Embed Size (px)
Citation preview

Medical Error Prevention in the Medical Error Prevention in the Emergency DepartmentEmergency Department Solutions for the Future Solutions for the Future
Graham Billingham, MD
The Second
Mediterranean Emergency Medicine Congress
Sitges/Barcelona, Spain
September 15, 2003
““I will do no harm”I will do no harm”Hippocratic OathHippocratic Oath
Medical error is the fifth leading cause of death in the United States. More people die from medical errors than from car accidents, breast cancer or AIDS.
The Institute of Medicine 1999
“Medication errors are one of the most common causes of avoidable harm to patients”
Joint Commission Report 1995
““To Err is Human”To Err is Human”
We have met the enemy and it is us Institute of Medicine Report 1999 The Public will not tolerate medical errorLeapfrog Group – payers will not tolerateJoint Commission – governmental mandateInstitute for Safe Medication PracticesOther industries have embraced information
technology, why haven’t we?
The TruthThe Truth 180,000 unnecessary US deaths per year 1.3 million injuries per year $ 8 billion increase in national health costs Cost- adds $4700 per hospital admission 1.4 medication errors for every hospital admission The largest cause of adverse events in hospitals is
Adverse Drug Events (ADEs) which occur at the alarming rate of 65 per 1000 hospital admissions
60% may be preventable
Source: NCVHS Data

Adverse Drug EventsAdverse Drug EventsWho’s at fault?Who’s at fault?
Physician responsible – 56%Nurse responsible – 34%Secretary – 6%Pharmacy – 4%
Source: The Advisory Board
Common Physician IssuesCommon Physician Issues
Illegible signature – 78%Orders not timed – 58%Incomplete orders – 24%Illegible orders – 20%Other: too busy, distracted, verbal orders,
no checks and balances, rely on memory,
not aware of drug allergy or interaction

Common Nurse IssuesCommon Nurse Issues
Calculating dose– 80% incorrectly calculate 10% of the time– 40% make mistakes > 30% of the time
Administering the wrong medicineGiving medicine to the wrong patientFrequency errorsMissing doses
Medication ErrorsMedication ErrorsEffect on US MalpracticeEffect on US Malpractice
3% of total malpractice claimsAverage malpractice award = $636,000
Cost of ClaimsCost of Claims
Short term morbidity - anaphylaxis, respiratory failure, GI bleed
Long term morbidity - renal failure, anoxia, death
Difficult to defend because of “expert witness” (PDR/FDA indications)
Medical Errors- Root CausesMedical Errors- Root Causes
• Allergic reactions • Excessive dose• Incorrect drug given• Error in writing or reading Rx• Drug interaction • Failure to monitor drug levels or toxic
effects
Medical Errors – Medical Errors – Where do they occur?Where do they occur?
28% in ordering11% in transcribing10% in preparing51% in administering
JAMA 1996; 274-35-43
Why Do Errors Occur?Why Do Errors Occur?
• Time pressure/high patient volume• Failure to recognize high risk areas• Medication delivery system is complex• Multiple caregivers involved• Extensive medication knowledge base
Poor communication (verbal/written)• Lack of checks and balances system
Pitfalls In Medication Delivery Systems:Pitfalls In Medication Delivery Systems:
• Request for medication administration
• Nurse identifies correct medication & dosage
• Patient identified• Allergy ruled out• Medication
administered correctly
• Legible correct prescription
• Pre-printed instructions
• Pharmacist-patient communication
• Compliance

High Risk AreasHigh Risk Areas
Joint Commission (JCAHO)Joint Commission (JCAHO)
• Began tracking 1995• Medical Error Prevention Issue 1-1998• High Alert Medications Issue 11-1999• Sound-alike Drug Names Issue 19 -2001• Dangerous Abbreviations Issue 23- 2001

Root Causes of Medication Errors Root Causes of Medication Errors 1995-20021995-2002
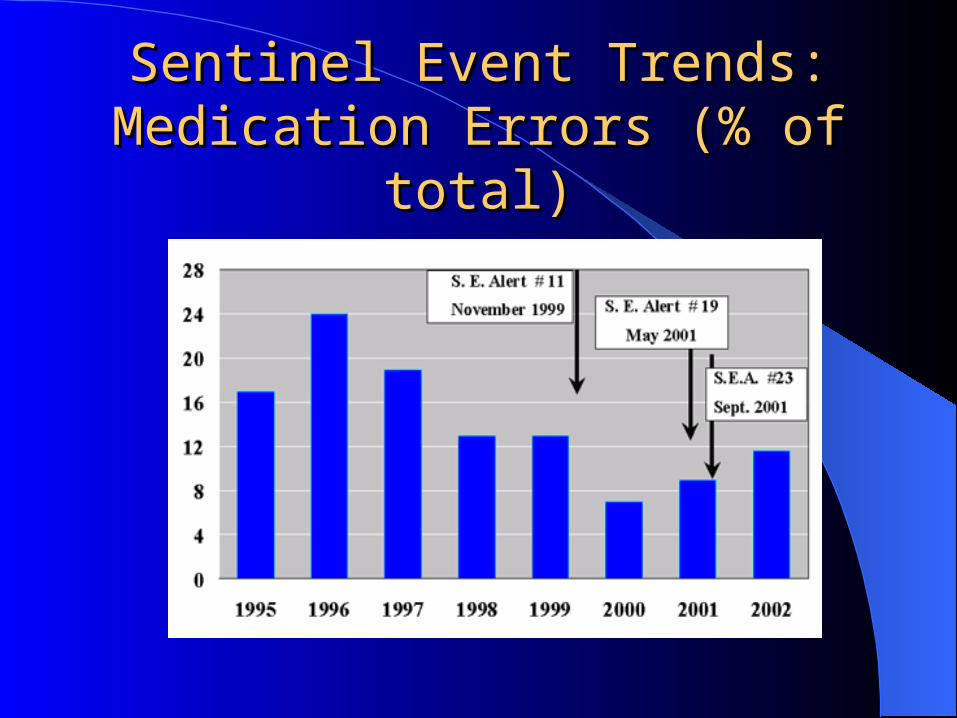
Sentinel Event Trends: Sentinel Event Trends: Medication Errors (% of total)Medication Errors (% of total)
Medication Errors : High Risk Areas Medication Errors : High Risk Areas
High alert medications
High risk patientsHigh risk diseasesInfusion pumps
Verbal ordersAbbreviationsLook-alike drugsNo standardizationLack of automation

Medication Errors : High Risk Areas Medication Errors : High Risk Areas (JCAHO) High Alert Medications(JCAHO) High Alert Medications
Potassium ChlorideOpiates and narcoticsInsulin and oral hypoglycemic agentsAnticoagulants (Heparin)Antihypertensive agentsPsychiatric medicationAnticonvulsantsCardiac drugs
High Alert MedicationHigh Alert MedicationKCL ExampleKCL Example
Potasium Chloride• 10 incidents of death
– 8 from direct infusion– 6 cases KCL mistaken for another drug
- Heparin- Lasix- Saline flush
• Recommendation: must be stored and prepared in the pharmacy
High Risk Patients and DiseasesHigh Risk Patients and Diseases
PregnantElderlyHIVTransplant patientsAnticoagulantsAllergiesPediatric patientsPsych PatientsPatients on 2 or
more drugs
CHFHTNDiabetes Renal failureLiver failurePsych disorders

Medication Errors : High Risk AreasMedication Errors : High Risk AreasHigh Risk PatientsHigh Risk Patients
Pregnant Elderly HIV Transplant Patients Anticoagulants Allergies Psych Patients Patients on 2 or more
drugs
DigoxinCoumadinAspirinElavilHCTZEnalaprilZantacIndocinXanaxZithromax

Medication Errors : High Risk AreasMedication Errors : High Risk AreasHigh Risk PatientsHigh Risk Patients
Multiple Medications
2 medications = 13% chance of an ADI
7 medications = 87% chance of an ADI
DigoxinCoumadinAspirinElavilHCTZEnalaprilZantacIndocinXanaxZithromax
47% of patients discharged from the ED have a new medication added

Medication Errors : High Risk Areas Medication Errors : High Risk Areas PediatricsPediatrics
Medication Errors in a Pediatric Emergency Department. Medication Errors in a Pediatric Emergency Department. Selbst SM et al. Pediatr Emerg Care 1999Selbst SM et al. Pediatr Emerg Care 1999..
Incorrect Dose = 35% of errors Incorrect Medication given = 30% of errors Incorrect recording of weight Failure to note drug allergy
High Risk Areas: Infusion PumpsHigh Risk Areas: Infusion Pumps
Major Source of Medication Errors• High risk medications• Inadvertent free-flow• Incorrect pump programming• Calculation / concentration errors• Wrong medication

Case Study Case Study
30 y/o F history of post strep AGN s/p renal transplant. Presents with URI symptoms.
Meds : cyclosporin, Prednisone
Dx : bronchitis
A. Cipro
B. Zithromax
C. Erythromycin
D. Biaxin
Medication Errors: Medication Errors: Solutions for the EDSolutions for the ED
Recommendations/Summary

Give medication only if Give medication only if indicated – do no harmindicated – do no harm
Physician verifies PMHx, meds and allergies
Be aware of FDA/PDR recommendationsGive least toxic drug“Low and slow” ruleBe aware of high risk patientsBe aware of high risk medications
Medication RulesMedication Rules
Consider contraindications Consider drug interactions Consider adverse drug event Use bolus rather than infusion when available Monitor drug levels when appropriate Avoid prescribing medicine outside of the
scope of emergency medicine
Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Infusion Pumps• Pumps with free-flow
protection• Standardize
– Medication use– # Of critical care drugs /
concentrations ( premix)
• Check system• Document dose calculation
on chart• Limit number of pump
types
“SMART” Infusion Pumps• Drug infusion protocol
library• Pre-defined dose limits• Automatic shut-off• Alarm system• Integrated Patient
Monitoring– Vital signs– Allergies– Age / Renal Function
The Future: Taking the Human The Future: Taking the Human Out of the ErrOut of the Err
• Reduce the reliance on memory• Pre-printed drug dosing protocols• PDA/bed side aides/wall charts• Automated drug dispensing• Standardize formulary• Automated drug calculator• Computerized Physician Order Entry• Clinical decision support• “Intelligent” EDIS
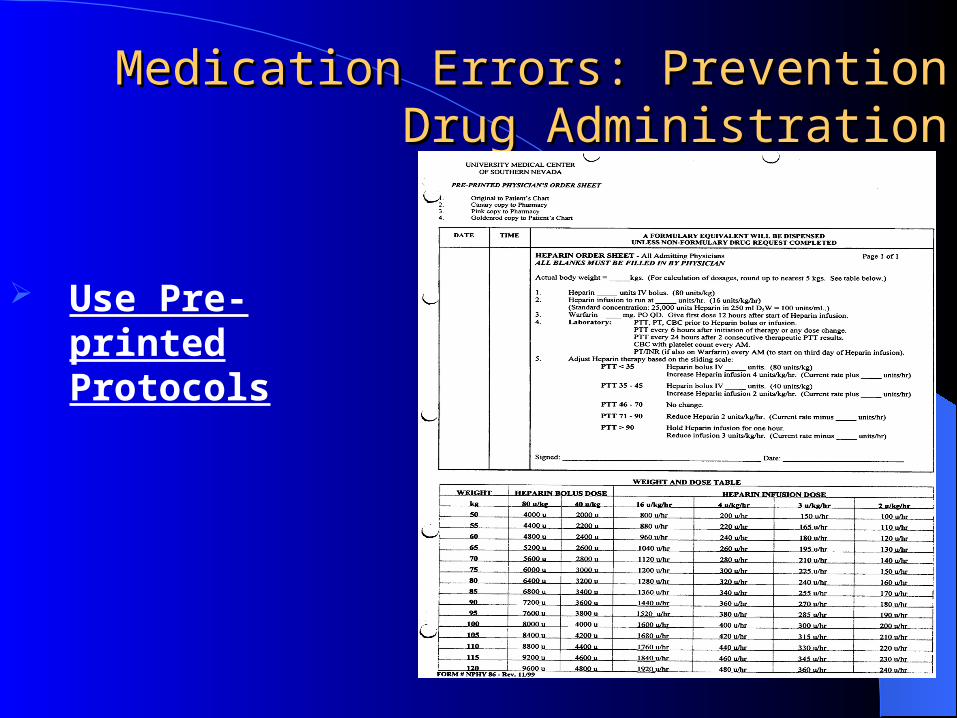
Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Use Pre- printed Protocols

Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Use Wall Charts
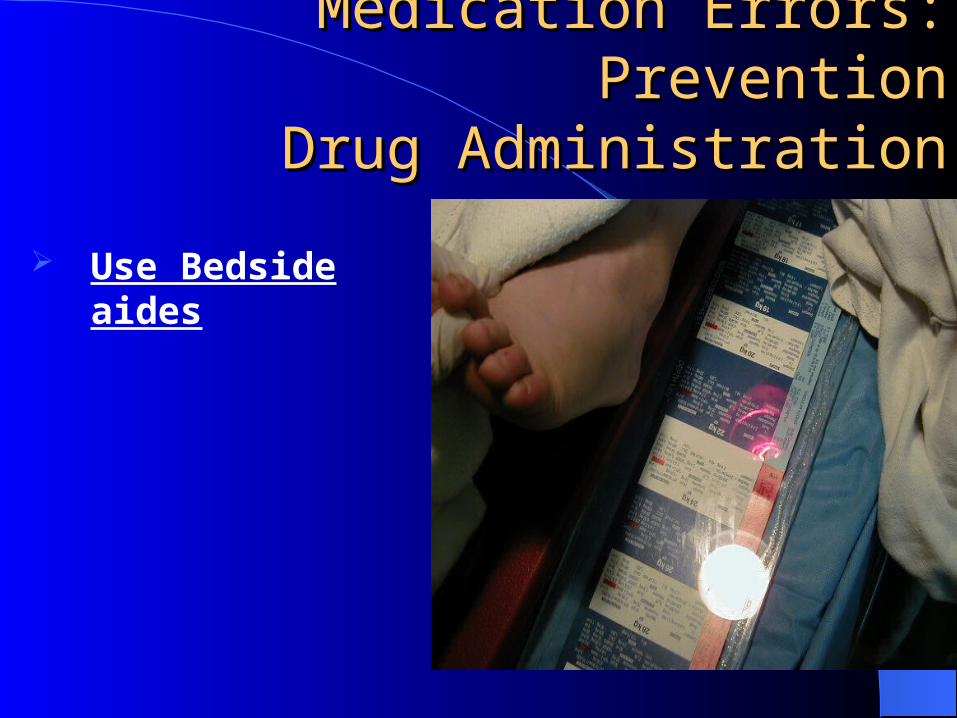
Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Use Bedside aides

Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Personal Digital Assistant

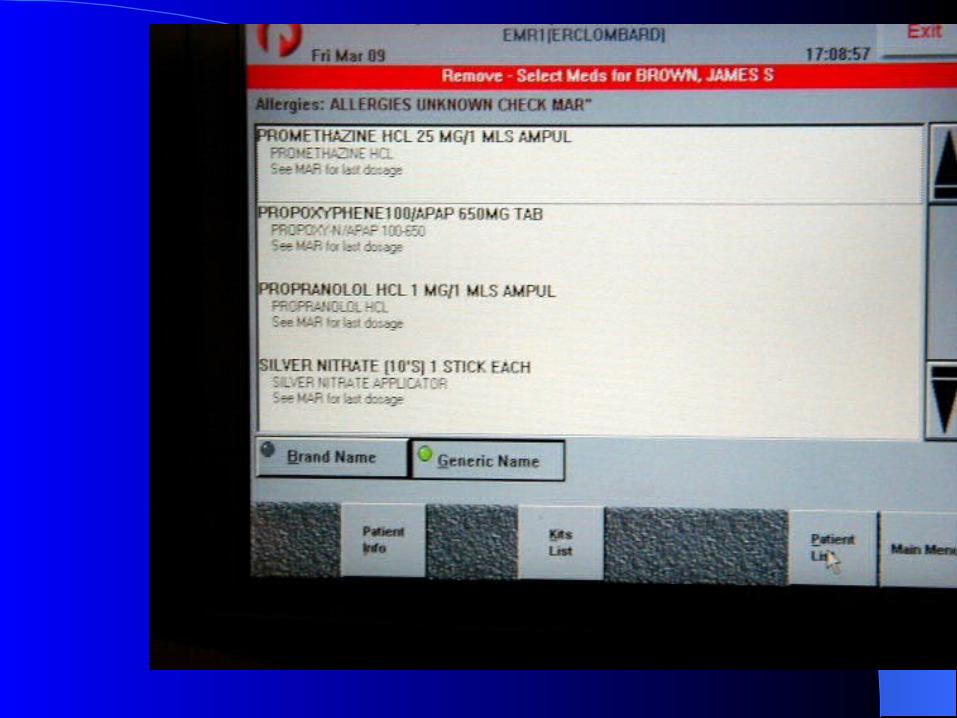
Medication Errors: PreventionMedication Errors: PreventionDrug AdministrationDrug Administration
Automated Drug dosing and Distribution
Medication Errors: PreventionMedication Errors: PreventionImprove CommunicationImprove Communication
• Standardize Prescriptions“unit” vs. “u” 20U NPH for 200 NPH“every” vs. “q”“use leading zero, not a trailing zero”
– 0.4 not .40– 4 not 4.0– 2 ½ not 2.5

Medication Errors: PreventionMedication Errors: PreventionImprove CommunicationImprove Communication
Patient– Dosage– Simplify regimen– 4 X day vs every 6 hours– Indication, side effect, duration– Pre-printed instructions– Include family
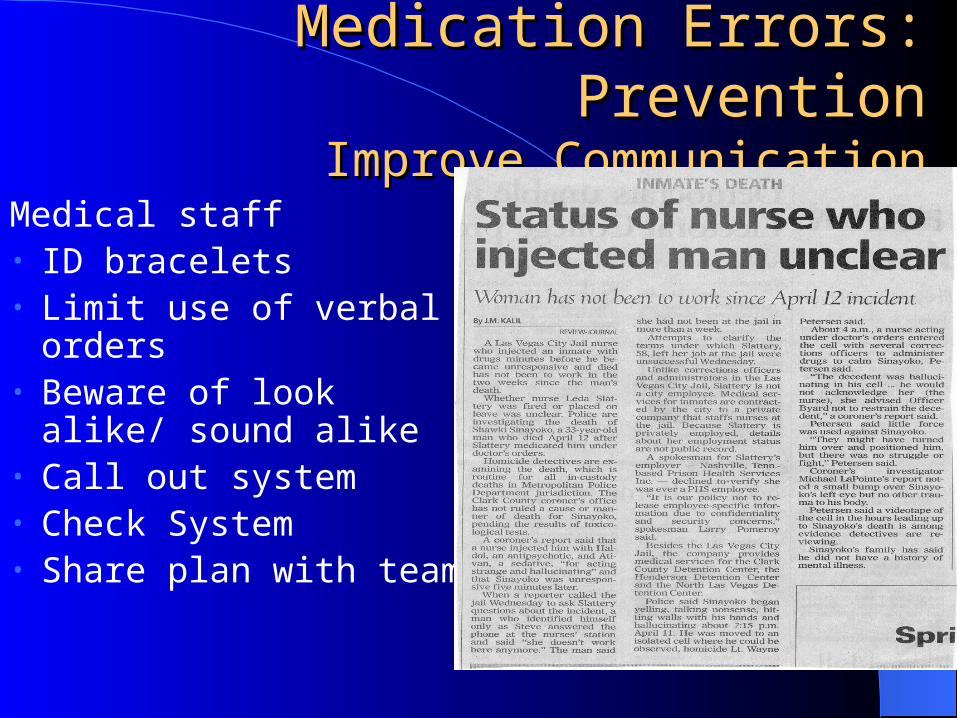
Medication Errors: PreventionMedication Errors: PreventionImprove CommunicationImprove Communication
Medical staff• ID bracelets• Limit use of verbal orders• Beware of look alike/
sound alike• Call out system • Check System• Share plan with team

Medication Errors: PreventionMedication Errors: PreventionImprove CommunicationImprove Communication
Caution with sound a likes / look a likesMgSO4 vs. MSO4Diprivan vs. DitropanNarcan vs. NorcuronNifedipine vs. Nicardipine vs. NimodipineBrevital vs. Brevibloc

Medication Errors: PreventionMedication Errors: PreventionInclude PharmacistInclude Pharmacist
Pharmacy Responsibilities Legible prescriptions• Controls all patient’s
medication• Checks for drug
interactions• Special Packaging• Provide information
sheet/Patient education

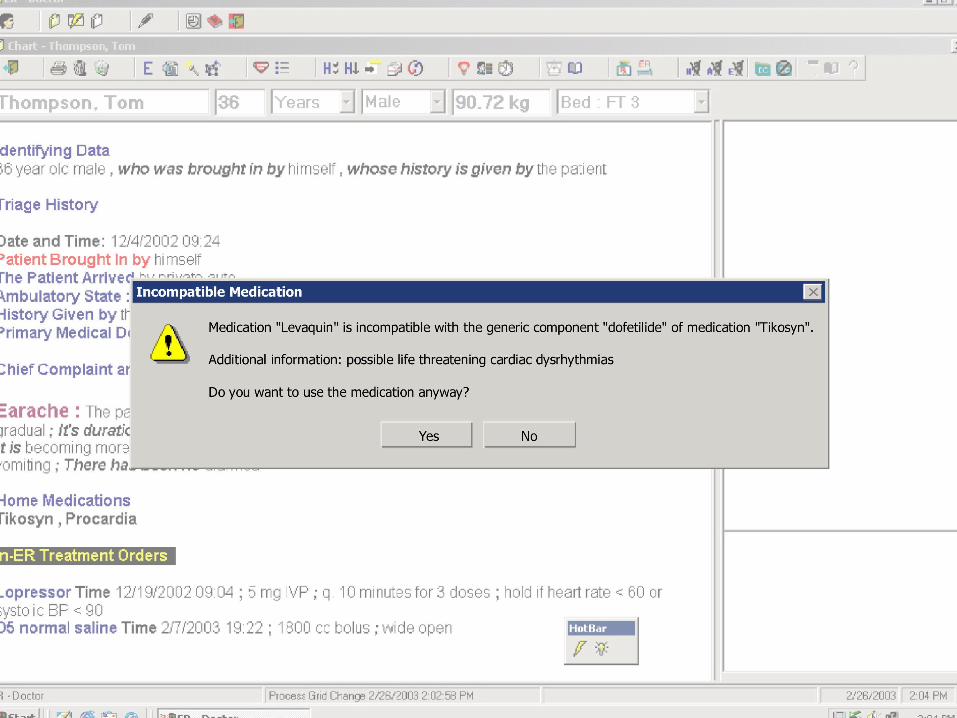
Medication Errors: PreventionMedication Errors: PreventionComputerized Physician Order Entry Computerized Physician Order Entry
(CPOE)(CPOE)
Benefits• Legible• Decreases number of hand-offs• No verbal orders• Guidelines displayed• Alternatives offered• Appropriate doses and frequencies• Built in alerts, allergies and interactions

Medication Errors: PreventionMedication Errors: PreventionComputerized Physician Order Entry Computerized Physician Order Entry
(CPOE)(CPOE)
Challenges• Changing behavior• Equipment availability• Equipment / software failure• Requires training• Orders entered on wrong patient • Cost

Computerized Physician Order Entry (CPOE) Computerized Physician Order Entry (CPOE)
Effect of CPOE on Prevention of Serious Medication Errors. Effect of CPOE on Prevention of Serious Medication Errors. Bates DW, JAMA 1998; 280: 1311-16Bates DW, JAMA 1998; 280: 1311-16
• Serious Medication Errors 55% • Decrease hospital LOS by one day• Decrease hospital charges by 13%• Adverse Drug Events
– Actual 17%– Potential 84%
The Role of Emergency The Role of Emergency Department Information Systems Department Information Systems
(EDIS)(EDIS)Passive tracking of patientsMedical error prevention tools built inImproves documentation and legibilityAutomates workflow – reduces hand-offsCQI tools for outcomes researchProvides clinical decision supportAutomates prescription writing
The FutureThe FutureBar code/RFID trackingDesign EDs around “Do no harm” principleStandardization of medications and processesAutomation of workflow and systemsCPOE becomes the new standard of careIntelligent EDIS with clinical decision supportPharmacy robotics and intelligent drugs

Final ThoughtFinal Thought
One thing is clear, our societies will not tolerate this rate of medical error, and neither should we. As it turns out, embracing information technology will be the easy part, changing human behavior will be the challenge of the future.

Web ResourcesWeb Resources
www.ismp.orgwww.nccmerp.orgwww.iom.eduwww.jcaho.orgwww.mederrors.comwww.advisoryboardcompany.com
Implementation of an EDISImplementation of an EDISA Case StudyA Case Study
Clifton A Sheets, MD, FAAEMMary Washington HospitalFredericksburg, VA USA

IntroductionIntroduction
Why an EDIS? Search Process Selection Process Implementation Impact Considerations

DisclosureDisclosure
A consultant for Patient Care Technology Systems Amelior ED®
Why an EDIS?Why an EDIS?
Process began in 1995– 300 bed Community hospital
Increasing ED patient volume– 60,000 annual visits in 1995– 87,000 annual visits (projected) in 2003
Increasing ED length of stayDecreasing patient satisfaction with ED
process strongly tied to LOS
Why an EDIS?Why an EDIS?
Paper/grease board/transcription – manual system – ineffective, and inefficient
Need for patient trackingNeed for automation of data collection and
processing
Driving forcesDriving forces
Community pressure to reduce time in ED US Compliance Issues JCAHO, EMTALA,
HIPAA Fundamental belief that CQI should be more
proactive Patient Safety
– Handwriting issues– IOM report 1999– Medication errors
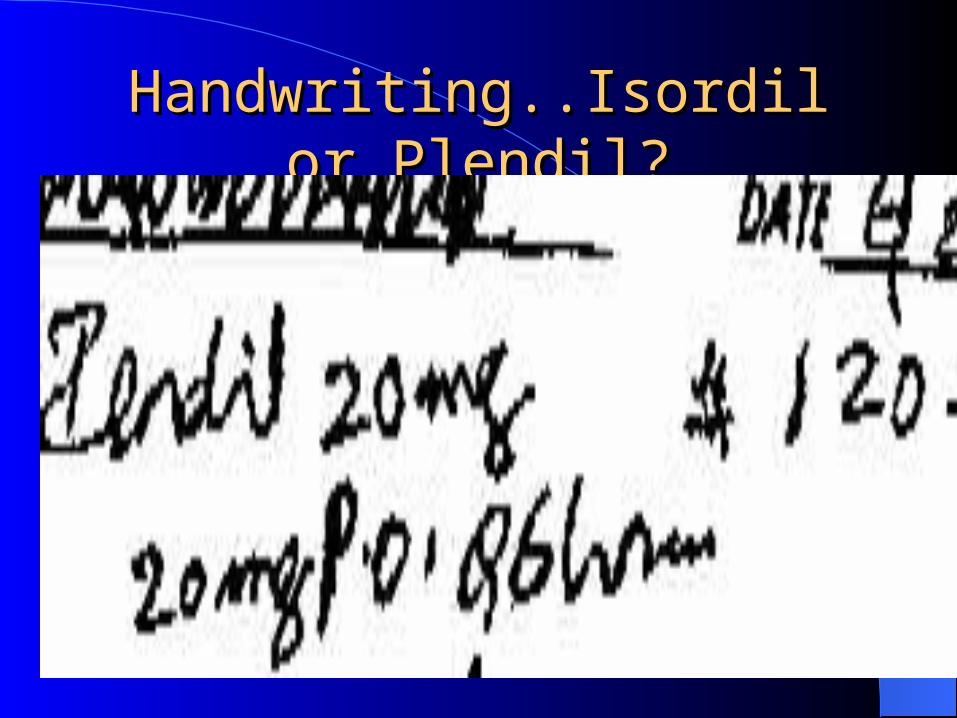
Handwriting..Isordil or Plendil?Handwriting..Isordil or Plendil?
Driving forcesDriving forces
ED expansion planned for 2002– From 30 beds to 55
beds– From 13,000 sq ft to
27,000 sq ft
Search ProcessSearch Process
Needs identified– Streamlined patient care – Complete/compliant
documentation– Reduced transcription
costs– Enhanced patient safety
and error reduction– Optimized
reimbursement
Solutions identified– Patient tracking– CPOE– Nurse and physician
charting– Prescription writing– Discharge instructions

Search ProcessSearch Process
Collaborative effort– Physician champions identified (3)– Nursing and hospital administration– Administrative assistant– Ancillary services– Information Services– Medical records
Search ProcessSearch Process
Sources of information– EDIS trade shows and conferences– Electronic bulletin boards– Word of mouth– ED Physician group prior exposure
Selection ProcessSelection Process
Vendor’s RFP– Main players– Beware of “vaporware”
Best Few– Complete systems– Track record of success– Desired features
Site visit to “kick the tires”

Selection Process Selection Process
Selected “best 2” vendors with complete solutions (late 2000)
Site visits revealed problems such as incomplete system feature implementation and stability issues
Fear of failure
– Upfront cost– Physician use– Speed issues– Return on investment

Selection ProcessSelection Process
Amelior ED® system identified as new vendor– Allergy and drug-drug interaction safety
features– Weight based dosing– Clinical decision support (protocols)– CPOE ease of use– Customization capability
Selection ProcessSelection Process
Amelior ED®
– All-inclusive pricing based on patient volume
Key challenges– Beta site, no installations to visit– Unknown company with unknown resources– Hospital IS chief afraid of being stuck with a
legacy system, and no support
AAmelior melior EDED®®
Clinical features– Patient tracking– Nurse charting– Physician charting– CPOE– Prescription writing– Discharge instructions– Reports engine– Forms engine– Onsite user training
Technology– Microsoft®-centric– Bedside workstations– Additional nursing and
physician workstations– ADT, Lab, X-ray interfaces– 365 x 24 x 7 technical
support– Quarterly software
upgrades– Hardware refreshes

ImplementationImplementation
“big bang” vs phased approach Initial big bang in Nov 2001
– Lack of complete lab and x-ray interface capability– Speed and process issues resulted in a mutual
agreement to take the system down
Proof-of-concept in Fast track– Completed interface work– System turned on for rest of ED

Current StatusCurrent Status
Continuous operation since July 200190,000+ visits100% use by physicians and nursesBi-directional Interfaces:
– Lab orders and results– X-ray orders and interpretations– ADT information transfer– Lifetime clinical record
ImpactImpact
Decreased LOS by almost 1 hr in 1st 6 months– Volume has increased 14% this year
Eliminated handwriting issues– No more pharmacy call backs– Reduction in medication errors– Reduction in “missed” orders
Automated time stamp improved process analysis, accountability, and order execution times
ImpactImpact
Greatly enhanced ability to determine prior visit actions, results and treatments
Reduced “door to decision” timeStreamlined orders process
– Unit clerks eliminated from process– Improved protocol compliance

ImpactImpact
Nearly paperless ED– No “paper chase” for lab or X-ray results– No fighting over who gets the chart– No lost or misplaced charts
Improved transfer documentation – Instant chart for the transfer now available– Prompting for transfer (COBRA)
documentation

ImpactImpact
Financial– Reduced walk-outs by 57% (> $1 million annually)– 90% reduction in lines of transcription ($300k annual
savings)– Improved physician documentation
Increased RVUs– Length of laceration– Critical care time well documented
– Reduction in calls for medical records– Automated ICD-9, CPT and APC codes– Charge capture
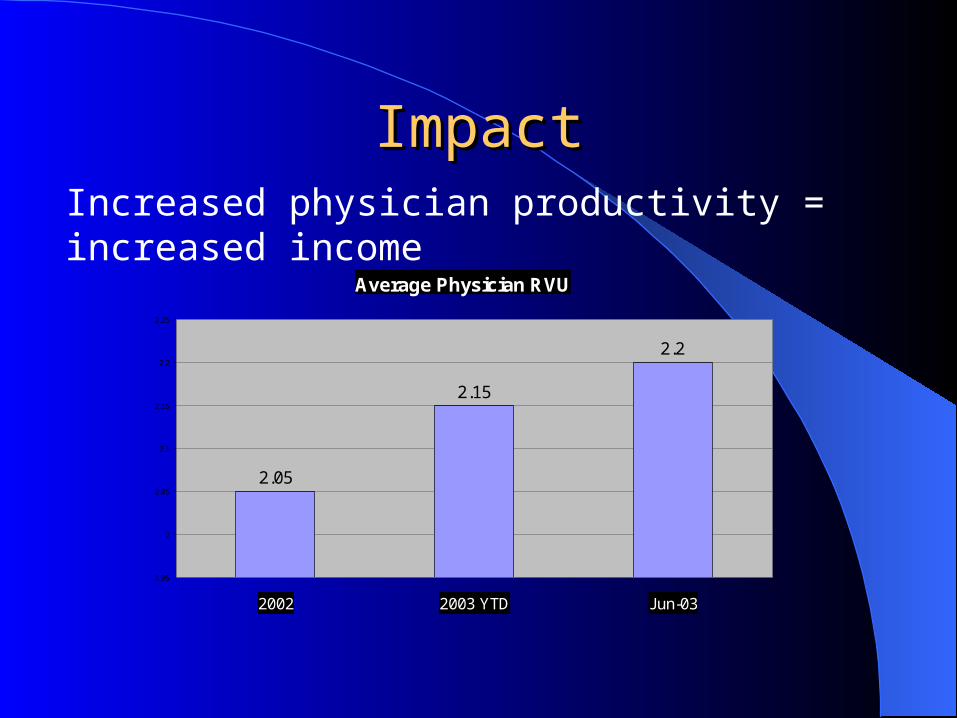
ImpactImpactIncreased physician productivity = increased income
Average Physician RVU
2.05
2.15
2.2
1.95
2
2.05
2.1
2.15
2.2
2.25
2002 2003 YTD Jun-03
Impact Impact
Concerns– New technology introduces complexities
New users Data entry Safety feature bypass
ImpactImpact
Concerns– Different looking chart
Medical staff outcry over change– Small but vocal minority– Education on benefits– Modifications in font size appeased most– Paper chart made available for consultants
– Additional layers of regulation Passwords HIPAA rules specific to EMRs

SummarySummary
A full feature EDIS can– Reduce errors and improve patient safety– Eliminate handwriting issues– Improve workflow by reducing turn around
times for lab, x-ray and nursing orders– Improve data analysis and collection– Enhance hospital and physician revenues– Reduce length of stay
SummarySummary
Plan for an evolution and not a revolution Needs assessment drives the process Collaborative process Physician champions key to success Vendor environment is competitive and evolving Biggest may not be the best solution for your ED
Future of EDISFuture of EDIS
Bioterrorism monitoring and alertsProactive CQIEnhanced automationEmbedded digital imagingArtificial intelligenceMobile connectivity

““We have met future and We have met future and it is us”it is us”

Resources
Dr. Clifton Sheets [email protected]
Mary Washington Hospital www.medicorp.org
Patient Care Technology Systems www.pcts.com
EDIS Symposium www.paacep.org
AAEM www.aaem.org
ACEP Emergency Medical Informatics Subsection www.acep.org