Embed Size (px)
Citation preview

32
Medical Evidence
From Academic Year 2014/15 SFE must be satisfied that a student has a disability which meets the Definition of a Disability as outlined in the Equality Act 2010. For students prior to 2014/15 SFE just needed to be satisfied that a student had a disability. Any ongoing 13/14 new applications will use the previous rules for reviewing Medical Evidence. Definition of a Disability – Equality Act 2010
As person has a disability for the purpose of the Act if he or she has a physical or mental impairment and the impairment has a substantial and long term adverse effect on his or her ability to carry out normal day to day activities. Equality Act Guidance 2010 – Forms and Guides Folder How to apply the Definition
In order to apply the definition it must be broken down and each of the following sections considered. Meaning of Impairment
The definition requires that the effects which a person may experience must arise from a physical or mental impairment. In many cases, there will be no dispute whether a person has an impairment. Any disagreement is more likely to be about whether the effects of the impairment are sufficient to fall within the definition and in particular whether they are long-term. Even so, it may sometimes be necessary to decide whether a person has an impairment so as to be able to deal with the issues about its effects. It is not possible to provide an exhaustive list of conditions that qualify as impairments for the purposes of the Act. Any attempt to do so would inevitably become out of date as medical knowledge advanced. A disability can arise from a wide range of impairments which can be: Sensory, such as those affecting sight or hearing Impairments with fluctuating or recurring effects such as rheumatoid arthritis, myalgic encephalitis (ME), chronic fatigue syndrome (CFS), fibromyalgia, depression and epilepsy Progressive, such as motor neurone disease, muscular dystrophy, and forms of dementia Auto-immune conditions such as systemic lupus erythematosis (SLE) Organ specific, including respiratory conditions, such as asthma, and cardiovascular diseases, including thrombosis, stroke and heart disease Developmental, such as autistic spectrum disorders (ASD) Learning disabilities, such as dyslexia Mental health conditions with symptoms such as anxiety, low mood, panic attacks, phobias, or unshared perceptions; eating disorders; bipolar affective disorders; obsessive compulsive disorders; personality disorders; post traumatic stress disorder, and some self-harming behaviour Mental illnesses, such as depression and schizophrenia; Produced by injury to the body, including to the brain. It is important to remember that not all impairments are readily identifiable. While some impairments, particularly visible ones, are easy to identify, there are many which are not so immediately obvious, for example some mental health conditions and learning disabilities. Long Term
The Act states that, for the purpose of deciding whether a person is disabled, a long-term effect of impairment is one: Which has lasted at least 12 months; or
Extracts from DSA Matrix v0.1 - pages 32 to 47

33
Where the total period for which it lasts, from the time of the first onset, is likely to be at least 12 months; or Which is likely to last for the rest of the life of the person affected This information must be clear in the Medical Evidence and as SFE staff are not medically trained we should not make assumptions. If it is not clear within the evidence then further evidence should be requested. However from experience we are aware that some conditions are lifelong and even though it may not be explicit in the evidence, it is a known fact that their condition would meet the long term definition. For example a student who provided a GP letter which confirmed they were an amputee. It is clear that they are always going to be an amputee so we can be satisfied that the long term definition is met. Some element of common sense must be applied here but if you are unsure please refer the case to your Team Manager. A person who has a Deemed Disability as listed below does not need to meet the definition of long term and can be accepted for DSAs. Special provisions apply when determining whether the effects of an impairment that has fluctuating or recurring effects are long-term. If an impairment has had a substantial adverse effect on a person’s ability to carry out normal day-to-day activities but that effect ceases, the substantial effect is treated as continuing if it is likely to recur. (In deciding whether a person has had a disability in the past, the question is whether a substantial adverse effect has in fact recurred.) Conditions with effects which recur only sporadically or for short periods can still qualify as impairments for the purposes of the Act, in respect of the meaning of ‘long-term’. For example, a person with rheumatoid arthritis may experience substantial adverse effects for a few weeks after the first occurrence and then have a period of remission. We would be unable to make any assumptions here and the Medical Evidence should confirm this. It is not necessary for the effect to be the same throughout the period which is being considered in relation to determining whether the ‘long-term’ element of the definition is met. A person may still satisfy the long-term element of the definition even if the effect is not the same throughout the period. It may change: for example activities which are initially very difficult may become possible to a much greater extent. The effect might even disappear temporarily. Or other effects on the ability to carry out normal day-to-day activities may develop and the initial effect may disappear altogether. Substantial Effect
A substantial effect is one that is more than a minor or trivial effect. The time taken by a person with an impairment to carry out a normal day-to-day activity should be considered when assessing whether the effect of that impairment is substantial. It should be compared with the time it might take a person who did not have the impairment to complete an activity. A person who has a Deemed Disability as listed below does not need to meet the definition of substantial and can be accepted for DSAs. An impairment might not have a substantial adverse effect on a person’s ability to undertake a particular day-to-day activity in isolation. However, it is important to consider whether its effects on more than one activity, when taken together, could result in an overall substantial adverse effect. For example, a person whose impairment causes breathing difficulties may, as a result, experience minor effects on the ability to carry out a number of activities such as getting washed and dressed, going for a walk or travelling on public transport. But taken together, the cumulative result would amount to a substantial adverse effect on his or her ability to carry out these normal day-to-day activities. Environmental conditions may exacerbate or lessen the effect of an impairment. Factors such as temperature, humidity, lighting, the time of day or night, how tired the person is, or how much stress he or she is under, may have an impact on the effects. When assessing whether adverse effects of an impairment are substantial, the

34
extent to which such environmental factors, individually or cumulatively, are likely to have an impact on the effects should, therefore, also be considered. The fact that an impairment may have a less substantial effect in certain environments does not necessarily prevent it having an overall substantial adverse effect on day-to-day activities. Where an impairment is subject to treatment or correction, the impairment is to be treated as having a substantial adverse effect if, but for the treatment or correction, the impairment is likely to have that effect. For example, if a person with a hearing impairment wears a hearing aid. The question as to whether his or her impairment has a substantial adverse effect is to be decided by reference to what the hearing level would be without the hearing aid. Similarly, in the case of someone with diabetes which is being controlled by medication or diet should be decided by reference to what the effects of the condition would be if he or she were not taking that medication or following the required diet. A person who develops pneumonia may be admitted to hospital for treatment including a course of antibiotics. This cures the impairment and no substantial effects remain. Normal Day to Day Activities
The Act does not define what is to be regarded as a ‘normal day-to-day activity’. It is not possible to provide an exhaustive list of day-to-day activities. Normal day-to-day activities can include general work-related activities, and study and education-related activities, such as interacting with colleagues, following instructions, using a computer, driving, carrying out interviews, preparing written documents, and keeping to a timetable or a shift pattern. The examples of what it would, and what it would not, be reasonable to regard as substantial adverse effects on normal day-to-day activities are indicators and not tests. They do not mean that if a person can do an activity listed then he or she does not experience any substantial adverse effects: the person may be affected in relation to other activities, and this instead may indicate a substantial effect. An illustrative and non-exhaustive list of factors which, if they are experienced by a person, it would be reasonable to regard as having a substantial adverse effect on normal day-to-day activities. Whether a person satisfies the definition of a disabled person for the purposes of the Act will depend upon the full circumstances of the case. That is, whether the substantial adverse effect of the impairment on normal day-to-day activities is long term. In the following examples, the effect described should be thought of as if it were the only effect of the impairment.
Difficulty in getting dressed, for example, because of physical restrictions, a lack of understanding of the concept, or low motivation Difficulty carrying out activities associated with toileting, or caused by frequent minor incontinence Difficulty preparing a meal, for example, because of restricted ability to do things like open cans or packages, or because of an inability to understand and follow a simple recipe Difficulty eating; for example, because of an inability to co-ordinate the use of a knife and fork, a need for assistance, or the effect of an eating disorder Difficulty going out of doors unaccompanied, for example, because the person has a phobia, a physical restriction, or a learning disability Difficulty waiting or queuing, for example, because of a lack of understanding of the concept, or because of pain or fatigue when standing for prolonged periods Difficulty using transport; for example, because of physical restrictions, pain or fatigue, a frequent need for a lavatory or as a result of a mental impairment or learning disability Difficulty in going up or down steps, stairs or gradients; for example, because movements are painful, fatiguing or restricted in some way A total inability to walk, or an ability to walk only a short distance without difficulty; for example because of physical restrictions, pain or fatigue Difficulty entering or staying in environments that the person perceives as strange or frightening

35
Behaviour which challenges people around the person, making it difficult for the person to be accepted in public places Persistent difficulty crossing a road safely, for example, because of physical restrictions or a failure to understand and manage the risk Persistent general low motivation or loss of interest in everyday activities Difficulty accessing and moving around buildings; for example because of inability to open doors, grip handrails on steps or gradients, or an inability to follow directions Difficulty operating a computer, for example, because of physical restrictions in using a keyboard, a visual impairment or a learning disability Difficulty picking up and carrying objects of moderate weight, such as a bag of shopping or a small piece of luggage, with one hand Inability to converse, or give instructions orally, in the person’s native spoken language Difficulty understanding or following simple verbal instruction Difficulty hearing and understanding another person speaking clearly over the voice telephone (where the telephone is not affected by bad reception) Persistent and significant difficulty in reading or understanding written material where this is in the person’s native written language, for example because of a mental impairment, or learning disability, or a visual impairment (except where that is corrected by glasses or contact lenses) Intermittent loss of consciousness Frequent confused behaviour, intrusive thoughts, feelings of being controlled, or delusions Persistently wanting to avoid people or significant difficulty taking part in normal social interaction or forming social relationships, for example because of a mental health condition or disorder Persistent difficulty in recognising, or remembering the names of, familiar people such as family or friends Persistent distractibility or difficulty concentrating Compulsive activities or behaviour, or difficulty in adapting after a reasonable period to minor changes in a routine
Progressive Conditions
Progressive conditions are conditions that have effects which increase in severity over time. A person with a progressive condition is to be regarded as having an impairment which has a substantial adverse effect on his or her ability to carry out normal day-to-day activities before it actually has that effect. The person will still need to show that the impairment meets the requirements of ‘long term’. Deemed Disabilities
The Act provides for a person with one of the below listed progressive conditions to be a disabled person from the point at which they have that condition, so effectively from diagnosis. In these cases we are satisfied they meet the definition of long term and there are substantial effects. Only evidence to show the person has that condition is required. MS HIV Cancer Registered with local Authority or certified as blind Severely sight impaired Sight impaired or partially sighted DSA Applications received for any of the above would be accepted for DSAs without the need to show long term substantial effects on day to day activities. Excluded Disabilities
Certain conditions are not to be regarded as impairments for the purposes of the Act. These are: Addiction to, or dependency on, alcohol, nicotine, or any other substance (other than in consequence of the substance being medically prescribed) Seasonal allergic rhinitis (e.g. hayfever), except where it aggravates the effect of another condition Tendency to set fires Tendency to steal Tendency to physical or sexual abuse of other persons; Exhibitionism

36
Voyeurism DSA applications received for any of the above would need to be rejected. When to Apply the Definition
The above should be applied to all students who applying for DSA in 14/15 onwards unless they fit into one of the following Mental Health Condition – using the Mental Health Proforma is sufficient Specific Learning Difficulty – using a diagnostic report is sufficient Deemed Disability – just need evidence of the condition Excluded Condition – application should be rejected Where a student presents evidence which does not meet the definition of long term and does not provide information to confirm the effect on day to day activities is substantial you would need to request further evidence. In previous years you may have felt you understood some conditions and what the effects are, however going forward this must be confirmed by the Medical Professional. For example Autism is condition which as a fact we know to be long term so this aspect of the definition would be met, however as autism is on a scale the effects on day to day activities will very much vary and we will need the Medical Professional to confirm in the evidence that they effects are substantial.

37
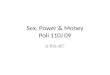
General Guide to the Definition
Does the student
have an
impairment?
Is it a Deemed
Disability?
Is it an Excluded
Condition?
Are the adverse
effects long term?
Does the impairment
adversely affect the ability to carry
out day to day
activities?
Is the adverse effect substantial, or would
it be but for the beneficial effects of ongoing medication or other treatment?
Physical or Mental Impairment Not defined in the Act Does not have to equate with a clinical condition
The following conditions are accepted without the need to prove the stages of the definition: Multiple Sclerosis, HIV, Cancer, Registered with Local Authority or certified as Blind, Severely sight impaired or Sight Impaired or partially sighted.
Tendencey to set fires, steal physical or sexual abuse of other persons Exhibitionism or voyeurism Hay fever (except where it might aggrevate another condition) Addition to alcohol, nicotine or any other substance, unless it originally results from the administarion of medically prescribed drugs or other medical treatment.
Has lasted at least 12 months Likely to last at least 12 months Is likely to last for the rest of the student’s life?
Day to day activities are things carried out by most people on a daily basis Not possible to provide an exhaustive list
Adverse effect must not be minor or trivial Cumulative effect of a number of minor impairments can qualify as substantial

38
What evidence do we require?
Physical Conditions Medical Conditions
A written statement / letter from a doctor or appropriate qualified medical professional.
Mental Health Conditions
A written statement / letter from a doctor or appropriate qualified medical professional. Or Mental Health Evidence Proforma
SpLD
A post-16 diagnostic report, written in accordance with the 2005 SPLD Working Group Guidelines, from either: A registered psychologist OR A suitably qualified specialist teacher, holding a SpLD Assessment Practicing Certificate.
Cost of Medical Evidence
It is the student’s responsibility to pay any cost in relation to obtaining medical evidence
GP / Medical Professional Letter
The most common type of Medical Evidence (outside of SpLDs) is a GP Letter. The reason we state GP/Medical Professional is because, generally, the letter should be written by a person qualified to make the diagnosis. However there are exceptions to this which are detailed below in the Healthcare Professionals section
Mental Health Evidence Proforma
The Mental Health Proforma was introduced on 30th January 2013 as was designed in conjunction with UMHAN (Universities Mental Health Advisory Network) as a tool for students to provide Medical Evidence. The Mental Health Proforma is available on the Practitioners Website for stakeholders to download. A copy is also available in the Forms and Guides - Medical Evidence Guides folder. Where a student has provided no Medical Evidence or unacceptable Medical Evidence of a Mental Health condition the student should be sent a copy of this proforma along with the DSA Mental Health Letter Template. Special Educational Needs SEN
We can accept a Statement of Special Educational Needs (SEN) issued by a Local Authority as evidence for Autistic Spectrum Disorders, AD(H)D, dyspraxia and lifelong medical conditions. However going forward for 14/15 students, the content would still need to meet the definition as outlined above. Considerations for Processing Medical Evidence
As the team receives a variety of medical evidence, there may be some cases where you cannot easily reach a conclusion. In these instances please refer the evidence to the Eligibility Team Leader. If still no decision can be reached, the Team Leader will seek guidance from senior management. This is to ensure that any decisions that set a precedent for future cases are recorded and fully comply with our internal SFE / DSA requirements. If the student has multiple conditions and we have satisfactory evidence for one of the conditions but not the others, then we are able to progress the application to the Study Needs Assessment stage and authorise the student to be assessed on the condition with the satisfactory evidence and request further information for the further conditions.

39
Healthcare Professionals - Letters
We are ok to accept medical evidence from certain professionals that are treating a student for a previously diagnosed condition. Evidence should state the condition for which they are being treated and be on signed, letter headed paper. From 14/15 onwards it should also meet the definition as outlined above. We must always check the credentials of the author to ensure the professional has the relevant qualifications for which they are practicing. Physiotherapists/Occupational Therapists and Speech and Language therapists often deal with the ongoing treatment for many conditions. Website to check credentials http://www.hpc-uk.org/ Care Coordinators are often Nurses that specialise in a specific area e.g. Mental Health. Website to check is www.nmc-uk.org We must treat each application on a case by case basis and be satisfied that the evidence received is relevant and acceptable. GMC Website, list of Registered Medical Practitioners: http://www.gmc-uk.org/doctors/register/LRMP.asp
Nurse Practitioner
We can accept evidence from a Nurse Practitioner. The key issue is about what the evidence is saying and whether there is enough information in the body of the evidence for us to be comfortable with agreeing eligibility for DSAs. Some points of interest are: Nurse practitioners will generally have more experience that nurses. They will often, but not exclusively, be from a charge or a sister grade and so will tend to have more experience in their specialty. Nurse practitioners will be well placed to speak about the potential ongoing impact of a condition on an applicant’s life and may have a good idea of the amount of time a condition is likely to last. It would normally be for a GMC registered medical professional to make a diagnosis, however with the emergence of ever more disciplines of nurse practitioners and prescribing nurses / pharmacists, the clearly established lines between the medical disciplines is blurring. Specific Learning Difficulties (SpLD)
"Specific Learning Difficulty" is an umbrella term which can cover the following (not an exhaustive list): Dyslexia Dyspraxia Dyscalculia Dysgraphia ADD or ADHD Aspergers Syndrome Where diagnosis is given as ’Specific Learning Difficulty’ it can be accepted and we would not require the author to be any more specific. Evidence of SpLDs would usually be in the format of a diagnostic report as detailed in the table above but we also can accept a GP Letter for some of these e.g. Dyspraxia, AD(H)D and Aspergers. As with any disability, no two individuals experience the same combination of difficulties and some students may exhibit signs of more than one SpLD. However, these learning difficulties typically affect students’

40
information processing, memory and motor skills and are often productive of high levels of anxiety. Form filling is a challenging for people with SpLD as organisational skills are often compromised. Clarity in information and instructions is required. Dyslexia: includes difficulties in areas such as word identification and processing, can affect spelling and grammar, speed of processing spoken instructions, short term memory difficulties and organisational skills. Dyslexia is characterised by specific problems in learning to read and write due to subtle problems in visual perception. Problems with arithmetic and reading musical notation are also common, as are poor working memory, difficulties with the sounds of words, and a poor sense of direction. Dyslexia affects around 5 per cent of the population in a severe form, though many more when milder forms are also included. Dyspraxia: includes difficulties in areas such as co-ordination difficulties, attention and concentration deficits, difficulty explaining/re-telling of events and/or complex situations and problems in flexible thinking. Dyspraxia is less well known, but its prevalence is similar to that of dyslexia. It is characterised by clumsiness and difficulties in carrying out complex, sequenced actions. Poor coordination results in difficulties with acts such as catching a ball, tying up shoelaces or doing up buttons, but more seriously results in extremely poor handwriting and difficulties with organisation, attention and concentration. Diagnosis of dyspraxia can be provided via a diagnostic report, doctor/consultant letter or a Statement of Educational Needs. Dyscalculia: is characterized by difficulties with mathematical skills and concepts; can also be seen in difficulties with abstract concepts of time and direction, following sequential instructions, sequencing events affects ability to acquire arithmetical/mathematical skills; “Dyslexia for numbers”, performing calculations, orientation and navigation around forms, relationship between numbers e.g. 10’s, 100’s, 1000’s Dysgraphia: is characterized by profound difficulties in hand-writing. Can be painful and slow writing down information, coordinating handwriting Attention Deficit Disorder (ADD) exists with or without hyperactivity. In most cases people with this disorder are often ‘off task’, have particular difficulty commencing and switching tasks, together with a very short attention span and high levels of distractibility. Specific learning differences
We may come across cases where a diagnostic (SpLD) report uses the phrase Specific Learning Difference in its diagnosis/conclusion (rather than Specific Learning Difficulty) After seeking opinion from PATOSS we received following reply; ‘Differences is a word that some authors use as they do not like to use the word difficulties as it could be deemed as non-PC and may apply a barrier against the student.’ Due to the above and provided the conclusion is clear, we can accept reports using this terminology. The conditions are one and the same with the two words having the same meaning.
Table of Acceptable Diagnostic Assessments
Diagnostic assessments carried out between September 2005 to August 2006
Accept diagnostic assessments carried out by psychologists and suitably qualified specialist teachers. Specialist teachers who assess dyslexia should hold AMBDA (Associate Membership of the British Dyslexia Association) or a qualification from an advanced training course which assesses adults for dyslexia and is recognised by the British Dyslexia Association’s Accreditation Board (see Annex 2).
Diagnostic assessments carried out between September 2006 and August 2007
Accept diagnostic assessments carried out by psychologists and suitably qualified specialist teachers as above.
Diagnostic reports to be in the format recommended in the SpLDs Working Group’s report.
Diagnostic reports to use tests recommended in the SpLDs Working

41
The Layout of a Diagnostic Assessment
Students with a Specific Learning Difficulty will need to provide evidence of this in the form of a Diagnostic Assessment / Psychological Report from a psychologist or suitably qualified specialist (in accordance with the Specific Learning Difficulties Working Group 2005 Guidelines). These reports should include: Assessor details Summary Background information Test conditions Attainments – literacy Underlying ability Cognitive processing Test scores Conclusion Summary Appendices When checking the Diagnostic Assessment, a DSA Assessor must give consideration of the following points:
Was the report carried out when the student was 16 years of age or above?
Is it also the appropriate format considering different year’s regulation?
Was the report carried out by a qualified professional?
Does it include the assessor’s name (and if carried out after 2007 the assessors practicing certificate number?)
Have the correct tests been used to assess the student?
Is it clear from the summary / conclusion that the assessment confirms a SpLD?
Group’s guidelines or added by the SpLD Test Evaluation Committee (STEC). See paragraph 18
Diagnostic assessments carried out between September 2007 and August 2008
Accept diagnostic reports from psychologists and specialist teachers. Specialist teachers must hold a current practising certificate in assessing specific learning difficulties issued by their relevant professional association (for example, the Professional Association of Teachers of Students with Specific Learning Difficulties (PATOSS) or Dyslexia Action). Psychologists must hold a current practising certificate issued by their relevant professional association (for example, the British Psychological Society).
Diagnostic reports to be in the report format recommended in the SpLDs Working Group’s guidelines
Diagnostic reports to use tests recommended in the SpLDs Working Group’s guidelines or added by the SpLD Test Evaluation Committee (STEC). See paragraph 183.
Diagnostic assessments carried out from September 2008
Procedures as from September 2007 above plus the following.
All training for assessing specific learning difficulties to incorporate the SpLDs Working Group’s guidelines.

42
The Necessary Tests to be included within a Diagnostic Assessment (from Sept 2006)
Certain tests must have been carried out in order for the author to ascertain a confirmed SpLD. The tests that we at SFE need to ensure are carried out are listed below. Please note that we do not need to concern ourselves with the results of these tests, we do however need to ensure that they were carried out and documented in the report including the results and scores from the appropriate acceptable tests The titles of acceptable tests are kept and listed in the accompanying handout. Attainments in Literacy
Reading Single words (a standardised single word reading test); non-word reading; text reading (both oral and silent) and reading comprehension; qualitative analysis of errors; evidence of strategies such as whole word recognition; decoding; fluency; reading speed (oral and silent) and ability to extract information from text; summary of student’s reading profile. Suitable tests: WRAT 3; WRAT 4; WRMT-R; TOWRE; WIAT- II; WIAT-ii UK-T; SDRT; ART; GORT-4, ARC. Spelling A standardised single word spelling test; free writing; dictation of sentences (optional) Qualitative analysis of errors. Suitable tests: WTAT 3; WTAT 4; HAST; BSTS; WIAT-II UK; WIAT-II UK-T. Writing Free writing analysed to cover vocabulary, ability to write grammatically, complexity of sentence structures, coherence of writing, writing speed and legibility of handwriting. Handwriting speed for copying should be reported separately. Suitable tests: Free Writing; DASH 17+. Underlying Ability
Information about both verbal and non-verbal ability; observations about test performance; discussion of profile of scores highlighting any significant discrepancies. Suitable tests: WRIT; WAIS-IIIUK; WAIS-IV UK; WASI (or WASI I) On 15/07/2014 SASC were contacted in relation to WASI II and queried when their guidance would be updated to list WASI II as an acceptable test. As a result of this they have updated their website today with an interim update which is detailed below in red.
Wechsler Abbreviated Scale of Intelligence® - Second Edition(WASI®-II) The WASI II is acceptable for DSA assessments in all areas the WASI I was listed. The WASI II is an updated version of the assessment battery. The WASI I is still acceptable as long as the forms are available. As a result of this update WASI II can be recognised as an acceptable test. Please note that WASI I and WASI II are only
acceptable for underlying ability.
Cognitive Processing
A range of tests selected by the assessor to probe relevant aspects of cognitive functioning: tests of working memory (if these have not been reported in the section Underlying Ability); tests of phonological processing (phonological awareness and phonological processing speed). Tests should be reported under separate headings. Suitable tests: WMS-III; WMS-IV UK; WRAML2; WAIS-III UK; TOMAL2; The Digit Memory Test; AWMA; CTOPP; SDMT; Speed of Writing Prose Task; DASH 17+, Suitable tests for Specific Learning Difficulties
(WRAT, WAIS, WIAT, CTOPP, Dash, Berry, etc) As we will still receive reports undertaken at various times, the most recent guidelines/checklist may not have been in effect at the time the student had their report done. As such, previous guidelines and checklists may need to be referred to. Please make sure you refer to the right checklist and guidelines relevant to the date of the Diagnostic Assessment Report you are reviewing.

43
Click here to open the 2005 WORKING PARTY GUIDELINES FOR SpLDs Click here to open the REVISED GUIDELINES FOR ACCEPTABLE TESTS (September 2013) Please note the above – under Underlying Ability – that WASI II has been added as an acceptable test in an interim update on the SASC website. Click here to open a GUIDE FOR DYSPRAXIA Click here to open the SpLD Working Group Tests Checklist September 2013 Click here to open the Medical Evidence Guides folder in the G-Drive, to access previous SpLD updates and Checklists (e.g., November 2012 updates) Pre 16 Diagnostic Reports
Under normal circumstances, a pre-16 diagnostic assessment is not acceptable for the purposes of DSA Eligibility. However under certain circumstances and if supplied with appropriate additional documentation we may still be able to accept these reports. If the diagnosis was carried out before the age of 16, the student should normally be asked to undergo an ‘Assessment of Performance Attainment’ which would provide an update on their current performance in reading, writing and spelling. Intelligence is unlikely to change significantly even if the student was diagnosed as a child and therefore there is no requirement for another assessment of intelligence. However, reading, writing and spelling could change in adulthood. The ‘Assessment of Performance Attainment’ is a ‘top up’ diagnosis which provides up to date evidence of the student’s current degree of difficulty in reading, writing and spelling. The top up diagnosis is to establish the likely impact of the student’s specific learning difficulties on the skills needed for higher education. The top up diagnosis should be based on tests recommended in the Specific Learning Difficulties Working Group’s guidelines or added by the SpLD Test Evaluation Committee (STEC). See paragraph 184. The Assessment of Performance Attainment is part of the diagnosis and the cost should be met by the student, although an application may be made to the institution’s discretionary Access to Learning Fund to meet the cost. The Assessment of Performance Attainment could be carried out by specialist teachers who hold a current practicing certificate in assessing specific learning difficulties issued by their relevant professional association (for example, the Professional Association of Teachers of Students with Specific Learning Difficulties (PATOSS) or Dyslexia Action), or by psychologists who hold a current practicing certificate issued by their relevant professional association (for example, the British Psychological Society) NOTE: For 14/15 academic year, the Access to Learning Fund (mentioned above) no longer exists. Students should not be advised to apply to this for money towards medical evidence. Letter templates etc have been updated but please ensure any personal templates or created e-mails do not refer to this fund. Visual Stress / Irlens Syndrome
Diagnosis of Visual Stress / Irlen Syndrome can be provided via a diagnostic report, including a specific learning difficulties (SpLD) report, a Visual Stress / Irlen assessment or Visual Stress / Irlen screening After providing diagnostic evidence, students with Visual Stress / Irlen only would be referred for Colorimetry Testing. This would be funded through the DSAs. If diagnosis has already been provided as part of the diagnostic report, then students will not need to be fully tested again and can be referred for Colorimetry testing which would be funded through the DSAs Please note if the report confirms that the student has Irlens or Scotopic / Colour Sensitivity / Visual Stress this should be added as an extra condition in the DSA1 Letter as the Needs Assessor will take this into consideration during the SNA. If it is not confirmed the EVIDNAC letter should be used.

44
Click here to open the GUIDE FOR IRLENS within this Matrix. There is also the FAQs document available on the Practitioners website. With regards to the recording of the above within the Application Tracker, it has been decided that where there is an SpLD plus one or more of the above, they should be recorded as Multiple Disabilities. E.g., Diagnostic assessment report confirms Dyslexia and Irlens Syndrome, these should both be recorded on the Application Tracker and not just classed as Dyslexia.
Other Conditions
From 14/15 evidence must conform to the definition of a disability as detailed above; meaning evidence must confirm that the impairment has a substantial and long term adverse effect on his or her ability to carry out normal day to day activities. AD(H)D (Attention Deficit (Hyperactivity) Disorder) The latest version of the Medical Evidence Guide For AD(H)D which can also be located here: G:\SFD_PILOT\Processing\Team Specific Information\Specialist Support\Disabled Students Allowance\DSA FORMS AND GUIDES\Medical Evidence Guides\Guide - AD(HD) v3.doc Previous guidance stated that AD(H)D required a medical diagnosis by a doctor, usually a child or adolescent psychiatrist, a pediatrician or pediatric neurologist or a GP, also a SEN can be accepted. As of 04/02/2013 a diagnosis of AD(H)D in a diagnostic report can be accepted. Asperger Syndrome / Autism / ASD
Because Aspergers Syndrome varies widely from person to person, making a diagnosis can be difficult. It is often diagnosed later in children than autism and sometimes difficulties may not be recognised and diagnosed until adulthood. The typical route for getting a diagnosis is to visit a GP. He or she can refer an individual to other health professionals who can make a formal diagnosis. Most frequently they will be psychiatrists or clinical psychologists and, in the case of children, paediatricians. Some people see a formal diagnosis as an unhelpful label; however, for many a diagnosis: helps the individual, families, friends, partners, carers, professionals and colleagues to better understand and manage their needs and behaviour and a diagnosis is also required to get DSA. A diagnosis is also the key needed to open the door to specialised support, e.g. supported living or finding suitable employment. There are diagnostic differences between conditions on the autism spectrum. Sometimes people may receive a diagnosis of autism or autistic spectrum disorder (ASD), high-functioning autism (HFA) or atypical autism instead of Asperger syndrome. Alternatively, they may be given a diagnosis of pervasive developmental disorder - not otherwise specified (PDD-NOS) or semantic pragmatic disorder. However, people who have been given these diagnoses will have similar difficulties and similar support needs to those who have Asperger syndrome. What is autism? Click here to open the GOOD PRACTICE INFORMATION SHEET on this condition Autism is a lifelong developmental disability. It is part of the autism spectrum and is sometimes referred to as an autism spectrum disorder, or an ASD. The word 'spectrum' is used because, while all people with autism share three main areas of difficulty, their condition will affect them in very different ways. Some are able to live relatively 'everyday' lives; others will require a lifetime of specialist support. The three main areas of difficulty which all people with autism share are sometimes known as the 'triad of impairments'. They are: difficulty with social communication

45
difficulty with social interaction difficulty with social imagination. Some professionals may refer to autism by a different name, such as autism or autistic spectrum disorder (ASD), classic autism or Kanner autism, pervasive developmental disorder (PDD) or high-functioning autism (HFA). Important We have received clarity that students that have an autistic spectrum disorder can be funded for social mentoring through the DSAs. There had previously been a misunderstanding that this was a provision which HEI’s needed to fund. Required Evidence: Doctor/Consultant letter, Psychiatrists, Psychologists, Paediatricians, Statement of Educational Needs, Diagnostic Report.. Asthma
In the past Asthma alone may not ordinarily be considered as an eligible condition for DSA unless it confirmed the Asthma was sever/chronic/brittle. However, going forward for 14/15, you would need to be satisfied that the impairment has a substantial and long term adverse effect on his or her ability to carry out normal day to day activities. Required Evidence: Doctor/Consultant letter. Crohn’s Disease
The main gastrointestinal symptoms are abdominal pain, diarrhea (which may be bloody) or constipation, vomiting and weight loss. Crohn's disease can also cause complications outside of the gastrointestinal tract such as skin rashes, arthritis, and inflammation of the eye. Although this can be controlled, there is no known medical or surgical cure for Crohn's. Required Evidence: Doctor/Consultant letter. Epilepsy
Epilepsy can be difficult to diagnose because there are many other conditions that can cause seizures, such as migraines or panic attacks. Patients are often referred to a Neurologist for diagnosis. When reviewing evidence against the definition of a disability you will need to take into account the re-occurrence as explained above to determine if the impairment is long term (as well as determining the substantial effect on day to day activities). Although seizures may only last a short amount of time, they may reoccur over the qualifying 12 month period. Where someone was diagnosed with epilepsy and only had one seizure/group of seizures but this did not span the period of 12 months it may not be accepted. Required Evidence: Doctor/Consultant letter. Lupus
Lupus can affect many parts of the body, including the joints, skin, kidneys, heart, lungs, blood vessels, and brain. Although people with the disease may have many different symptoms, some of the most common ones include extreme fatigue, painful or swollen joints (arthritis), unexplained fever, skin rashes, and kidney problems. Required Evidence: Doctor/Consultant letter. ME/CFS (Chronic Fatigue Syndrome)
Myalgic encephalomyelitis (ME) is characterised by a range of neurological symptoms and signs, muscle pain with intense physical or mental exhaustion, relapses, and specific cognitive disabilities. Required Evidence: Doctor/Consultant letter.

46
Mental Health
Examples of clinically recognised mental disorders include mental illnesses such as schizophrenia, bipolar disorder, anxiety or depression, as well as personality disorders, eating disorders, OCD and anxiety. The re-occurance of the condition can be an important factor when reviewing Mental Health conditions in order to determine long term. Required Evidence: Psychiatrist, Doctor/Consultant letter, Mental Health Proforma. Muscular Dystrophy
Muscular dystrophy is a genetic (inherited) condition where slow, progressive, muscle wasting leads to increasing weakness and disability. The symptoms of muscular dystrophy and their severity will vary depending on the particular type of the condition that a person has, and how old they were when the symptoms first appeared. However, generally, muscular dystrophy causes the following symptoms: difficulty walking, clumsiness, frequent falls, difficulty standing, and breathing problems. Required Evidence: Doctor/Consultant letter. Rheumatoid Arthritis
Rheumatoid arthritis is an inflammatory disease that causes pain, swelling, stiffness, and loss of function in the joints. It has several special features that make it different from other kinds of arthritis. Rheumatoid arthritis affects people differently. For some people, it lasts only a few months or a year or two and goes away without causing any noticeable damage. Other people have mild or moderate forms of the disease, with periods of worsening symptoms, called flares, and periods in which they feel better, called remissions. Still others have a severe form of the disease that is active most of the time, lasts for many years or a lifetime, and leads to serious joint damage and disability. The substantial and long term adverse effect on his or her ability to carry out normal day to day activities would need to be considered. Required Evidence: Doctor/Consultant letter. Sickle Cell Hemoglobin Disease
Sickle-cell disease, or sickle-cell anaemia (or drepanocytosis), is a life-long blood disorder characterized by red blood cells that assume an abnormal, rigid, sickle shape. Sickling decreases the cells' flexibility and results in a risk of various complications. The sickling occurs because of a mutation in the hemoglobin gene. Life expectancy is shortened, with studies reporting an average life expectancy of 42 and 48 years for males and females, respectively. Crises can last from a few hours to 10-14 days. Patients may be incapacitated and immobile due to pain and may require help with personal care until the crisis is resolved. Between attacks patients have to keep warm and maintain high fluid intake. Crisis’s can be brought on by cold temperature, dehydration, infections, mental and physical stress. Required Evidence: Doctor/Consultant letter. Obesity
We have had rare cases of applications citing obesity. If we believe that the obesity gives rise to impairments that would place the student within the definition of a disability, they could well be eligible for DSAs. As always, we need to look into the body of the evidence to ensure we are informed enough to be able to make a decision on eligibility. If we do not have enough information, we are obliged to seek more evidence. It is reasonable for us to refer to the Equality Act as guide to help our decision making. Some key points the person must have an impairment that is either physical or mental the impairment must have adverse effects which are substantial the substantial adverse effects must be long-term the long-term substantial adverse effects must be effects on normal day-to-day activities Required Evidence: Doctor/Consultant letter.

47
Foreign Medical Evidence
We often receive medical evidence that is written in a foreign language. All cases should be reviewed individually but there is no hard and fast rule if this should be declined or rejected. Please speak to your team leader for a decision if you are unsure. If it is decided you will accept the evidence we would expect it to have a certified translation document. Example 1. Deaf / Partial Hearing - we have in the past accepted a foreign doctors letter for this condition as being deaf would apply in any language. This evidence had a certified translation document. Example 2. Specific Learning Difficulty / Language Impairment – we have in the past declined this as it was based on the students 2nd language and we could not be certain if the difficulties were due to the disability or because English was not their first language. Also we would not be able to accept a foreign diagnostic report because we could not be certain that the appropriate tests had been performed as the report would not be written within the SpLD guidelines. We have got round this previously with an American report, by asking that a British registered psychologist confirms the tests are appropriate and that they concur with the diagnosis.