Embed Size (px)
Citation preview

Approach to Hematemesis and Melena
6th Year Medicine Dr Yasir M Khayyat
Assistant Professor/Gastroenterologist

Management Outline Airway Breathing Circulation Decide on Admission

Causes of UGIB ( Hematemesis/Melena)

Melena: passage of blackTarry offensive stool due to Bleeding form the upper GIT proximal to ligmant ofTretiz ( > 100 ml).Basic Mechanisms:1.Hyperacidity2.H pylori3.Vascular anomalies4.Autoimmune5.Malignancy
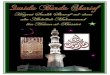
Ligament of Treitz





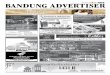
Endoscopic Diagnosis

Take home message
• Always think of hemodynamic stability ABC• Then think to do H & P• Common things are common• Careful not to kill the patient and know when
to call for somebody help• Common diseases are peptic ulcers, liver
disease, drug induced and malignancy.• Decide if you admit ( ward/ICU) or discharge.

Approach to Diarrhea

Diarrhea : • Increased frequency or stoolWeight ( > 200g) or frequency( ≥ 3 BM/d)
Onset:Acute: < 4 weeksChronic : > 4 weeks

Basic Pathologic Mechanisms


Now think of the causes of diarrhea and mention 4 causes under each category ( Acute vs. chronic)
1-2-3-4-
1-2-3-4-
1-2-3-4-
1-2-3-4-

General approach to Diarrhea
History:• Normal bowel habits• Onset: sudden/chronic• Frequency, Food relation• Stool appearance, Smell• Drugs• Tenesmus• Travel. Contact• Stress • Associated features• Nocturnal diarrhea• Thyrotoxicosis
Physical Examination:• Vital signs:• Volume status/Dehydration:• Eyes : anemia,thyrotoxicosi• Skin: flushing, rashes• L.N: • Abdomen:
mass,distension,tenderness,• Hands: clubbing

Investigations:
• CBC:WBC (…….),Hb (……..),Plt (……….),INR ?why• Serum Electrolytes, (BUN , Creatinine ),Album• Stool : analysis, O & P, Culture, ?Fat ,Occult
blood. Clostridium difficle,24 hr fat>10g( malabsorption),Osmolality and gap ?
• Specialized Tests: Endoscopy ( U & L)• DM : FBS,RBS• Thyroid : TSH,Ft3,Ft4• Malabsorption: Folate, Vit B12,Iron, serum
gastric,VIP,Calcitonin,Cortisol,5 HIAA (for what?)




Outline of Diarrhea management
• Assure ABC as always, assess volume status and replace lost fluids and electrolyte ( Na,K,Cl,HCO3)
• Antimotility : Loperamide,Atropine ( careful)• Antibiotics : not for everybody, Gram
negative,parasites,anaerobes• Prevention of spread, identification of the source• Treat the underlying cause of inflammatory,
Secretory chronic diarrhea.

Take home message
• Think of the patient ( immunocompetent/Immunocompromised)
• Back to the basics ( city, Incubation period, types of culture and Investigations)
• DO NOT GIVE ANTIBIOTICS TO ALL DIARRHEA .• Antimicrobials are not the only thing that the
patient need ( hydration,shock,renal/liver.F)• GO home and Read ???