Embed Size (px)
Citation preview

Medication Administration
Medications
Epinephrine (Epi-Pen)
Albuterol (MDI)
Atropine/2-PAM (Mark-1 Kit)
Oral Glucose
Oxygen

6 Rights of Med Aministration
Right Patient
Right Medication
Right Dose
Right Route
Right Time
Right Documentation

Epinephrine
Epi-Pen - single or dual dose
Adult - 1:1,000 solution, 0.3 mL(0.3 mg)
Peds - 1:2,000 solution, 0.3 mL(0.15 mg)
Onset : Seconds
Peak : Minutes
Duration : Several Minutes
What is it?
Non-selective Adrenergic Agonists (ɑ and β)
“Turns on” sympathetic nervous system
Increased HR and contractility
Increased RR
vasoconstrictor or vasodilator
bronchodilator
When to use it?
Allergic Reaction
Asthma
Cardiac Arrest

Allergic Reaction
Mild
itching, rash/hives, watery, red eyes, tingling in mouth
Moderate
anxiety, throat tightness, trouble breathing or swallowing, wheezing, rash/hives, abd pain/cramp, NV
Allergic Reaction
Severe
feeling of impending doom, respiratory distress, hives, decreased LOC, low BP, tachycardia
Anaphylactic shock
like severe accompanied by shock
SBP < 90, HR> 110, life threatening
Management
ABCDs
Oxygen
ID and remove allergen if possible
Monitor condition for worsening
Arrange transport
Epinephrine administration

Epi-Pen Administration
6 Rights of Medications
Remove safety cap
Grasp injector- don’t put thumb over end
Place over outer thigh muscle and push until needle deploys.
Hold in place 10 seconds
Massage sight

Side Effects
Tachycardia
Anxiety
Increased BP
Angina?
AlbuterolProventil, Ventolin, Xoponex
Metered Dose Inhaler (MDI or “Puffer”)
May have spacer
Onset: 5-15 minutes
Peak: .5 - 2 hours
Duration: 3-4 hours

What is it?
Selective β Adrenergic Agonists (β2 > β1)
Relaxes bronchial smooth muscle
other smooth muscle too - vascular, uterine etc.
Increased HR

When to use it?
Bronchospasm
Asthma
Allergic Reaction
Asthma
Mild
mild SOB, may have some wheezing
Moderate
increased SOB, pronounced wheeze, may have prolonged expiration, anxiety
Severe
respiratory distress, may have silent breath sounds, severe anxiety

Management
ABCDs
Oxygen
MDI
Monitor and/or transport
Epi-Pen, in extremis, if available
MDI AdministrationRemove Cap
Shake
Have patient exhale
Have patient place lips around mouthpiece
Have patient breathe in slowly
Depress top as they breathe in
Hold breathe for at least 10 seconds
Repeat every 30 - 60 sec as needed

Side Effects
Dysrythmia, tachycardia
Tremors, anxiety
Nausea, vomiting
Hyperglycemia
Rare paradoxical bronchospasm

Atropine/2 PAM
Mark 1 Kit (autoinjectors)
Atropine: 2 mg in 0.7cc
Pralidoxime (2 PAM) 600 mg in 2 cc
Onset : 1 minute
Peak : 2-5 minutes
Duration : 2 hours
What is it?
Atropine: Competitive antagonist of acetylcholine
2 PAM: Cholinesterase re-activator
Both act to turn off parasympathetic nervous system

When to use it?
Anticholinesterase exposre
Nerve Gas/WMD
Organophosphate (insecticide)
Atropine has other uses - including cardiac arrest, symptomatic bradycardia etc
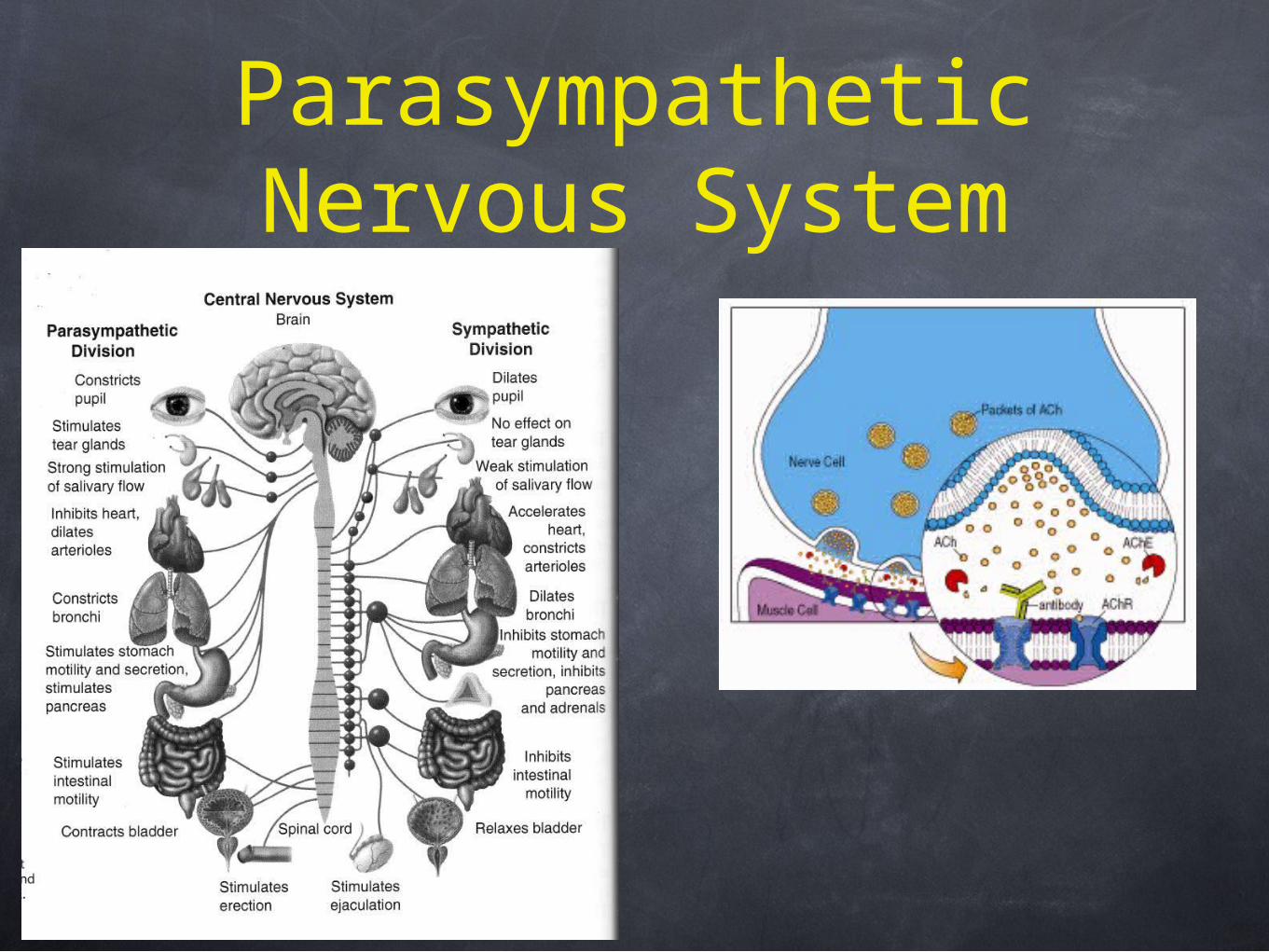
Parasympathetic Nervous System

AnticholinesteraseExposure
Turns on Parasympathetic nervous system
S - salivation
L - lacrimation
U - urination
D - defecation
G - GI distress
E - Eye constriction

AnticholinesteraseExposure
Turns on Parasympathetic nervous system
D - defecation
U - urination
M - miosis (pupil constriction)
B - bronchorhea, bradycardia
E - emesis
L - lacrimation
S - salivation
AnticholinesteraseExposure
Respiratory Arrest
Seizure
Coma
Death
Management
Do not expose yourself
ABCDs/Oxygen
Decontamination
Atropine
2 PAM
Arrange transport

Atropine/2 PAM Administration
6 Rights of Medications
Remove safety cap
Grasp injector- don’t put thumb over end
Place over outer thigh muscle and push until needle deploys.
Hold in place 10 seconds
Massage sight

Atropine/2 PAM Administration
Give atropine first
Mild
Atropine q5 minutes until effect
2 PAM q15 minutes times three
Severe
Give 3 doses each in rapid succession
Can give atropine q5 with no limit
Grasp injector- don’t put thumb over end
Place over outer thigh muscle and push until needle deploys.
Hold in place 10 seconds
Massage sight

Side Effects
Dry mouth, thirst
Hot, dry, flushed skin
Fever, palpitations, restlessnes
Delerium

Oral Glucose
Adult - 15-45 G PO
Peds - 5-45 G PO
Onset : 10 minutes
Duration : uncertain

When to use it?
Symptomatic Hypoglycemia

SymptomaticHypoglycemia
Typically patients on DM medication
Mild/Moderate
funny feeling, anxiety, sweatiness, shaky
Severe
altered mental status, decreased LOC, seizure
Patients typically can tell

Management
ABCDs
Check glucometer if possible
Administer PO glucose if patient can handle secretions
Give other food PO once recovered
Patients on oral hypoglycemic meds should be transferred due to long half-life

Side Effects
Hyperglycemia

Oxygen
Used liberally in pre-hospital setting
Air is ~20% oxygen
2LNC ~24%
10L FM ~57%
10L NRB ~68%
Oxygen
Generally safe
Oxygen toxicity from prolonged exposure to high partial pressures
COPD pts may have blunted respiratory response
In ski patrol setting there should be no contra-indication









![PATIENT MEDICATION INFORMATION · • Sympathomimetics (such as epinephrine [adrenaline], or salbutamol, albuterol or terbutaline used to treat asthma) • Growth hormone (medicine](https://img.pdfslide.net/doc/110x75/5e5027899cbbf304ec7f880c/patient-medication-information-a-sympathomimetics-such-as-epinephrine-adrenaline.jpg)