/07/2013 MRI cervical, without contrastImpression1. Cervical lordosis straightening;suggestive of pain or spasm.2. C2-3 disc protrusion, may contactanterior spinal cord3. C3-4 Posterior disc protrusion onlycontact spinal cord4. C4-5 Posterior disc protrusion;indents spinal cord with mild-moderatecentral canal stenosis
Cervical MRIshows multileveldisc protrusionswith cord contactand C4-5 spinalstenosis.
WC vol 1 01117
Mon 02/25/2013 Office visit - Erwin C, MDThe court ruled insurance is to pay hismedical careSymptoms: episodic violent vertigo,dizziness, falling tendency, disorientation,bilateral tinnitus, dysequilibrium, loss ofbalance
Erwin Cruz, MD0010
Mon 02/25/2013 Followup Neil A, DO
Mr. S has, as I suspected,protruding/herniated disk at C2-3, C3-4 andC4-5 most significantly with indentation ofspinal cord resulting in central stenosis as aresult of his work injuries. This canexplain his persistent neck, shoulder, andarm pain, particularly his radiating paindown his left arm and hand as he is havinga C5 radiculopathy here today. As a result,
WC v 1, 01143
Page 5 of 52
Medical Chronology James S
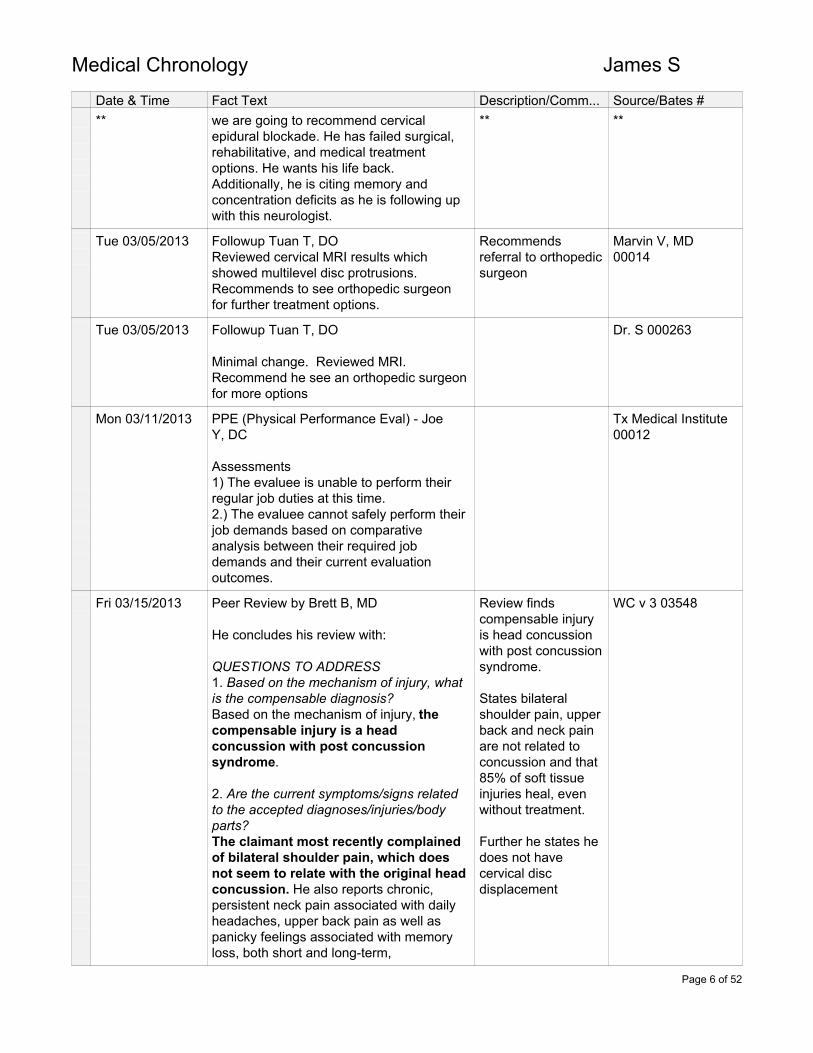
Date & Time Fact Text Description/Comm... Source/Bates #** we are going to recommend cervical
epidural blockade. He has failed surgical,rehabilitative, and medical treatmentoptions. He wants his life back.Additionally, he is citing memory andconcentration deficits as he is following upwith this neurologist.
** **
Tue 03/05/2013 Followup Tuan T, DOReviewed cervical MRI results whichshowed multilevel disc protrusions.Recommends to see orthopedic surgeonfor further treatment options.
Recommendsreferral to orthopedicsurgeon
Marvin V, MD00014
Tue 03/05/2013 Followup Tuan T, DO
Minimal change. Reviewed MRI.Recommend he see an orthopedic surgeonfor more options
Dr. S 000263
Mon 03/11/2013 PPE (Physical Performance Eval) - JoeY, DC
Assessments1) The evaluee is unable to perform theirregular job duties at this time.2.) The evaluee cannot safely perform theirjob demands based on comparativeanalysis between their required jobdemands and their current evaluationoutcomes.
Tx Medical Institute00012
Fri 03/15/2013 Peer Review by Brett B, MD
He concludes his review with:
QUESTIONS TO ADDRESS1. Based on the mechanism of injury, whatis the compensable diagnosis?Based on the mechanism of injury, thecompensable injury is a headconcussion with post concussionsyndrome.
2. Are the current symptoms/signs relatedto the accepted diagnoses/injuries/bodyparts?The claimant most recently complainedof bilateral shoulder pain, which doesnot seem to relate with the original headconcussion. He also reports chronic,persistent neck pain associated with dailyheadaches, upper back pain as well aspanicky feelings associated with memoryloss, both short and long-term,
Review findscompensable injuryis head concussionwith post concussionsyndrome.
States bilateralshoulder pain, upperback and neck painare not related toconcussion and that85% of soft tissueinjuries heal, evenwithout treatment.
Further he states hedoes not havecervical discdisplacement
WC v 3 03548
Page 6 of 52
Medical Chronology James S
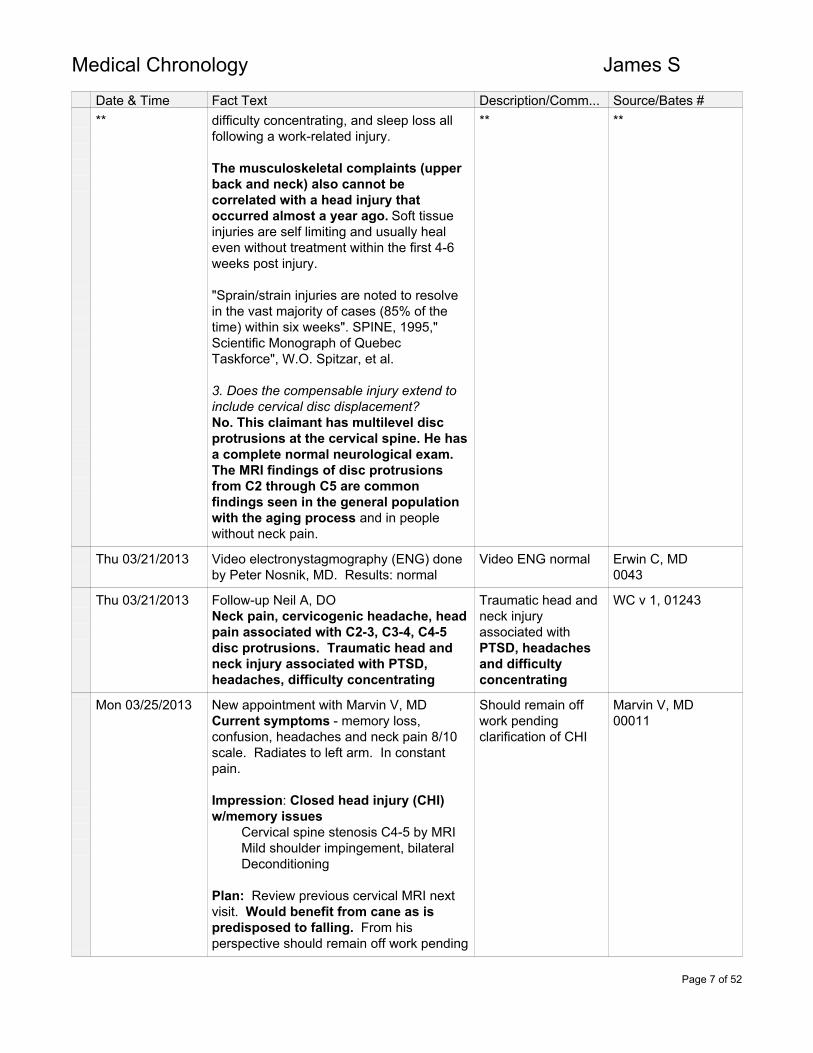
Date & Time Fact Text Description/Comm... Source/Bates #** difficulty concentrating, and sleep loss all
following a work-related injury.
The musculoskeletal complaints (upperback and neck) also cannot becorrelated with a head injury thatoccurred almost a year ago. Soft tissueinjuries are self limiting and usually healeven without treatment within the first 4-6weeks post injury.
"Sprain/strain injuries are noted to resolvein the vast majority of cases (85% of thetime) within six weeks". SPINE, 1995,"Scientific Monograph of QuebecTaskforce", W.O. Spitzar, et al.
3. Does the compensable injury extend toinclude cervical disc displacement?No. This claimant has multilevel discprotrusions at the cervical spine. He hasa complete normal neurological exam.The MRI findings of disc protrusionsfrom C2 through C5 are commonfindings seen in the general populationwith the aging process and in peoplewithout neck pain.
** **
Thu 03/21/2013 Video electronystagmography (ENG) doneby Peter Nosnik, MD. Results: normal
Video ENG normal Erwin C, MD0043
Thu 03/21/2013 Follow-up Neil A, DONeck pain, cervicogenic headache, headpain associated with C2-3, C3-4, C4-5disc protrusions. Traumatic head andneck injury associated with PTSD,headaches, difficulty concentrating
Traumatic head andneck injuryassociated withPTSD, headachesand difficultyconcentrating
WC v 1, 01243
Mon 03/25/2013 New appointment with Marvin V, MDCurrent symptoms - memory loss,confusion, headaches and neck pain 8/10scale. Radiates to left arm. In constantpain.
Impression: Closed head injury (CHI)w/memory issues Cervical spine stenosis C4-5 by MRI Mild shoulder impingement, bilateral Deconditioning
Plan: Review previous cervical MRI nextvisit. Would benefit from cane as ispredisposed to falling. From hisperspective should remain off work pending
Should remain offwork pendingclarification of CHI
Marvin V, MD00011
Page 7 of 52
Medical Chronology James S
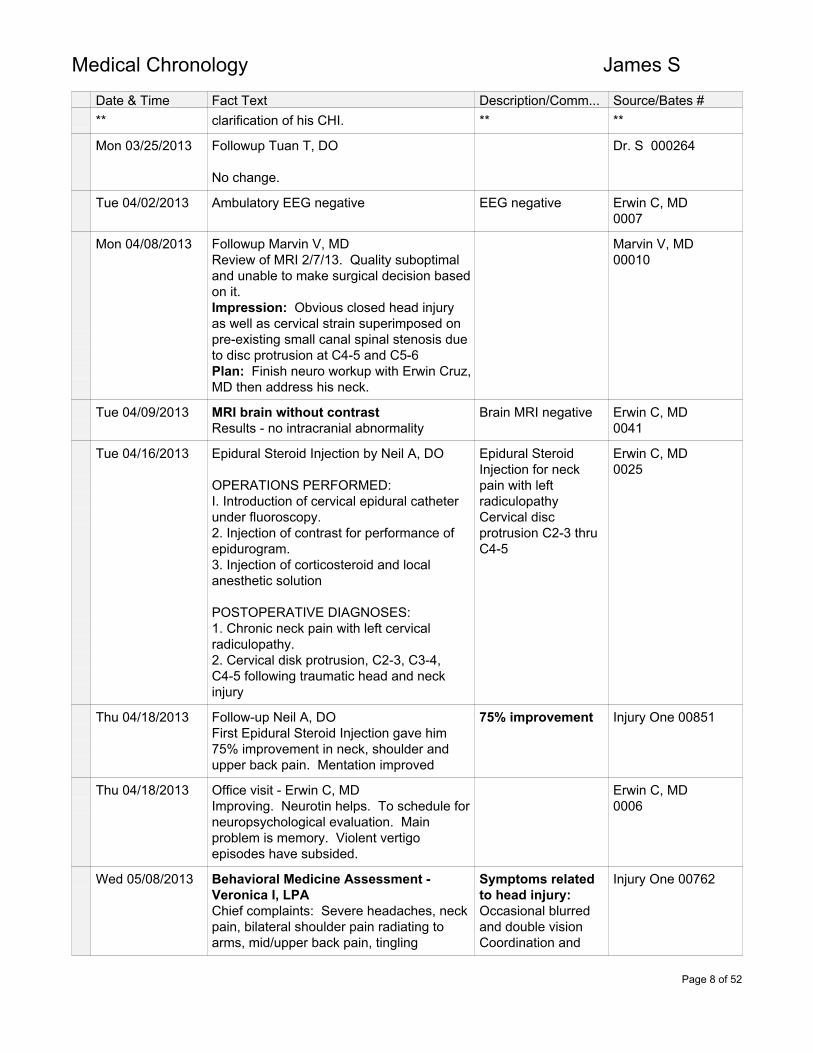
Date & Time Fact Text Description/Comm... Source/Bates #** clarification of his CHI. ** **
Mon 03/25/2013 Followup Tuan T, DO
No change.
Dr. S 000264
Tue 04/02/2013 Ambulatory EEG negative EEG negative Erwin C, MD0007
Mon 04/08/2013 Followup Marvin V, MDReview of MRI 2/7/13. Quality suboptimaland unable to make surgical decision basedon it.Impression: Obvious closed head injuryas well as cervical strain superimposed onpre-existing small canal spinal stenosis dueto disc protrusion at C4-5 and C5-6Plan: Finish neuro workup with Erwin Cruz,MD then address his neck.
Marvin V, MD00010
Tue 04/09/2013 MRI brain without contrastResults - no intracranial abnormality
Brain MRI negative Erwin C, MD0041
Tue 04/16/2013 Epidural Steroid Injection by Neil A, DO
OPERATIONS PERFORMED:I. Introduction of cervical epidural catheterunder fluoroscopy.2. Injection of contrast for performance ofepidurogram.3. Injection of corticosteroid and localanesthetic solution
POSTOPERATIVE DIAGNOSES:1. Chronic neck pain with left cervicalradiculopathy.2. Cervical disk protrusion, C2-3, C3-4,C4-5 following traumatic head and neckinjury
Epidural SteroidInjection for neckpain with leftradiculopathyCervical discprotrusion C2-3 thruC4-5
Erwin C, MD0025
Thu 04/18/2013 Follow-up Neil A, DOFirst Epidural Steroid Injection gave him75% improvement in neck, shoulder andupper back pain. Mentation improved
75% improvement Injury One 00851
Thu 04/18/2013 Office visit - Erwin C, MDImproving. Neurotin helps. To schedule forneuropsychological evaluation. Mainproblem is memory. Violent vertigoepisodes have subsided.
Erwin C, MD0006
Wed 05/08/2013 Behavioral Medicine Assessment -Veronica I, LPAChief complaints: Severe headaches, neckpain, bilateral shoulder pain radiating toarms, mid/upper back pain, tingling
Symptoms relatedto head injury:Occasional blurredand double visionCoordination and
Injury One 00762
Page 8 of 52
Medical Chronology James S
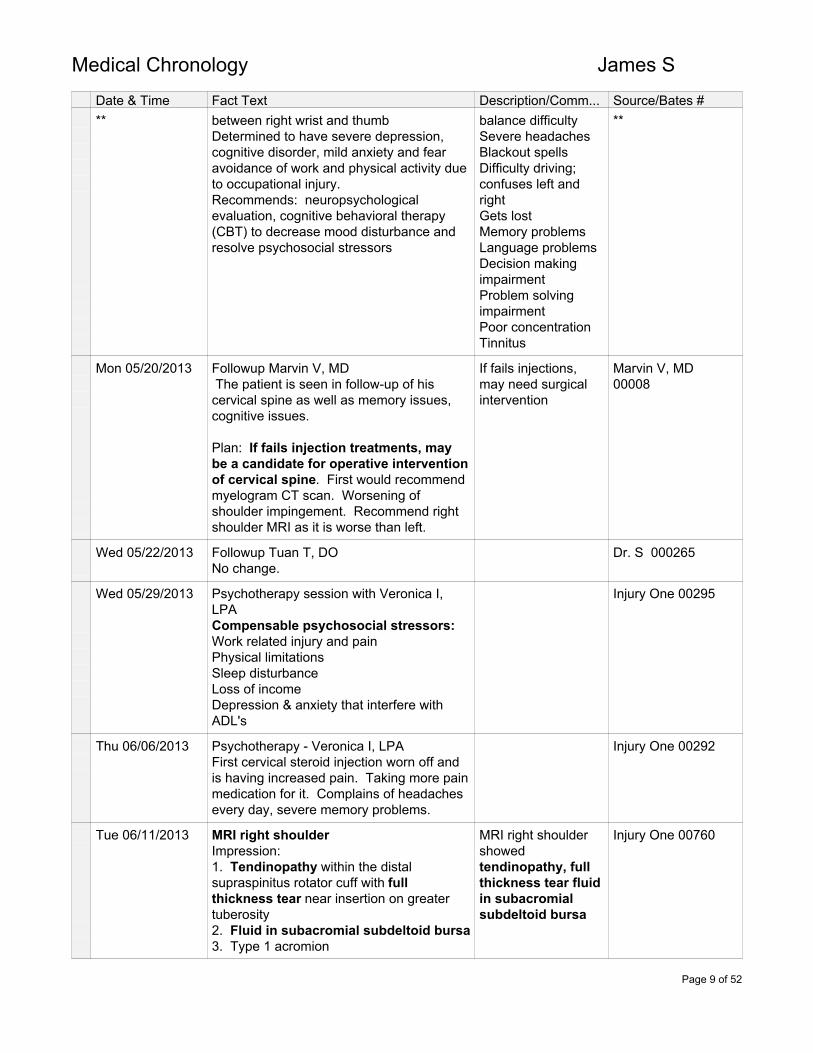
Date & Time Fact Text Description/Comm... Source/Bates #** between right wrist and thumb
Determined to have severe depression,cognitive disorder, mild anxiety and fearavoidance of work and physical activity dueto occupational injury.Recommends: neuropsychologicalevaluation, cognitive behavioral therapy(CBT) to decrease mood disturbance andresolve psychosocial stressors
balance difficultySevere headachesBlackout spellsDifficulty driving;confuses left andrightGets lostMemory problemsLanguage problemsDecision makingimpairmentProblem solvingimpairmentPoor concentrationTinnitus
**
Mon 05/20/2013 Followup Marvin V, MD The patient is seen in follow-up of hiscervical spine as well as memory issues,cognitive issues.
Plan: If fails injection treatments, maybe a candidate for operative interventionof cervical spine. First would recommendmyelogram CT scan. Worsening ofshoulder impingement. Recommend rightshoulder MRI as it is worse than left.
If fails injections,may need surgicalintervention
Marvin V, MD00008
Wed 05/22/2013 Followup Tuan T, DONo change.
Dr. S 000265
Wed 05/29/2013 Psychotherapy session with Veronica I,LPACompensable psychosocial stressors:Work related injury and painPhysical limitationsSleep disturbanceLoss of incomeDepression & anxiety that interfere withADL's
Injury One 00295
Thu 06/06/2013 Psychotherapy - Veronica I, LPAFirst cervical steroid injection worn off andis having increased pain. Taking more painmedication for it. Complains of headachesevery day, severe memory problems.
Injury One 00292
Tue 06/11/2013 MRI right shoulderImpression:1. Tendinopathy within the distalsupraspinitus rotator cuff with fullthickness tear near insertion on greatertuberosity2. Fluid in subacromial subdeltoid bursa3. Type 1 acromion
MRI right shouldershowedtendinopathy, fullthickness tear fluidin subacromialsubdeltoid bursa
Injury One 00760
Page 9 of 52
Medical Chronology James S
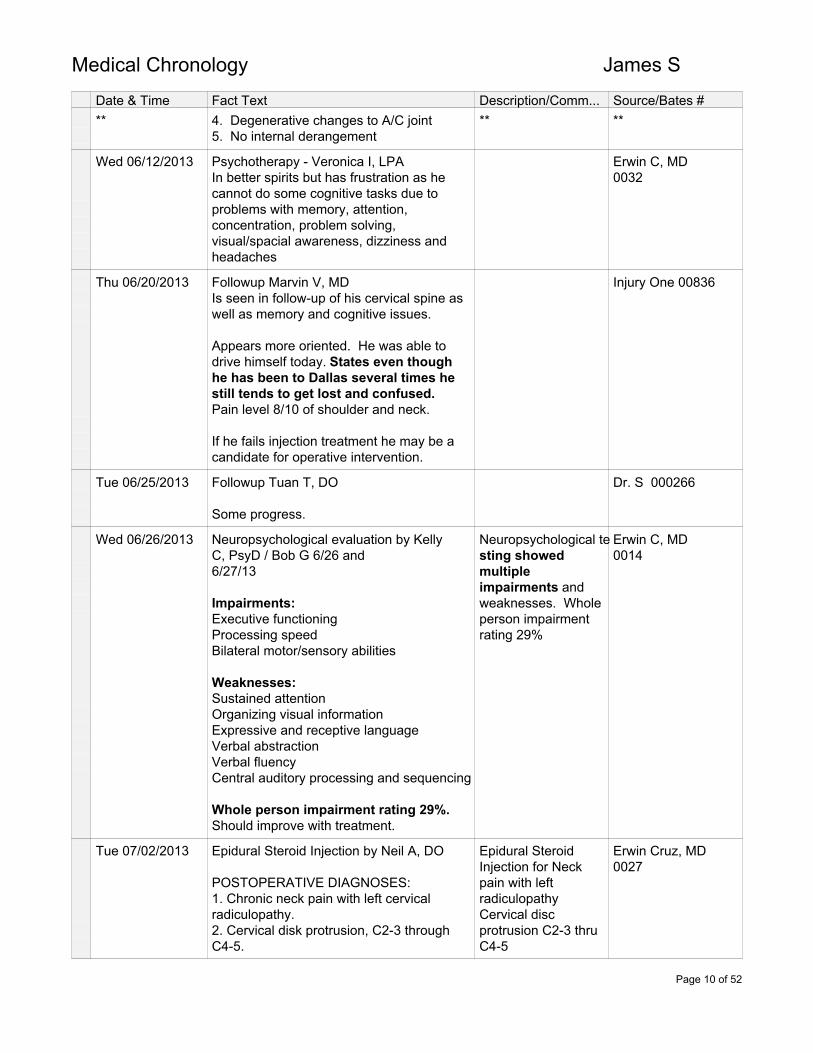
Date & Time Fact Text Description/Comm... Source/Bates #** 4. Degenerative changes to A/C joint
5. No internal derangement** **
Wed 06/12/2013 Psychotherapy - Veronica I, LPAIn better spirits but has frustration as hecannot do some cognitive tasks due toproblems with memory, attention,concentration, problem solving,visual/spacial awareness, dizziness andheadaches
Erwin C, MD0032
Thu 06/20/2013 Followup Marvin V, MDIs seen in follow-up of his cervical spine aswell as memory and cognitive issues.
Appears more oriented. He was able todrive himself today. States even thoughhe has been to Dallas several times hestill tends to get lost and confused.Pain level 8/10 of shoulder and neck.
If he fails injection treatment he may be acandidate for operative intervention.
Injury One 00836
Tue 06/25/2013 Followup Tuan T, DO
Some progress.
Dr. S 000266
Wed 06/26/2013 Neuropsychological evaluation by KellyC, PsyD / Bob G 6/26 and6/27/13
Impairments:Executive functioningProcessing speedBilateral motor/sensory abilities
Weaknesses:Sustained attentionOrganizing visual informationExpressive and receptive languageVerbal abstractionVerbal fluencyCentral auditory processing and sequencing
Whole person impairment rating 29%.Should improve with treatment.
Neuropsychological testing showedmultipleimpairments andweaknesses. Wholeperson impairmentrating 29%
Erwin C, MD0014
Tue 07/02/2013 Epidural Steroid Injection by Neil A, DO
POSTOPERATIVE DIAGNOSES:1. Chronic neck pain with left cervicalradiculopathy.2. Cervical disk protrusion, C2-3 throughC4-5.
Epidural SteroidInjection for Neckpain with leftradiculopathyCervical discprotrusion C2-3 thruC4-5
Erwin Cruz, MD0027
Page 10 of 52
Medical Chronology James S
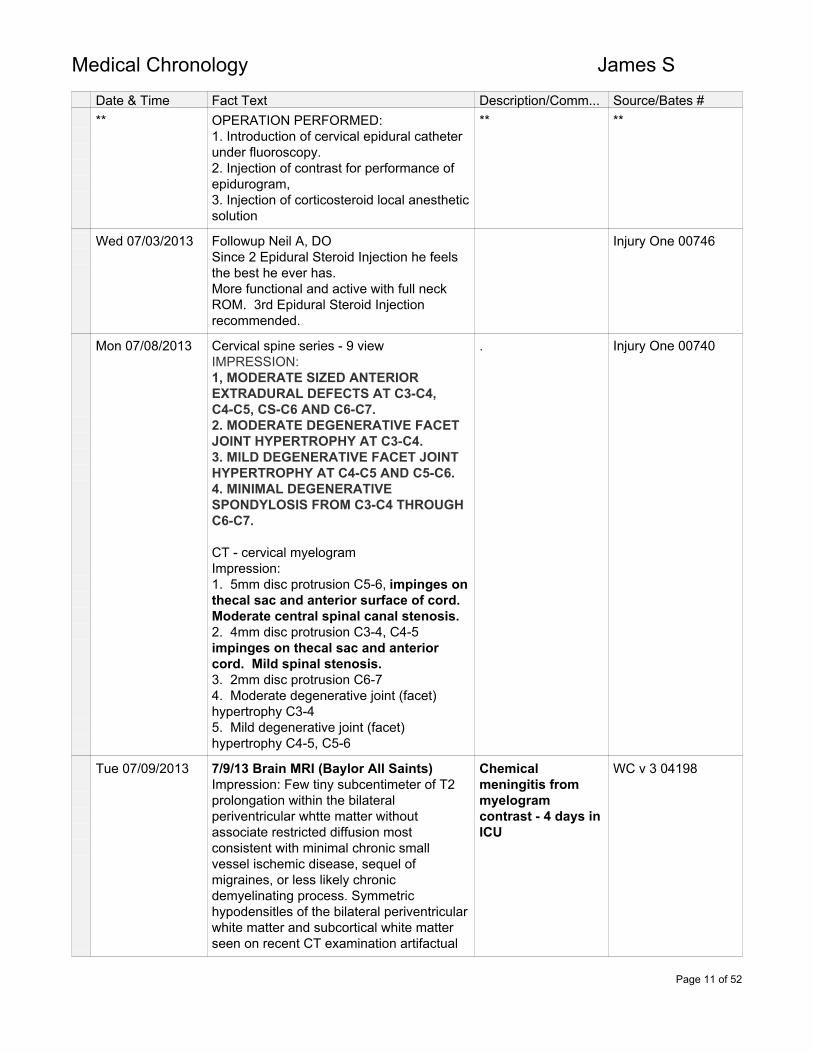
Date & Time Fact Text Description/Comm... Source/Bates #** OPERATION PERFORMED:
1. Introduction of cervical epidural catheterunder fluoroscopy.2. Injection of contrast for performance ofepidurogram,3. Injection of corticosteroid local anestheticsolution
** **
Wed 07/03/2013 Followup Neil A, DOSince 2 Epidural Steroid Injection he feelsthe best he ever has.More functional and active with full neckROM. 3rd Epidural Steroid Injectionrecommended.
Injury One 00746
Mon 07/08/2013 Cervical spine series - 9 viewIMPRESSION:1, MODERATE SIZED ANTERIOREXTRADURAL DEFECTS AT C3-C4,C4-C5, CS-C6 AND C6-C7.2. MODERATE DEGENERATlVE FACETJOINT HYPERTROPHY AT C3-C4.3. MlLD DEGENERATIVE FACET JOINTHYPERTROPHY AT C4-C5 AND C5-C6.4. MINIMAL DEGENERATlVESPONDYLOSIS FROM C3-C4 THROUGHC6-C7.
CT - cervical myelogramImpression:1. 5mm disc protrusion C5-6, impinges onthecal sac and anterior surface of cord.Moderate central spinal canal stenosis.2. 4mm disc protrusion C3-4, C4-5impinges on thecal sac and anteriorcord. Mild spinal stenosis.3. 2mm disc protrusion C6-74. Moderate degenerative joint (facet)hypertrophy C3-45. Mild degenerative joint (facet)hypertrophy C4-5, C5-6
. Injury One 00740
Tue 07/09/2013 7/9/13 Brain MRI (Baylor All Saints)Impression: Few tiny subcentimeter of T2prolongation within the bilateralperiventricular whtte matter withoutassociate restricted diffusion mostconsistent with minimal chronic smallvessel ischemic disease, sequel ofmigraines, or less likely chronicdemyelinating process. Symmetrichypodensitles of the bilateral periventricularwhite matter and subcortical white matterseen on recent CT examination artifactual
Chemicalmeningitis frommyelogramcontrast - 4 days inICU
WC v 3 04198
Page 11 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** in nature. Otherwise, normal MRI of the
brain. Specifically, no cerebral edema,mass, acute infarct, or extra-axial fluidcollection.
** **
Tue 07/09/2013 H&P Martha D, DO - Baylor admission
The patient has been admitted to thehospital in intensive care unit at this time.Dr. D with Pulmonary Critical Care hasbeen consulted on the case. [see above]
ASSESSMENT AND PLAN:1. Possible sepsis with leukocytosis andelevated segmented neutrophils. Again, thepatient has been started on vancomycin,will also be receiving Rocephin, as well asIV fluid. Recheck lactate in morning. Bloodcultures are pending. Urine culture ispending. The patient is to have MRI andsubsequent lumbar puncture in the nearfuture. We will adjust antibiotics based onculture data as needed.
2. Severe headache status postmyelogram. As needed morphine andNorco have been ordered. Lumbar punctureis dependent upon results of MRI. We willcontinue to monitor closely.
3. Mild hyperkalemia. Monitor potassium.
4. History of hypertension. Continue onlisinopril.
5. Diabetes mellitus. Place on sliding scaleinsulin before meals and at bedtime.Monitor blood sugar glucose closely.
6. Chronic pain disorder. Treat as needed.
7. Gastrointestinal prophylaxis withProtonix. Deep venous thrombosisprophylaxis with bilateral lower extremitysequential compression devices.
Pulmonary consult - Stephen D, MD
ASSESSMENT:1. Headache postmyelogram.2. Leukocytosis.3. Possible encephalopathy.
WC v 3 04166;04170
Page 12 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** PLAN:
1. Because he had a lumbar myelogramyesterday, with a white count and a fever Iam concerned that he could have aninfectious process within the CNS. MRIis pending due to the concern for cerebraledema. If he hassignificant cerebral edema, LP would not be safe. Otherwise, he may need an LP either later tonight or in themorning, based on his clinical course andthe results of the MRI.2. Diabetes. The patient's sugars will bemanaged at least temporarily with an insulinsliding scale.3. Hyperkalemia. The patient's potassiumwill be rechecked.4. Leukocytosis. As mentioned, this may berelated to a CNS infection; however, it mayalso represent simply a stress response tothe events of the last 24 hours. This willalso be monitored.
** **
Wed 07/10/2013 Consult report - Bryan Y, MD
ASSESSMENT AND PLAN:This is a 58-year-old with obesity, diabetes,hypertension, chronic pain, undergoingmyelogram on July 8 presenting withheadaches, nausea and vomiting along withback pain. Noted to have leukocytosis andrenal insufficiency. Spinal fluid showsprofound pleocytosis [increasedlymphocytes in the CSF] and elevatedprotein; however, his glucose is normal. Heis relatively afebrile and appearsuncomfortable, but not grossly toxic.Certainly, a secondary bacterial infectionfrom the procedure is possible; it is high onthe differential. However, I would expect alow glucose with this high of a white bloodcell count. Chemical meningitis from themyelogram should also be in thedifferential.PLAN:1. Continue vancomycin and ceftriaxone fornow, but change the ceftriaxone to q.12hour dosing.2. Change ceftriaxone to cefepime if heclinically deteriorates.3. Consider steroids if cultures remainnegative.4. Monitor cultures.5. Attempt to get outside records regarding
WC v 3 04173
Page 13 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** medications administered during the
myelogram.6. Send CSF for fungal culture.
** **
Wed 07/17/2013 Discharge Summary from Baylor All Saintsby Sally G, CNP
BRIEF HOSPITAL SUMMARY:This is a very pleasant 58-year-oldgentleman who presented to Baylor AllSaints with extreme fever, leukocytosis,and headache after myelogram. Thepatient presented to the hospital on the 9thof July, had myelogram on the 8th. Initially itwas offered by physician who performedthe myelogram that the patient could get ablood patch, but there was concern forpossible meningitis. The patient was startedon empiric antibiotics, pan cultures weredrawn. The patient was subsequently sentfor a lumbar puncture. Blood cultureshowed no growth. Urine cultureshowed no growth. Cerebrospinal fluidwas also negative. The patient's feversimproved, WBCs were also improving. Thepatient was weaned off of IV antibiotics, onthe day of discharge the patient has beenoff of antibiotics for approximately 48hours with continued improvement inWBCs and afebrile status. The patient'sheadache has significantly improved.The patient states that his pain is mostly athis baseline level. The patient is agreeableto discharge home, has no furthercomplaints or concerns.
DISCHARGE DIAGNOSES:1. Questionable chemical meningitis.2. Diabetes mellitus type 2.3. Hypertension.4. Headache.
CONSULTANTS:1. Dr. Y with Infectious Disease.2. Dr. D of Pulmonary Critical Care.
PROCEDURES:Lumbar puncture.
Does not confirm adefinite chemicalmeningitis diagnosis;only possible
WC v 3, 04177
Wed 07/24/2013 Followup Erwin C, MDRecently hospitalized in Ft Worthsecondary to aseptic meningitis fromcontrast medium given for his cervicalmyelogram. Followed by infectious disease
No signs ofmeningeal irritation
Erwin C, MD0003
Page 14 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** specialist.
Examination: no signs of meningealirritation.
** **
Wed 07/31/2013 Psychotherapy session with Veronica I,LPAComplains of nausea - almost passes outSunlight provokes headache and nausea
Compensable psychosocial stressors: - work related injury and pain - physical limitations - sleep disturbance - depression and anxiety; interferes withADL's
GAF (Global Assessment of Functioning)score - 50 Preinjury score - 85+
Diagnoses: Cognitive disorder, severemajor depressive disorder (MDD) withoutpsychotic features and pain disorderassociated with psychiatric and medicalconditions
GAF scoremeasures the social,occupational andpsychologicalfunctioning of adults.The score can range1-100 with 100 beingthe highestfunctioning level.
Injury One 00274
Thu 08/01/2013 To Baylor Emergency roomReferred to go there by Tuan T, DO forworsening headaches, nausea and tremors.Discharge diagnoses - chronic headachesand neck pain.
Baylor Pg 18
Mon 08/05/2013 Followup Marvin V, MDExam: Tenderness of neck on palpationfrom the occiput C2 region down to C7. Noradicular pain into arms. Has impingementdisorder of both shoulders. Concernedabout his chemical meningitis he washospitalized for.Impression: Cervical syndrome withradicular symptoms with narrowing of spinalcanal associated with disc osteophytes.Worse at C5-6 but also at C4-5, lesser atC6-7Plan: Reviewed myelogram CT scan.Flexion/extension views did not showinstability. There is decreased lordosis(less curvature). Advised not to haveanything else done around cervical spinesuch as Epidural Steroid Injection or anytype of myelographic dye.
Marvin V, MD00004
Tue 08/06/2013 Office visit - Neil A, DOHeadache and neck pain resolved afterconcussion/headache treatment, cognitive
Head and neck painresolved * (seebelow)
Injury One 00737
Page 15 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** therapy and cervical Epidural Steroid
Injection's** **
Mon 08/12/2013 Followup Tuan T, DOThe patient stated that on today's visit thatthere has been a slight worsening of hisneck pain. He states that the pain of hisright shoulder is slightly more severe thenlast visit. Mr. S further stated that theleft shoulder pain has become slightly moreintense. In addition to these complaints thepatient stated that there is a mild degree ofincreased headache pain.
Examination of the right upper extremitywas performed:Inspection reveals no significant edema atthe right shoulder. Further evaluationreveals no unusual color, no visibledeviation, no evidence of any masses and acontusion is noted on the right shoulder.Soft tissue palpation indicates moderatemuscular hypertonicity of the rotator cuff.Further evaluation reveals severe intensityof tenderness, a moderate degree ofadhesions, no discernible swelling, andmoderate trigger points in the rotator cuff.
Examination of the left upper extremity wasperformed:There is no perceptible swelling notedduring inspection of the left shoulder.Examination also reveals no abnormalcoloration in the tissues, no evidence ofdeviation/ no evidence of masses, and acontusion is noted on the left shoulder. Softtissue palpation indicates a moderateamount of muscle tightness of the leftshoulder. Examination also reveals severeintensity of tenderness, a moderate degreeof adhesion, no noticeable edema, and amoderate degree of trigger points in the leftshoulder.
*complains of neckpain
Injury One 00809
Mon 08/12/2013 Followup Marvin V, MDRecently to ER for bad neck painradiating to shoulder. Bilateral shoulderpain. Right > left. Reviewed MRI ofshoulder. He did bring the MRI of theshoulder for my review and we wentthrough that. I would agree with theradiologist that there is definite signalchange in the supraspinatus whichwould definitely be compatible with a
*complains of neckpain
Marvin V, MD00004
Page 16 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** full thickness tear near its insertion.
Plan: Recommend to Tuan T, DO forinjection of shoulder if approved by teamthat was dealing with his chemicalmeningitis.
** **
Tue 09/03/2013 Followup Neil A, DOStill treated for post concussion headacheand syndrome but overall his neck andaffect have improved dramatically. Sleepstill problematic. Recommend 3rd EpiduralSteroid Injection.
Injury One 00736
Tue 09/10/2013 Followup Tuan T, DO
On today's visit, the patient reported there isa mild degree of increased neck pain. Hefurther reports he's been feeling more rightshoulder pain since his last visit. Mr.Shelton states that the pain of his leftshoulder pain is slightly more severe thenlast visit. He also reports that the pain in thehead has become slightly more intense .
Injury One 00809
Mon 09/16/2013 Followup Marvin V, MDReviewed CT MyelogramMultiple areas of dysfunction:Hard discs C3-4 and C4-5Osteophyte complex C5-6Foraminal narrowing at several levelsC5-6 area of most concernImpressions:1. Cervical spondylosis, discosteophyte complex with pressuretowards spinal cord center. More atC5-62. Impingement disorder and syndromebilateral shoulders. Right shoulder theworst.Plan: Suggest to Tuan Trinh, DO to doshoulder injections.
Multilevel discprotrusions andosteophytes withpressureon spinalcord
Marvin V, MD00002
Wed 09/18/2013 Office visit Scott F, DOChief complaints: Headaches and headinjury Cervical neck pain Bilateral trapezius musclepainCervical pain 9/10 throughout all ROMImpressionDisc herniation C5-6Axial cervical neck painCervical facet joint pain from traumaCervical spine paraspinal muscle spasmNew onset headaches and postconcussive
If medical treatmentfails would needC4-6 anteriorcervicaldiscectomy andfusion
Scott F, DO00007
Page 17 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** syndrome
Plan:Return in 2-3 weeks after next EpiduralSteroid InjectionPossibly benefit from medial branch blocksand possibly rhizotomy.If ineffective would need C4-6 anteriorcervical discectomy and fusion
** **
Tue 09/24/2013 Cervical Epidural Steroid Injection by NeilA, DO.POSTOPERATIVE DIAGNOSES:I. Chronic neck pain syndrome associatedwith cervical disk protrusion.2. Cervical radiculopathy.OPERATIONS PERFORMED:1. Introduction of cervical epidural catheterunder fluoroscopy.2. Injection of contrast for performance ofepidurogram.3. Injection of corticosteroid local anestheticsolution.
Epidural SteroidInjection for neckpain with leftradiculopathyCervical discprotrusion C2-3 thruC4-5
Injury One 00734
Wed 09/25/2013 Psychotherapy - Veronica I, LPA
Psychological: Mr. S states he isfeeling hopeful now that treatment appearsto be approved. He states he feels lessnervous and anxious and attributes this tonoticing he is making progress, for examplehe can drive himself in Ft Worth and Dallaswithout getting confused and lost.
Memory: says he has noticed it isimproving, for example he used to have tohave a list of his medications andhas noticed he is slowly learning them. Thismakes him hopeful that with treatment hemay remember more and more.
Medical: Mr. S reports he has beengetting steroidal injections for his neck, thelast one done yesterday 9/24/13
Physical: he reports he has not had PT butthat his doctors have okayed him to walk.In addition he has been doing stretchingand isometric exercises at home. Heshares that since the chemical meningitishe has felt weaker and this is the reasonhe does not sit around all day but tries tomove as much as his doctors allow.
Hearing: His hearing goes "in and out" and
Injury One 00271
Page 18 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** explained it feels like the volume is turned
up and down.
Sleep: is sleeping 2 hours per night andtwo 15 minute naps during the day
** **
Wed 10/02/2013 Psychotherapy - Veronica I, LPA
Psychological & cognitive: reports he isfeeling optimistic today because he hadanother injection and notices that it not onlylowers his pain, but also, because his painis reduced, he is able to think more clearly.
Medical: had injection and reports that hehas been having night sweats and feelsclammy; he said this does not worry himbecause he usually feels these symptomsfor a few days after injections and then theygo away.
Sleep: continues to sleep only 1-2 hoursper night
Injury One 00267
Wed 10/09/2013 Followup Neil A, DONeck, shoulder and arm pain haveimproved >70% with epidural block.Pain and mentation improved
Injury One 00733
Mon 10/14/2013 Followup Tuan T, DO
ASSESSMENT: The patient has shownsome progress but is in a subacute phase.722.0 Cervical DiscDisplacement/Herniation729.2 Neuralgia, Neuritis, and Radiculitis,840.4 Rotator Cuff (Capsule) Sprain784.0 Headache850.9 Concussion, Unspecified
Referred to Injury One OMR program(rehab)
Injury One 00815
Wed 10/16/2013 Psychotherapy session with Veronica I,LPA
Psychological: Mr. S shares that hehas been feeling depressed and attributesthis to seeing that although he puts a lot ofeffort into his getting better, he still getsoverwhelmed by stimuli and stress, and canfeel tired and weak.
Physical: He continues to do exercises athome,
Injury One 00263
Page 19 of 52
Medical Chronology James
Date & Time Fact Text Description/Comm... Source/Bates #** and states the injection definitely has
helped.
Sleep: continues to sleep only 1-2 hoursper night
** **
Wed 10/16/2013 Followup Scott F, DOImpression:Axial cervical neck painDisc herniation C5-6Cervical facet joint painParaspinal muscle spasm bilateral cervicalspineParaspinal muscle spasm bilateraltrapezius muscle
Recommend:Continue home therapyMay begin return to work programContinue to see pain specialistIf reoccurrance or exacerbation ofsymptoms, may require C4-5 discectomyand fusion
Per Scott Farley,DO, If reoccurranceof symptoms, mayrequire C5-6discectomy andfusion
Scott F, DO00011
Wed 10/23/2013 Physical Performance Evaluation (FCE) byJoe Y, DCRecommends:Psych eval for emotional complicationsOutpatient Medical Rehab program
Does not meet requirements to do theirjob safely, confidently and effectively.
Tx Medical Institute00018
Wed 10/23/2013 Psychotherapy session with Veronica I,LPA
TxMut Rec pg 30
Thu 10/24/2013 Office visit Erwin C, MDImproved. Occasional headaches not asbad.Headaches probably cervicogenic.Trying to enroll him in long term brain injuryprogram.
Headaches lesssevere.Try to enroll in longterm brain injuryprogram
Erwin C, MD0001
Thu 10/24/2013 Evaluation done for Outpatient MedicalRehabilitation
MULTIAXIAL DIAGNOSIS:Axis 1: 294.9, Cognitive Disorder, NOS309.89 Post Traumatic Stress Disorder307.89, Pain Disorder associated with bothpsychological factors & a medical condition,chronicAxis II: V71.09, No diagnosis.Axis Ill: Injury to Head, Neck, Back, Seemedical records.
Injury One 00253
Page 20 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** Axis IV: Primary support group, social
environment, economic1 and occupationalissues.Axis V: GAF 55 (current) Estimatedpre-injury GAF = 80
We concur with Erwin A C MD 'srecommendation that the patient participatein the neurocognitive behavioral program.
** **
Mon 10/28/2013 Texas Mutual Notice of Disputed Issuesand Refusal to Pay Benefits
Disputes compensability of diabetes,hypertension,meningitis, depression, cervicaldisplacement, cervical protrusions atC2-C7, disks at C3-C4 and C-4-5,CS-C6with a disk osteophyte complex, cervicalspondylosis, and impingementsyndrome bilateral shoulders
Texas MutualNotice of Disputedissues and refusalto pay benefitsMultiple notices ofthis for other datesas well.
Injury One CD pg787
Wed 11/27/2013 Designated Doctor Evaluation by FaridaV, MD as ordered by Division ofWorkers CompensationJames reported that fusion surgery wasrecommended but does not want it at thistime.Current pain 6/10. Worst - 10/10Pain increased by sitting, reaching,sleeping, pushing, lifting, standing, walking,pulling, carrying, bending. Pain relief withmedications and injections.Not at MMI (maximum medicalimprovement)Expected MMI 4/27/14Rationale: Continues to have neck andbilateral shoulder pain. Injections don't last.Not able to do ADL's at his usual pace.Pain pills makes it unsafe for him to drive.Post concussion syndrome is beingaddressed by psychologist. Recommendto continue psychiatric treatment andpossible get cervical fusion surgerywhich has been recommended.
Designated DoctorEval determined heis not at MMI butexpects him to be by4/27/14
Injury One 00478
Wed 12/04/2013 Followup Neil A, DOHaving new pain with increased activity.May consider epidural block
Injury One 00715
Thu 12/05/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Rated pain 7/10. Patient also reportsdecreased focus and difficulty
Injury One 00249,00251
Page 21 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** concentrating. ** **
Mon 12/09/2013 Note by Marvin V, MD:
This is an addendum for the dictation of09/16/2013.
IMPRESSION: 1. Cervical sprain/strain with preexistingdisk osteophyte complex.2. Shoulder sprain/strain with symptomssuggestive of impingement and irritationinto the rotator cuff. This is presentbilaterally but worse on the right.3. Head concussion but no neurologicalsequela evident at this time.
Marvin V, MD00001
Tue 12/10/2013 Group Psychotherapy session InjuryOne/OMR cognitive rehab session
The patient attended the group andengaged in group process.
This was his first CogMed session. He wasorientated to the computer program and thepurposes behind it.
Injury One 00246
Wed 12/11/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Was receptive to the group topic. Patientwas actively engaged in the experientialgroup exercise.
Patient was seen this date for OMRProgram as per plan. Patient participated inthe activities listed above. Neutral spine andstabilization concepts were practiced.Patient utilized proper body mechanictechniques.
Injury One 00237,00240
Thu 12/12/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
The patient was observed attending andparticipating in the group process.
Second Cognitive rehab session. Hereported the activities were challenging butthat he was able to get through themwithout any help from the therapist.
Injury One 00232,00235
Fri 12/13/2013 Farida V, MD DDE states:
Functional Capacity Exam by Howard L
Injury One 00486
Page 22 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** DC concluded he is able to return to
work with restrictions.** **
Fri 12/20/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
The patient was receptive to the grouptopic. Patient was actively engaged in theexperiential group exercise.
Patient was seen this date for OMRProgram as per plan. Patient participated inthe activities listed above. Neutral spine andstabilization concepts were practiced.Patient utilized proper body mechanictechniques.
Injury One 00223,00227
Mon 12/23/2013 OMR BIOFEEDBACK THERAPY NOTE
DESCRIPTION OF TREATMENTPROVIDED: As this was the patient's firstsession of Biofeedback, Biofeedback, thesensors and rationale were explained.
Biofeedback training included: pain controltechniques, instructions in abdominalbreathing, & guided imagery.
Group therapy: The patient was involved inthe psychotherapeutic group. The patientwas expressive in the group process.Patient engaged appropriately with staff andother members of the group.
Injury One 00212,00215
Tue 12/24/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000606
Thu 12/26/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
The patient attended the group and wasengaged in the group process. Translationwas provided during facilitation of groupcommunication and interaction.
Injury One 00203
Fri 12/27/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000616
Mon 12/30/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000622
Tue 12/31/2013 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000627
Thu 01/02/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000630
Page 23 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #Fri 01/03/2014 Neurocognitive Rehab and Group
psychotherapy at Injury OneDr. S 000636
Mon 01/06/2014 Nicole M, Ph.D. letter ofopinion/causation re' his major depressivedisorder (MDD)"In my professional opinion and within areasonable degree of probability, Mr.Shelton's loss of physical functioningresulting from his injuries following themotor vehicle accident 04/1212012 was asubstantial factor in bringing about themajor depressive disorder.
Furthermore, in my professional opinionand within a reasonable degree ofprobability, the mechanism of injuryfollowing the motor vehicle accident, hasdisrupted his personal and vocationalfunctioning as he is unable to return to workat this time because of his injuries. Hehas also suffered significant interpersonalproblems as noted above. Mr. S'scontinuation to struggle with pain andfunctional problems that pose difficulty toperform routine demands of living andoccupational functioning are resultant fromhis work-related injury on 04/12/2012. Asa direct result of the pain and physicallimitations caused by the 04/I 2/2012 injuryMr. S developed the majordepressive disorder. Therefore, it is myclinical opinion that Mr. S'scompensable injury of 04/12/2012 alsoproduced major depressive disorder."
Nicole M,Ph.D. letter ofopinion on James'MDD
Injury One 00474
Mon 01/06/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000640
Tue 01/07/2014 Physical Performance Evaluation (PPE) byJoe Y, DCDetermined he is unable to perform regularjob duties.
Tx Medical Institute00024
Tue 01/07/2014 REASSESSMENT FOR CONTINUATIONIN OMR
Mr. S has completed 5 Cogmedtraining sessions. His overall startingCogMed index score was 78. After 5sessions his overall index score hasimproved to 93 revealing a 15 pointimprovement.
Injury One 00154
Tue 01/07/2014 Consultation with Ranil N, MD at Dallas Dr. N refused to Dr. Scott
Page 24 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** Spinal Rehab Center
Today he reports he continues to have painin his neck that can go to his shoulders. Healso has headaches. He can havenumbness and tingling and a sharp likepain in his shoulders and down the left arm.He has stabbing like pain in his hand, neckand shoulder. He rates his pain leveltoday at a 9. He has pain going up anddown his upper back as well. He deniesany history of similar injuries in the past.Occasionally he can lose use of the armsand shoulders.
RECOMMENDATIONS:The patient was here to see if we wouldtake over his case. After reviewing his casehe was informed I would not be able to takeover his case. There was nothing furtherthat we can offer him. There is a lot ofdispute including involvement of hisshoulders and that is why apparently whyhe has not been able to see a shoulderspecialist regarding his rotator cuff tears.
take his case. 000270-000273
Tue 01/07/2014 Reassessment for continuation in OMR atInjury One
Dr. S 000645
Wed 01/08/2014 History and physical by James G,MDImpression: Chronic left and right shoulderpainHeadachesHistory of head injury
Injury One 00690
Wed 01/08/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000667
Wed 01/08/2014 Followup Neil A, DO
His pain is improved more than 60% to70%. His remaining pain appears to befacet in origin. He has exclusive tendernessover the facet joints associated withcervicogenic headache. his main complaintappears to be over the facet regions,particularly on the left neck area C2-3,C3-4, and C4-5 where he has moderatetenderness with decreased neck range ofmotion. His pain does radiate into hisshoulder and we will go ahead andschedule him for injection therapy, pendinginsurance authorization.
Dr. S 000673
Page 25 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #Thu 01/09/2014 Neurocognitive Rehab and Group
psychotherapy at Injury OneDr. S 000674
Wed 01/15/2014 Followup Scott F, DONeck pain improving and lower left armnumbness/tingling. Neck pain fluctuatesfrom medium to high pain level.Bilateral shoulder pain especially whenreaching overhead or behind. Difficultysleeping on shoulders
Impression: Axial cervical neck pain withC5-6 herniationFacet joint pain of cervical spineParaspinal muscle spasms bilaterally andparacervical and trapezius musculatureInternatl derangement bilateral shoulders,possible impingementRefer to Michael Taba re' shoulders
Axial cervical neckpain with C5-6herniationFacet joint pain ofcervical spineParaspinal musclespasms bilaterallyand paracervicaland trapeziusmusculatureInternatlderangementbilateral shoulders,possibleimpingementRefer to MichaelTaba re' shoulders
Scott F, DO0014
Tue 02/04/2014 Followup Neil A, DOExcellent results with first Epidural SteroidInjection; improved ROM.Taking Lexapro, Ambien, Norco,gabapentin
Injury One 00663
Wed 02/05/2014 Followup James G, MD
CHIEF COMPLAINT: Left shoulder pain,right shoulder pain, and neck pain. He hasa history of closed head injury. (I do notsee cervical spine as a compensablebody part)
PHYSICAL EXAM: Left shoulder and rightshoulder-mild pain on abduction greaterthan 120 although he has full abduction.Reflexes are normal in both upperextremities. There are no motor or sensorydeficits noted in the extremities. Cervicalpain on range of motion in all directions.There is no spasm and no other motor orsensory deficits noted.
IMPRESSION:1. Left shoulder strain2. Right shoulder strain3. Closed head injury-concussion
PLAN:He is currently disputing the compensableinjury list. I'm recommending continuation ofthe brain injury program.
Does not seecervical spine ascompensable injury
Injury One 00134
Page 26 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #Thu 02/20/2014 Neurocognitive Rehab and Group
psychotherapy at Injury OneDr. S 000686
Fri 02/21/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000692
Mon 02/24/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000696
Tue 02/25/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000702
Thu 02/27/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000708
Fri 02/28/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000712
Mon 03/03/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000718
Tue 03/04/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000724
Fri 03/07/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000730
Mon 03/10/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000735
Tue 03/11/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000740
Wed 03/12/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000747
Thu 03/13/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000750
Fri 03/14/2014 Neurocognitive Rehab and Grouppsychotherapy at Injury One
Dr. S 000754
Tue 03/18/2014 OMR (Outpatient Medical Rehab) TeamConferenceDiagnoses: Closed head injury -concussionHe has been making significantbreakthroughs from his treatment. Hascompleted 7 sessions of Cogmed. Startingscore 78. Current - 94 showing a 16 ptgain.
He attended his neuro rehab sessions forthe day
Injury One 00031
Wed 03/19/2014 Followup James G, MDCC: Forgetfulness; neck and shoulder painImpression: Bilateral shoulder strainClosed head injury - concussion
Injury One 00021
Page 27 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** Plan: Recommend to continue Brain Injury
Program Referral to ortho for shoulders No lifting > 20 lb
** **
Wed 03/19/2014 Evaluation for OMR by Blythe TLPA, PsyDJames states he still experiences most ofthe symptoms he had prior to startingthe program but that most of them haveimproved significantly.It is recommended he continue in theneurocognitive behavior program.Diagnoses:331.83 Mild neurocognitive disordersecondary to brain injury.309.81 Post traumatic stress disorder300.82 Somatic symptoms disorder;persistant and severe
Diagnoses includesSomatic symptomsdisorder; persistantand severe. This isdefined as a mentaldisorder wherephysical symptomssuggest an illnessor injury but cannotbe explained by ageneral medicalcondition. Seesummary for moredetails.
Injury One 00024
Thu 03/20/2014 PPE by Joe Y, DC
Objective improvements in static strengthand dynamic lifting. Unable to performregular job duties at this time.
Recommend:Psych evaluation for emotionalcomplicationsParticipate in OMR programAccording to the objective findings from thetesting including: PILE lifting, static lifting,the clinical examination, and all otheractivities previously mentioned in thisreport; it is my opinion that this evalueedoes not meet the requirements, safety,and performance ability to do their jobsafely, effectively, and confidently (withoutrestrictions). The evaluee is not capable ofperforming their job duties (withoutrestrictions) until they demonstrate objectiveimprovement and the ability to performsafely and efficiently at their place ofemployment.
Tx Medical Institute00030
Tue 03/25/2014 OMR team conference with Injury One
Patient has been observed to make somesignificant breakthroughs while in treatmentwhich are visible in affect, increasedparticipation in groups etc.
Dr. S 000336
Mon 03/31/2014 Followup Neil A, DOJames is disappointed regarding denial fortreatment. Neil A, DO documents his
Injury One 00644
Page 28 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** frustration and states "I am appalled by this
peer review."** **
Wed 04/02/2014 Injury One request for additional hours forcognitive rehabilitation program
Dr. S 000337
Thu 04/10/2014 Evaluation for MMI by Chad B, DC
Determined to have 9% whole personimpairment using the AMA guide 4thedition.
Broke down:Memory - 2%Balance/coordination - 2%Cervicothoracic - 5%
MMI examdetermined a 9%whole personimpairment
Injury One 00299
Thu 04/24/2014 Reconsideration Determination / Peerreview by Maroj M, MD for medicalnecessity of requested additional 80 hrs ofCognitive Rehab.
It is noted that the patient has alreadyundergone 160 hours of treatment in hiscognitive rehabilitation program and hasalready shown improvement in severalfunctional outcomes. Given the substantialamount of treatment already provided andthe improvements already made, it isunclear why his remaining deficits andgoals could not be addressed withoutfurther intensive supervision in the contextof a cognitive rehabilitation program. Inagreement with the previousdetermination, the medical necessity ofthis request is not substantiated at thistime.
Peer review foradditional 80 hrscognitive rehab wasdenied
WC v 1 01493
Tue 04/29/2014 Followup Neil A, DOContinues to have mental fatigue,decreased neck ROM and stiffness.Continues on Norco and neurotin. Waitingto proceed with #2 Epidural SteroidInjection
Injury One 00642
Wed 05/21/2014 IRO review for dispute of MR CognitiveRehab Program - request for an additional80 hrs.- Previous denial upheld."Medical documentation does not supportthe medical necessity of the health careservices in dispute". It was determined hehas not shown much improvement and hewas determined to be at MMI on 4/10/14. Itwas further noted that he does not meet
IRO review - uphelddecision to denycognitive rehab.
Injury One 00579
Page 29 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** ODG requirements ** **
Wed 05/21/2014 Another review for approval of cognitiverehab concludes:
The second reviewer seems to haveproduced a correct opinion in stating thatthe ODG requirements have not been met.The employee is currently assessed ashaving reached MMI; the employee is nowable to drive, and should therefore havetransferrable skills for employment; andfinally, the requesting clinic has notprovided any evidence that continuedtreatment will result in a furtherimprovement in symptoms.
Additional review forcognitive rehabagain denies medicalnecessity
WC v 1 01457
Tue 05/27/2014 Followup James G, MDCC (chief complaint): Bilateral shoulderpain. Periods of forgetfulnessImpression:Bilateral shoulder strainClosed head injury - concussionPlan: Request another FCE (functionalcapacity eval) in anticipation of discharge.OMR program deniedNo lifting > 20 lb
Injury One 00014
Tue 06/03/2014 Epidural Steroid Injection with contrastDiagnosis:1. Chronic neck pain with multilevelcervical disc protrusion and left cervicalradiculopathy2. Chronic headache associated withcervicogenic and cervical facet syndrome3. Post intracranial head injury with postconcussion syndrome
Pine Creek medicalPt 1 0008
Wed 06/04/2014 FCE (Functional Capacity Eval) by JoeY, DCHas lack of cardiovascular fitness due todeconditioning.Currently cannot safely perform their jobdemands.
Tx Medical Institute00036
Thu 06/05/2014 Followup Neil A, DO
Reports more than 75% improvement of hisneck, left shoulder, arm, and hand paincomplaints following Epidural SteroidInjection therapy. As he has improvedfunction and decreased medications, weare going to go ahead and recommend asecond cervical epidural block. Each blockshould offer further and further
WC v 1, 01423
Page 30 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** improvement. ** **
Tue 06/24/2014 MRI Left shoulder
Impression:1. Mild to moderate spurring and edemaalong the acromioclavicular joint with mildac space narrowing.
2. Supraspinatus and infraspinatustendinosis without discrete rotator cufftendon tear.
Scott F, DO0040
Wed 06/25/2014 Followup James Galbraith, MDCC: cervical and bil shoulder painImpression:Left shoulder strainRight shoulder strain; possiblederangementCervical disc disease
Injury One 00012
Thu 07/03/2014 Followup Neil A, DO
We are treating him for chronic neck painsyndrome associated with cervical diskprotrusions and post-concussion headsyndrome. He has done well with thecombination of medication managementand injection therapy. His life has improveddramatically as he states.
He is showing good range of motion. He stillhas intermittent shooting pain in his left armand hand and today he has anapprehension test positive about his rightshoulder consistent with the rotator cuff tearsustained while on the job. He has apositive drop arm test as well. He is beingreferred for orthopedic evaluation.
Dr. S 000372
Wed 07/09/2014 Followup Scott F, DOTo have another Epidural Steroid Injection7/15/14States they help - he localizes pain to baseof his neck with rotation of head/neck andpain with extension. Neck and shoulderpain is at high end of pain scale.Impression1. Disc herniation C5-62. Axial cervical neck pain3. Facet joint pain secondary to trauma4. Cervical paraspinal muscular spasms5. Bilateral shoulder pain
Scott F, DO0017
Fri 07/11/2014 Followup Neil A, DO The apprehension Dr. S 000373
Page 31 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #**
Was approved for Epidural Steroid Injectiontherapy for his neck pain. He is beingworked up for shoulder pain as he recentlybad an MRI of the left shoulder, whichshowed some acromioclavicular spacenarrowing, spurring, and edema. We willrefer him for surgical evaluation. Injectiontherapy into AC joint may also be advised.
Apprehension test and drop arm test werenegative.
test is used todetermine if a patienthas suffered aninjury of theirglenohumeral joint.
The drop arm testchecks for asupraspinatus tear.
**
Tue 07/15/2014 Epidural Steroid Injection by Neil A, DO
PRE and POSTOPERATIVE DIAGNOSES:1. Chronic neck pain syndrome associatedwith cervical radiculopathy.2. Multiple level cervical disk protrusion.
OPERATIONS PERFORMED:1. Introduction of cervical epidural catheterunder fluoroscopy.2. Injection of contrast for performance ofepidurogram.3. Injection of corticosteroid local anestheticsolution.
Dr. S 000374
Thu 07/17/2014 Follow up Neil A, DO
Mr. S is pleased to report morethan 70% to 80%improvement of his neck, shoulder, andarm pain complaints following a singlecervical epidural block. He is morefunctional and more active. He states he isable to lift things and have better feeling inhis arms and hands.
We are going to go ahead and arrange for asecond procedure pending insuranceauthorization.
Dr. S 000376
Fri 07/25/2014 Cervical Spine XrayImpression: Mild disc space narrowingC5-6. Mild degenerative changes
Injury One 00373
Tue 07/29/2014 Followup James G, MDChief complaint: Neck and bilateralshoulder painImpression:Left shoulder strainRight shoulder strain; possiblederangementCervical disc disease
Injury One 00010
Page 32 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** Plan: See Scott Farley, DO No lifting >10
lb** **
Fri 08/01/2014 Followup Scott F, DOContinues to have significant pain. ADL'sare difficult and cannot reach. States cantlive with the painImpression:1. Severe facet joint arthrosis C3-C62. Disc herniation C3-C63. Severe axial neck pain4. Left arm pain and radicular symptomsPlan: Medial branch blocks left cervicalspine at C3-4, C4-5, C5-6. If doesn't workthen he will require anterior discectomy andfusion.
Scott F, DO0020
Sun 08/10/2014 Neuropsychological evaluation by Bob GantReport completed on 9/18/14
Dr. Valliani requested the evaluation todetermine if he is at MMI and provide animpairment rating (IR)
CONCLUSIONRecently completed neuropsychologicaltesting documents that Mr S iscontinuing to suffer from significantneurobehavioral and neurophysiologicalproblems over 2 years post injury.
Deficits noted in the domains of processingspeed, verbal reasoning, verbal memory,and dominant motor/sensory functioning.
The patient has received substantialmedical treatment and appears to be atMMI over 2 years post injury.
lt appears that Mr. S has evidence ofpersistent and chronic neurobehavioral,neurophysiological, neuropsychologicalimpairment. Suggests an impairmentrating of 15-20% for neuropsychologicalimpairment.
Bob G documents Mr. S hadinconsistent effort on some tests so testresults may not be uniformly valid. Healso states he was over reporting onsomatic and cognitive complaints.
The results indicatehe is continuing tosuffer fromsignificantneurobehavioral andneurophysiologicalproblems over 2years post injury.
Inconsistent efforton tests as well asover reportingsymptoms - sosome results maynot be valid.
Recommended IR -15-20%
Dr S 00007,00015-00016
Wed 08/13/2014 Designated Doctor Exam (DDE) by FaridaV, MD;
He assigned a 21%WPI
Dr. S 000855 -000868
Page 33 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** His 2nd DDE
Compensable injuries:Head concussion with post concusslonsyndrome, tendinopathy and full thicknessrotator cuff tear - right shoulder, herniateddisc C5-6 causing moderate spinal canalstenosis, herniated disc C3-4 and C4-5causing mild spinal stenosis, headachesand forgetfulness secondary to concussion
MMI DATE AS ASSIGNED Per thisEXAMINATION and THIS EVALUATOR:Statutory on 04-17-2014
IMPAIRMENT RATINGRIGHT SHOULDER: Range of motionyields 3% Whole Person ImpairmentHEAD: Concussion with residual persistingpost-concussion symptoms affecting hisneuropsychological functioning is assigneda 5% whole person impairmentCERVICAL SPINE DRE: CATEGORY II:5% whole person impairment
15% [previous IR?] combined with 5% =19% combined with 3% = 21% wholeperson impairment
** **
Tue 09/02/2014 Followup Neil A, DO
Dr. F has concerns over cervical facetsyndrome. My diagnosis today continues tobe multiple levels of diskprotrusion with radiculopathy. We revieweda letter from a peer review doctor whodenied this gentleman cervicalfacet treatments.
Dr. S 000377
Wed 09/10/2014 Followup Neil A, DO
No changes in symptoms. Will schedule fortrigger injections in the near future.
Dr. S 000378
Tue 10/14/2014 Peer review of Dr. V's DDE by CaseyC, DO for Tx Mutual
SPECIFIC QUESTIONS:1. Is the whole body impairment assignedan objective, accurate, fair and reproducibleevaluation of the injured worker's medicalimpairments?
A. No. The doctor assigned a 15%
Due toover-reporting ofsymptoms he wouldnot assign animpairment rating forBI. He assigned 8%for neck andshoulders
Dr. S00029-00032
Page 34 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** impairment based on Dr. G's report
suggesting IR of 15-20%. He did notreference any specific charts, graphs ortables of the AMA Guides. The reportwould be invalid.
Dr. G's report under the MMPI test, itwas stated that the claimant's profileindicated over-reporting ofpsychological dysfunction, mild overreporting of somatic symptoms, as wellas significant over reporting ofcognitive complaints. Perhaps thisexplains why the suggested impairment isnot consistent with the individual's actualfunction.
The doctor also assigned a 5% impairmeutfor cervical complaints. This would meetAMA Guides criteria.
2. Is the methodology applied indetermining the injured worker's wholebody impairment in compliance with theAMA Guides to the Evaluation ofPermanent Impairment, Fourth Edition?
A. The doctor did use the correctmethodology. However, the doctor didnot apply the methodology correctly.
3. Is the rating based on the compensableinjury alone?A. Yes.
4. Is the clinical history presented by theevaluating doctor's report supportive of theassessed impairment?
A. No. The extreme amount ofimpairment assigned for mental statusimpairment is not consistent with theclinical record. Even the testing that wasdone indicated that the individual was overreporting his symptoms and to a significantdegree, the symptoms for cognitivefunction. However, this amount ofimpairment is not consistent with his actualfunction, as the claimant clearly was ableto go out and about in the communityand does not require direction andsupervision of his daily living activities.
** **
Page 35 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** 5. Based on the compensable injury and
your review of the injured worker'simpairment rating report, what would beconsidered a reasonable assessment ofimpairment?
A. For the physiologic portion of theinjury, which includes the neck andshoulder, I would agree with a 5%impairment. That would then leave us withthe impairment for the head injury. At thispoint it is difficult to state that there isany supportive impairment since theindividual's symptoms were overreported. Before I would assignimpairment for this type of impairment Iwould obtain further additionalindependent neuropsychologicaltesting. At this point I can only confirman 8% impairment for the neck andshoulder.
** **
Mon 11/03/2014 Followup Neil A, DO
Continues to have chronic pain complaints.Still had some trigger points in his neck andupper back area, decreased neck ROM.
Dr. S 000379
Tue 12/16/2014 Designated Doctor Exam - AndrewB, MD
Report dated December 22, 2014- 44pages
After a very lengthy discussion and examhe concludes:The claimant is at Maximum MedicalImprovement August 6, 2013. This iswhen Dr. A documents that headachesand neck pain have all resolved and he isdoing much better. It is around this timeframe that all diagnostic studies have beencomplete, there is reference to havingnearly full range of motion, referring to theneck. There is also reference to nearly fullshoulder range of motion that isself-limited by Dr.G also in 2013, aswell as Dr. C documenting that mostsymptoms have subsided. There is alsoreference to multiple normal neurologicexaminations relative to upper extremities.
5% whole person impairment. This isbased on cervical only and nothing
He diagnosed himwith malingering dueto over-reporting ofcognitive symptomssuch asforgetfulness.
He also discussesthat Bob Gimpairment rating of15% is not valid orsubstantiated.
He assigned a 5%WPI
Dr. S00063-00072
Page 36 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** assigned for brain injury.
How he arrived at this impairment is anarrative discussion in which he points outsignificant over-reporting on things such asforgetfulness and headaches.
One of the neuropsychological tests headministered is "Test of MemoryMalingering" (TOMM). His scores wereconsistent with over-reporting memorydeficits.
DSM V Diagnoses were listed as thefollowing:
Axis I Mental Disorders:Persistent depressive disorder (dysthymia)MalingeringAxis II Personality and DevelopmentalDisorders:Rule out general personality disorderAxis III Medical Disorders:ObesityHypertensionPeriventricular white matter changes inthe brain on MRI secondary tohypertensionCervical sprain/strain and bilateral shouldersprain/strainDiffuse degenerative joint disease
** **
Wed 01/07/2015 Psychological Diagnostic Interview -Tommy O, EdD
Reason for referral: Mr. S wasreferred for evaluation to help developrehabilitation, pain management, andmedical plans.
Diagnostic lmpression:Axis I V79.09 Diagnosis Deferred, On AxisI. Refer To Dr. Bob 's EvaluationsAxis II- V79.09 Diagnosis Deferred On AxisII. Refer To Dr. Bob 's Evaluations
At this time I refer to the medical andphysical therapy evaluations for details. Dr.N believes that Mr. S is presentlyreceiving excellent support through Dr. Cand other healthcare providers. Mr. Sis going to return back to Dr. C and hisother healthcare providers for continued
Dr. S000272-000277
Page 37 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** support. ** **
Wed 01/07/2015 Physical performance evaluation at DallasSpinal Rehabilitation Center by C.B, PT. He states the DSRC teamdid not feel further rehab was warranted.
Dr. S 000946
Tue 01/27/2015 Followup James G, MD
CHIEF COMPLAINT: Patient has beenaddressing extent of injury with the carrier.He states the carrier is stating that thehead, neck and left shoulder iscompensable. He has seen Dr. Farley in thepast and was recommended for surgeryhowever it has not been done. In the pasthe has had two IRs, one with Dr. Blackwelland one with Dr. Gant. Dr. Gant addressedthe TBI which was not addressed in Dr.Blackwell's initial rating. He presently statesthat he has daily headaches that aresevere In nature. He states prior to theholidays he had some black out spellsand lost 24 lbs. over 6 weeks. He statesat times he forgets to eats and he hascognitive delayed. He has persistent neckpain is constant with left upper extremitynumbness and tingling with associatedweakness. Patient had a CT Myelogramthat showed a 5 mm Disc herniation at C5-6and a 4 mm at C4-5. He denies having anEMG/NCV. He states to date he has had 5cervical Epidural Steroid Injection's withminimal to no improvement.
PHYSICAL EXAM: Patient is cooperativeand concerned. Patient has difficulty attimes searching for words toexpress himself.
IMPRESSION:1. TBI2. Altered Mental Status3. Rotator Cuff Syndrome4. Post-Concussion Headaches5. Cervical Disc Herniation C4-5 and CS-66. Cervical Radiculopathy
PLAN:1. Recommend electrophysiologicaltesting to confirm radiculopathy of theleft upper extremity. Referral to Dr. C,MD; also to address the black outs.2. Consult for the left shoulder and right
Dr. R 00026
Page 38 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** shoulder with Dr. R.
3. Patient needs to be re-scheduled with Dr.F.4. Patient needs an alternate impairmentrating.
** **
Thu 02/05/2015 Followup Neil A, DO
Symptoms continue. Trigger injectiontherapy advised. Also discussed spinalstimulator.
Dr. S 000951
Tue 02/10/2015 Followup Scott F, DO
CHIEF COMPLAINT:1. Cervical neck pain.2. Left arm pain.3. Upper thoracic pain.
Continues to have significant pain in thecervical spine. He has pain both the rightand left side slightly greater on the left sideinto the bilateral trapezius musculature withpain with flexion, extension and rotation. Hehas severe pain rates it as 10/10. He hasdifficulty with all activity, pain with sleeping.The patient also has bilateral shoulder painfrom the time of the accident.
IMPRESSION1. Disc herniation from C3 to C6 with axialneck pain.2. Left arm radicular pain.3. Paraspinal muscle spasms and facetjoint pain cervical spine.
PLANI had a long discussion with the patientregarding his treatment.
On the last visit, I have recommendedmedial branch blocks to the cervicalspine. I will start on the left side at C3-C4,C4-C5, and C5-C6 and then a secondprocedure for right-sided facet injection. Hehas significant axial neck pain and I believethis would be beneficial for the patient.
If this is unsuccessful for the patient, thepatient will require a three-level cervicalfusion from C3 to C6. I discussed this withthe patient at length.
May need a cervicalfusion C3-C6
Dr. S 000955
Mon 02/16/2015 Evaluation for MMI by Chad B, DC MMI exam Casa View 0008
Page 39 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #**
Determined to have 14% whole personimpairment using the AMA guide 4thedition.
Broke down:Upper extremity - 5% combinedNeurological - 4% combinedCervical spine - 5%
determined a 14%whole personimpairment
**
Wed 02/18/2015 Followup Erwin C, MD
Notes: continued headaches, tendernessand stiffness of his neck, limited ROM, midcervical pain which radiates laterally andupwardly into both sides of his head andinto the frontal region (greater occipitalnerve and lesser occipital nervedistribution). States he passes out off andon; loses consciousness and is disoriented.Has difficulty providing full effort uponmotor examination because of hisshoulder. However, abduction, lift off,external and internal rotation almost full.
AssessmentIntermittent, episodic blackouts.Continues with significant cognitiveproblems (already worked up andestablished).Cervical radicular syndrome.Cervicogenlc headaches.
PlanContinue chronic pain management with Dr.Atlin as currently doing.Ambulatory EEG, because of his episodicblack outs (patient declined EEG)Electrical studies of the upper extremities(EMG and NCV's).
Documents he is notable to make fulleffort due to hisshoulder but he hadnearly full ROM
Dr. S 000964
Fri 02/20/2015 Followup Robert R, MD
Chief Complaint: Right shoulder pain
IMPRESSION: Full-thickness right shoulderrotator cuff tear, head injury and cervicalspine injury with disk problems.
PLAN: The patient will come back and seeme again in 2 weeks for a cortisone shotinto the right shoulder subacromial bursalspace. This patient will require a rightshoulder open rotator cuff repair in the
Will need a rightshoulder openrotator cuff repairin the future
Dr. R0019-00021
Page 40 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** future. This is medically necessary for
his work-related right shoulder injurycondition.
** **
Fri 02/27/2015 Followup Scott F, DO
Essentially unchanged from previous.Again recommend medial branch blocksand possibly C4 to C6 anterior cervicaldiscectomy and fusion, if the blocks donot work.
Dr. S 000969
Fri 03/06/2015 Followup Robert R, MD
PROCEDURE: Steroid injection - rightshoulder
PLAN: I injected the patient's right shouldertoday. The patient will need an open rightshoulder rotator cuff repair. He needs to geta medical clearance from his primary carephysician. He will come back and see meagain in about 6weeks. We will not be able to do the rightshoulder rotator cuff repair until at least themiddle or the end of April of this year. Wemay go ahead and set up a rotator cuffrepair surgery in the future. I am not goingto request that today.
Shoulder injectiondone
Dr. R 00015,00016
Tue 03/10/2015 Followup James G, MD
CHIEF COMPLAINT: Patient currently hasbilateral shoulder pain and recently had asteroid shot with Dr.R last week and will have a second oneand if it does not improve he wants to dosurgery on the right rotator cuff. He hasalso seen Dr. A who is waiting forauthorization for trigger point injections withnerve block. Dr. F has done a recentsurgical evaluation and recommended forhim to have a 3 level fusion. There appearsto be some confusion with his statutory MMIas he has had one performed by Dr. G,Phd and one by Dr. B.
IMPRESSION:1. TBI2. Altered Mental Status3. Rotator Cuff Syndrome4. Post-Concussion Headaches5. Cervical Disc Herniation C4-5 and C5-66. Cervical Radiculopathy
Dr. S 000975
Page 41 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #**
PLAN:Patient needs a MD that is IR certified inTexas Mutual network to combine the TBIImpairment with musculoskeletal for thestatutory MMI as Dr. B is onlyqualified for musculoskeletal and G forpsych.
** **
Tue 04/07/2015 Cerescan [SPECT] report - S. GregoryH, MD
The scan was done on 3/25/15 andreported on 4/7/15
Neuropsychiatric and CognitiveAssessments:1) The Mini International NeuropsychiatricInterview (MINI) was administered to JamesShelton on 3/25/15. Accordingly, he metcriteria for the following. - Major Depressive Episode - MDE with Melancholic Features - Suicidality - Agoraphobia - Generalized Anxiety Disorder
2) The Montreal Cognitive Assessment(MoCA) was administered to JamesShelton on 3/25/15. His score was 24 andoutside the normal range of 26-30.
Impressions:This is an abnormal brain SPECT studydemonstrating focal areas of abnormalcortical hypoperfusion in the frontal,temporal, occipital and cerebellar areas,as previously described. There was aleft-sided predominance to many of thefrontal and temporal findings. In addition,focal areas of abnormal subcorticalhypoperfusion were noted in the basalganglia and thalamic nucleus, aspreviously described. Paradoxical corticaldeactivation is noted with theconcentration task. The nature, locationand pattern of these abnormalities isprimarily consistent with the scientificliterature pertaining to traumatic braininjury and the patient's clinical historywhich was received after the blindreview. Given the apparent functionalatrophy seen in the frontal lobe area,
Cerescan abnormal -consistent withliterature re' TBI andthe patient's clinicalhistory. However hisfrontal lobe atrophycombined with hiscognitive impairmentmay be due to anongoingfronto-temporalneurodegenerativeprocess.
Cerescan report
Page 42 of 52
Medical Chronology James Shelton
Date & Time Fact Text Description/Comm... Source/Bates #** along with the patient's evidence of mild
cognitive impairment (MCI) on the MoCAinventory, the possibility is raised that aportion of these findings might berelated to an ongoing fronto-temporalneurodegenerative process. Furtherclinical evaluation is recommended tofurther sort this possibility out to include thepossibility of repeat functional imaging in6-12 months with either brain SPECTand/or brain FDG PET imaging. Correlationwith the patient's entire medical history isalso advised.
** **
Wed 04/22/2015 Designated Doctor Exam by James S,MD
Compensable Diagnoses:1. Right shoulder tendinopathy; full RTC[rotator cuff tear]2. Headaches/forgetfulness due to postconcussion3. HNP C3-4, C4-5, mild stenosis4. HNP C-6, moderate stenosis
Primary focus: address the left shoulderEOI [extent of injury] and RTW issues.
Questions I Purpose of Examination:1. Extent of InjuryThe mechanism of injury was a vehicularaccident. The claimant sustainedcontusions and strains to the head, cervicalspine and shoulders.
Disputed Issue: Left shoulder rotator cufftearWhile the claimant presented initially withmultiple injuries including left shoulder pain.The claimant also states that more than onephysician has told him that he has damagethat requires surgery (the records do notreflect this, however). While my physicalexamination reflects significant guardingand pain behaviors, I found no evidenceof shoulder instability. In this case, theleft shoulder MRI of 6/24/2014 isdispositive: While degenerative changesand tendinosis were reported, the reportstates: "The soft tissues of the rotatorinterval. .. maintained ... without a discreterotator cuff tendon tear".
Concludes that thereis not a left rotatorcuff repair and is notpart of injuries andthat due to cognitive,behavior andmedication effectshe cannot work inany capacity.
Dr. S DDE 4-2200002,00006-00007,00017-00018
Page 43 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** Therefore there is no objective evidence
of rotator cuff tear; not part of extent ofinjury.
2. Return to Work Status- from 2/15/2015 topresent:Clearly, at the present time, cognitivesymptoms, chronic pain and behavioralissues are all major barriers to return towork. He cannot possibly pass the COLre-licensing examination, so return to truckdriving is not feasible. There is debate byhealth care professionals as to howmuch of the cognitive symptoms are dueto brain injury. There can be no doubtthat from a chronic pain and behavioralstandpoint, this man has a majoralteration to his pre-injury status.
In my opinion, this man is still not ableto work in any capacity. Even if oneconsiders the least physically demandingjobs, his behaviors, cognitive symptomsand medication side effects are all such thathe could not adequately function at theworkplace.
** **
Mon 04/27/2015 Baylor H&P -Taken by EMS to Baylor ER in severerespiratory distress. He was intubated andput on a ventilator. He was discharged5/5/15. His respiratory failure wasattributed to severe exacerbation of hisasthma.
This admission is notrelated to his MVCinjuries. I didascertain there werenot any relevantissues discussed inMD reports orrevealed indiagnostics. I did notfind anything relatedto his injuries.
Baylor 4.27.1500044-00048
Mon 05/04/2015 Medical Opinion Report by S. GregoryH, MD
His conclusions include:
According to available records, this injurywas at least a mild traumatic injury and bymedical documentation by Dr. C andothers, probably rose to the level of amoderate traumatic brain injury by criteriapreviously described. Following thistraumatic brain injury, the patient developedsymptoms of post-concussion syndrome asdocumented by almost every provider, saveDr. V, as previously noted. By
The actual report isdated May 4, 2013rather than 2015.Since his timelinereferences eventsfrom 2015 it is logicalto say May 4, 2015 isthe correct date.
A significant pointDr. H makesis that Mr. S'sbrain injury ispossibly a moderatebrain injury rather
Hipskind MedicalOpinion00001-00008
Page 44 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** definition, given that the patient's symptoms
persisted beyond 6 months, the patienttechnically developed persistentPost-Concussion Syndrome. The patient'ssymptoms of traumatic brain injury werevalidated both by neuropsychologicaltesting and objective brain SPECT imaging,which showed very good correlationbetween areas of impairment andweakness neuropsychologically and areasof brain abnormality associated with thosefunctionalities. As appropriately pointed outby Ms. Irvine in her evaluation,"Compensable psychosocial" effects ofthe traumatic brain injury are consistentwith the scientific literature (Jorge, 2007,Fann, 2004) indicating the developmentof emotional dysregulation following atraumatic brain injury which exerts a"double-whammy" effect on the initialcognitive insults."
Finally, regarding the status of Mr. S'straumatic brain injury, he was appropriatelyreferred to CereScan in Denver for brainSPECT imaging by Dr. G. The results ofthat study confirm objective evidence ofbrain injury to Mr. Shelton's frontal,temporal, occipital and cerebellar lobesas well as subcortically to his basalganglia and thalamic regions.
Interestingly, the blind read performed bymyself did show a relative left greaterthan right preponderance of injury whichcorrelates with the alleged anddocumented mechanism of injury.Further, the frontal lobe damagecorrelates with the patient's symptomsand findings of cognitive dysfunction,the temporal lobe findings correlate withthe central auditory processing issues,the occipital findings correlate withvision and balance issues as do thecerebellar findings. The basal gangliaand thalamic findings have beenreported to be involved with emotionalregulation issues. Thus, there appearsto be excellent correlation with thepatient's objective neuropsychologicalfindings and the brain SPECT imagingfindings. Of significant note is that thespecific patterns of traumatic injury
than mild due toconfusion of > 30min.
Also important thathe notes is: Thebasal ganglia andthalamic findingshave been reportedto be involved withemotionalregulation issuesand that thespecific patterns oftraumatic injuryseen here are notcapable of beingmanipulated bypatient effort."
**
Page 45 of 52

Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** seen here are not capable of being
manipulated by patient effort.** **
Fri 05/15/2015 Followup Robert R, MD
CHIEF COMPLAINT: Right shoulder pain.
IMPRESSION: He has a full-thicknessrotator cuff tear in the right shoulder.
PLAN: The patient will come back and seeus again in 2 months.
Dr. R 00007
Mon 06/01/2015 Neuropsychological Eval - Bob GDate of report - 6/2/15
This was his 3rd neuropsychological test.He underwent a battery of tests. He states,"Consistent with previous examinations,inconsistent effort was observed."The details are described in the report.
He documents: The degree to whichresponse styles may have affected ordistorted the report of symptomatology onthe inventory is also assessed. Certain ofthese indicators fall outside of thenormal range, suggesting that thepatient may not have answered in acompletely forthright manner; the natureof his responses might lead theevaluator to form a somewhatinaccurate impression of the clientbased upon the style of respondingdescribed below. With respect to positiveimpression management, there is noevidence to suggest that the patient wasunduly defensive or motivated to portrayhimself as being relatively free ofcommon shortcomings or minor faults.With respect to negative impressionmanagement, there are subtlesuggestions that the client attempted toportray himself in a negative orpathological manner in particular areas.Some concern about distortion of theclinical picture must be raised as aresult; the patient presents with certainpatterns or combinations of featuresthat are unusual or atypical in clinicalpopulations but relatively commonamong individuals feigning mentaldisorder. It is suggested that thecritical items, as well as certain aspects of
He notesinconsistent efforts.There are some testresponses by Mr.Shelton that mayrepresent he isfeigning mentaldisorder.
G June 201500001-00016
Page 46 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** the clinical history, be reviewed to evaluate
the possibility of such distortion. Althoughthis pattern does not necessarily indicate alevel of impression management that wouldrender the test results uninterpretable, theclinical hypotheses presented in this reportshould be reviewed with theseconsiderations in mind. The clinical scaleelevations may overrepresent the extentand degree of significant test findings incertain areas.
ConclusionsTesting provides evidence of a persistentpostconcussion syndrome/mild traumaticbrain injury as a result of the rolloveraccident on April 12, 2012.Neuropsychological inconsistencies areprobably related to variable effort providedduring the examinations. There isconsistent evidence however of persistentimpairment over time. Recently, evidence ofa brain injury was confirmed when a brainSPECT examination was completedconfirmingevidence of cerebral impairment.
The patient has been treated as part of hisworkers compensation claim. Based on thisclaim, he has beengiven a 20% impairment rating and isadministratively considered at MaximumMedical Improvement (MMI). Mr. Sdisplays evidence of permanentimpairment in his psychological andneurophysiological functioningincluding evidence of persistentcomplaints of pain, depression,imbalance, blurred vision, mild cognitiveimpairment, anxiety, headaches, etc.
Mr. S appears to be somaticallypreoccupied and dispirited. This appears tobe related to frustration he has experiencedas part of a dysfunctional workerscompensation system that significantlydelayed his access to treatment and hasprovided multiple barriers to his obtainingaccess for suggested medical care. Afterexperiencing multitrauma, he remains offwork with poor prospects for returning towork after 38 months of progressivedisability.
** **
Page 47 of 52

Medical Chronology James Shelton
Date & Time Fact Text Description/Comm... Source/Bates #**
Mr. Shelton continue to experiencesignificant barriers to recovery and returningto work including persistent psychologicalimpairment, persistent physiologicalimpairment, etc. He will need ongoingmedical care including access to clinicalneurology, psychiatry, andneuropsychology. In my opinion, he wouldbenefit from referral to a intensiveoutpatient brain injury rehabilitation programwhich provides multidisciplinary care.
** **
Tue 06/09/2015 Followup - Eric N, FNP-C under Dr.G
CHIEF COMPLAINT: PatientsNeuropsych IR with Dr. G ispending authorization which is due today.Hecurrently rates his pain a 8/10 with 10 beingthe worse pain imaginable in the bilateralshoulders, neck and head. He continuesto have cognitive difficulties andpersistent headaches. He states that hehas had more recent episodic fainting.
IMPRESSION:1. TBI2. Altered Mental Status3. Rotator Cuff Syndrome4. Post-Concussion Headaches5. Cervical Disc Herniation C4-5 and C5-66. Cervical Radiculopathy
PLAN:1. Check on status of approval as it is duefor a decision today for the Neuropsychevaluation.2. CCH on June 22 for extent of injury.3. Request records from Dr. G4. Form 73 Completed
Dr. R 00003
Fri 07/10/2015 Followup - Robert R, MD
CHIEF COMPLAINT: Right shoulder pain.
IMPRESSION: He has a smallfull-thickness right shoulder rotator cufftear.
PLAN: I am not going to schedule surgeryyet. He was very sick with acute respiratorydistress syndrome on 04/13/15. He has not
Dr. R 00002
Page 48 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** been medically cleared. He has not been
through all his court battles with his workinjury. He will come back and see me againin about 3 months in Fort Worth. He maycall before that time to get an injection.
** **
Wed 08/05/2015 Telephone call from Robert R, MD toDr. Rodney I.
I told him that the patient is going to need aright shoulder open rotator cuff repair for asmall full-thickness rotator cuff tear. I toldhim the cost estimate for the surgery andrehabilitation is around $75,000.
Dr. R 00001
Thu 08/06/2015 Designated Doctor Exam by James S,MD
Compensable diagnoses/codes are listedas:1) Post traumatic brain injury w/ postconcussi 850.02) Post traumatic headaches 339.203) Memory/cognitive/emotional dysfunction 780.93 Memory loss 331.83 Mild neurocognitive disorder 313.9 Unspecified emotional disturbanceof childhood4) Cervical strain 847.05) Cervical HNP 722.0 [this code iscervical disc displacement without myelopathy]6) R shoulder strain 840.97) R. impingement syndrome 726.2 [thiscode is Other affections of shoulder region, notelsewhere classified]8) Black outs 780.2
Additional Claimed Diagnosis orConditionThe compensable injury was a substantialfactor in bringing about the additionalclaimed diagnoses/conditions below[checked yes or no]:1) Lt rotator cuff tear 840.4 - NO2) Lt shoulder impingement 726.2 - YES[this code is Other affections of shoulderregion, not elsewhere classified]3) Lt shoulder strain 840.9 - YES4) Seizures 345 [epilepsy] - NO
Reached statutory MMI on 4/17/14. Hasnot met clinical MMI
See full report for alldetails
He documents thathe does not feelcervical andshoulder ROMmeasurements arevalid.
Feels he has a WPIof 19% based onScenario C whichexcludes leftshoulder cuff tearand seizures.
Dr. S DDE 0002,00004, 00023-00026
Page 49 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #**
EXAMINATIONGeneral: Anxious Caucasian man inmoderate emotional distress. Speech attimes tangential, redirectingcommunication to ongoing chronic paincomplaints.
Cervical spine: Marked apparent AROMdeficit in all planes when formallymeasured. Able to move neck betterwhen scanning room and walking.Paracervical muscles tense but not in truespasm. Could not position neck toperform Spurling's.
Both Shoulders: Tense and guarded.Marked AROM loss demonstrated (seeworksheet) No scapular winging.impingement signs positive bilaterally.
Neurological exam: Subjectively globallyreduced sensation in entire left armcompared to right - does not followdermatomal pattem. Muscle strength 3+/5with diffuse and marked make-breakweakness. No toneabnormalities. Arm and forearmcircumferences within 1/2 cm (seeworksheet). DTR's 1+ and symmetric atbilateral biceps. brachioradialis, triceps.Hoffman's negative bilaterally.
Diagnosis1. Status post traumatic brain injury withpost-concussion features: the 4/7/2015SPECT scan provides additional evidenceof probable TBI sequela;2. Post-traumatic headaches3. Memory and other cognitive/emotionaldysfunction felt to be concussion/TBIrelated4. Status post cervical strain5. Adjudicated diagnoses of post-traumaticcervical disc herniations6. Status post right shoulder strain with rightrotator cuff tear and impingement,7. Status post left shoulder strain withimpingement.8. History of "blackouts" without objectiveevidence of true seizure disorder.
Questions/Purpose of Examination:
** **
Page 50 of 52

Medical Chronology James Shelton
Date & Time Fact Text Description/Comm... Source/Bates #** Disputed injuries include left shoulder
rotator cuff tear, left shoulderimpingement syndrome, left shouldersprain/strain and seizures.
I am further hampered in that medicalrecords begin on 7/18/2012. This is a fullthree months post injury.Therefore, I have no objective data at allas to how the examinee was doing in theinitial three monthsfollowing the work accident.
He gives 3 scenarios for impairmentratings:
Scenario A: All of the previously listedaccepted injuries to the head, cervical spineand right shoulder. WPI - 15%
Scenario B: Includes all accepteddiagnoses plus all of the left shoulder andseizure diagnoses. WPI - 23%
Scenario C: Incudes all accepteddiagnoses plus left shoulder strain plusimpingement; excludes left shoulderrotator cuff tear and seizures. WPI - 19%
It is my opinion that Scenario C isaccurate here.
Impairment Rating- 4th Edition AMAGuides to the Evaluation of PermanentImpairment
He narrates a disclosure:I am satisfied that the physical AROMmeasurements that I obtained bothtoday and on 4/22/2015 are invalid anddo not reflect the examinee's truecapabilities. Much better shoulder AROMmeasurements were present on initialmeasurements in 2012 again as measuredby Dr's V and B in 2014 andagain by Dr. B in 2015.
There is no physical explanation as towhy cervical and shouldermeasurements should change vastly upand down from month to month. This isnot explained by medical treatment efforts.In my opinion chronic pain and subsequent
** **
Page 51 of 52
Medical Chronology James S
Date & Time Fact Text Description/Comm... Source/Bates #** behavioral manifestation accounts for the
wide range of AROM findings over theyears.While by rule I am directed to usemeasurements obtained at or nearest to theMMI date, I am sure that I am notcompelled to use what I consider to beinvalid measurements. Therefore, for thepurposes of this report, themeasurements closest to statutory MMIdate that appear most valid are those Ichose to use. This would be the rightshoulder measurements by Dr. V on9/23/2014 and the left shoulder AROM ofDr. B on 12/22/2014. I concedethat it is possible that none of themeasurements obtained by anyone arevalid.
** **
Page 52 of 52