Embed Size (px)
Citation preview
3/23/2015
1
Medications Update – New and Emerging Therapies
WADE 2015 Annual Conference: Pathways to Positive Outcomes
Joshua J. Neumiller, PharmD, CDE, FASCPAssociate ProfessorDepartment of PharmacotherapyWashington State University
Disclosures to Participants
Conflicts of Interest and Financial Relationships Disclosures:
Presenter:
Joshua J. Neumiller, PharmD, CDE, FASCP - Speakers Bureau: Janssen Pharmaceuticals, Novo Nordisk; Advisory Board: Janssen Pharmaceuticals, Sanofi; Research Grant Support to WSU: AstraZeneca, Johnson & Johnson, Merck, Novo Nordisk.
Sponsorship / Commercial Support: None.
Non-Endorsement Of Products:
Accredited status does not imply endorsement by AADE, ANCC, ACPE or CDR of any commercial products displayed in conjunction with this educational activity.
Off-Label Use:
Participants will be notified by speakers to any product used for a purpose other than that for which it was approved by the Food and Drug Administration.
Learning Objectives
1. Identify new and emerging therapies for the treatment of diabetes mellitus;
2. Compare and contrast efficacy and safety data for SGLT-2 inhibitors currently available and in late-stage development; and
3. Discuss new and emerging insulin therapies and their potential place in therapy among currently available insulin products;
4. Outline emerging GLP-1 receptor agonist therapies and their potential role in combination therapy for people with type 1 and type 2 diabetes.
Pathophysiology of T2DM: The Ominous Octet
DeFronzo RA, Triplitt CL, et al. Diabetes Spectrum 2014;27(2):100-112.
ADA Standards of Medical Care in Diabetes – 2015. Diabetes Care. 2015.
SGLT-2 Inhibition
Glucose
Glomeruli
Blood Vessel
SGLT1
SGLT2
SGLT2 Inhibitor Urine
SGLT1
Small Intestine
Idris I, et al. Diabetes Obes Metab. 2009.
Inhibition of SGLT2 transporters in the proximal tubule blocks the reabsorption of filtered
glucose = increased glucose excretion via urine.
3/23/2015
2
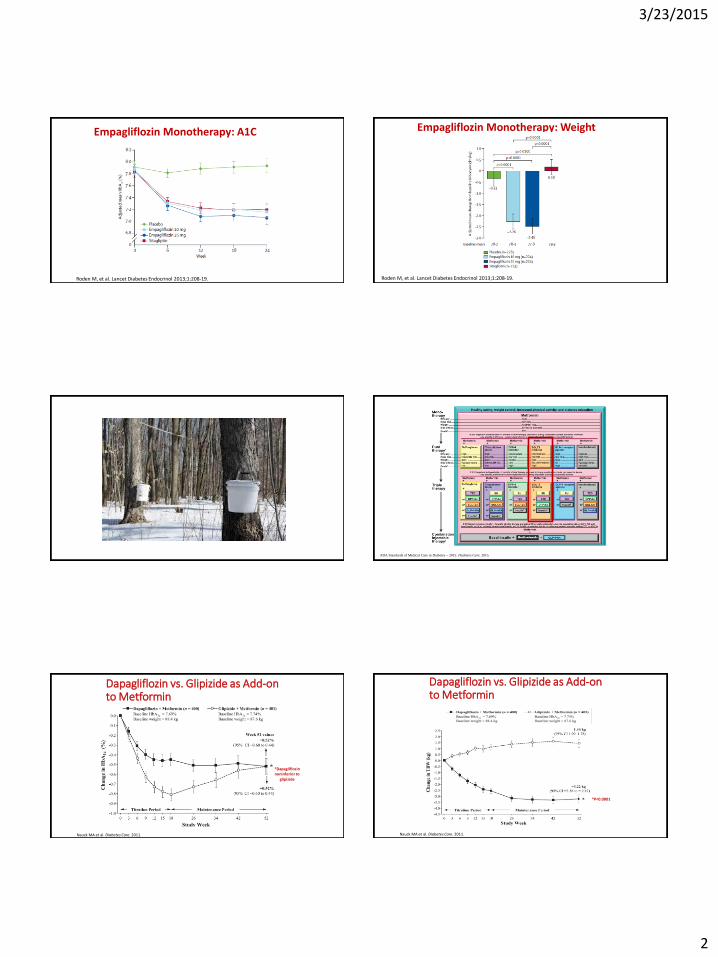
Empagliflozin Monotherapy: A1C
Roden M, et al. Lancet Diabetes Endocrinol 2013;1:208-19.
Empagliflozin Monotherapy: Weight
Roden M, et al. Lancet Diabetes Endocrinol 2013;1:208-19.
ADA Standards of Medical Care in Diabetes – 2015. Diabetes Care. 2015.
Dapagliflozin vs. Glipizide as Add-on to Metformin
Nauck MA et al. Diabetes Care. 2011.
*Dapagliflozinnoninferior to
glipizide
Dapagliflozin vs. Glipizide as Add-on to Metformin
Nauck MA et al. Diabetes Care. 2011.
*P<0.0001*

3/23/2015
3
Canagliflozin versus Glimepiride as add-on to MET: A1C
Cefalu WT, et al. Poster presented at: The 73rd Scientific Session of the ADA, June 21-25, 2013, Chicago, IL.
Canagliflozin versus Glimepiride as add-on to MET: Weight
Cefalu WT, et al. Poster presented at: The 73rd Scientific Session of the ADA, June 21-25, 2013, Chicago, IL.
Canagliflozin and eGFR
Yale J, et al. Poster presented at: The 73rd Scientific Session of the ADA, June 21-25, 2013, Chicago, IL.
SGLT-2 Inhibitor Comparison/Contrast
Characteristic Canagliflozin Dapagliflozin Empagliflozin
Hypoglycemia Risk (monotherapy)
Low Low Low
Dose 100 mg daily before breakfast, Increase to
300 mg daily if needed
5 mg daily in the AM; Increase to 10 mg
daily if needed
10 mg daily in the AM; Increase to 25 mg if
needed
Weight Loss Loss Loss
SGLT-2 Inhibitors: Renal Dosing
Canagliflozin Prescribing Information. 2013.Dapagliflozin Prescribing Information. 2014.Empagliflozin Prescribing Information. 2014Woo V, et al. Poster presented at: The 73rd Scientific Session of the ADA, June 21-25, 2013, Chicago, IL.Kohan DE, et al. Kidney Int. 2013; doi: 10.1038/ki.2013.356. [Epub ahead of print]
Agent Dosing in CKD stages 3, 4 and 5 (non-dialysis)
Canagliflozin • eGFR ≥ 60 ml/min/1.73m2
No dosage adjustment needed• eGFR 45—59 ml/min/1.73m2
Do not exceed 100 mg/day PO• eGFR < 45 ml/min/1.73m2
Do not initiate and discontinue in patients currently receiving drug
Dapagliflozin Do not initiate and discontinue with eGFR <60 mL/min/1.73 m2
Empagliflozin • eGFR ≥ 45 ml/min/1.73m2
No dosage adjustment needed• eGFR < 45 ml/min/1.73m2
Do not initiate and discontinue in patients currently receiving drug

3/23/2015
4
Canagliflozin Efficacy
Woo V, et al. Poster presented at: The 73rd Scientific Session of the ADA, June 21-25, 2013, Chicago, IL.
SGLT-2 Late Developmental Pipeline
Agent Lead Company Phase
Ipragliflozin (ASP1941) Astellas Pharma 3
Luseogliflozin (TS071) Taisho Pharmaceutical 3
Tofogliflozin (CSG452) Chugai, Kowa, Sanofi 3
Ertugliflozin (PF-04971729) Pfizer, Merck & Co. 3
Sotagliflozin* Lexicon Pharmaceuticals 3
Nauck MA. Drug Design, Development and Therapy 2014;8:1335-1380.Bays H. Diabetes Ther 2013;4:195-220.Misra M, et al. JPP 2013;65:317-327.
*Dual SGLT-1/SGLT-2 Inhibitor
SGLT-2 Inhibitor Key Points• Unique MOA – have been studied in combination
with a variety of other medication classes• Oral administration• Low hypoglycemia risk as monotherapy – caution
when used with secretagogues or insulin• Can result in some weight loss and modest
decrease in BP• Common SE’s to be aware of:
– Genital mycotic infections – Lower UTIs– Urinary urgency– Orthostasis (especially in elderly, CKD, diuretic use)
• Watch volume status
New and Emerging Insulin Products
0 2 4 6 8 10 12 14 16 18 20 22 24
Pla
sm
a I
nsu
lin
Levels
Regular (6–10 hr)
NPH (10–20 hr)
Time (hr)
Glargine (~24 hr)
Aspart, Lispro, Glulisine, (4–5 hr)
Rosenstock J. Clin Cornerstone. 2001;4:50-61.
Detemir once daily(~24 hr)
Technosphere Insulin- Kinetics Curve
Technosphere Insulin Package Insert. 2014.
3/23/2015
5
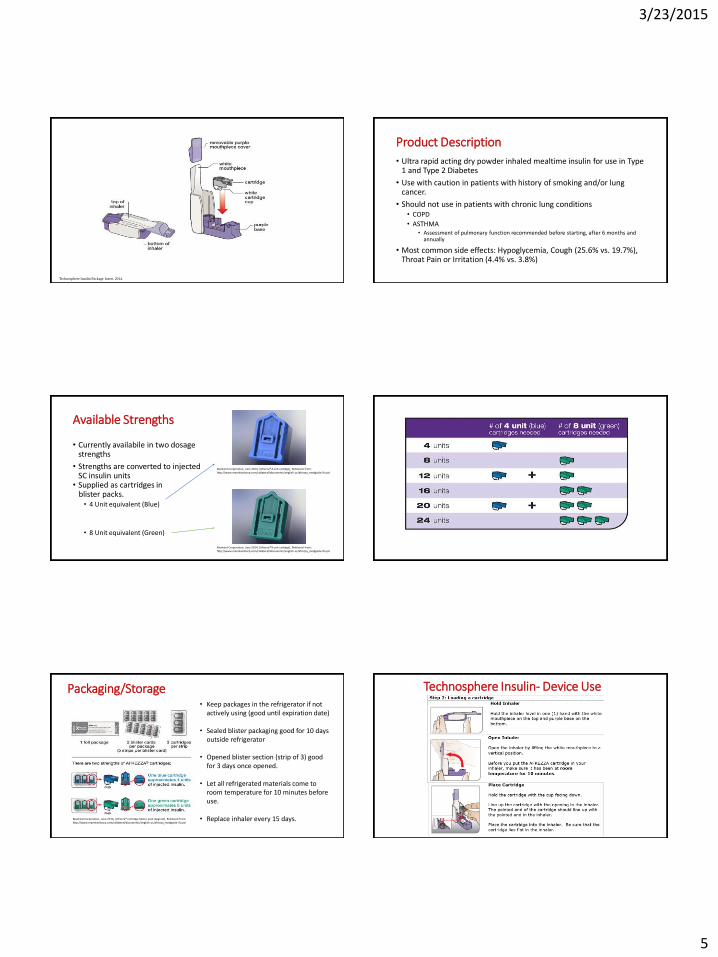
Technosphere Insulin Package Insert. 2014.
Product Description
• Ultra rapid acting dry powder inhaled mealtime insulin for use in Type 1 and Type 2 Diabetes
• Use with caution in patients with history of smoking and/or lung cancer.
• Should not use in patients with chronic lung conditions• COPD
• ASTHMA• Assessment of pulmonary function recommended before starting, after 6 months and
annually
• Most common side effects: Hypoglycemia, Cough (25.6% vs. 19.7%), Throat Pain or Irritation (4.4% vs. 3.8%)
Available Strengths
• Currently availabile in two dosage strengths
• Strengths are converted to injected SC insulin units
• Supplied as cartridges in blister packs.
• 4 Unit equivalent (Blue)
• 8 Unit equivalent (Green)
Mankind Corporation, June 2014, [Afrezza® 4 unit cartidge], Retrieved from: http://www.mannkindcorp.com/collateral/documents/english-us/afrezza_medguide-ifu.pd
Mankind Corporation, June 2014, [Afrezza® 8 unit cartidge], Retrieved from: http://www.mannkindcorp.com/collateral/documents/english-us/afrezza_medguide-ifu.pd
Packaging/Storage• Keep packages in the refrigerator if not
actively using (good until expiration date)
• Sealed blister packaging good for 10 days outside refrigerator
• Opened blister section (strip of 3) good for 3 days once opened.
• Let all refrigerated materials come to room temperature for 10 minutes before use.
• Replace inhaler every 15 days.Mankind Corporation, June 2014, [Afrezza® cartridge blister pack diagram], Retrieved from: http://www.mannkindcorp.com/collateral/documents/english-us/afrezza_medguide-ifu.pd
Technosphere Insulin- Device Use

3/23/2015
6
Technosphere Insulin- Device Use Technosphere Insulin- Device Use
Other Select Emerging Prandial Insulins
• U200 Lispro – currently approved in Europe
• Pen device holds 3 mL of insulin – 600 total units per pen
• Possibly target people on larger volumes of mealtime insulin
• Faster-acting Insulin Aspart (FIAsp)
http://www.pipelinereview.com/index.php/2014100355623/Proteins-and-Peptides/European-Commission-Grants-Marketing-Authorisation-to-Humalog-200-units/ml-KwikPen-Insulin.html?utm_source=Closer+Look+Subscribers+2013&utm_campaign=5fbbdddc71-2014-10-03_%28HTML_LINKS%29_Intarcia%3B_Humal10_03_2014&utm_medium=email&utm_term=0_c55d924bf1-5fbbdddc71-411756565
U-300 Insulin Glargine• When compared to U-100 glargine, similar efficacy with less risk of
hypoglycemia
Bolli GB, et al. EDITION 3. Diabetes, Obesity and Metabolism. 2015;17:386-394.
U300 Insulin Glargine
• Type 2 DM (EDITION 1)• U300 Glargine vs. U100 Glargine in PM• Open label, 2 arm, parallel group over 1 year• End of Study
• U300- 1.03units/kg/day vs. U100- 0.9units/kg/day
Outcome U300 U100 P value
HbA1c (%) -0.86 -0.69 0.0074
FPG (mg/dl) -29.6 -26.0 NS
Weight (kg) 1.17(0.8-1.5) 1.4 (1.1-1.8) NS
Hypoglycemia
Severe 6.7% 7.5% ---
Any* 74.8% 82.8% RR 0.9(0.84-0.97)
Nocturnal** 44.6% 57.2% RR 0.78(0.68-0.89)
*<70mg/dl with symptoms; **Same definition, between 00:00-05:59hourRiddel MC, et al. Diabetes Care 2014;37(10):2755-2762.
U-300 Insulin Glargine: Determining Starting Dose
www.toujeopro.com
Prior Treatment: Start with:
Once-daily basal insulin 1:1 conversion
Twice-daily NPH 80% of total daily NPH dose
No current basal insulin 0.2 units/kg
• Available in SoloStar® Pen

3/23/2015
7
Long-acting Basal Insulin Analogs in Development
• Insulin degludec
• Phase 3
• Pegylated insulin lispro
• Phase 3
Degludec: Steady Release Occurs for More Than 24 Hours Following Injection
[Zn2+ ]
Insulin degludec
multihexamers
Zinc diffuses slowly, causing individual hexamers to disassemble, releasing
monomers.
Subcutaneous depot
Monomers are absorbed from the depot into the circulation. Slow
release
Jonassen I et al. Pharm Res. 2012;29(8):2104–1214.
BEGIN Basal-Bolus Type 2: A1C Over Time
6.0
6.5
7.0
7.5
8.0
8.5
9.0
0 4 8 12 16 20 24 28 32 36 40 44 48 52
A1
C (
%)
Time (weeks)
Treatment difference: noninferior
0
IDeg + IAsp (n = 744)
IGlar + IAsp (n = 248)
IDeg = insulin degludec; IGar = insulin glargine.
Garber A et al. Lancet. 2012;379(9825):1498–1507.
BEGIN Basal-Bolus Type 2: Confirmed Nocturnal Hypoglycemia
25% risk reductionRR: 0.75[0.58; 0.99]significant
Co
nfi
rmed
No
ctu
rnal
Hyp
ogl
ycem
ia
(Cu
mu
lati
ve N
um
ber
of
Even
ts p
er P
atie
nt-
year
)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
Time (weeks)
0 4 8 12 16 20 24 28 32 36 40 44 48 52
IDeg + IAsp (n = 753)
IGlar + IAsp (n = 251)
Garber A et al. Lancet. 2012;379(9825):1498–1507.
PEGylated Insulin Lispro vs Insulin Glargine in Patients With T2D: Glucose Control at Week 12
• 12-week, randomized, open-label, Phase 2 study of
patients with T2D (A1C ≤10.5%), taking metformin
and/or sulfonylurea with once-daily basal insulin
PEGylated Lispro
(n=195)
Insulin Glargine
(n=95)
P Value
Change from
baseline at 12 weeks
Change from
baseline at 12 weeks
FBG (SMBG [mg/dL]) –25.9 ± 2.5 –24.5 ± 3.8 0.388
A1C level (%) –0.7 ± 0.1 –0.7 ± 0.1 0.197
FBG = fasting blood glucose.
Bergenstal RM et al. Diabetes Care. 2012;35(11):2140–2147.
With comparable glucose control
Bergenstal RM et al. Diabetes Care. 2012;35(11):2140–2147.
40
80
120
00 4 8 12
Cu
mu
lati
ve N
oct
urn
al
Hyp
ogl
ycem
ia E
ven
ts
(per
10
0 p
atie
nts
)
Week Since Randomization
Insulin glargine
PEGylated insulin lispro
PEGylated Insulin Lispro vs Insulin Glargine in Patients With T2D: Nocturnal Hypoglycemia
3/23/2015
8
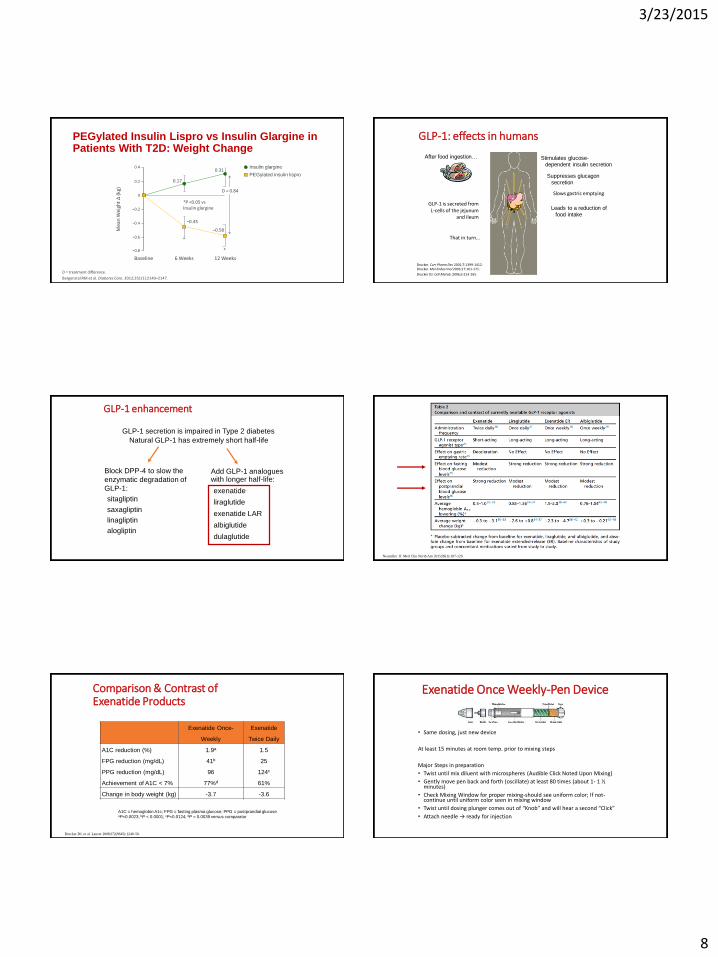
–0.8
–0.6
–0.4
–0.2
0
0.2
0.4
Mea
n W
eigh
t Δ
(kg
)
Baseline 6 Weeks 12 Weeks
Insulin glargine
PEGylated insulin lispro
0.17
0.31
D = 0.84
–0.45
–0.58
*P <0.05 vsInsulin glargine
*
*
D = treatment difference.
Bergenstal RM et al. Diabetes Care. 2012;35(11):2140–2147.
PEGylated Insulin Lispro vs Insulin Glargine in Patients With T2D: Weight Change
GLP-1: effects in humans
GLP-1 is secreted fromL-cells of the jejunum
and ileum
That in turn…
Stimulates glucose-dependent insulin secretion
Suppresses glucagonsecretion
Slows gastric emptying
Leads to a reduction offood intake
After food ingestion…
Drucker. Curr Pharm Des 2001;7:1399-1412. Drucker. Mol Endocrinol 2003;17:161-171.
Drucker DJ. Cell Metab. 2006;3:153-165.
GLP-1 enhancement
GLP-1 secretion is impaired in Type 2 diabetes
Natural GLP-1 has extremely short half-life
Add GLP-1 analogues with longer half-life:
exenatide
liraglutide
exenatide LAR
albiglutide
dulaglutide
Block DPP-4 to slow the
enzymatic degradation of
GLP-1:
sitagliptin
saxagliptin
linagliptin
alogliptin
Neumiller JJ. Med Clin North Am 2015;99(1):107-129.
Comparison & Contrast of Exenatide Products
Exenatide Once-
Weekly
Exenatide
Twice Daily
A1C reduction (%)
FPG reduction (mg/dL)
PPG reduction (mg/dL)
Achievement of A1C < 7%
1.9a
41b
96
77%d
1.5
25
124c
61%
Change in body weight (kg) -3.7 -3.6
A1C = hemoglobin A1c; FPG = fasting plasma glucose; PPG = postprandial glucoseaP=0.0023; bP < 0.0001; cP=0.0124; dP = 0.0039 versus comparator
Drucker DJ, et al. Lancet 2008;372(9645):1240-50.
Exenatide Once Weekly-Pen Device
• Same dosing, just new device
At least 15 minutes at room temp. prior to mixing steps
Major Steps in preparation
• Twist until mix diluent with microspheres (Audible Click Noted Upon Mixing)
• Gently move pen back and forth (oscillate) at least 80 times (about 1- 1 ½ minutes)
• Check Mixing Window for proper mixing-should see uniform color; If not-continue until uniform color seen in mixing window
• Twist until dosing plunger comes out of “Knob” and will hear a second “Click”
• Attach needle → ready for injection

3/23/2015
9
Albiglutide
• 97% homology to native GLP-1(7-36)
• 2 copies of a modified GLP-1 fused to human Albumin (C-terminus end of the modified GLP-1 sequence to the N-terminus of the human albumin)
• Resistant to DPP-4 metabolism- glycine replaces native GLP-1 alanine
• Half-life of 3.6-6.8 days
Eperzan, EMA, Accessed 12-11-14: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002735/WC500165119.pdf
• Dosing• 30mg Weekly• May increase to 50mg weekly
Albiglutide Efficacy vs Liraglutide
• Albi 50mg weekly versus Lira 1.8mg daily • At week 32 (n=422)• A1C: Albi -0.78%, Lira -0.99%
(difference 0.21%; 0.08—0.34; non-inferiority p value=0.0846)• GI SE: Albi 36%, Lira 49%• Injection site reactions: Albi 12.9%, Lira 5.4%
Pratley RE et al. Lancet Diabetes & Endo. 2014;2:289-297
Albiglutide- Device, Reconstitution, and Injection
• Storage of Pen Device• In refrigerator until expiration, and <4 weeks at room temp. • Pen needs 15 minutes at room temp before start mixing process
• Recommendation: take out next week’s dose when inject this week
• Injection site- subcutaneous delivery in abdomen, arm, or leg
• Must be injected within 8 hours of reconstitution• Inject weekly, without regard to meals
• “1” shows in window, twist until “2’” shows- slowly swirl 5 times, then let sit:
• 30mg dose- 15 minutes• 50mg dose- 30 minutes
Package Insert, GSK 2014, accessed 7-9-14, http://www.gsksource.com/gskprm/htdocs/documents/TANZEUM-PI-MG-IFU-COMBINED.PDF#nameddest=MG
Albiglutide-Injection Technique
Medication Guide, GSK 2014, accessed 7-9-14, http://www.gsksource.com/gskprm/htdocs/documents/TANZEUM-PI-MG-IFU-COMBINED.PDF#nameddest=MG
Albiglutide- Injection Technique
Medication Guide, GSK 2014, accessed 7-9-14, http://www.gsksource.com/gskprm/htdocs/documents/TANZEUM-PI-MG-IFU-COMBINED.PDF#nameddest=MG
Dulaglutide
• Recombinant GLP-1 Fc fusion protein linking GLP-1 analog to a human IgG4 Fc fragment
• Results in:• Prolonged t1/2: ~5 days• Once weekly dosing • Important difference: A solution- No reconstitution
needed
American Diabetes Association 74th Scientific Sessions, San Francisco, LB-110, P-979, P-962
3/23/2015
10
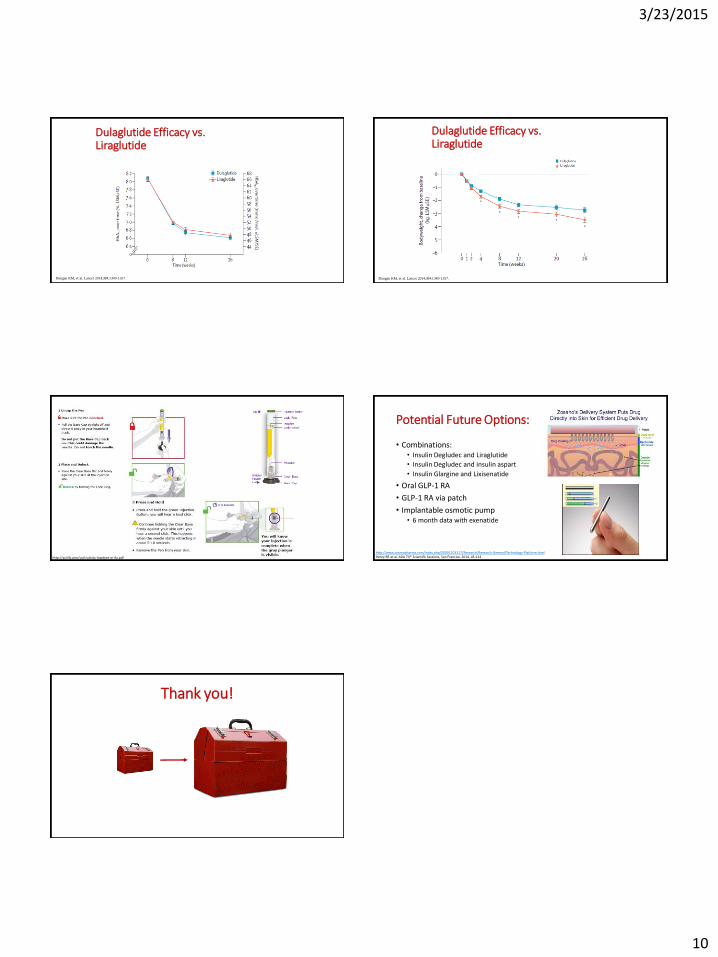
Dulaglutide Efficacy vs. Liraglutide
Dungan KM, et al. Lancet 2014;384:1349-1357.
Dulaglutide Efficacy vs. Liraglutide
Dungan KM, et al. Lancet 2014;384:1349-1357.
http://pi.lilly.com/us/trulicity-lowdose-ai-ifu.pdf
Potential Future Options:
• Combinations:• Insulin Degludec and Liraglutide
• Insulin Degludec and insulin aspart
• Insulin Glargine and Lixisenatide
• Oral GLP-1 RA
• GLP-1 RA via patch
• Implantable osmotic pump• 6 month data with exenatide
http://www.zosanopharma.com/index.php/20091103117/Research/Research-General/Technology-Platform.htmlHenry RR et al. ADA 74th Scientific Sessions, San Franciso, 2014, LB-114
Thank you!












![2 GREENBAUM WADE PRESENTATION MARCH 2014 [Read-Only]wadepage.org/files/2_GREENBAUM WADE PRESENTATION MARCH 2… · 300 people withouta family member with diabetes X 0.3% = 1 with](https://img.pdfslide.net/doc/110x75/5f7d1e3017a65079300d2229/2-greenbaum-wade-presentation-march-2014-read-only-wade-presentation-march-2.jpg)
















