Embed Size (px)
Citation preview

MEMORANDA TABLE OF CONTENTS
MEMORANDA OF SPECIFIC INCIDENTS (date recorded and brief title)
5/25/17 – Grossly inadequate death investigation and lack of Coroner policies
5/30/17 – Delayed case closure / Misclassification of homicide
6/05/07 – Postmortem alteration of body by non-physicians
6/14/17 – Inadequate death investigation and Misclassification as suspicious death
6/14/17 – Intentional deception of case load by omission of a homicide case
6/19/17 – Absence of coroner protocols / Mismanagement of resources for physician-certified deaths
7/03/17 – Office inefficiency with major delay in transcribed narratives
7/24/17 – Intentional misrepresentation by Coroner Sergeant to alter physician scheduling
7/28/17 – Poor management of Coroner's Office with inexperienced personnel
8/01/17 – Misclassification of manner of death without pathologist consultation
8/25/17 – Gross negligence of management of possible fetal homicide
9/05/17 – Restrictive 9 am police briefings
10/01/17 – Significant delay in report transcription delaying finalization of reports
10/05/17 – Unwillingness/Refusal of Sheriff to furnish investigative reports in homicides
10/08/17 – Scheduling and control by Sheriff-Coroner is a disaster
10/18/17 – Release of drug evidence to family in a homicide
11/02/17 – Inadequate death investigation in drowning death
11/09/17 – Inability to recognize appropriate Coroner's Cases
11/27/17 – Inadequate child death investigation (drowning)
12/01/17 – Incomplete death scene investigation
PREVIOUSLY SUBMITTED DOCUMENTS / MEETINGS WITH SHERIFF MOORE
1/15/17 – Quality assurance memo to Dr. Omalu regarding physician scheduling by Coroner
7/20/17 – Complaint against Coroner Sergeant submitted to San Joaquin County Human Resources
7/31/17 – Meeting with Sheriff and Asst. Sheriff/Harassment by Sheriff and inherent conflict of interest
8/17/17 – Meeting with Sheriff et al. regarding physician scheduling/Retaliation, harassment, and
threats against physicians by Sheriff
8/21/17 – Physician Schedule Memorandum submitted by Dr. Parson and Dr. Omalu to Sheriff-Coroner
10/01/17 – Attempt at Physician Control memo submitted to San Joaquin General Hospital

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
GROSSLY INADEQUATE DEATH INVESTIGATION (recorded on 5/25/17 at 3:52 PM):
During the morning of this autopsy (17-1203) on 5/25/17, I read the Coroner narrative and synopsis of this case regarding a decedent who was “found lying on the ground in a grape vineyard wearing a skydiving suit”. The rest of the report described EMS arriving and pronouncing the decedent, etc. but there was literally no other information regarding the circumstances of this man’s death. Specifically, an appropriate and complete death investigation (had one been carried out) would have included, at a minimum, answers to the following questions:
• What kind of plane/aircraft was involved? Was this a commercial business or a private plane? • When did the plane take off? Where was it headed? • Where was the decedent meant to jump and land? • Were there other passengers on the plane? • What were the circumstances of his exiting the aircraft (was he pushed? Did he jump voluntarily?
Did he trip and fall out?)? • What was the elevation of the plane when he exited the aircraft? • What was his demeanor prior to (intoxicated appearing? Excited/nervous? Depressed? – I
subsequently discovered after the autopsy that his father died exactly 2 weeks prior)? • Did other skydivers complete their trip? • What was the decedent’s level of experience with skydiving – was this his first time or was he an
experienced jumper? • Where did he get his equipment (did he rent it, was it his own?) and when was it last checked? • Did witnesses on the aircraft or on the ground see him deploy his parachute and/or attempt to
deploy his safety parachute? • Did his parachute seem to deploy properly? • Was there any radio communication between the decedent while skydiving?
None of this information was present in the Sheriff’s Patrol Deputy’s narrative. It should be noted that a single line in the pre-hospital care/EMS report contained more information than the entire Coroner narrative and synopsis (the EMS report stated that the decedent appeared to freefall for approximately 500 feet per a witness).
Furthermore, although I did not see this article until after the autopsy was complete, more information regarding the circumstances of this man’s death was available through a FOX40 news article1 posted the evening before the autopsy took place (5:54 PM on 5/24/17). Thus, while answers to several of the most basic questions listed above were widely available to the public, the patrol deputy who responded to the scene failed to ascertain them or include them in his/her report.
ABSENCE OF OFFICIAL CORONER PROTOCOLS OR POLICIES
In a related discussion of this case, it should be noted that when I began work on 10/3/16, one of my first questions of the Coroner Sergeant when I acquired access to my desk computer was where I could find the protocols for Coroner’s Office (including, but not limited to: scene investigation for specific scenarios (motor vehicle collisions, infants, drownings, known homicides or suspicious deaths, etc.),
1 http://fox40.com/2017/05/24/skydiver-wearing-wingsuit-killed-in-accident-near-lodi-parachute-center/

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
decedent identification, use of postmortem radiography, morgue safety, specimen handling, evidence collection and handling, postmortem photography, decedent transfer and release, etc.). I was informed that no such written protocols existed, despite the fact that all other departments of the Sheriff’s Office have extensive protocols that are easily available on the department intranet. The complete lack of a single protocol for an entire bureau within the Sheriff-Coroner’s Office demonstrates either a complete disinterest in ensuring that accepted and expected standards of practice are met, a complete ignorance of understanding how and why standards of practice should be created, or a combination of both. Since the performance of an autopsy is a medical procedure performed by licensed physicians, it is no surprise that autopsy and safety protocols are legal requirements in accredited hospitals or other facilities that perform them. I am frankly dumbfounded that not a single protocol exists for any part of the death investigation or morgue functions within this office. Formally written protocols would serve as profoundly useful resources to patrol deputies who physically respond to death scenes, the Coroner detectives who handle the office duties of death investigation, and the Autopsy technicians who prepare everything for and assist with the autopsy. An absence of protocols is exactly the permissive and negligent work environment, created by Sheriff Moore, where massive and irreparable mistakes and negligent or even criminal behaviors can thrive.
Determining the circumstances surrounding a person’s death is the most basic – and essential – duty for which the Coroner’s Office is responsible. In San Joaquin County, a Sheriff’s Patrol Deputy must be able to perform this task in its entirety when s/he responds to the scene of a death. The San Joaquin Sheriff-Coroner system is designed by Sheriff Moore such that Patrol Deputies are the sole representatives for the Coroner’s Office at a death scene – the individuals responding to a body and providing the primary investigation into a death, which ultimately becomes the Coroner narrative that the Forensic Pathologist performing the autopsy must reference prior to the beginning of the examination. The fact that the average Patrol Deputy undergoes no official education or training in death investigation is often blatantly obvious to me when I read Coroner narratives as seen in this case. This lack of experience and training is further exacerbated by the total absence of official written policies and procedures for the Coroner’s Office. Ultimately, this synergistic lack of experience, training, and death investigatory policy sets the stage for incompetent death investigation and serves to increase the workload of the daytime Coroner Deputies/Detectives, Autopsy Technicians and myself, ultimately all at the County taxpayers’ expense. In so many death investigation cases in the County, even the most basic information regarding a person’s death (circumstances and timing of when the decedent was last known alive, how they were acting, scene investigation to suggest non-natural manners of death such as violence or drug intoxication, medical histories or prescription medications, etc.) is non-existent in the Coroner narratives, which wholly undermines the medical investigation into a person’s death.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INAPPROPRIATELY DELAYED CASE CLOSURE (17-0290) (recorded 5/30/17 at 8:12 PM):
In the mid-afternoon on 3/27/17, the senior office assistant forwarded me an email from the Deputy DA (DDA) assigned to the prosecution of the individuals involved in the death of this decedent, who was a pedestrian victim of a hit-and-run; I had already performed the autopsy on 1/30/17. In an email exchange with the DDA, I agreed to expedite the report within 1-2 weeks, and carbon copied (CC) the Coroner Sergeant for his information (he ultimately signs the Coroner’s Report, closing the entire case). I sent an additional email on 3/29/17 to the current Coroner Detectives (the original Coroner Detective on the case had already been transferred out of the Coroner’s Office) while CC’ing the Coroner Sergeant to request the associated police report, stating that I was expediting this report. I subsequently received the police report and was able to finalize my autopsy report on 4/4/17. I submitted my report that day to Dr. Omalu for signature (our standard practice for homicide cases) and sent a new email to the Coroner Detectives, the Coroner Sergeant, the senior office assistant, and Dr. Omalu stating that I was expediting this report and that the DDA would need a copy once the Coroner’s case is closed. Dr. Omalu completed his review and signed it on 4/11/17, where upon it was supposed to have been passed onto the Coroner Detective and then the Coroner Sergeant for completion of the Coroner report. I heard nothing further regarding this case until the DDA emailed me on 5/18/17, stating that a preliminary hearing was scheduled for 6/1/17 and asked if the report was completed, as he had not yet received his copy. That same afternoon (5/18/17) I emailed the Detective and the Coroner Sergeant (CC’ing the office assistant) to inquire as to the status of the case. I received a reply from the office assistant on 5/19/17 saying that she had the case and would get it closed for the DDA. In an additional email exchange with the office assistant on 5/27/17, she stated that she would find the report to get it closed. Then, on 5/30/17 (after a holiday on Monday), I spoke with the office assistant on the phone to discuss where the case was in the review process and that it was still open (i.e. the death certificate manner of death was still listed as “pending”).
After Dr. Omalu signed the autopsy report, I have no knowledge as to the whereabouts of this case or why it was stalled for an additional 7 weeks such that no Coroner’s report was finalized when there was an active request for the case and a set day for a preliminary hearing. This case has been ready for closure for almost 2 months, as the bulk of the work (creating the autopsy report, which integrates toxicology results, gross and microscopic findings, and understanding the circumstances of the incident based on the lengthy police department investigative report I reviewed) was completed by early April, and yet this case remains open just 48 hours before I am scheduled to testify as to my pathological findings in a preliminary hearing. Furthermore, because I originally made the manner of death “pending” after the completion of the autopsy, that manner of death currently stands on the death certificate until it gets updated and closed. I have yet to see if the Sheriff-Coroner’s final manner of death (homicide, as per national guidelines1) will be rendered appropriately, as the death certificate has not yet been amended. In addition, the DDA has been unable to review my autopsy report and thus the injuries that the decedent sustained, which potentially compromises his case and attempt to seek justice for the decedent. It is unfair to render any officer of the court completely unprepared by delaying a public record like the autopsy report and Coroner’s report.
1 Hanzlick R, Hunsaker III JC & Davis GJ. A Guide for Manner of Death Classification. 1st edition. National Association of Medical Examiners. February 2002.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
MISCLASSIFICATION OF MANNER OF DEATH (17-0290) (recorded on 6/1/17 at 8:31 PM):
Also of importance in this case, I originally rendered a “PENDING INVESTIGATION” manner of death at the time of autopsy, as it was only known that it was a hit-and-run with no leads on the vehicle or driver involved. After reviewing the police department’s report prior to finalizing my autopsy report, it had been learned that a witness to the death (in the passenger seat of the very same car that struck the decedent) made statements that supported a deliberate act of the driver to hit the decedent using his vehicle. Per national guidelines for manner of death classification1, using a vehicle as a weapon to harm or kill another person is classified as a medicolegal homicide, which is the conclusion I drew when I submitted my opinion on the final manner of death (an internal Coroner’s worksheet shows which manner of death I selected). On 5/31/17, the day before I was scheduled to testify, I was told that the Coroner’s case was finally completed and on 6/1/17, I was informed by the Coroner Detective on the case that the Coroner Sergeant told him to change the manner of death to “Accident”, which is now what her official death certificate reads. I was never consulted by the Sheriff-Coroner or anyone in the Coroner’s Office as to why I rendered this case a “homicide,” which is a legal requirement by the Coroner according to CA Senate Bill 11892. It should be noted that arriving at different conclusions for manner of death is not due to arbitrary or personal standards – all medical examiners and forensic pathologists routinely refer to these guidelines generated by the National Association of Medical Examiners (NAME). The Sheriff-Coroner cannot claim to be ignorant of the NAME guidelines either, as he referenced them as a source on page 20 in his “2016 Annual Report of the Coroner for San Joaquin County Sheriff”3. Clearly, this is not a difference in the definition of a medicolegal homicide, rather, it is a difference in the education and training of a forensic pathologist (Dr. Omalu and I are both members of NAME) and a peace officer. Although I do not fully understand why a change of the manner of death was made, I can only presume that at a minimum, he does not understand or appreciate the nuanced differences between calling a death a medicolegal homicide (where criminal intent is not necessarily indicated nor implied) and the legal implication of fulfilling the elements of the crime of homicide (often with criminal intent). In addition, I was finally able to speak with the DDA this evening (6/22/17 at 5:51 PM) for the first time since I was made aware of the change in the manner of death. The DDA confirmed the circumstances of the case, as the eye witness was the passenger in the car that struck the decedent. He reaffirmed my understanding of the police investigation in that the driver deliberately accelerated the vehicle to strike the decedent. At no point has the defendant ever claimed that this was an accidental incident. When I informed the DDA that although my opinion on the manner of death was a medicolegal homicide and that the Sheriff-Coroner changed the manner to an accident, the DDA was shocked and upset, since he was prosecuting this case as some variation of a homicide. Time will tell if the Coroner’s inappropriate down-classification of manner of death in this case will have an adverse impact on seeking justice for the victim of this medicolegal homicide.
2 California Senate Bill No. 1189 was passed into law on 9/28/16 which states in SEC. 7. Section 27522 (d): “For purposes of this section, the manner of death shall be determined by the coroner or medical examiner of a county. If a forensic autopsy is conducted by a licensed physician and surgeon, the coroner or medical examiner shall consult with the licensed physician and surgeon in the determination of the manner of death.” 3 https://www.sjgov.org/sheriff/report2016.pdf

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
POSTMORTEM ALTERATION OF BODY (17-1087) WITHOUT INVOLVEMENT OF PHYSICIAN (recorded 6/5/17 at 6:34 PM):
Around approximately 10:30 A.M., the county Forensic Odontologist was present in the morgue and asked if I could remove the jaws1 of a decedent for this particular case. I was unaware of the details of the case (as it was not my case), so I requested to see the Coroner narrative and synopsis on this case. First, I noted that the decedent’s name was already in our system and per the narrative, he had been identified on scene (within the kitchen of his residence), so when I asked why the jaws were needed, the Odontologist said that he had been requested to perform a dental examination for “confirmation of identification”. I also noticed that this case was a physician-certified death and that his cause of death had already been determined by his primary care physician. Based on these circumstances, I explained to the Odontologist and the Coroner detective who happened to be present in the morgue that in order for me to make an incision into the body to remove the jaws, that it would first have to be an actual coroner’s case. Once made a Coroner’s case, only then could I proceed with requesting his medical records and performing an examination of the body in order to determine a cause of death. Since I was not willing to remove the jaws in such a case, the Odontologist said he would try to create a dental chart without removing the jaws, which I explained was of no concern of mine, as it was not a coroner’s case and as such, I was not involved. The Odontologist was subsequently able to confirm the decedent’s identity without removal of the mandible and maxilla. However, after the Odontologist was done, one of the autopsy technicians approached me and informed me that the decedent’s hands had previously been removed for identification purposes (sent to the Department of Justice (DOJ) where they were unable to render identification using fingerprint comparison). When I double checked the Coroner narrative case notes, there was no notation whatsoever that described the fact that the hands had been removed and submitted to DOJ. Had I been made aware that the Coroner Sergeant instructed one of the technicians to make permanent alterations of the body (by removing the hands), I would have recused myself from this case immediately. It is strictly inappropriate for the Coroner, or his designee, to order an autopsy technician to make any such incision into a body without first making it a coroner case and second, providing a venue for a licensed forensic pathologist to be involved in a postmortem examination first. At no point ever is it appropriate, or legal, for anyone other than a licensed forensic pathologist (or qualified technical personnel under the supervision of a licensed forensic pathologist) to make any incision, obtain any sample, or remove a part of a body for purposes relating to death investigation, as CA law stipulates that only a licensed physician may perform an autopsy2. It was expressed to me that the technician who removed the hands and the others present were uncomfortable with what the Coroner, or his designee, asked them to do, as this was not a routine practice. I subsequently sent an email to the Coroner Sergeant and Dr. Omalu explaining my recusal from this case (see email below, redacted for decedent privacy). Furthermore, the importance of requesting the forensic pathologist to perform any type of examination/procedure on a body that is not a coroner’s case has huge potential consequences for the licensed pathologist. In the practice of medicine, if a physician/nurse/other licensed medical professional forces treatment on a patient without his or her consent (except in cases where implied
1 Removal of the jaws is a forensic practice performed in order to perform dental x-rays and thus forensic dental
comparison for identification; such a practice is performed only in cases of severe decomposition that precludes the ability to identify the body by more common means, such as fingerprints, visual identification, etc.
2 California Senate Bill No. 1189

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
consent applies), that physician/medical professional may be held liable for committing the criminal offense of battery. This is precisely the reason why, as employees of San Joaquin General Hospital, Dr. Omalu and I are unable to perform hospital autopsies without consent from the next of kin. The only reason we are able to perform forensic autopsies without specific consent from next of kin is due to the legal authority bestowed on the Coroner in specific death settings (California Government Code § 27491). Once a case becomes a coroner’s case, it is now under the jurisdiction of the Coroner, wherein consent from the next of kin is no longer needed for a forensic pathologist to conduct a postmortem examination. I am not an attorney however, it seems that when the Coroner, or his designee, decides to remove parts of a body from non-coroner cases, that may violate the California government code and be classified as the unlicensed practice of medicine by a non-physician3. If I had not recused myself in this case and had I removed the jaws as requested, I would have been jeopardizing my medical license and exposing myself to potential criminal indictment. This incident, which I am aware has occurred on more than one occasion, is a primary example of what is allowed to happen when no official written Coroner policies or procedures exist.
ATTACHMENT:
3 http://www.mbc.ca.gov/About_Us/Laws/laws_guide.pdf

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INADEQUATE DEATH INVESTIGATION AND MISCLASSIFICATION AS “SUSPICIOUS” DEATH (recorded 6/14/17 at 10:59 AM):
When I reviewed the Coroner narrative for this case (17-1277) on 6/6/17, I saw that the report
authored by a Patrol Deputy stated simply that the young adult male decedent had a history of diabetes
and was found nude (in a closet) of a building. This Patrol deputy responded to the scene and
subsequently labeled this a “suspicious death” and arranged for evidence bags to be placed on the
hands of the decedent. There was no further information regarding the circumstances, such as:
• In what kind of building was the decedent found – was it his residence or that of a friend? A public
place? A business? A place he was known to hang out?
• What was the state of the interior of the building (abandoned, dilapidated, furnished, items in
disarray, etc.)?
• What, if anything, was near the decedent or also accessible in the building (drugs, drug
paraphernalia, insulin needles, his clothing, weapons, medical paperwork, etc.)?
• And most importantly, what about the death made it seem “suspicious” (i.e. potential homicide)
to the patrol deputy? Was there evidence of a struggle or obvious injuries sustained?
Unable to begin the autopsy because no substantive information was available, I requested scene
photos and more investigative information from the assigned Coroner Deputy prior to beginning an
autopsy. By the end of that day on 6/6/17, the Coroner Deputy stated that he had tried to contact the
police agency investigating the case to gain more information, but that their supervisor was unavailable
and no one could answer these very basic scene investigation questions.
Two days passed and I was still waiting for scene photos (which could answer several of my
questions described above) and information regarding why this case was thought to be suspicious.
Finally, I was informed that the scene photo disc was ready for pickup from the police agency but that
the office was closed every other Friday (including this day, 6/9). I did not want to delay the case any
further, as it had then been days since the body was discovered. I spoke with the Coroner Deputy who,
in the interim, was able to speak with someone at the investigating police agency; this Coroner Deputy
informed me that the building was an abandoned building and that the patrol deputy who responded
was relatively new and as such, called it a suspicious death more due to his lack of experience in death
investigation as opposed to concrete details or findings that would raise the possibility of a homicide.
The Coroner Deputy said that he still had no information about pertinent scene positives or negatives
(whether drug paraphernalia or clothing was found around the decedent), but was able to say that the
decedent had a history of multiple diabetic episodes, prompting hospital admission and treatment.
With that information, and not wanting to delay the autopsy any longer (for reasons described below), I
then conducted the autopsy on 6/9/17; by this point the body showed early signs of decomposition that
had developed due to the delay in access to basic investigative information. Unfortunately, part of the
decomposition process includes loss of tissue architecture and as it pertains to the eyes, loss of vitreous
fluid, which is the ideal specimen to perform ancillary tests that could indicate an individual was
suffering from diabetic ketoacidosis or a hyperosmolar hyperglycemic state. The volume of vitreous
obtained for toxicology testing was potentially compromised after a few days of postmortem change,
which could jeopardize the results of such a case, either resulting in an undetermined cause of death or
being forced to conduct additional and very expensive ancillary tests (cardiac channelopathies, etc.).

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
The scene photos were finally available and uploaded to our computer database on 6/12/17, a full
week after the decedent died. Review of the scene photographs clearly showed empty baggies (possible
drug paraphernalia), a knife, scattered clothing throughout the house, other personal items, and the fact
that the house was vacant/abandoned and in poor condition. None of these scene details were ever
included in the Coroner Narrative, which unfortunately is the only documented information available to
the Forensic Pathologist prior to performing autopsies at the San Joaquin Sheriff-Coroner. The caliber of
death investigation as it pertains to scene investigations performed by Sheriff Patrol Deputies is
sometimes appalling at best and only serves to handicap the forensic pathologist performing
examinations on these cases.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INTENTIONAL DECEPTION OF CASE LOAD/OMISSION OF HOMICIDE (recorded on 6/14/17 at 11:10 AM)
I was scheduled to perform autopsies on Saturday 6/10/17 while Dr. Omalu was away and scheduled to return on Monday 6/12/17. At 8:04 AM, the Autopsy Technician texted me to inform me that we had 1 case that day - a vehicle collision - to which I asked if the Coroner narrative had been transcribed yet so I could plan my arrival and autopsy start time. She responded that the Coroner Detective was listening to the transcription at that time and would type the synopsis, during which time I received a call from the Coroner Sergeant who was requesting that I push the case back to Monday. I responded to the Coroner Sergeant that I did not want to leave any cases for Dr. Omalu (Mondays can be heavy since no autopsies occur on Sunday), to which he explained that one of the other Coroner Detectives had a seizure and would not be able to come to work Monday, which was this particular Coroner Detective’s day off. The Coroner Sergeant explained that he wanted to “cut everyone loose” early on Saturday to accommodate the rescheduling due to a medical incident. The Coroner Sergeant said that it was just the vehicle collision case and one that “required more information”, which I took to mean that the narrative was incomplete (sometimes this happens, as occasionally the Coroner Detectives need to contact the Patrol Deputy who originally dictated the Coroner narrative because a part of their dictation was incomplete or cut off). I agreed to the Coroner Sergeant’s request, thinking that there was only 1 case ready to go that would be postponed until Monday. When I spoke with Dr. Omalu on Mon 6/12/17, he asked me what had happened on Saturday, and I explained why the vehicle case was postponed. He said that it was a vehicle accident and a homicide that had been postponed, which was news to me. The Coroner Sergeant never informed me that a known homicide was the case that required more information. Since I began working at San Joaquin County, the Coroner Sergeant has made several prior requests of me to delay performing homicide autopsies to reportedly accommodate the investigating police agency. In all of these requests, Dr. Omalu was scheduled the following day, causing me to suspect that their reason for requesting a delay in autopsy performance was to actually to ensure that Dr. Omalu would be the physician performing the autopsy. In all of these requests, I either denied the request to delay the case or made sure that I still performed the autopsy the following day, by taking Dr. Omalu’s scheduled autopsy day. Thus, with the Coroner Sergeant’s prior experience with my resistance in delaying homicide cases, I believe that he knew that I would have insisted on doing this particular case on Saturday, because homicides need to be performed as soon as possible, ideally within 24 hours after death. Instead, I later found out that it had been requested by the investigating agency to postpone the case until the weekday because a detective did not want to attend an autopsy on a Saturday. Unnecessary delays in autopsy performance jeopardizes the medical accuracy of the autopsy, which should never occur, especially when high legal stakes are present, as is in the case of homicides. Dr. Omalu then explained that the avoidable delay in the autopsy performance forced him to fix the brain (an additional expense of a few thousand dollars); please reference Dr. Omalu’s memo regarding this case.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
ABSENCE OF CORONER PROTOCOLS WHICH DELAY AUTOPSY AND POSSIBLY OBSCURE ACTUAL CAUSES OF DEATH
MISMANAGEMENT OF PERSONNEL AND RESOURCES FOR PHYSICIAN-CERTIFIED DEATHS (recorded 6/19/17 at 9:38 PM):
Today (Monday 6/19) I was scheduled to perform autopsies, so I made my usual call to the morgue before 9 am (at 8:43 AM), to ascertain what cases I had for the day. I was informed by the Autopsy Technician that a total of 11 bodies came in since Saturday, in addition to one case that was held over from last week awaiting medical records. She informed me that there was one possible homicide that the police agency wanted to attend (they require 1-hour notice so they may attend the autopsy), so I scheduled that case for 10:30 AM. She was unable to tell me anything about any of the other 10 cases, as those case narratives were not yet transcribed. As such, I told her I would re-assess the case load when I came in approximately one hour later.
I arrived at the morgue before 10 am and by that point, 5 cases had been transcribed (in addition to the one held over). After reviewing the Coroner narratives, I saw that this was a case of an elderly female for which the investigating police agency wanted to attend because of suspected elder neglect or abuse (A17-1358), which, if their suspicions were confirmed, would constitute a homicide. Over the past 8+ months I have been at San Joaquin County, there have been several cases where the possibility of “elder abuse/neglect” was raised, but the investigating agency never once wanted to attend the autopsy. I have since learned that police agencies will always want to attend homicide or suspected homicide cases, as there have been several cases of “suspicious deaths” which imply a non-natural death, such as a drug overdose. Thus, when an agency wants to attend a suspicious death case like this, it indicates that their level of suspicion for an actual homicide is higher, and thus, should be treated like a homicide. Because of this, I requested a CT scan for that case around 10 AM, which meant that the body had to be taken from the morgue to the hospital where postmortem radiography would be performed, and then brought back to the morgue, while we waited for a compact disc of the CT images could be made and then picked up by a Coroner investigator.
Because there is no official Sheriff-Coroner protocol regarding when bodies should undergo CT radiography, there is often a delay in performing the autopsy, which is precisely what happened in this case. By the end of the work day (6/9) the CT disc was still not available for my review, meaning that a potential homicide case had to be pushed to the following day, where my colleague Dr. Omalu, would have to perform the autopsy. In this particular case, however, it was noted by the Coroner deputy in the narrative that the decedent showed multiple bed sores, which is a clear nidus of infection and a potential cause of death (sepsis) in an otherwise frail elderly adult. Unfortunately, as time passes and the body decomposes, bacteria from the gut are no longer contained, and if a blood culture is attempted, it is likely to appear contaminated, which mixed bacterial populations present. In this way, because the Coroner did not recognize that a possible elder abuse case so suspicious that even the police agency wanted to attend could turn out to be a homicide, no CT was performed and the autopsy was not carried out in a timely manner. An adequately trained death investigator could have seen the potential homicide aspect of this case, and would have thus, arranged for the body to undergo CT radiography prior to arriving at the morgue.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
In addition, of the 11 new bodies that came in over the weekend, 4 were signed out as physician-certified deaths by the end of the day – the transport of non-coroner cases to the Coroner’s Office unnecessarily costs the Sheriff-Coroner money, which in turn is passed onto the family (there is a $350 fee for any body transported to the morgue that is not a victim of homicide). In physician-certified death (non-Coroner cases), the decedent’s personal physician signs the death certificate, allowing the body to be processed at a funeral home. However, at the San Joaquin County Sheriff-Coroner, it is routine for non-coroner cases (approximately 40% of all bodies that arrive at the morgue) to be brought to the morgue, thereby forcing the family to pay the Coroner hundreds of dollars for unnecessary transportation of the body. When Sheriff Patrol deputies respond to death scenes and determine that it does not fall under the Coroner’s jurisdiction, I hardly think that a family would opt to pay this fee to the Coroner for simply storing the body until they decide which funeral home will then take custody of the body.
While the Sheriff-Coroner bills each family $350 for the unnecessary transportation of all each of these four bodies that were outside of his jurisdiction to move, an additional workload was simultaneously imposed on the already understaffed Coroner investigators and Autopsy Technicians, particularly in the setting of very limited cold-storage of the bodies.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
OFFICE INEFICIENCY / MAJOR DELAY IN TRANSCRIBED NARRATIVES (recorded on 7/3/17 at 9:20 AM):
As is the usual routine, I called the morgue at 8:30 AM to inquire into the cases that we had today and was told by the Autopsy Assistant that 7 new bodies had come in, 2 of which still needed to be entered into the Coroner tracking system. Not a single Coroner narrative had been transcribed, so without any written report from the responding Patrol deputy, the autopsy technician was unable to tell me about any of the circumstances of death for all of these new cases. She explained that the Coroner’s newly hire office assistant (to replace the front office assistant who had resigned several months prior) had started work and that this brand-new employee was responsible for transcribing all Coroner narratives on the morning that we needed to know about these cases. I asked if any cases had a lock tag or a CT disc (containing postmortem CT radiographic images; the presence of such a disc might indicate a possible homicide or suspicious death), to which the technician was able to tell me that one of those cases did in fact have one, but that the circumstances were unavailable to her, as the Coroner narrative was still blank.
I called back at 9:17 AM in the hopes that at least one or two narratives had been transcribed (which has happened on prior occasions, hence waiting 30 min – 1 hour to call back), but still, of the 7 new bodies present, no Coroner narratives were typed. By this point, the senior office assistant had been recruited to assist in transcribing the Coroner narratives; I was told that apparently the new office assistant did not yet have access to the Coroner tracking system (which is not an unforeseen event with new employees, considering that it takes some time to set up the necessary computer access – I experienced this expected delay in computer access when I first started). It is professionally unreasonable to expect that a newly hired employee could jump right in to performing a critical and time-sensitive task, without the appropriate access and time and training in performing computer-based duties.
During this phone call with the technician, I learned that the body with a lock tag and the CT disc was indeed a homicide, and yet the narrative was not available, so I was unable to even set up an autopsy start time. For these homicide cases, it is necessary to give the investigating agency who plans to attend at least one hour’s notice, so despite the fact that the Coroner’s Office opens at 8 am, my hands are tied – I could not even propose an autopsy start time without the written narrative, thereby delaying the autopsy, which wastes county resources (predominantly in the form of personnel salaries, including mine and the 2 autopsy technicians waiting to get started with autopsies for the day). Furthermore, tomorrow being a county holiday means that no autopsies will be performed that day. In an effort to be as efficient as possible, it would have been best for the narratives to be typed up on time, so I could have triaged the cases and made appropriate requests (medical records, scene photos, CT scans, etc.). When access to the circumstances of a person’s death (written in the narrative) are delayed in the morning, that inevitably pushes the workload to the afternoon or the following day, depending on how quickly the Coroner Investigators are able to comply with our requests for medical records, scene photos, etc.
Although delayed Coroner narrative transcription is a common occurrence particularly on Mondays, this morning has been the worst delay since I began working here over 8 months ago. This unnecessary delay could have been avoided had the office supervisor/Coroner had the foresight to realize that the responsibility of transcribing 7 cases on a Monday morning is not suited for a new employee who is still learning (and trying to access) the Coroner tracking system.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
CONTINUATION (recorded on 7/3/17 at 9:48 PM):
It should be noted that it wasn’t until 11:57 AM that the first narrative was completed (17-1482, a solo vehicle collision). (It is also important to note that when the Office assistant has the task of transcribing narratives in the morning, there is no way for her to tell which case is which, and thus, she would have been unable to determine how to triage transcriptions, like prioritizing homicide cases, without first listening to the Patrol Deputy’s dictation.) When the homicide case narrative was finally transcribed and available around 12:15 PM, I asked the Coroner Detective to notify the investigating police agency that I was going to begin the autopsy at 1:30 PM (to give them 1 hour of notice). Since there was insufficient time to perform the motor vehicle collision in that amount of time and it was still unknown as to whether an agency wanted to attend that case, I was only able to perform that single homicide case (17-1485) today. By the time I started the homicide case, I had learned that 2 of the 7 original cases were physician sign-outs, and thus not actual Coroner cases (again, a significant detail that the transcribing Office assistant does not have access to without listening to the dictation). Thus, there were no transcriptions for 3 cases (17-1479, 17-1481, and 17-1484) when I began my autopsy today at 1:30 PM, which meant that I was not even able to start a request for the necessary items, such as medical records, etc.
Due to the mismanagement of personnel responsibilities this morning, there are now 3 bodies in the morgue that will be forced to stay an additional 2 days, as tomorrow (7/4) is a holiday. When Dr. Omalu returns to the morgue on Wednesday for his scheduled day of autopsies, not only will he have the 3 residual cases that I was unable to work on today, but he will have any number of new cases that arrive today and tomorrow for his workload on Wednesday. Aside from the possibility of having more cases than time in which to do them on Wednesday, delays such as these can interfere with scheduled funeral services as well, which is an enormous injustice to the families of this county who are already grieving for their loved one.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INTENTIONAL MISREPRESENTATION BY CORONER SERGEANT TO ALTER PHYSICIAN SCHEDULING (recorded on 7/24/17 at 7:01 PM):
On Friday 7/21/17 at approximately 10:30 AM, the Coroner Sergeant came back to the morgue where I was working in order to speak to me. He explained that one of the Coroner Deputies was out for an unspecified amount of time and that Sheriff Moore just transferred another Coroner Detective, who was currently out on medical leave, out of the Coroner's office. As such Sheriff Moore arranged for a new Sheriff deputy to replace him beginning Monday 7/24/17. In light of all of these changes, I was led on to believe that the Coroner Sergeant had limited staffing for the weekend, and as such, was requesting to postpone Saturday autopsies, saving them for Monday. Being sympathetic to limited staffing, I agreed to this UNLESS there were any homicides, multiple motor vehicle collision/trauma cases, or any suspicious cases/possible homicides for which a police agency would want to attend. The Coroner Sergeant stated that he had the ability to see what cases came into the morgue remotely (he could check online from his own home), so that the only remaining Coroner Detective wouldn’t have to come into the office just to see what cases had come in. The Coroner Sergeant stated that he would check the cases around 6:30 AM and let me know early Saturday (7/22/17) morning, so I could determine if we needed to do any autopsies.
When I had not heard from the Coroner Sergeant by 8:14 AM, I texted him to inquire as to what cases came in overnight. Since he had previously deceived me regarding a Saturday caseload which included a homicide on a previous occasion (see my separate memo dated 6/14/17), I texted several follow-up questions to ensure that none of the cases needed to be performed on Saturday. I also learned that both the autopsy technician and the Coroner Detective (who I thought was supposed to have the day off) were already at work, so I sent the following text message (redacted to remove specific names) to the Coroner Sergeant in which I inquired as to why we were holding off on doing Saturday cases if both the technician and Detective were at work:

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
I have two feelings about his response: first, it is inappropriate and deceitful to mislead the forensic pathologist into arranging my caseload in a certain way in order to conform to a misguided interpretation of an email communication Dr. Omalu had with him regarding scheduling. When Dr. Omalu originally made the July schedule, he attempted to include the County’s contracted pathologists for a few days during his scheduled 2-week vacation so that I did not have to cover the autopsy service for 2 straight weeks (not an ideal work situation for any forensic pathologist, as performing autopsies may be mentally and physically exhausting). Dr. Omalu did this not because I was incapable of doing so (I did this routinely during fellowship without even Sundays off), but because he appreciated the fact that this is my first year out of fellowship and an adjustment to being an attending physician. I am more than willing to work with the Coroner Sergeant to accommodate limited staffing when necessary, but it is frankly dishonest and misleading when staffing is not the actual issue at hand.
Secondly, Dr. Omalu has been creating the monthly physician schedule for autopsy coverage for years now (and certainly since I’ve been with the county over the past 9 months), as it is only appropriate for a physician to create physician coverage schedules. It is an inappropriate management of physician services for the Coroner Sergeant to decide when I need a day off without my input and knowledge of the daily caseload or how it many impact myself and the autopsy technicians come

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
3
Monday morning. I am a professional and I am a physician, and I can manage my own workload. A day off from performing autopsies (or postponing cases) is best deployed when I determine for myself that I need it, when a light caseload permits it, when it does not interfere with ongoing investigations or funeral arrangements, or when it will not overburden the physician and the morgue staff the following day. Furthermore, it goes against hospital and medical practice (based on California Medical Board guidelines1) for a peace officer with no medical education or training to make changes in the physician’s scheduling and certainly when it is done by intentionally misleading the physicians covering a specific medical service.
1 http://www.mbc.ca.gov/About_Us/Laws/laws_guide.pdf

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
POOR MANAGEMENT OF CORONER’S OFFICE WITH INEXPERIENCED PERSONNEL (recorded on 7/28/17 at 10:49 PM):
Today the Coroner Sergeant asked me into his office for a private conversation in which he sought my input on the newest Autopsy Technician, since I work regularly with her. Although she is still learning the skills needed in autopsy, I explained that she’s doing a terrific job and that I’m impressed by her. This conversation led to the topic of the newest Coroner investigator to the office. He was transferred by Sheriff Moore to the Coroner’s Office on Monday 7/24/17 who, per the Coroner Sergeant in a text to me, stated that this new investigator “just completed his training on the street”. The Coroner Sergeant also acknowledged that this new investigator was meant to replace the Coroner Detective who had been gone on medical leave. As it currently stands, one Coroner Deputy is assumed (my assumption) to be permanently dismissed, leaving only one experienced Coroner Detective to maintain some sense of continuity. This constitutes major understaffing of the Coroner’s Office by Sheriff Moore, given the number of cases the Coroner’s Office handles annually. In addition, the Coroner Sergeant recognized that with one new office assistant (now 2 weeks into this position) and this new Coroner investigator, that this was going to “critical time” for the Coroner’s Office.
Clearly the Coroner Sergeant has identified this transition as a delicate time, which will require extra time, attention, and training of those involved to ensure that the missions and standards of the Coroner’s Office can still be maintained in what may aptly be called “occupational/personnel chaos”.
Then, during the meeting with the Coroner Sergeant, he updated me on a child homicide case that had not yet come in, as the child was awaiting a second brain death declaration and an organ harvest, which would mean it would still be a couple of days before we received the body for autopsy. I was involved and up to date on the status of this case, as I ultimately decided what organs or tissues could or could not be procured during harvest, so as not to jeopardize the death investigation aspect. During this meeting, the Coroner Sergeant stated that he had decided to give the brand-new Coroner investigator, with minimal patrol and certainly death investigation experience, this child homicide case when it arrived, as his first case ever in the Coroner Office. Understanding the demands for thorough investigations particularly in child homicide cases, I was surprised, responding that assigning him that case was like “throwing him into the deep end” to which he replied, “yup, sink or swim.” I was stunned and shocked to hear such a sentiment.
I hardly think that investigating a child homicide should be left in the hands of the most inexperienced investigator in the office, especially for his first case ever, with only 1 week on the job. Case in point, the previous day (7/27/17) I performed an autopsy on a suspicious infant death, during which this new Coroner investigator was present, as he had been instructed to conduct a brief visual examination of the body for completion of the Coroner narrative (no Patrol deputy had been able to do this prior, because the body bag was sealed). I noticed that this Coroner investigator helped to unzip the body bag, which I attributed to him trying to be helpful, albeit unusual. Then, as soon as the body bag was opened and we saw that the infant was wrapped in a blanket, he immediately reached in to remove the blanket. The technicians, evidence technician present from the investigating police agency, and myself were simultaneously shocked and responded, “NO!”, “Stop!” or such comments. This Coroner investigator had previously informed us that he had never seen an autopsy before, so although I believe that his attempt to remove potential evidence on his own accord was done out of sheer ignorance of standard autopsy practices are and did not actually mean to possible jeopardize the case.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
However, this “rookie mistake” makes it clear to me that he has much to learn about death investigation before he ever touches or is responsible for a homicide, let alone a homicide involving a child.
To my personal knowledge and that shared with me from Dr. Omalu, we have never been consulted or requested to provide any sort of training about the autopsy procedure for new Coroner investigators, which is typically standard training at other offices. This speaks to the Sheriff’s overall mission and dedication to ensuring that the Coroner’s Office receives as much training as other department under his authority and supervision.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
MISCLASSIFICATION OF MANNER OF DEATH WITHOUT PHYSICIAN CONSULTATION (recorded on 8/1/17 at 9:34 AM):
On 11/30/16 I performed a full autopsy on an adult female who was found by her husband floating in their pool (16-2446). This case initially came in as a suspicious death due to several circumstances including: marital distress/an impending divorce due to the decedent discovering the husband’s infidelity, the decedent taking money out of their joint bank account prior to death, and threats made by the husband to the decedent that he would kill her before she got his money. Within days of making these threats, she was found deceased.
During the autopsy, I discovered hemorrhage in the deep posterior neck tissues (a standard dissection in possible diving-related deaths to rule out neck injury) and I rendered a “Pending” cause and manner of death until I received the toxicology, her medical records, and reviewed the tissue slides I had obtained at autopsy. After I had received all I needed to determine the cause of death, I requested a meeting with the detective from the investigating Police Department to inquire into any additional follow-up information regarding her death. During this meeting with the police Detective and a Coroner Detective present, I explained that her cause of death was an acute drug toxicity with “Submersion in water” as a contributory factor. I explained that when I reviewed the scene photos, I saw what seemed to be an empty prescription bottle in the husband’s name of the drug that caused her death (the decedent had no current medications prescribed to her). I also explained that she had posterior neck hemorrhage, as previously described. Despite the police Detective’s gut feeling that the husband was involved in her death, he shared that he did not have definitive evidence to link him to her murder. He also stated that she was a poor swimmer.
I described 3 possible forensic scenarios with varied manners of death to the police Detective to account for her death:
1) Suicide: She took her husband’s medication with the intent to die/hurt herself and whilst under the influence of this drug, intentionally or unintentionally went into the pool. Per the Detective, although the decedent was upset about the conflict with her husband, she had not expressed any suicidal ideations.
2) Homicide: The husband drugged her and once intoxicated, she ended up in the pool (with or without his assistance). Alternatively, she could have willfully taken her husband’s medication, but once in the pool, he could have applied force to her neck to keep her head underwater, thereby drowning her. The posterior neck hemorrhage would be compatible with that scenario.
3) Accident: She unintentionally took too many of her husband’s pills and unintentionally fell into the pool once intoxicated.
As I described these hypothetical scenarios to the Detectives, I explained that there were no additional autopsy findings that could rule in or rule out any of those scenarios. Thus, I informed the police Detective that until and unless additional investigative information became available, I considered the manner of death in this case to be Undetermined – it was not possible for me to render a Suicide, Homicide, or Accident manner of death. I explained that by making it “Undetermined”, if new information came to light that supported a specific forensic scenario, the death certificate and manner of death could easily be amended. Any suspicious death without clear circumstances surrounding the death should not be forced into a suicidal, homicidal or accidental manner of death, which could

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
possibly affect the ability to prosecute the case at a later time if it was discovered that it was indeed a homicide. I finalized my autopsy report on 3/15/17.
Several months later, I overheard a different Coroner Deputy discussing the circumstances with the Coroner Detective who had been present at the original meeting, as this Coroner Deputy was trying to render a manner of death prior to submission of his report to the Coroner Sergeant. I did not hear the entire conversation, but hearing it prompted me to check the status of this case in the computer from time to time, to see if the final cause and manner of death would change from my recommendation. On 7/28/17, I checked the Coroner computer system and I saw that the case had been finalized (I was unable to view the date of finalization, but knew it had been within a week or two since my last computer inquiry). My cause of death remained the same, but the manner of death had been changed to “Accident”. Neither the Sheriff-Coroner nor any member of the Coroner’s Office ever consulted me regarding this case or why “Undetermined” was the most appropriate manner of death.
This is now the second time (that I’m aware of) where the manner of death classification has been changed without consulting with me (see separate memo regarding case 17-0290). Although the Sheriff-Coroner is legally responsible for determining the manner of death, California law also stipulates that the Coroner must consult with the licensed physician who performed the autopsy1. Since I have never been consulted when the Sheriff-Coroner renders a different manner of death from my professional medical opinion, it is entirely possible that there are additional cases in which the manner of death has been changed without my knowledge.
1 California Senate Bill No. 1189 was passed into law on 9/28/16 which states in SEC. 7. Section 27522 (d): “For purposes of this section, the manner of death shall be determined by the coroner or medical examiner of a county. If a forensic autopsy is conducted by a licensed physician and surgeon, the coroner or medical examiner shall consult with the licensed physician and surgeon in the determination of the manner of death.”

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
GROSS NEGLIGENCE OF MANAGEMENT OF POSSIBLE FETAL HOMICDE (recorded on 8/25/17 at 9:22 PM):
At approximately 10:30 am today (8/25/17), a Coroner Detective came back to the morgue, requesting to run a case by me. He relayed the following information to me: a funeral home was currently in possession of a 32 weeks gestational age fetus, which was originally signed by a physician citing the cause of death as “Asphyxiation due to Placental abruption.” The mother of the fetus informed the funeral home employee that she had been assaulted by her boyfriend, but did not tell the physician who delivered the baby because she was afraid of her boyfriend. She reportedly did not inform the police regarding this most recent abuse, but disclosed that approximately 1 month prior, police were involved in a domestic violence dispute, the details of which were unknown to the Coroner Detective at this time.
I asked the Coroner Detective when the baby died versus when the alleged last assault occurred. He did not know when the assault occurred, but informed me that the baby was born/died on 7/9/17. Astounded that this baby died so long ago (approximately 7 weeks prior), I asked when the funeral home reported it to him, to which the Coroner Detective admitted that the funeral home told him right away after the death. I asked why he didn’t bring this to my or Dr. Omalu’s attention sooner and he responded that he has “been busy”. He asked me what I wanted to do: did I need medical records to do a Medical Records Review? Did I need the body in order to do an autopsy? I told him that since it had been 7 weeks since the baby died and that this was the first I was hearing about it, I needed more information – I asked him to call the funeral home to find out more details about when the alleged assault was in relation to the baby’s death and how the baby had been stored over the past several weeks (room temperature, cooler, or freezer).
After lunch at approximately 2 PM, the Coroner Detective had more information to share, as he had been in contact with the funeral home as requested. He said the following: the alleged assault involved the boyfriend hitting the mother and pushing her out of the front door, causing her to fall on her gravid abdomen, which resulted in her going to the hospital and delivering the stillborn baby. She had a prenatal checkup in June after which she was also assaulted by the boyfriend, which is when police first became involved. The body had been stored in a cooler and still reportedly looked to be intact, according to the funeral home employee.
I asked that the Coroner Detective request the hospital record where she delivered the stillborn infant and her last prenatal checkup to gain more information as to the health of the fetus before delivery and what exactly occurred during her delivery. He noted that he would work on that and get the records I requested as soon as possible. I also sent him an email that afternoon requesting that he send me the narrative/synopsis on this case indicating the timeline of events, as this case did not have an assigned coroner case number yet, and thus, no written information in the Coroner database regarding the circumstances was available for review.
CONTINUATION (recorded on 8/30/17 at 7:49 PM):
On 8/29/17, the Coroner Detective contacted me via email to send me a brief narrative of events regarding this case, however, he did not specify when the Coroner office was informed. He also informed me that he received a CD containing the medical records from St. Joseph’s Medical Center as I

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
had requested, so I reviewed them this morning (8/30/17) when I got into work. Contained on the compact disc were medical records from two prior visits (one in March of 2017, and the other from June 2017 for which the mother was seen after a reported assault by her boyfriend) in addition to the record of her stillbirth. She presented on 7/9/17 with sudden, severe abdominal pain and was found to have placental abruption and fetal demise on abdominal ultrasound, so she underwent a cesarean section for delivery. She indicated that she had not been assaulted since June, but the social worker who met with her indicated that s/he had concerns that this placental abruption might be related to the previous assault, and as such, needed to confirm with his/her supervisor whether or not this was a Coroner’s case. It was not noted in the medical records whether or not the Coroner was ever notified.
Because I did not see a clear medical rationale to explain the abruption that ruled out assault as a precipitating factor (urine toxicology was notably positive for THC and negative for amphetamines), I sent an email to the Coroner Sergeant (and CC’ed Dr. Omalu) at 12:34 PM on 8/30/17 describing that I had been informed of this case, that the Coroner Detective advised that he had been informed of this case soon after the fetus’ death several weeks ago, and that due to the prolonged time period between death and my initial consultation, I would have to recuse myself from this case, as I found the preventable delay in consulting me in a possible fetal homicide to be “highly distressing” and appearing to be “grossly negligent”.
The Coroner Sergeant responded at 2:09 PM, CCing Dr. Omalu, the Coroner Detective, Investigations Lieutenant, and Investigations Captain, to say that “this case was not presented to the Coroner’s Office 7 weeks ago” and that death was “never reported to the Coroner’s Office by the hospital and went directly to a funeral home”. He said that they learned about the death and the circumstances surrounding the fetus approximately a week and a half to two weeks prior to 8/28/17. He said that during that period of time the Coroner Detective was in contact with the investigating police agency and when they learned that there was a history of domestic violence, that is when the Coroner Detective approached me. The Coroner Sergeant said that he “felt that it warranted an investigation based off what was relayed to us by the mother and funeral home and wanted to confirm the cause with one of our pathologists and get a second opinion.” Although Dr. Omalu was first on the schedule on Friday 8/28 (Dr. Omalu had not yet arrived to the morgue when the Coroner Detective first approached me), the Coroner Sergeant stated that he requested that the Coroner Detective consult with me. He then ended the email asking what I wanted to do with this case – should the body be brought in or would a medical records review be sufficient?
At this point, I met with Dr. Omalu in the morgue to discuss this case, and we were in agreement in terms of the most appropriate course of action. I responded to all recipients via email to say that I was still uncomfortable with the timeline as initially provided to me verbally and the lack of reporting by the hospital. As such, I maintained my stance of recusal from this case.
Around 4:00 to 4:30 PM, while sitting at my desk, I overheard the Coroner Detective make a phone call to the investigating police agency, requesting information about the timeline of events on this case, as he had not taken any notes regarding his previous contact with this person. Although I only heard his end of the conversation, I gathered that some contact had occurred sometime during the “week of the 14th” (the month was not indicated). Later on, just before 5:00 PM, I heard the Coroner Sergeant approach the Coroner Detective to say that he had done an excellent narrative so far, and to submit the final version to him by tomorrow in preparation of the “memorandum format”.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
3
It should be noted that perhaps until late today, no Coroner case number has been generated by the office, confirmed by the Coroner Detective when I asked him for the case number this morning. Even if the Coroner Detective was mistaken or misspoke when he informed me that the Coroner’s Office was notified of this death just a couple of days after 7/9/17, I am puzzled as to why the Coroner Sergeant waited 2 weeks before requesting consultation with either myself or Dr. Omalu. As soon as there was an allegation of domestic violence, a Coroner case should have been generated and a pathologist involved, so we could have provided our expertise and recommendations as soon as possible. As I explained in my initial recusal email to the Coroner Sergeant this morning, a 7-week postmortem interval in an infant will undoubtedly result in ongoing autolysis and decomposition, which irreparably diminishes the integrity of the tissues/fluid and the interpretation of postmortem examination findings. The time to either rule in or rule out an assault-related fetal death has passed. Although the specific details, dates and times of what the Coroner’s Office knew when has yet to be solidified, I am deeply troubled that somewhere along the line, gross negligence occurred in the management of this case, allowing a potential fetal homicide to fall through the cracks. It is disturbing to me that the Coroner Sergeant fails to understand the very basic concept of postmortem interval, especially in an infant, and the profound impact that can have on determining the cause of death. Although I believe that the Sheriff-Coroner was made aware of this case, I have not since been contacted about this case, so I am unable to comment on the final resolution of such a case, except to say that to my knowledge, the body was never brought to the Coroner’s Office.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
RESTRICTIVE 9 AM BRIEFINGS / MOST CASES NOT TYPED BY 9:15 AM (recorded on 9/5/17 at 8:53 AM, updated at 9:44 PM same day):
The first issue regarding today’s briefing stems from their inherently restrictive quality that impedes the forensic pathologists’ ability to control his or her caseload and remain independent. A couple weeks ago, after a meeting with the Sheriff and the Sheriff’s chain of command for the Coroner’s Office (see separate memo), Dr. Omalu and I have been compelled to participate in 9 am briefings in which the Coroner Sergeant, occasionally the Investigations Lieutenant, the Coroner Investigators (Deputies and Detectives) and Autopsy Technicians meet in the conference room and call the Forensic Pathologist scheduled for the day to inform us of the cases. To avoid actual or perceived bias of law enforcement in this setting, Dr. Omalu and I discuss as little as possible about each case, which is a constraint in and of itself, but necessary in an attempt to maintain our independence in an undesirable situation in which we are forced to be.
Aside from the issue of potential bias involving the forensic pathologist and sworn officers, the 9 am briefing is unnecessarily restrictive in how we manage our cases for the day. Case in point: today (Tuesday 9/5) is the first day back after a Monday holiday, so I anticipated that today would be heavier than a typical Monday case-wise. I texted the Coroner Sergeant around 7:30 AM to remind him that I was scheduled to cover autopsies today and he responded back via text that close to 20 bodies came in over the weekend. Thus, with the long holiday weekend in mind, if we were allowed to practice our normal routine of contacting the morgue technicians at our discretion in order to inquire into the caseload for the day, I would have called the autopsy technicians earlier than normal, around 8:30 AM or so (they begin their shift at 8:00 AM). Instead, the Coroner Sergeant subsequently texted me to say that they would be calling around 9:15 AM today and that there were 16 cases to review. Due to the high number of cases, the phone call briefing alone took approximately 10 – 15 minutes. With 3 homicide cases and 1 infant case in which an agency wanted to attend, the earliest time I could schedule an autopsy at that point was 10:30 AM (to provide 1-hours’ notice to the agency who wants to attend the autopsy), thus effectively shortening the available work hours of the technicians, who are scheduled until 5:00 PM. Although I frequently stay later than the technicians to finish my work (usually dictations or reports) for the day, I cannot perform autopsies without the assistance of technicians.
In the original long-term practice, Dr. Omalu and I were better able to effectively manage our caseload depending on the number and types of cases that came in. The restrictive constraint of forcing us to participate in a police briefing as our only way to inquire about cases, only serves to limit our abilities to be efficient with our own and the technicians’ work hours, resulting in a waste of county resources (largely personnel wages), and thereby delaying when cases are complete and when families can move forward with funeral arrangements.
The second issue stemming from today’s briefing originates from the fact that only 6 of the 16 cases were typed up and had case information available (2 homicides, 1 potential homicide, 1 infant, 1 suicide and 1 potential overdose). The circumstances of death or medical histories of the remaining cases were not known at the time of the briefing, so I was unable to place my requests for items necessary to make a decision on the type of exam I needed. After completing autopsies for the day and prior to the autopsy technicians leaving work, I requested that they print out the remaining previously unavailable Coroner narratives from the morning (cases 17-1899, 17-1901, 17-1902, 17-1905, 17-1908, 17-1909, 17-1911, 17-1912, 17-1923), so I could review the narratives after they left and make a list of what was

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
needed on each case. These cases mostly involved decedents with medical conditions who died anywhere between Sat 9/2 through Mon 9/4, and most cases required medical records to make a decision on the type of exam I needed to do. In several of these cases, the narrative was not typed for 3 days since their death, which is an unacceptable delay in making that case information available. Since I was reviewing these narratives after 5 pm today, I had to leave my requests at the autopsy technicians’ desk for their return to work the following morning at 8:00 am.
The inaccessibility of case information about a decedent due to the current administrative and functional design of the Coroner’s Office by Sheriff Moore during an expectedly heavy weekend ultimately delayed my request for medical records, which ultimately delays my receipt and review of such records. For many of these cases, it may be a week since their death until I’m able to finally perform an examination, which also jeopardizes the interpretation and ability to obtain certain toxicology specimens while the bodies undergo autolysis and decomposition. For a few cases, I requested admission blood, so it is my hope that after 4 days (or possibly more depending on when the Coroner Investigator makes the request amongst the number of cases requiring medical records), that the respective hospitals have not yet discarded those specimens.
It is profoundly limiting to be tethered to a briefing phone call at a time determined by the Coroner with up to 6 Sheriff-Coroner Investigators (especially when my preference would be to call earlier when it is reasonable to do so). In addition, this briefing limits my ability to schedule my case load for the day when most case narratives are unknown to all officers and staff present. Being compelled to participate in these briefings wastes not only the forensic pathologists’ and autopsy technicians’ time and ability to be efficient, but it also provides for limitless opportunities to be exposed to real or perceived pressure or bias from said officers, ultimately threatening the physicians’ ability to practice medicine with complete independence from law enforcement.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
SIGNIFICANT DELAY IN REPORT TRANSCRIPTION DELAYING FINALIZATION OF REPORTS (recorded on 10/1/17 at 9:13 AM)
Over the past few months, I have noted a complete stall when it comes to transcribing reports. In early August, the delay was more obvious and by the end of the month, cases from as far back as early March had still not been transcribed, including suspicious deaths or homicide cases. Although I worked on the transcribed cases that were available to me, I frequently had to contact the Office Staff to request that a specific case be transcribing as soon as possible because the family had been repeatedly calling about the cause of death. On 8/31/17 I took a screenshot of my dictation list (see attachment with redacted Office assistant names on the next page), which also shows when I dictated a specific case and when (and if) it had been transcribed. It is clear to see in the dictation computer system that most cases are not transcribed for at least 3 – 5 months after dictating the case. This delay in transcription of autopsy reports ultimately creates a downstream effect on finalizing these and future cases, resulting in massive delays of at least 5 – 6 months or more before the autopsy report is available to the family, attorneys, investigating agencies, etc.
I should be clear in stating that this is through no fault of the Office assistants themselves – due to staffing issues earlier this year and the delay in bringing in adequate staffing (a responsibility of the Sheriff-Coroner), the responsibility of transcribing both Dr. Omalu’s and my reports fell squarely on the shoulders of a single individual (in addition to all of her numerous other daily tasks) – this being a responsibility that should have been shared by at least two people. The Coroner’s Office has since hired an additional Office assistant to transcribe my reports – and she has been doing an excellent job – but still, the amount of work that she must catch up on is unbelievable. Still, the Sheriff-Coroner’s Office expects these two Office assistants to handle all transcribed autopsy reports in addition to their numerous other daily duties. This is an unreasonable professional expectation, even of the hardest working and most efficient staff member (which they both are).

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
UNWILLINGNESS/REFUSAL OF SHERIFF TO FURNISH INVESTIGATIVE REPORTS IN HOMICIDES (recorded on 10/5/17 at 1:16 PM):
In the practice of forensic pathology when it comes to cases of homicide, it is standard practice to have access to the related investigating police agency report, which details how the body was found, what the investigation reveals at that moment in terms of how and when the victim was injured, the weapon used, what evidence was found at the crime scene, etc. It is also standard practice in death investigation that this information, when known, be included in the Coroner narrative report. Written documentation of the scene investigation is crucial for the forensic pathologist performing the autopsy to have, as it is related to the interpretation of wound patterns, allowing the forensic pathologist to determine whether or not the known forensic scenario is consistent with what is seen at autopsy. This information also guides specific testing that needs to be requested, what evidence is collected at the time of autopsy, and ultimately, what the cause of death is.
However, at the San Joaquin County Sheriff-Coroner Office, the Coroner Narrative is often so cursory, incomplete, and/or vague (see additional memos regarding this topic), that they are essentially useless to the forensic pathologist. Thus, it is mandatory to receive and review all police investigatory reports prior to finalizing my autopsy reports in cases of homicides or suspicious deaths (this is also standard practice at other Medical Examiners across the country and Coroner Offices within California). Although in several cases it takes weeks or months to receive the completed reports, I have almost always received the local police agency reports, thereby allowing me to finalize my report.
However, since I joined the County just over 1 year ago now, I have had approximately 7-10 homicide or suspicious death cases that were investigated by the Sheriff’s Office (SO), and I have never once received an SO investigative report despite my requests. I was initially advised by my colleague, Dr. Omalu, that I could set up a meeting with the Homicide investigator in order to answer any pending questions, which I did on 1 or 2 prior occasions.
This past weekend (October 1st), two bodies (cases 17-2130 and 17-2134) were discovered within a dense cornfield showing evidence of firearms injury. The Investigations Lieutenant called me on the evening of 10/2/17 and verbally described the rather complex and detailed circumstances as to how the bodies were discovered (they were well hidden amongst the corn), when and how they were recovered, etc. By the time I came into the autopsy suite the following morning to perform these autopsies, based on the Investigations Lieutenant’s verbal information, I had a good understanding of what the investigation had revealed up until that point. However, when I read the Coroner Narrative, it essentially reads as follows, "a body was found in a cornfield with defects consistent with gunshot/shotgun wounds." No additional or forensically significant information regarding the scene or circumstances was reported, including the timeline of events, what other evidence was recovered (shotgun wadding), that CHP used their helicopter with heat mapping to find the bodies because they were so well concealed, that witnesses heard gunshots Saturday morning (9/30/17) in the area, how the SO came to learn where they needed to search in order to find the bodies, the fact that the bodies were not recovered until Monday (10/12/17), etc. All of this information was conveyed verbally to me, but no written report was available to me that included it, so I requested a copy of the SO Investigation report when it became available.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
The Coroner Sergeant and the Coroner Detective responded via email on 10/4/17 and 10/5/17 stating that they could set up a meeting with the SO Investigator to answer my questions. However, an in-person meeting in lieu of a documented report is unacceptable to me. If the SO does not furnish an investigative report, there is literally nothing in writing for me to review that describes the circumstances now known and previously verbally relayed to me. I do not understand why the SO is the only agency in the entire County who will not provide even preliminary investigative reports for homicides to a sister intradepartmental bureau, i.e. the Coroner’s Office.
My concern with the SO being unwilling to provide investigative reports opens the door to being misled (intentionally or not) by the Investigative agency, as it is possible to verbally convey information important in making determinations about autopsy practice and pathologic investigation, which may be untrue or incomplete and is later documented differently. At that point, the Forensic Pathologist would have no recourse in defending his or her actions taken during autopsy. This is precisely what occurred in this case:
The Investigations Lieutenant admitted that the reason for his phone call on Mon 10/2/17 (which is a highly unusual event, as he has never once contacted me regarding any case I’ve had before), was to request that I perform an autopsy on the younger decedent first. He said that their evidence technicians did not take fingerprints at the scene because they wanted to preserve possible DNA under his nails (please note: it is routine to collect fingernail clippings for homicides, however, ever since I have been with the County, bodies have always been fingerprinted on scene first and then transported to the morgue where we would then collect fingernails at the time of autopsy). He stated that the younger male (believed to be a minor) is currently un-identified and as such, Sheriff detectives are unable to make notification to the family. One particular family had been in contact with the SO, concerned that their son was one of the victims and the Investigations Lieutenant made an emotional appeal to me to give them closure sooner. I eventually agreed to proceed with that case first, for the family’s sake.
Before beginning the autopsy on Tues 10/3/17, I noticed that the younger decedent was identified by name in our computer database (instead of the traditional “John Doe #X” used for un-identified bodies) and the older decedent was actually still listed as a “John Doe”. I heard the senior evidence technician who was present (and standing right near me) telling the junior/trainee evidence technicians that they still had to get GSR evidence and fingerprints on the younger decedent because “someone sealed the body bag on scene too soon”, thus preventing them from doing it. She continued to say that they had already collected GSR evidence and fingerprints on the older decedent (“John Doe”). Thus, it became clear to me that someone on scene made an innocent mistake and sealed the body bag of the younger decedent prematurely. Instead of being forthcoming with that information, the Investigations Lieutenant made an emotional appeal to me to influence my decision to perform that autopsy first. In this way, the SO could correct their procedural oversight as soon as possible, even though he appeared to be identified in our computer AND the Lieutenant’s rationale for preserving evidence for autopsy does not hold water considering they had already obtained GSR and fingerprints on the victim who was actually still a John Doe. As this example shows, I can be told anything about a case verbally, whether it’s true or not, but unless I see it in writing, no one is accountable to the veracity or their words.
Finally, no other police agency in the entire county of San Joaquin refuses to furnish physical police reports in cases of homicide. I am completely baffled that the SO would be unable to provide investigatory reports to the Forensic Pathologist who performs the autopsy and ultimately determines

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
3
the cause of death. This goes against every standard procedure and practice in forensic pathology and the fact that it is perpetrated by the Sheriff’s Office is particularly astonishing and unacceptable.
UPDATE 12/3/17 at 2:43 P.M.:
Almost two months after the original authoring of this memo, I have yet to receive any requested report for any homicide or suspicious death investigated by the San Joaquin County Sheriff’s Office.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
With input from Bennet I. Omalu MD, MBA, MPH, CPE, DABP (AP,CP,FP,NP)
1
SCHEDULING AND CONTROL OF PHYSICIANS BY SHERIFF-CORONER IS A DISASTER (Week of October 8th, 2017)
October 8, 2017, 6:50 A.M.
The Sheriff has been hell-bent on taking over the scheduling of physicians and determining when and how physicians will work or not work for no other reason but to have control of the physicians. Beginning October 1, 2017, the Coroner Sergeant released a schedule for the physicians without involving or considering other duties physicians are involved with. The result was a total disaster.
Between Sunday October 1, 2017 and Wednesday October 4, 2017, there were approximately 13 new bodies in the office, including one child, three homicides, and one in-custody death. The Sergeant had scheduled Dr. Parson to perform autopsies Monday through Wednesday without consulting her on other professional engagements she had, such as attending a professional interview and attending a professional medical evaluation. Dr. Parson had to attend to her other professional duties and could perform only a limited number of autopsies. Between Monday and Wednesday, she could only perform 7 autopsies, prioritizing the three homicides, the child, and two older cases for which she finally received medical records (funeral homes were calling about these very cases, often because funeral services were scheduled and they needed the bodies). By Thursday, October 5, 2017, Dr. Omalu had over nine bodies waiting for him and some of the bodies had been at the morgue since Sunday 10/1/17. This is simply not acceptable and goes against every standard of practice of medicine. Physicians should be the ones handling their scheduling while evaluating the cases available since autopsies should be performed within 24 hours of a body arriving at the morgue.
The same trend happened with Dr. Omalu, who had family engagements at his children’s school on Friday, October 6, 2017, and had scheduled Dr. Parson to perform autopsies on Friday. The Coroner Sergeant changed the schedule and as a result Dr. Omalu could not perform autopsies until late afternoon when he got back from the school. Cases were delayed. On 10/7/17, upon arriving at work, Dr. Omalu performed an autopsy on a body, which had been in the morgue since 10/1/17; the case of a 48-year-old woman [A17-2116] who had died suddenly and unexpectedly. The autopsy was performed six days later. This means that at autopsy, Dr. Omalu could not collect adequate blood samples to perform laboratory analyses to find out if this woman may have suffered an anaphylactic reaction to any type of drug or allergen, in addition to other tests that Dr. Omalu may have wanted to perform because of the prolonged post-mortem interval. This is grossly below every standard of practice of medicine.
This trend is bound to occur again this coming week, as Dr. Parson is scheduled to perform autopsies on Monday, Tuesday Wednesday. However, the Coroner Sergeant failed to consult with Dr. Parson, as she has a meeting with separate Deputy District Attorneys (DDAs) on Monday and Wednesday and is scheduled to appear in court on Tuesday, possibly on Wednesday, and also on Thursday, which will undoubtedly impact the autopsy service. When Dr. Omalu originally created the October schedule, he took these dates into account in order to ensure full coverage of the autopsy service.
Update on October 11, 2017, 7:44 P.M.
On Monday 10/9/17, anticipating a heavy Monday workload, Dr. Parson was in her car on the way to work when she received the “9 am briefing” call (which actually occurred at 9:20 am). She was told

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
With input from Bennet I. Omalu MD, MBA, MPH, CPE, DABP (AP,CP,FP,NP)
2
there was a John Doe pedestrian struck by a car (in addition to 3 pending cases awaiting medical records from the previous week), but would not be able to give an autopsy start time because she was awaiting confirmation from the DDA regarding their meeting time. When she arrived at work minutes later, additional details she read about the incident in the narrative prompted her to call the Coroner Detective on the case and request a CT scan on the decedent. Minutes later, the Coroner Sergeant called Dr. Parson to inform her that the Coroner Sergeant set up an autopsy time without consulting Dr. Parson, as he had already informed the investigating police agency that the autopsy was scheduled for 11:00 AM. She explained that she had ordered a CT scan on the body and that the body and scanned radiographic images would not be available by 11 am, so that time would not work. She was later informed by the Coroner Detective that the investigating police agency was now refusing to attend the autopsy that day because that police Detective had already driven 45 minutes from out-of-county to make the 11 am start time determined solely by the Coroner Sergeant. Dr. Parson explained the importance of doing that case on Monday, because with court and DDA meetings scheduled Tuesday and Wednesday, she did not want to hold over any cases. Eventually the investigating police agency arrived in the afternoon for the case, but not without experiencing an unnecessary amount of wasted drive time, due solely to the Coroner Sergeant’s attempt to schedule cases without the Forensic Pathologist’s knowledge or input.
On Tuesday 10/10/17, Dr. Parson was informed during the morning briefing that there were 4 new cases (in addition to the 3 pending) on a day that she was scheduled to appear in court at 1:30 pm. During the 9 am briefing, the technician explained that there was an additional body at a funeral home with a report of possible elder abuse and that Adult Protective Services were involved. When she requested that the body be brought in, the Coroner Sergeant requested that she review the medical records first, as the decedent’s primary care physician was willing to sign, so the body had not been assigned a Coroner case number. This was an alarming response, as any designated Coroner or designee should know that any cases of possible or suspected elder abuse automatically fall under Coroner jurisdiction, and should be investigated. Dr. Parson requested a Coroner narrative on the case, which was not provided until the following morning and the body was not brought in until the following afternoon (Wednesday 10/11/17). It wasn’t until the opinion of the DA confirmed that this should be a Coroner case, that this finally was made a Coroner’s case late on Wednesday (17-2180).
Nevertheless, Dr. Parson was able to complete 2 of the Tuesday cases prior to lunch and her scheduled court appearance. She was informed during lunch that court was postponed, so she continued with performing autopsies, however, had to wait until the Coroner narrative for a motor vehicle collision was actually typed (this case had been presented that morning during the 9 am briefing, but not typed until after 12 pm).
On Wednesday 10/11/17, there were 3 new cases and 4 pending (the possible elder abuse case had not yet arrived). With a meeting scheduled with the DDA in the afternoon, Dr. Parson was only able to complete 3 cases, leaving 4 for the next day, in addition to the possible elder abuse case; Dr. Omalu was scheduled to cover autopsies the following day. The Coroner Sergeant’s attempt at scheduling physicians without taking into consideration previously scheduled meetings or court time, has been a disaster these past two weeks and has created unnecessary stress, confusion, and most importantly, a delay in the performance of autopsies. This underscores our point that only physicians, who are

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
With input from Bennet I. Omalu MD, MBA, MPH, CPE, DABP (AP,CP,FP,NP)
3
intimately acquainted with the specific daily duties of physicians in the same medical specialty, should create the working schedule for physicians. When left to the authority of police officers, who have no specialized knowledge or true understanding of what forensic pathologists do, easily avoidable conflicts are created, which may delay death investigations or create unnecessary distractions in the work place.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
RELEASE OF DRUG EVIDENCE TO FAMILY IN HOMICIDE (recorded on 10/18/17 at 7:16 PM)
This afternoon I came to learn through the autopsy technicians that one of the Coroner Detectives released presumed marijuana back to family members who came to collect decedent property for the reason that “Weed is legal now”. When I inquired into which case this was, I learned that it was a homicide case (17-2127) on which I performed an autopsy on the morning of 10/4/17. Since I did not recall there being any presumed marijuana on the decedent, I went back to my autopsy notes and the Coroner Narrative I was provided prior to autopsy and confirmed that not only was there no mention of presumed marijuana being discovered in the narrative, but the page indicating the decedent’s property was blank (which is often the case when the Coroner does not actually collect any property). The presumed marijuana was collected by the Coroner Detective (listed as a “blue jar of green leafy substance”) along with other items including cash, a wallet with identification and debit cards, and rolling papers that, according to the Coroner database, was store in safekeeping on 10/2/17 at 7:00 AM. I was never informed that any additional personal items/property were collected from this decedent prior to autopsy. This practice is highly atypical, especially in the setting of a known homicide, when all property should be kept with the decedent so that it may be examined and documented at autopsy prior to being transferred over to the investigating police agency. Also, at this current time, it is still unclear to me whether the investigating agency (San Joaquin County Sheriff) is aware that personal items were collected by the Coroner Detective.
Aside from the fact that evidence should not be removed from the body in homicide cases before autopsy, I was dumbfounded to learn that evidence, especially a drug, was returned to this decedent’s family. Routinely, Coroner investigators remove legal prescriptions from decedent’s residences in all manners of death, so that they may be marked for destruction by the Coroner’s Office. It is particularly worrisome that this Coroner Detective concluded that because recreational marijuana was legalized in CA recently, that what he assumed to be marijuana could be returned to the surviving family of a victim of homicide. No chemical analysis was performed to confirm that this “green leafy substance” was in fact marijuana and only marijuana, as it is entirely possible for marijuana to be laced with other illicit drugs or dangerous chemicals. As such, it is routine for the Forensic Pathologist to collect such materials at the time of autopsy and submit it for drug identification when it is not deemed to be evidence that needs to be collected related to a criminal death (i.e. homicide).
This action of 1) removing evidence from the body of a homicide victim before autopsy, 2) not alerting the forensic pathologist that it was done through the written narrative or property sheet printed 2 days later at the time of autopsy, and 3) releasing it to the family instead of the investigating agency or a toxicology lab goes against all standards of practice of death investigation. This action not only potentially jeopardizes this case but it also poses a health risk to whomever decides to use this substance, when it is not confirmed to be absent of additional chemicals or illicit drugs.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INADEQUATE INVESTIGATION IN DROWNING DEATH (recorded on 11/2/17 at 6:49 PM)
I performed an autopsy on a young woman who apparently drowned (17-0523) on 2/25/17. Since drowning is a diagnosis made only after excluding other potential causes of death (traumatic, medical, toxicologic), I rendered the cause and manner of death at that time as “Pending”. Because the Coroner narrative I was supplied (authored by a Sheriff Patrol Deputy) contained little to no information regarding the circumstances (essentially, only that the local police agency was investigating this as a drowning), I made several to include scene photographs, the investigating Police report, medical records, etc.
I was able to complete most of my final report after integrating the toxicology results, her medical history, histology findings, etc. but I had not yet received the photos of the scene, which were critical to my understanding of how she came to be in the water in the first place. I did receive the Police report, which gave the account of two witnesses as it pertained to this death. However, several items of information that are essential to drowning deaths and are standard in these types of death investigations, were glaringly absent from the Coroner’s Narrative and the Police report, such as the following:
• Where did the decedent go into the water? Where was she recovered in relation to her entry point?
• Was the water moving, and if so, how fast, and in which direction? • What was the depth of the water where she went in, along her path (if any linear movement took
place), and where she was extricated? • What was the ambient temperature? • What was the temperature of the water? • What was the decedent’s swimming ability?
These are basic and essential elements that need to be covered in order to understand how/why someone went into the water and why they stayed in the water (or were unable to get to safety). Also, in this particular scenario, there was a bridge over the body of water with a guardrail along the side. Another pertinent piece of information would be to know how high up was the top of the guardrail from the ground – is that a height over which she could have easily have fallen or be pushed, or was it tall enough where climbing would be necessary? It should be noted that the Police report indicated that she was extricated from 2 feet of muddy silt – however, no mention of the actual water depth was ever given. To be quite frank, there was more information about the circumstances of this woman’s death in the city police report than in the Coroner’s Narrative (this is a common theme in which the Coroner’s reports are almost entirely useless, as they contain little or no information of importance to death investigation; additional memos cover this topic). And although it is useful to include the above listed information in the Police report, it is the Coroner’s responsibility to investigate the circumstances of the death, so the Coroner holds full accountability for making sure the basic death investigation questions are answered in their reports.
However, none of those questions were ever asked and months down the line when seasons have changed, these questions cannot be asked with reliable answers (water depth, temperature, etc.). It should be noted that when the decedent was taken to the hospital, she was found to be hypothermic. However, although the Police report indicated that she was in the water for approximately 30 minutes,

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
without knowing what the water temperature was at that time, I am unable to determine if hypothermia also played a role in her death.
After multiple requests and reminders to several Coroner Deputies and the Coroner Sergeant over the past several months, I finally received the “scene” photographs on approximately 10/25/17 – a full 8 MONTHS after the incident. When I viewed the photos, I was stunned and disappointed to see pictures only of the decedent laying deceased in a hospital bed – no scene photographs were ever taken. I finally resorted to using Google Maps to get an idea of what the area looked like, although there is no way for me to know exactly where the decedent went into the water or where she was recovered.
The level of incompetence in this death investigation is embarrassing for the Sheriff-Coroner. All I expect of the San Joaquin Coroner’s Office is meeting the bare minimum standard of death investigation, and it repeatedly fails in this regard. Incompetent death investigation, where even the most basic scene investigative questions are not covered, is dangerous and detrimental to San Joaquin as a community. The level of competence displayed by the San Joaquin Coroner’s Office is unacceptable by any standard of practice in death investigation and further reinforces why appropriate education/training and standard written protocols/policies in death investigation need to exist for the Coroner’s Office.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INABILITY TO RECOGNIZE APPROPRIATE CORONER’S CASES (recorded on 11/9/17 at 6:44 PM):
This morning (11/9/17), the Coroner Sergeant called back to the morgue where I was working to request that I review a case in which a patrol deputy had responded to the death the previous evening. In the narrative provided by the responding patrol deputy, an elderly male with multiple co-morbidities had undergone orthopedic surgery the day before his death due to a fall the decedent sustained several days prior. Despite the fact that the decedent died within 24 hours of a surgical procedure for a traumatic injury, this patrol deputy accepted this case as a physician-certified death in which the attending physician cited “Aspiration Pneumonia” as the cause of death and contributory factors as some of the decedent’s medical co-morbidities.
When I asked how he found out about this case, the Coroner Sergeant explained that the Assistant Sheriff (previously the Coroner Sergeant several years ago), was reviewing the patrol narratives for death cases and requested that one of the doctors (Dr. Omalu or myself, although I happened to be scheduled today) take a look.
As a Forensic Pathologist in the Sheriff-Coroner system, I have no specific authority to determine which cases qualify as Coroner’s cases, although I am sometimes consulted for my medicolegal opinion. Thus, in this case, I reviewed the medical records they provided and advised that this indeed should have been a Coroner’s case, as the temporal relation of the surgery for a sustained injury could not be ignored. The fact that the responding patrol deputy – serving as a Deputy Coroner on holidays or after normal business hours - clearly demonstrates the inadequate knowledge base in death investigation and the ability to determine which cases require further investigation by the Coroner’s Office. Had the Assistant Sheriff not caught this case, this man’s death would have been attributed to a natural event, whilst completely ignoring the accidental injury he sustained.
It is worrisome to me that Sheriff Moore has structured the work-flow of death reporting to be routed through patrol deputies, thus making peace officers with no formal knowledge or experience in death investigation, be the conduit through which cases are brought to the attention of the Coroner’s Office or allowed to remain uninvestigated as physician-certified deaths. This example demonstrates why non-medically trained police officers are ill suited to not only investigate medical aspects of death, but assume the responsibilities of the Coroner for the County of San Joaquin.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INADEQUATE CHILD DEATH INVESTIGATION – DROWNING (recorded on 11/27/17 at 8:49 PM):
On Saturday 11/25/17, of the 10 new bodies that had arrived at the morgue after the Thanksgiving holiday, one of those cases involved the death of a child (17-2509). Although I routinely request Pre-Hospital Care reports (“PCRs”; essentially, the terminal Emergency Medical Services report documenting the encounter after 911 was called) on all autopsy cases, I was told it was unavailable/had not yet been received on this case. As such, I had to rely solely on the Coroner’s Narrative which stated only that this case was being investigated as an “accidental drowning” by the local police agency. There was no single additional detail regarding the circumstances of this death in the Coroner’s narrative. There was no mention or description of the scene, the body of water the child allegedly drowned in (whether it was a pool, bathtub, lake, hot tub, etc.), the depth of water, the temperature of water, etc. or any additional information regarding the scene (who else was present? when the child was last seen? when was the child was found? who found the child? etc.). The only words of any substantive meaning in the Coroner Narrative was simply that it was an “accidental drowning”.
I always request PCRs because they reliably, more often than not, contain more information about the circumstances of death than the actual Coroner Narrative. Unfortunately, without the PCR available and with a completely useless Coroner Narrative, there would have been no way I could have performed the autopsy had it not been for the investigating police agency’s presence during autopsy, during which they provided the necessary details regarding the circumstances of this child’s death.
Any person who dies any unnatural, unattended, or sudden and unexpected death in San Joaquin County deserves more than a two-word investigation by the Coroner’s Office (here: “accidental drowning” which remains unsupported by the rest of the actual Coroner’s Narrative). Any child, who is unfortunate enough to die prematurely, is especially deserving of a death investigation that meets even the bare minimum standards of death investigation, which were not afforded to this child in this case.
Per California Government Code 27491: “It shall be the duty of the coroner to inquire into and determine the circumstances, manner, and cause of all violent, sudden, or unusual deaths… deaths due to drowning…”
Simply responding to a dead body at a hospital as a Patrol Deputy for the Sheriff-Coroner’s Office is wholly inadequate in meeting the minimum standards of death investigation as determined by, not only national regulations and standards, but also by California Law. Although the investigating police agency was able to answer or ascertain details critical in understanding the circumstances around this particular death, it is the duty of the Coroner to investigate death. It is inadequate, embarrassing, and irresponsible to rely solely on local police agencies to carry the added responsibility of death investigation when there is an entire county agency (the Coroner) who is charged to do just that.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
INCOMPLETE DEATH SCENE INVESTIGATION (recorded on 12/2/17 at 7:70 PM):
Yesterday on 12/1/17, I printed my finalized report on a case (17-1026) for which the original Coroner narrative indicated that an older man was found at home without evidence of trauma or foul play. According to the Sheriff’s patrol deputy, who investigated the death and spoke with the local police agency present, witnesses on scene stated that the decedent was secretive about his medical history, so no medical history was known. The Patrol deputy also stated that no prescribed medications were collected on scene. Although I would have wanted to see his medical records, without prescription medications or witnesses who could provide a lead for a potential doctor, obtaining medical records seemed like a futile exercise. No other information in the Coroner narrative suggested that this was anything but a natural death. As such, I performed a partial autopsy on him and found significant heart disease sufficient to explain his death. Although it is not every Forensic Pathologist’s practice to request toxicology testing in otherwise natural appearing deaths, Dr. Omalu and I submit specimens for toxicology routinely. When the toxicology report was available, I was surprised to see methamphetamine in addition to two prescribed medications in his system.
I searched the Coroner case folder for more information and found that the Coroner Deputy had received the investigating police agency’s report, which I read. The police agency’s report was significantly more comprehensive as it pertained to the decedent’s history and last know circumstances. From this police report I learned the following additional details that should have been included in the Coroner narrative:
• The initial welfare check request was made because the decedent’s friend was concerned about him – the last time she spoke to him, he was threatening to harm himself.
• The decedent’s roommate revealed that he thought that the decedent had been using methamphetamine the night prior to his body being found.
• The decedent had reportedly been to a Kaiser doctor to be seen for his heart, suggesting that he did in fact have concern for, or a previous diagnosis of, heart disease.
• The police officer found two bottles of medication prescribed to the decedent, so the decedent did in fact, have medications on scene.
It is unfortunate when an investigating police agency writes a more comprehensive and detailed report than the actual Coroner when it comes to the circumstances of a person’s death, which includes any possible medical history. Because I was provided insufficient history on a decedent by the Sheriff-Coroner’s office, I was forced to do a more extensive, and thus costly, examination on the decedent, when an external exam with the appropriate medical records and toxicology would have been sufficient to render a cause and manner of death (in his case, methamphetamine toxicity).
This example substantiates the chronic, nagging feeling of incomplete Coroner investigations, often performed by Sheriff patrol deputies. Many Coroner narratives contain some variation of the phrase, “no known medical history or medications,” which always makes me suspicious, particular in older individuals who are more likely to suffer from chronic medical diseases. Unfortunately, short of abandoning the Coroner investigation altogether in lieu of relying on the local police agency’s investigation, it is more likely that Dr. Omalu and myself consequently perform more costly examinations on decedents to compensate for inadequate, and frankly negligent, death investigations carried out by the Sheriff-Coroner.

January 15, 2017
Dear Bennet,
Greetings. Ever since I accepted this position as Forensic Pathologist with San Joaquin County, you have continually made yourself available and open to questions, comments or concerns. I truly appreciate your time and efforts in maintaining this open line of communication and I am thankful that the Sheriff and the Sergeant have repeatedly offered their time as well for any concerns, as I strongly believe that it fosters an environment of professional and intellectual discussion and serves as a foundation upon which I am able to work effectively and independently in my duties as a Forensic Pathologist.
That said, I have had some time to reflect on the brief meetings I had with Sergeant Reynolds this past Tuesday and Thursday (1/10/17 and 1/12/17), during which he explained that he will be taking over the doctor scheduling, a task that you had already been doing when I began in October. Although Sgt. Reynolds stated that he was open to ideas regarding how the scheduling would be done, he offered one of two scenarios where we effectively handle autopsies a week at a time, either Mon – Sat or Thurs – Wed (Sundays being off). With some time to reflect on these options, I was reminded of my time in Baltimore where we performed autopsies for weeks at a time, and sometimes up to 12 days in a row if we were scheduled for an intervening weekend. It is through that experience that I have come to realize that the coverage of autopsies for large periods of time (i.e. a week), can be emotionally, physically and mentally taxing and overall, to a forensic pathologist’s detriment. I must say that your current scheduling arrangement has easily mitigated that and I feel that covering autopsies for up to a few days at a time is preferable to me. Due to our open line of communication, when one of us is unable to cover autopsies on a certain day, it has been effortless to switch said days without experiencing the taxing physical and mental effects described above.
In addition, it should be emphasized that, as you know, in any medical specialty the scheduling of physicians is an administrative task performed by physicians of the same specialty. Performing autopsies is coverage of a specific medical service in anatomic or forensic pathology, and as such, requires supervision from only another anatomic or forensic pathologist. Due to the highly subspecialized nature of this field of medicine, only a fellow pathologist can truly understand the time and resource demands of performing autopsies, and ultimately scheduling them. It is for these reasons, that I am concerned that transferring the task of scheduling our autopsy coverage to a member of law enforcement may encroach on my professional autonomy and make vulnerable our ability to uphold our commitment to medical excellence. In the same way that as a physician I would be ill-suited to manage or schedule members of law enforcement, as I possess neither the practical experience or knowledge base to even understand the nuances of such a task, I believe it is inappropriate for anyone other than an anatomic or forensic pathologist to engage in scheduling autopsy coverage based on calculations of perceived usages of time in performing a medical procedure as complex as a postmortem examination.
Of course, if scheduling autopsy coverage is a task that you are able to maintain, I fully commit to ensuring that changes to the schedule will be relayed immediately to Sgt. Reynolds and any other members of our office as necessary, so as to avoid confusion or delays in communication to the on-call forensic pathologist. Now that I have had some time to settle in and get used to the office, I sincerely hope that you will be able to continue the task of physician scheduling, as I believe that to be the most conducive to maintaining the medical professional integrity of this office and San Joaquin’s reputation

January 15, 2017
for thorough postmortem examinations, free from any potential bias and undue pressures, in a setting that minimizes physician stress and fatigue.
Thank you very much for your time and consideration.
Sincerely,
Susan J. Parson, M.D., M.S.

MEMORANDUM OF EVENTS
1
INFRINGEMENT OF PHYSICIAN INDEPENDENCE/COMPLAINT OF SGT. REYNOLDS CONDUCT (initially recorded 7/20/17 at 7:35 AM):
Wednesday afternoon (7/19/17), Coroner Sergeant Michael Reynolds came back to the morgue
in between autopsies at around 2:45pm to speak to me privately, in which he told me about a conflict between personnel (issues involving the technicians), and then also brought up a second issue. This second issue, and the behavior of Sgt. Reynolds, are the topics of this memorandum.
During this conversation, Sgt. Reynolds stated that the Sheriff wants greater accountability of
where Bennet and I were are for all hours of the day, citing that sometimes Dr. Omalu was is a hard to get a hold of (he reassured me that he has never had trouble getting a hold of me). He also reassured me that there was not related to a work performance issue. Sgt. Reynolds’s solution was to have Dr. Omalu and I attend (initially in person and then perhaps move to a conference call) what he called "briefings" where Dr. Omalu and I would meet with himself, all the detectives, and all the technicians to discuss the cases for the day at 9 am everyday. To this end, he said he had an IT person in the conference room at the moment of our conversation to set the phone up for conference calls. Until now, Dr. Omalu and I have been calling the morgue to speak directly with the morgue technicians to find out about cases and make requests (medical records, CT scan, scene photos, etc.) and it has been working fine; neither the doctors nor the technicians report any complaints with this practice, as this is what Dr. Omalu has been doing for years and I have been doing since I began employment with the county 9 months ago.
I responded by explaining that the physical presence of the physician for a meeting to determine
what the doctor needed is an inefficient use of my time, as there is often a waiting period to receive such items or give an agency the required 1-hour notice for a case that they want to attend. Sgt. Reynolds then suggested that I work at my desk while I'm waiting for such things. I explained that as a physician, this is not how physician scheduling in the hospital works, but the Sgt. implied that since they provide a desk and cubicle for me at the Sheriff-Coroner office, the Sheriff is able to impose such a schedule on physician employees of San Joaquin General Hospital.
Both the timing of such a precise and premeditated request and its very nature are wholly
inappropriate. The Sgt. attempted to implement a change in pathologist practice when only the newer, less experienced, younger female pathologist (myself) is present and the supervisory pathologist, Dr. Omalu, is unavailable on a scheduled vacation. Additionally, the Sgt.’s attempt to force our involvement in law enforcement meetings with the threat of the Sheriff restricting physician independence at the office by requiring that we remain at our desks from 8 AM to 5 PM similar to other law enforcement staff is coercion without the authority to do so.
As Dr. Omalu and I are employees of the hospital, it should be noted that physicians do not have
set hours in which they must be present at their desks between certain times. We are professionals, and as such, once we complete our work at the hospital (or in our case, the morgue), we are free to leave, as many times we take work home with us. Monitoring our discussions when we make requests for case information infringes on our independence and ethics as physicians to remain free from law enforcement bias.
That last point is underpinned by the fact that approximately 2-3 weeks ago, in a separate
private meeting with me, the Sgt. stated his concern that I am requesting too many medical records on cases. As a sworn law enforcement officer who has no medical experience or significant medical
MEMORANDUM OF EVENTS
2
knowledge, it is distressing to feel pressure from a Sheriff Sergeant to alter my medical investigative practices when I review cases to ultimately decide what the medical history is on a decedent and thus, the type of postmortem examination I should perform. It would be medical negligence on my behalf if I obtained inadequate medical histories on my “patients” (decedents) and therefore, despite the complaints of the Sgt. of the Coroner’s Bureau, I will not be intimidated or persuaded to perform incomplete examinations on decedents. The fact remains, however, that as a forensic pathologist assigned to a Sheriff-Coroner, one of the most important steps I can take to minimize the potential for bias or influence from law enforcement on my postmortem medical evaluations, is to communicate my needs to the morgue technicians (medically trained, non-sworn civilians, who assist me during autopsy), who have thus far, faithfully made all requests to the Detectives in regards to my needing medical records, scene photos or postmortem CT radiography.
As a result of the conversation had on Wed 7/19/17, at 7:26am on the following morning on
Thurs 7/20/17, I sent an email to the Sgt. (CC’ing my attorney and Physician Union Representative) informing him that I would not be participating in the briefings, namely because attempts to change pathologist work habits is related to our duties as pathologists, which is related to the duties set forth in my contract, and secondly, that as a physician I am not a law enforcement official, and should not be participating in law enforcement briefings, which could undermine my independence as a physician and thus create an environment where my impartial judgement and integrity may be threatened, challenged or subject to bias. I then called the morgue at approximately 8:30 AM as I usually do and spoke with Etta (morgue technician) to find out that the only new case was not yet typed, but thought to be a physician-certified death, so essentially there were no new cases for me that day.
With no new autopsies to perform, I continued to work through the morning at home, preparing
my autopsy reports as I normally do. It was soon after I arrived at work (in time for my scheduled afternoon meeting, the Child Death Review Team or CDRT), that the Sgt. stopped by my cubicle, asking to speak with me privately in his office. For the next 30 – 35 minutes, I was involved in an uncomfortable and sometimes inflammatory conversation. I listened to him patiently as he began the conversation posing many questions seeking clarification on the contents of the email I sent him this morning. He described several of his responsibilities of the office, including his desire to improve communication between the morgue technicians and the detectives.
I responded saying that I was uncomfortable with the timing of his request to make changes in
the practices of the pathologist, as it occurred on the very first day that Dr. Omalu was unavailable, and that I preferred to have this discussion upon Dr. Omalu’s return, since these practices involve him as well. The Sgt. cited the fact that two morgue technicians had each made memorandum complaints against each other recently, which is why he wanted to implement the briefings as soon as Dr. Omalu “happened to be” absent. The truth is that both of these memos were dated 7/14/17, which I noted when I read them on 7/19/17 – a full 5 days after his initial meeting with me to make a sudden change in daily pathologist practice. In fact, Dr. Omalu confirmed that the Sgt. spoke to him about these memos on the 16th, but the topic of implementing morning briefings was never brought up with Dr. Omalu. Thus, not only is the Sgt.’s perceived validation for implementing briefings illogical and unrelated (interpersonal complaints between 2 morgue technicians has nothing to do with their independent abilities to relay my requests to the Detectives), but it was also deceptive and false, as he had the course of 5 days to arrange a time to meet with both Dr. Omalu and I to discuss his briefings idea, instead of springing it on me the very day Dr. Omalu was unavailable due to air travel. Thus, during this meeting with the Sgt., it was clear that he was unable

MEMORANDUM OF EVENTS
3
to provide a viable rationale for the sudden need to implement a change in pathologist practice, even in Dr. Omalu’s absence.
In addition, during this meeting, whenever I spoke, I was almost always interrupted by Sgt.
Reynolds. After it had happened a couple of times, instead of stopping myself, I continued to speak and at that moment, the Sgt. continued to interrupt me, but only louder in order to speak over me, before I finally stopped what I was explaining. After this, when he continued to interrupt me, I stopped and identified his inappropriate conduct by saying, “…if you’ll let me finish…” to which he stopped talking the first time, but then retorted, “but you’re repeating yourself!” the second time. At several points I stated that I was uncomfortable continuing this conversation without Dr. Omalu’s input (since he would also be affected by this change in practice) and that I wanted to leave. I stated that I was uncomfortable with the conversation at least 3 times until I eventually said, “this conversation is going nowhere, you and I are both repeating the same things so I’d like to leave” but he pushed to continue the discussion and I felt pressured to stay in a discussion that was beginning to feel like an argument. He went on to say that I should have “gone up the chain of command” and sent my email to apparently the Lieutenant, Captain and the Sheriff. I responded that per my contract, I am under the direction of only 3 people: the Sheriff-Coroner, the Chair of the Department of Surgery at SJGH and the Chief Medical Examiner, Dr. Omalu. He responded by saying that as the Sgt. of the Coroner’s bureau, that he is my supervisor and oversees all that I do, which I disagree with, as he possesses neither the medical knowledge or authority to be supervising any physician.
I had stated several times during the meeting that I wanted to end the conversation. However,
my announced discomfort with the incendiary climate he created was completely ignored, met with complete dismissal, or belittling comments (“oh, you can’t do anything without Bennet present?”). He made frequent interruptions, raised his voice, and made condescending statements (“Let me give you a piece of advice… not from Sgt. Reynolds to Dr. Parson but from Mike to Sue… There are politics here and you lit a match by mentioning an attorney and union rep so you’ll probably be hearing directly from the Sheriff this afternoon when he comes.”).
Finally, at one point in the meeting, the Sgt. stated that he “instructed the girls [adult female
technicians in the morgue] not to provide any information about cases over the phone” when I make my morning call. When I first heard this, I was shocked, so I requested clarification by saying, “Do you mean to say that if I call the morgue in the morning as I usually do (and have been doing for the past 9 months), that they won’t even tell me what cases we have?”. The Sgt. said that my assessment was correct, as he had “ordered the technicians” not to share information with me.
I explained that his action was obstructing my ability to perform my duties. He declared that the
9am briefing was going to happen, with or without me, and I had the opportunity to join the briefings as previously described. He disagreed with my assessment that the briefing was a law enforcement briefing, stating that “the Coroner is a bureau under the direction of the Sheriff – the coroner is not law enforcement. Yes, we’re all sworn officers, but the Coroner is not law enforcement”. This is a completely absurd statement and a total misunderstanding of what a Sheriff-Coroner is. Most concerning, the Sgt. made it clear that he intended to obstruct the normal practices of the pathologist (which have been around for years, predating my employment here), thereby creating unnecessary constraints on my ability to triage cases and schedule autopsies, in order to force me into his poorly conceived plan of briefings.

MEMORANDUM OF EVENTS
4
I finally left that meeting when the Sgt. acknowledged that another meeting I had scheduled was about to start, leaving me less than 5 minutes to prepare mentally and get organized. After that regularly scheduled meeting (CDRT) I walked out to the morgue around 2:40 P.M. to review the medical records I was waiting on for a case, which upon review, I found to be to sufficient in order to proceed with an autopsy. Unfortunately, the Sgt. had scheduled a meeting with all of the technicians and Detectives, to presumably discuss the briefing process for the next day, with which I repeatedly informed him that I would not be involved. Thus, with the technicians expected at a meeting, I was unable to proceed with the autopsy, so I returned to my cubicle to attempt to review histology slides for another case. However, the Sgt.’s previous conduct impeded my ability to continue to work.
It should be noted that when Dr. Omalu began working for the county several years ago, he too
was approached by the Coroner Sgt. at the time (who has since left the Coroner’s office) about participating in morning briefings. Dr. Omalu’s rationale for declining then is the same as mine for declining now – to avoid any real or perceived bias or influence from law enforcement during the medicolegal death investigation process, and especially in cases of homicides, high profile, or law enforcement-related deaths. Often when a forensic pathologist is asked to testify in court, one of the first questions we get asked as “What were you told about this case before your autopsy? Who told you this information?”. Even the perception of being influenced by the police results in not only a miscarriage of justice, but a loss of faith in our abilities to be impartial physicians investigating a person’s death. This is precisely why the standard of practice is to have a typed and printed report of the circumstances of death (so it’s not left up to the interpretation of a sworn officer based on what he read or heard) and why Dr. Omalu and I communicate with the morgue technicians directly when we need additional information on a case.
In summation, the Sgt.’s inappropriate demeanor and demands made for an unproductive,
combative, and intimidatory situation. The Sgt. has no qualifications whatsoever to insert himself into the practice of medicine, thereby impeding my ability to perform my job duties. Although I’ve ignored previous occasions when he was curt or condescending to me without provocation or cause (giving him the benefit of the doubt that perhaps he was having a bad day), this meeting hit a new level in which I was specifically and vocally uncomfortable being in a closed, private office with him. Therefore, it is my sincere request that as a physician of SJGH, that shall not be left alone in a room with him where I am forced to be the target of his unprofessional, rude, and condescending conduct. I also stand by my previous statement that Sgt. Reynolds possesses neither the medical knowledge or authority to supervise any physician, and as a result, I do not legally or ethically see fit to acquiesce to his requests, particularly ones that seek to impede, threaten, or influence the impartiality to which I am professionally and ethically bound.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
MEETING WITH SHERIFF AND ASSISTANT SHERIFF ON 7/31/17 AT 1300 HOURS
HARASSMENT BY SHERIFF AND INHERENT CONFLICT OF INTEREST (recorded on 7/31/17 at 3:30 PM):
On Sunday 7/30/17, I sent an email to Coroner Sergeant Reynolds and Dr. Omalu voicing my concern regarding an incident on Friday 7/21/17 in which I was misled by the Coroner Sergeant to believe that his request to postpone cases the following day (Saturday 7/22/17) was based on a staffing issue with the Coroner Investigators, as opposed to his true rationale, which was based on an email communication he sent to Dr. Omalu on July 3rd (please see separate memo on this incident). When I checked my work email this morning, I saw that he had responded to my email and CC’ed Sheriff Moore, Assistant Sheriff Mondavi, Captain Pehl, and Investigations Sergeant Barnes. Then this morning, Sergeant Reynolds notified me via text message that the Sheriff wanted to meet with me at 1 pm.
What follows is a summary of the content discussed in that meeting with Sheriff Moore and Assistant Sheriff Mondavi, that lasted approximately 10 minutes in duration:
Sheriff Moore began by stating that he called this meeting because he was dismayed/disappointed by the timbre of the email I had sent to the Coroner Sergeant, which he had printed out and sitting before him. He wanted me to explain what the email was in order to get my take before coming to any conclusion. I explained that I was frustrated to learn that the Coroner Sergeant’s actual reason for requesting to postpone cases was different from what he told me; I explained that that sort of conduct undermines my ability to manage my own cases and workload. He responded to my explanation by saying that first, I used a “poor choice of words”, as he interpreted the content of my email as my questioning the Coroner Sergeant’s ability to manage the Coroner unit. The Sheriff cited my email: “From this point on, if there are any schedule concerns regarding my coverage of autopsies, they will need to be discussed with me truthfully and not in any misleading way, intentionally or unintentionally,” as an example of my poor word choice, saying that there was more involved in this issue (but he did not specify exactly what he meant) and that I “went off prematurely”.
He continued to cite my original email: “Dr. Omalu and I are beholden to practice medicine governed by established physician standards of ethical practice and medical guidelines,” and continued on to say, “well that’s all nice doctor, but this is still the Coroner’s office and I’m the Coroner, okay? So I get to make the rules, okay? And I get to decide what we do and what we don’t do.”
Sheriff Moore went on to say that he “lets” Dr. Omalu “participate” in making the physician schedule. Sheriff Moore began making specific comments about Dr. Omalu’s schedule (that have nothing to do with me) as a way to support his assertion that there were scheduling issues (which had never before been brought to my, and as far as I know, Dr. Omalu’s, attention), hence the Sheriff’s desire for a separate meeting with myself, Dr. Omalu, the Coroner Sergeant, the Investigations Captain and the Assistant Sheriff. Sheriff Moore went on to talk about Dr. Omalu’s word choice of an upcoming “leave of absence”, to which I stated that I couldn’t comment on Dr. Omalu’s intended meaning as that was a conversation more appropriate to have with Dr. Omalu himself.
The Sheriff advised that if I have issues with the Coroner Sergeant, I should go up the chain of command. By that he meant I should go up the Sheriff’s Office chain of command (Investigations Lieutenant, Investigations Captain, and so on), even though I am a San Joaquin General Hospital physician. The Sheriff said that if I don’t know all the facts, that I should ask questions before I “fire off

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
an email”. I explained that I would have appreciated it if the Coroner Sergeant had informed me of the discussion to give me Saturdays off, rather than giving the excuse he gave me, especially if his intent was to give me days off without my knowledge. The Sheriff said that the Coroner Sergeant didn’t have to tell me about that, although he did understand about changing the schedule, as the Sheriff stated that he tries to ensure that Sheriff’s employees are given 5 days’ notice of a chance in schedule. He said that Dr. Omalu is not in charge and then informed me of Dr. Omalu’s desire to renegotiate his contract (which is not my business and I am still unclear as to why he was sharing this with me).
Sheriff Moore ended this topic of discussion by asking that I “check the facts and talk to other people” before I go off “half-cocked”. I explained that that wasn’t my intention and he retorted that I was basically calling the Coroner Sergeant a “fibber”. I repeated that the Coroner Sergeant misled me. The Sheriff stated that he didn’t know if that was the case and he needed more answers, which he planned on obtaining before the general meeting he wanted to have. He said that in the future, if I am frustrated by anything, I should follow the chain of command and inform the Lieutenant, Captain, Assistant Sheriff and then himself. When I sought clarification as to the Sheriff’s opinion as to whether or not he felt it inappropriate that I emailed the Coroner Sergeant directly as I had, he said that the untruthful element to my email was overdone and cited the line from my email again (“From this point on, if there are any schedule concerns regarding my coverage of autopsies, they will need to be discussed with me truthfully and not in any misleading way, intentionally or unintentionally.”). He interpreted this line to mean that I was calling the Coroner Sergeant “untruthful and misleading” and I explained that I was simply stating that the Coroner Sergeant’s initial conversation with me was “misleading”.
He moved on to a couple of other topics unrelated to the email (getting together to discuss the plans for the new morgue and upcoming changes in deputy staffing for the Coroner’s office). In total, the meeting lasted approximately 10 minutes. However, the Sheriff’s overall tone towards me during the meeting made it feel as if he was scolding me for insisting that I needed non-misleading information about my cases so that I can remain as independent and unbiased as possible, especially as a hospital physician working in a Sheriff-Coroner setting.
Upon reflection of the Sheriff’s comments during this meeting, it was clear to me that the Sheriff called this meeting to re-assert his authority as Sheriff-Coroner by treating me similar to how he treats his sworn officers under his direction. Telling me that I need to report up the chain of command, in essence, creates an environment where, despite being a physician employed by San Joaquin General Hospital, I am subordinate to and can be ordered to perform my duties by the Coroner Sergeant, Investigations Lieutenant, Investigations Captain, Assistant Sheriff, and Undersheriff. Suddenly, despite being a hospital physician, the Sheriff has integrated my position into his administrate hierarchy, and uses verbal and non-verbal tactics to scold and harass me for voicing my concerns regarding limitations and unprofessional behaviors imposed on me in the performance of my medical duties. Forcing a physician into the bottom of his law enforcement hierarchy ultimately creates a situation where superior law enforcement officers can tell the physician what to do. This is the most obvious conflict of interest in conducting objective medicolegal death investigations, free from pressure or influence from the Sheriff-Coroner or his peace officer subordinates.

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
1
MEETING WITH ALL CORONER STAFF REGARDING “DOCTOR SCHEDULING” ON 8/17/17
RETALIATION, HARASSMENT, AND THREATS AGAINST PHYSICIANS BY SHERIFF (recorded on 8/17/17 at 9:25 PM):
On approximately 8/7/17, the Sheriff’s secretary sent out an Outlook notice requesting a meeting with the doctors regarding scheduling, which was scheduled for and took place today. The meeting began at approximately 11:00 AM and lasted until approximately 12:45 PM. It was attended by the following people: myself and Dr. Omalu on one side of the oblong table, Sheriff Moore at the head of the table, Undersheriff Picone in a chair in the corner near the Sheriff, and Assistant Sheriff Mondavi, Investigations Captain Pehl, Investigations Lieutenant Barnes and Coroner Sergeant Reynolds all on the other side of the table, opposite to Bennet and I, lending itself to a socio-physical seating arrangement that set the tone for the rest of the meeting.
The Sheriff began the meeting by saying that before he could get to the topic of physician scheduling, there were other problems in the office regarding specially myself, as he looked at me, said my name, and gestured towards a document that he was holding. Having no idea what he was referring to, I requested to look at the document in his possession. He pushed the document over to me across the table in front of everyone there and I immediately recognized it as a copy of my memorandum of events, entitled “Infringement Of Physician Independence/Complaint Of Sgt. Reynolds Conduct,” which was a complaint I filed with the San Joaquin General Hospital (SJGH) Human Resources (HR) Department on 7/21/17 and for which I had met with the Deputy Director of HR on 7/25 to discuss my complaint (see separate HR complaint). I was immediately stunned and blindsided by the fact that Sheriff Moore not only knew about my complaint, but had obtained a physical copy of it, all before I actually met with the appropriated HR representative (after my initial meeting with HR, a decision needed to be made regarding whether I needed to meet with an SJGH HR representative or the Sheriff’s Office HR representative. In either case, it had not yet been determined who I needed to meet with at this time. In my initial meeting with the Deputy Director of HR, I was reassured several times that I would be contacted by someone in HR prior to them contacting Coroner Sergeant Reynolds for resolution).
Although the specific contents of my complaint were not discussed openly in the meeting with the Sheriff and his entire Coroner chain-of-command staff, the document was in plain sight of everyone present, particular as he pushed it over to me to review. The Sheriff’s tone was disapproving of my complaint (per the Sheriff, I was responsible for this new problem in the Coroner’s Office) and I can only assume that everyone else at the table was aware of either its existence and/or contents – why else would it have been brought up in this meeting? I was astonished and bewildered that Sheriff Moore was retaliating against me, through his comments, tone, and use of my physical HR complaint as a prop, right in front of the Sheriff-Coroner’s administrative staff for pursing my right to file an HR complaint before I formally spoke to the appropriate HR representative. It is critical to note that no HR representative was present at any point during this meeting, as had been the previous reassurance provided by the Deputy Director of HR.
The Sheriff then proceeded to cover three main issues: 1) his authority as Coroner, 2) forensic pathologist participation in the 9 am daily briefings, and 3) transferring the responsibility of creating the physician schedule from Dr. Omalu to Coroner Sergeant Reynolds. To make his first point, the Sheriff reiterated his position as Sheriff-Coroner, stating that both Dr. Omalu and I were not employees of San

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
2
Joaquin General Hospital (despite actually being Attending Physicians at SJGH who are assigned to the Coroner’s Office; our contracts with the county are literally entitled “San Joaquin General Hospital Physician Part-Time Employee Contract” and indicate that we work under the direction of the Chairperson of Surgery and the Sheriff-Coroner), and as such, he wanted to change our titles to “Sheriff Pathologist” (which, again, is not indicated in our contract, as the title contained in our contracts is “forensic pathologist”). Essentially, the Sheriff reminded us that he is in charge, he is the Coroner, he gets to make the decisions, and we have to do what he, or any of this delegated Coroner staff (present at the meeting), says. The Sheriff also stated to me that if I disagreed with what he was saying and wanted to change the terms of my contract (which I took to mean “resign” based on his stern tone and body language), then I should speak to him about that. At some point around this portion of the meeting, Dr. Omalu requested for both him and myself to meet with the Sheriff privately regarding another matter. The Sheriff offered to meet with us individually regarding personal issues, but flatly refused to meet with us together, despite the fact that Dr. Omalu and myself share very similar concerns regarding physician independence as it pertains to maintaining our respective medical licenses, etc. Dr. Omalu wanted to discuss his concerns regarding the “aiding and abetting of the unlicensed practice of medicine” as it pertains to the Sheriff-Coroner’s interference in our duties, but the Sheriff did not want to discuss this issue at appropriate depth with Dr. Omalu.
The Sheriff’s next point was in regards to informing us that the doctors would be participating in the daily 9 am briefings, despite my initial objection via email to the Coroner Sergeant on 7/20/17, and Dr. Omalu’s objection in a personal conversation with the Coroner Sergeant on approximately 8/14/17 (which undoubtedly were passed up the chain-of-command to Sheriff Moore, as he was well aware of our objections to participating and hence this current meeting to compel us to participate). Along the lines of the rationale for our initial objections, Dr. Omalu brought up the issue of the importance of maintaining our medical licensure, which the Sheriff likened to a peace officer’s maintenance of their certification. It should be noted that a physician’s medical license and a peace officer’s certification are totally unrelated and incomparable credentials. When the discussion turned to that of the Medical Board of California, Sheriff Moore made it known that as Sheriff, he should be privy to confidential matters that exist only between the CA Medical Board and a CA-licensed physician, even despite strict instructions to maintain confidentiality and no reasonable expectation to share such an issue with an employer during active investigations. As the Sheriff was speaking, my impression was that he seemed to believe that he has some authority over the Medical Board of California, as he stated that he would take it upon himself to contact the Medical Board directly, if need be. Although the sentiment is troubling at best, I think it also underscores the Sheriff’s arrogance in terms of his role versus that of a physician and how completely ignorant he is in Physician matters, standards of practice, and most importantly, the fact that the privilege to practice medicine as physicians is granted only through a State Medical Board, and not through any Law Enforcement agency, including the Sheriff’s Office.
Finally, on the issue of Physician scheduling, the Sheriff advised that Coroner Sergeant Reynolds would now be responsible for creating the Physician schedule, despite our continued objections and despite the fact that physician scheduling has been a responsibility of Dr. Omalu’s since he stated working for the County several years ago. In an attempt to explain why physician schedules are always created by physicians, Dr. Omalu’s explanation fell on deaf ears, as this appeared to be a topic that was not open to discussion with the Sheriff (please see my original letter to Dr. Omalu in January 2017 when the Sheriff first wanted to take over physician scheduling). At around this time, the Sheriff had to excuse

MEMORANDUM OF EVENTS Susan J. Parson, MD, MS, DABP (AP, FP)
3
himself from the meeting and Undersheriff Picone moved into his seat to continue. We continued to discuss some of these issues in more depth, including physician scheduling. In an attempt to refute the idea that physicians create physician schedules, the Undersheriff shared that his wife is a non-medically trained employee at a local hospital who creates the schedules of the Physicians for the Emergency Department. Although that may be how it is perceived, it is more likely that the physician schedules he referred to are made under the supervision and approval of the medical director (physician) of that department.
At the conclusion of the meeting, Dr. Omalu and I reluctantly agreed to participate in a trial of morning briefings – we had no other option – agreeing to participate only to convey what we needed on a certain case (medical records, CT scan, scene photos, etc.), and absolutely not to discuss our approach to the case or what kind of examination we planned to do, so as to avoid any perception of bias from law enforcement and maintain our independence as physicians, while being forced to participate in these briefings against our will.
I walked away from this meeting emotionally and mentally exhausted – it was after all, almost 2 hours of Sheriff Moore retaliating against the fact that I had filed an HR complaint, asserting his authority and that of his Coroner hierarchy over the physicians, threatening to change our employment titles in our contracts to make us his official employees which would ultimately strip us of our hospital physician privileges, forcing the physicians to participate in morning briefings with law enforcement against our continued and strong objections, and taking the physician’s duty of physician scheduling away from Dr. Omalu also against our sustained and strong objections.
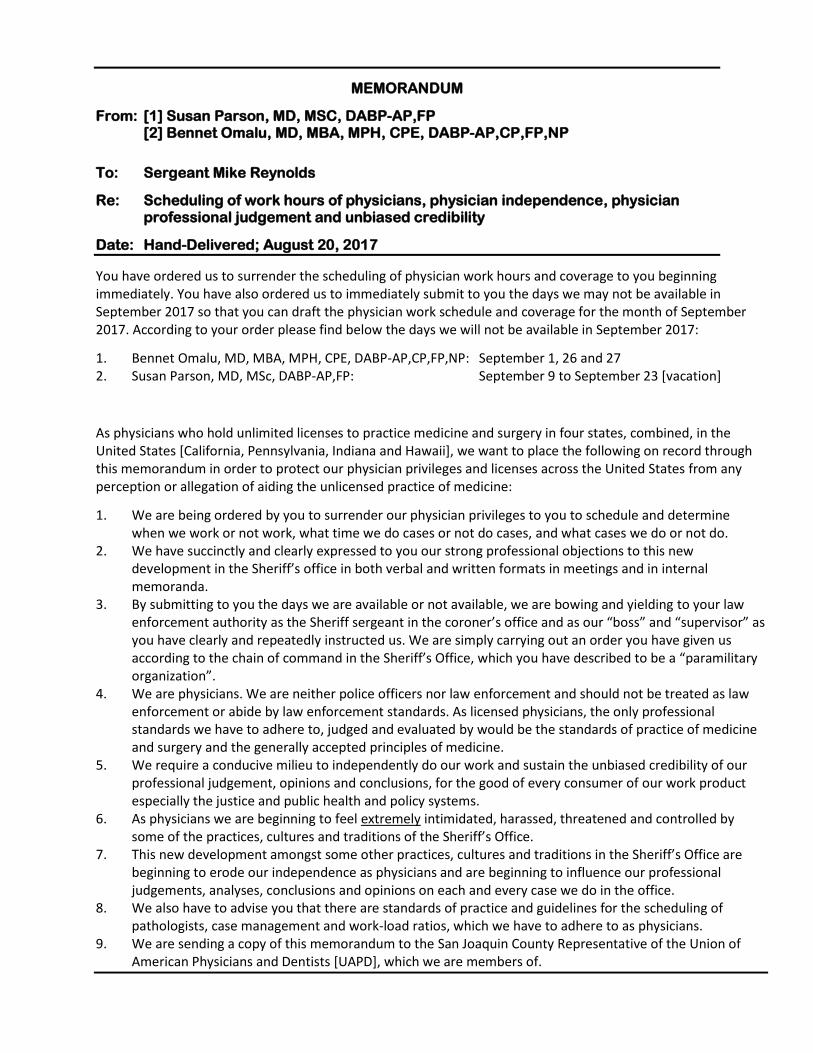
MEMORANDUM
From: [1] Susan Parson, MD, MSC, DABP-AP,FP [2] Bennet Omalu, MD, MBA, MPH, CPE, DABP-AP,CP,FP,NP
To: Sergeant Mike Reynolds
Re: Scheduling of work hours of physicians, physician independence, physician professional judgement and unbiased credibility
Date: Hand-Delivered; August 20, 2017
You have ordered us to surrender the scheduling of physician work hours and coverage to you beginning immediately. You have also ordered us to immediately submit to you the days we may not be available in September 2017 so that you can draft the physician work schedule and coverage for the month of September 2017. According to your order please find below the days we will not be available in September 2017:
1. Bennet Omalu, MD, MBA, MPH, CPE, DABP-AP,CP,FP,NP: September 1, 26 and 27 2. Susan Parson, MD, MSc, DABP-AP,FP: September 9 to September 23 [vacation]
As physicians who hold unlimited licenses to practice medicine and surgery in four states, combined, in the United States [California, Pennsylvania, Indiana and Hawaii], we want to place the following on record through this memorandum in order to protect our physician privileges and licenses across the United States from any perception or allegation of aiding the unlicensed practice of medicine:
1. We are being ordered by you to surrender our physician privileges to you to schedule and determine when we work or not work, what time we do cases or not do cases, and what cases we do or not do.
2. We have succinctly and clearly expressed to you our strong professional objections to this new development in the Sheriff’s office in both verbal and written formats in meetings and in internal memoranda.
3. By submitting to you the days we are available or not available, we are bowing and yielding to your law enforcement authority as the Sheriff sergeant in the coroner’s office and as our “boss” and “supervisor” as you have clearly and repeatedly instructed us. We are simply carrying out an order you have given us according to the chain of command in the Sheriff’s Office, which you have described to be a “paramilitary organization”.
4. We are physicians. We are neither police officers nor law enforcement and should not be treated as law enforcement or abide by law enforcement standards. As licensed physicians, the only professional standards we have to adhere to, judged and evaluated by would be the standards of practice of medicine and surgery and the generally accepted principles of medicine.
5. We require a conducive milieu to independently do our work and sustain the unbiased credibility of our professional judgement, opinions and conclusions, for the good of every consumer of our work product especially the justice and public health and policy systems.
6. As physicians we are beginning to feel extremely intimidated, harassed, threatened and controlled by some of the practices, cultures and traditions of the Sheriff’s Office.
7. This new development amongst some other practices, cultures and traditions in the Sheriff’s Office are beginning to erode our independence as physicians and are beginning to influence our professional judgements, analyses, conclusions and opinions on each and every case we do in the office.
8. We also have to advise you that there are standards of practice and guidelines for the scheduling of pathologists, case management and work-load ratios, which we have to adhere to as physicians.
9. We are sending a copy of this memorandum to the San Joaquin County Representative of the Union of American Physicians and Dentists [UAPD], which we are members of.

MEMORANDUM OF EVENTS ATTEMPTS OF OVERT OR SUBTLE CONTROL OVER PHYSICIAN PRACTICE BY SHERIFF-CORONER
1
October 1, 2017
As one of the only two Forensic Pathologists for San Joaquin County, several concerns have been evolving over the past few months that have led my colleague, Dr. Bennet Omalu, and myself to reach out to the San Joaquin General Hospital Medical Chiefs for guidance and support, which most recently entails the Sheriff’s attempt to control Physician scheduling. Regrettably, I have had some additional personal experiences with Sheriff-Coroner personnel, in which an attempt to influence or control aspects of my practice as a physician has been made, which cannot and must not be tolerated. The importance of maintaining physician independence in the setting of a para-military organization like the Sheriff-Coroner system is paramount, so as to preserve my ethical and practical duties by adhering to the standard physician guidelines to which I, and every California licensed physician, am beholden.
First, in early June of this year, Coroner Sgt. Reynolds called me into his office asking to speak with me privately. Amongst other unrelated topics, he stated that I had been requesting medical records on all of my cases and wanted to know why I needed so many. I corrected him by saying that I request records for seemingly natural deaths where a person has a vague or known medical history or in injury/poisoning cases where the presence of natural disease needs to be further investigated (usually, I request the last 2-3 PCP visits). Certainly, when a person goes to the hospital and dies there, I always expect to see those records. He explained that I was requesting too many medical records and this was putting undue amounts of work on the Coroner Investigators, who fax over my requests. As a law enforcement officer who has no medical experience or significant medical knowledge, it is distressing to feel pressure from a peace officer to alter my medical investigative practices when I review cases to ultimately decide what the medical history is on a decedent, the type of postmortem examination I should perform, and ultimately the cause of death. It would be medical negligence on my behalf if I obtained inadequate medical histories on my “patients” (decedents) and therefore, despite the Sgt.’s complaints, I will not be intimidated or persuaded to perform incomplete medical history reviews on decedents.
Second, on the morning of Saturday 6/10/17, the Sgt. called me to request that I push cases until Monday, citing an emergency medical situation with the only scheduled Investigator for Saturday. When I asked what cases were pending, he said just one case (a traffic fatality). I reluctantly agreed because I felt like he left me no choice and because Dr. Omalu was scheduled to cover autopsies on Monday. After the weekend, I was informed by Dr. Omalu that a homicide had come in late Friday night, which the Sgt. knowingly omitted when I asked him about cases because it was inconvenient for the investigating agency to attend an autopsy on a Saturday. The financial and medical ramifications in delaying the performance of an autopsy for this specific case can be further described by Dr. Omalu, as it was his case.
On a similar note, the loss of staffing in July of this year led to the shifting of Investigator workloads to only one Detective instead of three. On one particular weekend while Dr. Omalu was away on vacation (7/22/17), the Sgt. approached me in the morgue on Friday 7/21/17 requesting to hold off on doing Saturday autopsies so that the single Investigator could take a day off. Being sympathetic to the staffing dilemma, I agreed to this UNLESS there were any homicides, multiple motor vehicle collision/trauma cases, or any suspicious cases/possible homicides that a police agency would want to attend. Since the Sgt. had previously intentionally deceived me regarding the case workload on a Saturday before, I pushed for more specific details when I asked him about the cases on that Saturday morning. Ultimately, I discovered that despite there being several cases I could and preferred to complete on Saturday, the Sgt.’s ultimate motive in asking me to push cases to Monday was to give me Saturday off even though a) I was unaware of his intent, and b) it was inconvenient and impractical to do so (Monday is generally a heavy day since no autopsies are performed on Sunday). Although I am more than willing to work with the Sgt. to accommodate limited staffing when necessary, it is frankly dishonest to convey staffing as the root issue when it’s not the case at all (that Investigator was planning on coming in on Saturday anyway). It is an inappropriate management of physician services for the Sgt. to decide when I need a day off without my input, knowledge of the daily caseload, or how it many impact myself and the morgue technician staff come Monday morning. Furthermore, it goes against hospital and medical practice for a non-physician to intentionally deceive physicians in order to make changes in their service schedule.
Overall, it is clear that the Sheriff and his peace officer staff, despite having zero medical knowledge, education or training, feel emboldened to challenge and attempt to influence or control the forensic pathologists

MEMORANDUM OF EVENTS ATTEMPTS OF OVERT OR SUBTLE CONTROL OVER PHYSICIAN PRACTICE BY SHERIFF-CORONER
2
in this setting. When law enforcement has the ability to assert any level of control or influence over the practice of forensic medicine, we as physicians are failing not only our community, but also our pledge of the Hippocratic Oath and professional ethical standards and practice.
Susan J. Parson, MD, MS, DABP (AP, FP) Forensic Pathologist / Medical Examiner San Joaquin General Hospital San Joaquin County Sheriff-Coroner















![PERSONAL MEMORANDA [Office Copy]](https://img.pdfslide.net/doc/110x75/61bd3a5561276e740b10a203/personal-memoranda-office-copy.jpg)