Embed Size (px)
Citation preview
Medical Genetics BranchMedical Genetics BranchMedical Genetics BranchMedical Genetics Branch
A Safety Concern?
Human Teratogenicity of Lovastatin:
Robin J. Edison, MD, MPHMaximilian Muenke, MD
Medical Genetics BranchDivision of Intramural Research
National Human Genome Research InstituteNational Institutes of Health
Method: Review of Case ReportsTeratologic Assessment
All available MedWatch case report forms, and literature reports
Hypothesis-generating strategy: assessment includes search for patterns of malformation, comparison with animal data, and plausibility of biological association
No existing epidemiologic data have sufficient exposures or follow-up to generate reliable risk estimates

HMG-CoA
Mevalonate
Isoprenoids
Protein PrenylationGrowth Factor ActivityCell Signaling, MigrationMitochondrial CoEnz Q10
Cholesterol Cell Membranes Steroid Synthesis
HMG-CoA Reductase
Statin Mechanism of Action
STATINS
Morphogenetic Signaling (CNS, skeleton, viscera)

1st Trimester Exposures (N=214)
Evaluable = 71
Structural Anomaly
= 22
Atorvastatin: 4Lovastatin: 7Simvastatin: 10 Cerivastatin: 1
“Normal”=40
Intra-UterineFetal Demise
= 5
Lovastatin: 2Simvastatin: 3
Simvastatin: 4
Adverse Outcomes = 31
IUGR
= 4

Lovastatin Malformation Reports (N = 7)3 of 7 reports include midline CNS defects
1. Incomplete separation of lateral cerebral ventricles (Holoprosencephaly); aortic hypoplasia, ASD, death dose: 40 mg/d, gestational weeks 0 - 7 birth prevalence: 1/16,000
Holoprosencephaly was also reported as 1 of 1 cerivastatin malformation (dose 0.25 mg/d, weeks 0-8)
2. Aqueductal stenosis with hydrocephalus dose: 40 mg/d, gestational weeks 0 – 4.5 birth prevalence: 1/10,000
3. Extensive neural tube defect, absent palate dose: 20 mg/d, gestational weeks 0 - 18 birth prevalence: < < 1/10,000

Lovastatin Malformation Reports (N = 7)non-CNS malformations
1 report of VACTERL association (vertebral, anal,
cardiac, tracheo-esophageal, renal, limb defects) dose: 10 mg/d, gestational weeks 6-11 birth prevalence: 1/500,000 (5 VACTERL features) VACTERL was also reported as 1 of 10 simvastatin
malformation cases dose: 10 mg/d simvastatin, gestational weeks 0 - 13 birth prevalence: 1/50,000 (4 VACTERL features)
4 additional malformations reported: microtia with absent auditory canal (40 mg/d); unspecified cardiovascular malformation; unspecified “severe deformity” (doses unknown)
Biological Plausibility: Statin Pharmacodynamics & Clinical Reports
All lipophilic statins were associated with reports of malformation following exposure
Pravastatin, hydrophilic and minimally detectable in the embryo, generated 20 evaluable reports of exposure but no reports of malformation or adverse pregnancy outcome
Insufficient exposure data were available to assess fluvastatin; no data available on rosuvastatin exposure
Lovastatin Pharmacodynamics:Distribution to Embryo
Lovastatin is lipophilic crosses placenta and blood-brain barrier
Concentration of lovastatin in embryonic tissues is approximately 25% of maternal plasma concentration (esp. liver, adrenal)
Neuroepithelium of early embryo shows highest expression of HMG-CoA reductase (CNS is first tissue to undergo expansion)
Biological Plausibility:Teratogenicity in Animals
Lovastatin: Rat: vertebral/skeletal defects; neural tube defect; gastroschisis; neuro-
behavioral deficits (low-dose) Mouse: skeletal and visceral malformations without maternal toxicity Rabbit: visceral “variations”; delayed ossification (very low dose)
Other lipophilic statins (none reported for pravastatin): Simvastatin: neural tube defect; malformations of gut, heart, skeleton Atorvastatin: neuro-behavioral deficits; visceral variations; fetal loss Cerivastatin: skull defects; major vascular anomalies; clefting; death Fluvastatin: vertebral malformations; perinatal mortality
Other chemical inhibitors of cholesterol biosynthesis: Holoprosencephaly (many species); aqueductal stenosis;
hydrocephalus; malformations of vertebrae, limbs, palate, gut, heart In susceptible species, any of the above malformations may be
observed, depending on timing of exposure
Biological Plausibility: Biomechanisms Under Study
Lovastatin in vivo decreases cholesterol levels in the CNS and alters neuron membrane properties and synapse formation. Decreases caveolae, site of folate receptors.
Lovastatin induces neuronal cell death in vitro at sub-physiologic concentrations
VACTERL association is induced in mice by decreasing the activity of a cholesterol-regulated patterning molecule (sonic hedgehog).
Mevalonate pathway intermediates (dolichols, prenylation of proteins, Co-enzyme Q10) modulate many critical regulatory and metabolic functions used by dividing cells
Factors Supporting Potential Teratogenicity Of Lovastatin in Humans
Most malformations reported following lovastatin exposure are similar to those observed in animal studies of lovastatin and other lipophilic statins
Two rare malformations (holoprosencephaly and the VACTERL association) were reported following exposures to both lovastatin and another lipophilic statin (cerivastatin and simvastatin, respectively)
The recurrence of these particular malformations could be interpreted as unexpected given the apparently small population of exposed pregnant women (manufacturer reports, registries)

Clinical Points to Consider
Observed malformations are generally induced very early, shortly after implantation and before the likely recognition of pregnancy
11% of CUSTOM uptake was by women <45 years of age, 5% < 40 years of age. Unplanned pregnancy is common throughout the population
Discontinuation of a teratogenic medication upon recognition of pregnancy may be insufficient to prevent severe effects

Conclusions
According to standard criteria for assessing teratogenicity, the data shown suggest the hypothesis that lovastatin MAY be a human teratogen, particularly in the central nervous system.
Prospective studies following exposed pregnancies and offspring through the age of five years are essential to test the teratogenic hypothesis and to characterize any adverse neurodevelopmental or other impact of lovastatin (or any statin) on the developing fetus
Acknowledgments
This work was supported by the Division of Intramural Research at the National Human Genome Research Institute, National Institutes of Health.
The views expressed here are those of the authors alone and do not represent the official position of the NHGRI, the NIH, or the Department of Health and Human Services.
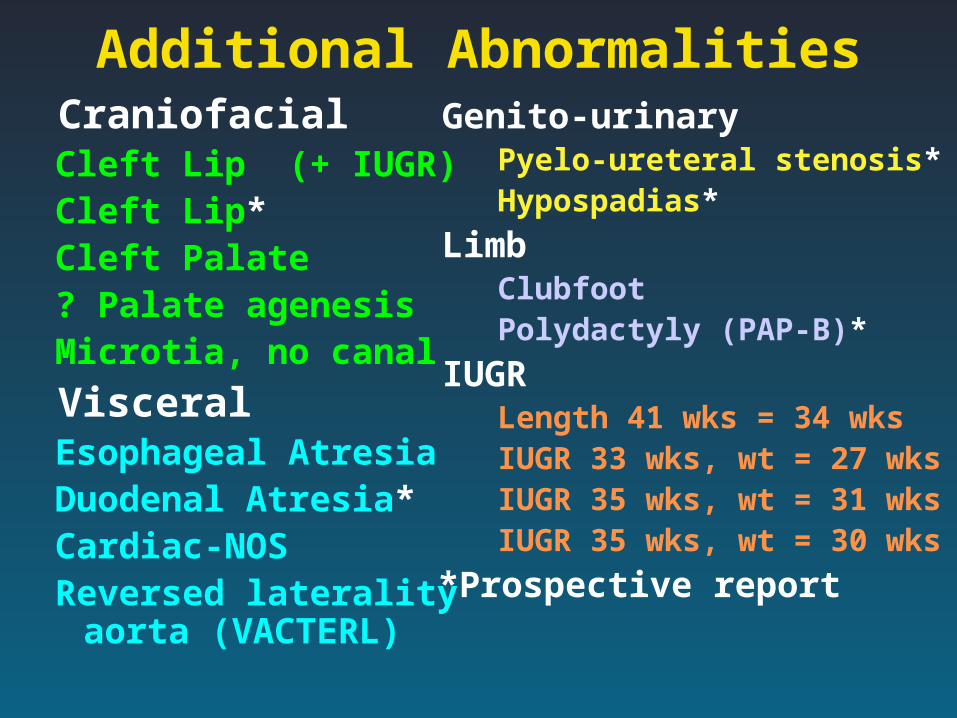
Additional Abnormalities Craniofacial
Cleft Lip (+ IUGR)Cleft Lip*Cleft Palate? Palate agenesisMicrotia, no canal
VisceralEsophageal AtresiaDuodenal Atresia*Cardiac-NOSReversed laterality
aorta (VACTERL)
Genito-urinary Pyelo-ureteral stenosis* Hypospadias*
Limb Clubfoot Polydactyly (PAP-B)*
IUGR Length 41 wks = 34 wks IUGR 33 wks, wt = 27 wks IUGR 35 wks, wt = 31 wks IUGR 35 wks, wt = 30 wks
*Prospective report
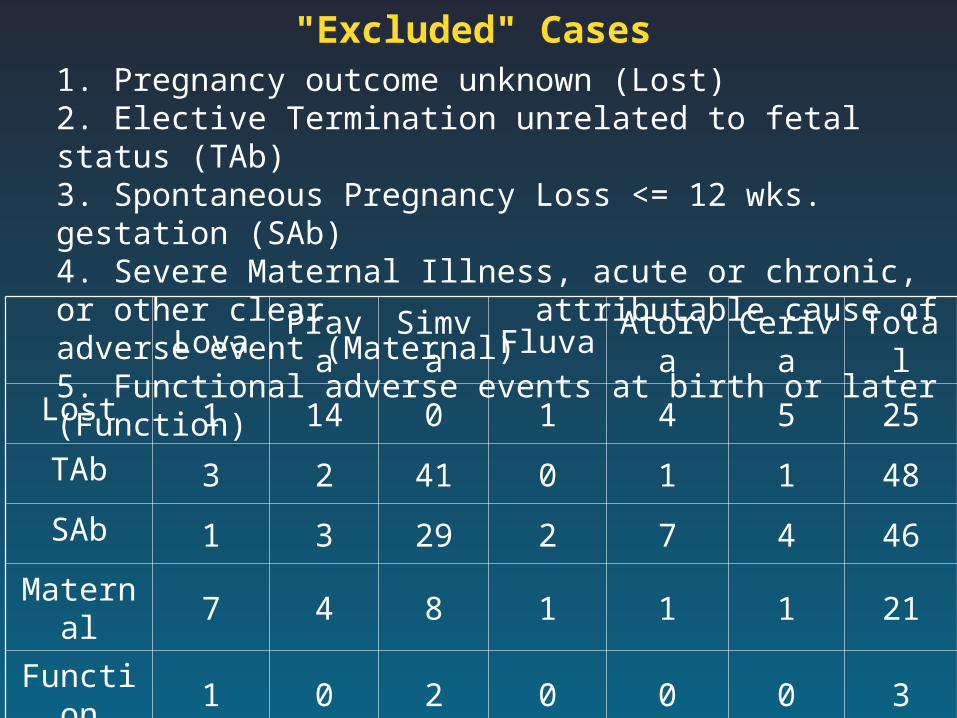
1. Pregnancy outcome unknown (Lost)2. Elective Termination unrelated to fetal status (TAb)3. Spontaneous Pregnancy Loss <= 12 wks. gestation (SAb)4. Severe Maternal Illness, acute or chronic, or other clear attributable cause of adverse event (Maternal)5. Functional adverse events at birth or later (Function)
"Excluded" Cases
Lova Prava Simva Fluva Atorva Ceriva Total
Lost 1 14 0 1 4 5 25
TAb 3 2 41 0 1 1 48
SAb 1 3 29 2 7 4 46
Maternal 7 4 8 1 1 1 21
Function 1 0 2 0 0 0 3
Total 13 22 80 4 13 11 143
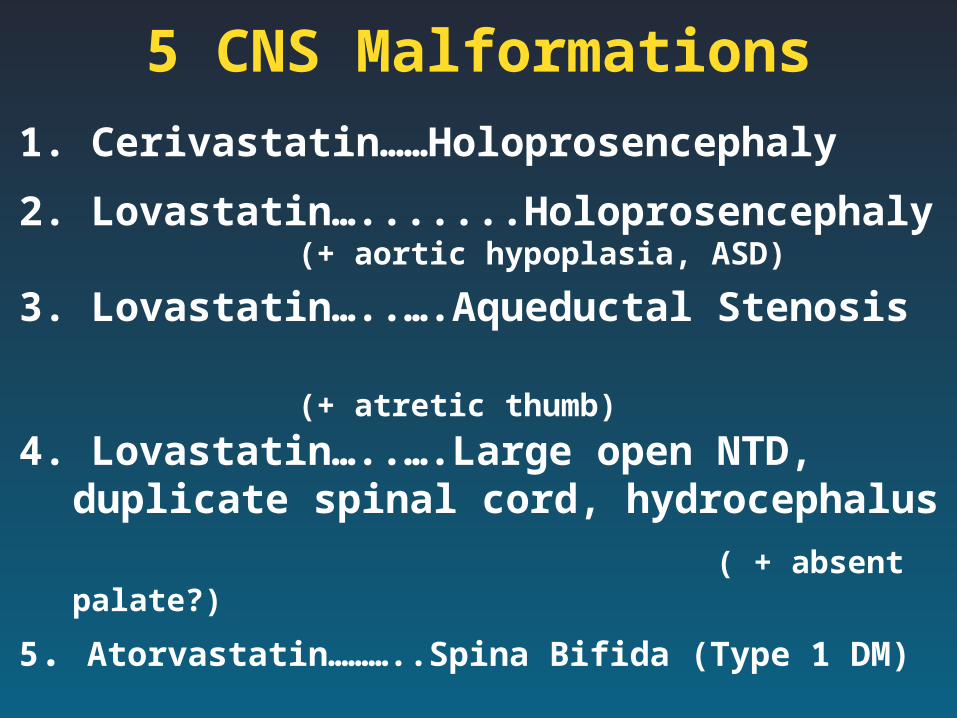
5 CNS Malformations
1. Cerivastatin……Holoprosencephaly
2. Lovastatin….......Holoprosencephaly
(+ aortic hypoplasia, ASD)
3. Lovastatin…..….Aqueductal Stenosis (+ atretic thumb)
4. Lovastatin…..….Large open NTD, duplicate spinal cord, hydrocephalus
( + absent palate?)
5. Atorvastatin………..Spina Bifida (Type 1 DM)
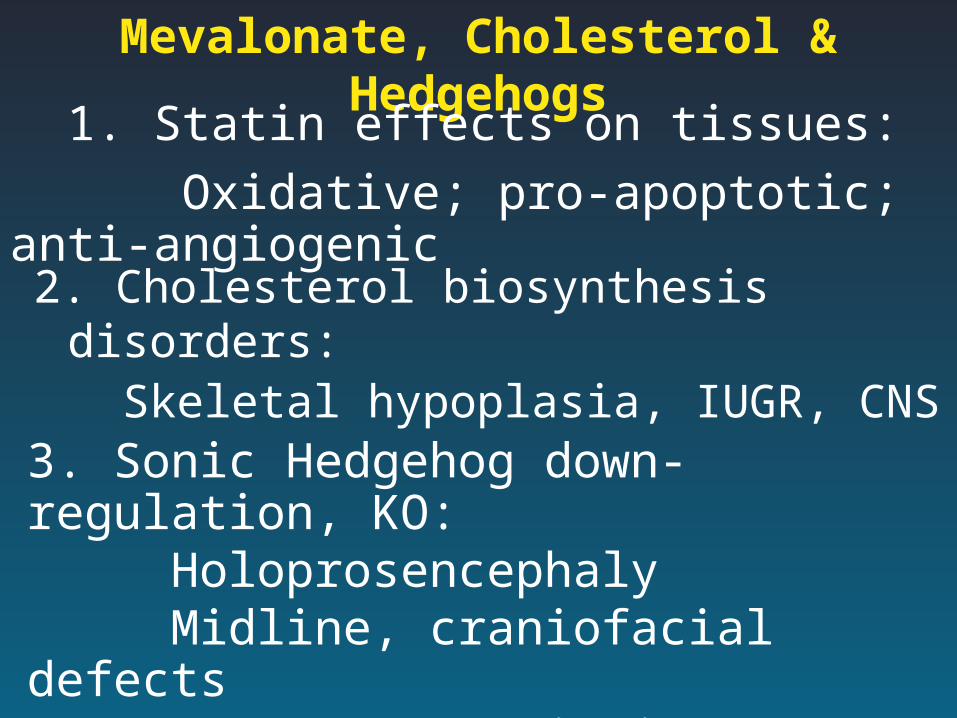
Mevalonate, Cholesterol & Hedgehogs
2. Cholesterol biosynthesis disorders: Skeletal hypoplasia, IUGR, CNS
3. Sonic Hedgehog down-regulation, KO: Holoprosencephaly Midline, craniofacial defects VACTERL association
1. Statin effects on tissues:
Oxidative; pro-apoptotic; anti-angiogenic
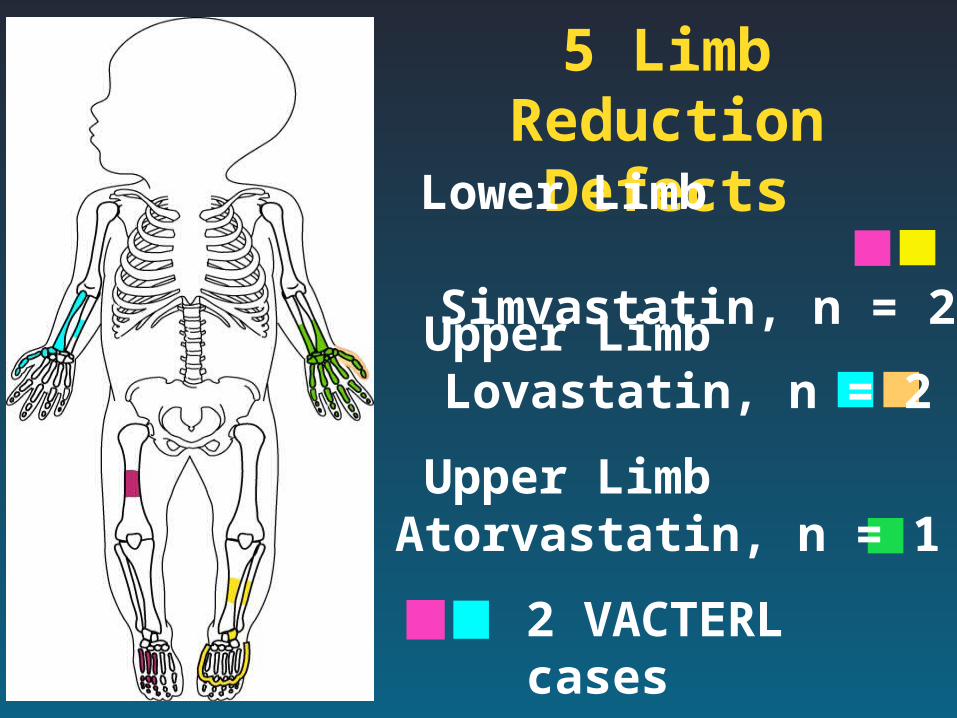
5 Limb Reduction Defects
Lower Limb Simvastatin, n = 2
Upper Limb Lovastatin, n = 2
Upper Limb Atorvastatin, n = 1
2 VACTERL cases

Epidemiologic ComparisonsSelected Reports
“Mixed” LRD (n = 3)
1 / 100,000 births
VACTERL (n = 2) 1 / 50K – 500K births
Holoprosencephaly (n = 2)
1 / 16,000 births
Exposure Estimates
through year 2000:
Ceriva: 150 births Simva: 5000 births Lova: 3500 births Atorva: 6000 births Fluva: 200 births Prava: 3200 births
Experimental Findings HMG-CoA expressed in blastocyst, gastrula,
neuroepithelium at high levels
Lovastatin alters gastrulation by depletion of dolichol for cell migration (echinoderm)
Lovastatin cholesterol in vivo brain: plasma membranes, caveolae, synaptic vesicles
Simvastatin target organ includes thyroid Range animals had complex limb defects and
HPE: exposure from conception on to inhibitor of Hedgehog signal transduction.

Estimated Statin Exposures in Pregnancyfor the year 2000, by Drug and Country
Prava Simva Fluva Atorva Total
USA 407 1030 45 2055 3537
UK 50 184 17 123 374
France 215 159 50 250 674
Total 672 1373 112 2428 4585
Numbers of exposed pregnancies are tiny relative to occurrence of rare outcomes
Pravastatin use is non-trivial: a meaningful negative control

Multiple Malformation Cases1. Semi-lobar HPE; ASD; aortic hypoplasia (died)2. Aqueductal Stenosis; banded, atretic thumb3. Large NTD; cerebellar herniation;palate absent4. VACTERL # 1 (Lovastatin): esophageal atresia;
radial ray aplasia; hypoplastic ulna; fused ribs, butterfly vertebrae, scoliosis; renal dysplasia; anal atresia. Plus: torticollis; hemi-hypertrophy; ptosis. 46,XX Fanconi negative.(1/ 500,000)
5. VACTERL # 2 (Simvastatin): lower limb reduction defects (femur, foot); aortic arch laterality reversed; disorganized lumbo-sacral vertebrae; renal dysplasia (1 / 50,000)