Embed Size (px)
Citation preview
Menopausal hormone therapy and risk of gastrointestinalcancer: nested case–control study within a prospectivecohort, and meta-analysis
Jane Green1, Gabriela Czanner1,2, Gillian Reeves1, Joanna Watson1, Lesley Wise3,4, Andrew Roddam1,5 and Valerie Beral1
1 Cancer Epidemiology Unit, University of Oxford, Oxford OX3 7LF, United Kingdom2 Department of Statistics, University of Warwick, Coventry CV4 7A, United Kingdom3Medicines and Healthcare products Regulatory Agency, London SW1W 9SZ, United Kingdom4 Takeda Global Research and Development Centre (Europe) Ltd, London WC2B 4AE, United Kingdom5 Center for Observational Research, Amgen Ltd, Uxbridge, UB8 1DH, United Kingdom
Use of menopausal hormone therapy (HT) has been associated with reduced risk of colorectal cancer; evidence for its effect
on other gastrointestinal cancers is limited. We conducted a nested case–control study within a UK cohort, and meta-analyses
combining our results with those from published studies. Our study included women aged 501 in the UK General Practice
Research Database (GPRD): 1,054 with oesophageal, 750 with gastric and 4,708 with colorectal cancer, and 5 age- and
practice-matched controls per case. Relative risks (RRs) and 95% confidence intervals (CIs) for cancer in relation to
prospectively-recorded HT prescriptions were estimated by conditional logistic regression. Women prescribed HT had a
reduced risk of oesophageal cancer (adjusted RR for 11 vs. no HT prescriptions, 0.68, 95% CI 0.53–0.88; p 5 0.004), gastric
cancer (0.75, 0.54–1.05; p 5 0.1) and colorectal cancer (0.81, 0.73–0.90; p < 0.001). There were no significant differences in
cancer risk by HT type, estimated duration of HT use or between past and current users. In meta-analyses, risks for ever vs.
never use of HT were significantly reduced for all three cancers (summary RR for oesophageal cancer, 0.68, 0.55–0.84, p <0.001; for gastric cancer, 0.78, 0.65–0.94, p 5 0.008; for colorectal cancer, 0.84, 0.81–0.88, p < 0.001). In high-income
countries, estimated incidence over 5 years of these three cancers combined in women aged 50–64 was 2.9/1,000 in HT
users and 3.6/1,000 in never users. The absolute reduction in risk of these cancers in HT users is small compared to the HT-
associated increased risk of breast cancer.
Although the use of certain types of hormone therapy (HT)for the menopause has been associated with increased risk ofcancers of the reproductive tract, including breast, ovary andendometrium,1,2 there is also evidence for a reduced risk ofcolorectal cancer in HT users.3–7 However it is unclearwhether the association with colorectal cancer differs by HTtype or pattern of use, or by cancer site.8–10 Epidemiologicalevidence for an association between HT use and risk of theless common cancers of the gastrointestinal tract is limited,with most published results showing non-significant reduc-
tions in risk in HT users both for oesophageal cancer11–14
and for gastric cancer.12,13,15–17
We report here on the relation between prospectivelyrecorded prescribing information for HT and the subsequentincidence of cancers of the oesophagus, stomach and colorec-tum in the UK General Practice Research Database (GPRD)cohort. We also report the results of meta-analyses combin-ing our findings with other published data on the relationbetween HT use and the risk of each of the three gastrointes-tinal cancers.
Material and MethodsThe general practice research database
The General Practice Research Database (GPRD) is a compu-terised database containing linked anonymised patientrecords for about 10 million people in the UK registered witha National Health Service (NHS) primary care physician(General Practitioner, or GP); http://www.gprd.com (accessedJuly 13, 2010). All GP consultations, prescriptions issued bythe GP, test results and diagnoses from primary and second-ary care, referrals to outpatient clinics, hospital admissionsand deaths are coded by the GP and entered onto the GPRDdatabase. For each individual, basic demographic and somelifestyle data are also recorded. GPRD prescription data have
Key words: hormone therapy, cancer, colorectal cancer, oesophageal
cancer, gastric cancer, menopause
Grant sponsors: Medical Research Council, Independent Scientific
Advisory Committee of the GPRD; Grant number: protocol number
10_006R; Grant sponsor: Cancer Research UK
DOI: 10.1002/ijc.26236
History: Received 24 Jan 2011; Accepted 24 May 2011; Online 13
Jun 2011
Correspondence to: Dr. Jane Green, Cancer Epidemiology Unit,
University of Oxford, Oxford OX3 7LF, United Kingdom,
Tel.: þ44-1865-289-659; Fax: þ[44-1865-289-610], E-mail: jane.
Epidemiology
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC
International Journal of Cancer
IJC

been shown to be accurate and virtually complete, andGPRD data on cancer incidence on average 95% accurate.18
Patients are recorded as entering the GPRD when they areregistered with a participating GP (and the research-activestart date is this date or, if later, the date at which the partic-ipating practice data is declared up to standard), and leavethe database when they move to a non-participating GP,leave the NHS (e.g., through emigration), or die. The data-base thus consists of longitudinal medical records where indi-viduals’ length of follow-up is the time between entering andleaving the GPRD.
Study design
We conducted a nested case–control study of gastrointestinalcancer in women in the GPRD cohort. Cases were defined aswomen aged 50 or more years with a diagnosis of incidentinvasive cancer of the oesophagus (ICD-10 code C15), stom-ach (C16) or colorectum (C18–20) recorded between 1995and 2005, and with at least 12 months of follow-up withinGPRD before the date of diagnosis. For each case, five con-trol women without prior gastrointestinal cancer wereselected, matched on participating general practice, age (6 2years) and observation period in the GPRD. The observationperiod for this study was identical for cases and theirmatched controls. For cases, the observation period was thetime between the start date of the case in the GPRD and thedate of diagnosis. Controls were eligible if their follow-upwithin the GPRD included the start and end dates of the ob-servation period of their matched case, and for all analysesthe observation period of the controls was set to match thatof the cases exactly. Women were defined as exposed to HTif they had a record within the observation period (i.e., priorto the index date, the date of diagnosis of cases) of at leastone prescription for any HT preparation (as classified by theBritish National Formulary: Sections 6.4.1.1 [oestrogens forhormone replacement therapy, including tibolone] and6.4.1.2 [progestagens]). We did sensitivity analyses in whichHT exposure was defined as having at least two HT prescrip-tions within the observation period. For some analyses, HTwas classified by type: oestrogen-only, combined oestrogen–progestagen (either a combined preparation or prescriptionson the same day for an oestrogen and a progestagen) orother. Women with their most recent HT prescription in the12 months before the index date were classified as having acurrent HT prescription. Duration of use of HT was esti-mated as the time between first prescription and last pre-scription. The dataset used for this study is part of a largerdataset used for a study of gastrointestinal cancer in relationto prescribing of oral bisphosphonates.19
Conditional logistic regression was used to calculate rela-tive risks (RRs) and 95% confidence intervals (CIs) for oeso-phageal, stomach and colorectal cancer in relation to HT pre-scription. All analyses used the STATA computing package(STATACorp, 2009, release 10.1). The main analyses wereconditioned on the matching factors of age, general practice
and observation time and adjusted for smoking status (latestrecord before index date: never, past and current), alcoholintake (latest record before index date: non-drinker anddrinker) and body mass index (latest record at least 2 yearsbefore index date: <25, 25–30 and 30þ). Women with miss-ing values for each of these variables were assigned to a sepa-rate category. Sensitivity analyses were done restricting analy-ses to patients with complete data on smoking, alcohol andbody mass index, and to women whose first available HTprescription was at least 12 months after the start of the ob-servation period.
Meta-analyses
For our meta-analyses, we reviewed published epidemiologi-cal studies of use of HT for the menopause and risk of inci-dent invasive cancer of the oesophagus, stomach or colorec-tum. Relevant studies published between 1945 (Web ofScience), 1970 (PubMed), 1974 (Embase) and January 2011were identified through searches of electronic databases usingcombinations of the search terms: *esophageal neoplasms,stomach neoplasms, colorectal neoplasms; hormone replace-ment therapy, *estrogen; risk factors and from referencescited in identified papers. No limits were placed on date orlanguage of publication. Studies were included in the meta-analyses if they provided at least one age-adjusted relative riskwith 95% CIs for HT use compared with never use, and had atleast 10 exposed cancer cases. The most fully adjusted estimatesof relative risk were extracted for each study. To estimate theoverall result for exposure categories comparable across studies,results from published subgroups were combined, where neces-sary, in proportion to the numbers in each subgroup.20 Sum-mary RRs for all studies were estimated by calculating theweighted average of the study-specific log RRs, with weightsproportional to the inverse of the variances of the study-specificlog RRs. Studies were grouped according to study design, andsummary estimates were calculated separately for randomisedtrials and for observational studies with prospective and thosewith retrospective determination of exposure.
For estimation of absolute risks associated with HT use,the summary RRs calculated here were applied to incidencerates typical of women aged 50–64 in North America and inEurope, for each cancer site.21
Role of the funding source
The funders of this study played no role in the study design,analysis or in writing of the paper.
ResultsGPRD study
The GPRD study included 1,054 women with incident cancerof the oesophagus, 750 with incident gastric cancer, 4,708with incident colorectal cancer and a total of 32,457 matchedcontrols. The mean observation period of cases and controlsin the GPRD was 7.4 years, with mean year of diagnosis2001. General practice consultation rates were similar for
Epidemiology
2388 Menopausal HT and risk of gastrointestinal cancer
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

cases and controls (mean number of consultations per year,14 [SD13] and 13 [SD12], respectively, excluding the 12months prior to the index date). Table 1 shows the character-istics of cases and controls for each of the three cancer sites.Women with gastric cancer, and their age-matched controls,were on average older (mean age 76.4 years) than those withoesophageal or colorectal cancer (mean ages 75.4 and 73.8years, respectively). Overall, 13% of cases and 15% of controlshad at least one prescription for HT during the observationperiod and for each cancer site the proportion with at leastone HT prescription was lower in cases than in controls. Dif-ferences in the proportion with at least one HT prescriptionamong the controls for each cancer site—10%, 14% and 16%for gastric, oesophageal and colorectal cancer controls,respectively—are accounted for by the differences in averageage of the groups. Control women with HT prescriptionswere on average younger (mean age 63 years, compared withmean age 76 years for women with no HT prescriptions) andthey were less likely to have missing data on smoking (4%missing in those with HT prescriptions vs. 16% in thosewithout), alcohol intake (12% vs. 27% missing) and bodymass index (13% vs. 33% missing).
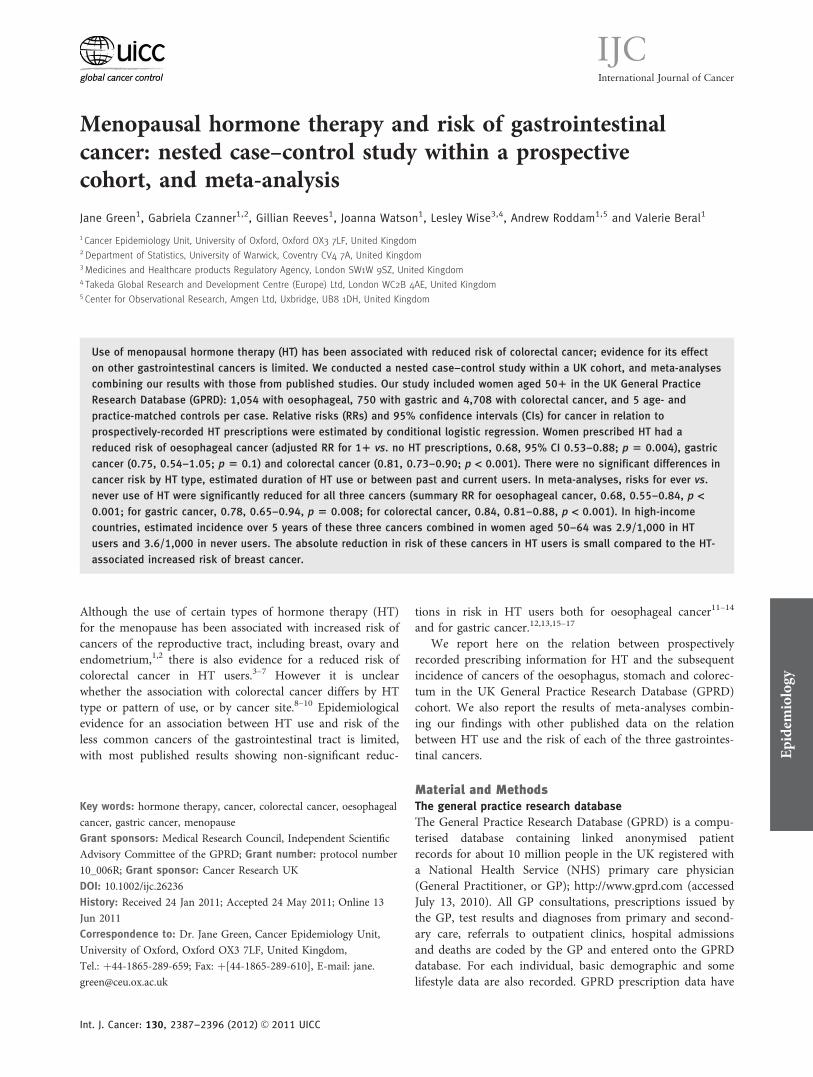
Table 2 shows the relation between prospectively recordedHT prescribing and cancer incidence by site. Compared withwomen who had no prescription for HT during the observa-
tion period, women prescribed HT had a relative risk lessthan 1.00 at all three cancer sites, with the RRs for oesopha-geal cancer (adjusted RR 0.68, 95% CI 0.53–0.88; p ¼ 0.004)and for colorectal cancer (0.81, 0.73–0.91, p < 0.001) beingstatistically significant and that for gastric cancer (0.75, 0.54–1.05, p ¼ 0.10) non-significant. For cancers at all three sites,there were no significant differences in risk between thosewith current and past HT prescriptions, by number of pre-scriptions, by estimated duration of use of HT or by type ofHT prescribed.
The HT-related risks were not significantly modified byage at index date, smoking status, alcohol intake or bodymass index (Table 3). In sensitivity analyses, results similarto those in the main analyses were found for HT exposuredefined as two or more prescriptions during the observationperiod, for analyses restricted to women with complete dataon adjustment variables and for analyses restricted to womenwith a first HT prescription at least 12 months after the startof the observation period (data available on request).
For colorectal cancer, there was no significant differencebetween the HT-related RRs by site: for cancer of the colon(2,961 cases, 388 with HT exposure), RR for any HT vs. noHT was 0.76 (0.67–0.87); and for cancer of the rectum (1,480cases, 229 with HT exposure), 0.92 (0.76–1.10): p for hetero-geneity ¼ 0.1). For oesophageal and gastric cancers, analyses
Table 1. Characteristics of women with gastrointestinal cancer and of control women1
Oesophageal cancer Gastric cancer Colorectal cancer
Cases,n 5 1,054
Controls,n 5 5,245
Cases,n 5 750
Controls,n 5 3,722
Cases,n 5 4,708
Controls,n 5 23,490
Mean years of observation 7.7 7.7 7.5 7.5 7.4 7.4
Age at index date, n (%)
50–64 years 171 (16) 855 (16) 100 (13) 498 (13) 973 (21) 4,867 (21)
65–74 years 281 (27) 1,403 (27) 182 (24) 907 (24) 1,347 (29) 6,729 (29)
75þ years 602 (57) 2,987 (57) 468 (62) 2,317 (62) 2,388 (51) 11,894 (51)
Smoking status, n (%)
Never 532 (51) 3,108 (59) 418 (56) 2,226 (60) 2,792 (59) 13,917 (59)
Past 147 (14) 700 (13) 133 (18) 464 (13) 585 (12) 2,967 (13)
Current 227 (22) 655 (13) 111 (15) 447 (12) 744 (16) 3,386 (14)
Missing 148 (14) 782 (15) 88 (12) 585 (16) 587 (13) 3,220 (14)
Alcohol intake, n (%)
Non-drinker 216 (21) 1,137 (22) 193 (26) 850 (23) 972 (21) 4,780 (20)
Drinker 582 (55) 2,792 (53) 385 (51) 1,853 (50) 2,668 (57) 12,997 (55)
Missing 256 (24) 1,316 (25) 172 (23) 1,019 (27) 1,068 (23) 5,713 (24)
Body mass index [kg/m2], n (%)
<25.0 349 (33) 1,563 (930) 228 (29) 1,078 (29) 1,400 (30) 6,992 (30)
25.0–29.9 236 (22) 1,312 (30) 169 (23) 909 (24) 1,189 (25) 6,144 (26)
30.0þ 128 (12) 751 (14) 117 (16) 491 (13) 688 (15) 3,463 (15)
Missing 341 (32) 1,619 (31) 236 (32) 1,244 (33) 1,431 (30) 6,891 (29)
1þ HT prescriptions, n (%) 114 (11) 716 (14) 64 (9) 377 (10) 656 (14) 3,702 (16)
1Controls matched to cases on age at index date, general practice and observation period in GPRD (see Methods).
Epidemiology
Green et al. 2389
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC
Table
2.Relative
risks(RRs)
and95%
confidence
intervals
(CIs)forincidentgastrointestinalcancerfor1þ
versusnoHTprescriptions
Oeso
phagealcancer
Gastriccancer
Colorectalcancer
HTmean
nRx/mean
years
1Cases/
controls
RR2
(95%
CI)
HTmean
nRx/mean
years*
Cases/
controls
RR2
(95%
CI)
HTmean
nRx/mean
years*
Cases/
controls
RR2
(95%
CI)
Overallresu
lts
NoHTprescriptions
–940/4
,529
1.00
–686/3
,345
1.00
–4,052/1
9,788
1.00
1þ
HTprescriptions
15/4
.3114/7
16
0.68(0.53–0.88)
13/4
.264/3
77
0.75(0.54–1.05)
14/3
.9656/3
,702
0.81(0.73–0.90)
SubgroupsbyHTuse
Recency
ofprescription3
Current(<
1year)
22/5
.955/3
45
0.68(0.49–0.94)
19/5
.931/1
98
0.69(0.44–1.10)
17/4
.73,16/1
,826
0.79(0.69–0.91)
Past,1–4years
12/3
.428/1
89
0.64(0.42–0.99)
12/3
.517/9
40.77(0.44–1.35)
13/4
.0162/9
96
0.75(0.62–0.90)
past,5þ
years
7/2
.331/1
82
0.76(0.49–1.15)
4/1
.416/8
50.87(0.49–1.53)
6/2
.3178/8
80
0.94(0.78–1.12)
Numberofprescriptions
1–9
4/1
.950/3
42
0.64(0.45–0.89)
4/1
.433/1
82
0.83(0.55–1.25)
4/1
.6328/1
,901
0.80(0.70–0.91)
10þ
24/6
.264/3
74
0.73(0.53–1.00)
24/7
.131/1
95
0.68(0.43–1.06)
24/6
.2328/1
,801
0.84(0.73–0.96)
Estim
ateddurationofuse
<¼1
year
3/0
.322/1
73
0.60(0.38–0.96)
2/0
.218/1
12
0.74(0.44–1.25)
2/0
.3172/9
95
0.80(0.67–0.95)
1–4years
10/2
.646/2
66
0.73(0.51–1.04)
11/2
.923/1
26
0.82(0.50–1.35)
11/2
.9274/1
,474
0.86(0.74–0.99)
5þ
years
27/7
.946/2
77
0.69(0.48–1.00)
25/8
.523/1
39
0.70(0.42–1.17)
27/8
.0210/1
,233
0.77(0.65–0.91)
HTtypeprescribed
Everoestrogen-only
20/5
.041/2
81
0.65(0.45–0.93)
17/5
.524/1
55
0.70(0.43–1.12)
18/4
.4253/1
,460
0.80(0.69–0.93)
Everoestrogenþ
progestagen
14/4
.776/4
21
0.77(0.57–1.04)
14/4
.839/2
06
0.83(0.55–1.24)
14/4
.2383/2
,117
0.83(0.73–0.94)
1nRx¼
numberofprescriptions;
years
¼estim
ateddurationofuse.Allprescribinginform
ationis
within
thestudyobservationperiod.2Relative
risksconditionedonmatchingfactors
(age,general
practiceandcalendartimeandlength
ofobservationin
GPRD),andadjustedforsm
oking,alcoholintakeandbodymass
index(seeMethods).3Timebetweenlatest
HTprescriptionandindexdate.
Abbreviation:HT¼
horm
onetherapyforthemenopause.
Epidemiology
2390 Menopausal HT and risk of gastrointestinal cancer
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

by tumour histology or subsite were not possible becausesuch information was lacking for the majority of cases.
Meta-analyses combining our results with published data
Figure 1 shows results for oesophageal cancer and for gastriccancer from our study, together with those from other pub-lished studies.11,13–17 One study by Lindblad et al.,12 whichincluded 299 cases of esophageal cancer and 313 of gastriccancer recorded in GPRD between 1994 and 2001, was notincluded in this meta-analysis because of overlap with thepresent study (as expected, Lindblad et al. found RRs forthese cancers similar to ours).
Results from the four studies of oesophageal cancer (twowith retrospective, and two with prospective, data on expo-sure; and with a total of 177 cases exposed to HT) gave a sig-nificantly reduced summary RR of 0.68, 95% CI 0.55–0.84(p < 0.001). RR was lower than 1.00 in each individual study.Two of the studies included cases with squamous cellcarcinoma only, one included cases with adenocarcinomaand the current study included all histological types, butthere was no significant heterogeneity between study results(v23 ¼ 1.5, p ¼ 0.7).
For gastric cancer, the combined results from five studies(two with retrospective and three with prospective exposure
data; with a total of 208 cases exposed to HT) gave a signifi-cantly reduced summary RR of 0.78 95% CI 0.65–0.94 (p ¼0.008), again with no significant heterogeneity between stud-ies (v24 ¼ 0.5, p ¼ 1.0). Two studies of gastric cancerincluded all histological types; the remaining three wererestricted to adenocarcinomas.
For colorectal cancer, the meta-analyses include resultsfrom 30 studies in total (the estrogen-only and estrogen–pro-gestagen arms of the Women’s Health Initiative trials areclassed here as separate studies): the present study, threerandomised trials,3,4,8 12 other studies with prospectively col-lected exposure data9,10,22–31 and 14 studies with retrospec-tively collected exposure data.32–45 Of the 30 studies, 16examined colorectal cancer risk separately in relation to useof oestrogen-only HT (2,285 exposed cases) and 17 in rela-tion to use of oestrogen–progestagen HT (1,355 exposedcases). There were statistically significant reductions in risk ofcolorectal cancer for both HT types, and very little differencebetween these risks (summary RRs in ever compared withnever users, 0.83, 95% CI 0.79–0.88 and 0.81, 0.75–0.87 foroestrogen-only HT and oestrogen–progestagen HT, respec-tively; Table 4). The main analyses, therefore, show resultsfor use of all types of HT, including studies that did notspecify which type of HT was used.
Table 3. Relative risks (RRs) and 95% confidence intervals (CIs) for incident gastrointestinal cancer for 1þ versus no HT prescriptions, withincategories of characteristics of women
Oesophageal cancer Gastric cancer Colorectal cancer
n exposedcases/controls
RR1
(95% CI)n exposedcases/controls
RR1
(95%CI)n exposedcases/controls
RR1
(95%CI)
All women 114/716 0.68 (0.53–0.88) 64/377 0.75 (0.54–1.05) 656/3,702 0.81 (0.73–0.90)
By characteristics
Age at index date, years
50–64 73/436 0.63 (0.44–0.92) 41/219 0.83 (0.51–1.36) 405/2,275 0.79 (0.68–0.92)
65–74 30/214 0.65 (0.42–1.00) 17/112 0.67 (0.38–1.18) 197/1,080 0.88 (0.74–1.04)
75þ 11/66 0.82 (0.43–1.57) 6/46 0.66 (0.28–1.57) 54/347 0.76 (0.56–1.02)
p het ¼ 0.8 p het ¼ 0.8 p het ¼ 0.6
Smoker
Yes 63/252 0.69 (0.44–1.07) 22/132 0.50 (0.27–0.92) 236/1,321 0.76 (0.61–0.95)
No 48/437 0.83 (0.55–1.25) 39/228 0.96 (0.60–1.54) 399/2,219 0.88 (0.76–1.02)
p het ¼ 0.1 p het¼ 0.1 p het¼ 0.5
Alcohol drinker
Yes 78/520 0.67 (0.49–0.94) 42/267 0.63 (0.40–1.00) 492/2,747 0.81 (0.71–0.92)
No 20/100 0.68 (0.28–1.65) 14/64 1.41 (0.54–3.68) 97/532 0.79 (0.52–1.20)
p het ¼ 0.2 p het ¼ 0.4 p het ¼ 0.7
Body mass index, kg/m2
<25 50/292 0.49 (0.28–0.84) 29/147 1.23 (0.63–2.29) 241/1,456 0.76 (0.61–0.94)
25þ 50/339 0.78 (0.55–1.10) 29/183 0.65 (0.41–1.02) 327/1,765 0.87 (0.76–1.00)
p het ¼ 0.9 p het ¼ 0.4 p het ¼ 0.1
1Relative risks conditioned on matching factors (age, general practice and calendar time and length of observation time in GPRD) and adjusted asappropriate for smoking, alcohol intake and body mass index (see Methods); p het ¼ p for heterogeneity between category groups.
Epidemiology
Green et al. 2391
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

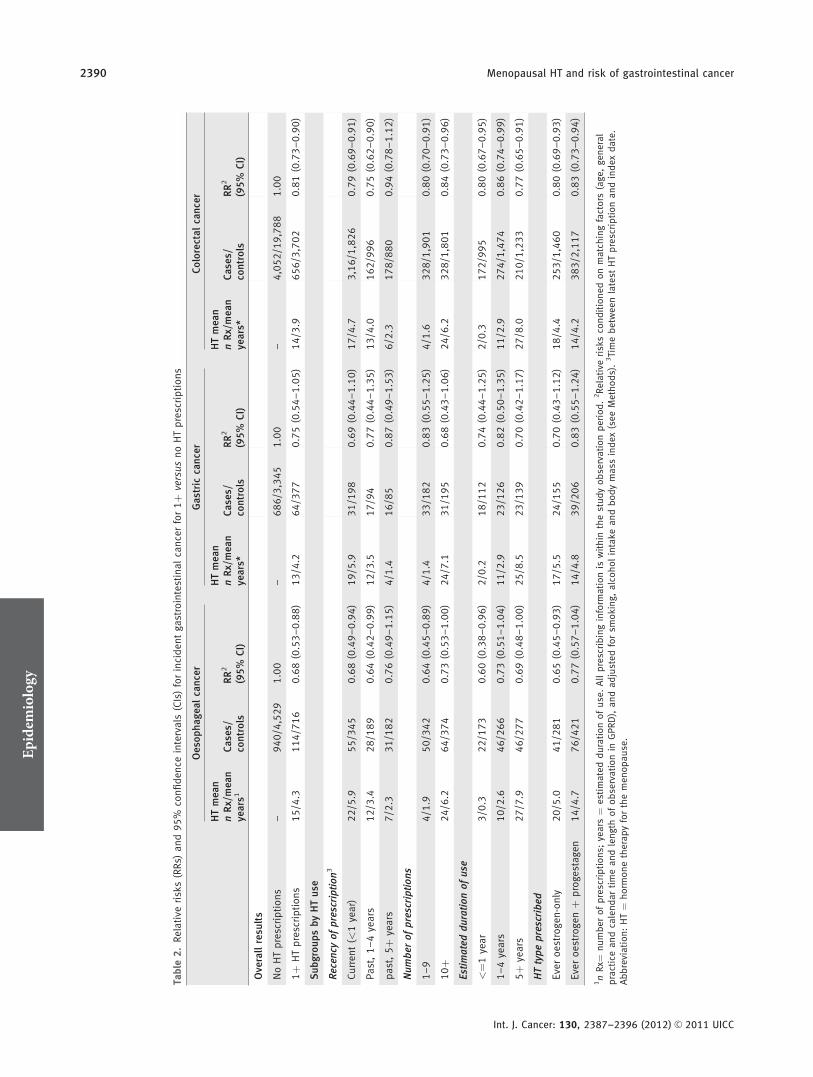
The RRs for colorectal cancer in ever compared withnever HT users in all 30 available studies, (6,256 exposedcases), are shown in Figure 2. The summary RR was 0.84,95% CI, 0.81–0.88 (p < 0.001), with no significant heteroge-neity in risk by study type but with some heterogeneityacross studies with retrospective recording of exposure. Justover half of the 30 studies provided information on risk ofcolorectal cancer in relation to use of HT by timing of use(current and past use, and short and long duration of use).Table 4 summarises the results of meta-analyses by type andtiming of HT use (study-specific results available on request).There is a suggestion of a greater reduction in risk of colo-rectal cancer in current compared to past users of HT, andfor long duration compared with shorter duration use; how-ever, the published results on this aspect of HT use includeonly about half of the available studies, and reported meas-ures of timing of use are limited (for example, past usersmay include varying proportions of those with very recentuse; and duration of use and time since last use are usuallystrongly related). In 16 studies, results were reported sepa-rately for cancers of the colon and rectum; summary RRs inrelation to ever vs. never use of any HT were very similar forthe two sites (colon: 0.85, 95% CI 0.81–0.90 and rectum:0.87, 95% CI 0.80–0.95).
For all of the meta-analyses, similar results were seenwhen the GPRD data were omitted.
Estimation of absolute risks
Incidence rates for women aged 50–64 years in North Amer-ica and Europe are typically three cases per 1,000 over 5years for colorectal cancer, and much lower at around 0.3cases per 1,000 over 5 years both for oesophageal and forgastric cancers.21 Applying the summary RRs from our meta-analyses to these rates, we estimate that the incidence ofcolorectal cancer in women aged 50–64 years would fall fromabout three cases per 1,000 women over 5 years to about 2.6cases per 1000 with 5 years’ use of HT. The correspondingincidence for all three gastrointestinal cancers combined isestimated at about 3.6 cases per 1,000 women per 5 years in
non-users of HT, and 2.9 cases per 1,000 over 5 years in HTusers.
DiscussionIn the large UK GPRD cohort, and in meta-analyses combin-ing findings from the GPRD with other published data, wefound reduced risks for oesophageal, gastric and colorectalcancers associated with the use of HT for the menopause. Inthe GPRD cohort, HT-related risks for each of the three can-cers did not vary materially by recency or duration of use ofHT, by HT type or between subgroups of women defined byage, smoking status, alcohol intake or body mass index.Meta-analyses for colorectal cancer produced summary RRswhich were similar for oestrogen-only and for oestrogen–pro-gestagen HT and for cancers of the colon and of the rectum,and some evidence of a lower risk in current than in pastHT users, and for long duration compared with short dura-tion HT use.
The GPRD study, with over 6,500 cases of gastrointestinalcancer, is the largest to date examining the risk of these can-cers in relation to HT use, and has reliable and completeprospectively recorded data on HT prescriptions. Participantswere followed for an average of about 7 years, and therewere enough cases and controls with 10 or more HT pre-scriptions over several years to allow analysis by number ofprescriptions and estimated duration of use. Data were avail-able for the majority of study participants on smoking, alco-hol intake and body mass index, factors that have been asso-ciated with gastrointestinal cancer risk. Adjustment for thesefactors minimised the scope for confounding by them, andsensitivity analyses that excluded participants with missingdata on any of the adjustment variables gave results virtuallyidentical to those for all women. In the UK, organisedscreening for colorectal cancer began in 2006, after the enddate for this study, and elective screening is rare, so althoughdata on cancer screening are not available, potential con-founding by screening is unlikely to be a problem.
Limitations of the study include the fact that the GPRDrecords prescriptions issued, but not whether the drugs were
Figure 1. Meta-analysis of results from published studies of ever vs. never use of any HT and risk of oesophageal and gastric cancers.
Adenoca ¼ adenocarcinoma. Dotted lines represent overall results for all women. *Includes 137 cases of adenocarcinoma of the stomach
and 25 cases of adenocarcinoma of the oesophagus.
Epidemiology
2392 Menopausal HT and risk of gastrointestinal cancer
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC
used. Not all women prescribed HT preparations will usethem, but this is less likely to be true among those withmany prescriptions or with prescriptions over several years.In a sensitivity analysis, the results were similar for HT expo-sure defined as two or more prescriptions, rather than one ormore as in the main analyses. Furthermore, low compliancewould result in dilution of the risk associated with HT use,and should not produce spurious associations. We had no in-
formation on HT prescriptions prior to an individual’s entryinto the GPRD, but results were similar when analyses wererestricted to women with their first prescription at least ayear after the start of their period of observation in theGPRD. The paucity of data on cancer histology meant thatwe were unable to examine HT-related risks separately forsquamous cell and adenocarcinoma of the oesophagus. Forcolorectal cancer, few major risk factors have been
Figure 2. Meta-analysis of results from published studies of ever vs. never use of any HT and risk of colorectal cancer. The dotted line
represents the overall result for all women. †Published results combined (see Methods). HERS ¼ Heart and Estrogen/progestin Replacement
Study.3 WHI ¼ Women’s Health Initiative trials.4,8 O ¼ oestrogen, P ¼ progestagen.
Epidemiology
Green et al. 2393
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

consistently identified, and data were not available in theGPRD dataset for some of potential relevance, such as past useof oral contraceptives, physical activity and diet.17,46,47 Con-founding by these or by other, unknown, risk factors couldpotentially affect the association seen with HT use. Use of aspi-rin and other non-steroidal anti-inflammatory drugs (NSAIDs)has been associated with reduced risk of colorectal cancer.48 Inthe GPRD analyses we found similar results in relation to HTuse for all three cancers in women who were and were not pre-scribed NSAIDs during the observation period, although inter-pretation of such results is not straightforward as prescriptionof NSAIDs is likely to be related to gastrointestinal symptoms.
Our meta-analyses showed similar results for HT-relatedrisk of each of the three gastrointestinal cancers from studiesof varying design, in varying settings and with varyingdegrees of adjustment (including, in many of the studies ofcolorectal cancer, adjustment for physical activity, for dietaryand reproductive factors and for use of aspirin). The possibil-ity that HT users may differ from non-users by unknownfactors related to gastrointestinal cancer risk cannot be ruledout in our and other observational studies: evidence fromrandomised trials is not available for the upper gastrointesti-nal cancers, and is very limited for colorectal cancer.
Various possible mechanisms for the observed reductionin risk of colorectal cancer with HT use have been suggested,including effects on bile acids, insulin and insulin-like growthfactors as well as direct effects on intestinal epithelium.49
Whether the mechanisms for oesophageal and gastric cancersare similar needs to be considered.
Different effects by different types of HT, which have beenfound for breast and endometrial cancers, were not seen eitherin the GPRD data for any of the three gastrointestinal cancers,or in our meta-analysis on colorectal cancer. The lack of a
strong effect of either recency or duration of use of HT ongastrointestinal cancer risk, both in our study and in previouspublished studies, is also in contrast to the HT-associated risksfor female reproductive cancers, where HT-associated risksappear to diminish soon after use ceases.1 If the associationbetween use of HT and risk of oesophageal, gastric and colo-rectal cancers is mediated by mechanisms involving female sexhormones, risk of these cancers might be expected to berelated to reproductive factors, such as parity and menopausalstatus, which are related to endogenous sex hormone levels;but evidence on the role of reproductive factors in influencingrisk of gastrointestinal cancers is inconsistent.17,50
Colorectal cancer and HT use are both relatively commonin middle-aged women in developed countries. We estimatedthat in women aged 50–64 years, use of HT would reducethe incidence of cancers of the oesophagus, stomach and col-orectum from 3.6 per 1,000 to 2.9 per 1,000 over 5 years.However, these results need to be considered in the contextof other effects of HT use: for instance, gastrointestinal can-cers are less common than breast cancer, where HT use isestimated to increase cancer incidence from 14 to 24 casesper 1,000 women aged 50–64 over 5 years.1
In conclusion, results from this prospective study andfrom meta-analyses of published data show reduced risks foroesophageal, gastric and colorectal cancers associated withuse of HT for the menopause.
AcknowledgementsAuthors are grateful to patients and General Practitioners participating inthe GPRD, and to GPRD staff for help and advice. All authors participatedin the design of the study, the interpretation of the analysis and the writingof the report. Analyses were performed by G.C.. All authors have seen andapproved the final version of the report. The current employers of two of theauthors (Amgen Ltd [A.R.], Takeda Ltd [L.W.]) played no role in this study.
References
1. Beral V; Million Women StudyCollaborators. Breast cancer and hormone-replacement therapy in the MillionWomen Study. Lancet 2003;362:419–27.
2. Medicines and Healthcare productsRegulatory Agency. Hormone replacement
therapy; updated advice. Drug SafetyUpdate 2007;1:2–4.
3. Hulley S, Furberg C, Barrett-Connor E,Cauley J, Grady D, Haskell W, Knopp R,Lowery M, Satterfield S, Schrott H,Vittinghoff E, Hunninghake D; HERSResearch Group. Noncardiovascular
disease outcomes during 6.8 years ofhormone therapy: Heart and Estrogen/progestin Replacement Studyfollow-up (HERS II). JAMA 2002;288:58–66.
4. Chlebowski RT, Wactawski-Wende J,Ritenbaugh C, Hubbell FA, Ascensao J,
Table 4. Summary RRs and 95% CIs from meta-analyses of HT use and colorectal cancer incidence, by type and timing of use
n studies n exposed cases Summary RR1 (95% CI)
Ever vs. never use, any HT (shown in Figure 2) 30 6,256 0.84 (0.81–0.88)
Ever vs. never use, Oestrogen-only HT 16 2,285 0.83 (0.79–0.86)
Ever vs. never use, Oestrogen þ Progestagen HT 17 1,355 0.81 (0.75–0.87)
Current use, any HT 18 2,362 0.77 (0.73–0.82)
Past use, any HT 17 2,107 0.89 (0.84–0.95)
Short duration use (� <5 years), any HT 19 2,264 0.85 (0.81–0.90)
Long duration use (� 5þ years), any HT 19 2,042 0.78 (0.74–0.83)
1Summary RR combining most-adjusted results from individual studies (see Methods).
Epidemiology
2394 Menopausal HT and risk of gastrointestinal cancer
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

Rodabough RJ, Rosenberg CA, Taylor VM,Harris R, Chen C, Adams-Campbell LL,White E; Women’s Health InitiativeInvestigators. Estrogen plus progestin andcolorectal cancer in postmenopausalwomen. N Engl J Med 2004;350:991–1004.
5. Farquhar C, Marjoribanks J, Lethaby A,Suckling JA, Lamberts Q. Long termhormone therapy for perimenopausal andpostmenopausal women. CochraneDatabase Syst Rev 2009;(2):CD004143.
6. Beral V, Banks E, Reeves G, Appleby P.Use of HRT and the subsequent risk ofcancer. J Epidemiol Biostat 1999;4:191–210;discussion 210–15.
7. Grodstein F, Newcomb PA, Stampfer MJ.Postmenopausal hormone therapy and therisk of colorectal cancer: a review andmeta-analysis. Am J Med 1999;106:574–82.
8. Ritenbaugh C, Stanford JL, Wu L, ShikanyJM, Schoen RE, Stefanick ML, Taylor V,Garland C, Frank G, Lane D, Mason E,McNeeley SG, et al.; Women’s HealthInitiative Investigators. Conjugated equineestrogens and colorectal cancer incidenceand survival: the Women’s HealthInitiative randomized clinical trial. CancerEpidemiol Biomarkers Prev 2008;17:2609–18.
9. Hildebrand JS, Jacobs EJ, Campbell PT,McCullough ML, Teras LR, Thun MJ,Gapstur SM. Colorectal cancer incidenceand postmenopausal hormone use by type,recency, and duration in cancer preventionstudy II. Cancer Epidemiol Biomarkers Prev2009;18:2835–41.
10. Tsilidis KK, Allen NE, Key TJ, SanjoaquinMA, Bakken K, Berrino F, Fournier A,Lund E, Overvad K, Olsen A, TjønnelandA, Byrnes G, et al. Menopausal hormonetherapy and risk of colorectal cancer in theEuropean Prospective Investigation intoCancer and Nutrition. Int J Cancer 2011;128:1881–9.
11. Gallus S, Bosetti C, Franceschi S, Levi F,Simonato L, Negri E, La Vecchia C.Oesophageal cancer in women: tobacco,alcohol, nutritional and hormonal factors.Br J Cancer 2001;85:341–5.
12. Lindblad M, Garcıa Rodrıguez LA,Chandanos E, Lagergren J. Hormonereplacement therapy and risks ofoesophageal and gastric adenocarcinomas.Br J Cancer 2006;94:136–41.
13. Freedman ND, Lacey JV, Jr, HollenbeckAR, Leitzmann MF, Schatzkin A, AbnetCC. The association of menstrual andreproductive factors with uppergastrointestinal tract cancers in the NIH-AARP cohort. Cancer 2010;116:1572–81.
14. Cronin-Fenton DP, Murray LJ, WhitemanDC, Cardwell C, Webb PM, Jordan SJ,Corley DA, Sharp L, Lagergren J; Barrett’sEsophagus, Adenocarcinoma
Consortium(BEACON) Investigators.Reproductive and sex hormonal factorsand oesophageal and gastric junctionadenocarcinoma: a pooled analysis. Eur JCancer 2010;46:2067–76.
15. Fernandez E, Gallus S, Bosetti C,Franceschi S, Negri E, La Vecchia C.Hormone replacement therapy and cancerrisk: a systematic analysis from a networkof case–control studies. Int J Cancer 2003;105:408–12.
16. Frise S, Kreiger N, Gallinger S, TomlinsonG, Cotterchio M. Menstrual andreproductive risk factors and risk forgastric adenocarcinoma in women: findingsfrom the canadian national enhancedcancer surveillance system. Ann Epidemiol2006;16:908–16.
17. Duell EJ, Travier N, Lujan-Barroso L,Boutron-Ruault MC, Clavel-Chapelon F,Palli D, Krogh V, Mattiello A, Tumino R,Sacerdote C, Rodriguez L, Sanchez-Cantalejo E, et al. Menstrual andreproductive factors, exogenous hormoneuse, and gastric cancer risk in a cohort ofwomen from the European ProspectiveInvestigation into Cancer and Nutrition.Am J Epidemiol 2010;172:1384–93.
18. Herrett E, Thomas SL, Schoonen WM,Smeeth L, Hall AJ. 2009 Validation andvalidity of diagnoses in the GeneralPractice Research Database: a systematicreview. Br J Clin Pharmacol 2010;69:4–14.
19. Green J, Czanner G, Reeves G, Watson J,Wise L, Beral V. Oral bisphosphonates andrisk of cancer of oesophagus, stomach, andcolorectum: case–control analysis within aUK primary care cohort. BMJ 2010;341:c4444.
20. Berrington A, Cox DR. Generalized leastsquares for the synthesis of correlatedinformation. Biostatistics 2003;4:423–31.
21. Curado M P, Edwards B, Shin HR, StormH, Ferlay J, Heanue M, Boyle P, eds.Cancer incidence in five continents, vol.IX.IARC Scientific Publications No. 160.Lyon: IARC, 2007.
22. Adami HO, Persson I, Hoover R, SchairerC, Bergkvist L. Risk of cancer in womenreceiving hormone replacement therapy.Int J Cancer 1989;44:833–9.
23. Folsom AR, Mink PJ, Sellers TA, HongCP, Zheng W, Potter JD. Hormonalreplacement therapy and morbidity andmortality in a prospective study ofpostmenopausal women. Am J PublicHealth 1995;85:1128–32.
24. Grodstein F, Martinez ME, Platz EA,Giovannucci E, Colditz GA, Kautzky M,Fuchs C, Stampfer MJ. Postmenopausalhormone use and risk for colorectal cancerand adenoma. Ann Intern Med 1998;128:705–12.
25. Paganini-Hill A. Estrogen replacementtherapy and colorectal cancer risk in
elderly women. Dis Colon Rectum 1999;42:1300–5.
26. Csizmadi I, Collet JP, Benedetti A, BoivinJF, Hanley JA. Defining hormonereplacement therapy in longitudinalstudies: impact on measures of effect.Pharmacoepidemiol Drug Saf 2004;13:215–25.
27. Hannaford P, Elliott A. Use of exogenoushormones by women and colorectal cancer:evidence from the Royal College of GeneralPractitioners’ Oral Contraception Study.Contraception 2005;71:95–8.
28. Kabat GC, Miller AB, Rohan TE. Oralcontraceptive use, hormone replacementtherapy, reproductive history and risk ofcolorectal cancer in women. Int J Cancer2008;122:643–6.
29. Johnson JR, Lacey JV, Jr, Lazovich D,Geller MA, Schairer C, Schatzkin A, FloodA. Menopausal hormone therapy and riskof colorectal cancer. Cancer EpidemiolBiomarkers Prev 2009;18:196–203.
30. Prentice RL, Pettinger M, Beresford SA,Wactawski-Wende J, Hubbell FA, StefanickML, Chlebowski RT. Colorectal cancer inrelation to postmenopausal estrogen andestrogen plus progestin in the Women’sHealth Initiative clinical trial andobservational study. Cancer EpidemiolBiomarkers Prev 2009;18:1531–7.
31. Delellis Henderson K, Duan L, Sullivan-Halley J, Ma H, Clarke CA, NeuhausenSL, Templeman C, Bernstein L.Menopausal hormone therapy use and riskof invasive colon cancer: the CaliforniaTeachers Study. Am J Epidemiol 2010;171:415–25.
32. Weiss NS, Daling JR, Chow WH. Incidenceof cancer of the large bowel in women inrelation to reproductive and hormonalfactors. J Natl Cancer Inst 1981;67:57–60.
33. Potter JD, McMichael AJ. Large bowelcancer in women in relation toreproductive and hormonal factors: a case–control study. J Natl Cancer Inst 1983;71:703–9.
34. Furner SE, Davis FG, Nelson RL, HaenszelW. A case–control study of large bowelcancer and hormone exposure in women.Cancer Res 1989;49:4936–40.
35. Peters RK, Pike MC, Chang WW, MackTM. Reproductive factors and coloncancers. Br J Cancer 1990;61:741–8.
36. Newcomb PA, Storer BE. Postmenopausalhormone use and risk of large-bowelcancer. J Natl Cancer Inst 1995;87:1067–71.
37. Kampman E, Potter JD, Slattery ML, CaanBJ, Edwards S. Hormone replacementtherapy, reproductive history, and coloncancer: a multicenter, case–control study inthe United States. Cancer Causes Control1997;8:146–58.
Epidemiology
Green et al. 2395
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC

38. Fernandez E, La Vecchia C, Braga C,Talamini R, Negri E, Parazzini F,Franceschi S. Hormone replacementtherapy and risk of colon and rectalcancer. Cancer Epidemiol Biomarkers Prev1998;7:329–33.
39. Jacobs EJ, White E, Weiss NS, HeckbertSR, LaCroix A, Barlow WE. Hormonereplacement therapy and colon canceramong members of a health maintenanceorganization. Epidemiology 1999;10:445–51.
40. Prihartono N, Palmer JR, Louik C, ShapiroS, Rosenberg L. A case–control study ofuse of postmenopausal female hormonesupplements in relation to the risk of largebowel cancer. Cancer Epidemiol BiomarkersPrev 2000;9:443–7.
41. Dinger JC, Heinemann LA, Mohner S,Thai do M, Assmann A. Colon cancer riskand different HRT formulations: a case–control study. BMC Cancer 2007;7:76.
42. Campbell PT, Newcomb P, Gallinger S,Cotterchio M, McLaughlin JR. Exogenoushormones and colorectal cancer risk inCanada: associations stratified by clinically
defined familial risk of cancer. CancerCauses Control 2007;18:723–33.
43. Newcomb PA, Zheng Y, Chia VM,Morimoto LM, Doria-Rose VP, TempletonA, Thibodeau SN, Potter JD. Estrogen plusprogestin use, microsatellite instability, andthe risk of colorectal cancer in women.Cancer Res 2007;67:7534–9.
44. Rennert G, Rennert HS, Pinchev M, LavieO, Gruber SB. Use of hormone replacementtherapy and the risk of colorectal cancer. JClin Oncol 2009;27:4542–7.
45. Hoffmeister M, Raum E, Krtschil A,Chang-Claude J, Brenner H. No evidencefor variation in colorectal cancer riskassociated with different types ofpostmenopausal hormone therapy. ClinPharmacol Ther 2009;86:416–24.
46. Harriss DJ, Atkinson G, Batterham A,George K, Cable NT, Reilly T, Haboubi N,Renehan AG; Colorectal Cancer, Lifestyle,Exercise And Research Group. Lifestylefactors and colorectal cancer risk (2): asystematic review and meta-analysis ofassociations with leisure-time physical
activity. Colorectal Dis 2009;11:689–701.
47. Gonzalez CA, Riboli E. Diet and cancerprevention: contributions from theEuropean Prospective Investigation intoCancer and Nutrition (EPIC) study. Eur JCancer 2010;46:2555–62.
48. Rothwell PM, Wilson M, Elwin CE,Norrving B, Algra A, Warlow CP, MeadeTW. Long-term effect of aspirin oncolorectal cancer incidence andmortality: 20-year follow-up of fiverandomised trials. Lancet 2010;376:1741–50.
49. Gunter MJ, Hoover DR, Yu H,Wassertheil-Smoller S, Rohan TE, MansonJE, Howard BV, Wylie-Rosett J, AndersonGL, Ho GY, Kaplan RC, Li J. Insulin,insulin-like growth factor-I, endogenousestradiol, and risk of colorectal cancer inpostmenopausal women. Cancer Res 2008;68:329–37.
50. Pike MC, Pearce CL, Wu AH. Preventionof cancers of the breast, endometrium andovary. Oncogene 2004;23:6379–91.
Epidemiology
2396 Menopausal HT and risk of gastrointestinal cancer
Int. J. Cancer: 130, 2387–2396 (2012) VC 2011 UICC