Embed Size (px)
Citation preview

1
Clinical Application ofQualitative and QuantitativeDietary Methods
Melissa Armstrong, APD, CDESt Vincent’s Hospital Diabetes CentreJenny McQueen, AdvAPDSWAHS community dietitian
Overview
♦RDIs & NRVs♦Food guides♦Qualitative & Quantitative assessment of dietary
intake♦Break
♦Case studies♦Discussion
Next week….Quantitative assessment with Ready Reckoners
Medical Nutrition Therapy
♦ Assessment Medical Dietary intake Psychosocial Physical Activity
♦ Education/treatment: prescription
• energy, nutrients (macro & micro), fibre and fluid implementation
• diet plan/ provision of diet (in hospital)• strategies• practical issues
♦ Monitoring & evaluation and of outcomes
Clinical Situations - location
♦Hospital settings Wards Outpatient department
♦Outpatient facility Diabetes Centre Community Health Centre Private practice rooms
♦Client’s home
♦Aged care facilities
Clinical Situations - format
♦The aim of the intervention is to ensure the patient’sdietary intake is “adequate” for their individualrequirements
♦May include interventions via: Group education One-to-one counseling
How do we assess “adequacy”?
♦Start with a dietary assessment of the individual
♦Compare this to a criteria specifically determined tomeasure suitability of intake
What is a balanced diet? – not “a bit ofeverything”, but enough of everything from eachfood group
What is an adequate diet? – meets energy &nutrient (macro/micro) requirements
2
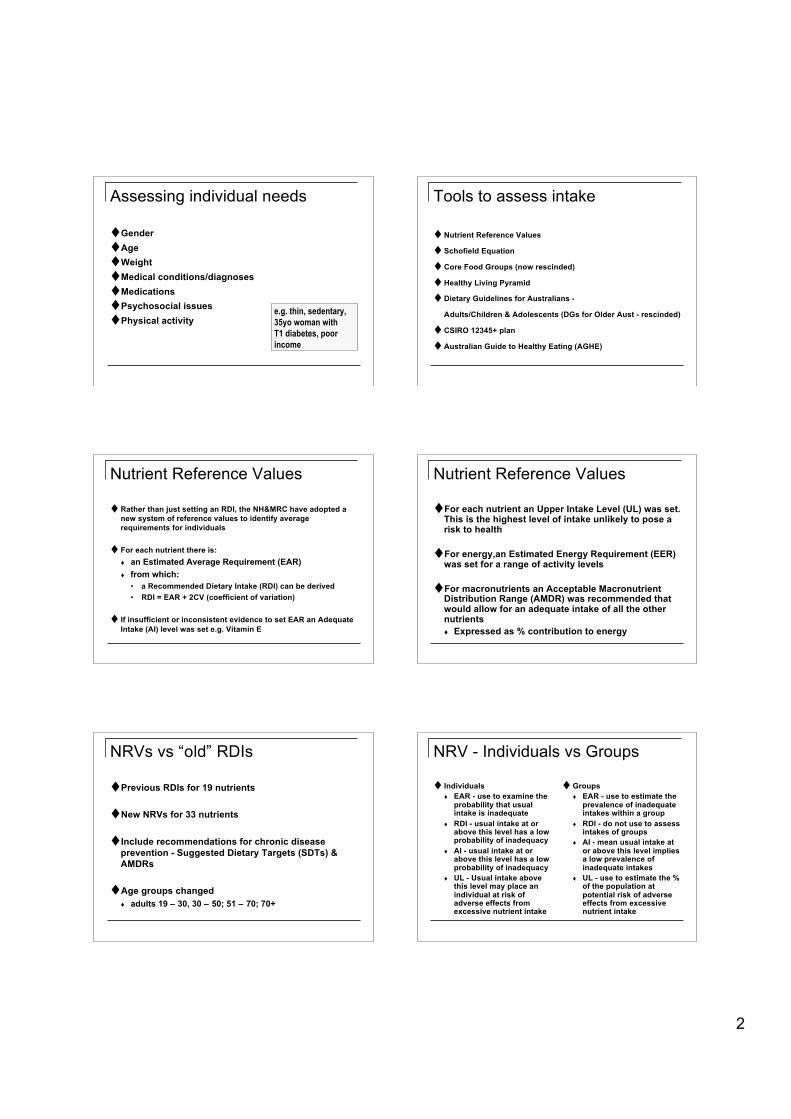
Assessing individual needs
♦Gender♦Age♦Weight♦Medical conditions/diagnoses♦Medications♦Psychosocial issues♦Physical activity
e.g. thin, sedentary,35yo woman withT1 diabetes, poorincome
Tools to assess intake
♦Nutrient Reference Values
♦ Schofield Equation
♦Core Food Groups (now rescinded)
♦Healthy Living Pyramid
♦Dietary Guidelines for Australians -
Adults/Children & Adolescents (DGs for Older Aust - rescinded)
♦CSIRO 12345+ plan
♦Australian Guide to Healthy Eating (AGHE)
Nutrient Reference Values
♦Rather than just setting an RDI, the NH&MRC have adopted anew system of reference values to identify averagerequirements for individuals
♦ For each nutrient there is: an Estimated Average Requirement (EAR) from which:
• a Recommended Dietary Intake (RDI) can be derived• RDI = EAR + 2CV (coefficient of variation)
♦ If insufficient or inconsistent evidence to set EAR an AdequateIntake (AI) level was set e.g. Vitamin E
Nutrient Reference Values
♦For each nutrient an Upper Intake Level (UL) was set.This is the highest level of intake unlikely to pose arisk to health
♦For energy,an Estimated Energy Requirement (EER)was set for a range of activity levels
♦For macronutrients an Acceptable MacronutrientDistribution Range (AMDR) was recommended thatwould allow for an adequate intake of all the othernutrients Expressed as % contribution to energy
NRVs vs “old” RDIs
♦Previous RDIs for 19 nutrients
♦New NRVs for 33 nutrients
♦Include recommendations for chronic diseaseprevention - Suggested Dietary Targets (SDTs) &AMDRs
♦Age groups changed adults 19 – 30, 30 – 50; 51 – 70; 70+
NRV - Individuals vs Groups
♦ Individuals EAR - use to examine the
probability that usualintake is inadequate
RDI - usual intake at orabove this level has a lowprobability of inadequacy
AI - usual intake at orabove this level has a lowprobability of inadequacy
UL - Usual intake abovethis level may place anindividual at risk ofadverse effects fromexcessive nutrient intake
♦Groups EAR - use to estimate the
prevalence of inadequateintakes within a group
RDI - do not use to assessintakes of groups
AI - mean usual intake ator above this level impliesa low prevalence ofinadequate intakes
UL - use to estimate the %of the population atpotential risk of adverseeffects from excessivenutrient intake

3
Use of NRVs
♦Can be difficult to accurately assess “usual intake”
♦When the AI is based on median intakes of healthypopulations, the assessment of “adequacy” is madewith less confidence
♦UL - Upper Limit of IntakeUsually not occurring through food intake - butthrough inappropriate supplementation
Use of NRVs
♦For individuals Moving towards the SDTs & below the ULs makes a lot
of sense!
♦For groups Using the AI is OK or placing the curve of intakes
between EAR & UL looks “right”
♦Accept that the scientific basis of the NRVs is not asstrong as we might wish!!
Chronic Disease Prevention
♦AMDR: Acceptable Macronutrient Distribution Range Estimated range of intake of macronutrients which
provide adequate intakes whilst maximising generalhealth outcomes
♦SDT: Suggested Dietary Target Daily average intake from food and beverages for
certain nutrients that may help in prevention of chronicdisease
NOTE: these AMDRs and SDTs apply only to adultsand adolescents >/= 14yrs
Food Guides
Evolved over time….
♦Five Food Groups
♦Dietary guidelines for Australians
♦Healthy Living Pyramid
♦CSIRO 12345+ guide (1991-2005)
♦Australian Guide to Healthy Eating (2003)

4
Food Guides
♦ Aim: simple guide for healthy eating
♦ Uses: Health promotion & chronic disease prevention
• Nutrient-focused recommendations expressed in terms of foodchoices
• Modeled to assist food choice & national teaching tool(consistent message)
Clinical setting• Basis for assessment & education tool• Basis for simple dietary modifications• Framework for therapeutic objectives• Often used in group education programs
Food Guides
♦help consumers put dietary guidelines into a healthyeating pattern
♦emphasises proportions
♦flexibility – many different foods; age groups;cultural preferences; cost; availability
♦balance – variety of foods

5
Food Guides - limitations
♦New NRVs make previously used food guidesobsolete♦Changes in the food supply and current public
health issues also make old models inappropriate♦Example 1: AGHE - the current recommended
number of meat & alternatives serves fail to meetcurrent EARs for iron, Zn, vitamin B12 & omega 3 fain some people♦Example 2: AGHE - the “extras” group are actually
major contributors to dietary intakes of someessential fatty acids, vitamins D & E
Food Guides - limitations
♦Complex dietary modelling is now possible, enabling moreaccurate guides to be developed
♦ Some issues… devising a separate food guide for vegetarians or pregnant
women Should legumes be positioned with meat or vegetables? Do we need a “healthy fats” group? Are 5 food groups enough? Check reasons for decisions
made for the AGHE & NRVs - NHMRC website Check reasons for decisions made for the AGHE & NRVs -
NHMRC website
The future?
♦Federal budget 2007
Food guide to support the new NRVs
National Nutrition Survey
Food Guides - Limitations
♦Refs: Gillen LJ, Tapsell LC. Development of food groupings to
guide dietary advice for people with diabetes. Nutr Diet 2006;63: 36-47.
Shrapnel B, Baghurst K. Adequacy of fatty acid, vitamin Dand vitamin E intake: Implications for the ‘core’ and ‘extras’food group concept of the Australian Guide to HealthyEating. Nutr Diet 2007: 64: 78-85.
Shrapnel B, Baghurst K. Lack of nutritional equivalence inthe “meat and alternatives” group of the Australian Guide toHealthy Eating. Nutr Diet 2007: 64: 254-260.
Rangan A, Hector D, Randall D, Gill T, Webb K. Monitoringconsumption of “extra” foods in the Australian diet:Comparing two sets of criteria for classifying foods asextras. Nutr Diet 2007: 64: 261-267.
Adequate diet - definition
♦meets all the nutritional needs of an individual formaintenance, repair, living processes, growth &development
♦provides energy & all nutrients in proper amounts
♦reduces the risk of developing chronic degenerativediseases & conditions
Qualitative vs Quantitative
♦Qualitative Assessment of Intake Looking at the overall QUALITY of the diet
• i.e. comparing intake to a general measure of appropriateintake e.g. Core Food Groups
• e.g. health promotion/public health approach;general/brief overview of diet
♦Quantitative Assessment of Intake Looking at the measurable QUANTITY of the diet
• i.e. ensuring an absolute quantity is being provided• e.g. Computerised nutrient analysis or using Ready
Reckoner to check amount ingested/provided/prescribed

6
Assessing Nutrition Adequacy
What do you need to ask…?
Qualitative (quality / type)
How many serves/day, size of serve Food type: lean vs fatty meat, type of added
fat, high vs low fibre cereal products,cooked vs salad vegetables, etc
When would you use thismethod?
Assessing Nutrition Adequacy
What do you need to calculate…?
• Quantitative (quantity / HOW MUCH) Be specific re food items:
150g meat/fish/chicken, 2 tsp of fat, 1/2 cup peas,200 ml of supplement, etc
Then calculate: Energy – e.g. 5000kJ (1200kcal) Nutrients – e.g. 60g protein, 50 mmol K+, 5ug of
folate, 25g fibre
When would you use this method?
Ways to assess intake
♦Qualitative Healthy Eating
Pyramid Dietary Guidelines for
Australians CSIRO 12345+ plan
♦Quantitative Nutrient Reference
Values Schofield Equation CSIRO 12345+ plan AGHE
e.g. Diet Hx & discussion of class volunteer
Assessing Nutrition Adequacy -individualsGeneral Nutrition:♦Meet AMDR
energy (P/F/CHO)
♦Meet RDI for: nutrients fluid fibre
Therapeutic diets:(for specific conditions)♦Meet energy & protein♦Meet requirements for
nutrients that requiremodification eg proteinfor renal failure, fat forGI malabsorption etc
& meet RDI for: nutrients fluid fibre
Nutrition adequacy - Qualitative
♦General guidelines (population/ public healthmessages) - not specific enough to meet RDIs ofindividuals e.g. Dietary Guidelines for Australians Healthy Eating Pyramid
♦Other methods - can meet RDIs and can be modifiedfor individual needs (correct serving sizes must beobserved) e.g. 12345+ plans
Nutrition adequacy – Quantitative
♦When greater accuracy required
♦Used for Individualised assessments Diet calculation Diet prescription
♦Important clinical tools Ready Reckoners Computerised nutrient intake analysis

7
Useful Hints / Practice Tips
♦Adequate servings from the 5 food groups will meetRDIs for nearly all essential nutrients, but notnecessarily for Vitamins D & E Iron Potassium Folate Zinc
• depending on age, gender, food choices (smallamounts of specific nutrient-dense foods mayhelp to overcome these problems, eg.Nuts/seeds, oily fish, unsatd oils)
Useful hints
♦Always combine qualitative and quantitativemethods for assessment and diet prescription/plan
Do not assume serving size – check carefully!
Practise calculating diets until you are very goodat it
Be practical – effective use of time
Messages → MNT
Balanced diet withmodified total fatintake/fat types
Fat < 30% total energywith sat. fat <10%
Eat less fat
Balanced diet with3 serves/d dairyproducts1 serve = 1c milk or200g yoghurt or 40gcheese
Ca 2+ 1000-1300 mg/dEat more calcium
Balanced diet withtotal Na+ 80 –100mmol /d
80 –100 mmol Na+ /dEat less salt
Diet advice / planClinical prescriptionPublic Healthmessage
Target requirements
Weight loss Assess:
current energy intake & energy expenditure weight loss target (5-10%)
• Calculate: Energy deficit required to reach target weight loss
• Provide: Balanced diet & optimal variety/amount of food in the
meal plan Exercise goals
Don’t• Tell patient to “eat less fat”, “eat less sugar”• Advise “do more exercise”
Target requirements
Nutritional support (oral) Diet calculation -
• Energy: xxxx kJ/d• Protein: xx g/d (or x g/kg BW/d)
Assess current intake & provide a DIETARYPRESCRIPTION
• INCLUDE the right amount of additional foodand/or supplements to meet requirements (mealplan)
Don’t just advise “try some supplements” or “eatmore food”
Target requirements
Wound healing
Consider: Are the energy & protein intakes adequate?• Calculate
protein req’ments i.e.. ~1.5g/kg IBW/d energy req’ments - use Schofield
• Develop a dietary prescription• Include: balanced diet & optimal variety/amount of food in
the menu plan
Don’t just advise “eat more protein foods”

8
Target requirements
Diabetic diet and malnutrition Assess:
Energy: intake and req’ment Protein: intake; ~xxg /kg IBW/d (prescription)
• Provide: Balanced diet & optimal variety/amount of food in the
meal plan Appropriate amount and distribution of CHO
Don’ts• Give only general low fat/high fibre advice• Advise to restrict energy intake
Practice Tips
♦Nutrient levels can vary a lot depending on the“type” of foods included in each food groups e.g. for a low K diet, appropriate choices of
“type and amount” of fruit /vegetables/ canlower K, but maintain other nutrients
e.g. for a high fibre diet the choices within thebread and cereal group will effect fibre intake
♦In general : a diet <1500 Kcal/d (~6000KJ) &<60g/d protein becomes marginal in somevitamins & minerals
Art of Dietetics
♦Be able to effectively: Assess Prescribe Implement Monitor outcomes
♦Activities: Today - Case studies – do these diets meet RDIs (basic) & are
balanced? Next session: Ready Reckoner – a more quantitative method
(quick and practical)