Embed Size (px)
Citation preview

Medical Management of Cushing’s Disease
Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine
Division of Endocrinology & Metabolism Dalhousie University, Halifax, NS

List of topics that we will cover
The pertinent pituitary physiology
An update on the medical management of ACTH producing pituitary tumours
Details of surgical management will not be covered during the talk but you are welcome to ask about it in the Q&A session
Amy’s case
- Gained 50 lbs in 1 year - Amenorrhea for 10
months - New-onset hypertension - Proximal muscle
weakness - Depression

Amy’s case
- Gained 50 lbs in 1 year - Amenorrhea for 10
months - New onset hypertension - Seen by psychiatry for ‘psychosis’

Hypothalamo-pituitary system
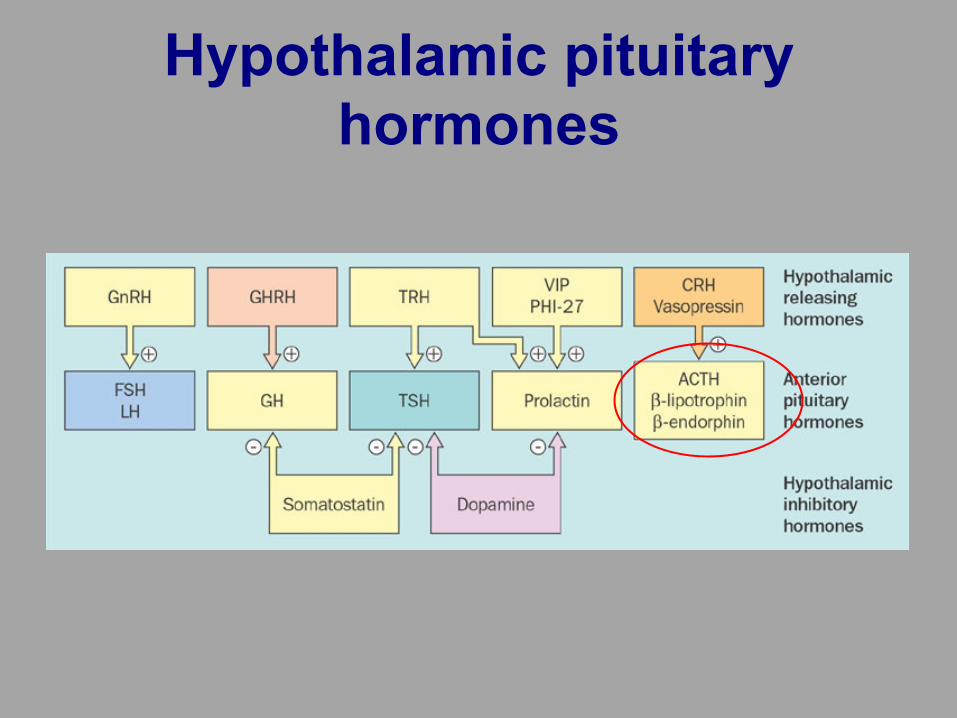
Hypothalamic pituitary hormones

Goals of therapy for functioning sellar tumors
Remove (or shrink) the tumour
Normalize hormone levels

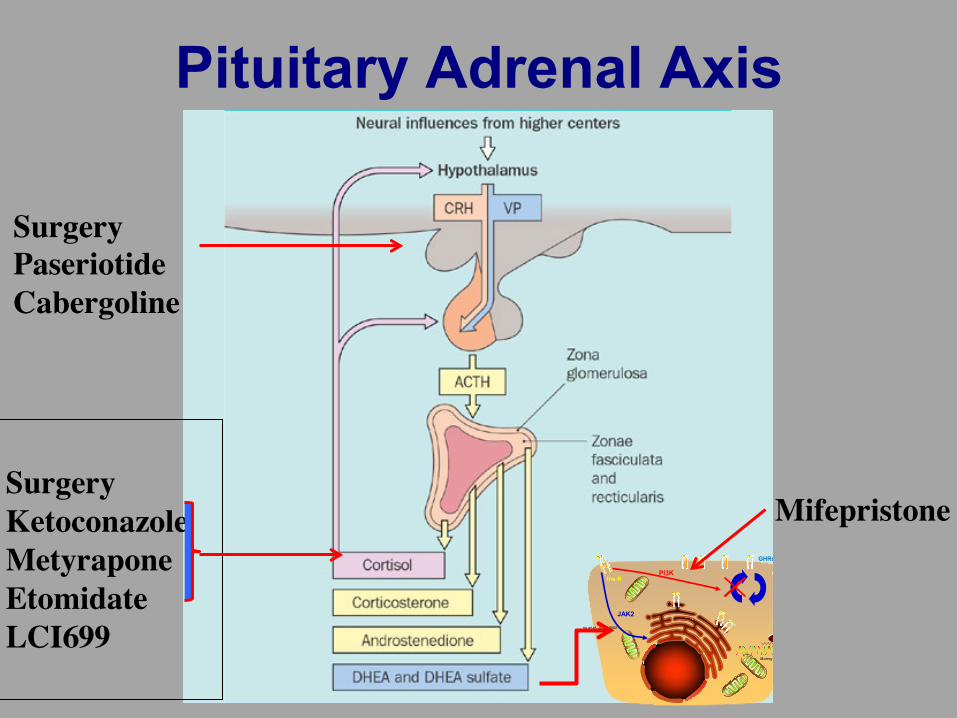
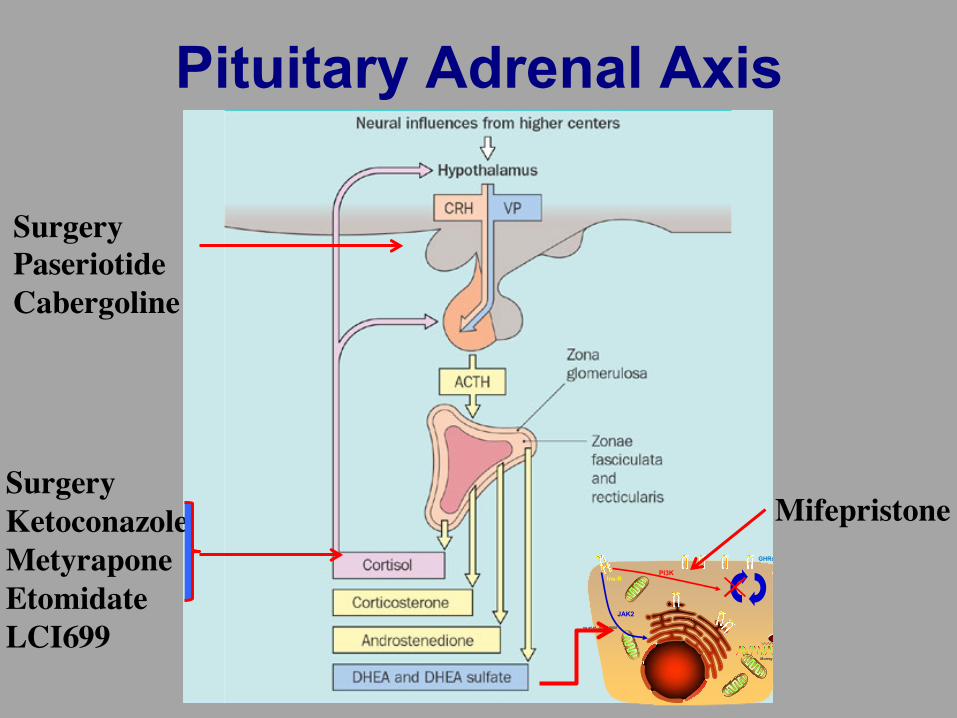
Pituitary Adrenal Axis
Surgery PaseriotideCabergoline
SurgeryKetoconazoleMetyraponeEtomidateLCI699
MifepristoneY
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn IIIFn III
Fn III
Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Insulin
SSS
S
SS
Insulin
SSS
S
SS
PI3K
JAK2
Ins Ins-R
GHRs
IGF-I
During co-treatment with SSAs, PEG (being a competitive GHR blocker) has less GH to compete with, and less GHRs to block on the liver. Moreover, SSAs inhibit IGF-1 generation by liver directly
Leung et al. JCEM 2000
Murray RD et al. JCI 2004
SSAs, decreasing portal insulin concentration, may reduce the number of GHRs expressed in the liver, and may also directly inhibit liver IGF-1 generation

Cortisol Synthesis
Pregnenolone
11-deoxycortisol
Cortisol
17-OH pregnenolone
17-OH progesterone
Cholesterol
ACTH
Aldosterone
Corticosterone
18-OH corticosterone
Feedback loop malfunctioning in Cushing’s
Progesterone
Dehydroepiandrosterone
Androstenedione
Testosterone
11-deoxycorticosterone
Estradiol
Estrone
11-deoxycortisol
ACTH
Testosterone
11-deoxycorticosterone

First-line therapy: Transsphenoidal adenomectomy
First-line therapy for patients with Cushing’s disease is transsphenoidal adenomectomy to remove the ACTH-secreting pituitary adenoma
Treatment goals
Normalization of cortisol levels
Reversal of clinical features
Long-term biochemical control
Removal of tumor mass
Preservation of normal pituitary function

Biochemical remission
• Post-operative biochemical assessment is used to: – Evaluate whether patients are in remission – Inform decisions about the need for further therapy, such as repeat
surgery or medical therapy – Provide an idea of overall surgical success
• There are three possible outcomes of pituitary surgery:
ACTH +++
Cortisol +++ Adrenal
ACTH �ve
Failure
Adrenal No cortisol
ACTH �ve
No ACTH
Success
Adrenal Cortisol +
ACTH+ ACTH �ve
Partial success

Post-operative remission rates and long-term recurrence rates vary widely
Remission
Recurrence
0
Swearingen 1999 (n=161)
Invitti 1999 (n=236)
Sonino 1996 (n=103)
Knappe 1996 (n=310)
Bakiri 1996 (n=50)
Favia 1994 (n=110)
Trainer 1993 (n=45)
McCance 1993 (n=57)
Lindholm 1992 (n=48)
Robert 1991 (n=78)
Burke 1990 (n=41)
Guilhaume 1988 (n=64)
Mampalam 1988 (n=216)
Nakane 1987 (n=93)
Fahlbusch 1986 (n=101)
Lüdecke 1985 (n=100)
Boggan 1983 (n=100)
10 20 30 40 50 60 70 80 90 100 Patients (%)
Newell-Price J. IPC 2011;abst P13

Post-operative remission rates and long-term recurrence rates vary widely
Remission
Recurrence
0
Swearingen 1999 (n=161)
Invitti 1999 (n=236)
Sonino 1996 (n=103)
Knappe 1996 (n=310)
Bakiri 1996 (n=50)
Favia 1994 (n=110)
Trainer 1993 (n=45)
McCance 1993 (n=57)
Lindholm 1992 (n=48)
Robert 1991 (n=78)
Burke 1990 (n=41)
Guilhaume 1988 (n=64)
Mampalam 1988 (n=216)
Nakane 1987 (n=93)
Fahlbusch 1986 (n=101)
Lüdecke 1985 (n=100)
Boggan 1983 (n=100)
10 20 30 40 50 60 70 80 90 100 Patients (%)
In 17 studies published from 1983 to 1999, remission rates ranged from 46–93% recurrence rates ranged from 0–28%
Newell-Price J. IPC 2011;abst P13

Similar rates reported in more recent studies
Remission
Recurrence
Valassi 2010 (n=620) Alwani 2010 (n=79)
Jagannathan 2009 (n=261) Fomekong 2009 (n=40)
Atkinson 2008 (n=42)
Hammer 2004 (n=289) Rollin 2004 (n=41)
Pereira 2003 (n=78) Chen 2003 (n=174)
Flitsch 2003 (n=147) Shimon 2002 (n=82)
Rees 2002 (n=54) Barbetta 2001 (n=68)
Chee 2001 (n=61) Imaki 2001 (n=49)
Patients (%)
Jehle 2008 (n=193) Prevedello 2008 (n=167)
Xing 2008 (n=266) Carrasco 2008 (n=68)
Romanholi 2008 (n=57) Patil 2008 (n=215)
Rollin 2007 (n=108) Pouratian 2007 (n=111)
Acebes 2007 (n=44) Shah 2006 (n=65)
Hoffmann 2006 (n=100) Esposito 2006 (n=40) Atkinson 2005 (n=63)
10 20 30 40 50 60 70 80 90 100 0
Newell-Price J. IPC 2011;abst P13

Currently used medical therapies in Cushing’s disease
Steroido- genesis inhibitors
• Mitotane, metyrapone, ketoconazole, etomidate
• Reduce cortisol levels via inhibition of steroid synthesis in the adrenal gland
• Temporary, palliative treatment
Biller BMK et al. J Clin Endocrinol Metab 2008;93:2454–2462
Pituitary Adrenal Axis
Surgery PaseriotideCabergoline
SurgeryKetoconazoleMetyraponeEtomidateLCI699
MifepristoneY
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn IIIFn III
Fn III
Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Insulin
SSS
S
SS
Insulin
SSS
S
SS
PI3K
JAK2
Ins Ins-R
GHRs
IGF-I
During co-treatment with SSAs, PEG (being a competitive GHR blocker) has less GH to compete with, and less GHRs to block on the liver. Moreover, SSAs inhibit IGF-1 generation by liver directly
Leung et al. JCEM 2000
Murray RD et al. JCI 2004
SSAs, decreasing portal insulin concentration, may reduce the number of GHRs expressed in the liver, and may also directly inhibit liver IGF-1 generation

Ketoconazole
• Efficacy as monotherapy (200–1200 mg/day):1
– Retrospective study of 38 patients with active Cushing’s disease
– Treatment was stopped in first week in 5 patients due to clinical or biological intolerance
– 17 (51%) had normalized UFC at follow-up (mean: 23 months) – Clinical regression of signs of hypercortisolism – 5 patients with no visible adenoma at baseline developed a visible
tumor during follow-up
• Adverse events associated with ketoconazole include:2 – GI events – Pruritus and rash – Liver toxicity – Gynecomastia – Impairment of testicular function – Adrenal insufficiency
1. Castinetti F et al. Eur J Endocrinol 2008;158:91–99 2. Dang CN & Trainer P. Arq Bras Endocrinol Metabol 2007,51:1339–1348

Pituitary Adrenal Axis
Surgery PaseriotideCabergoline
SurgeryKetoconazoleMetyraponeEtomidateLCI699
MifepristoneY
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn IIIFn III
Fn III
Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Insulin
SSS
S
SS
Insulin
SSS
S
SS
PI3K
JAK2
Ins Ins-R
GHRs
IGF-I
During co-treatment with SSAs, PEG (being a competitive GHR blocker) has less GH to compete with, and less GHRs to block on the liver. Moreover, SSAs inhibit IGF-1 generation by liver directly
Leung et al. JCEM 2000
Murray RD et al. JCI 2004
SSAs, decreasing portal insulin concentration, may reduce the number of GHRs expressed in the liver, and may also directly inhibit liver IGF-1 generation

Cabergoline
• Potent dopamine type 2 receptor (DR2) agonist
• Approximately 80% of ACTH-secreting adenomas express the dopamine D2 receptor1
• Studies (n=20–27) have demonstrated the effective use of cabergoline in persistent or recurrent Cushing’s disease2,3
• The phenomenon of escape has been described
• Studies in larger patient populations are required to establish efficacy and safety
1. Pivonello R et al. J Clin Endocrinol Metab 2004;89:2452–2462
2. Pivonello R et al. J Clin Endocrinol Metab 2009;94:223–230 3. Godbout A et al. Eur J Endocrinol 2010;163:709–716
N
NH
NH
N
N H
O
O

The Medical Treatment of Cushing’s Disease:Effectiveness of Chronic Treatment with theDopamine Agonist Cabergoline in PatientsUnsuccessfully Treated by Surgery
Rosario Pivonello, Maria Cristina De Martino, Paolo Cappabianca, Monica De Leo,Antongiulio Faggiano, Gaetano Lombardi, Leo J. Hofland, Steven W. J. Lamberts,and Annamaria Colao
Departments of Molecular and Clinical Endocrinology and Oncology (R.P., M.C.D.M., M.D.L., A.F., G.L., A.C.),and Neurosurgery (P.C.), “Federico II” University, 80131 Naples, Italy; and Department of Internal Medicine(R.P., L.J.H., S.W.J.L.), Erasmus Medical Center, Rotterdam 3015 CE, The Netherlands
Background: The role of dopamine agonists in the treatment of Cushing’s disease (CD) has beenpreviously debated.
Aim: The aim of this study was to evaluate the effectiveness of short-term (3 months) and long-term(12–24 months) treatment with cabergoline in patients with CD.
Patients and Methods: 20 patients with CD unsuccessfully treated by surgery entered the study.Cabergoline was administered at an initial dose of 1 mg/wk, with a monthly increase of 1 mg, untilurinary cortisol levels normalized or the maximal dose of 7 mg/wk was achieved. The responsivenessto treatment was evaluated according to changes in urinary cortisol excretion. A decrease greaterthan 25% was considered as a partial response, whereas complete normalization was consideredas a full response at short-term evaluation; persistence of normal cortisol excretion was the onlycriterion to evaluate the response at long-term evaluation.
Results: After short-term treatment, 15 (75%) patients were responsive to cabergoline treatment.Among these, normalization of cortisol excretion was maintained in 10, whereas treatment escapewas observed in five patients after 6–18 months. Among the 10 long-term responsive patients,eight were followed for 24 months, whereas the remaining two were followed for 12–18 months,due to cabergoline withdrawal for intolerance. A sustained control of cortisol secretion for 24month cabergoline treatment at the maximal dose ranging from 1-7 mg/wk (median: 3.5) withoutsignificant side effects, was obtained in eight of 20 (40%) patients.
Conclusions: The results of this study demonstrated that cabergoline treatment is effective incontrolling cortisol secretion for at least 1–2 yr in more than one third of a limited population ofpatients with CD. If this evidence is confirmed by additional studies, this agent may be consideredas a useful treatment option in patients with CD who are unsuccessfully treated by neurosurgery.(J Clin Endocrinol Metab 94: 223–230, 2009)
Cushing’s disease (CD) is the most common form of Cushing’ssyndrome, caused by a corticotroph pituitary tumor, and
often complicated by hypertension and impaired glucose toler-ance and associated with increased morbidity and mortality for
cardiovascular diseases (1–3). The first-line treatment of CD issurgery, with the objective of removing the pituitary tumor, al-though it is effective in inducing immediate disease remission inaround 70% and late disease remission in around 50% of pa-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2009 by The Endocrine Societydoi: 10.1210/jc.2008-1533 Received July 16, 2008. Accepted October 17, 2008.First Published Online October 28, 2008
Abbreviations: CD, Cushing’s disease; HOMA-B, homeostasis model of assessment-!-cellfunction; HOMA-IR, homeostasis model of assessment-insulin resistance; MRI, magneticresonance imaging; PRL, prolactin.
O R I G I N A L A R T I C L E
E n d o c r i n e R e s e a r c h — B r i e f R e p o r t
J Clin Endocrinol Metab, January 2009, 94(1):223–230 jcem.endojournals.org 223
The Medical Treatment of Cushing’s Disease:Effectiveness of Chronic Treatment with theDopamine Agonist Cabergoline in PatientsUnsuccessfully Treated by Surgery
Rosario Pivonello, Maria Cristina De Martino, Paolo Cappabianca, Monica De Leo,Antongiulio Faggiano, Gaetano Lombardi, Leo J. Hofland, Steven W. J. Lamberts,and Annamaria Colao
Departments of Molecular and Clinical Endocrinology and Oncology (R.P., M.C.D.M., M.D.L., A.F., G.L., A.C.),and Neurosurgery (P.C.), “Federico II” University, 80131 Naples, Italy; and Department of Internal Medicine(R.P., L.J.H., S.W.J.L.), Erasmus Medical Center, Rotterdam 3015 CE, The Netherlands
Background: The role of dopamine agonists in the treatment of Cushing’s disease (CD) has beenpreviously debated.
Aim: The aim of this study was to evaluate the effectiveness of short-term (3 months) and long-term(12–24 months) treatment with cabergoline in patients with CD.
Patients and Methods: 20 patients with CD unsuccessfully treated by surgery entered the study.Cabergoline was administered at an initial dose of 1 mg/wk, with a monthly increase of 1 mg, untilurinary cortisol levels normalized or the maximal dose of 7 mg/wk was achieved. The responsivenessto treatment was evaluated according to changes in urinary cortisol excretion. A decrease greaterthan 25% was considered as a partial response, whereas complete normalization was consideredas a full response at short-term evaluation; persistence of normal cortisol excretion was the onlycriterion to evaluate the response at long-term evaluation.
Results: After short-term treatment, 15 (75%) patients were responsive to cabergoline treatment.Among these, normalization of cortisol excretion was maintained in 10, whereas treatment escapewas observed in five patients after 6–18 months. Among the 10 long-term responsive patients,eight were followed for 24 months, whereas the remaining two were followed for 12–18 months,due to cabergoline withdrawal for intolerance. A sustained control of cortisol secretion for 24month cabergoline treatment at the maximal dose ranging from 1-7 mg/wk (median: 3.5) withoutsignificant side effects, was obtained in eight of 20 (40%) patients.
Conclusions: The results of this study demonstrated that cabergoline treatment is effective incontrolling cortisol secretion for at least 1–2 yr in more than one third of a limited population ofpatients with CD. If this evidence is confirmed by additional studies, this agent may be consideredas a useful treatment option in patients with CD who are unsuccessfully treated by neurosurgery.(J Clin Endocrinol Metab 94: 223–230, 2009)
Cushing’s disease (CD) is the most common form of Cushing’ssyndrome, caused by a corticotroph pituitary tumor, and
often complicated by hypertension and impaired glucose toler-ance and associated with increased morbidity and mortality for
cardiovascular diseases (1–3). The first-line treatment of CD issurgery, with the objective of removing the pituitary tumor, al-though it is effective in inducing immediate disease remission inaround 70% and late disease remission in around 50% of pa-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2009 by The Endocrine Societydoi: 10.1210/jc.2008-1533 Received July 16, 2008. Accepted October 17, 2008.First Published Online October 28, 2008
Abbreviations: CD, Cushing’s disease; HOMA-B, homeostasis model of assessment-!-cellfunction; HOMA-IR, homeostasis model of assessment-insulin resistance; MRI, magneticresonance imaging; PRL, prolactin.
O R I G I N A L A R T I C L E
E n d o c r i n e R e s e a r c h — B r i e f R e p o r t
J Clin Endocrinol Metab, January 2009, 94(1):223–230 jcem.endojournals.org 223

The Medical Treatment of Cushing’s Disease:Effectiveness of Chronic Treatment with theDopamine Agonist Cabergoline in PatientsUnsuccessfully Treated by Surgery
Rosario Pivonello, Maria Cristina De Martino, Paolo Cappabianca, Monica De Leo,Antongiulio Faggiano, Gaetano Lombardi, Leo J. Hofland, Steven W. J. Lamberts,and Annamaria Colao
Departments of Molecular and Clinical Endocrinology and Oncology (R.P., M.C.D.M., M.D.L., A.F., G.L., A.C.),and Neurosurgery (P.C.), “Federico II” University, 80131 Naples, Italy; and Department of Internal Medicine(R.P., L.J.H., S.W.J.L.), Erasmus Medical Center, Rotterdam 3015 CE, The Netherlands
Background: The role of dopamine agonists in the treatment of Cushing’s disease (CD) has beenpreviously debated.
Aim: The aim of this study was to evaluate the effectiveness of short-term (3 months) and long-term(12–24 months) treatment with cabergoline in patients with CD.
Patients and Methods: 20 patients with CD unsuccessfully treated by surgery entered the study.Cabergoline was administered at an initial dose of 1 mg/wk, with a monthly increase of 1 mg, untilurinary cortisol levels normalized or the maximal dose of 7 mg/wk was achieved. The responsivenessto treatment was evaluated according to changes in urinary cortisol excretion. A decrease greaterthan 25% was considered as a partial response, whereas complete normalization was consideredas a full response at short-term evaluation; persistence of normal cortisol excretion was the onlycriterion to evaluate the response at long-term evaluation.
Results: After short-term treatment, 15 (75%) patients were responsive to cabergoline treatment.Among these, normalization of cortisol excretion was maintained in 10, whereas treatment escapewas observed in five patients after 6–18 months. Among the 10 long-term responsive patients,eight were followed for 24 months, whereas the remaining two were followed for 12–18 months,due to cabergoline withdrawal for intolerance. A sustained control of cortisol secretion for 24month cabergoline treatment at the maximal dose ranging from 1-7 mg/wk (median: 3.5) withoutsignificant side effects, was obtained in eight of 20 (40%) patients.
Conclusions: The results of this study demonstrated that cabergoline treatment is effective incontrolling cortisol secretion for at least 1–2 yr in more than one third of a limited population ofpatients with CD. If this evidence is confirmed by additional studies, this agent may be consideredas a useful treatment option in patients with CD who are unsuccessfully treated by neurosurgery.(J Clin Endocrinol Metab 94: 223–230, 2009)
Cushing’s disease (CD) is the most common form of Cushing’ssyndrome, caused by a corticotroph pituitary tumor, and
often complicated by hypertension and impaired glucose toler-ance and associated with increased morbidity and mortality for
cardiovascular diseases (1–3). The first-line treatment of CD issurgery, with the objective of removing the pituitary tumor, al-though it is effective in inducing immediate disease remission inaround 70% and late disease remission in around 50% of pa-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2009 by The Endocrine Societydoi: 10.1210/jc.2008-1533 Received July 16, 2008. Accepted October 17, 2008.First Published Online October 28, 2008
Abbreviations: CD, Cushing’s disease; HOMA-B, homeostasis model of assessment-!-cellfunction; HOMA-IR, homeostasis model of assessment-insulin resistance; MRI, magneticresonance imaging; PRL, prolactin.
O R I G I N A L A R T I C L E
E n d o c r i n e R e s e a r c h — B r i e f R e p o r t
J Clin Endocrinol Metab, January 2009, 94(1):223–230 jcem.endojournals.org 223
The Medical Treatment of Cushing’s Disease:Effectiveness of Chronic Treatment with theDopamine Agonist Cabergoline in PatientsUnsuccessfully Treated by Surgery
Rosario Pivonello, Maria Cristina De Martino, Paolo Cappabianca, Monica De Leo,Antongiulio Faggiano, Gaetano Lombardi, Leo J. Hofland, Steven W. J. Lamberts,and Annamaria Colao
Departments of Molecular and Clinical Endocrinology and Oncology (R.P., M.C.D.M., M.D.L., A.F., G.L., A.C.),and Neurosurgery (P.C.), “Federico II” University, 80131 Naples, Italy; and Department of Internal Medicine(R.P., L.J.H., S.W.J.L.), Erasmus Medical Center, Rotterdam 3015 CE, The Netherlands
Background: The role of dopamine agonists in the treatment of Cushing’s disease (CD) has beenpreviously debated.
Aim: The aim of this study was to evaluate the effectiveness of short-term (3 months) and long-term(12–24 months) treatment with cabergoline in patients with CD.
Patients and Methods: 20 patients with CD unsuccessfully treated by surgery entered the study.Cabergoline was administered at an initial dose of 1 mg/wk, with a monthly increase of 1 mg, untilurinary cortisol levels normalized or the maximal dose of 7 mg/wk was achieved. The responsivenessto treatment was evaluated according to changes in urinary cortisol excretion. A decrease greaterthan 25% was considered as a partial response, whereas complete normalization was consideredas a full response at short-term evaluation; persistence of normal cortisol excretion was the onlycriterion to evaluate the response at long-term evaluation.
Results: After short-term treatment, 15 (75%) patients were responsive to cabergoline treatment.Among these, normalization of cortisol excretion was maintained in 10, whereas treatment escapewas observed in five patients after 6–18 months. Among the 10 long-term responsive patients,eight were followed for 24 months, whereas the remaining two were followed for 12–18 months,due to cabergoline withdrawal for intolerance. A sustained control of cortisol secretion for 24month cabergoline treatment at the maximal dose ranging from 1-7 mg/wk (median: 3.5) withoutsignificant side effects, was obtained in eight of 20 (40%) patients.
Conclusions: The results of this study demonstrated that cabergoline treatment is effective incontrolling cortisol secretion for at least 1–2 yr in more than one third of a limited population ofpatients with CD. If this evidence is confirmed by additional studies, this agent may be consideredas a useful treatment option in patients with CD who are unsuccessfully treated by neurosurgery.(J Clin Endocrinol Metab 94: 223–230, 2009)
Cushing’s disease (CD) is the most common form of Cushing’ssyndrome, caused by a corticotroph pituitary tumor, and
often complicated by hypertension and impaired glucose toler-ance and associated with increased morbidity and mortality for
cardiovascular diseases (1–3). The first-line treatment of CD issurgery, with the objective of removing the pituitary tumor, al-though it is effective in inducing immediate disease remission inaround 70% and late disease remission in around 50% of pa-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2009 by The Endocrine Societydoi: 10.1210/jc.2008-1533 Received July 16, 2008. Accepted October 17, 2008.First Published Online October 28, 2008
Abbreviations: CD, Cushing’s disease; HOMA-B, homeostasis model of assessment-!-cellfunction; HOMA-IR, homeostasis model of assessment-insulin resistance; MRI, magneticresonance imaging; PRL, prolactin.
O R I G I N A L A R T I C L E
E n d o c r i n e R e s e a r c h — B r i e f R e p o r t
J Clin Endocrinol Metab, January 2009, 94(1):223–230 jcem.endojournals.org 223
ysis calculating the Pearson’s coefficient. Data are expressed as mean ! SE.Significance was set at 5%.
Results
Responsiveness to treatment with cabergolineAt short-term treatment, 15 (75%) patients were responsive
[eight (40%) partial and seven (35%) full responders], whereasfive (25%) were resistant. Cabergoline was withdrawn in allresistant patients, except in one, who continued treatment for 12months. Among the 15 responsive patients, six of the eight (75%)partial responders normalized cortisol levels after 6–12 monthtreatment with increasing cabergoline dose. However, two of theseven (28.6%) full responders and three of the eight (37.5%)partial responders experienced a treatment escape after 12–18month treatment, and stopped treatment. At the 12-month fol-low-up, 10 (50%) patients were persistently controlled at themedian cabergoline dose of 6 mg/wk (1–7 mg/wk). Cabergo-line was discontinued during the second year of follow-up intwo (10%) patients who did not tolerate the treatment be-cause of severe asthenia associated with hypotension. At the24-month follow-up, eight (40%) patients were persistentlycontrolled at a median cabergoline dose of 3.5 mg/wk (1–7mg/wk) (Figs. 1 and 2). In these patients, all multiple urinarycortisol levels were within the normal range, or very close tothe upper limit of the normal range. A flowchart explaining thedisposition of the different patients during the short-term and long-term study and the corresponding outcome of the treatment isshown in Fig. 3. The presence of hyperprolactinemia was signifi-
cantlyassociatedwiththeresponsiveness toshort-term(!2"5.455;P " 0.038), but not long-term (!2 " 5.051; P " 0.070), treatment.
Effectiveness of treatment with cabergoline
Short-term treatment (Table 2)The clinical picture improved in the majority of responsive
patients, whereas it mildly improved, remained stable, ormildly worsened in resistant patients. Despite a mild increaseof body mass index, waist to hip ratio significantly decreased,as well as blood pressure, serum glucose and insulin, HOMA-IR, and tumor volume. Systolic and diastolic blood pressuresignificantly decreased in resistant patients as well, whereasHOMA-B did not change both in responsive and resistancepatients. PRL levels were lower than the normal range in allpatients.
Long-term treatmentResponsive patients (Table 3). The clinical picture further im-proved during treatment. Body mass index slightly increasedduring the first 3–6 months, but significantly decreased there-after, whereas waist to hip ratio progressively decreased. Theprevalence of overweight or obesity decreased from 87.5% atbaseline to 62.5% at the 24-month treatment. The distributionof fat mass was modified from an abdominal to a generalizedpattern in the majority of patients. Muscle mass and strength aswell as skin features slightly or significantly improved in themajority of patients. Systolic and diastolic blood pressure valuessignificantly decreased, becoming stable after 6–12 month treat-ment. The prevalence of hypertension decreased from 50% at
0 3 6 9 12 15 18 21 24
0
250
500
750
1000
months
urin
ary
cort
isol
leve
ls( µ
g/da
y)
FIG. 1. Urinary cortisol levels during the entire period of treatment in all 20 patients treated with cabergoline. The patients long-term response to cabergolinetreatment are shown with black lines, those with early response and late escape are shown with purple lines, and those nonresponders to the treatment areshown with red lines. The shaded area indicates the normal range of urinary cortisol levels (35–135 "g/d). Urinary cortisol levels represent the mean of threedifferent urine collections performed on three different nonconsecutive days of the same week.
226 Pivonello et al. Cabergoline Treatment in CD J Clin Endocrinol Metab, January 2009, 94(1):223–230
Eight out of 20 patients normalized their cortisol

Effectiveness of cabergoline in monotherapy and combinedwith ketoconazole in the management of Cushing’s disease
Lucio Vilar • Luciana A. Naves • Monalisa F. Azevedo • Maria Juliana Arruda •
Carla M. Arahata • Lidiane Moura e Silva • Rodrigo Agra • Lisete Pontes •
Larissa Montenegro • Jose Luciano Albuquerque • Viviane Canadas
Published online: 27 November 2009! Springer Science+Business Media, LLC 2009
Abstract The expression of dopamine receptor subtypeshas been reported in corticotroph adenomas, and this
finding support the possibility for medical treatment of
Cushing’s disease (CD) with dopamine agonists whenconventional treatment has failed. The aim of this study
was to evaluate the effectiveness of cabergoline (at doses
of up 3 mg/week), alone or combined with relatively lowdoses of ketoconazole (up to 400 mg/day), in 12 patients
with CD unsuccessfully treated by transsphenoidal surgery.
After 6 months of cabergoline therapy, normalization of24 h urinary free cortisol (UFC) levels occurred in three
patients (25%) at doses ranging from 2–3 mg/week,
whereas reductions ranging from 15.0 to 48.4% were foundin the remaining. The addition of ketonocazole to the nine
patients without an adequate response to cabergoline was
able to normalize UFC excretion in six patients (66.7%) atdoses of 200 mg/day (three patients), 300 mg/day (two
patients) and 400 mg/day (one patient). In the remaining
patients UFC levels did not normalize but a significant
reduction ranging from to 44.4 to 51.7% was achieved. Intwo of the six responsive patients to combination therapy,
the weekly dose of cabergoline could be later reduced from
3 to 2 mg. Our findings demonstrated that cabergolinemonotherapy was able to reverse hypercortisolism in 25%
of patients with CD unsuccessfully treated by surgery.
Moreover, the addition of relatively low doses of keto-conazole led to normalization of UFC in about two-thirds
of patients not achieving a full response to cabergoline.
Keywords Cushing’s disease ! Cabergoline !Ketoconazole
Introduction
Cushing’s disease (CD), the most common form of
endogenous Cushing’s syndrome, is caused by an ACTH-secreting pituitary tumor and is associated with increased
morbidity and mortality particularly due to metabolic and
cardiovascular complications [1–3]. The treatment ofchoice for CD is transsphenoidal surgery (TSS) which
yields immediate disease remission in about 70% ofpatients but the late disease remission rate is around 50%
[4, 5]. Pituitary irradiation [6] and bilateral adrenalectomy
[7] are alternative treatment approaches but they can beassociated with serious complications, such as hypopitu-
itarism and Nelson’s syndrome, respectively [4, 5].
There is currently no medical therapy for CD that targetsthe pituitary adenoma. Pharmacotherapy, particularly
ketoconazole (an adrenal blocking drug), is rather used
before surgery or as a transient palliative treatment beforedefinitive cure in patients submitted to pituitary radio-
therapy [4, 8]. There are also few reports of successful
primary therapy with ketoconazole in patients that refused
L. Vilar ! M. J. Arruda ! C. M. Arahata ! L. Moura e Silva !R. Agra ! L. Pontes ! L. Montenegro ! J. L. Albuquerque !V. CanadasDivision of Endocrinology, Hospital das Clınicas, FederalUniversity of Pernambuco, Recife, Brazil
L. VilarPernambuco Center for Diabetes and Endocrinology, FederalUniversity of Pernambuco, Recife, Brazil
L. A. Naves ! M. F. AzevedoDivision of Endocrinology, Hospital Universitario de Brasilia,Brasilia, Brazil
L. Vilar (&)Rua Clovis Silveira Barros, 84/1202, Boa Vista, Recife CEP50.050-270, Brazile-mail: [email protected]
123
Pituitary (2010) 13:123–129
DOI 10.1007/s11102-009-0209-8
Cabergoline alone
Statistical analysis
In the analysis of qualitative variables, the v2 test or theFisher exact test (when necessary) was used. The Student
t-test was performed for the comparative analysis of
quantitative variables. Results are expressed as percent-ages and mean values ± SD unless otherwise indicated.
P values\0.05 were considered statistically significant.
Results
Responsiveness to treatment with cabergoline
Comparing the last value during cabergoline monotherapywith baseline (Table 1), mean ± SD UFC levels decreased
from 637.8 ± 245.7 (range 226–991) lg/day to 434.1 ±
256.8 (range 82–791) lg/day (P\ 0.001). Normalizationof UFC levels occurred in three patients (25%) at caberg-
oline doses ranging from 2 to 3 mg/week (mean ± SD,
2.5 ± 0.5), whereas reductions ranging from 15.0 to 48.4%were found in the remaining. Three patients were labeled
as resistant to cabergoline (UFC decrease\25%). In two
patients, the normalization of UFC excretion was achievedat the dose of 2 mg/week (Table 1) (Fig. 1).
Regardless the UFC normalization, all patients reported
improvement of clinical symptoms during the treatmentwith cabergoline.
Responsiveness to treatment with cabergolineand ketoconazole
The addition of ketonocazole, at doses ranging from 200
to 400 mg/day (mean ± SD, 325 ± 103.5), to the nineTable
1Characteristicsofthepatients
andtheirresponse
tothetreatm
entwithcabergoline(CAB)
Patients
Age/
sex
IHC
CABdose
(mg/week)
Durationoftreatm
ent
(months)
UFC
norm
alization
UFC
reduction(%
)UFCbefore
CAB(lg/d)
UFCafter
CAB(lg/d)
Baseline
PRL
No.1
34/F
ACTH
(?)
2.0
6Yes
66.7
226
82
Nl
No.2
37/F
ACTH
(?)
2.0
6Yes
68.6
280
88
Nl
No.3
40/F
ACTH
(?)
3.0
6Yes
77.6
368
82.5
Nl
No.4
47/M
ACTH
(?)
3.0
6No
34.6
523
342
Nl
No.5
43/M
ACTH
(?)
3.0
6No
37.4
591
370
Nl
No.6
44/M
ACTH
(?)
3.0
6No
48.4
680
351
Nl
No.7
52/M
ACTH
(?)
3.0
6No
26.4
735
541
Nl
No.8
38/F
ACTH
(?)
3.0
6No
26.1
720
532
Nl
No.9
51/F
ACTH
(?)
3.0
6No
26.5
792
582
Nl
No.10
48/F
ACTH
(?)
3.0
6No
19.2
882
712
Nl
No.11
46/F
ACTH
(?)
3.0
6No
15.0
866
736
Nl
No.12
34/F
ACTH
(?)
3.0
6No
20.2
991
791
Nl
IHC
immunohystochemistry,PRLprolactin,Nlnorm
al
Urinary
freecortisol(U
FC)norm
alrange=
10–90lg/day
Fig. 1 Changes in 24 h urinary free cortisol levels after treatmentwith cabergoline. The number on each arrow indicates the maximaldose of cabergoline expressed in mg/week administered to eachpatient
Pituitary (2010) 13:123–129 125
123
patients without a full response to cabergoline yielded a
mean ± SD UFC levels decrease from 520.7 ± 156.1(range 342–791) lg/day to 149.6 ± 124.1 (range 72–385)
lg/day (P\ 0.001). Normalization of UFC levels were
achieved at doses of 200 mg/day in three patients, 300 mg/day in two patients and 400 mg/day in one patient. In the
remaining patients UFC levels could not be normalized but
a significant reduction ranging from to 44.4 to 51.7% wasachieved (Table 2) (Fig. 2). As shown in Table 2, UFC
levels in patients that did not respond to combinationtherapy was significantly higher than those of responsive
patients: 746.3 ± 40.5 (range 712–791) lg/day versus
453 ± 109.7 (range 342–582) lg/day (P\ 0.001). Bycontrast, there was no correlation between the response to
treatment and PRL levels (normal in all patients) or the
expression of PRL by immunohystochemistry (negative inall subjects). In two out of the six responsive patients to
combined therapy, the weekly dose of CAB could be later
reduced from 3 to 2 mg without elevation UFC levelsbeyond the upper limit of the normal range.
Overall, normalization of daily UFC excretion could be
obtained in nine patients (75%), three (25%) submitted tocabergoline monotherapy and in six (66.7%) undergoing
the combination of cabergoline with ketoconazole. The
response was not infleuTreatment escape, manifested asrelapse of hypercortisolism and elevation of UFC levels
during the use of cabergoline alone or combination therapy,
was not observed in any patient.
Tolerability
Cabergoline and ketoconazole were well tolerated and
none of the patients had to interrupt the treatment. Tran-
sient moderate dizziness and/or nausea were reported bythree patients treated with cabergoline. After the addition
of ketoconazole, mild transient elevation of transaminaseswas found in one out of nine patients (11.1%). No patients
developed symptoms of hypoglycemia while on cabergo-
line or combined therapy. Moreover, none of the patientsexperienced any significant symptom or sign related to
cardiac disease; particularly, no patients developed cardiac
valve regurgitation.
Discussion
Unlike prolactinomas and acromegaly, currently there is
not an effective medication to treat Cushing’s disease thatacts at the level of the pituitary gland inhibiting ACTH
secretion by the corticotroph tumor [1, 2]. Some neuro-
modulatory drugs were used in the past, however, due to
Table 2 Characteristics of the patients and their response to the treatment with cabergoline (CAB) ? ketoconazole (KTCZ)
Patients CAB dose(mg/wk)
KTCZ dose(mg/d)
Duration oftreatment(months)
UFCnormalization
UFCreduction(%)
UFC beforeKTCZ (lg/d)
UFC afterKTCZ (lg/d)
No. 4 3.0 200 6 Yes 75.1 342 85
No. 5 3.0 200 6 Yes 76 370 89
No. 6 3.0 200 6 Yes 74.3 351 90
No. 7 3.0 300 6 Yes 86.7 541 72
No. 8 3.0* 300 6 Yes 85.3 532 78
No. 9 3.0* 400 6 Yes 85.2 582 86
No. 10 3.0 400 6 No 44.4 712 316
No. 11 3.0 400 6 No 51.7 736 381
No. 12 3.0 400 6 No 48.7 791 385
In patients No. 8 and 9 the dose of cabergoline could be later reduced to 2 mg/week
Urinary free cortisol (UFC) normal range = 10–90 lg/day
Fig. 2 Changes in 24 h urinary free cortisol levels after treatmentwith cabergoline and ketoconazole. The number on each arrowindicates the maximal dose of ketoconazole expressed in mg/dayadministered to each patient
126 Pituitary (2010) 13:123–129
123
Cabergoline plus KetoconazoleEffectiveness of cabergoline in monotherapy and combinedwith ketoconazole in the management of Cushing’s disease
Lucio Vilar • Luciana A. Naves • Monalisa F. Azevedo • Maria Juliana Arruda •
Carla M. Arahata • Lidiane Moura e Silva • Rodrigo Agra • Lisete Pontes •
Larissa Montenegro • Jose Luciano Albuquerque • Viviane Canadas
Published online: 27 November 2009! Springer Science+Business Media, LLC 2009
Abstract The expression of dopamine receptor subtypeshas been reported in corticotroph adenomas, and this
finding support the possibility for medical treatment of
Cushing’s disease (CD) with dopamine agonists whenconventional treatment has failed. The aim of this study
was to evaluate the effectiveness of cabergoline (at doses
of up 3 mg/week), alone or combined with relatively lowdoses of ketoconazole (up to 400 mg/day), in 12 patients
with CD unsuccessfully treated by transsphenoidal surgery.
After 6 months of cabergoline therapy, normalization of24 h urinary free cortisol (UFC) levels occurred in three
patients (25%) at doses ranging from 2–3 mg/week,
whereas reductions ranging from 15.0 to 48.4% were foundin the remaining. The addition of ketonocazole to the nine
patients without an adequate response to cabergoline was
able to normalize UFC excretion in six patients (66.7%) atdoses of 200 mg/day (three patients), 300 mg/day (two
patients) and 400 mg/day (one patient). In the remaining
patients UFC levels did not normalize but a significant
reduction ranging from to 44.4 to 51.7% was achieved. Intwo of the six responsive patients to combination therapy,
the weekly dose of cabergoline could be later reduced from
3 to 2 mg. Our findings demonstrated that cabergolinemonotherapy was able to reverse hypercortisolism in 25%
of patients with CD unsuccessfully treated by surgery.
Moreover, the addition of relatively low doses of keto-conazole led to normalization of UFC in about two-thirds
of patients not achieving a full response to cabergoline.
Keywords Cushing’s disease ! Cabergoline !Ketoconazole
Introduction
Cushing’s disease (CD), the most common form of
endogenous Cushing’s syndrome, is caused by an ACTH-secreting pituitary tumor and is associated with increased
morbidity and mortality particularly due to metabolic and
cardiovascular complications [1–3]. The treatment ofchoice for CD is transsphenoidal surgery (TSS) which
yields immediate disease remission in about 70% ofpatients but the late disease remission rate is around 50%
[4, 5]. Pituitary irradiation [6] and bilateral adrenalectomy
[7] are alternative treatment approaches but they can beassociated with serious complications, such as hypopitu-
itarism and Nelson’s syndrome, respectively [4, 5].
There is currently no medical therapy for CD that targetsthe pituitary adenoma. Pharmacotherapy, particularly
ketoconazole (an adrenal blocking drug), is rather used
before surgery or as a transient palliative treatment beforedefinitive cure in patients submitted to pituitary radio-
therapy [4, 8]. There are also few reports of successful
primary therapy with ketoconazole in patients that refused
L. Vilar ! M. J. Arruda ! C. M. Arahata ! L. Moura e Silva !R. Agra ! L. Pontes ! L. Montenegro ! J. L. Albuquerque !V. CanadasDivision of Endocrinology, Hospital das Clınicas, FederalUniversity of Pernambuco, Recife, Brazil
L. VilarPernambuco Center for Diabetes and Endocrinology, FederalUniversity of Pernambuco, Recife, Brazil
L. A. Naves ! M. F. AzevedoDivision of Endocrinology, Hospital Universitario de Brasilia,Brasilia, Brazil
L. Vilar (&)Rua Clovis Silveira Barros, 84/1202, Boa Vista, Recife CEP50.050-270, Brazile-mail: [email protected]
123
Pituitary (2010) 13:123–129
DOI 10.1007/s11102-009-0209-8
Pituitary Adrenal Axis
Surgery PaseriotideCabergoline
SurgeryKetoconazoleMetyraponeEtomidateLCI699
MifepristoneY
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn IIIFn III
Fn III
Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Insulin
SSS
S
SS
Insulin
SSS
S
SS
PI3K
JAK2
Ins Ins-R
GHRs
IGF-I
During co-treatment with SSAs, PEG (being a competitive GHR blocker) has less GH to compete with, and less GHRs to block on the liver. Moreover, SSAs inhibit IGF-1 generation by liver directly
Leung et al. JCEM 2000
Murray RD et al. JCI 2004
SSAs, decreasing portal insulin concentration, may reduce the number of GHRs expressed in the liver, and may also directly inhibit liver IGF-1 generation

Mifepristone
• Glucocorticoid receptor (GR) antagonist blocks the action of cortisol by binding to the GR-II (cortisol) receptor – 3–4-fold higher affinity than dexamethasone – 18-fold higher affinity than cortisol
• In Phase III clinical development as a treatment for endogenous Cushing’s syndrome Screening
42 days 24-week treatment
Day 1 Week 6 Week 10 Week 16 Week 24
n=50 enrolled
n=84 screened
Dose escalation until week 10
n=34 completed
Fleseriu M et al. Endocr Rev 2011;32:OR09-5

Mifepristone in Cushing’s disease: Conclusions
• Mifepristone treatment was associated with clinical improvements in patients with refractory Cushing’s syndrome – Glucose tolerance and hypertension improved in 60% and 38%,
respectively – Body weight decreased by an average of 5.7 kg – Waist circumference decreased by an average of 7 cm
in women and 8 cm in men
• However, mifepristone blocks the glucocorticoid receptor rather than targeting the underlying cause of Cushing’s disease
• Increases in ACTH and UFC levels were observed on mifepristone treatment

Pituitary Adrenal Axis
Surgery PaseriotideCabergoline
SurgeryKetoconazoleMetyraponeEtomidateLCI699
MifepristoneY
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn II
I
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn II
I
Fn III
Fn II
I
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
GrowthHormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Growth
Hormone
Y
Y
Y
Y
PPPP
Fn III
Fn III
Fn III
Fn III
Y
Y
Y
Y
Y
PP
Fn III
Fn III
Y
Y
Y
Y
Y
PPPP
Fn III
Fn IIIFn III
Fn III
Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150Y1146
Y1151
Y960
Y1316
Y1322
Kinase
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Y
Y
Y9
Y1
Y1
Kina
se
Y1150
Insulin
SSS
S
SS
Insulin
SSS
S
SS
PI3K
JAK2
Ins Ins-R
GHRs
IGF-I
During co-treatment with SSAs, PEG (being a competitive GHR blocker) has less GH to compete with, and less GHRs to block on the liver. Moreover, SSAs inhibit IGF-1 generation by liver directly
Leung et al. JCEM 2000
Murray RD et al. JCI 2004
SSAs, decreasing portal insulin concentration, may reduce the number of GHRs expressed in the liver, and may also directly inhibit liver IGF-1 generation

Pasireotide
• Multireceptor-targeted somatostatin analogue – 30-, 5- and 39-fold higher affinity for sst1, sst3 and
sst5 than octreotide, and similar affinity for sst21
• Expression of sst5 predominates in ACTH-secreting pituitary adenomas2,3
– sst1, sst2 and sst3 are also expressed
• Broad binding profile means that pasireotide may be an effective treatment for Cushing’s disease
N H
O
N H
O N
O
O N H
N H
N H
N H N H
O
O
O O
N H 2
O
N H 2
1. Bruns C et al. Eur J Endocrinol 2002;146:707–716 2. Strowski MZ et al. Neuroendocrinology 2002;75:339–346
3. Sharma K et al. Mol Endocrinol 1999;13:82–90

2500
Change in UFC from baseline to month 6 in the 103 patients with baseline and month-6 UFC measurements
Individual patients sorted by baseline UFC
UFC
(�g/
24 h
)
0
180
360
540
720
1400
600 µg bid
900 µg bid
ULN†
Baseline UFC Month-6 UFC Month-6 UFC �ULN *
†Reference line is the upper limit normal UFC, which is 52.5 �g/24 h (145 nmol/24 h)
Median percentage UFC change from baseline was –47.9% in both groups

Response status
600 µg bid (n=82)
900 µg bid (n=80)
Overall (n=162)
6-month response, n (%)* 12 (14.6) 21 (26.3) 33 (20.4)
95% confidence interval (7.0, 22.3) (16.6, 35.9) (14.2, 26.6)
12-month response, n (%)† 11 (13.4) 20 (25.0) 31 (19.1)
Primary efficacy results
Predetermined criterion for the primary efficacy endpoint: lower bound of the 95% CI >15% for either of the dose groups;
this was met for the 900 µg group
*NOTE: Responder was a patient with UFC ������������ ���������uptitration
†NOTE: Responder was a patient with UFC �����irrespective of uptitration
LCI699
1Menard J et al. J Am Coll Cardiol 2010;55:A61.E583
Highly potent inhibitor of 11β-hydroxylase (Three times more potent then metyrapone for inhibiting 11β-hydroxylase Also inhibits aldosterone synthase

LCI699 mechanism of action
Pregnenolone
11-deoxycortisol
Cortisol
17-OH pregnenolone
17-OH progesterone
Cholesterol
ACTH
Aldosterone
CYP11B
2
Corticosterone
18-OH corticosterone
LCI699
CYP11B1 LCI699
Feedback loop malfunctioning in Cushing’s
Progesterone
Dehydroepiandrosterone
Androstenedione
Testosterone
11-deoxycorticosterone
Estradiol
Estrone
Potent inhibitor of 11β-hydroxylase (CYP11B1) and aldosterone synthase (CYP11B2)Blocks last steps in cortisol and aldosterone production
• It is administered orally and it displays a half-life longer than metyrapone, allowing twice-daily dosing
• It has a three times higher potency (in vitro IC50 for CYP11B1 ���of 2.5 nM vs 7.5 nM) than metyraponeIC50, half maximal inhibitory concentration
X
X
11-deoxycortisol
ACTH
Testosterone
11-deoxycorticosterone
Pivonello R. et al. Oral presentation OR17-4 ENDO 2014, Chicago, IL, USA, June 22, 2014 14MDL160E July 5th, 2014

LCI699 early study Inclusion
Male or female patients aged 18–75 years Confirmed Cushing’s disease UFC >1.5x ULN (mean of three 24-hour urine samples) No other current medical treatment for Cushing’s disease
Exclusion Tumour with chiasmal compression Poorly controlled diabetes (HbA1c >9%)
HbA, hemoglobin A; ULN, upper limit of normal
Pivonello R et al. Endocr Rev 2012;33:abst OR49-1 14MDL160E July 5th, 2014
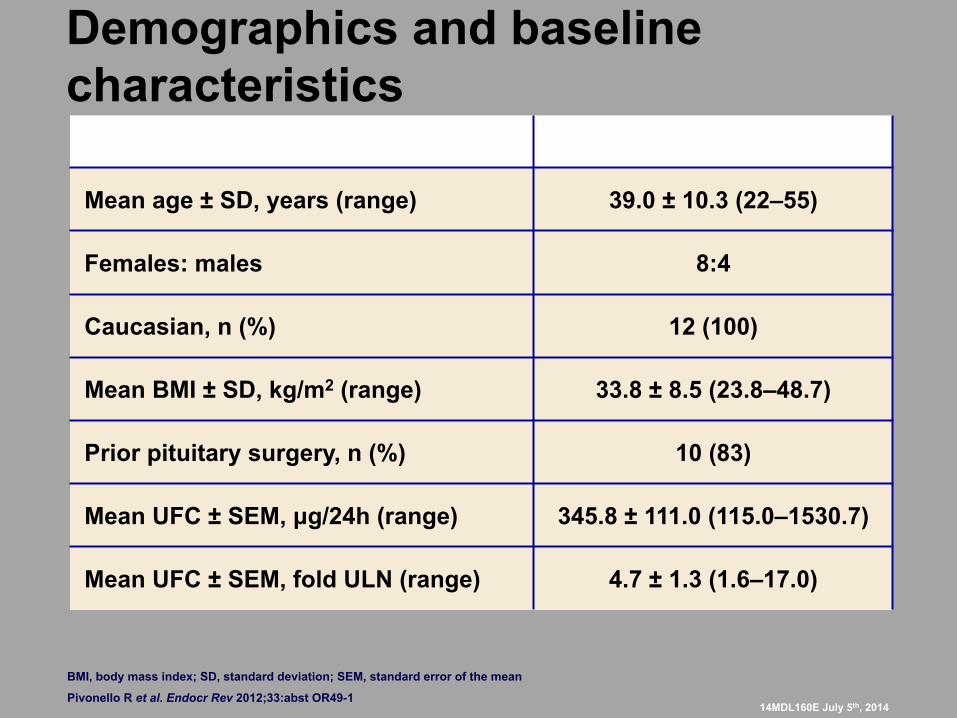
Demographics and baseline characteristics
Patients (N=12)
Mean age ± SD, years (range) 39.0 ± 10.3 (22–55)
Females: males 8:4
Caucasian, n (%) 12 (100)
Mean BMI ± SD, kg/m2 (range) 33.8 ± 8.5 (23.8–48.7)
Prior pituitary surgery, n (%) 10 (83)
Mean UFC ± SEM, µg/24h (range) 345.8 ± 111.0 (115.0–1530.7)
Mean UFC ± SEM, fold ULN (range) 4.7 ± 1.3 (1.6–17.0)
Pivonello R et al. Endocr Rev 2012;33:abst OR49-1
BMI, body mass index; SD, standard deviation; SEM, standard error of the mean
14MDL160E July 5th, 2014

Urinary cortisol over time in all patients
Mea
n U
FC ±
SEM
(fol
d U
LN)
0
1
2
3
4
5
6
7
1 14 28 42 56 70 84
Day
LCI699 dose escalation Washout
All 12 patients had normalized UFC or >50% reduction in UFC by day 70 – 11/12 (92%) had normal 24-hour UFC at day 70 – Urinary cortisol normalized at least once in all 12 patients
Pivonello R et al. Endocr Rev 2012;33:abst OR49-1

LCI699 doses required to normalize UFC
The doses most frequently associated with 24-hour UFC normalization were 10 and 20 mg/day
0
1
2
3
4
5
6
<10 10 20 30 40 100Dose (mg/day)
Patie
nts
(n)
Pivonello R et al. Endocr Rev 2012;33:abst OR49-1 14MDL160E July 5th, 2014

Changes in clinical and laboratory features during LCI699 treatment
Baseline (n=12)
Day 70 (n=12)
Change from baseline (n=12)
SBP, mmHg 139.3 ± 4.4 129.3 ± 5.5 –10.0 ± 4.3
DBP, mmHg 88.8 ± 3.8 82.8 ± 3.0 –6.0 ± 4.3
Weight, kg 96.8 ± 8.8 100.3 ± 9.5 3.5 ± 1.4
Glucose, mmol/L 5.4 ± 0.5 5.7 ± 0.4 0.3 ± 0.3
Potassium, mEq/L 4.1 ± 0.1 3.8 ± 0.2 –0.3 ± 0.2
Sodium, mEq/L 140.3 ± 1.1 140.8 ± 1.0 0.5 ± 1.1
Pivonello R et al. Endocr Rev 2012;33:abst OR49-1
NOTE: Data presented as mean ± SEM DBP, diastolic blood pressure; SBP, systolic blood pressure
14MDL160E July 5th, 2014

LINC 1: Most common AEs* during treatment with LCI699 (occurring in at least two patients)
Patients, n (%) Fatigue 7 (58.3) Nausea 5 (41.6) Diarrhea 3 (25.0) Headache 3 (25.0) Hypokalemia 3 (25.0) Muscle spasms 3 (25.0) Vomiting 3 (25.0) Abdominal discomfort 2 (16.6) Abdominal pain 2 (16.6) Arthralgia 2 (16.6) Arthropod bite 2 (16.6) Dizziness 2 (16.6) Lipase increased 2 (16.6) Pruritus 2 (16.6)
*Assessed based on MedDRA definitions Pivonello R et al. Endocr Rev 2012;33:abst OR49-1 14MDL160E July 5th, 2014

Mitotane, Etomidate and Metyrapone
These drugs are only used in malignant cortisol producing tumours of the adrenal gland Long-term use of these agents in ACTH producing pituitary tumours is NOT indicated.

Amy’s case
- Underwent surgery - In remission since then - Lost over 75 lbs - BP normal - Working as a nurse

Watercolor – Fall River, NS S. Ali Imran, 2011













![Cushing’s disease: current trends in treatment - Open Access … · 2019-07-12 · pituitary adenoma (Cushing’s disease [CD]) or an ectopic tumor [1]. CD is responsible for 80–90%](https://img.pdfslide.net/doc/110x75/5e6162aac277d3606a6e5a7f/cushingas-disease-current-trends-in-treatment-open-access-2019-07-12-pituitary.jpg)