Embed Size (px)
Citation preview
The Patient-Centered Medical Home Model
Jasmine D. Gonzalvo, PharmD, BCPS, BC-ADM, CDE, LDE
Clinical Associate Professor
College of Pharmacy, Purdue University
Clinical Pharmacy Specialist, Ambulatory Care
Eskenazi Health
OBJECTIVES
2
Define the patient‐centered medical home model (PCMH)
List essential components of a successful PCMH
Outline rationale for establishing a PCMH
Describe potential payment models for PCMHs
Provide details about the NCQA standards for PCMHs
OBJECTIVES
3
Patient Centered Medical Home:
Defined
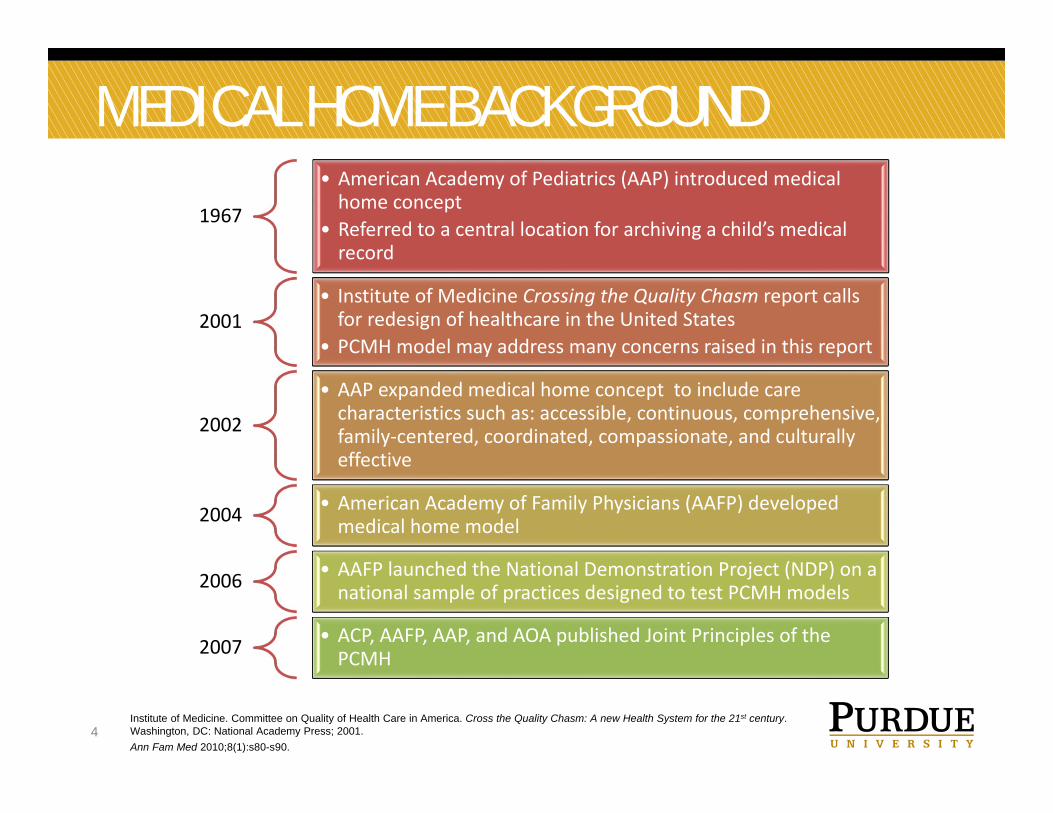
MEDICAL HOME BACKGROUND
4
1967
• American Academy of Pediatrics (AAP) introduced medical home concept
• Referred to a central location for archiving a child’s medical record
2001• Institute of Medicine Crossing the Quality Chasm report calls for redesign of healthcare in the United States
• PCMH model may address many concerns raised in this report
2002
• AAP expanded medical home concept to include care characteristics such as: accessible, continuous, comprehensive, family‐centered, coordinated, compassionate, and culturally effective
2004 • American Academy of Family Physicians (AAFP) developed medical home model
2006 • AAFP launched the National Demonstration Project (NDP) on a national sample of practices designed to test PCMH models
2007 • ACP, AAFP, AAP, and AOA published Joint Principles of the PCMH
Institute of Medicine. Committee on Quality of Health Care in America. Cross the Quality Chasm: A new Health System for the 21st century. Washington, DC: National Academy Press; 2001.Ann Fam Med 2010;8(1):s80-s90.
U.S. MEDICAL HOME MODELS
5https://www.pcpcc.org/initiatives/national
MEDICAL HOME MODEL – DEFINED
6
• Core features• Widely accepted model for how primary care should be
organized and delivered throughout the health care system• Philosophy of health care delivery that encourages providers and
care teams to meet patients where they are• Place where patients are treated with respect, dignity, and
compassion, and enable strong and trusting relationships with providers and staff
• PCMH is not a final destination instead, it is a model for achieving primary care excellence so that care is received in the right place, at the right time, and in the manner that best suits a patient's needs
Model or philosophy of primary care that is patient-centered, comprehensive, team-based, coordinated,
accessible, and focused on quality and safety
https://www.pcpcc.org/about/medical-home
MEDICAL HOME MODEL – DEFINED
7
• Core features• Provides enhanced primary care services of value to patients,
their families, and the care teams who work with them• Provides improved access to high-quality, patient-centered
primary care through trusted relationships with patients, families, and caregivers
• Incorporates team-based care with clinicians and staff working at the top of their skill set
• Provides cost-effective care coordination and population health management connecting patients to the “medical neighborhood” and to their community
An innovation in care delivery designed to advance and achieve the Triple Aim of improved patient experience, improved population health, and reduced cost of care
Nielsen, M., Buelt, L., Patel, K, & Nichols, L.(2016). The Patient‐Centered Medical Home's Impact on Cost and Quality, Review of Evidence, 2014‐2015. ‐See more at: https://www.pcpcc.org/resource/patient‐centered‐medical‐homes‐impact‐cost‐and‐quality‐2014‐2015#sthash.MNtkVtTI.dpuf
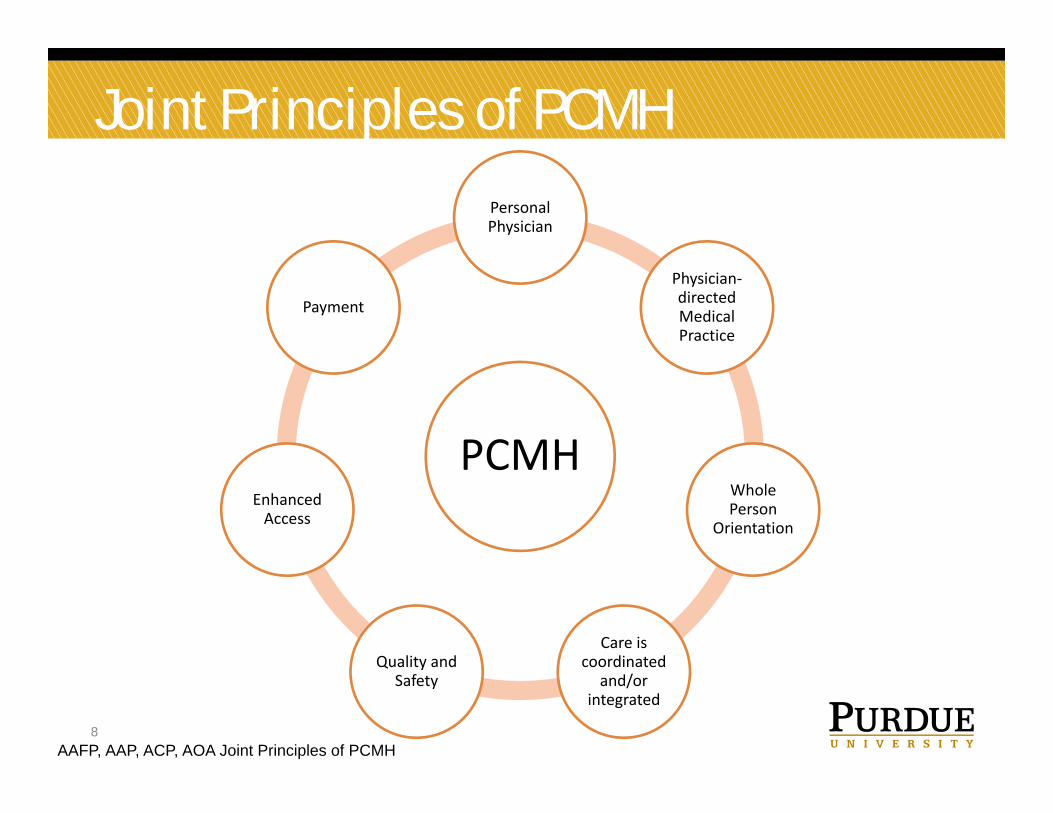
Joint Principles of PCMH
8
PCMH
Personal Physician
Physician‐directed Medical Practice
Whole Person
Orientation
Care is coordinated
and/or integrated
Quality and Safety
Enhanced Access
Payment
AAFP, AAP, ACP, AOA Joint Principles of PCMH

http://www.ncqa.org/programs/recognition/practices/patient-centered-medical-home-pcmh/why-pcmh/overview-of-pcmh/the-medical-home-neighborhood
Personal Physician
11
Essential Components
Personal Physician
12AAFP, AAP, ACP, AOA Joint Principles of PCMH
Each patient has an ongoing relationship with a personal physician trained to provide first contact, continuous, and comprehensive care
Physician Directed Medical Practice
13AAFP, AAP, ACP, AOA Joint Principles of PCMH
The personal physician leads a team of individuals at the practice level who collectively take responsibility for the ongoing care of patients
Whole Person Orientation
14AAFP, AAP, ACP, AOA Joint Principles of PCMH
The personal physician is responsible for providing for all the patient’s health care needs or taking responsibility for appropriately arranging care with other qualified professionals
Includes care for all stages of life: acute care, chronic care, preventive services, and end of life care
Coordinated/Integrated Care
15AAFP, AAP, ACP, AOA Joint Principles of PCMH
Care is coordinated or integrated across all elements of the complex health care system and the patient’s community
Care facilitated by registries, information technology, and health information exchange to assure that patients get the indicated care when and where they need and want it in a culturally and linguistically appropriate manner
Quality and Safety
16AAFP, AAP, ACP, AOA Joint Principles of PCMH
Practices advocate for their patients to support the attainment of optimal, patient‐centered outcomes that are defined by a care planning process driven by a compassionate, robust partnership between physicians, patients, and the patient’s family
Evidence‐based medicine and clinical decision‐support tools guide decision making
Physicians in the practice accept accountability for continuous quality improvement through voluntary engagement in performance measurement and improvement
Patients actively participate in decision‐making and feedback is sought to ensure patients’ expectations are being met
Quality and Safety
17AAFP, AAP, ACP, AOA Joint Principles of PCMH
Information technology is utilized appropriately to support optimal patient care, performance measurement, patient education, and enhanced communication
Practices go through a voluntary recognition process by an appropriate non‐governmental entity to demonstrate that they have the capabilities to provide patient‐centered services consistent with the medical home model
Patients and families participate in quality improvement activities at the practice level
Enhanced Access
18AAFP, AAP, ACP, AOA Joint Principles of PCMH
Available through systems such as open scheduling, expanded hours, and new options for communication between patients, their personal physician, and practice staff
Payment
19AAFP, AAP, ACP, AOA Joint Principles of PCMH
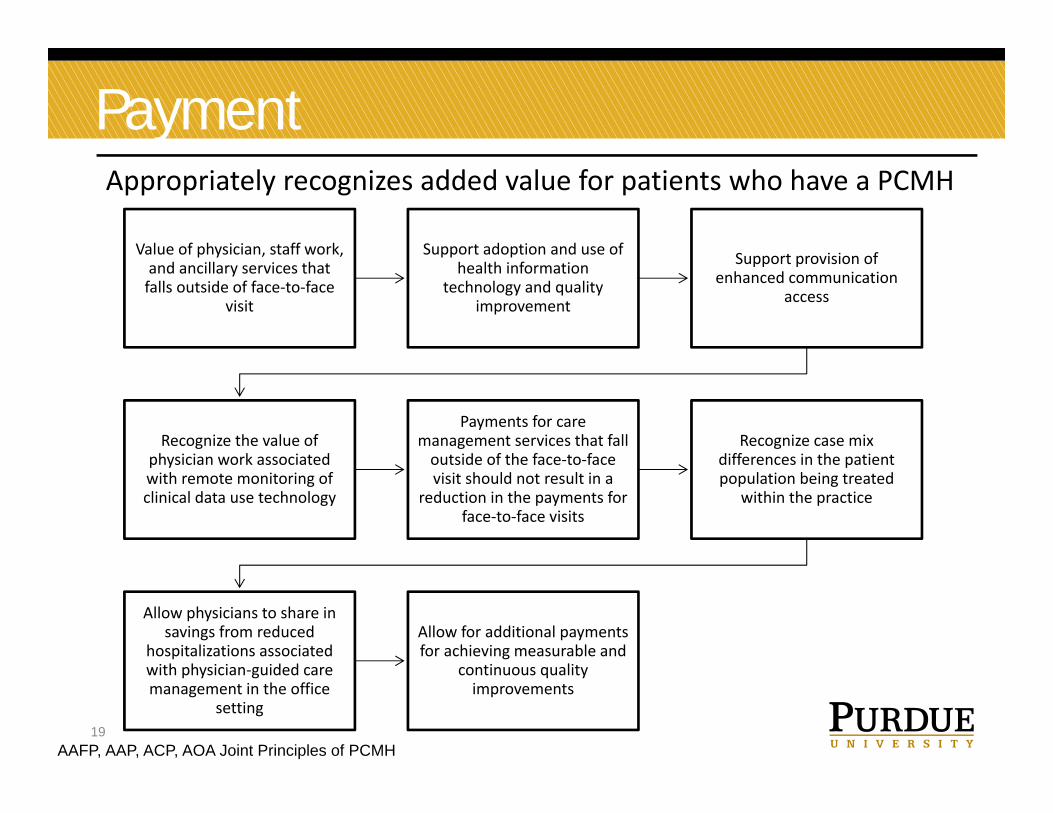
Appropriately recognizes added value for patients who have a PCMH
Value of physician, staff work, and ancillary services that falls outside of face‐to‐face
visit
Support adoption and use of health information
technology and quality improvement
Support provision of enhanced communication
access
Recognize the value of physician work associated with remote monitoring of clinical data use technology
Payments for care management services that fall outside of the face‐to‐face visit should not result in a
reduction in the payments for face‐to‐face visits
Recognize case mix differences in the patient population being treated
within the practice
Allow physicians to share in savings from reduced
hospitalizations associated with physician‐guided care management in the office
setting
Allow for additional payments for achieving measurable and
continuous quality improvements
20
Rationale
The patient‐centered medical home can help health centers meet their clients’ care needs in a more coordinated, effective way.
Medical Homes are more prepared to undertake quality improvement activities, which can improve health outcomes and
lower costs.
Medical Homes can provide access to the nonmedical services that many low‐income people need, such as transportation, nutritious
food, and supportive housing.
Access to behavioral health services and dental care improves with medical home implementation.
RATIONALE
http://www.commonwealthfund.org/publications/lists/community-health-centers-becoming-medical-homes-top-5
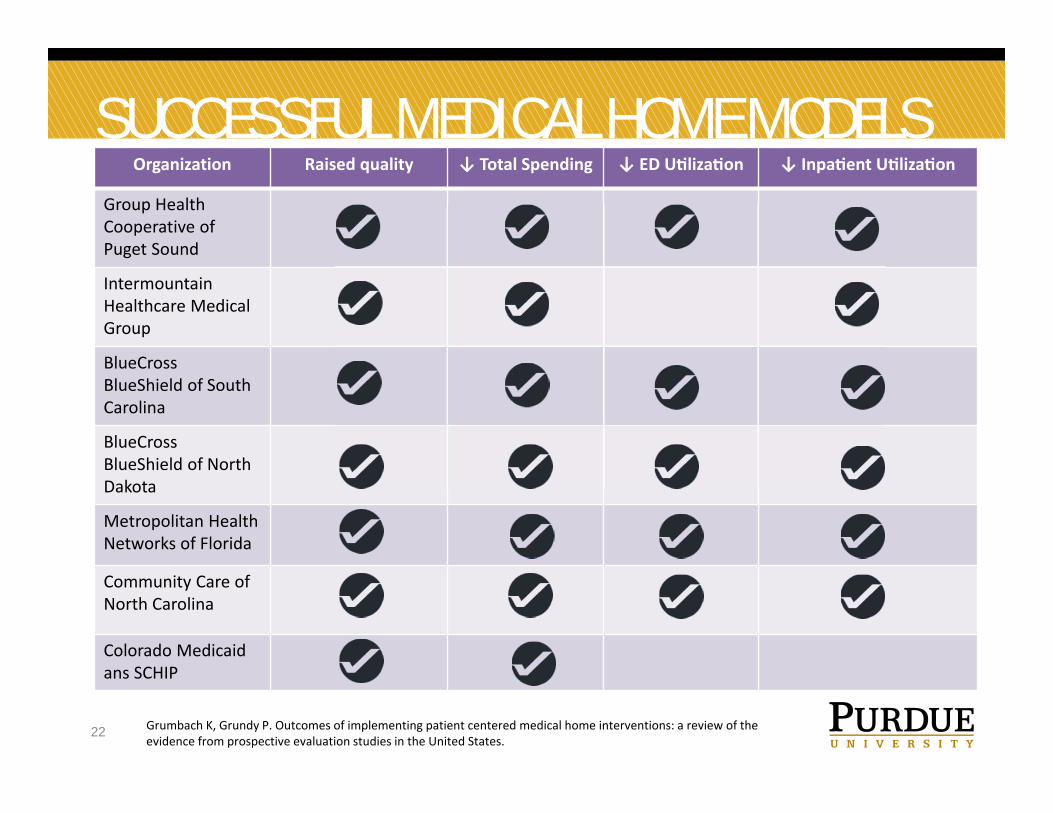
SUCCESSFUL MEDICAL HOME MODELS
22 Grumbach K, Grundy P. Outcomes of implementing patient centered medical home interventions: a review of the evidence from prospective evaluation studies in the United States.
Organization Raised quality ↓ Total Spending ↓ ED U liza on ↓ Inpa ent U liza on
Group Health Cooperative of Puget Sound
IntermountainHealthcare Medical Group
BlueCross BlueShield of South Carolina
BlueCross BlueShield of North Dakota
Metropolitan Health Networks of Florida
Community Care of North Carolina
Colorado Medicaid ans SCHIP
CONFLICTING EVIDENCE
23 http://www.commonwealthfund.org/publications/in-brief/2017/mar/patient-centered-medical-homes-systematic-differences
The National Demonstration Project (NDP) examined PCMH models over 2 years in a diverse sample of 36 family practices
11 PCMH initiatives did little to improve costs, utilization, or quality
Neither inpatient admissions nor ED visits declined for PCMH patients compared to study
controls and most quality metrics were unchanged
PCMH vary significantly due to differences in their design and implementation
HOW TO BUILD A PCMH
24
The National Demonstration Project (NDP) examined PCMH models over 2 years in a diverse sample of 36 family practices
Start small and build• Initially make changes for a small group of patients and build from lessons learned
Use data to understand your patient population• Stratify patients by age, chronic condition, and risk levels to learn best practices for care management
Think long term; think partnership
Engage patients and families
FIRST YEAR COSTS
25
• Proposed first year costs for one physician practice utilizing existing staff can range from $10,500 to $52,100
• Proposed first year costs for a five physician practice with two health coaches can range from $126,000 to $346,500
• Costs take into consideration: RN health coaches Medical home administration time Training costs and associated lost revenue EMR implementation Disease registry NCQA certification Point of care lab testing supplies Patient education supplies Miscellaneous costs
26
Payment Models
Primary Care Payment Models
27
CMS Alliance to Modernize Healthcare
https://www.mitre.org/centers/cms-alliances-to-modernize-healthcare/who-we-are
Primary Care Payment Models (PCPMs)
28
Reduce administrative burden, encourage team-based approaches to primary care and care coordination, and
allow the flexibility needed to innovate value-based delivery approaches, particularly with respect to
establishing connections between primary care and behavioral health and community services.
Nielsen, M., Buelt, L., Patel, K, & Nichols, L.(2016). The Patient‐Centered Medical Home's Impact on Cost and Quality, Review of Evidence, 2014‐2015. ‐See more at: https://www.pcpcc.org/resource/patient‐centered‐medical‐homes‐impact‐cost‐and‐quality‐2014‐2015#sthash.MNtkVtTI.dpuf
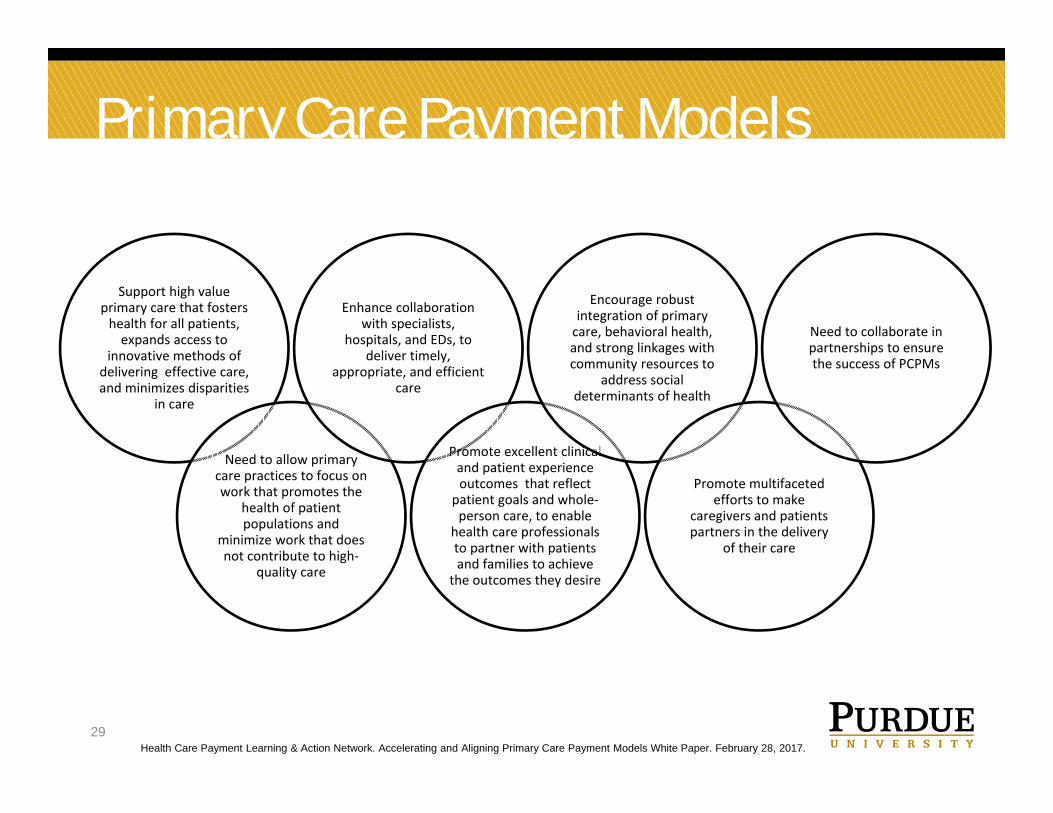
Primary Care Payment Models
29Health Care Payment Learning & Action Network. Accelerating and Aligning Primary Care Payment Models White Paper. February 28, 2017.
Support high value primary care that fosters health for all patients, expands access to
innovative methods of delivering effective care, and minimizes disparities
in care
Need to allow primary care practices to focus on work that promotes the
health of patient populations and
minimize work that does not contribute to high‐
quality care
Enhance collaboration with specialists,
hospitals, and EDs, to deliver timely,
appropriate, and efficient care
Promote excellent clinical and patient experience outcomes that reflect
patient goals and whole‐person care, to enable
health care professionals to partner with patients and families to achieve
the outcomes they desire
Encourage robust integration of primary care, behavioral health, and strong linkages with community resources to
address social determinants of health
Promote multifaceted efforts to make
caregivers and patients partners in the delivery
of their care
Need to collaborate in partnerships to ensure the success of PCPMs
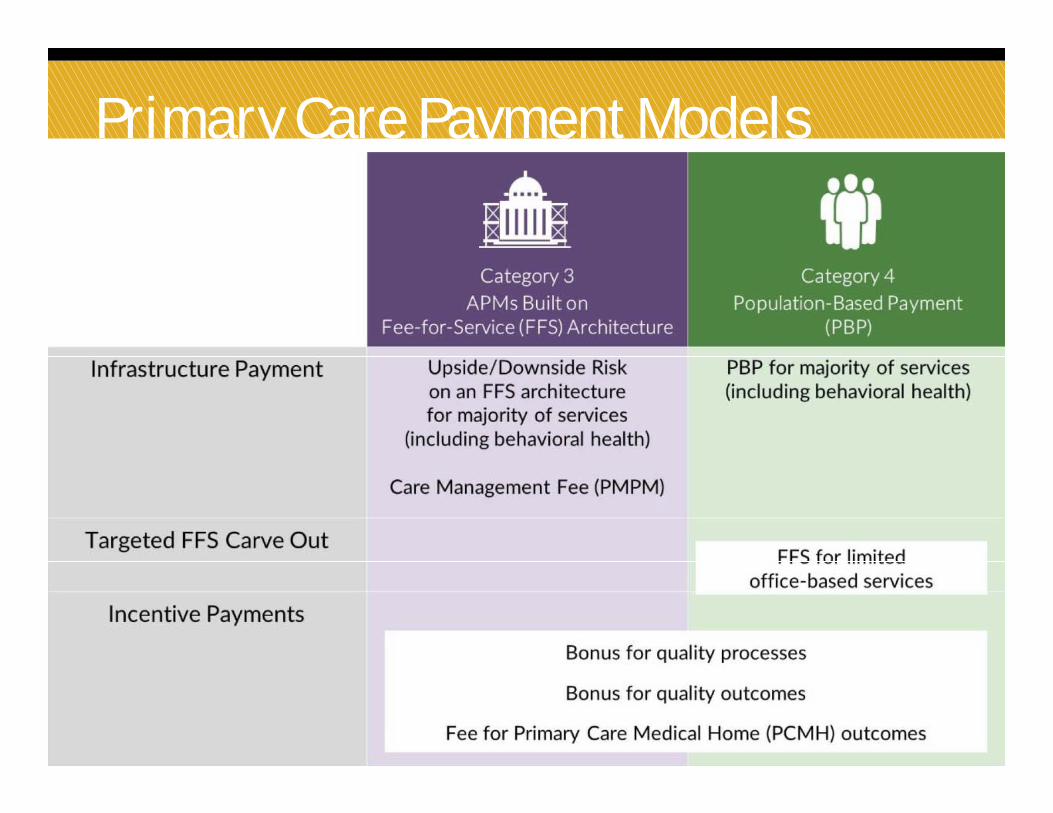
Primary Care Payment Models
30Health Care Payment Learning & Action Network. Accelerating and Aligning Primary Care Payment Models White Paper. February 28, 2017.
31
NCQA Standards
http://store.ncqa.org/index.php/recognition/patient-centered-medical-home-pcmh.html?___SID=U

LESSONS
33
• Establishing a PCMH is a significant undertaking
• Long‐term success of any PCMH implementation depends on practices’ ability to manage a successful, efficient practice in an environment of constant change
• It is easy to lose sight of the patient in developing a PCMH
• Specific components of the PCMH that contribute to successful outcomes should be identified
• NCQA recognition may be helpful in the development of a PCMH
RESOURCES
34
• National Committee for Quality Assurancehttp://www.ncqa.org/tabid/631/default.aspx
• National Center for Medical Home Implementation (American Academy of Pediatrics)http://www.medicalhomeinfo.org/national/projects_and_initiatives.aspx
• Patient‐Centered Primary Care Collaborative https://www.pcpcc.org/
The Patient-Centered Medical Home Model
Jasmine D. Gonzalvo, PharmD, BCPS, BC-ADM, CDE, LDE
Clinical Associate Professor
College of Pharmacy, Purdue University
Clinical Pharmacy Specialist, Ambulatory Care
Eskenazi Health