Embed Size (px)
Citation preview

ISSN 2517-7516, Membranes and Membrane Technologies, 2019, Vol. 1, No. 4, pp. 201–211. © Pleiades Publishing, Ltd., 2019.Russian Text © The Author(s), 2019, published in Membrany i Membrannye Tekhnologii, 2019, Vol. 9, No. 4, pp. 235–246.
Membranes in Extracorporeal Blood Oxygenation TechnologyA. K. Evseeva, S. V. Zhuravela, A. Yu. Alentievb, *, I. V. Goroncharovskayaa, and S. S. Petrikova
aSklifosovsky Research Institute of Emergency Medicine, Moscow, 129090 RussiabTopchiev Institute of Petrochemical Synthesis, Russian Academy of Sciences, Moscow, 119991 Russia
*e-mail: [email protected] December 19, 2018; revised March 18, 2019; accepted April 5, 2019
Abstract—The development and implementation of the extracorporeal membrane oxygenation (ECMO)technique for the treatment of patients in critical conditions make it possible to effectively and safely supportgas exchange processes in the blood for a long time. One of the main components of the ECMO unit is a gaspermeable membrane which is a barrier separating the blood from the gas phase. Since the 1950s, the devel-opment of this technology has been aimed at improving the safety and duration of use of membranes, whichled to the creation of oxygenators that provide life support for several weeks. This review is devoted to thedevelopment of the extracorporeal membrane oxygenation technology including the choice of materials,methods to improve their hemocompatibility, and approaches to the design of the membrane contactor.
Keywords: membranes, extracorporeal membrane oxygenationDOI: 10.1134/S2517751619040024
INTRODUCTION
The technology of extracorporeal membrane bloodoxygenation is used in modern surgery in the case ofheart surgical interventions, in transplantology, and inthe case of injuries associated with massive blood loss.Here, along with the organization of artificial circula-tion, an extracorporeal blood oxygenation apparatus(an oxygenator) performs the lung function by saturat-ing the venous blood with oxygen and removing car-bon dioxide from it. For the first time, a surgical inter-vention with the use of an oxygenator was performedby Gibbon in the mid-1950s [1].
The oxygenator developed by Gibbon belonged todevices of the stationary film type and was a set of sixto eight wire screens with a length of 60 cm and a widthof 10 cm vertically placed into a plastic container, inwhich blood f lew from top to bottom, thus forming astable blood film contacting with oxygen [2]. The sec-ond variety of film-type oxygenators was representedby rotating oxygenators, in which a large area of thecontact of blood with the gas was achieved due to therotation of the moving parts, cylinders [3] or disks [4].One of the main disadvantages of film-type oxygen-ators were their bulkiness resulting from the require-ment of providing an acceptable area of the contact ofblood and the gas phase and time-consuming andcomplex maintenance.
Bubble oxygenators [5], which replaced film oxy-genators, became the most common among direct-contact oxygenators due to the smaller size and someother advantages. In a general case, a bubble oxygen-
ator was a vertical column, to the bottom part of whichblood and gaseous oxygen were fed, and the foamyblood from the upper part of the column entered adefoaming chamber, where the surface tension of thegas bubbles decreased due to the silicone coating of thesurface of the chamber, which led to the merging ofsmall bubbles into large bubbles that f loated up in aspiral tubular tank, while oxygenated blood f lew down[2]. The popularity of bubble oxygenators was associ-ated with a series of advantages, namely, a high effi-ciency due to the large surface of oxygen bubbles, por-tability, simplicity of design free from moving parts,and the fact that the components of the unit were dis-posable and ready-to-sterilize.
The main disadvantage of direct-contact oxygen-ators was a short duration of application withoutadverse effects, which was limited to four hours [2].The direct contact of blood with air and plastic ormetallic parts of the unit led to the damage and break-down of erythrocytes and platelets, denaturation ofproteins, a high risk of hemolysis, disruption of thecoagulation system, and risk of hemorrhages [2, 6]. Inaddition, prolonged extracorporeal perfusion couldlead to the deterioration of peripheral perfusion, aci-dosis, and progressive organ failure [2]. The applica-tion of bubble oxygenators was also associated with arisk of gaseous embolism [4].
The main disadvantages of direct-contact oxygen-ators associated with a short duration of operation anda high risk of development of complications were over-come with the introduction of membrane-type oxy-genators [4], in which the blood is separated from the
201

202 EVSEEV et al.
gas phase by a semipermeable membrane and the gas-eous exchange is executed in the process of diffusion ofgases through the membrane, into clinical practice.The modern extracorporeal membrane oxygenationtechnology (ECMO) is aimed not only at saving apatient in a critical state during surgical interventionsbut is also intended for patients with potentially invert-ible disorders of cardiovascular and/or respiratory sys-tems, the treatment of which using standard therapy isineffective [7].
NONPOROUS (DIFFUSION) POLYMER MEMBRANES FOR ECMO
The development of membrane technology andappearance of new polymer asymmetric gas-separa-tion membranes in the late 1950s [6] made it possibleto apply such membranes as a diffusion barrier for theseparation of blood from the gas phase. Thus, one ofthe first attempts of creating membrane oxygenatorswas the use of a nonporous membrane made of ethylcellulose with an area of 25 m2 in an oxygenator [8].However, a quite high hydrophilicity of ethyl celluloseled to the leakages of plasma through the membrane,which substantially shortened its service life [2].Replacing the material of the membrane by moremechanically strong and hydrophobic materials such aspolyethylene [9] and polytetrafluoroethylene (Teflon)[10] made it possible to solve this problem [2].
Overall, decreasing the degree of damage of eryth-rocytes was an obvious advantage of membrane oxy-genators upon comparison with direct-contact oxy-genators; at the same time, researchers came across aseries of problems from the very start of the develop-ment [2]:
—the membrane became an additional barrier forgas exchange;
—there were still no suitable materials for mem-branes possessing high gas permeability, mechanicalstrength, possibility for obtaining thin films withoutthrough defects, and absence of the interaction ofblood with the artificial surface in the late 1950s;
—a problem of optimum distribution of the f lowsof gas and blood for the provision of efficient gasexchange emerged.
The aforementioned transition to hydrophobicmaterials at first also possessed a series of limitationsassociated with the low velocity of transport of oxy-gen and CO2. The problem was partially solved bythe introduction of hydrophobic membranes basedon polyorganosiloxanes possessing high oxygen per-meability; here, the CO2 permeability for thesematerials is five- to sevenfold higher [11]. Thus, forpolydimethylsiloxane (PDMS), the coefficient ofoxygen permeability P(O2) is 600 Barrer (1 Barrer =10−10 cm3 (STP) cm cm−2 s−1 cmHg−1), while it is20 Barrer for ethyl cellulose, 1 to 8 Barrer for poly-ethylene, and 0.004 Barrer for Tef lon [11]. According
MEMBRANES AND M
to the data of [2], the oxygen permeability for PDMSmembranes with different thicknesses of the continuouslayer varies from 35 to 90 cm3 (O2) cm−2 s−1 cmHg−1,while it is 40-fold smaller for Teflon membranes.Because of this, a membrane made of PDMS developedby Kolobov [12] has been a standard of a membranematerial for oxygenators for almost 50 years [13].
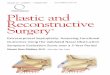
The problem of intensification of the gas exchangeprocess in an oxygenator was tried to be solved bymeans of design decisions. Flat sheet membranes sep-arated by separating screens were used in the firstmembrane oxygenators for the provision of the f low ofgas and blood (Fig. 1) followed by their assembly intoa f lat-parallel structure like, e.g., in a Travenol oxy-genator [4], or in the form of a spiral-wound-typeapparatus like in a cylindrical Kolobov oxygenator [4].
As opposed to alveolar capillaries, the diameter ofwhich (3–7 μm) is smaller than the erythrocyte size(6–8 μm), the channels in f lat-plate-type or spiral-wound-type oxygenators are much wider. Because ofthis, one of the limiting stages of the membrane oxy-genation process is the rate of diffusion of the gas inthe liquid phase of blood. Thus, it was experimentallyshown [14] that the velocity of the transport of oxygenin blood corresponds to the Fick law, i.e., it is propor-tionate to the square thickness of the blood film con-tacting with the membrane and diffusion resistance ofthe boundary layer. In the case of a laminar f low in theboundary layer of the blood contacting with the gas-exchange membrane, the equilibrium with the gasphase is rapidly achieved. Further movement of thegas in the blood is limited by the rate of molecular dif-fusion in the liquid phase. The experimentally deter-mined coefficients of diffusion in blood at 37°C are1.73 × 10−5 cm2/s for oxygen and 1.45 × 10−5 cm2/s forcarbon dioxide [2]. Here, the also experimentallydetermined thickness of the blood layer contactingwith the membrane under saturation with oxygen is 50to 700 μm at different velocities of the blood f low [14].Therefore, more effective gas exchange requires eitherthe sizes of the channels in the oxygenator to be smallerthan the corresponding thickness of the blood layer in thecase of laminar flow along the membrane or the bloodflow along the membrane not to be laminar.
The problem of diffusion resistance of the bound-ary layer was proposed to be solved by introducing sec-ondary f lows in the blood, which lead to the distur-bance of the laminar f low and intensification of theconvective mass transfer, which leads to an increase inthe efficiency of gas exchange. Secondary f lows can beboth passive, formed due to the movement of theblood along concave channels along a spiral contouror due to the placement of additional turbulence pro-moters into the channels [15, 16], and active, inducedby an external action, e.g., periodic deformation of themembrane, rotation of the membrane, etc. [17–21].
The development of membrane technology led tothe creation of polymer membranes in the form of hol-
EMBRANE TECHNOLOGIES Vol. 1 No. 4 2019

MEMBRANES IN EXTRACORPOREAL 203
Fig. 1. The layout view of the element of a membrane oxygenator and its use in a (1) parallel-plate and (2) cylindrical versions.
Blood
Blood
O2
O2
Blood flow
Blood flow
O2 flow
O2 flow
1
2
low fibers (capillaries), the internal and external diam-eter of which is set by the parameters of the die holeupon their formation. Consequently, this led to thedevelopment of capillary oxygenators, the first ofwhich had capillaries with a diameter of 100–500 μm[22]. The small diameter of the hollow fibers made itpossible to increase the efficiency of gas exchange duethe decrease in the size of the channels and thicknessof the blood layer under saturation with oxygen nearthe gas-exchange surface. In addition, capillary oxy-genators had another advantage consisting in the bet-ter control of the f lows in the gas and blood chambersin comparison with the f lat plate and spiral woundoxygenators. Further studies in this field were aimed atthe search for the optimum configuration of the f lows,namely, with a blood f low inside the fiber and oxygenoutside [23, 24] (Fig. 2, 1) or an inverse configurationwith a blood f low outside the fiber and oxygen inside[25–27] (Fig. 2, 2).
The advantage of the configuration of hollow-fibermembranes with a selective layer and a blood f lowinside the fiber consists in the possibility for creating alaminar blood f low without diffusion limitationsbecause, in the case of a laminar f low, the thickness ofthe blood layer under saturation with oxygen can besmaller than the internal diameter of the fiber, whichis overall close to the configuration of alveolar capil-laries. However, a substantial disadvantage of suchhollows fibers was an increase in the hydrodynamicresistance of the channels, which led to an increase inthe pressure differential in the oxygenator and defor-mation of the formed elements. In addition, the
MEMBRANES AND MEMBRANE TECHNOLOGIES V
defects of a continuous diffusion layer of such mem-branes, especially in the orifice of the hollow-fibermodule, led to an increased adsorption of blood pro-teins and an increase in the probability of clotting.Because of this, the configuration of hollow-fibermembranes with a selective layer and a blood f lowoutside the fiber is adopted in the modern hollow-fiber oxygenators. The advantage of such a configura-tion is the possibility to control the packing of thefibers for the creation of a small thickness of channelswith a turbulent blood f low. It was shown during thetests that a configuration, in which the blood f low isperpendicular to the hollow fiber, through which oxy-gen is fed, possesses the best characteristics of gasexchange [28–30] (Fig. 3). Currently, the design ofmost oxygenators is based on this principle.
However, the question about the influence of theorientation of the fibers in the module still remainsopen [31–33] because both their parallel and criss-cross arrangement is possible (Fig. 4).
One of the latest promising achievements in thefield of creation of oxygenators is the implementationof the inventions of the microfluidics technology,which makes it possible to create, thus far at a level oflaboratory specimens, microoxygenators with a thick-ness of the membrane of up to 10 μm and a size of thechannel for blood of up to 15 μm, which substantiallyincreases the efficiency of gas exchange [4, 34] anddecreases the blood prime volume in comparison withhollow-fiber ones.
Such microoxygenators are generally created usinga microlithography technology in several steps. One of
ol. 1 No. 4 2019

204 EVSEEV et al.
Fig. 2. The layout view of the blood f low (1) inside and (2) outside a hollow-fiber membrane.
Blood flow
Blood flow
Blood flow Blood flowO2 flow
O2 flow
O2 flow
O2 flow
1 2
Fig. 3. The layout view of the element of a hollow-fiber membrane oxygenator and its use in (1) parallel-plate and (2) cylindricalversions.
Blood
Blood
Blood
Blood
O2
O2
O2
O2
Blood
O2 flow
1
2
flow
such processes is described in detail in [34]. First, pro-
filed lithographic molds with the pattern for the chan-
nels for gas and blood are created on a silicon plate.
Then the molds are filled with PDMS, and plates
MEMBRANES AND M
made of PDMS with the rectangular profiles of the
channels for gas and blood with a height of 15–80 μm
and a width of 100–500 μm are formed (Fig. 5, 1). A
thin diffusion membrane (10–20 μm) is formed on a
EMBRANE TECHNOLOGIES Vol. 1 No. 4 2019

MEMBRANES IN EXTRACORPOREAL 205
Fig. 4. The scheme of orientation of the fibers in the module of an oxygenator in (1) parallel and (2) crisscross designs.
21
Blood O2
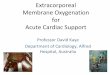
Fig. 5. The layout view of a microfluid module of an oxygenator: (1) plates made of PDMS with the channels for blood and gas,(2) a diffusion membrane, (3) an assembled micromodule, and (4) the assemblage of micromodules.
2
3
41
1
PDMS with channels for blood
PDMS with channels for О2
15–80 µm
100–500 µm
100–500 µm
10–20 µm
15–80 µm
silicon support generally made of the same PDMS(Fig. 5, 2). Then all the three parts are stacked and airtightened to form a single micromodule (Fig. 5, 3).
The advantage of such a technology is the modu-larity (Fig. 5, 4), i.e., the possibility for achieving therequired productivity of the oxygenator via the assem-blage of an appropriate number of micromodules [35].The profiles of the corresponding channels for gas andblood depend on both the applied microprinting tech-nology and the design of the micromodule. These pro-files can be complex [36] and even three-dimensional[37]. The disadvantage of such structures is the princi-pal limitation of the microlithographic technology,namely, the rectangular shape of the channels forblood, which promotes the formation of stagnationzones. The use of PDMS as the material, which limitsthe duration of use of a microoxygenator, is a disad-vantage as well.
MICROPOROUS MEMBRANES FOR ECMO
As it was already noted above, PDMS-based mate-rials were the most widely used for the creation ofmembranes for ECMO. However, these polymerspossess a series of substantial disadvantages, the mainof which is clotting on the surface of the membranesupon prolonged operation [38–42]. In addition, the
MEMBRANES AND MEMBRANE TECHNOLOGIES V
need for preserving the mechanical strength of themembrane imposed certain limitations on its thick-ness, which, consequently, affects the efficiency of gasexchange. An alternative approach turned out to be theuse of microporous materials (Fig. 6, 2) proposed forthe first time by McCaughan [43], which, as opposedto nonporous (diffusion) membranes (Fig. 6, 1), havethrough pores providing a direct contact of blood withair, which leads to an increase in the efficiency of gasexchange.
The first experiments were performed with the useof membranes made of microporous polyethylene,sintered nickel, and cellulose acetate-based hydropho-bic polymers [2]; however, due to the large pore diam-eter (1–10 μm), significant plasma leakage [44] and ahigh risk of air embolism in the case of exceedance ofthe gas pressure were noted. Only with the appearanceof hydrophobic ultrafiltration membranes with submi-cron pores, the most widely used of which is micropo-rous polypropylene (PP) [45, 46] with a pore diameterof up to 0.03 μm and porosity of up to 55% [47], thepenetration of plasma into the pores started to be pre-vented by surface tension forces. However, completeprevention of plasma leakage failed, in which connec-tion the effective duration of operation of oxygenatorswith microporous membranes was limited to severaldays. Several mechanisms of leakage of plasma into
ol. 1 No. 4 2019

206 EVSEEV et al.
Fig. 6. The layout view of (1) diffusion and (2) microporous membranes.
Blood flow
O2 flow
2Blood flow
O2 flow
1
the pores were proposed including the evaporation ofwater from plasma followed by the condensation by acooling gas [48] and formation of a wetting film, thepenetration of plasma due to the increased pressure ofthe blood f low [49] as well as the participation ofphospholipids in the wetting micropores [50]. By non-specifically binding to the surface of the material,blood phospholipids lead to the hydrophilization ofthe entrance to the pores, which provides the penetra-tion of plasma deep into the pores due to the capillaryforces and further coating of the pore walls with phos-pholipids until the entire length of the pore is filledwith plasma, which significantly decreases the gastransfer through the membrane due to the lower rate ofdiffusion of oxygen in plasma in comparison with air.Ultimately, all this leads to the need for the replace-ment of the oxygenator. Despite this, the high effi-ciency of gas exchange, minor blood trauma, portabil-ity, simplicity, and relatively low cost allowed oxygen-ators with microporous membranes to completelyreplace bubble oxygenators [40].
MODERN POLYMER MEMBRANESFOR ECMO
For preventing plasma leakage [51–54], it was pro-posed to use composite membranes—microporousfibers coated with siloxane derivatives. Here, in thecase of incomplete coating of the surface pores of themembrane, the high hydrophobicity of the PDMSlayer prevents the penetration of water into the chan-nels for gas. In the case of complete coating of the sur-face pores, blood contacts with a continuous thin layerof PDMS like in the case of Kolobov oxygenators.Despite the decrease in the efficiency of gas exchangedue to the diffusion gas transfer through the thin con-tinuous PDMS coating, this solution was consideredas an acceptable compromise for increasing the dura-bility of the oxygenator.
MEMBRANES AND M
Three-layered membranes on the basis of microp-
orous polyethylene with a continuous internal layermade of thermoplastic polyurethane [55] (P(O2) = 1–
3 Barrer [56]) or asymmetric membranes made of f lu-orine-containing polyimide [57] (P(O2) = 14–16 Bar-
rer [58]) were proposed as the alternative versions ofdiffusion hollow-fiber membranes. Since the permea-
bility of these materials is substantially lower than the
permeability of PDMS, hollow-fiber membranesmade of polyurethanes and polyimides did not find
their application. Hydrophobic amorphous perfluori-
nated copolymers of tetrafluoroethylene and perflu-oro(2,2-dimethyl-1,3-dioxole), Teflons AF, in partic-
ular, AF 2400 [59], the oxygen permeability of which(P(O2) = 990–1100 Barrer [56, 60]) exceeds the per-
meability of PDMS, were proposed as the materialsfor the continuous coating of composite membranes
alternative to PDMS. In recent years, a perfluorinated
amorphous polymer, polyperfluoro(2-methyl-2-ethyl-dioxole-1,3), has also been proposed as the
material for the continuous coating [61]. This polymer
is also a very promising material due to the high oxy-gen permeability coefficient (P(O2) = 850 Barrer [62])
in comparison with PDMS and high hemocompatibil-ity that is higher when compared to AF 2400 [61].
However, the implementation of diffusion mem-
branes made of poly(4-methyl-1-pentene) (PMP)[63–66] which combine a microporous internal struc-
ture with a dense external layer contacting with blood
[4] can be considered as the most practically import-ant achievement in the field of membrane materials
for ECMO. Due to the higher hemocompatibility in
comparison with membranes on the basis of PDMS[67], high efficiency of gas exchange and relatively low
resistance [68], absence of plasma leakages [69], andpossibility of operating for several weeks [67], PMP
became the most widely used membrane material for
oxygenators (Table 1) despite a significantly lower
EMBRANE TECHNOLOGIES Vol. 1 No. 4 2019

MEMBRANES AND MEMBRANE TECHNOLOGIES Vol. 1 No. 4 2019
MEMBRANES IN EXTRACORPOREAL 207
Tabl
e 1.
Ch
ara
cte
rist
ics
of
ox
ygen
ato
rs
PP
is
po
lyp
rop
yle
ne,
PM
P i
s p
oly
meth
ylp
en
ten
e,
an
d N
DA
is
no
data
ava
ila
ble
.
Man
ufa
ctu
rer
Sy
stem
Mem
bra
ne
ma
teri
al
Mem
bra
ne
are
a,
m2
Blo
od
velo
cit
y,
L/m
in
Pri
min
g
vo
lum
e,
cm
3
Op
era
tio
n
life
, d
ay
sR
ef.
Med
tro
nic
Aff
init
y F
usi
on
PP
2.5
1.0
–7.0
26
00
.25
[7
0]
Aff
init
y N
TP
P2
.51.0
–7.0
27
00
.25
[71
]
Ma
qu
et
PL
SP
MP
1.8
0.5
–7.0
25
014
[7
2]
HL
SP
MP
1.8
0.5
–7.0
273
30
[73
]
QU
AD
RO
X-i
Ad
ult
PP
1.8
0.5
–7.0
215
0.2
5 [
74
]
Teru
mo
CA
PIO
X®
RX
25
PP
2.5
0.5
–7.0
25
00
.25
[75
]
So
rin
Eo
s E
CM
OP
MP
1.2
Up
to
5.0
15
05
[7
6]
Xen
ios
Med
os
Hil
ite
PP
1.9
1.0
–7.0
32
00
.25
[7
7]
Med
os
Hil
ite L
TP
MP
1.9
1.0
–7.0
32
010
–14
[7
7]
Eu
rose
tsE
CM
O A
DU
LT
PM
P1.3
50
.3–
4.0
19
014
[7
8]
A.L
.ON
E A
F P
LU
SP
P1.6
5U
p t
o 7
.02
25
0.2
5 [
79
]
Mic
rop
ort
Kew
ei
Ox
ygen
ati
on
Sy
stem
PP
2.0
Up
to
6.0
16
00
.25
[8
0]
Nip
roV
ita
lP
P2
.00
.5–
7.0
18
0n
ot
detd
. [
81
]
Bri
zio
PP
2.2
Up
to
7.0
237
'' [
82
]

208 EVSEEV et al.
Table 2. Biocompatible coatings of the membranes used in oxygenators
Manufacturer Trade name Key component Ref.
Medtronic Balance Poly(ethylene oxide)/sulfate/sulfide groups [86]
Trillium Poly(ethylene oxide)/sulfate/sulfide groups/heparin [103, 104]
Cortiva BioActive Surface Heparin [105]
Maquet Bioline Heparin [106]
Terumo X-coating Poly(2-methoxyethyl acrylate) [88]
Sorin P.h.i.s.i.o Phosphoryl choline [76]
Xenios rheoparin Heparin [107]
X.EED Nonheparin coating
Eurosets AGILE Phosphoryl choline [79]
Nipro E8 Polymer on the basis of polyethylene glycol [82]
oxygen permeability (P(O2) = 27 Barrer [56]) in com-
parison with PDMS.
Overall, currently, a situation with the division ofoxygenators to two main classes with respect to theduration of use has arisen, namely, oxygenators withmicroporous membranes for short-term use and oxy-genators with nonporous membranes for long-termoperation [2]. The main characteristics of the cur-rently used oxygenators are presented in Table 1.
One of the key parameters of oxygenators is theprime volume, a decrease in which promotes adecrease in the risk of development of hemodynamiccomplications in critical patients. The most importantparameters are the area of the membrane and bloodvelocity through the oxygenator which determine theefficiency of gas exchange, i.e., the possibility ofincreasing the level of the partial pressure of oxygenpO2 from 50–70 to 300–500 mmHg and attainment of
a normal concentration of carbon dioxide at the outletfrom the oxygenator. Generally, the blood velocity is60–80 mL/kg/min [83].
SURFACE MODIFICATION OF ECMO MEMBRANES
The need for providing the operational capacity ofdiffusion membranes upon long-term operation dic-tates the modern trends in the development of mem-brane technology which consist not only in the searchfor new biocompatible materials which can be used asmembranes but also in the improvement of the existingmembrane materials by means of modifying the surfacefor the purpose of increasing its biocompatibility.
On the one hand, the problem of increasing thebiocompatibility was proposed to be solved by meansof modifying the surface of a membrane by variouspolymer compounds that change its properties. Forexample, the polymerization of acrylamide on the sur-face of a silicone membrane led to a decrease in theadsorption of protein and adhesion of platelets [84],the crosslinking of D-gluconamido ethyl methacrylate
MEMBRANES AND M
to the surface of polypropylene led to an increase inthe hydrophilicity and biocompatibility [85],Medtronic uses a composite coating on the basis ofpoly(ethylene oxide) which provides hydrophilicity aswell as sulfate and sulfonate groups for imparting thesurface with a negative charge [86, 87], and Terumouses a coating on the basis of poly(2-methoxyethylacrylate) [88, 89]; in addition, poly(vinylpyrrolidone)[90], α-allyl glycoside [91] as well as polyethylene gly-col and its derivatives [92–95] are used for the modifi-cation. For example, the efficiency of the latter as ahemocompatible coating of the PDMS membraneand channels for blood of a microfluidic artificial lungwas shown [96].
However, one of the most widely used modifica-tion methods is the covalent binding of heparin mole-cules with the surface of a membrane; it is currentlyused by many companies in their coatings (Table 2). Ithas been found that a heparin coating decreases theactivation of platelets and complement [97, 98] as wellas possesses anti-inflammatory properties [99, 100].
Another widely used option of increasing biocom-patibility is coating with phosphoryl choline (Table 2)which mimics the external surface of an erythrocytemembrane [101], which leads to a decrease in the adsorp-tion of proteins on the surface of the membrane and, as aconsequence, an increase in biocompatibility [102].
The main currently used biocompatibility coatingsof membranes are presented in Table 2.
Therefore, the doubtless importance of ECMO forthe life support of patients in the case of critical statesfound a reflection in the development of membranetechnology. By using the recent advances in the fieldof creation of membranes, a huge way of evolution ofboth design approaches (the transition from flat mem-branes to a hollow fiber) and use of membrane mate-rials (from Teflon and polydimethylsiloxane to poly-methylpentene) has been overcome over 60 years.However, the development has not stopped on this,which manifests itself in the implementation of themethods of modification of the surface of membranes
EMBRANE TECHNOLOGIES Vol. 1 No. 4 2019

MEMBRANES IN EXTRACORPOREAL 209
for increasing their biocompatibility, synthesis of newmembrane materials as well as development of newapproaches in the design engineering of oxygenators.
FUNDING
This work was performed within the state task to the
Topchiev Institute of Petrochemical Synthesis, Russian
Academy of Sciences.
REFERENCES
1. J. H. Gibbon, Jr., Minn. Med. 37, 171 (1954).
2. M. W. Lim, Anaesthesia 61, 984 (2006).
3. J. A. Wegner, J. Cardiothorac. Vasc. Anest. 11, 275(1997).
4. T. Yeager and S. Roy, Artif. Organs 41, 700 (2017).
5. R. A. DeWall, V. L. Gott, C. W. Lillehei, et al., Surg.Clin. North Am. 36, 1025 (1956).
6. L. De Bartolo, E. Curcio, and E. Drioli, MembraneSystems: For Bioartificial Organs and Regenerative Med-icine (Walter de Gruyter, Berlin, 2017).
7. S. V. Zhuravel’, D. A. Kosolapov, and M. V. Ketskalo,Transplantologiya, No. 4, 28 (2014).
8. G. H. Clowes, Jr., A. L. Hopkins, and W. E. Neville,J. Thorac. Surg. 32, 630 (1956).
9. W. J. Kolff and R. Balzer, Trans. Am. Soc. Artif. Int.Organs 1, 39 (1955).
10. G. H. Clowes, Jr. and W. E. Neville, ASAIO J. 3, 52(1957).
11. W. L. Robb, Ann. N. Y. Acad. Sci. 146, 119 (1968).
12. T. Kolobow and R. L. Bowman, ASAIO J. 9, 238(1963).
13. L. Lequier, S. B. Horton, D. M. McMullan, andR. H. Bartlett, Pediatr. Crit. Care Med. 14 (Suppl. 1), 7(2013).
14. T. I. Marx, W. E. Snyder, A. D. St. John, and C. E. Moeller,J. Appl. Physiol. 15, 1123 (1960).
15. W. Dorson, Jr., E. Baker, and H. Hull, Trans. Am. Soc.Artif. Int. Organs 14, 242 (1968).
16. E. C. II. Peirce and W. R. Dibelius, Trans. Am. Soc.Artif. Int. Organs 14, 220 (1968).
17. S. L. Frantz, P. Chopra, A. L. Goldenberg, et al., Trans.Am. Soc. Artif. Int. Organs 14, 233 (1968).
18. R. H. Bartlett, P. A. Drinker, N. E. Burns, et al., Trans.Am. Soc. Artif. Int. Organs 18, 369 (1972).
19. J. D. Gaylor, J. F. Murphy, J. A. Caprini, et al., Trans.Am. Soc. Artif. Int. Organs 19, 516 (1973).
20. B. J. Bellhouse, F. H. Bellhouse, C. M. Curl, et al.,Trans. Am. Soc. Artif. Int. Organs 19, 72 (1973).
21. K. L. Dorrington, J. P. Gardaz, B. J. Bellhouse, andM. K. Sykes, J. Biomed. Eng. 8, 36 (1986).
22. B. R. Bodell, J. M. Head, L. R. Head, et al., J. Thorac.Cardiovasc. Surg. 46, 639 (1963).
23. M. H. Weissman and L. F. Mockors, J. Eng. Mech. Div.94, 857 (1968).
24. K. Tanishita, G. Panol, P. D. Richardson, and P. M. Gal-letti, Artif. Organs 18, 797 (1994).
MEMBRANES AND MEMBRANE TECHNOLOGIES V
25. J. D. S. Gaylor, S. Hickey, G. Bell, and J. M. Pei, Per-fusion 9, 173 (1994).
26. G. Catapano, A. Wodetzki, and U. Baurmeister, Int. J.Artif. Organs 15, 327 (1992).
27. N. Matsuda and K. Sakai, J. Membr. Sci. 170, 153(2000).
28. S. Rajasubramanian, K. D. Nelson, P. Shastri, et al.,ASAIO J. 43, M710 (1997).
29. M. C. Yang and E. L. Cussler, AIChE J. 32, 1910(1986).
30. L. F. Mockors and R. Leonard, Trans. Am. Soc. Artif.Int. Organs 31, 628 (1985).
31. S. R. Wickramasinghe, M. J. Semmens, and E. L. Cus-sler, J. Membr. Sci. 69, 235 (1992).
32. K. Nagase, F. Kohori, and K. Sakai, Biochem. Eng. J.24, 105 (2005).
33. K. Nagase, F. Kohori, K. Sakai, and H. Nishide,J. Membr. Sci. 254, 207 (2005).
34. T. Kniazeva, J. C. Hsiao, J. L. Charest, and J. T. Boren-stein, Biomed. Microdevices 13, 315 (2011).
35. T. Kniazeva, A. A. Epshteyn, J. C. Hsiao, et al., Lab.Chip. 12, 1686 (2012).
36. D. M. Hoganson, J. L. Anderson, E. F. Weinberg,et al., J. Thorac. Cardiovasc. Surg. 140, 990 (2010).
37. N. Rochow, A. Manan, W. I. Wu, et al., Artif. Organs38, 856 (2014).
38. M. P. Kaye, J. B. Pace, S. J. Blatt, and R. J. Ferguson,J. Surg. Res. 14, 58 (1973).
39. R. C. Dutton and L. H. Edmunds, J. Biomed. Mater.Res. 8, 163 (1974).
40. J. D. S. Gaylor, J. Biomed. Eng. 10, 541 (1988).
41. E. Khoshbin, C. Westrope, S. Pooboni, et al., Perfu-sion 20, 129 (2005).
42. M. C. Belanger and Y. Marois, J. Biomed. Mater. Res.58, 467 (2001).
43. J. S. McCaughan, Jr., R. Weeder, J. Schuder, andW. S. Blakemore, J. Thorac. Cardiovasc. Surg. 40, 574(1960).
44. P. Aebischer, M. Goddard, and P. M. Galletti, MaterialsScience and Technology—A Comprehensive Treatment,vol. 14: Medical and Dental Materials, Ed. by R. W. Cahn,P. Haasen, E. J. Kramer, and D. F. Williams, (Wiley–VCH, Weinheim, 1992), p. 131.
45. K. Suma, T. Tsuji, Y. Takeuchi, et al., Ann. Thorac.Surg. 32, 558 (1981).
46. J. J. Kim, T. S. Jang, Y. D. Kwon, et al., J. Membr. Sci.93, 209 (1994).
47. W. J. Federspiel, and K. A. Henchir, in Encyclopedia ofBiomaterials and Biomedical Engineering (Marcel Dek-ker, 2004), p. 910.
48. K. Mottaghy, B. Oedekoven, H. Starmans, et al., Trans.Am. Soc. Artif. Int. Organs 35, 640 (1989).
49. Y. Tamari, A. J. Tortolani, M. Maquine, et al., Artif.Organs 15, 15 (1991).
50. J. P. Montoya, C. J. Shanley, S. I. Merz, and R. H. Bart-lett, ASAIO J. 38, M399 (1992).
51. T. Shimono, Y. Shomura, I. Hioki, et al., Ann. Thorac.Surg. 63, 1730 (1997).
52. S. Kawahito, T. Maeda, T. Motomura, et al., Artif.Organs 25, 494 (2001).
ol. 1 No. 4 2019

210 EVSEEV et al.
53. S. Kawahito, T. Motomura, J. Glueck, and Y. Nose,Ann. Thorac. Cardiovasc. Surg. 8, 268 (2002).
54. H. J. Eash, H. M. Jones, B. G. Hattler, and W. J. Feder-spiel, ASAIO J. 50, 491 (2004).
55. J. Kamo, M. Uchida, T. Hirai, et al., Artif. Organs 14,369 (1990).
56. L.W. McKeen, Permeability Properties of Plastics andElastomers, 4th Ed. (Elsevier, Amsterdam, 2017).
57. H. Kawakami, Y. Mori, J. Takagi, et al., ASAIO J. 43,M490 (1997).
58. Database on Gas Separation Parameters of Glassy Poly-mers (Informregistr RF, 1998), No. 3585 [in Russian].
59. S. M. Nemser and J. Olpin, US Patent No. 5902747(1999).
60. A. Yu. Alentiev, Yu. P. Yampolskii, V. P. Shantarovich,et al., J. Membr. Sci. 126, 123 (1997).
61. A. Yu. Alentiev, N. A. Belov, R. Yu. Nikiforov, et al.,Pet. Chem. 58, 740 (2018).
62. N. Belov, R. Nikiforov, E. Polunin, et al., J. Membr.Sci. 565, 112 (2018).
63. G. Peek, H. Killer, R. Reeves, et al., ASAIO J. 48,M480 (2002).
64. S. Horton, C. Thuys, M. Bennett, et al., Perfusion 19,17 (2004).
65. J. M. Toomasian, R. J. Schreiner, D. E. Meyer, et al.,ASAIO J. 51, 390 (2005).
66. F. Formica, L. Avalli, A. Martinoet al., ASAIO J. 54, 89(2008).
67. M. Cypel, and S. Keshavjee, Regenerative MedicineApplications in Organ Transplantation, Ed. by G. Orlando(Elsevier, Amsterdam, 2014), p. 683.
68. E. Khoshbin, N. Roberts, C. Harvey, et al., ASAIO J.51, 281 (2005).
69. M. Strueber, Thorac. Surg. Clin. 25, 107 (2015).
70. Medtronic: Affinity Fusion (2017). http://medtronic.com/content/dam/medtronic-com/products/cardiovascular/cardiopulmonary/affinity-fusion-oxygenation/docu-ments/201303375cEN_Affinity_Fusion_Brochure.pdf.Assessed November 22, 2018.
71. Medtronic: Trillium Affinity NT. https://webroot146.s3.amazonaws.com/img/catalogues/1485754378-BrochureTrillium Affinity NT.pdf. Assessed November 22, 2018.
72. Maquet Medical Equipment and Instruments: Life-Sus-taining Systems PLS (2012) [in Russian]. http://www.maquet.ru/files/products/maquet_PLS_2.pdf. AssessedNovember 22, 2018.
73. Getinge HLS Set Advanced Brochure (2015). www.getinge.com/siteassets/products-a-z/hls-set-advanced/hls_set_advanced_mcp_br_10039_en_1_screen.pdf. AssessedNovember 22, 2018.
74. Getinge Quadrox-i Small Adult and Adult (2015).www.getinge.com/siteassets/products-a-z/quadrox-i-adult-small-adult/quadroxi_smalladult_adult_mcp_br_10075_en_1_screen.pdf. Assessed November 22, 2018.
75. Cardion CAPIOX® RX 25 Oxygenators (2005). http://www.cardion.cz/file/387/brozura-rx25-oxygenator.pdf.Assessed November 22, 2018.
76. LivaNova EOS ECMO (2016). https://d3sgr6wl8mk08r.cloudfront.net/livanova-public/media/resources01/
ous_only_livanova_livanova_eos_ecmo_09295-85b.pdf.Assessed November 22, 2018.
77. Xenios: Hilite Product Family (2016). www.xenios-campus.com/Customizing/global/plugins/Services/UICom-ponent/UserInterfaceHook/SimpleCms2/Resource/Public/Media/Bestellformular Partner Vorschaubilder/Medos_product_brochure_hilite_product_family_EN_001_2016_02.pdf. Assessed November 22, 2018.
78. Eurosets Adult Oxygenators Catalogue (2017). www.euro-sets.com/wp-content/uploads/2016/07/Adult_catalogue_oxy_52017.pdf. Assessed November 22, 2018.
79. Eurosets AF Plus Catalogue (2017). www.eurosets.com/wp-content/uploads/2016/07/AF_Plus_catalogue_12-2017.pdf. Assessed November 22, 2018.
80. MicroPort Kewei Membrane Oxygenation System. http://www.kewei.com.cn/en/show_product.aspx?ProductsId=172&CateID=100&ProductsCateID=100&Order=98.Assessed November 22, 2018.
81. Nipro VITAL Hollow Fiber Oxygenator for Adult.www.nipro.co.jp/en/business/device/cardiopulmonary/oxygenator/document/vital.pdf. Assessed November 22,2018.
82. Brizio Nipro Membrane Oxygenator and Venous Reservoirwith Integrated Cardiotomy Filter—Adult. www.nipro.co.jp/en/business/device/cardiopulmonary/oxygenator/docu-ment/brizio_delux_cat.pdf. Assessed November 22, 2018.
83. C. E. Ventetuolo and C. S. Muratore, Am. J. Respir.Crit. Care Med. 190, 497 (2014).
84. Y. Ikada, Polym. J. 23, 551 (1991).
85. Q. Yang, Z.-K. Xu, Z.-W. Dai, et al., Chem. Mater. 17,3050 (2005).
86. Medtronic: Balance Biosurface (2011). http://www.medtronic.com/content/dam/medtronic-com/global/mdt-balance-biosurface.pdf. Assessed November 22,2018.
87. L. Teligui, E. Dalmayrac, G. Mabilleau, et al., Int. Car-diovasc. Thorac. Surg. 18, 763 (2014).
88. L. Schiel, S. Burns, A. Nogawa, et al., Can. Perfus.Can. 11, 8 (2001).
89. B. T. Nutter, A. H. Stammers, R. G. Schmer, et al.,J. Extra-Corp. Technol. 36, 36 (2004).
90. Z.-M. Liu, Z.-K. Xu, J.-Q. Wang, et al., Eur. Polym. J.40, 2077 (2004).
91. R.-Q. Kou, Z.-K. Xu, H.-T. Deng, et al., Langmuir 19,6869 (2003).
92. A. S. Abedneja, G. Amoabediny, and A. Ghaee, Adv.Mater. Res. 816–817, 459 (2013).
93. W. Wang, Z. Zheng, X. Huang, et al., J. Biomed. Mater.Res., Part B: Appl. Biomater. 105, 1737 (2017).
94. S. Zanini, M. Orlandi, C. Colombo, et al., Eur. Phys. J.,D 54, 159 (2009).
95. J. V. Alexander, E. A. Grulke, and J. B. Zwischen-berger, ASAIO J. 62, 690 (2016).
96. K. M. Kovach, M. A. LaBarbera, M. C. Moyer, et al.,Lab. Chip. 15, 1366 (2015).
97. V. Videm, J. L. Svennevig, E. Fosse, et al., J. Thorac.Cardiovasc. Surg. 103, 806 (1992).
98. T. B. Averina, E. A. Andreeva, and E. A. Kiseleva, Klin.Fiziol. Krovoobrashch., No. 1, 68 (2008).
99. S. Gunaydin, Perfusion 19 (Suppl. 1), 33 (2004).
MEMBRANES AND MEMBRANE TECHNOLOGIES Vol. 1 No. 4 2019

MEMBRANES IN EXTRACORPOREAL 211
100. I. V. Ponomarenko, V. M. Shipulin, O. N. Ogurkova,and T. E. Suslova, Patol. Krovoobrashch. Kardiokh-irurg. 17 (2), 51 (2013).
101. Y.-B. Wang, M. Gong, S. Yang, et al., J. Membr. Sci.452, 29 (2014).
102. A. S. Thiara, V. Y. Andersen, V. Videm, et al., Perfu-sion 25, 9 (2010).
103. Medtronic: Trillium (2011). http://www.medtronic.com/content/dam/medtronic-com/products/cardiovascular/cardiopulmonary/trillium-biosurface/documents/trilium-brochure.pdf. Assessed November 22, 2018.
104. D. A. Palanzo, D. L. Zarro, R. M. Montesano, et al.,Perfusion 14, 473 (1999).
105. Medtronic: Cortiva Bioactive Surface (2018). http://www.medtronic.com/us-en/healthcare-professionals/products/cardiovascular/cardiopulmonary/cortiva-bioactive-surface.html. Assessed November 22, 2018.
106. Maquet: Bioline Coating. www.maquet.com/int/products/bioline-coating. Assessed November 22, 2018.
107. Xenios Medos Product Portfolio (2016). www.xenios-campus.com/Customizing/global/plugins/Services/UIComponent/UserInterfaceHook/SimpleCms2/Resource/Public/Media/Bestellformular%20Partner%20Vorschaubilder/Medos_product_portfolio_bro-chure_EN_001_2016_02.pdf. Assessed November 22,2018.
Translated by E. Boltukhina
MEMBRANES AND MEMBRANE TECHNOLOGIES Vol. 1 No. 4 2019