Embed Size (px)
Citation preview

The Japanese Journal of Psychiatry and Neurology, Vol. 41, No. 4, 1987
Medroxyprogesterone Acetate and Sleep Apnea
Hiroharu Ohshima, M.D.
Department of Neuropsychiatry, Kurume University School of Medicine, Kurume
Abstract: Seven patients with sleep apnea DOES and one with sleep apnea DIMS were treated with medroxyprogesterone acetate (MPA). The therapeutic effect was confirmed in most of them by polysomnographic recording. A marked increase of TST was ob- served in two patients whose AI and/or %SAT remarkably decreased. Contrarily, three patients exhibited a considerable decrease in TST, and A1 and/or %SAT were reduced remarkably in two of them with MPA. After the MPA medication a few patients com- plained of disturbed nocturnal sleep. A significant positive correlation was observed between the decreased rate of TST and that of the mean duration of apneas. From these results, it was considered that MPA has a mild activating action on the arousal system in the CNS, and that the action may be partly responsible for the therapeutic effects of MPA on sleep apneas.
Key Words: sleep apnea, medroxyprogesterone acetate, arousal action
Jpn J Psychiatr Neurol 41: 645-650, 1987
INTRODUCTION
Both progesterone and medroxyprogester- one acetate (MPA), a synthetic progesterone, have been demonstrated to have a stimulant action on the respiratory system,l l4 l5 2o
and have been used in the treatment of pa- tients with the sleep apnea syndrome.8 As of the present, the author has treated seven patients with sleep apnea DOES syn- drome (SADOES) and one with sleep apnea DIMS syndrome (SADIMS) with MPA, and confirmed polysomnographically an obvious decrease in the apnea index (AI) and %time of sleep apnea (%SAT) in most of them.
It was of much interest, however, that two patients with SADOES exhibited a marked decrease in total sleep time (TST)
Received for publication March 3, 1987
even though considerable reductions were found in A1 and/or %SAT with MPA, and that a pronounced decrease was observed in the TST of another patient with SADOES whose A1 and %SAT were not affected by MPA. Moreover, a few patients with SADOES or SADIMS complained of a re- duced time of nocturnal sleep or of early morning awakening during the MPA medi- cation. These observations led the author to suppose that MPA might have a weak action as a stimulant on the arousal system in the CNS. In actual fact, a recent study by Kotorii et a1.9 experimentally revealed using normal healthy subjects that MPA has a stimulating action on the arousal sys- tem. Accordingly, it may be possible that MPA reduces the arousal threshold which would then lead to an early termination of each apneic episode, because a termination of the apneic episode is preceded by arousal

646 H. Ohshima
Table 1: Subjects
Patient Age Sex Diagnosis
1 43 M SADOES 2 43 M 0
3 62 M 0 4 48 M //
5 56 F 0
6 58 M 0
7 33 M 0 8 54 M SADIMS
- _ _ ~
~
from s l x i ~ . ~ '3 In
The present study, therefore, was retro- spectively carried out on patients with the sleep apnea syndrome to investigate whether the therapeutic effects of MPA on sleep apnea can bz partly attributable to its stimulating action on the arousal system.
jected to the present study. Their age and sex are presented in Table 1.
After a polysomnographic recording was performed for one night before medication, MPA (30-100 mg) was orally given to each patient (b.i.d.). One to four months later a second recording was conducted for one night during the MPA medication. Each recording lasted from between 1O:OO and 11 :O p.m. until the patient awoke sponta- neously the next morning. The sleep stage was scored at every 20-sec epoch during the recording, according to the criteria of Rechtschaffen and Kales.12 An apnea was defined as a cessation of the airflow at the nose and mouth lasting for more than 10 SW.7
The t-test or Mann-Whitney U-test was employed for the statistical analysis of two related samples.
SUBJECTS AND METHODS RESULTS
Seven patients with SADOES and one with SADIMS, all of whom were treated with MPA in the Sleep Disorders Clinic of Kurume University Hospital, were sub-
Tables 2 and 3 indicate TST, AI, %SAT, mean duration of apneas, percentage of each sleep stage and the total time spent for
Table 2: TST, AI, %SAT and Mean Duration of Apneas before and during MPA Medication
A1 Mean Duration of Apnea (sec)
C M Mean % SAT 0 C M Mean
I - 384 81.7 0 16.4 98.1 60.0 22 .o 0 22.1 22.0 MPA 60mg 452 43.4 0 3.7 47.1 24.1 18.6 0 16.4 18.4
2 - 397 42.3 1.1 0 43.4 18 .O 14.9 13.6 0 14.9 MPA 45mg 373 19.1 1.3 0 20.4 8.8 15.7 16.3 0 15.8
3 - 383 4.2 1.1 0.3 5.6 4.4 28.7 22.1 35.0 27.8 MPA 30mg 329 4.7 1.3 2.0 8.0 5.0 22.9 12.1 28.2 22.5
4 - 469 2.8 0.8 0.1 3.7 1.4 14.1 10.8 20.0 13.6 MPA 90mg 457 4.5 0 0.1 4.6 1.7 13.2 0 15.0 13.3
5 - 323 47.0 0.4 0.6 48.0 34.6 26.1 17.5 20.0 26.0 MPA 30mg 230 16.4 0.5 0.3 17.2 6.1 12.7 12.5 15.0 12.7
- 377 57.3 4.8 16.7 78.8 77.2 36.3 13.5 37.9 35.3 6 MPA 100mg 253 27.7 14.5 29.2 71.4 38.5 18.1 15.7 22.5 19.4
7 - 264 66.1 4.5 1.8 72.4 29.0 14.5 11.5 16.9 14.4 MPA 60mg 360 27.8 1.2 5.5 34.5 23.8 22.7 25.0 35.5 24.8
8 - 307 9.6 0.6 0.4 10.6 5 . 5 18.7 11.7 32.5 18.8
TST - Pt. Treatment (min) - ~ .~ __ _ ~~ ~-
0 ~- -- --___
MPA 45mg 333 4.1 0 0 4.1 2.6 22.2 0 0 22.2 - ~- ____ ~
0: obstructive, C: central, M: mixed.
Medroxyprogesterone Acetate and Sleep Apnea 6 47
Table 3: Stages of Sleep (%) and TIA before and during MPA Medication
Pt.
1
2
3
4
5
6
7
~ ~~
Treatment
- MPA COmg
MPA 45mg
MPA 30mg
MPA 90mg
MPA 30mg
MPA 100mg
MPA 60mg
-
-
-
-
-
-
St. 1 (%)
31.6 6.7
26.4 18.5 21.9 27.7 19.6 9.4
31.3 20.4 49.1 44.3 54.9 44.4
___ ~
St. 2 (%)
48.9 55.3 54.2 68.3 68.9 61.4 64.4 74 .o 57.3 68.7 38.5 51 .O 25 .O 45.3
8 - 14.7 MPA 45mg 15.3
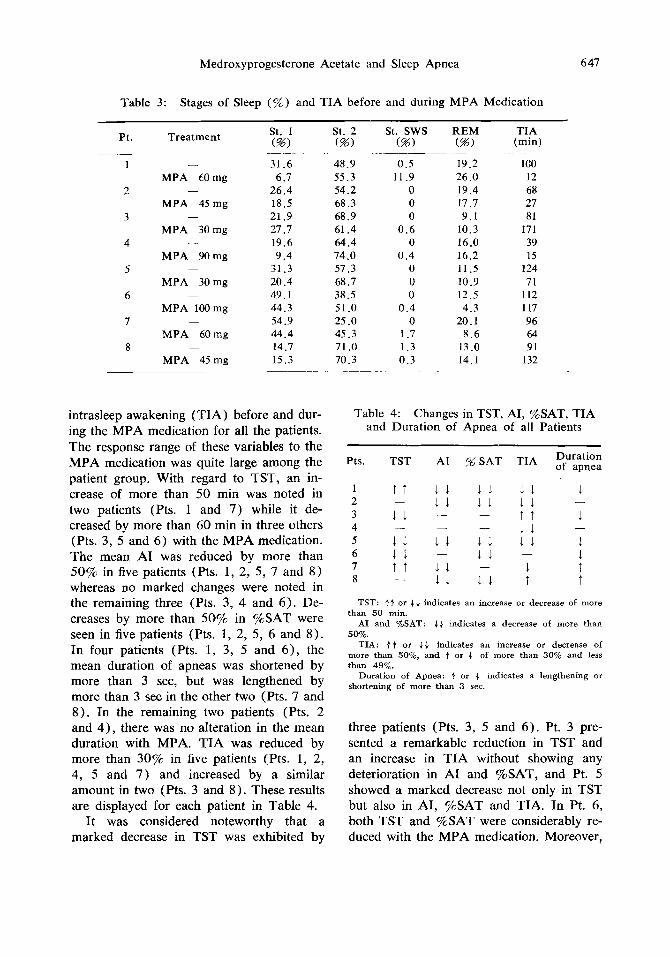
intrasleep awakening (TIA) before and dur- ing the MPA medication for all the patients. The response range of these variables to the MPA medication was quite large among the patient group. With regard to TST, an in- crease of more than 50 min was noted in two patients (Pts. 1 and 7) while it de- creased by more than 60 min in three others (Pts. 3, 5 and 6) with the MPA medication. The mean A1 was reduced by more than 50% in five patients (Pts. 1, 2, 5, 7 and 8) whereas no marked changes were noted in the remaining three (Pts. 3, 4 and 6). De- creases by more than 50% in %SAT were seen in five patients (Pts. 1, 2, 5, 6 and 8 ) . In four patients (Pts. 1, 3, 5 and 6), the mean duration of apneas was shortened by more than 3 sec, but was lengthened by more than 3 sec in the other two (Pts. 7 and 8). In the remaining two patients (Pts. 2 and 4), there was no alteration in the mean duration with MPA. TIA was reduced by more than 30% in five patients (Pts. 1, 2, 4, 5 and 7) and increased by a similar amount in two (Pts. 3 and 8). These results are displayed for each patient in Table 4.
It was considered noteworthy that a marked decrease in TST was exhibited by
St. sws (%I
REM (%)
0.5 11.9
0 0 0
0 . 6 0
0 .4 0 0 0
0 . 4 0
1.7
19.2 26 .O 19.4 17.7 9.1
10.3 16.0 16.2 11 .5 10.9 12.5 4 .3
20.1 8 .6
TIA (min)
100 12 68 27 81
171 39 15
124 71
112 117 96 64
71 .O 1 . 3 13 .O 91 70.3 0 . 3 14.1 132
~ ~
Table 4: Changes in TST, AI, %SAT, TIA and Duration of Apnea of all Patients
Pts. TST A1 % SAT TIA
1 T T 1 1 -11 .11 1 1 1 1 1 1 2
T T 3 1 1 - 1 1 4
5 11. 1 1 1.1 1 1 6 -11 - 1 1 - 7 T T 1 1 - 1
1 1 1 1 T
- -
- - -
- 8
Duration of apnea
1
1
1 1 t T
-
-
TST: .E+ or J.J. indicates an increase or decrease of more than SO min.
A1 and %SAT: &+ indicates a decrease of more than 50%.
TIA: .E+ or J.J. indicates an increase or decrease of more than SO%, and t or J. of more than 30% and less than 49%.
Duration of Apnea: 1. or J. indicates a lengthening or shortening of more than 3 sec.
three patients (Pts. 3, 5 and 6 ) . Pt. 3 pre- sented a remarkable reduction in TST and an increase in TIA without showing any deterioration in A1 and %SAT, and Pt. 5 showed a marked decrease not only in TST but also in AI, %SAT and TIA. In Pt. 6, both TST and %SAT were considerably re- duced with the MPA medication. Moreover,
648 H. Ohshima
c .- 0 %
Z 5 0 -
n
L =l
m W
c a 4
0
W
m E
'CI W
ul m W L
U W m
c
*
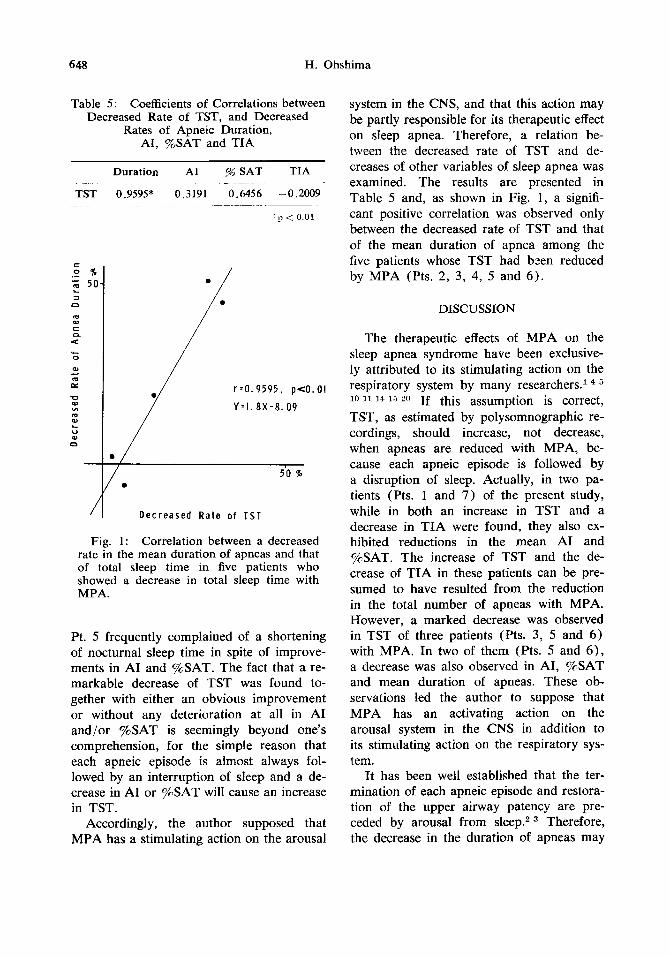
Table 5: Coefficients of Correlations between Decreased Rate of TST, and Decreased
Rates of Apneic Duration, AI, %SAT and TIA
Duration A1 % SAT TIA ~ .~
TST 0.9595* 0.3191 0.6456 -0.2009
p < 0.01
/ /
/ r . 0 . 9 5 9 5 , pe0 .01
Y - 1 . 8 X - 8 . 0 9
1 D e c r e a s e d R a t e o f T S T
Fig. 1: Correlation between a decreased rate in the mean duration of apneas and that of total sleep time in five patients who showed a decrease in total sleep time with MPA.
Pt. 5 frequently complained of a shortening of nocturnal sleep time in spite of improve- ments in A1 and %SAT. The fact that a re- markable decrease of TST was found to- gether with either an obvious improvement or without any deterioration at all in A1 and/or %SAT is seemingly beyond one's comprehension, for the simple reason that each apneic episode is almost always fol- lowed by an interruption of sleep and a de- crease in A1 or %SAT will cause an increase in TST.
Accordingly, the author supposed that MPA has a stimulating action on the arousal
system in the CNS, and that this action may be partly responsible for its therapeutic effect on sleep apnea. Therefore, a relation be- tween the decreased rate of TST and de- creases of other variables of sleep apnea was examined. The results are presented in Table 5 and, as shown in Fig. 1, a signifi- cant positive correlation was observed only between the decreased rate of TST and that of the mean duration of apnea among the five patients whose TST had bzen reduced by MPA (Pts. 2, 3, 4, 5 and 6) .
DISCUSSION
The therapeutic effects of MPA on the sleep apnea syndrome have been exclusive- ly attributed to its stimulating action on the respiratory system by many researchers.l
'I l4 2o If this assumption is correct, TST, as estimated by polysomnographic re- cordings, should increase, not decrease, when apneas are reduced with MPA, be- cause each apneic episode is followed by a disruption of sleep. Actually, in two pa- tients (Pts. l and 7) of the present study, while in both an increase in TST and a decrease in TIA were found, they also ex- hibited reductions in the mean A1 and %SAT. The increase of TST and the de- crease of TIA in these patients can be pre- sumed to have resulted from the reduction in the total number of apneas with MPA. However, a marked decrease was observed in TST of three patients (Pts. 3, 5 and 6) with MPA. In two of them (Pts. 5 and 6) , a decrease was also observed in AI, %SAT and mean duration of apneas. These ob- servations led the author to suppose that MPA has an activating action on the arousal system in the CNS in addition to its stimulating action on the respiratory sys- tem.
It has been well established that the ter- mination of each apneic episode and restora- tion of the upper airway patency are pre- ceded by arousal from sleep.* Therefore, the decrease in the duration of apneas may

Medroxyprogesterone Acetate and Sleep Apnea 649
also be explained by the MPA action on the arousal system since a lowering of the arousal threshold will result in an early ter- mination of apneic episode. In the present study, a relation between the decreased rate of TST and the decreases in the mean dura- tion of apneas, AI, %SAT and TIA among patients whose TST was reduced with MPA administration was investigated. A signifi- cant positive correlation was found between the decreased rate of TST and that of the mean duration of apneas. These observa- tions suggest that MPA has an activating action on the arousal system in the CNS, and that this action of MPA may be partly responsible for its therapeutic action on sleep apneas.
Pt. 5 frequently complained of a reduced time in nocturnal sleep after the MPA ad- ministration, and a reduction in TST was demonstrated polysomnographically even though AI, %SAT and TIA have all re- markably improved. Although Pt. 8 re- ported that he awoke earlier in the morning after the MPA medication, a reduction in TST was not confirmed by the polysom- nographic recording. I t can be said, how- ever, that the reports of these patients on their nocturnal sleep may indicate an ac- tivating action of MPA on the arousal sys- tem in the CNS.
Recently Kotorii et al.9 demonstrated that MPA given to normal healthy men resulted in a decrease of TST and Stage 4 sleep and an increase in TIA and Stage 1 sleep. From these results, they concluded that MPA has a mild activating action on human sleep, and the concluding remark of the present study is consistent with this. A further study, however, is necessary to elucidate the mecha- nism which induces the activating action of MPA on the arousal system in the CNS.
ACKNOWLEDGMENT
The author sincerely thanks Prof. K. Ina- naga and Associate Prof. Y. Nakazawa for their support and encouragement of the study.
1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
1 1 .
REFERENCES
Block, A. J., Wynne, J.W., Boysen, P.G., Lindsey, S., Martin, C. and Cantor, B.: Menopause, medroxyprogesterone and breathing during sleep. Am J Med 70: 506-510, 1981. Bowes, G., Woolf, G.M., Sullivan, C.E. and Phillipson, E.A.: Effect of sleep frag- mentation on ventilatory and arousal re- sponses of sleeping dogs to respiratory stimuli. Am Rev Dis 122: 899-908, 1980. Bowes, G., Townsend, E.R., Bromley, S.M., Kozar, L.F. and Phillipson, E.A.: Role of the carotid body and of afferent stimuli in the arousal response to airway occlusion in sleeping dogs. Am Rev Resp Dis 123: 644-647, 1981. Doring, G.K. and Loeschcke, H.H.: Atmung und Saure-Basengleich-Gewicht in der Schwangerschaft. Arch Ges Physiol 249: 437-451, 1947. England, S.J. and Farhi, L.E.: Fluctua- tions in alveolar CO, and in base excess during the menstrual cycle. Resp Physiol 26: 157-161, 1976. Gastaut, H., Tassinari, C.A. and Duron, B.: Polygraphic study of the episodic diurnal and nocturnal (hypnic and re- spiratory) manifestations of the Pick- wickian syndrome. Brain Res 2: 167- 186, 1966. Guilleminault, C. and Dement, W.C.: Sleep apnea syndromes and related sleep disorders. In: Williams, R.L. and Karacan, I. (Eds.), Sleep disorders. Diagnosis and treatment. A Wiley Medical Publication, New York, pp. 9-28, 1978. Hensely, M.J., Saunders, N. and Strohl, K.P.: Medroxyprogesterone treatment of obstructive sleep apnea. Sleep 3: 441-446, 1980. Kotorii, T., Nonaka, K., Nakazawa, Y., Matsunaga, H., Mieno, K., Hatase, T., Kodama, H. and Nishida, T.: Effects of medroxyprogesterone acetate on sleep of healthy young male adults. Jpn Psychiatr Neurol 41: 261-267, 1987. Kryger, M., McCulloough, R.E., Collins, D., Scoggin, C., Weil, J.V. and Grover, R.F.: Treatment of excessive polycythemia of high altitude with respiratory stimulant drugs. Am Rev Dis 117: 455-464, 1978. Prowse, C.M. and Gaensler, E.A.: Re- spiratory and acid-base changes during pregnancy. Anesthesiol 2 6 381-392, 1965.
650
12.
13.
14.
15.
16.
H. Ohshima
Rechtschaffen, A. and Kales, A.: A manu- al of standardized terminology, tech- niques, and scoring system for sleep stages of human subjects. Washington, D.C.: U.S. Government Printing Office, 1968. Remmers, J.E., deGroot, W.J., Sauerland, E.K. and Anch, A.M.: Pathogenesis of upper airway occlusion during sleep. J Appl Physiol Respirat Environ Exercise Physiol 44: 931-938, 1978. Schoene, R.B., Pierson, D.J., Lakshi- narayan, S., Schrader, D.L. and Butler, J.: Effect of medroxyprogesterone acetate on respiratory drives and occlusion pressure. Bull Europ Physiopath Resp 16: 645- 653, 1980. Skatrud, J.B., Dempsey, J.A. and Kaiser, D.G.: Ventilatory response to medroxy- progesterone acetate in normal subjects: time course and mechanism. J Appl Physiol 44: 939-944, 1978. Skatrud, J.B., Iber, C., Ewart, R.,
17.
18.
19.
20.
Thomas, G., Rasmussen, H. and Schulz, B.: Disordered breathing during sleep in hypothyroidism. Am Rev Resp Dis 124: 325-329, 1981. Strohl, K.P., Henseley, M.J., Saunders, N.A., Scharf, S.M., Brown, R. and Ingram, R.H. Jr.: Progesterone adminis- tration and progressive sleep apnea.
Sutton, F.D., Zwillich, C.W., Creagh, C.E., Pierson, D.J. and Weil, J.V.: Pro- gesterone for outpatient treatment of Pickwickian syndrome. Ann Int Med 83: 476-479, 1975. Walsh, R.E., Michaelson, E.D., Harkle- road, L.E., Zighelboim, A. and Sackner, M.A.: Upper airway obstruction in obese patients with sleep disturbance and som- nolence. Ann Int Med 76: 185-192, 1972. Zwillich, C.W., Natalino, M., Sutton, F. and Weil, J.: Effects of progesterone on chemosensitivity in normal men. J Clin Lab Med 92: 262-269, 1978.
JAMA 245: 1230-1232, 1981.