Embed Size (px)
Citation preview

MEDICATION ASSISTED TREATMENT
Michael Fingerhood MD FACP

Medications
• Opiates• Naltrexone• Methadone• Buprenorphine
• Alcohol• Naltrexone• Acamprosate• Disulfiram
• Nicotine• Buproprion• Varenicline
• Cocaine• ????

1. Tolerance2. Withdrawal3. Larger amounts/longer period than intended4. Inability to/persistent desire to cut down or
control5. Increased amount of time spent in activities
necessary to obtain6. Social, occupational and recreational activities
given up or reduced7. Opioid use is continued despite adverse
consequences
DEFINING the DISEASE: Opioid Dependence (DSM IV)
THREE OR MORE IN THE PAST YEAR

1. Tolerance2. Withdrawal3. Larger amounts/longer period than intended4. Inability to/persistent desire to cut down or control5. Increased amount of time spent in activities
necessary to obtain6. Social, occupational and recreational activities
given up or reduced7. Opioid use is continued despite adverse
consequences
DEFINING:Opioid Dependence?

Opium History• First cultivation of opium poppies was in
Mesopotamia, approximately 3400 B.C., plant called Hul Gil, the "joy plant”
• The Greek gods Hypnos (Sleep), Nyx (Night), and Thanatos (Death) were depicted wreathed in poppies
• The Persian physician, al-Razi (845-930 A.D.) made use of opium in anesthesia and recommended its use for the treatment of melancholy.

Opium History• Between 400 and 1200 AD, Arab traders
introduced opium to China.• 14th century Ottoman Empire-opium used to
treat headache and back pain. • 15th century China- first officially recorded use
of opium as a recreational drug.• 1874- heroin developed• 1898-heroin marketed by Bayer as safe
pediatric cough suppressant

Opiates = naturally present in opium
• e.g. morphine, codeine, thebaine
Opioids = manufactured• Semisynthetics are derived from an
opiate• heroin from morphine• buprenorphine from thebaine
• Synthetics are completely man-made to work like opiates
• methadone
Opiates & Opioids

Narcotic Regulation in US
• 1914- Harrison Narcotics Tax Act
• 1925- Linder vs United States
• 1964- Methadone introduced as experimental treatment for opioid addiction
• 1968- Bureau of Narcotic and Dangerous Drugs formed (changed to DEA in 1973)

Rationale for Opioid Replacement Therapy
• Traditional treatment has been to provide opioid agonist therapy• Methadone (Dolophine®)• Levo-Alpha Acetyl Methadol (LAAM) – not available
• Stabilize neuronal circuitry• Mu occupation/blockade • Cross-tolerant, long-acting, oral
• Prevent withdrawal and craving• Extinguish compulsive behavior• Prevent spread of HIV and HCV• Prevent criminal activity

Traditional 12 Step Drug Treatment
1. Accepting powerlessness2. Disease identification 3. Surrender to a Higher Power4. Commitment to AA/NA5. Commitment to abstinence6. Sober social support7. Intention to avoid high-risk situations

Effective Treatment of Opiate AddictionNIH Consensus Development Conference
November 17-19, 1997
Opiate dependence is a brain-related medical disorder Treatment is effective-
“Although a drug-free state represents an optimal treatment goal, research has demonstrated that this goal cannot be achieved or sustained by the majority of opiate-dependent people.”
Reduce unnecessary regulation of long-acting agonist treatment programs
Improve training of health care professionals in treatment of opiate dependence

THE PROBLEM:Emergency room mentions of opioid use
95,000
88 89 90 91 92 93 94 95 96 97 99 00 019830,000
40,000
50,000
60,000
70,000
80,000
90,000
DAWN, 2002

Trends In Emergency DepartmentMentions of Opioids:1991-2001
0
20,000
40,000
60,000
80,000
100,000
120,000
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
Other Opioid Analgesics Heroin/Morphine
DAWN, 2003

Changing Route of Heroin Administration
0%
20%
40%
60%
80%
100%
1992 1993 1994 1995 1996 1997 1998 1999 2000
Injection Inhalation Smoking Oral Other
Treatment Episode Data System, 1992-2000

Thousands of New UsersThousands of New Users
00
500500
1,0001,000
1,5001,500
2,0002,000
2,5002,500
3,0003,000
1965 19701970 19751975 19801980 19851985 19901990 19951995 20002000
All AgesAll Ages
Aged Under 18
Aged Under 18
Aged 18 or OlderAged 18 or Older
New Non-Medical Use of Opioid Medications
NSDUH, SAMHSA, 2003

Non-Medical Use of Opioid Medications
• Non-medical use of any prescription psychotherapeutic drug was second only to past-year use of marijuana (11.3 million vs. 25.5 million)
• Ages 18-25 had highest rates for all pain relievers, followed by 12 to 17 year olds
• Males had higher rates except for youths 12-17, where females had higher rates
• Most non-medical users of psychotherapeutic drugs also used other illicit drugs (82%)
NSDUH, 2004

Source: SAMHSA
OPIOID Treatment Admissions per 100,0001994
5-9
<5
Incomplete data
14-24
10-13
25+

Source: SAMHSA
OPIOID Treatment Admissions per 100,000 2000
5-9
<5
Incomplete data
14-24
10-13
25+

Source: SAMHSA
OPIOID Treatment Admissions per 100,0002005
5-9
<5
Incomplete data
14-24
10-13
25+

Opioid dependence is costly
• Medical Costs• Mental illness
• An environmental and disease stressor• Co-morbid interactions
• Trauma and infections• Hepatitis and HIV• $20 billion per year total costs• $1.2 billion per year health care costs
• Non-medical costs- work, legal, prison

Problems With System Prior to 2000
• Less than 20% of opioid dependent persons are receiving treatment in traditional settings
• Poor clinic retention• Environment inhibits recovery• Highly regulated doses & take homes
• Criteria exclude persons under age 18• Infrastructure of care
• High turnover of staff• Ability to get to treatment may be limited

What the opioid dependent patient feels…
Dole, Arch Int Med, 1966

The Opioid Disease Process
• Repeated exposure to short acting opioids leads to neuronal adaptations• Meso-limbic dopaminergic system
• adaptations in G protein-coupled receptors• up regulation of cyclic cAMP second messenger pathway
• These changes:• Mediate tolerance, withdrawal, craving,
administration• Basis of specific pharmacotherapies to stabilize
neuronal circuits

Rationale for Opioid Replacement Therapy
• Traditional treatment has been to provide opioid agonist therapy• Methadone (Dolophine®)• Levo-Alpha Acetyl Methadol (LAAM) – not available
• Stabilize neuronal circuitry• Mu occupation/blockade • Cross-tolerant, long-acting, oral
• Prevent withdrawal and craving• Extinguish compulsive behavior• Prevent spread of HIV and HCV• Prevent criminal activity

Problems With System 1999• Less than 20% of opioid dependent
persons are receiving treatment in traditional settings
• Poor clinic retention• Environment inhibits recovery• Highly regulated doses & take homes
• Criteria exclude persons under age 18• Infrastructure of care
• High turnover of staff• Ability to get to treatment may be limited

Drug Abuse Treatment Act (DATA) of 2000
• Allowed “Qualified” physicians to treat opioid dependence outside methadone facilities1. Addiction certification from approved organization, or
2. Physician in clinical trial of qualifying medication, or
3. Complete 8-hour course from approved organization
• DEA issues (free) to qualifying physicians a new DEA number to use medication for opioid dependence
• As of today, only one medication formulation is approved for this use

Opioid Treatment: Changing Approach
Methadone Clinic Buprenorphine
• Criteria:
Withdrawal
12 months use
• Criteria:
DSM IV
No time criteria
• Dose regulated • MD sets dose
• Age > 18 • Age > 16
• Limited take homes • Take homes (30 days)
• Services “required” • Services must be “available”

MarkedAbsentEuphoria
3-6 hours24-36 hoursDuration
Immediate30 minutesOnset
IV, INOral or SL
Route
HeroinMethadone
Buprenorphine
Treatment vs. Addiction

Stabilization by Blockade Treatment

Methadone EffectivenessGunne & Gronbladh, 1984
H H HH
H H HH
H H HH
H H HH
H
H H HH
H H HH
H H HH
H H HH
H
Methadone Regular Outpatient
Baseline

Methadone EffectivenessGunne & Gronbladh, 1984
P H HH
H
P HP
H H HH
H H HH
H H H
Methadone No Methadone
After 2 Years
1
32
1- Sepsis & endocarditis2- Leg amputation3- Sepsis

Methadone EffectivenessGunne & Gronbladh, 1984
P H H
H
P P
P
Methadone No Methadone
After 5 Years


Methadone Treatment Decreases HIV Seroincidence
Metzger et al. JAIDS 1993;6:1049.
0
5
10
15
20
25
30
35
40
45
Baseline 1 yr. 2 yr. 3 yr.
% s
erop
ositiv
e
Methadone Out-of-treatment

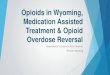
Buprenorphine, Methadone, LAAM: Treatment Retention
Per
cent
Ret
aine
d
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
20% Lo Meth
58% Bup
73% Hi Meth
53% LAAM
Study Week Johnson RE, et al (2000)

Discrepancy Between Population Abusing Opioids and Population Treated
Opioid Abuse
NSDUH Past Month Use 2002
96% Non-heroin Only
4,549,570 reported opioid abuse
Methadone Treatment
TEDS 2002 Admissions Involving Methadone Treatment
83% Heroin Only
111,885 admissions involved methadone treatment
Treatment Under the Waiver (BUP)
434 patients recruited from 132 sites
40% Non-heroin Only
Patient Study BUP Evaluation 2005
Heroin Only BothNon-heroin Opioids Only
(courtesyCSAT/SAMHSA)

Buprenorphine’s Properties
• Modest agonist activity with ceiling
• Long half life
• Precipitated withdrawal if taken after full agonist
• Decreased risk of respiratory, CNS depression
• Sublingual route of administration
• “Combo” tablet with naloxone limits abuse by injection

Buprenorphine Safety• No alteration of cognitive functioning
• feel “normal”
• No organ damage• Early concern of hepatic toxicity unconfirmed
• No evidence of QT prolongation
• Ceiling prevents respiratory depression, OD(Overdose reports with combining use with
benzodiazepines)
• No clinically significant interactions with other drugs

Appropriateness for Office-based Treatment
• Patient is less likely to be an appropriate candidate for office-based treatment: • Dependence on high doses of benzodiazepines,
alcohol, or other CNS depressants
• Significant psychiatric co-morbidity
• Multiple previous treatments (methadone) and relapses

Most often heard quotes with Buprenorphine
“Doc, I feel normal”“I wake up not sick”“I have my life back”
• Treatment in normal medical settings:• Encourages continuity of medical/specialty care• Encourages relationship building with clinicians• Legitimize opioid dependence as a normal, treatable,
chronic illness

Buprenorphine: Retention and Mortality
All Patients received group CBT Relapse Prevention, Weekly
Individual Counseling, 3x Weekly Urine Screens. n=20 per group
Treatment duration (days)
Rem
aini
ng in
tre
atm
ent
(nr
)
0
5
10
15
20
0 50 100 150 200 250 300 350
Bup 6 day detoxBup Maintenance
4 deaths
0 deaths
Kakko J, Lancet 2003

Who were the first patients?
0%
10%
20%
30%
40%
50%
60%
New to SubstanceAbuse Treatment
New to Medication-Assisted Treatment
Transitioned fromMethadone
Addicted to Non-Heroin Opioids*
Per
cen
t o
f P
atie
nts
Tre
ated
Addiction Physician Survey 2003

Opioid Dependence Treatment in Primary Care
Stein, JGIM 2005
At 24 weeks, 59% remained in treatment

Buprenorphine: Reduces Other Drug Use
Fudala, NEJM 2003

Buprenorphine Diversion
Cicero, NEJM 2005
OXYCODONE
METHADONE
BUPRENORPHINE

Patient 1• LS is a 48F, hospital communications
supervisor, started snorting heroin at age 17. On methadone several times- did not like “crowd at methadone program.” Single mom, raised son, who just graduated college. She uses heroin 3x day “to not be sick”; failed detox many times. Already my patient for HTN and family issues related to Huntington’s disease

Patient 2
• SB is a 34M with Type I DM, HTN and retinopathy, recently moved to Baltimore. Works as concierge at downtown hotel. Using heroin since age 21- snort and IV. Active in NA, but keeps relapsing. Was on methadone- made too drowsy. Heard about buprenorphine and interested in finding out more.

Our Buprenorphine Outcomes at One Year
• All patients initiated on buprenorphine August 2003 through September 2007
• Visits 15 minutes; frequency at discretion of provider; non-witnessed urines checked for temperature

Outcomes Comprehensive Care Practice
• Co-morbidities- Heptatitis C-49%; psychiatric disorders 49%; HIV 14%; chronic pain 18%
Outcomes-• At the end of one year- 145 patients
(57%) were still receiving buprenorphine treatment
• Overall 65% of month-long treatment blocks were opioid negative

Outcomes Comprehensive Care Practice
• Co-morbidities- Heptatitis C-49%; psychiatric disorders 49%; HIV 14%; chronic pain 18%
Outcomes-• At the end of one year- 145 patients
(57%) were still receiving buprenorphine treatment
• Overall 65% of month-long treatment blocks were opioid negative

Buprenorphine Outcomes Comprehensive Care Practice
• Treatment success higher for non-heroin users; all other demographic variables not significantly different
• Non-retained patients (109)- 63 lost to f/u; 10 lost insurance; 21 discontinued; 8 transferred to methadone maintenance; 2 had adverse effect; 5 deaths – 3 overdose (none on buprenorphine at time of death); 1 AIDS; 1 cerebral hemorrhage.


Combined pharmacotherapies…
• Randomized controlled trial- 11 centers• N=1383 divided in 9 arms- CBI & no pills,
MM/CBI and naltrexone, MM/CBI and acamprosate, MM/CBI and placebo, MM/CBI and both acamprosate and naltrexone, MM amd acamprosate, MM and naltrexone, MM and placebo, MM and both acamprosate and naltrexone.

• Medical Management- provider provided support during 9 visits, focusing on support of abstinence (e.g. go to AA) and medication adherence
• Cognitive Behavioral Intervention- intensive counseling delivered by outside addiction specialist
• Patients enrolled after 4-21 days of abstinence• Met DSM criteria and quantity >14/week in
women, >21/week in men and >2 heavy drinking days in 30 day period
• Exclusion-other substance abuse (nicotine and cannabis okay), on psych meds, unstable medical condition

• Study population- 428 women and 955 men, mean age 44, 71% had at least 12 years of education, 42% were married.
• Prior to randomization, 2.3% were medically detoxified.
• Across treatment groups, no significant differences in baseline measures; % days abstinent ranged from 23.5-29.8%.

Adverse events
• Acamprosate- nausea 24%, diarrhea 65%*• Naltrexone- nausea 34%*, diarrhea 31%• Both- nausea 42%*, diarrhea 56%*• Placebo- nausea 21%, diarrhea 35%

Results• Mean % days abstinent-• Only significant change was in no CBI/
naltrexone v. placebo- 80.6 v 75.1 p=.009• In no comparison was acamprosate better
than placebo.• CBI/naltrexone was no better than placebo


Injectable, sustained release naltrexone…
• Randomized, double-blind, placebo controlled 6 month trial of 624 subjects.
• 3 treatment groups- placebo, depot naltrexone 190 mg or 380 mg.

Copyright restrictions may apply.
Garbutt, J. C. et al. JAMA 2005;293:1617-1625.
Median Heavy Drinking Days per Month for Each Treatment Group Overall and by Sex

Author conclusions
• “Long acting naltrexone was well tolerated and resulted in reductions in heavy drinking”
• “These data indicate that long acting naltrexone can be of benefit in the treatment of opoid dependence”


Study 1
• Multi-center randomized double blind placebo controlled study of 1210 smokers who received 12 weeks of either placebo or varenciline 1mg 2x/day
• Outcome measures- abstinence for weeks 13-24 and weeks 13-52. (Subjects on varenicline who were abstinent for at least 7 days at week 12 were re-randomized to receive placebo or varenicline for another 12 weeks)

Study 1 Results
placebo varenicline
Abstinence for weeks 13-24
49.6% 70.5%
p<.001
Abstinence for weeks 13-52 (if successful for >7 days before week 13)
36.9% 43.6%
p=.02


Study 2
• Double-blind placebo controlled multi-center study of 12 weeks of treatment with placebo, buproprion 150 2x/day and vareniciline 1mg 2x/day in 1025 smokers
• Participants could have no more than 3 months abstinence in past year and could not have ever received buproprion before
• Outcome measures- abstinence rates for weeks 9-12 and abstinence at 52 weeks

Study 2- Results
Placebo buproprion varencline
Abstinence weeks 8-12
17.7% 29.5% 44.0%
Abstinence weeks 9-52
8.4% 16.1%
(p=.057)
21.9%
(p<.001)