Embed Size (px)
Citation preview
Dr. Khalid Al-Ansari, MD Dr. Mohammed Al-Amri, MD Dr. Robert Hoffman, MD
Nida Siddiqi, PharmD Amr Soliman, PharmD
Third QPEM Conference 11-13th of January 2019
Medication Errors: A Panel Discussion
Disclosure
We do not have any relevant financial relationship with commercial interest
to disclose.
Learning Objectives
During this Panel Discussion, we will:
1. Go over a brief introduction to Medication Errors
a) Statistics
b) Important terms
c) Classification
2. Recognize drug classes at highest risk for Medication Errors
3. Discuss real Medication Errors, and strategies to prevent them in the future
Medication Errors: A Brief Introduction
“To Err is Human”-Institute of Medicine (IOM) Report, 1999
Introduction
What is a “Medication Error” ?
"A medication error is any preventable event that may cause orlead to inappropriate medication use or patient harm while themedication is in the control of the health care professional,patient, or consumer.
Such events may be related to professional practice, health careproducts, procedures, and systems, including prescribing, ordercommunication, product labeling, packaging, and nomenclature,compounding, dispensing, distribution, administration, education,monitoring, and use."
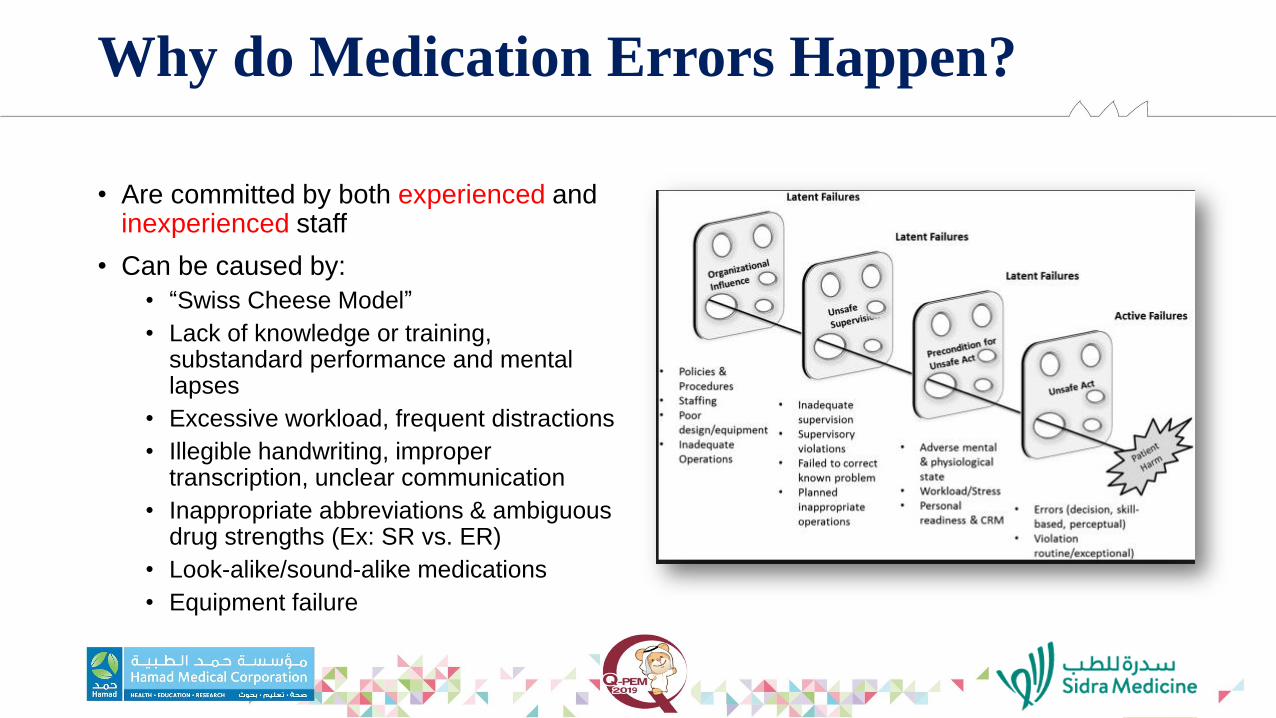
Why do Medication Errors Happen?
• Are committed by both experienced and inexperienced staff
• Can be caused by:
• “Swiss Cheese Model”
• Lack of knowledge or training, substandard performance and mental lapses
• Excessive workload, frequent distractions
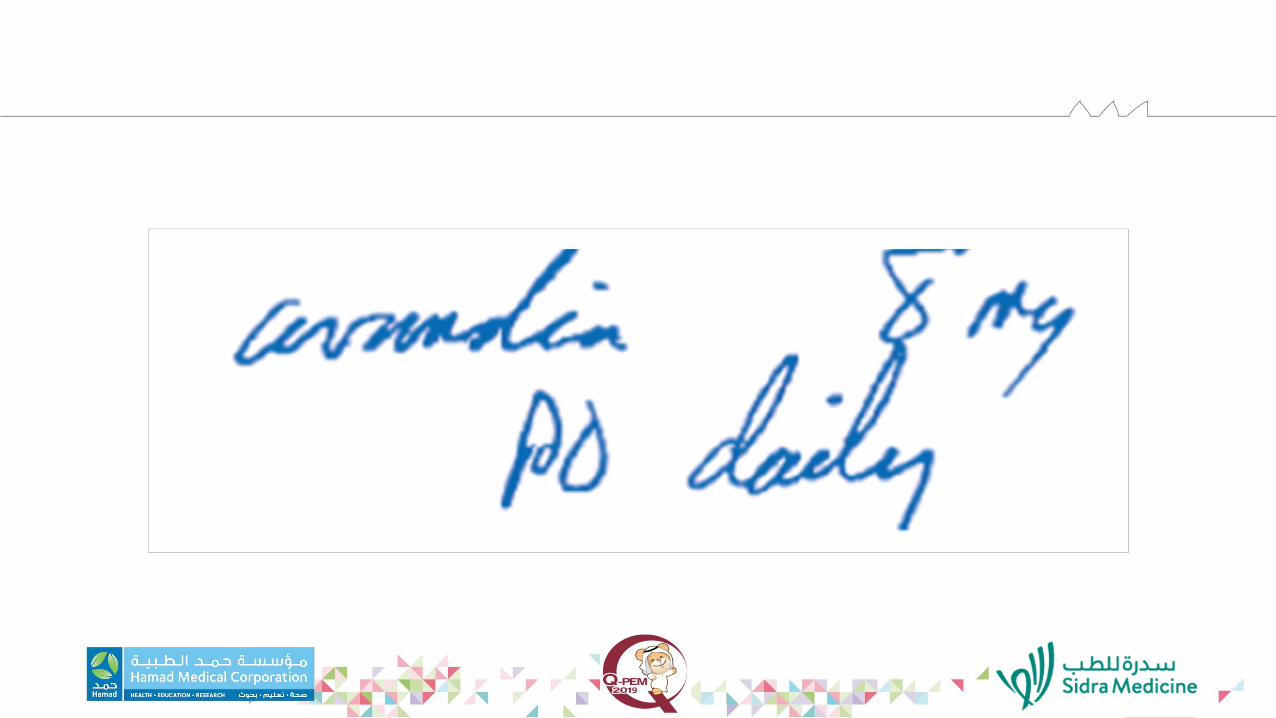
• Illegible handwriting, improper transcription, unclear communication
• Inappropriate abbreviations & ambiguous drug strengths (Ex: SR vs. ER)
• Look-alike/sound-alike medications
• Equipment failure
Impact of Medication Errors
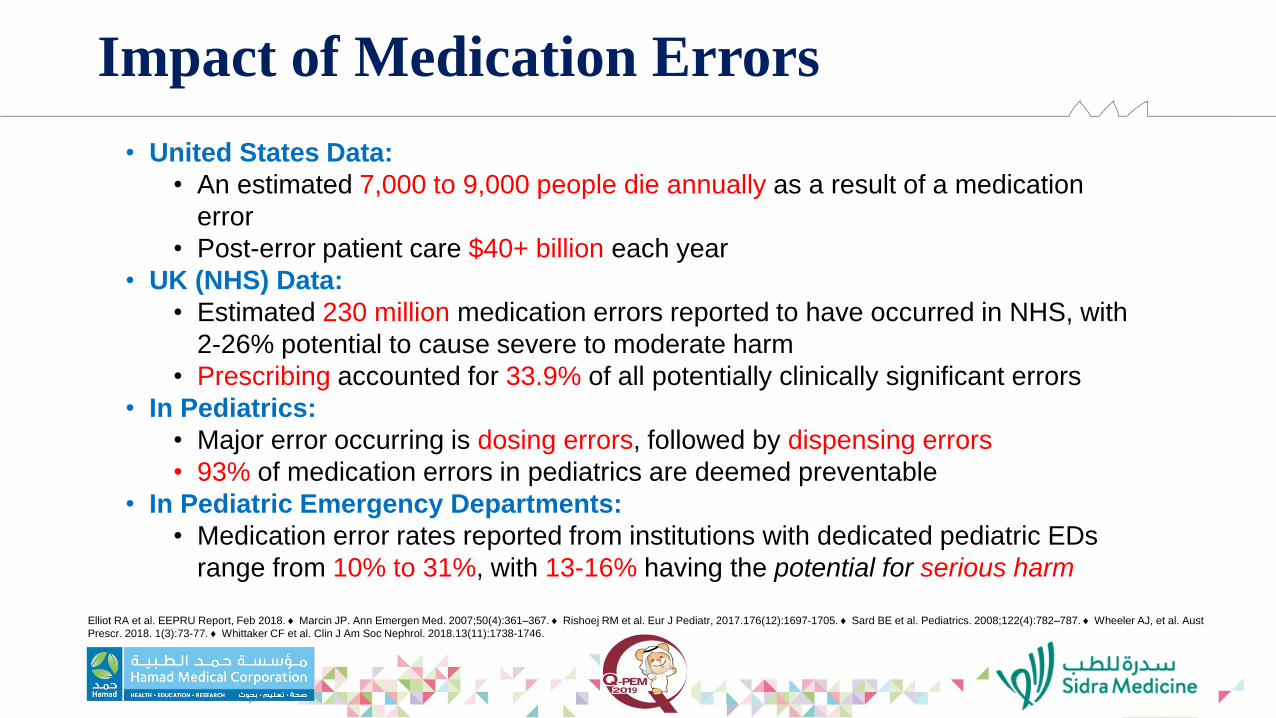
• United States Data:
• An estimated 7,000 to 9,000 people die annually as a result of a medication
error
• Post-error patient care $40+ billion each year
• UK (NHS) Data:
• Estimated 230 million medication errors reported to have occurred in NHS, with
2-26% potential to cause severe to moderate harm
• Prescribing accounted for 33.9% of all potentially clinically significant errors
• In Pediatrics:
• Major error occurring is dosing errors, followed by dispensing errors
• 93% of medication errors in pediatrics are deemed preventable
• In Pediatric Emergency Departments:
• Medication error rates reported from institutions with dedicated pediatric EDs
range from 10% to 31%, with 13-16% having the potential for serious harm
Elliot RA et al. EEPRU Report, Feb 2018. Marcin JP. Ann Emergen Med. 2007;50(4):361–367. Rishoej RM et al. Eur J Pediatr, 2017.176(12):1697-1705. Sard BE et al. Pediatrics. 2008;122(4):782–787. Wheeler AJ, et al. Aust
Prescr. 2018. 1(3):73-77. Whittaker CF et al. Clin J Am Soc Nephrol. 2018.13(11):1738-1746.
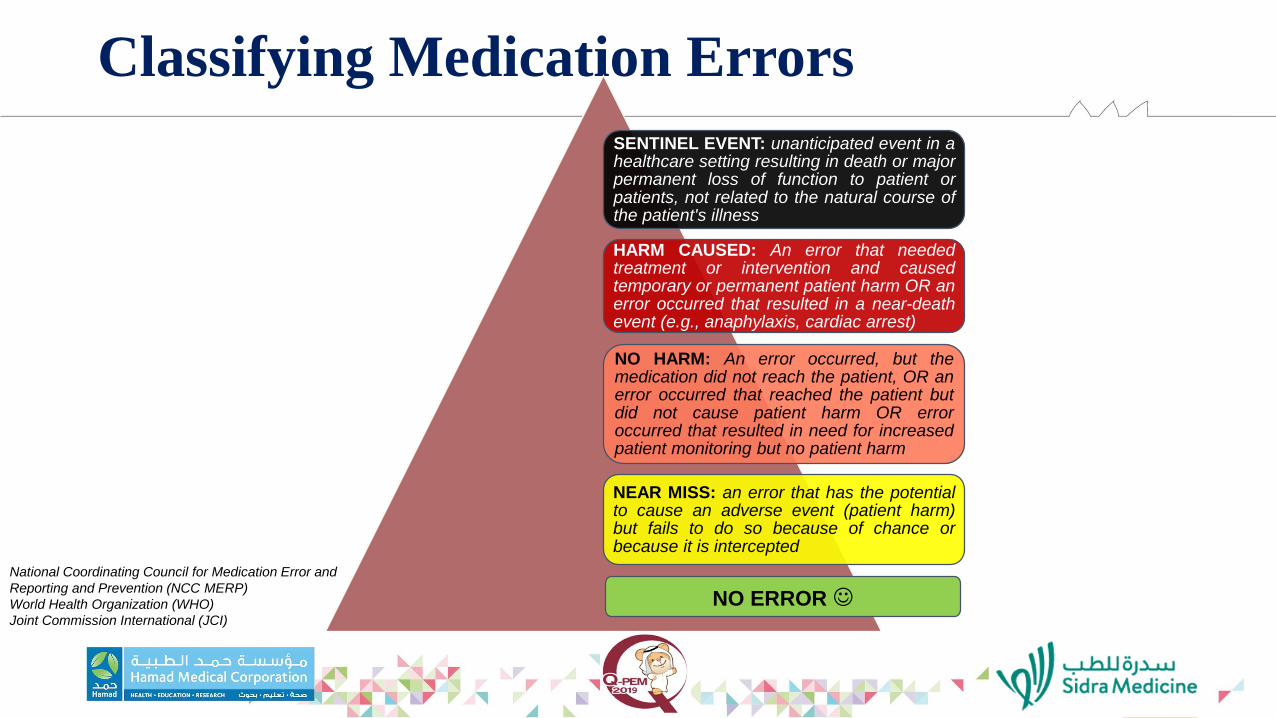
Classifying Medication Errors
SENTINEL EVENT: unanticipated event in a healthcare setting resulting in death or major permanent loss of function to patient or patients, not related to the natural course of the patient's illness
HARM CAUSED: An error that needed treatment or intervention and caused temporary or permanent patient harm OR an error occurred that resulted in a near-death event (e.g., anaphylaxis, cardiac arrest)
NO HARM: An error occurred, but the medication did not reach the patient, OR an error occurred that reached the patient but did not cause patient harm OR error occurred that resulted in need for increased patient monitoring but no patient harm
NEAR MISS: an error that has the potential to cause an adverse event (patient harm) but fails to do so because of chance or because it is intercepted
National Coordinating Council for Medication Error and
Reporting and Prevention (NCC MERP)
World Health Organization (WHO)
Joint Commission International (JCI)
NO ERROR
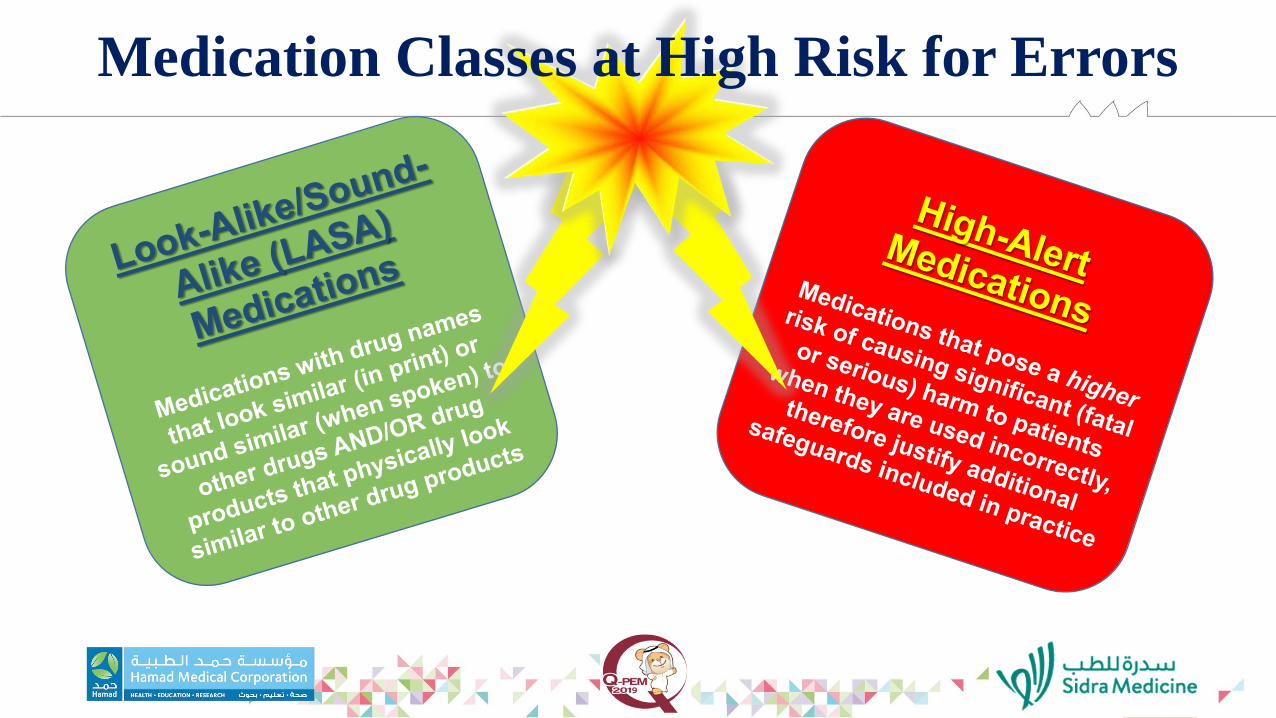
Medication Classes at High Risk for Errors
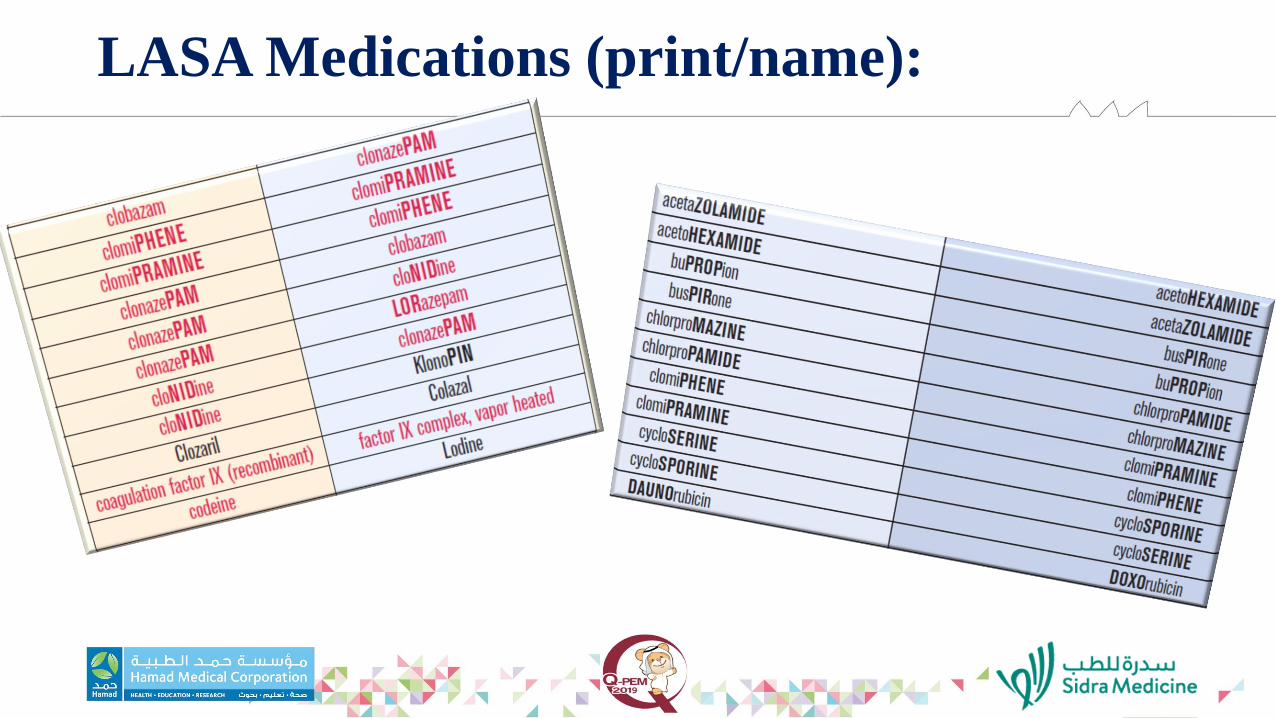
LASA Medications (print/name):

LASA Medications (physical/appearance):

LASA Medications (print, name, and look!)

LASA Medications
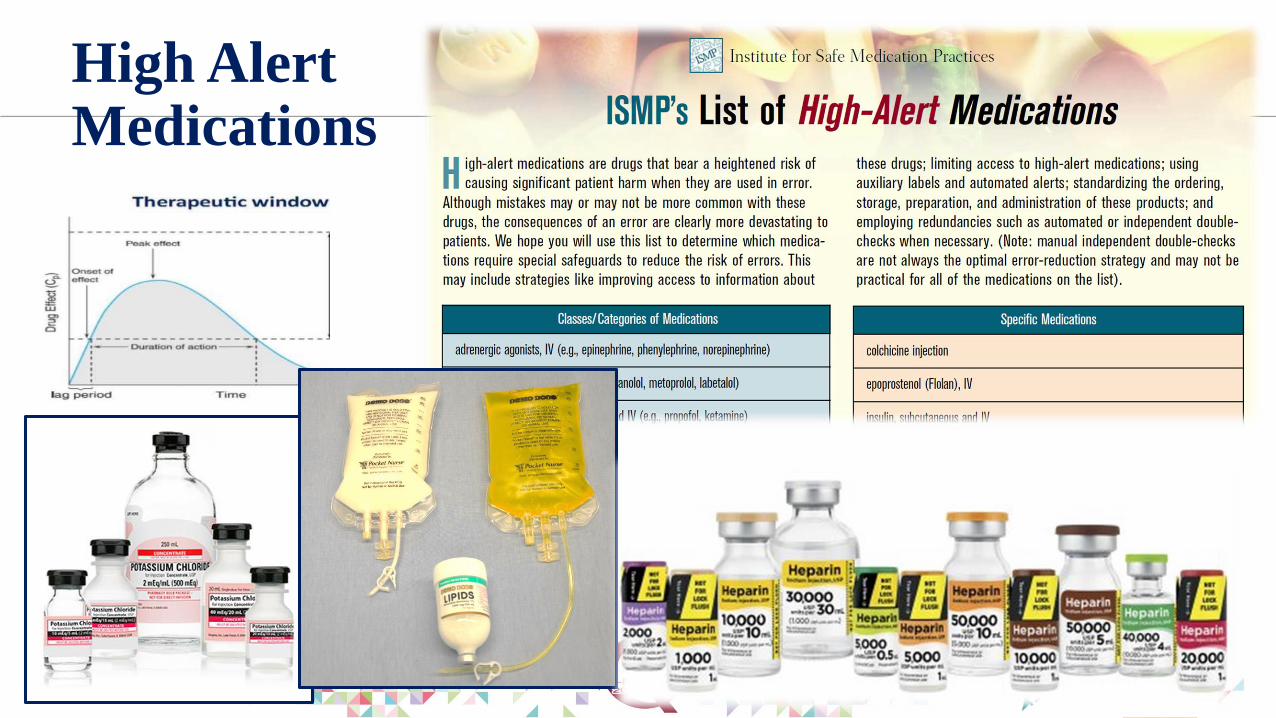
High AlertMedications
Reporting Medication Errors
• PRIMARY GOAL: increase awareness and improve patient safety
• Historical approach:• Retrospective filing of incident report once an error discovered, direct blame on individual
involved
• Current approach: • Retrospective filing of incident report once error discovered with formal investigation, goal to
analyze systems, identify trends, or make recommendations for overall improvements to minimize FUTURE occurrence of same/similar medication errors
• Strategies for improving reporting and outcomes…
“Just Culture” : What–Why–How
• Emily’s Law… Mom’s versus Dad’s perspective
• Definition of “Just Culture”
• Why is it important?
• How do we accomplish it?
https://www.ismp.org/resources/just-culture-and-its-critical-link-patient-safety-part-i
https://www.ismp.org/resources/just-culture-and-its-critical-link-patient-safety-part-ii

Strategies for thePrevention of Medication Errors
CPO-WHAT? I MISS THE GOOD OLD
DAYS… WITH PAPER CHARTS
CPO-WHAT? I MISS THE GOOD OLD
DAYS… WITH PAPER CHARTS
Strategies: CPOE
ADVANTAGES
• (See Previous slide!)
• Online access from anywhere with wi-fi
• Useful monitoring of quality, safety, efficacy (very advanced reports can be generated)
• Useful tools to guide users to safer, better prescribing
• Exchange of information about patients with other healthcare systems
DISADVANTAGES
• Must know how to use the system… and well !!
• Many errors with Copy, Renew & Modify of old orders and progress notes
• Build & Configuration errors will lead to medication errors
• Work-arounds and deviations from proper workflow will lead to medication errors
Strategies: Organization/System
• AVOID BRAND NAMES (especially in an international healthcare system)
• Customized CPOE system with TALLman lettering, High-Alert flagging, Nurse-Witness requirement, standard med admin times, standard IV med concentrations, BarCode Medication Administration (BCMA), Dose Range Checking (DRC), etc.
• Robust, Effective Pharmacy & Therapeutics Committee or similar
• Medication Safety Officer & Quality Improvement Team / Initiatives
• Promoting Just Culture with established systems of reporting/review (Datix, etc.)
• Sufficient and competent staff to perform tasks adequately
• Suitable work environment without frequent distractions
• A 24-hour pharmaceutical service is strongly recommended in hospital settings, with very minimal non-pharmacy preparation of medication
Strategies: Prescribers
• Must follow proper CPOE ordering & documentation process
• Little to NO orally communicated orders (Prostin heard as prostaglandin… epoprostenol versus alprostadil)
• Avoid unapproved abbreviations (o.d. = once daily or right eye?)
• Order dose as strength (mg, mcg, units) rather than volume (mL, tab) when possible
• Use PRN if intend PRN, and include PRN directive
Strategies: Pharmacists
• Must follow proper CPOE medications processes: verification, dispensing, monitoring of therapy, documentation
• Competence is key: must stay abreast of new pharmacotherapeutic trends
• Must follow compounding standards (sterile, non-sterile)
• Culture should encourage:• consultation with Prescribers when there are questions… should never
assume intent of Prescriber then avoid asking
• the constant availability of Pharmacists as drug information resources for all staff and patients/families
• Unless in an emergency or impractical, all orders should be reviewed by a Pharmacist before dispensing, with high risk meds checked by a second Pharmacist
Strategies: Nurses
• Must follow proper CPOE medications processes: administration (especially BarCode Medication Administration), monitoring and documentation, etc.
• Must be very familiar with infusion pumps and other med admin devices
• Nurses should ask “why” and “how” for every patient medication… adequate drug info should be obtained from all available resources
• What is med for? appropriate for my patient? the 5 Rights…
• If dose calls for 22 vials of drug… something is not right
• All medication orders should be reviewed & verified before administration
• Calculations should be double-checked by 2nd nurse, especially if high-alert, over-riding pump/system or other risky scenario
Strategies: Patient / Family / Caregiver
Acetaminophen concentrations Cough & Cold combinations Dosing cup versus oral syringe Graduations on oral syringe Fentanyl, lidocaine and other patches thrown into trash bin or left out on counters (kids and pets play with) Gummy multivitamins and other meds that look and smell like candy left out in the open
Patients/Family/Caregivers should:
• Provide accurate & complete med history information
• Feel free to ask questions about any prescribed treatments
• Learn med names, doses and schedules; best to keep an updated list of current meds and meds they cannot take
• Ensure compliance with prescribed regimens, and should feel free to discuss with their healthcare providers any potential obstacles to compliance

Vignettes: Medication Errors
Error #1 (Emily’s Law) : Discussion
• Etoposide usually diluted in 0.9% sodium chloride (NS)… Pharmacy Technician accidentally used 23.4% sodium chloride as diluent instead, added to empty IV bag along with the etoposide
• 26x the usual sodium concentration for IV administration
• Pharmacist failed to detect the error… was extremely busy, so asked technician if NS was added, and technician replied “Yes”
• This error led to the creation of National Licensure requirement for Pharmacy Technicians throughout the United States
Error #1 (Emily’s Law) : Discussion cont’d
• Trust But Verify !
• High-Alert medications: double-check always required, both for Pharmacy and Nursing
• Pharmacy team was short-staffed when error occurred (over the weekend)
• Pharmacy computer system was down for maintenance (weekend)
• Prescriber entered chemotherapy order as a STAT, causing Pharmacy to rush in processing it
• Mom wanted pharmacist punished… Dad wanted system fixed… which of these would be more effective in protecting the most patients in the future? (concept of Just Culture)
Error #2 : Epinephrine IV Infusion
• Epinephrine infusion prescribed by physician as 4 mg in 50 mL (concentration: 0.08 mg/mL) at 0.05 mcg/kg/minute.
• Order was verified by Pharmacy.
• Nurse placed epinephrine syringe into the infusion pump, but could not find this concentration in the smart pump drug library. She used the pump’s manual input option to input concentration, rate, and patient information.
• The Nurse reported double-checking the rate (herself) and began the infusion.
• 15 minutes into the infusion, patient became distressed and mottled on all four limbs. Consultant was called urgently. As Nurse went to access line the pump alarmed that it is near end of infusion (after only 15 min).
• Pump immediately discontinued and found to have an empty infusion.
Error #2 : Discussion
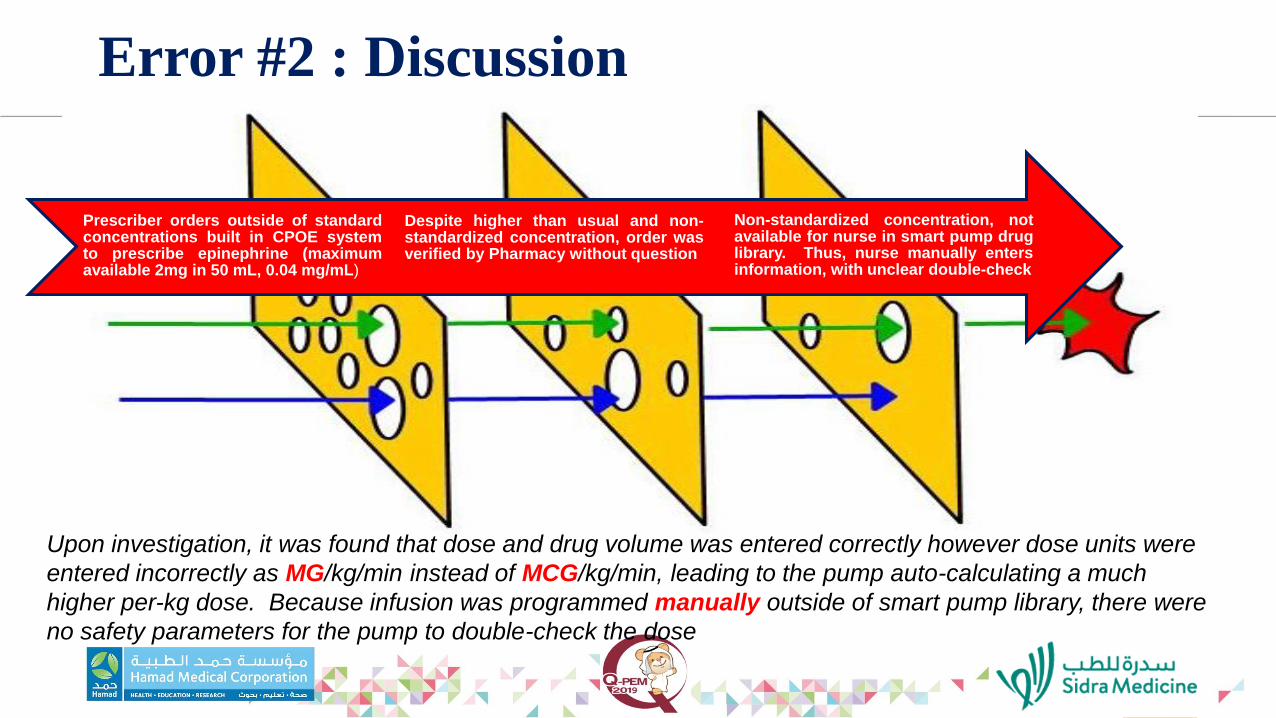
Prescriber orders outside of standardconcentrations built in CPOE systemto prescribe epinephrine (maximumavailable 2mg in 50 mL, 0.04 mg/mL)
Despite higher than usual and non-standardized concentration, order wasverified by Pharmacy without question
Non-standardized concentration, notavailable for nurse in smart pump druglibrary. Thus, nurse manually entersinformation, with unclear double-check
Upon investigation, it was found that dose and drug volume was entered correctly however dose units were
entered incorrectly as MG/kg/min instead of MCG/kg/min, leading to the pump auto-calculating a much
higher per-kg dose. Because infusion was programmed manually outside of smart pump library, there were
no safety parameters for the pump to double-check the dose
Error #3 : Versed® IV-Push
• Patient presents to hospital with vision loss and R/O subdural hematoma; transported to Radiology for a PET scan scheduled at 14:00
• While awaiting scan, patient requests something for claustrophobia-related anxiety
• Prescriber places an order for Versed® 2 mg given IV-push, and order is verified & processed by Pharmacist a few minutes later
• Patient’s assigned Nurse (RN-1) is extremely busy, so RN-2 is requested to obtain & administer medication. RN-2 removes medication vial from the automated dispensing cabinet (ADC) in the ICU using the override function, and heads to Radiology to administer it
• RN-2 administers medication in Radiology and heads back to the ICU
• Shortly thereafter, Prescriber calls for code-blue in Radiology… patient found pulseless and unresponsive in PET scanner…
Error #3 : Discussion
• Back in ICU, RN-1 sees that the medication vial handed to her by RN-2 is actually a vial of VECURONIUM, not VERSED® (midazolam)
• Problems & Prevention:
• Did Prescriber order as brand-name in system? If so, why did system allow that?
• Bar-Code Medication Administration (BCMA) was not performed
• Nurse overriding of medication in ADC
• Staffing issues: RN-2 was the “all-help Nurse” that day, an unofficial role, and did not know patient’s clinical situation (med: why? how? 5 rights); RN-2 was also training an Orientee that day
• RN-2 was looking for “Versed” in ADC medication list, not midazolam. First two letters VE matched vecuronium during search, and both come in 10 mg vial sizes.
• No double-check (nurse-witness) of medication, when both of these meds are High-Alert meds
• Administration of medication not charted in patient’s chart
Error #4 : Digoxin as Outpatient Rx
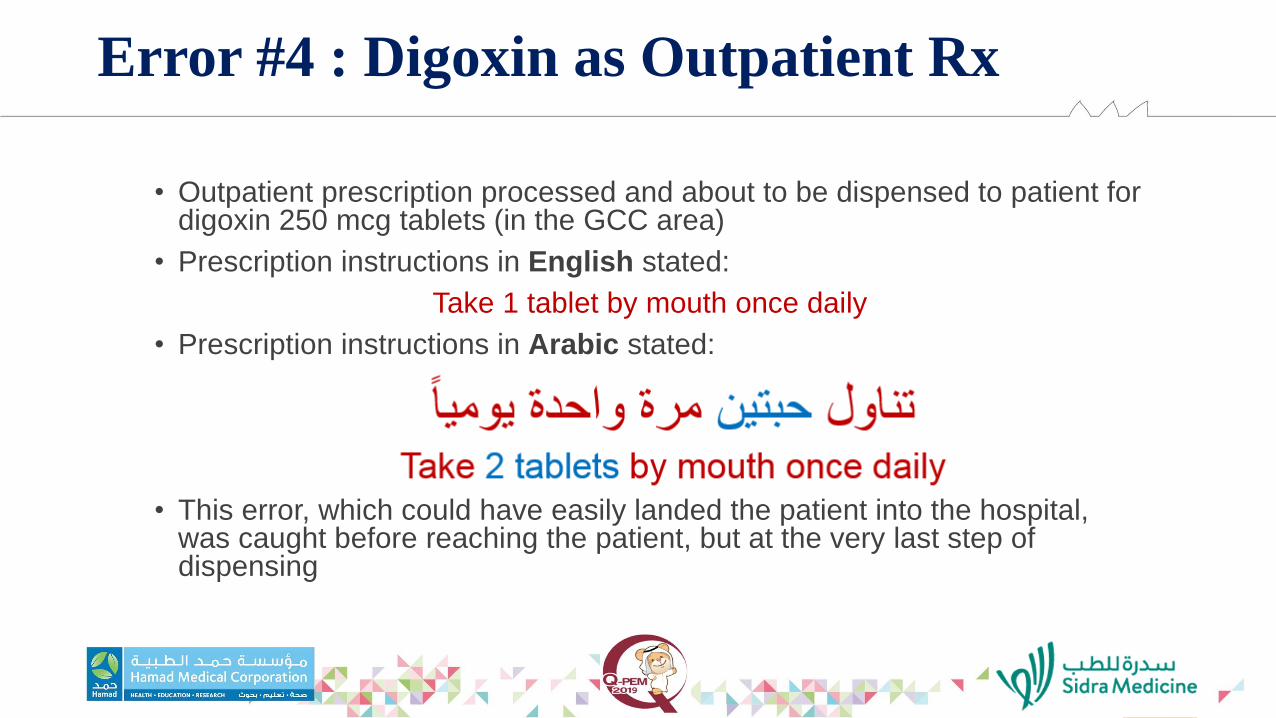
• Outpatient prescription processed and about to be dispensed to patient for digoxin 250 mcg tablets (in the GCC area)
• Prescription instructions in English stated:
Take 1 tablet by mouth once daily
• Prescription instructions in Arabic stated:
• This error, which could have easily landed the patient into the hospital, was caught before reaching the patient, but at the very last step of dispensing
Error #4 : Discussion
• Trust But Verify !
• Know the System !
• The outpatient prescription dispensing system had a flaw in it… it translated English to Arabic correctly if instructions were entered in the “translation” instructions field, but not if entered in another (possible) instructions field
• At initial data entry for the prescription, digoxin 125 mcg tablets were selected for filling this order, using 2 tablets per dose in the correct (translation) instructions field in the system (staff was unaware that the 250 mcg tablets were in stock)
• However, during dispensing, the product selection was changed to 250 mcg tablets, and the dose was changed to 1 tablet in one particular instructions field, but not the translation instructions field
• The company that owns and manages the software was contacted to be made aware of this and provide a fix
Error #5 : Insulin IV Infusion
• Patient with diagnosis of DKA, prescribed an
IV infusion of Regular Insulin
• Pharmacy calls Prescriber back and informed
him/her that the insulin dose as prescribed in
the CPOE system is 100x the usual dose
• How did this happen?
Error #5 : Discussion
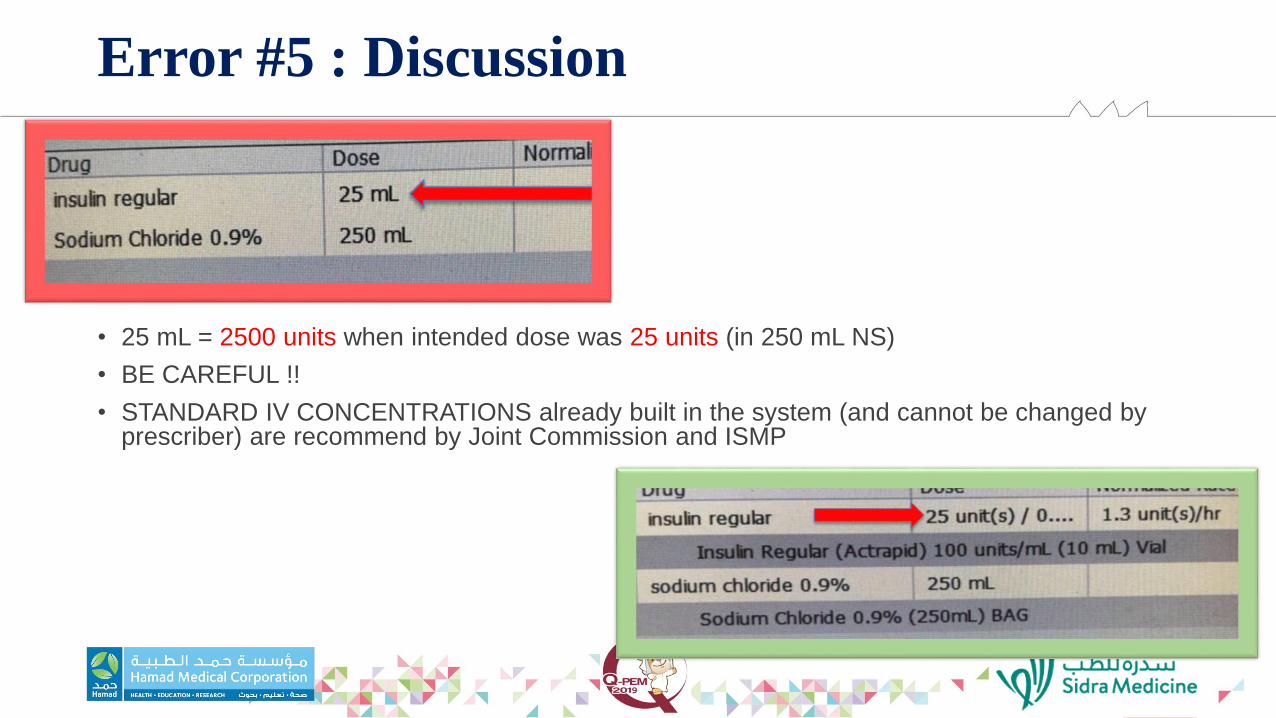
• 25 mL = 2500 units when intended dose was 25 units (in 250 mL NS)
• BE CAREFUL !!
• STANDARD IV CONCENTRATIONS already built in the system (and cannot be changed by prescriber) are recommend by Joint Commission and ISMP
Error #6 : Vitaros® Cream
• A female patient presents to her general practitioner with symptoms of significant, irritating dry eyes and corneal erosions
• Prescriber writes a hand-written prescription for a topical agent to be applied to the eyes for ophthalmic lubrication
• Patient gets prescription filled, and begins therapy as instructed
• A few days later, she is seen in the Emergency Department with significant eye pain, blurred vision, redness and swollen eyelids.
Error #6 : Discussion
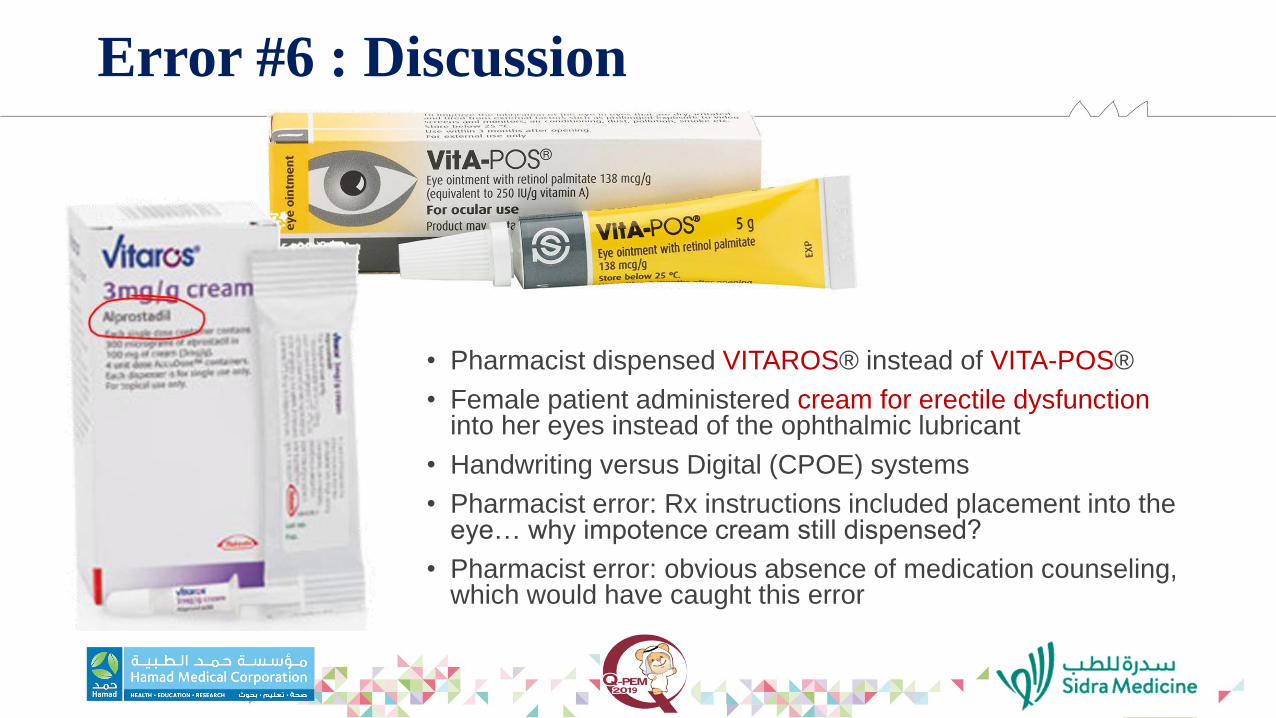
• Pharmacist dispensed VITAROS® instead of VITA-POS®
• Female patient administered cream for erectile dysfunction into her eyes instead of the ophthalmic lubricant
• Handwriting versus Digital (CPOE) systems
• Pharmacist error: Rx instructions included placement into the eye… why impotence cream still dispensed?
• Pharmacist error: obvious absence of medication counseling, which would have caught this error

Error #7 : Diazepam IV-Push
• 8 week old patient presents to ED in with C/O colic
• Normal vitals, normal exam, but then has a seizure in the ED
• IV started, diazepam 0.1 mg/kg ordered and medication administered
• Patient proceeds to have respiratory arrest, intubated, planned for PICU admission.
• Chief Pediatric Resident Physician comes to ED to examine patient before PICU admission, and notices pinpoint pupils
• pinpoint pupils + respiratory arrest = gives NALOXONE
• patient wakes up immediately
Error #7 : Discussion
• Urine drug test repeated twice, was positive for opioids both times
• Multiple drug tests for benzodiazepines were negative
• Intensive interrogation of parents due to family is from Afghanistan (patient with colic, leading to question of opium use in patient by parents); parents deny, Mom’s urine drug tests are negative, breast milk tests are negative (uncertain about father’s testing)
• Patient admitted to PICU, family loses custody of the child pending investigation
• Hospital investigation: ADC and pharmacy records confirm drawer storing MORPHINEwas accessed, and a morphine med count discrepancy occurred that same shift
• Prevention:• ED environment: panic, hectic… must routinely reset back to calm, cool, collected
environment
• Some ED’s have implemented BCMA… saves lives
• Double-check (nurse-witness) for all High-Alert and High-Risk medications
• Minimize as much as possible the overriding of medications from the ADC (Pharmacist verification needed to prevent overriding)
• Flag LASA meds with LASA labels

Error #7 : Discussion cont’d

Take-HomePoints
Take-Home Points
• KNOW THE SYSTEM… how to use and why !!
• Medication Errors are VERY PREVENTABLE, especially in the PEDIATRIC population
• Swiss Cheese events: make sure all safety events are in place and UTILIZED
• Just Culture: INCREDIBLY important, or else errors will continue to be repeated
• TRUST BUT VERIFY…
• Automation
• Peers
• Own practice / performance
• Many EFFECTIVE strategies are available but need to be implemented & supported
• Sufficient staff needed, who are competent in their fields, to work in a safe, controlled environment that is free from excessive distraction
• PATIENT SAFETY is the responsibility of each and every one of us, including parents, family and caregivers

Thank You!