Embed Size (px)
Citation preview

This article was downloaded by: [Gebze Yuksek Teknoloji Enstitïsu ]On: 21 December 2014, At: 17:55Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
The Journal of Forensic PsychiatryPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/rjfp19
Medium secure provision in NHS andprivate unitsNikki De Taranto a , Paul Bester b , Peter Pier Czhniak a , AlisonMccallum c & Harry Kennedy da Medium Secure Unit, 2 Crozier Terrace , Hackney, London, E9 6BEb Child and Family Psychiatry Unit , 5 Collingham Gardens, London,SW5 0HRc Department of Primary Care and Population Sciences , Royal FreeHospital School of Medicine , Rowland Hill Street, London, NW3 2 PFd Camlet Lodge Regional Secure Unit, Chase Farm Hospital , TheRidgeway, Enfield, Middlesex, EN2 8JLPublished online: 04 Jan 2008.
To cite this article: Nikki De Taranto , Paul Bester , Peter Pier Czhniak , Alison Mccallum & HarryKennedy (1998) Medium secure provision in NHS and private units, The Journal of Forensic Psychiatry,9:2, 369-378, DOI: 10.1080/09585189808402203
To link to this article: http://dx.doi.org/10.1080/09585189808402203
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &

Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

* .
Medium secure provision in NHS and private units
N I K K I D E T A R A N T O , P A U L BESTER, PETER P I E R C Z H N I A K , A L I S O N M c C A L L U M and
HARRY K E N N E D Y
ABSTRACT The use of private sector medium-secure units is a practice now firmly entrenched in forensic psychiatry. An assessment of patients in both N H S and private sector medium-secure provision was undertaken, looking at all medium-secure patients funded by three adjacent North East Thames health authorities. Case-notes and clinical measures were studied for each patient and comparisons made between the patients in the NHS and private sector units. The major differences between the two groups were not in clinical measures but in the types of acts or offences the patients had committed to get them into medium security, and in the length of stay in hospital. The patients in the N H S units were more likely to have committed violent offences, more often against strangers, and to have spent more time in hospital in their lives than the patients in the private sector units. Some of these differences may be explained by differing admission policies in the two types of units. We look at this phenom- enon and some of the issues needing to be addressed as a result of the parallel development of the private sector units alongside the N H S service.
Keywords: medium security, private sector medium-secure units, service pro- vision, mentally disordered offenders
Gunn, writing in 1977, spoke of t h e ‘third service’ in mental health provision, referring t o the secure accommodat ion service, projected to s tand alongside the penal system and t h e general psychiatric services. I t appears that now a ‘fourth service’, that of health-authority funded care in the private sector, has appeared in the gaps left by the o ther services.
I t now seems evident that t h e ‘yawning gap’ described by the Butler Repor t
The Journal of Forensic Psychiatry Vol9 No 2 September 1998 369-378 0 Routledge 1998 ISSN 0958-5184
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

370 J O U R N A L OF FORENSIC PSYCHIATRY Vol. 9 No. 2
in the 1970s has not been adequately bridged by provision within the National Health Service and with the increase in pressure for medium-secure beds, a shortfall has become increasingly obvious. Eastman, in his detailed review of forensic psychiatry services in 1993, emphasizes this while also dis- cussing the difficulties inherent in assessing need within this service. Taylor, also writing in 1993, describes resources for this population as ‘lacking or imbalanced’. Health purchasers too are recognizing the gap in service pro- vision and their use of services outside the N H S has made the private sector a major provider of secure accommodation. Indeed, these privately owned hospitals are solely populated by health-authority funded patients.
In the context of a growing and changing secure-provision service, a number of studies have been published over the past 15 years describing the iunctioning of the interim secure units and regional secure units, and the characteristics o f the patients treated by the service. Most of these studies haw focused on individual units and provided valuable information about patients and practices in these units (for example, Treasaden, 1985; Snowden, 19S5; Faulk and Taylor, 1986; Bullard and Bond, 1988; Hodgkinson and Clasby, 1991). Murray, writing in 1996, reviewed case-notes of all patients in NHS medium-secure units in November 1991. H e postulated that the patients accommodated in private sector beds were ‘broadly similar’ to patients from the same catchment area in N H S units, but no analysis of private sector patients was undertaken on that occasion.
In some areas, including the areas of North London focused on in this paper, the private sector is a major provider of secure provision. This situ- ation appears to have arisen for a number of reasons, as postulated by Coid (1 99 1 ), including funding inadequacies, managerial strategy and health-care philosophy and policy. Coid looked at a population of patients in private medium-secure units and concluded that many were there as a result of inad- equate provision of services (including specific lack of provision for chroni- call!- disturbed, longer-stay patients) in the NHS. Moss et al., writing in 1996, described one particular private unit and discussed the fact that they too felt such units were meeting a national need arising from inadequacies in pro- vision within the NHS.
Our project was originally commissioned as a needs assessment exercise by three London health authorities who purchase medium-secure care from both the N H S regional secure unit in Enfield (Camlet Lodge) and other secure units in the NHS and private sector. They were mindful of the recommendations of the Reed Report on Mentally Disordered Offenders (Department of Health and Social Security and the Home Office, 1992) that the group of patients in medium-secure accommodation requires careful assessment and measurement of care provided to it. These three authorities cover adjoining areas containing a population of approximately 1.5 million. About f 10 million a year is spent by the purchasers on the whole group of patients in medium security.
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

MEDIUM SECURE PROVISION 371
METHODOLOGY
Included in the assessment were all patients funded in medium-secure accommodation, on a specific single day, by each of three health authorities in the North East Thames area. For two of the authorities this was a single day in 1994, for the third it was a day in 1995. This population therefore included patients in Camlet Lodge RSU and those funded as medium-secure patients (not open or rehabilitation wards) in private sector places. The private sector places were spread over five different units, all outside London.
For each patient, information was first obtained and recorded from reading all the available case-notes. This information included demographic details and information about past violent behaviour. Various parameters related to the lengths and numbers of admissions were recorded, including the length of the present admission defined as the total continuous length of time spent in hospital to the date of assessment, which may have been spent in more than one hospital. This was felt to be more pertinent than looking at the length only of the admission in the present placement, which was often only a portion of a far lengthier admission.
The nature of the event or offence that precipitated the present admission was recorded in detail and this information was later classified into types as follows:
major violence: causing any significant injury, hospital care needed for
minor violence: any other violence; for example, slaps, shoves, etc.; no violence: acquisitive offences or threats only; sexual: offences involving a sexual motive where no physical injury was
arson; where no injuries were sustained; self-harm only.
The patient was then assessed by a research registrar using standardized clini- cal tools including the Brief Psychiatric Rating Scale, the Social Behaviour Schedule and the Health Related Insight Questionnaire. These instruments were largely chosen because of their previously proven validity and because, after trying several different combinations of tools in practice runs, they were judged to offer the largest amount of the type of information requested by the commissioning authorities in the shortest time. The interviews were structured to last no longer than an hour in order to maximize response rate in patients who were often reluctant to sit for a prolonged interview.
victim, or any use of a weapon;
sustained;
RESULTS
In this paper we focus on demographic and historical data about the patient group. A future paper will focus on the clinical findings in the population and
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

372 J O U R N A L O F F O R E N S I C P S Y C H I A T R Y Vol. 9 No. 2
the use of a multidisciplinary needs assessment panel to discuss present and future needs.
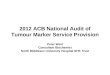
Basic demographic data
The population comprised 96 patients, 42 of them in NHS placements and 54 accommodated in the private sector. Table 1 shows the demographic
Tuble 1 Characteristics of patient groups
A'HS Private sector (N = 42) (N = 54)
Mean age on admission/ transfer to current placement
Mean age at time of needs assessment
Sex ratio M:F
Ethnicity
Transferred into present placement from another h 0 s pit a1
Mental Health Act Status
Axis I diagnosis recorded in medical notes
Other diagnoses recorded in medical notes
White AfricadCarib bean Asian
s.3 s.37 ss.37/41 s.38 ss.48/49 ss.47/49 Schizophrenia Paranoid psychosis Manic psychosis Depressive psychosis Organic brain disease No Axis I diagnosis Obsessive-compulsive disorder Schizoaffective disorder Personality disorder Substance abuse Learning disability
31
34
3 8 4 (= 90% male) 20 (48%) 19 (45%) 3 (7%)
12 (28%)"
4 (9%);' 7 (17%)
21 (50%) 2 (5%) 6 (14%) 2 (5%)
4 (1 0%)
2 (5%)
3 (7%)
30 (71 Yo)
3 (7%)
0
0
0 7 (1 6%) 4 ( I OY") 4 (1 0%)
31
34
41:13 (= 76% male) 35 (65%) 16 (30%) 3 ( 5 % )
37 (69%)"-
29 (53%);: 4 (8%)
20 (37%)
1 (2%)
43 (79%) 2 (4%)
1 (2%) 2 (4%) 4 (7%) 1 (2%)
0
0
0
1(2%) 4 (7%)
10 (18%) 9 (16%)
'' Significant ditference
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

M E D I U M S E C U R E P R O V I S I O N 373
details and diagnoses of both these groups. The diagnoses recorded were those given in the medical notes; if there were differences in the primary diag- nosis recorded then the latest one was used.
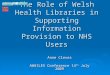
History of violence
Table 2 shows the information, collected from the case-notes, related to violent acts, and to the event or offence which precipitated the current admission. The patients in the NHS unit were shown to be more likely to have been admitted as a result of serious violence, and to have committed a violent act against a stranger, whereas there was a significant group of patients in the private units whose present admission began after they had been violent or threatening towards nurses or other professionals.
Table 2 History of violent behaviour
NHS Private sectoy (N = 42) (N = 54)
History of violent behaviour
Event precipitating admission
Relationship of victims of precipitating event to patient
No previous convictions for violence Multiple previous convictions for violence Violent behaviour in the past month Maior violence
Minor violence No violence Sexual Arson Self-harm only Stranger Professional (nurse, teacher, police) Family/cohabitee Acquaintance Self Unknown
18 (43%)
15 (36%)
20 (48%)
24 (57%"'), 4 being homicides
3 (7%) 7 (17%)
2 (5%) 4 (9%)
2 (5%) 17 (400/~:::!) 7 (170/~:!.,,, "7 8 (19%) 6 (14%) 2 (5%) 2 (5%)
28 (52%)
12 (22%)
17 (32%)
16 (30%:')), 2 being homicides
9 (16%) 13 (24%)
8 (15%) 5 (9%) 3 (6%) 8 (150/~;>:!)
23 (420/~:!:>:>)
3 (6%)
3 (6%) 7 (13%)
10 (18%)
'; Significant difference: p = 0.009 'i:i Significant difference: p = 0.04 '!wp Significant difference: p = 0.02 Of the 30 cases where victims were classified as 'professionals', 26 involved nursing staff.
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

374 I O U R N A L OF F O R E N S I C PSYCHIATRY Vol. 9 No. 2
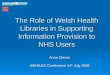
Tablr, 3 Time in hospital
NHS Private sector (N = 42) (N = 54)
Present admission: Mean continuous period Median up to date of assessment (months)
admissions
spent in hospital, Median prior to present admission (months)
Number of previous Mean
Total time in life Mean
29.5 57.2 14.2'" 29.3 ::.
3.2 5.7
:I Significant difference on Mann-Whitney U Test: p = 0.002 ':-':- Significant difference on Mann-Whitney U Test: p < 0.001
Time spent in hospital
Table 3 shows the data related to the time patients had spent in hospital. There were significant differences between the NHS and private unit groups in the length of the present admission and the total length of time patients had spent in hospital in their lives prior to the present admission. The private unit patients were therefore seen to be longer-stay patients in both senses.
DISCUSSION
Looking at the demographic data for the studied population as a whole, find- ings were similar to those in other studies of medium-secure groups. The niean age and ethnicity ratios were not statistically different between the two groups (NHS and private unit), although, as in other studies of medium security (Cope and Ndegwa, 1990; Murray, 1996), African and African- Caribbean patients were markedly over-represented in the total population. There was, however, a marked difference between the two groups in terms of their detention under the Mental Health Act, with far more of the private unit patients being detained under s.3 (civilly detained patients).
All studies looking at medium-secure populations in the UK have shown that patients with schizophrenia are very much in the majority in such set- tings, with percentages between 60 and 85%. We found a similar pattern.
We became aware that the number of convictions for violent offences was not trulv representative of the actual history of violence by the patient. It was
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

MEDIUM SECURE PROVISION 375
repeatedly noticeable that many patients who had few or no convictions for violent offences had in fact committed many violent and aggressive acts, often directed towards family members or hospital staff, which had not resulted in prosecution.
It appears from this survey that medium-secure beds within the NHS and those in the private sector, extensively used by some purchasers, have been used differently. Criteria for admission to the NHS medium-secure units often include the stipulation that patients should be those expected to require no longer than 18 months or 2 years in medium-secure accommodation, whereas the private units have inore flexibility, as described by Moss et al. (1 996). Patients who have therefore already demonstrated their possible need for longer stays in medium security by previous lengthy admissions may tend to be admitted to the private sector units. The majority of the patients in the private units had been transferred there from another hospital, some after assaulting staff there.
It is now the case in all the health authorities surveyed that a patient requir- ing medium-secure accommodation, wherever placed, would need to be referred via the forensic psychiatry service. However, this was not always the case in the past, especially with some of the patients who were referred to private medium-secure units several years ago. Difficult-to-manage patients from general psychiatric wards were sometimes, in the case of several of these patients, placed directly into the private sector units without any direct contact with the (at that time very limited) forensic service. In all these circumstances, therefore, it would seem that the private sector had by default, through less selective or different criteria, taken patients who were seen as long-stay patients in the absence of specific provision for these patients within the NHS.
There are also some qualitative differences between the two groups. Patients in NHS beds were more likely to be those who have harmed a stranger, to have committed an index offence involving higher levels of vio- lence and to be detained under Part I11 of the Mental Health Act (i.e. what would be considered as the more ‘forensic’ cases). Patients in the private sector beds, however, tended to be civilly detained patients, they were more likely to be female, and a group of them was admitted to medium security after violence against nursing staff in other hospitals. Four patients (two men and two women) were admitted to private sector units after serious self-harm, while only one patient in the RSU fell into this category.
Coid, writing in 1991, had already formed the impression, based on a small sample at that time, that patients in the private units had longer hospital stays, and postulated some reasons why this might be so. In keeping with his com- ments, we feel that an alternative explanation for the longer hospital stays of some of the private patients (other than the considerations on admission leading to truly ‘long-stay’ patients being admitted there as a result of differ- ent admission criteria) is that at least some of the patients in the private sector
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

376 T O U R N A L O F F O R E N S I C P S Y C H I A T R Y Vol. 9 No. 2
are spending longer in hospital for reasons arising because of where they are placed. Such reasons might include organizational factors within the private hospitals, geographical distance meaning that the practicalities of rehabili- tation into often distant home communities are more difficult to arrange, or the difficulties of communicating with the distant catchment area service. This could mean that those patients who are out of sight often remain out of mind for the busy NHS service, which would in theory be keeping track of patients placed in the private sector. This problem has been acknowledged in practice and, in the area surveyed and beyond, special services to address these problems are now being put in place in the form of Risk Share teams which perform this ‘keeping track’ function on behalf of the purchasers: the ‘regular monitoring’ that Coid felt essential to produce the impetus to ensure the eventual return of these patients to their catchment area.
C O N C L U S I O N
The Norrh London health authorities which commissioned the work leading to this paper were interested in scrutinizing the use of mediuni- secure psychiatric beds, a very expensive resource. O u r study found in general a population of medium-secure patients similar to those described in other areas, but within that population uncovered significant differences between the N H S and private unit patients. Some of these differences may be explained by policy factors in the units, meaning that certain types of patient are more likely to end up on one side of the divide or the other by virtue of the perception that different types of provision are available in the different areas, and different selection criteria. Reasons for significantly longer admission times for the private unit patients have also been postu- lated by clinicians working in the service as being related to the distance, both geographically and in communication, between the two types of units, and practical measures are being put into place to address these difficulties. We believe that further work looking at the effect of improved involvement and communication by the NHS forensic services monitoring the private sector provision will be essential to clarify the relative importance of these factors.
This study provided an initial database and ‘template’ for monitoring of the use of the difterent kinds of units in medium-secure provision, which is now ongoing in this North London area. A dedicated Risk Share team con- tinues to monitor the parametei s reported here and facilitate improved inter- digitation between the N H S secure unit and the private units. Follow-up on the patients surveyed in this study and addition of new patients to the data- base as they enter the medium-secure service means that the use of these beds
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

M E D I U M S E C U R E P R O V I S I O N 377
and the progress of patients are continually scrutinized. These data will be used as the basis of future publications and continuing provision of relevant information to the purchasing authorities.
Moss et ul. (1996) concluded that the use of the independent sector for pro- vision of medium-secure beds is now becoming ‘firmly entrenched in foren- sic psychiatry’, driven by the demands of market forces for them to have a flexibility in admitting criteria which is sometimes greater than that of the NHS medium-secure units. We feel that if this is the case, as it does appear to be, then it is vital that the use and development of all parts of the medium- secure service are monitored and decision-making in the development and purchasing of services is based on detailed, updated information about the patients who use this expensive but vital resource.
Dr N i k k i de Taranto, MBBCh, MRCPsych, senior registrar an forensicpsychiatry, Medium Secure Unit, 2 Crozier Terrace, Hackney, London E9 6BE
D r Paul Bester, MBBCh, MRCPsych, specialist registrar in child and adolescent psychiatry with forensic special interest, Child and Family Psychiatry Unit, J Collingham Gardens, London
SWJ OHR
Dr Peter Pierczhniak, MBBS, MRCPsych, specialist registrar in forensic psychiatry, Medium Secure Unit, 2 Crozier Terrace, Hackney, London E9 6BE
D r Alison McCallum, MBChB, MSc, MSPHM, senior lecturer in public health medicine, Department of Primary Care and Population Sciences, Royal Free Hospital School of Medicine,
Rowland Hill Street, London N W 3 2 PF
D r Harry Kennedy, BSc, MD, MRCI: MRCPsych, consultant forensic psychiatrist and honorary senior lecturer in forensic psychiatry, Camlet Lodge Regional Secure Unit, Chase Farm
Hospital, The Ridgeway, Enfield, Middlesex EN2 8JL
REFERENCES
Bullard, H. and Bond, M. (1988) ‘Secure Units: Why They Are Needed’. Medicine, Science & the Law 28(4): 312-18.
Coid, J. W. (1991) ‘A Survey of Patients from Five Health Districts Receiving Special Care in the Private Sector’. Psychiatric Bulletin 15: 257-62.
Cope, R. and Ndegwa, D. (1990) ‘Ethnic Differences in Admissions to a Regional Secure Unit’. Journal of Forensic Psychiatry 1: 215-36.
Department of Health and Social Security and the Home Office (1992) Review of Health and Social Services fo r Mentally Disordered Offenders and Others Requiring Similar Services (the Reed Report). Cmnd 2088. London: HMSO.
Eastman, N. (1993) ‘Forensic Services in Britain’. International Journal of L a w and Psychiatry 16: 1-26.
Faulk, M. and Taylor, J. (1986) ‘Psychiatric Regional Interim Secure Unit: Seven Years’ Experience’. Medicine, Science & the Law 26( 1): 17-22.
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14

378 I O U R N A L O F F O R E N S I C P S Y C H I A T R Y Vol. 9 No. 2
Gunn. J. (1977) ‘Management of the Mentally Abnormal Offender: Integrated or Parallel’. Proceedings of the Royal Society of Medicine 70(12): 877-80.
Hodgkinson, P. and Ckasby, S. (1991) ‘The First Three Years of Operation of a Forensic Psychiatry Service’. Medicine, Science & the L a w 31(4): 299-305.
Home Office and Department of Health and Social Security (1975) Report o f t h e Committee on Mentally Abnormul Offenders (the Butler Report). Cmnd 6244. London: HMSO.
hloss, K. R. et a f . (1996) ‘A Study of Admissions to an Independent Medium Secure Hospital’. Medicine, Science 6 the LUW 36(3): 242-8.
Murray, K. (1996) ‘The Use of Beds in NHS Medium Secure Units in England’. J o u r n d o f Forensic Psychiatry 7(3): 504-24.
Snowden, P. (1985) ‘A Survey of the Regional Secure Unit Programme’. British Journal of Psychiutry 147: 499-507.
Treasaden, I . (198.5) ‘Current Practice in Regional Interim Units’. In Gostin, L. (ed.) Secure Provision. London: Tavistock, pp. 176-207.
Dow
nloa
ded
by [
Geb
ze Y
ukse
k T
ekno
loji
Ens
titïs
u ]
at 1
7:55
21
Dec
embe
r 20
14