Embed Size (px)
Citation preview
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable external content.
Diagnosis and Management
Dr K Govender
Gastroenterologist
Medication for IBD – What’s new?
Dr Kugan Govender
Gastroenterologist
Entabeni Hospital
Durban
Inflammatory Bowel Disease (IBD)
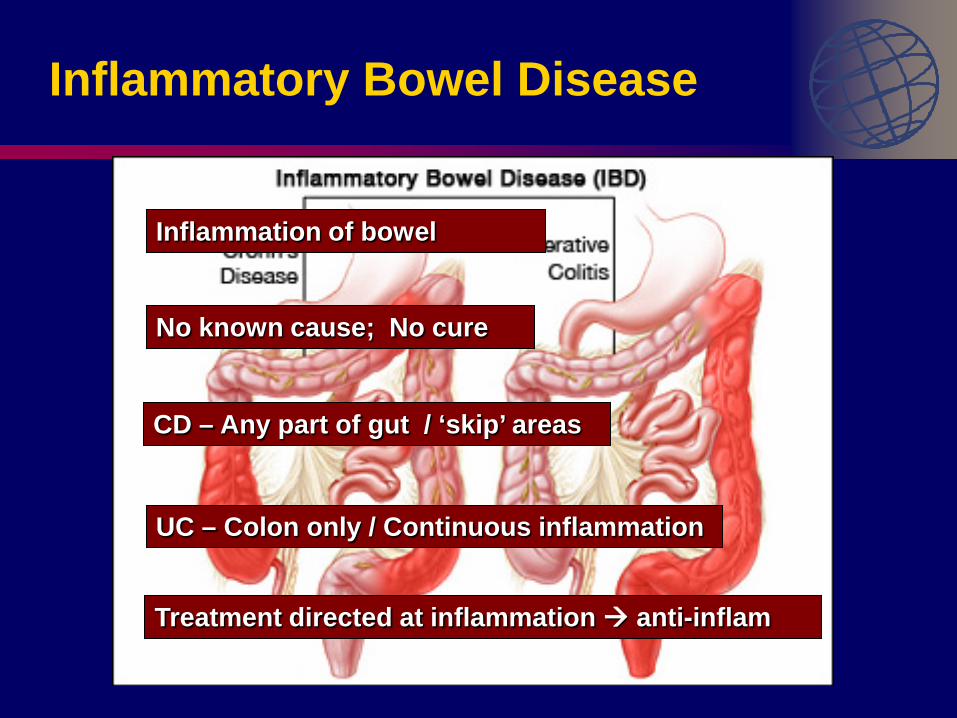
Inflammatory Bowel Disease
Inflammation of bowel
No known cause; No cure
CD – Any part of gut / ‘skip’ areas
UC – Colon only / Continuous inflammation
Treatment directed at inflammation anti-inflam
Overview Goals of treatment?
Currently available medications for IBD?
How do we use IBD drugs?
Which treatment to use?
How to optimise current medical therapy?
Newer treatment strategies?
New IBD drugs?
Future concepts?
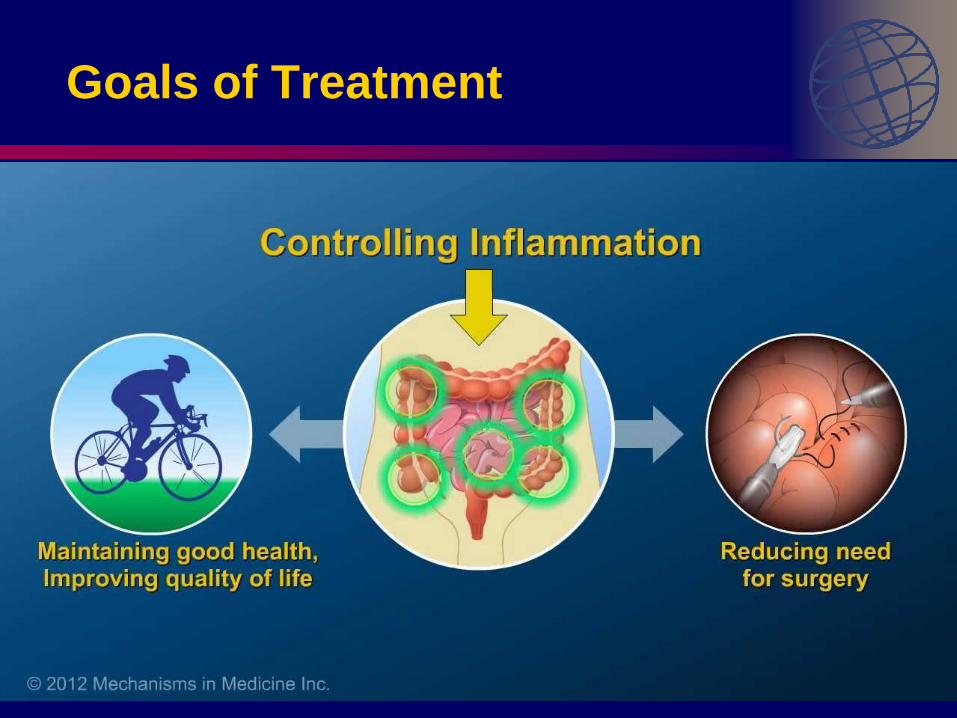
Goals of Treatment
Doctor
Healing of the intestine
Prevent long-term complications of IBD
Drug safety
Patient
Feel healthy
No drug side effects
Medication that is simple to use
Avoid surgery

Goals of Treatment
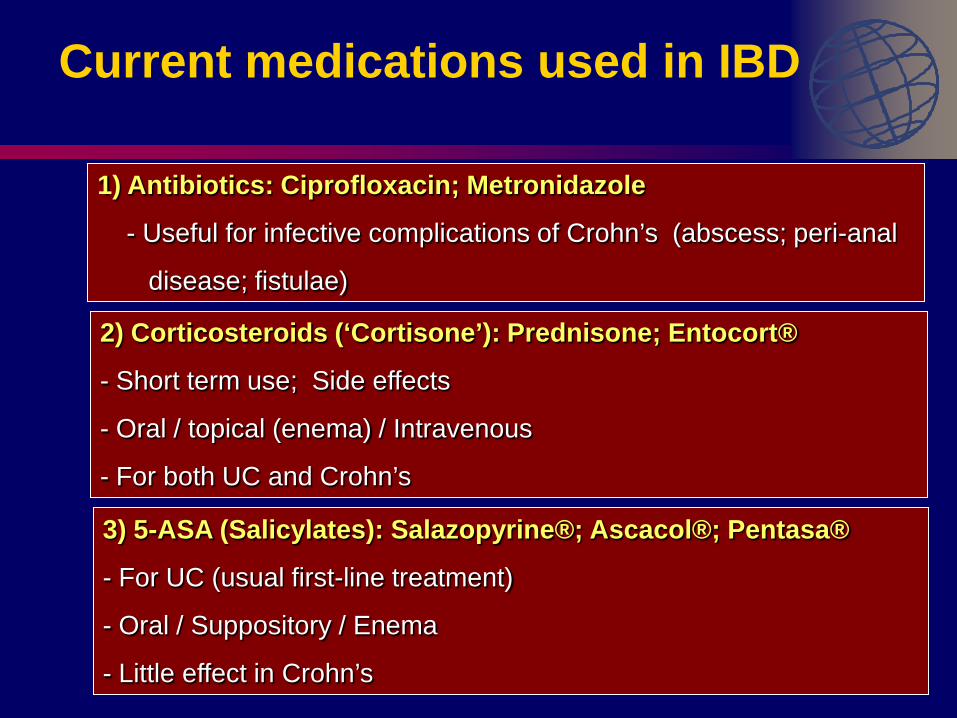
Current medications used in IBD
1) Antibiotics: Ciprofloxacin; Metronidazole
- Useful for infective complications of Crohn’s (abscess; peri-anal
disease; fistulae)
2) Corticosteroids (‘Cortisone’): Prednisone; Entocort®
- Short term use; Side effects
- Oral / topical (enema) / Intravenous
- For both UC and Crohn’s
3) 5-ASA (Salicylates): Salazopyrine®; Ascacol®; Pentasa®
- For UC (usual first-line treatment)
- Oral / Suppository / Enema
- Little effect in Crohn’s
Current medications used in IBD
4) Immune-modulators: Azapress®; Azamun®; Puri-Nethol®;
Methotrexate
- Useful in both UC and Crohn’s
- ‘Steroid sparing’
- Takes 2-4 months to work
5) Biologicals (Anti-TNF): Revellex®; Humira®
- For both UC and Crohn’s
- Most effective therapy in IBD
- Reserved for severe disease
Why are they called Biologicals?
Products made from natural sources – human / animal etc
Produced by biotechnology
Expensive to make
Your immune system can “react to them” TNF-α (Tumor necrosis factor) is a key player in the immune response in IBD
Common IBD biologics – are antibodies against TNF-α (therefore Anti-TNF) NB: Risk of infections while on Biologics
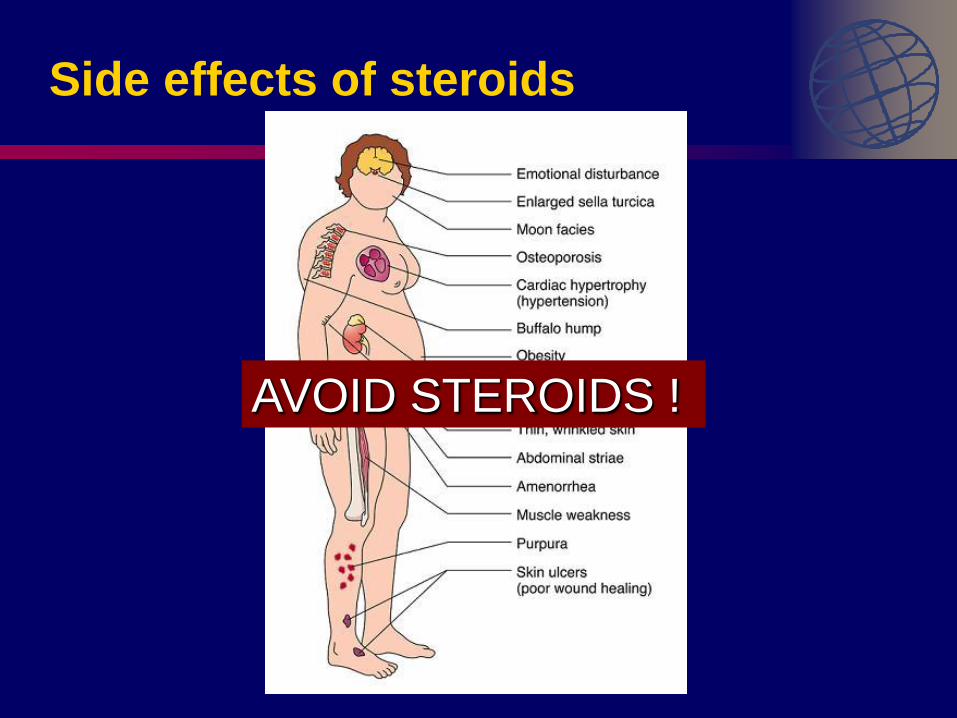
Side effects of steroids
AVOID STEROIDS !
How do we use IBD drugs?
2 phases of treatment: 1) Induce Remission - Steroids (Prednisone; Budesonide) - Biologics (Revellex® ; Humira®) 2) Maintain Remission - 5-ASA (Pentasa®; Asacol®) - Immune-modulators (Azapress®; Methotrexate) - Biologics
INDUCTION
MAINTENANCE
Which treatment to use?
Crohn’s or Ulcerative Colitis? Extent (How much bowel involved?) Severity (How bad is it?) Age / Sex Personal preference Other illnesses / chronic disease
How do we optimise current drug therapy?
1) Right drug for the right patient
Individualise treatment Tailor according to your symptoms / severity / extent /
other illnesses / affordability Adequate dosage Try to avoid / reduce steroids
Optimising treatment
2) Optimising 5-ASA treatment (Pentasa®; Asacol®; Mezavant®)
Useful for Ulcerative Colitis Patients don’t usually take the drugs (poor compliance due to frequent dosing) Once daily equivalent to 3 times daily (better compliance) Combining oral tablets with enema / suppository useful Modified release tabs available (Mezavant)
Optimising treatment
3) Optimising use of Azathioprine (and 6-MP)
Thiopurine methyltransferase activity (TPMT) 1 in 300 patients may have severe bone marrow suppression with Azathioprine (Azapress®) TPMT level predicts who will have suppression Low level Cannot use Azathioprine
Optimising treatment
4) Combination therapy
Drugs act together to control disease Biologics + Immune-modulator 5-ASA + Immune-modulator Reduce need for steroids
Reduce overall side effects
Optimising treatment
5) Monitoring disease and predicting flares
Blood markers (CRP)
Stool markers (Calprotectin) Monitoring of Biologic (Anti-TNF levels)
Monitoring of Azathioprine (6-TGN levels)
Newer Treatment Strategies
“Step-up” Treatment Early “Top-down”
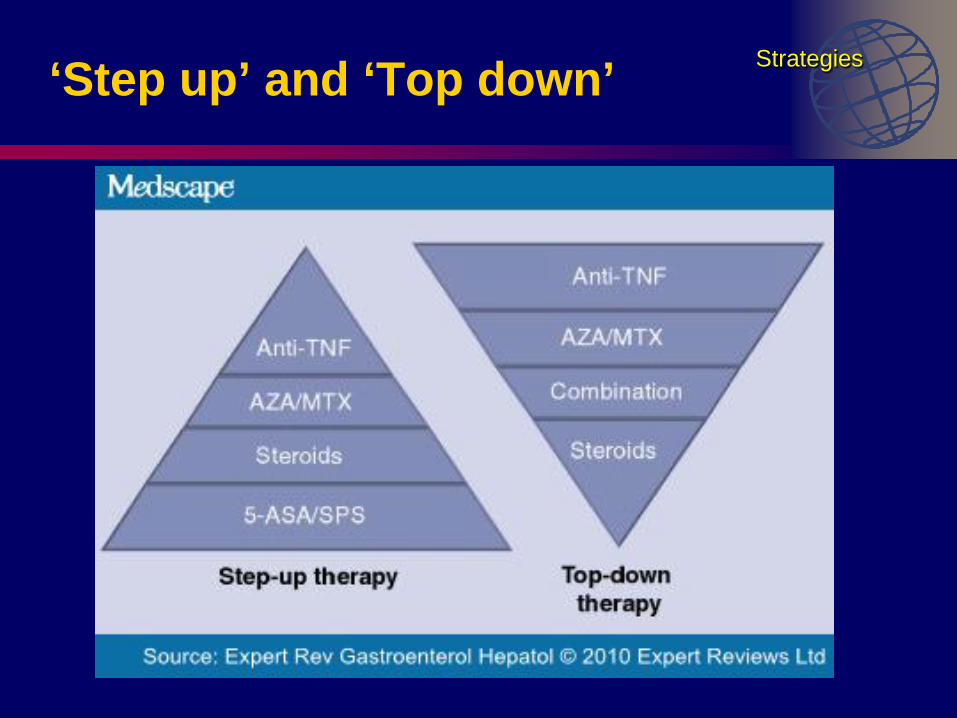
‘Step up’ and ‘Top down’ Strategies
Step-up treatment
- Start with steroids / 5-ASA - Then add on immune-modulator if no response - Biological agents later if no response
Strategies
Early top-down
- Start with Biological agent and immune-modulator at outset
- Taper treatment as required
- May be considered for: - Severe disease on presentation - Early onset (<40 yrs) - Extensive disease - Peri-anal / fistulising - Involvement of areas outside of the bowel
Strategies
New drugs for IBD
1) Golimumab (Simponi®) 2) Vedolizumab (Entyvio®) 3) Biosimilars
Golimumab (Simponi ®)
- Human antibody (similar to Humira®)
- Now approved for UC in South Africa
- Subcutaneous injection
- 4 weekly injections
- Similar side effect profile to other biologics
New drugs
Vedolizumab (Entyvio ®)
- Biologic - Not Anti-TNF; Specific drug designed for IBD
- Blocks receptors on inflammatory cells
- Prevents adhesion of the inflammatory cells to the wall of
blood vessels
- Prevents inflammatory cells from reaching the gut mucosa
- Useful in patients who have failed on other treatments
New drugs
Biosimilars
- Generic biologics
- Not available yet
- Lower cost?
- Similar efficacy?
- Greater affordability may make biosimilars available to more patients
New drugs
Future concepts?
“Mongersen” - Oral Biologic agent - Fast acting with response within 2 weeks - Longer trial required
Ongoing trials
Multiple drugs / pathways
Take home messages
Avoid steroids Use of drugs in combination / at correct dose
Markers to predict inflammation / flare
Once daily use of 5-ASA drugs works
Combining oral and topical 5-ASA effective TPMT activity prior to starting Azathioprine Step up vs Top down tailor treatment for individual patient
Vedolizumab – new exciting biologic