Embed Size (px)
Citation preview

In the Bookstores Section Editors:
Alison [email protected]
Stephen [email protected]
The Spirit Level: Why Equality is Betterfor Everyoneby Richard Wilkinson and Kate Pickett;Penguin Books, 2010.ISBN: 978-0-241-95429-4.10.99 GBP. 375 pages.
The Spirit Level
Ever had a ‘ping’ moment? This book might havebeen mine. I’m not a natural pessimist, but Westernsociety today seems less cohesive and people morematerialistic, stressed, unhealthy, and unhappy thanin times gone by. Wealth and status seem to bevalued above everything else. Consumerism is see-mingly unstoppable as the world hurtles towards anArmageddon of its own making. My personal viewsare not that uncommon, as discussions with friendsand family show. Why we are in this situation andwhat can be done about it is less obvious. What Ireally need is someone to join up the dots…Wilkinson and Pickett, both UK-based academics
with economics and epidemiology backgrounds,present a compelling ideological argument, appar-ently underpinned with copious economic and pol-itical evidence. They hypothesise how materialsuccess has led to social failure and back this upwith statistical meta-analyses of international (23of the world’s 50 richest countries) and US-based(50 American states) socioeconomic data. Graphs –with advice on how to interpret them – are used toconvey key outcomes messages. The graphs mostlyshow income inequality (x-axis) in relation tovarious health and social outcomes (y-axis) with aregression line to show the ‘best fit’ relationship.The outcomes are broadly defined as community
life and social relations (including trust, women’sstatus, and spending on foreign aid); mental healthand drug use (including mental illness, mental dis-tress, and use of illegal drugs); physical health andlife expectancy (including infant deaths); obesity(both adults and children); educational performance(including literacy scores, high school drop out, and15-year olds aspiring to low-skilled work); teenagepregnancy (both births and abortions); violence
(including homicide and children’s experience ofconflict); imprisonment and punishment (includingprisoner numbers); and social mobility.
Most of the negative health and social outcomes, itseems, are more prevalent in more unequal societies,and the positive measures (levels of trust betweenmembers of the public and women’s status [as a com-bined index of women’s political participation,employment, earnings, and social and economicautonomy]) show higher values in more equalsocieties. This is apparently true both internationallyand in the US. The authors claim that the relation-ships are too strong to be dismissed as chance find-ings; the differences between more and less equalsocieties are large, and these differences are appli-cable to whole populations rather than subgroups.The conclusion is ‘… that greater equality usuallymakes most difference to the least well-off, but stillproduces some benefits for the well-off’.
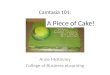
The individual outcomes are combined into asingle index of health and social problems, shownin relation to income equality, in Figure 1.
The findings are balanced to an extent by limiteddiscussion of whether or not inequality plays acausal role, and other possible explanations. In this2010 edition of The Spirit Level, the authors addressthe critics of the original 2009 edition in a newchapter and add evidence that came to light afterthe spring of 2008 – when they finished writingthe original book – and overwhelmingly supportstheir findings.
So, what can be done to iron out inequalitieswhen political will is seemingly lacking? Theauthors assert that ‘greater equality can be gainedeither from using taxes and benefits to redistributevery unequal incomes or by greater equality ingross incomes before taxes and benefits, whichleaves less need for redistribution’, indicating mul-tiple routes to greater equality. Research apparentlyalso suggests that many of us want to narrowincome differences – just think of the banking andcorporate bosses with more than 500 times the earn-ings of their average employees.
The alternatives include developing the alreadyhuge non-profit sector, including communityschemes and co-operatives, and limiting business
205© The European Medical Writers Association 2013DOI: 10.1179/2047480613Z.000000000123 Medical Writing 2013 VOL. 22 NO. 3

expenses and bosses’ pay. A key proposed solutionis democratic employee ownership (where shareownership is combined with participative manage-ment). This leads to bottom-up rather than top-down management; the authors feel this couldtransform our societies. They assert that such abusiness model can co-exist with conventionalmodels in operation now, so the transformationcan be gradual, controlled, and gain in strength ifsupported by government incentives.On a hopeful note, we should consider that the
human urge for equality and fairness has continuedthroughout time, and that our ‘moment’ could con-ceivably be a blip. Let us hope so. In the meantime,visit the Equality Trust’s website (http://www.e-qualitytrust.org.uk), founded by the authors, forfurther insights into their ideas.Now what did I say earlier about a possible ‘ping’
moment? As I read on, and as you may havedetected, doubts began to creep in. Why did theauthors narrow their 50 richest countries to only
23? Why was there little or no discussion aroundother possible causative factors besides inequality?Why, when this theory was publicised in 2009,have governments the world over not made drasticpolicy changes at grass-roots level? And why didthe new chapter addressing their critics barelyadmit to any criticism, let alone address it? I’m noexpert in socioeconomics or epidemiology. Time tofind someone who is…
Acknowledgements
The Equality Trust, on behalf of RichardWilkinson and Kate Pickett, kindly granted per-mission for the use of Figure 1. Figure 1 is areproduction of Figure 2.2 originally publishedin The Spirit Level.
Reviewed by Stephen [email protected]
The Spirit Level Delusion: Fact Checkingthe Left’s New Theory of Everythingby Christopher John Snowdon;Democracy Institute/Little Dice, 2010.ISBN: 978-0-9562265-1-8.8.99 GBP. 172 pages.
The Spirit Level Delusion
Snowdon, an author and freelance journalist basedin the UK, systematically critiques the claims madein The Spirit Level. He reminds us that at the time ofits release, The Spirit Level was ‘rapturously receivedby much of the media…’ and became ‘…one of thepublishing sensations of the year’. By early 2010, the
Figure 1: Index of health and social problems in relation to income inequality.
In the Bookstores
206 Medical Writing 2013 VOL. 22 NO. 3

Spirit Level’s analysis, oft-cited in the British Houseof Lords, was threatening to shape governmentpolicy.Snowdon points out that Wilkinson and Pickett
wrote their book as though they were informingthe public about issues that were established andagreed upon by the academic community, althoughthis was not so. He asserts that they often misrepre-sented other authors’ work and based claims ontheir own published reviews of the work of others.Wilkinson and Pickett also misled by presentingonly supportive data, leaving the (non-expert)reader with the impression that little or no debateexisted among experts on the information theypresent as fact. When added to the fact that only23 of the world’s 50 richest countries were includedin the analysis, and that more recent data was some-times omitted, the suggestion is that data wereselected and manipulated to fit an argument.In The Spirit Level, countries with populations of
under 3 million (to incorporate tax havens) togetherwith countries without reliable data on inequalitywere excluded. Snowdon agrees that tax havensshould have been excluded, but he suggests –rather sensibly – that known tax havens shouldsimply have been ignored, rather than beingexcluded through an arbitrary population cut-offof 3 million. He also re-examines the exclusion ofcountries with ‘unreliable data’ and reinstatesthose inexplicably excluded where reliable dataclearly are available. Reinstated countries includenotable absentees from the Wilkinson/Pickett listof 23 of the 50 richest countries, such as Slovenia,Singapore, Republic of Korea, Hong Kong, CzechRepublic, and Hungary. In his analyses, he retainsthe same measure of inequality and use of linearregression analysis as in The Spirit Level, adds the
square of the correlation coefficient (allowingeasier comparisons between datasets), andencourages readers to use their own judgement forscatter graph interpretation. The same sources ofdata are used as in The Spirit Level. Further methodo-logical detail and discussion are available atwww.spiritleveldelusion.com.
Graphs based on the expanded country cohort forthe outcomes in The Spirit Level show the disappear-ance of the relationship between the outcomes andinequality, with the odd country outlier here andthere. Snowdon re-examines all outcomes investi-gated in The Spirit Level and rightly discusses otherpossible causative factors including culture, religion,diet, race, and genetics, as well as considering thedifferences between individual countries inmethods of recording data and in their welfare,prison, and other national systems. The myth ofinequality as the root cause of just about all socialills is dismantled.
Wilkinson emerges as a somewhat isolated figurein his own academic community, with a knownhistory of questionable selection of data in order tomake a point. Snowdon’s thorough appraisal ofavailable data and literature, and examination ofalternative causes – all underpinned by acerbic wit– sees to that. Snowdon reminds us to remain scep-tical at all times – as indeed we must, both here andin aspects of our work as medical writers too. Thispaired book review is a noteworthy reminder ofour profession’s responsibility to remain objective;exacting in research; and mindful of the implicationsand ramifications of drawing conclusions from‘selected’ data.
Reviewed by Sam [email protected]
Medical Statistics Made Easy 2by M Harris and G Taylor;Scion Publishing Ltd., 2008 (2ndedition).ISBN: 978-1-904-84255-2 (tradepaperback).15.99 GBP. 116 pages.
Any book title that promises Made Easy or the morewidely imitated, jocular For Dummies stokes ourhopes in big ways. We expect its topic to be unques-tionably demystified. We expect it to transmit itscontents to us instantly, as if through a metempsy-chotic education. Not infrequently, however, what
we get is less than what we want, and we surrenderin our quest of effortless learning. A book ForDummies on building websites, to give oneexample, is organised for effortless navigationbetween its sections, but it is 760 pages andweighs just short of 1.2 kg. To its credit, it ispresented as a ‘desk reference’. Medical StatisticMade Easy 2 (MSME2), on the other hand, isfree of most of the common deterrents to thesatisfying use of books specifically targeted to neo-phytes to a topic. It endears itself even as it emergesout of its shipping bindings. It is sized to behandled comfortably and with a tactile pleasureenhanced by its satiny cover. The smile-inducingcolourful graphics of its cover bring to mind a
In the Bookstores
207Medical Writing 2013 VOL. 22 NO. 3

luscious ice cream cone – and the intense urge tolick it.An uncustomary amplitude of white space in this
book strikes the reader on first glimpse of itsinnards. On reflection, this aspect is entirely logicaland compatible with, in fact necessary to, the fulfil-ment of the promise of the book’s title. First, itincreases readability. Second, definitions anddescriptions are given discrete individualities bybeing separated from each other by extra spaces (asort of highlighting by excision of neighbouringchaff ). Crucial ideas stand out without being runinto each other in long, dense paragraphs. Finally,to render any text ‘easy’, it must be edited andpared extensively down to the fundamentals of itstopic. It takes hard work to make things look easyto learn. The blank spaces in this book are theresults of a Herculean effort to simplify conceptsto their bare bones. I imagine the authors sittingdown with a much longer text and highlighting (inyellow, let’s say) essential ideas, and then debridingand excising a lot of repetitious/prolix passages,and leaving in their places white spaces. Theauthors clearly know medical statistics; otherwisewe would have had a longer book with pretensionsof having made its topic ‘easy’.The book is for ‘… health care students and pro-
fessionals who need a basic knowledge of whencommon statistical terms are used and what theymean’. For each concept of statistics, the authorsfirst note, on a scale of 1–5 (using stars forexample), a measure of importance (frequency ofuse [read incidence and prevalence] in medical litera-ture). They follow that with a rating of how easy theconcept is to understand (the frequency of use of aconcept in medical literature does not coincide withincreased comprehensibility of the concept). The situ-ation in which a statistical concept would be used isdescribed next, and following that its meaning, i.e.what information it communicates to the reader ofa clinical report, for example. Clear graphs andtables (where appropriate) and applied examples(in boxes) complement the textual treatment of eachconcept. Under the subheading ‘Watch out for…’the authors post alerts to potential misconceptionsand common pitfalls and how to avoid them.The motivated reader is going to find the authors
intelligent, reflective, and reassuringly dedicated totheir readers. Deep and honest reflection will con-vince many of us that many statistical concepts arecontrived constructs. To demystify a subject that isin part comprised of conventions, one must beready to adopt slightly irreverent attitudes. Who
would not be alerted, cheered, and edified by free-standing declarations the authors make, such as‘Even easier than mean!’ (about the comprehensibil-ity of median)? Or de-stressed by the statement ‘It isnot an intuitive concept’ (about standard deviation)?Or by ‘It is not important to know how the P value isderived—just to be able to interpret the result’. ‘Aha’one says, and stops feeling like a dense, maladroitdummy. In another chapter, titled Statistics AtWork, the authors present extracts from somepapers actually published in journals such as BMJ,The Lancet, and NEJM, and discuss the statisticaltreatments used in them.Infrequent inconsistencies in formatting (copyedit-
ing and productional oversights) and the occasionaldistraction provided by telegraphic sentence frag-ments aside, I did not discover any errors or omis-sions in my reading of this book. The contents ofthis book are a distillate of the corpus of medical/scientific statistics. Nothing important or relevantseems to have been left out. A reliable opinion onthe volume’s accuracy and completeness should,however, come from a qualified statistician. A glos-sary at the end is quite useful: its entries recapitulatethe principal concepts and, like a supplementalindex, refer the reader to the sections where theywere elucidated. Surprisingly improvident, and inex-cusable, is the absence of a short list of suggestedreadings from this non-fiction, instructional book. A5-, 6-item bibliography (there are a couple ofseminal titles that come to mind immediately)would have staved off this criticism; and it wouldhave served well those who may wish to delvebeyond the excellent introductory distillate theauthors have provided.Although many of us medical writers and editors
do not need to have an operational command ofmedical statistics and do statistical analysis per se,we do need to have familiarity with its conceptsand applications. For that purpose, I would rec-ommend taking an introductory workshop (suchas those offered at EMWA conferences or byAMWA) and at the same time buying MSME2 – tobrowse for review, for additional details, or for refer-ence. Its utility aside, the pleasure and reassuranceprovided by the knowledge that such user-friendlybooks can be, and are, written and published iswell worth the price of what rightly can be con-sidered the eminently provident ultimate chapbookof medical statistics.
Reviewed by Jack [email protected]
In the Bookstores
208 Medical Writing 2013 VOL. 22 NO. 3

Bioethics for Beginners 60 Cases andCautions from the Moral Frontier ofHealthcareby Glenn McGee;Wiley-Blackwell, 2012.ISBN-13: 978-0470659113.14.99 GBP. 169 pages.
Deeply flawed (non-)introduction tobioethics
Bioethics for Beginners comprises 60 “Cases” – shortarticles (mostly opinion pieces) written by bioethicistGlenn McGhee for blogs and magazines – that areintended to introduce the reader to some of theethical issues around science and medicine.Some of its better passages provide interesting intro-ductions to subjects such as ethical training forresearchers, the unacceptable exploitation of poorand uneducated people in clinical trials in India,and conflicts of interest. Other highlights are Cases20, 37, 40, 41, and 50, which respectively deal withhuman cloning, quarantine, sanitation, codes ofconduct for Internet health, and the misrepresenta-tion of case reports.The problem is, for a book purporting to be about
bioethics, there is very little discourse on ethics.Rather there is much discussion of pragmaticissues relating to biotechnological advances. Forexample, the essence of Case 1 is that syntheticorganisms are okay if there are safeguards. This isnot bioethics! Instead of debate, we get opinion,hearsay, and politics. Case 2 can be summarised asMcGee dislikes the teaching of intelligent design.So do I, but this is just opinion. The book’s title ledme to believe that it would illustrate key bioethicalissues with pertinent examples. It doesn’t. Mostcases are simply not instructive.According to the information on the inner front
cover, the book boasts ‘the very latest from the fron-tiers of science and medicine’. That is plain mislead-ing. Some of the material dates back as far as 1998,and certain statements are dreadfully dated (‘Mostphysicians know about and have used the Internetin some way’ – find me one who hasn’t). Updatingthe book to include mentions of Facebook, Twitter,and apps does nothing to hide the fact that muchof the content is old.And just who is McGee’s audience? While he
makes multiple references to films such as BladeRunner and TV shows such as Star Trek, indulgesin cheap plays-on-words, and describes joiningDNA sequences as ‘stacking the bits together like
toy blocks’, he uses words such as mesenchymal,pluripotent, and parthenotes without definingthem. The truth is there is no one audience. Thesearticles were written for different blogs/websites/magazines with different readerships/users.
The inner front cover describes Bioethics forBeginners as ‘eminently readable’ and demonstrat-ing ‘clear thinking’. Nothing could be further fromthe truth. This passage from Case 8 (Stem Cells: TheGoo of Life and the Debate of the Century) is notunrepresentative:
Everyone is up in arms about stem cell research:adult versus embryonic, iPSCs, and parthenotes.And maybe not up in arms exactly. But certainlyeveryone has a champion, a favorite kind of stemcell, the cell on the verge of curing cancer,macular degeneration, or male pattern baldness.
You what?!Many of the articles that make up the book are
poorly written. Some sentences I read severaltimes without making sense of them. There are pro-blems with logic, typos, (‘sue of the raw materials’),and repeated explanations of the same thing. Thepresident of an institute is quoted as saying ‘Whatwill not stop this from happening misgovernmentoversight.’ I’ll bet he didn’t say that! And thenthere is the logic-defying reference to ‘more thanboth senses of the word’. These and the manyother issues suggest a complete lack of editorialinvolvement, while the following note, appendedto one case, gives a clue as to how much careMcGee invests in his writing:
A previous version of this story incorrectly said that45 to 100 million Americans die each year of medicalmistakes.
Perhaps trying to connect with non-scientist readers,McGee revels in his own ignorance: ‘If you are likeme you won’t be able to read the articles about thehuman genome in the prestigious journals Natureand Science. … the articles are no more comprehen-sible than the actual DNA code itself – TAC, CTA,GAS and so on’. He confesses to being ‘cluelessabout what it is that nanotechnology means’,while his statement that ‘We don’t really knowhow to turn genomics on and off, and we can’tquite figure out whether it is working for us oragainst us’ shows that he has not even botheredtrying to understand genomics.
Bioethics for Beginners has a clear US perspective,rooted in ‘American family values’, money, fear of
In the Bookstores
209Medical Writing 2013 VOL. 22 NO. 3

bioterrorism, and controversy surrounding stem cellresearch, and assumes a fair amount of knowledgeof US institutions. More than this, it has a partisantone that borders on the offensive. McGee writesthat ‘the real concern isn’t that the other guys arewinning, it is what happens when they bend therules to do so’; that ‘ethics can get forgotten asother nations … race to fill the void’; that ‘Only aproperly funded US stem cell research programwill guarantee oversight and the protection of allinvolved.’ A lot of this seems to stem from theHwang Woo-suk cloning scandal in Korea, whichMcGee returns to over and over again and whichappears to have coloured his view of non-USresearch. He refers, insultingly in my view, to a‘grossly irresponsible lack of American leadershipin the regulatory and funding arena’ in the contextof the Woo-suk case.The book’s standout passage is Case 59, an
extended and highly enjoyable introduction to andrepudiation of William Hurlbut’s pseudoscientificstem cell research, which has been challenged inseveral forums, including the New England Journalof Medicine.1,2 But how many readers will make itthat far? Viewed individually, many of the articlesthat make up Bioethics for Beginners are deeplyflawed. Viewed as a collection, they are a totalmess. This book was poorly conceived and poorlyexecuted. The idea of assimilating an author’s mul-tiple works on a range of subjects under a mislead-ing heading (‘bioethics’) is a shabby contrivance.
Those seeking a more coherent introduction to thesubject could do worse that get hold of a copy ofWhite Coat, Black Hat by Carl Elliot,3 on whomMcGhee repeatedly (and inexplicably) pours scornin his writings.Wrapping things up after the last case, McGee
argues that the race to make scientific advancesmust not lead to ethical issues being ignored, butembarrasses himself by explaining (again) whoWoo-suk is, having previously referred to hisfraud at least half a dozen times. The disjointednature of this conclusion, which comprises unre-lated articles originally published in 2005 and2007, encapsulates one of the book’s main problems:a lazy approach, and one that should not berewarded with your money.
Reviewed by Stephen GilliverScience Editor, Center for Primary Health Care
Research, Malmö, [email protected]
References1. Melton DA, Daley GQ, Jennings CG. Altered nuclear
transfer in stem-cell research – a flawed proposal. NEngl J Med. 2004;351(27):2791–2.
2. Byrnes WM. The flawed scientific basis of the alterednuclear transfer-oocyte assisted reprogramming(ANT-OAR) proposal. Stem Cell Rev. 2007;3(1):60–5.
3. Elliott C. White Coat, Black Hat. Adventures on theDark Side of Medicine. Beacon Press, Boston; 2010.
Behind Closed Doors: IRBs and theMaking of Ethical Researchby Laura Stark;University of Chicago Press, 2012.ISBN-13: 9780226770871.£18.00 GBP. 229 pages.
A fascinating insight into how IRBsoperate and why they exist
Researchers and investigators the world over mustlook upon ethical review as a pesky hurdle to over-come before getting started with a study, but justhow do institutional review boards (IRBs, ethicscommittees) operate and how did our system ofethical review come into being? In Behind ClosedDoors: IRBs and the Making of Ethical Research, assist-ant professor Laura Stark seeks to answer both thesequestions.
In part one (of two), Stark describes her experi-ences of the decision making process from sittingin on meetings of three IRBs. Her source materialincludes recordings of 19 IRB meetings, complemen-ted by interviews with 33 IRB members and arandom sample of 20 IRB chairs. The far reach ofethical review is highlighted by the fact that theauthor’s proposed research for this book was itselfsubject to IRB scrutiny.The three chapters that make up this half of the
book collectively describe the ways IRB membersargue for their views to be accepted, and how thehandling of previous applications guides the wayIRBs deal with new ones. Other interesting topicsthat are highlighted include situations whereconsent can be waived and times when ethics andlaws come into conflict. The author also considersthe way requests for minor language changes instudy documents can affect the conduct of a study.Her account is revealing. The operations of the
IRBs she observed were greatly affected by the
In the Bookstores
210 Medical Writing 2013 VOL. 22 NO. 3

biases/prejudices/backgrounds of their members,and researchers were judged based on the writingof their applications, including typos andinconsistencies.What becomes clear is that IRBs operate by a
process of case-based learning (using previousdecisions as the basis for future ones), rather thanthe application of a general set of rules or principles.This leads to different IRBs making different judge-ments, which can be a big problem for multi-sitestudies, where IRBs covering different sites mayrequest different amendments. As a way of increas-ing consistency in decision making, the author pro-poses training IRB members with a common set ofreal cases.Stark argues cogently that the fact that IRB meet-
ings are closed allows subjective experience (e.g. theexperiences of family members and acquaintances)to have a greater influence on decision makingthan it might if the meetings were open.Interestingly, she further asserts that IRB meetingminutes provide a selective picture, obscuring dis-agreements, giving the impression of consensus,and shielding individual board members frombeing linked to particular requests for changes,thereby enabling them to make such requestswithout fear of reprisal.The book’s second half paints a less than noble
picture of ethical review as a form of insurance, away of preventing lawsuits, a system instituted toprotect the interests of researchers, the NationalInstitutes of Health (NIH), and the NIH ClinicalCenter, rather than those of patients.Stark explains how the system of medical research
ethics we have today was developed at the NIHClinical Center in the 1950s and 60s, including themove away from trusting in the judgement of theindividual researcher, in matters relating topatients/research subjects, to reliance on committeesof experts. She argues that the obvious alternative, acode of ethics, was not adopted because it wouldhave curbed the freedom of researchers to agreater extent, and also claims that the policy atthe Clinical Center in the early 1950s was thatresearch came first, patients second.To place the development of research ethics at the
Clinical Center in context, Stark provides details ofits operations during its formative years, whichincluded efforts to increase the number of healthyresearch subjects (‘Normals’) by recruiting prisonersand conscientious objectors (to whom becoming atest subject was sold as an heroic service). Some ofthese research practices, by today’s standards, defy
belief. Take this telling description of one Normal’stime at the Clinical Center:
After a year on several other wards for studies ofthe thyroid and of new steroids, Sarah moved to the3-West nursing ward as the only person in thecontrol arm of Dr. Savage’s studies that examinedwhether LSD helped schizophrenics in psychotherapy.
A year? The only person in a control arm? This is notthe kind of research the New England Journal ofMedicine is interested in.
One especially absorbing chapter is devoted toconsent. Here Stark describes the initial resistance tothe use of signed informed consent forms; the battleover signed consent/liability release forms betweenlawyerswhowanted to protect theNIH from litigation,and researchers whowanted to do as they pleased; andthe astonishing argument that theremust be somethinginherently wrong with young people who volunteerfor medical testing, and that they are thus incapableof providing meaningful consent.
In the final chapter Stark outlines how and whyethics committees spread to other sites, arguing thatit was a way of transferring liability from the NIHto the institutes where it funded research, and of pla-cating Congress (responsible for approving NIHfunding) and a concerned public. While somewhatless fascinating than the rest of the book, this dis-course nevertheless reinforces the author’s apparentview that ethical review was established in the inter-ests of anyone but patients and research subjects.
In summary, Stark’s exploration of the history andworkings of IRBs should appeal to anyone with aninterest in research ethics. Those keen to find outmore about topics of particular relevance tomedical writers – the importance of ethics appli-cations being well written and targeted to the rightaudience, and the potential role of medical writersin preparing such applications – could perhapsalso read the reflections of a current EMWAmember who sits on an ethics committee.1,2
Reviewed by Stephen GilliverScience Editor, Center for Primary Health Care
Research, Malmö, [email protected]
References1. Jacobs A. Patient information leaflets: the ethics com-
mittee view. TWS 2005;14(3):82.2. Jacobs A. Inside a research ethics committee. TWS
2008;17(4):173–4.
In the Bookstores
211Medical Writing 2013 VOL. 22 NO. 3