Embed Size (px)
Citation preview
Merced County Community Health Improvement Plan
2017 - 2022
Merced County Community Health Improvement Plan
Table of Contents
Executive Summary……………………………………………………………………………………………………………………………..….3
Acknowledgements…………………………………………………………………………………………………………………………………4
Section 1: Background, Context, and Results..………………………..….…………....................................................5
Section 2: Planning for Success.……………………………………………………………………………………………………………....9
Section 3: Community Engagement Approach……………………………………………………………………………………....13
Section 4: Ranked Health Priorities……………………………………………………………………………..……………………….. 22
Section 5: Summary of Community Discussions on the Health Priorities ...……..…………………………………….24
Section 6: Introduction to the Work Plan - Goals, Objectives, & Strategies………………………….…..…………...30
Work Plan…………………………………………………….……………………………………………………………………...31
Appendices…………………………..………………………………………………………………………………………………………………. 45
Appendix A: Community Engagement Handouts………………………………………………………………...46
Appendix B: List of Community Outreach………………………….…………………………………………………48
Appendix C: Top Health Priorities from Community Meetings ……………………………..…………….49
February 2017 | 2

Merced County Community Health Improvement Plan
Executive Summary
Through collaborative efforts with community partners, the Merced County Department of Public Health has developed the Merced County Community Health Improvement Plan (CHIP) which will serve as a blueprint for collective action to address health disparities and to promote health equity with the goal of health and wellness for all county residents.
Health and wellness cannot be realized through medical care alone. Quality, accessible medical care is an important component of a healthy community and is identified as one of the CHIP’s top three health priorities. But, the framework to achieve health and wellness must also be present at home, in neighborhoods and communities, at work, and at school.
To build that framework, the social determinants of health – safe, violence-free environments, affordable housing, adequate education and training, and a broad base of livable-wage employment opportunities - must be available. Health and wellness can be attained only when all residents have an equal chance to lead healthy lives regardless of race, ethnicity, sexual orientation, gender identity, socio-economic conditions, or immigration status.
The CHIP’s work plan is meant to support a variety of actions by a wide range of partners. With a focus on policy, systems, and environmental strategies, the work plan’s intent is to establish and strengthen factors that influence health and wellness in our community.
The Merced County Community Health Improvement Plan reflects the engagement and efforts of many community residents and organizational partners in their ongoing work to improve health and wellness for all Merced County residents.
Thank you for your commitment to making Merced County a healthy place for all. Kathleen Grassi, RD, MPH Director Merced County Department of Public Health February 17, 2017
February 2017 | 3
Merced County Community Health Improvement Plan
Acknowledgements The development of the Merced County Community Health Improvement Plan was accomplished through the contributions of many. In addition to those who are acknowledged below, I want to sincerely thank the many Merced County residents who participated in community meetings, visited our “traveling booth” and helped us to identify the health priorities found herein. Dedicated organization partners formed the Accreditation External Task Force which was charged with developing, reviewing, and commenting at all stages of the CHIP development. Members of the Task Force represented the following organizations: • Building Healthy Communities, Merced • Livingston Community Health
• Central California Alliance for Health • Merced County Department of Behavioral Health and Recovery Services
• Dignity Health Mercy Medical Centers Merced • Merced County Department of Public Health
• First 5 Merced County • Sutter Health Memorial Hospital Los Banos
• Golden Valley Health Centers • United Way Merced County
• University of California, Merced
Resource Development Associates, a California-based consulting firm, was retained to assist the Task Force members in the formulation of materials and messaging that formed the backbone of the CHIP community engagement process. RDA was also instrumental in describing the activities and results of the community engagement process, as well as the collaborative strategy sessions, incorporated in this document. The photographs of Merced County residents, which were used on the front and back covers of the CHIP, were taken by Kara Brodgesell, Photographer. Finally, I want to acknowledge Merced County Public Health Department staff who have been engaged in every aspect of the CHIP – from the vision to the plan – and who, with many community partners, will take this plan into action. For more information on the CHIP and current implementation efforts, contact: Kristynn Sullivan, Epidemiologist and Accreditation Coordinator at [email protected] 209-381-1200.
February 2017 | 4

Merced County Community Health Improvement Plan
Section I. Background, Context, and Results
The Merced County Department of Public Health (MCDPH) is dedicated to protecting and improving community members’ health and long-term wellbeing. In order to better understand and meet the County’s diverse health needs, MCDPH, in collaboration with an Accreditation External Task Force of community partners, completed a Community Health Assessment (CHA) to provide an overview of the county’s health status and leading health concerns. This CHA was produced through a two-year process of data collection and analysis, supplemented by key informant interviews, and a random-digit-dial survey of residents gleaned from local hospital community health assessments.
Using the CHA as a starting point, MCDPH carried out a community engagement process to develop strategies to address countywide health issues though a Community Health Improvement Plan (CHIP). The CHIP will be used by a range of community agencies and organizations, in partnership with MCDPH, to roll-out CHIP strategies. The CHA and CHIP are also prerequisite documents for MCDPH to be eligible for accreditation through the National Public Health Accreditation Board (PHAB).
Section 1 of the CHIP describes MCDPH’s planning approach to ensure success. Section 2 describes the community engagement activities, including the facilitation process used to guide community stakeholders in the selection of priority health issues, along with a summary of meeting locations and participant characteristics. Section 3 presents the ranked health priorities that emerged from the community engagement process. Section 4 synthesizes the themes that arose in the community discussions around health priorities in Merced County. Section 5 presents the CHIP goals, objectives, and strategies developed through planning sessions with MCDPH and community partners.
Merced County Department of Public Health
Vision
Merced County: A healthy place for all.
Mission
To promote, protect, and preserve healthy living and safe environments.
Values
Equity: Recognizing disparities and having a purposeful commitment to improve social conditions.
Innovation: Creative, data-driven solutions that make a difference.
Integrity: Honest, respectful, and non-judgmental with high ethical standards.
Leadership: Trusted key partner, creating change through inclusive collaboration.
Quality: Promoting, expecting, and maintaining excellence through an expert workforce.
Responsiveness: Agile and able to adapt to community needs.
Service: Committed to beneficial system change, education, advocacy, and prudent regulation.
Stewardship: Responsible and transparent management of resources.
February 2017 | 5
Merced County Community Health Improvement Plan
Through collaborative efforts with community partners, MCDPH strives to make Merced County a safer and healthier place for residents to live, work, and play. MCDPH understands that health and wellness cannot be realized by medical care alone. Instead, health and wellness begins in our homes, neighborhoods and workplaces, in our school systems, and at our community parks and playgrounds. Keeping this in mind as an organizing principle to move towards a healthier community, the CHIP intentionally incorporates strategies around the broader social and environmental issues that impact the public’s health.
Factors that contribute to health inequities in Merced County include, but are not limited to, low educational attainment and high rates of unemployment; poverty; and inequitable access to healthy foods, safe public spaces, and adequate housing. Additionally, health disparities that are seen among racial, ethnic, and marginalized social groups point to underlying systemic biases that constitute a root cause of poor health outcomes. Using the Community Health Assessment as a foundation, and ensuring community engagement in the development of the CHIP, MCDPH implemented a process to bring forth strategies which move beyond interventions that target individual health behaviors to strategies addressing the underlying factors that affect the community’s health.
Each objective outlined in the CHIP incorporates one or more of the identified socio-environmental concerns and provides an upstream or policy level intervention to promote equity and quality of life for all of Merced County’s residents.
Focus on Health Equity and the Social Determinants of Health
February 2017 | 6
Merced County Community Health Improvement Plan
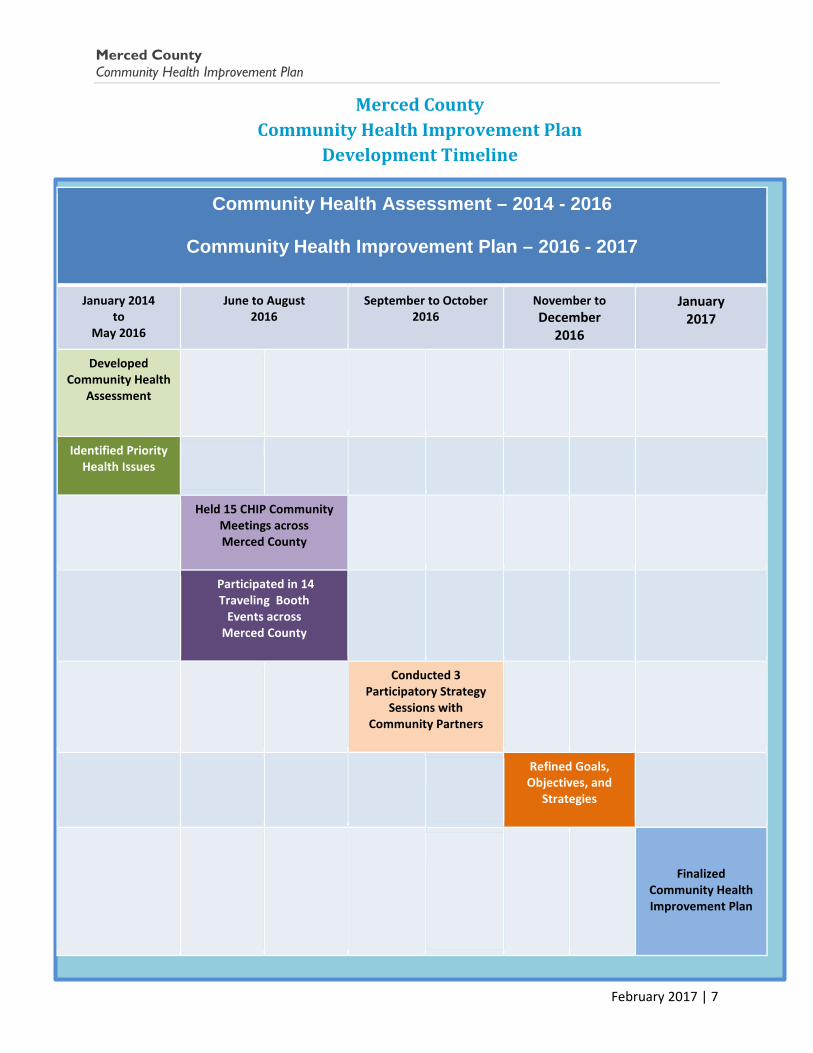
Community Health Assessment – 2014 - 2016
Community Health Improvement Plan – 2016 - 2017
January 2014 to
May 2016
June to August 2016
September to October 2016
November to December
2016 January
2017
Developed Community Health
Assessment
Identified Priority Health Issues
Held 15 CHIP Community Meetings across Merced County
Participated in 14 Traveling Booth
Events across Merced County
Conducted 3 Participatory Strategy
Sessions with Community Partners
Refined Goals, Objectives, and
Strategies
Finalized Community Health Improvement Plan
Merced County Community Health Improvement Plan
Development Timeline
February 2017 | 7
Merced County Community Health Improvement Plan
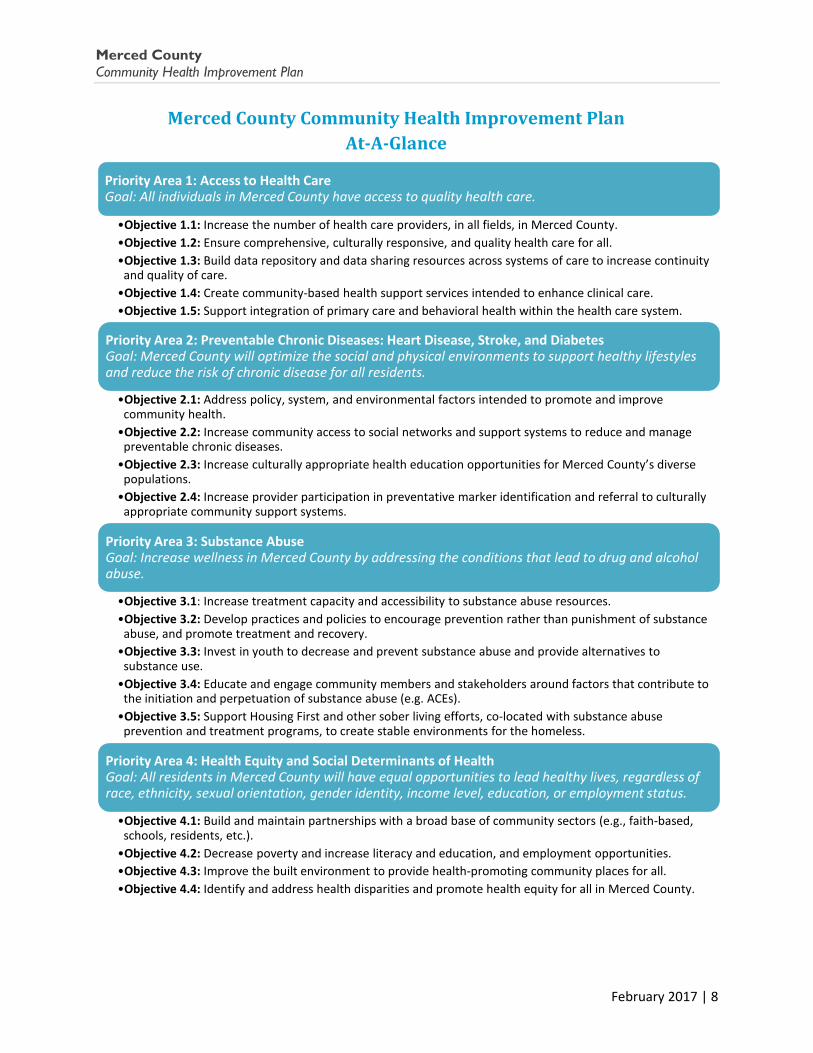
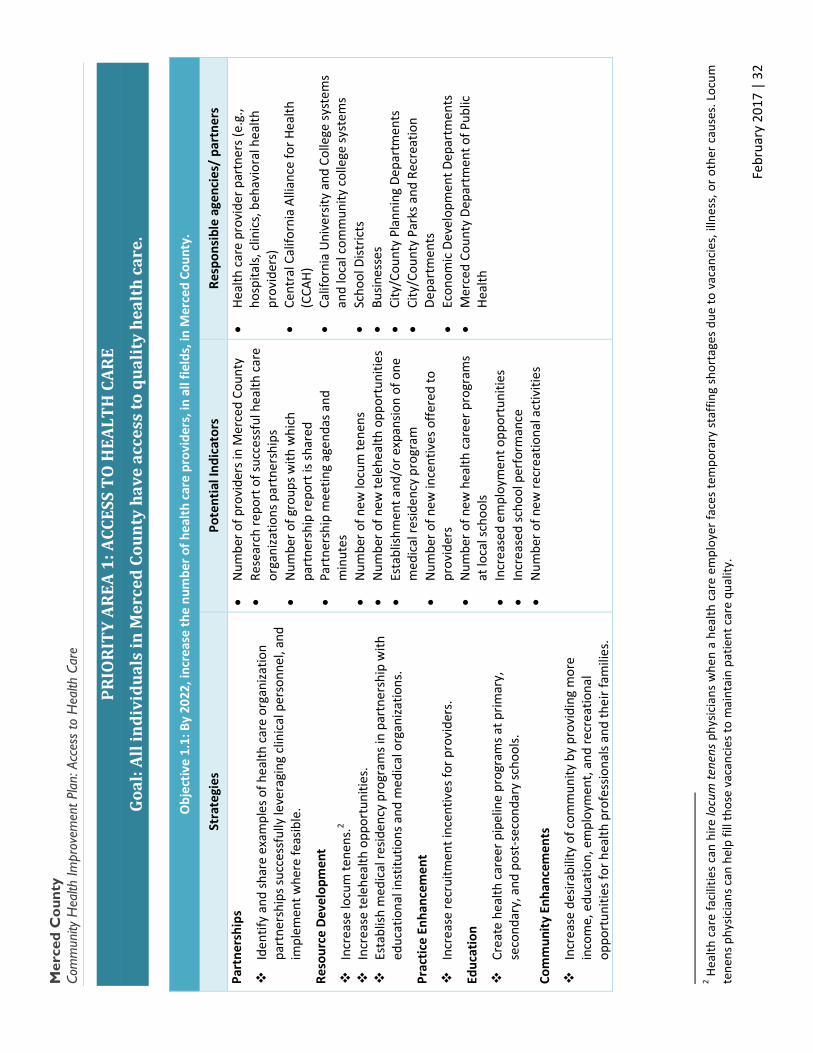
Priority Area 1: Access to Health Care Goal: All individuals in Merced County have access to quality health care.
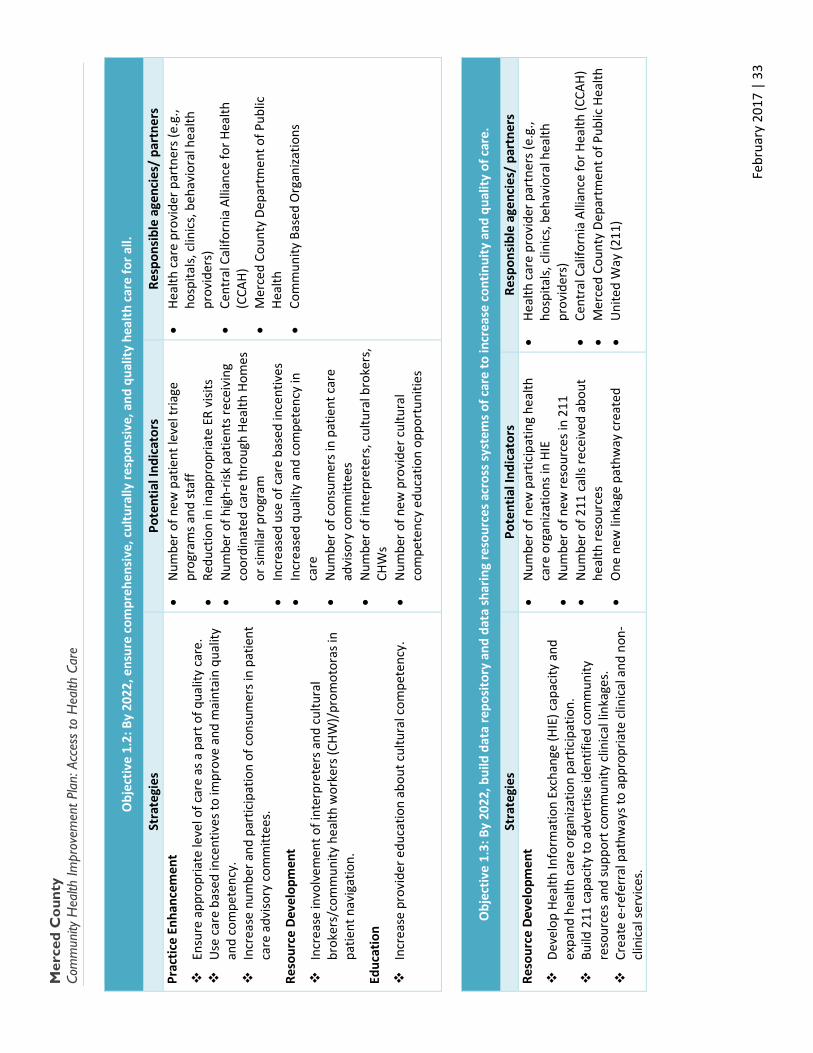
•Objective 1.1: Increase the number of health care providers, in all fields, in Merced County. •Objective 1.2: Ensure comprehensive, culturally responsive, and quality health care for all. •Objective 1.3: Build data repository and data sharing resources across systems of care to increase continuity
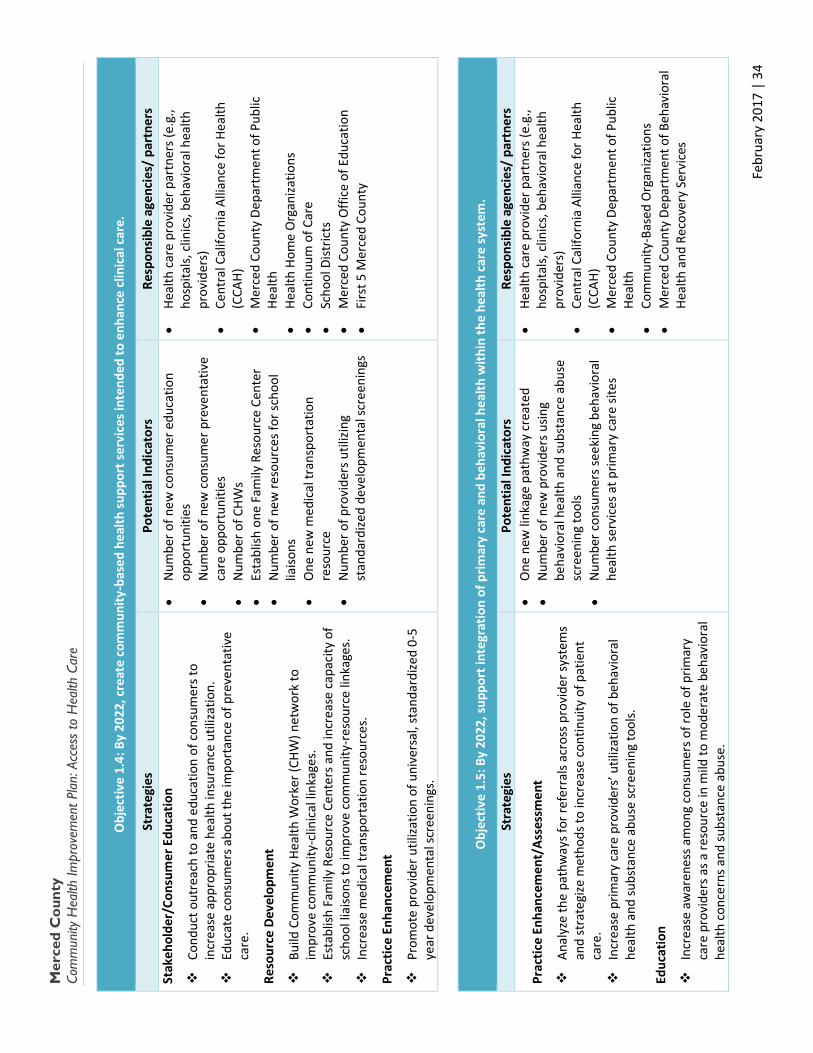
and quality of care. •Objective 1.4: Create community-based health support services intended to enhance clinical care. •Objective 1.5: Support integration of primary care and behavioral health within the health care system.
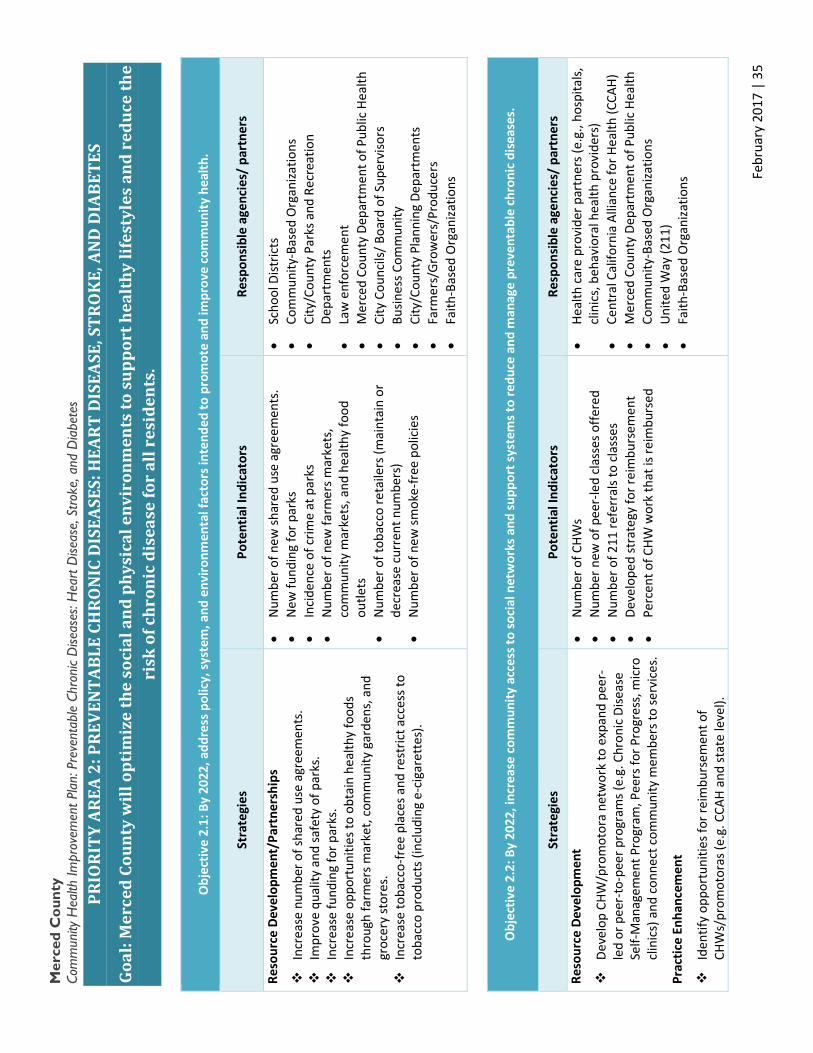
Priority Area 2: Preventable Chronic Diseases: Heart Disease, Stroke, and Diabetes Goal: Merced County will optimize the social and physical environments to support healthy lifestyles and reduce the risk of chronic disease for all residents.
•Objective 2.1: Address policy, system, and environmental factors intended to promote and improve community health. •Objective 2.2: Increase community access to social networks and support systems to reduce and manage
preventable chronic diseases. •Objective 2.3: Increase culturally appropriate health education opportunities for Merced County’s diverse
populations. •Objective 2.4: Increase provider participation in preventative marker identification and referral to culturally
appropriate community support systems.
Priority Area 3: Substance Abuse Goal: Increase wellness in Merced County by addressing the conditions that lead to drug and alcohol abuse.
•Objective 3.1: Increase treatment capacity and accessibility to substance abuse resources. •Objective 3.2: Develop practices and policies to encourage prevention rather than punishment of substance
abuse, and promote treatment and recovery. •Objective 3.3: Invest in youth to decrease and prevent substance abuse and provide alternatives to
substance use. •Objective 3.4: Educate and engage community members and stakeholders around factors that contribute to
the initiation and perpetuation of substance abuse (e.g. ACEs). •Objective 3.5: Support Housing First and other sober living efforts, co-located with substance abuse
prevention and treatment programs, to create stable environments for the homeless.
Priority Area 4: Health Equity and Social Determinants of Health Goal: All residents in Merced County will have equal opportunities to lead healthy lives, regardless of race, ethnicity, sexual orientation, gender identity, income level, education, or employment status.
•Objective 4.1: Build and maintain partnerships with a broad base of community sectors (e.g., faith-based, schools, residents, etc.). •Objective 4.2: Decrease poverty and increase literacy and education, and employment opportunities. •Objective 4.3: Improve the built environment to provide health-promoting community places for all. •Objective 4.4: Identify and address health disparities and promote health equity for all in Merced County.
Merced County Community Health Improvement Plan At-A-Glance
February 2017 | 8
Merced County Community Health Improvement Plan
Section 2: Planning for Success
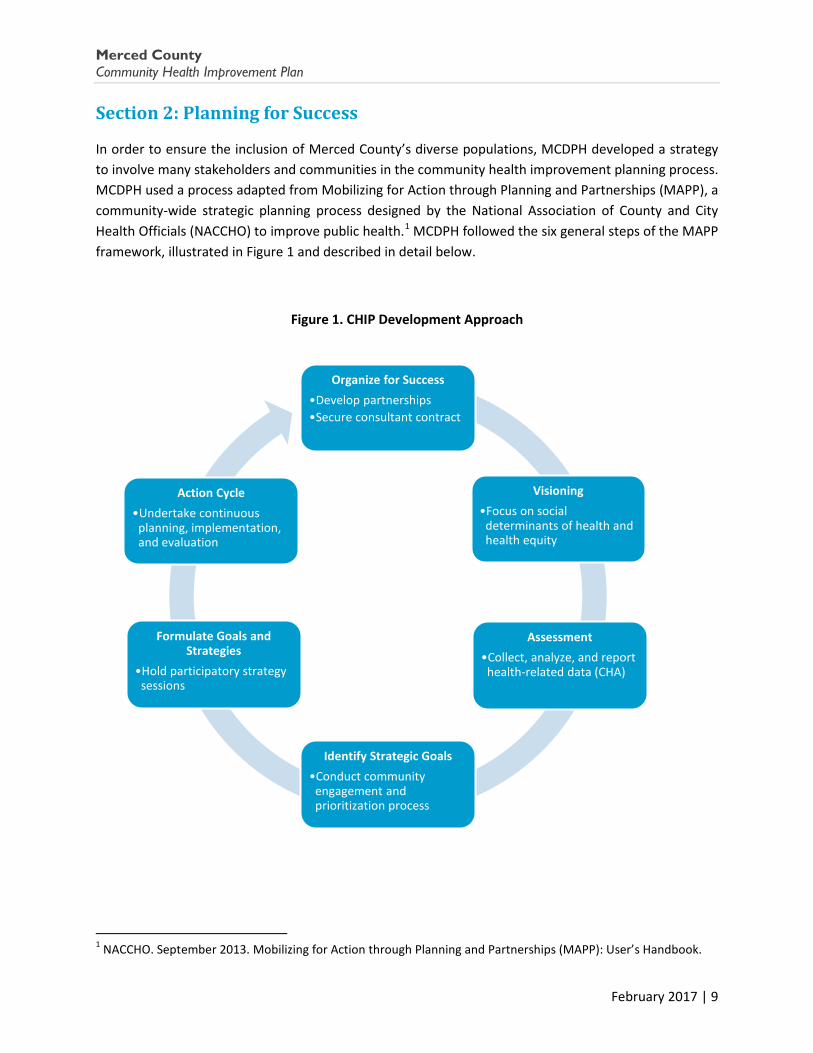
In order to ensure the inclusion of Merced County’s diverse populations, MCDPH developed a strategy to involve many stakeholders and communities in the community health improvement planning process. MCDPH used a process adapted from Mobilizing for Action through Planning and Partnerships (MAPP), a community-wide strategic planning process designed by the National Association of County and City Health Officials (NACCHO) to improve public health.1 MCDPH followed the six general steps of the MAPP framework, illustrated in Figure 1 and described in detail below.
Figure 1. CHIP Development Approach
1 NACCHO. September 2013. Mobilizing for Action through Planning and Partnerships (MAPP): User’s Handbook.
Organize for Success •Develop partnerships •Secure consultant contract
Visioning •Focus on social
determinants of health and health equity
Assessment •Collect, analyze, and report
health-related data (CHA)
Identify Strategic Goals •Conduct community
engagement and prioritization process
Formulate Goals and Strategies
•Hold participatory strategy sessions
Action Cycle •Undertake continuous
planning, implementation, and evaluation
February 2017 | 9
Merced County Community Health Improvement Plan
1. Organize for Success. In early 2014, MCDPH convened a task force of community partners to start the process of developing the CHA and the CHIP. This Accreditation External Task Force met monthly to discuss topics related to community health assessment and improvement. The Accreditation External Task Force developed the scope of work for a vendor to take the results of the CHA, when completed, to the community for discussion, facilitate a process for the community to prioritize the health concerns identified in the CHA, and summarize these findings in a CHIP. MCDPH contracted with Resource Development Associates (RDA), a California-based consulting firm, to assist with these tasks.
2. Visioning. In this step, MCDPH and the Accreditation External Task Force developed a vision for the project that focused on health equity and social determinants of health, in alignment with MCDPH’s emphasis on addressing structural factors influencing health. This approach was selected after a countywide pattern of high mortality rates paired with low prevalence rates was identified across several health conditions. Rather than indicating true low prevalence, this suggests that Merced County residents, in particular within communities of color, are diagnosed at later stages of disease, leading to higher mortality rates. As a result of this visioning process, the CHA included not only physical health conditions, but also focused heavily on broader environmental factors such as income, education, employment, housing, and violence.
3. Assessment. To develop the CHA, MCDPH gathered both quantitative and qualitative data on the community’s health status through a two-year process of data collection and analysis, which included publicly available population data as well as survey and interview data collected by Professional Research Consultants (PRC) for Dignity Health’s 2015 Community Health Needs Assessment. While the development of the CHA was spearheaded by MCDPH, several drafts were presented to the Accreditation External Task Force for review and discussion. The CHA was finalized and made publicly available in 2016.
4. Identify Strategic Goals. Using the CHA, MCDPH developed a community engagement process to determine the strategic issues that should be addressed in order to improve health and wellness in Merced County according to the Accreditation External Task Force’s vision. Considering prioritization criteria developed by NACCHO, including size of the issue, seriousness of the issue, trends over time, demographic disparities, and feasibility and resources, Task Force members prioritized the broad sections of the CHA (e.g., Leading Causes of Death, Mental Health, Infectious Disease, etc.) and the chapters within each section (e.g., Heart Disease, Diabetes, Depression, etc.). Rankings were
Accreditation External Task Force Members
• Building Healthy Communities, Merced • Central California Alliance for Health • Dignity Health Mercy Medical Centers
Merced • First 5 Merced County • Golden Valley Health Centers • Livingston Community Health • Merced County Department of Behavioral
Health and Recovery Services (formerly the Mental Health Department)
• Merced County Department of Public Health • Sutter Health Memorial Hospital Los Banos • United Way-Merced County • University of California, Merced
February 2017 | 10

Merced County Community Health Improvement Plan
averaged, and priorities from the top rankings of each major section were selected (i.e. at least one topic was chosen from each major section). The Accreditation External Task Force vetted the final selections and determined the following 10 priority areas to bring to the community for further discussion and prioritization. (See Section 3 for details on the community engagement process.)
Health Conditions Social Determinants of Health
Hearth Disease and Stroke Access to Care
Chronic Lung Disease Income, Education, and Employment
Diabetes
Healthy Foods and Physical Activity
Drug and Alcohol Abuse Injury and Violence
Sexually Transmitted Diseases Housing and Homelessness
5. Formulate Goals and Strategies. After an extensive countywide community engagement process in July and August 2016, MCDPH held three participatory strategizing sessions in September and October 2016 with community partners including members of the Accreditation External Task Force, the Merced County Health Care Consortium and other organizations to assure broad representation.
In September, participants split into workgroups based on each of the identified health priority areas and used an interactive and sequential process of developing a goal statement, four to six
CHIP Strategy Session Participating Agencies – September 22, 2016 Session
• Franklin-Beachwood Committee for Improvement
• BHC Health Equity Project
• Building Healthy Communities, Merced
• Central California Alliance for Health
• City of Gustine
• Dignity Health Mercy Medical Centers Merced
• First 5 Merced County
• Golden Valley Health Centers
• Livingston Community Health
• Merced County Behavioral Health and Recovery Services
• Merced County Board of Supervisors
• Merced County Department of Public Health
• Merced County Human Services Agency
• Merced County Office of Education
• Merced County Sheriff's Department
• Sutter Health Memorial Hospital Los Banos
• The California Endowment
• University of California Merced
• University of California Merced-Blum Center for Developing Economies
February 2017 | 11
Merced County Community Health Improvement Plan
objectives for each goal, and up to three strategies for each objective. MCDPH then met with the External Task Force on October 27, 2016 to validate and refine the goals and objectives.
Also, on October 27, 2016, there was a strategy session with members of the Merced County Health Care Consortium. The Consortium membership includes 91 e-list invitees from local hospitals, county departments (public health, human services, and behavioral health), health plan organizations (Medi-Cal Managed Care plan, Covered CA and one of its plans, Blue Cross), safety net clinics, community-based organizations, educational institutions, representatives from state and federal elected officials’ offices and interested non-affiliated individuals.
Participants again split into groups based on the health priority areas and brainstormed strategies for policy, system, and environmental changes that would need to be in place to support the CHIP’s goals and objectives.
Following the strategy sessions, MCDPH refined the goals, objectives, and strategies to ensure the CHIP maintained a focus on social determinants of health and reflected a comprehensive plan of action with strategies in the following categories:
CHIP Strategic Action Categories Partnerships Evaluation
Communication Assessment
Policy Development/Implementation Youth/Adult Engagement
Resource Development Stakeholder/Consumer Education
Practice Enhancement Other 6. Action Cycle. Following the development of the CHIP, MCDPH and its community partners will
undertake continuous planning, implementation, and evaluation to ensure that the community achieves the goals set out in the CHIP.
MCDPH is also engaged in a concurrent strategic planning effort, through a Quality Oversight Group, which will develop action plans for the strategies identified in the CHIP that will guide the Department’s efforts over the next five years.
The CHIP will inform new and ongoing collaborative efforts such as a coalition to address health equity co-facilitated by the Merced County Departments of Behavioral Health and Recovery Services and MCDPH (new); ongoing collaborations to address preventable chronic diseases through MCDPH’s Partnerships to Improve Community Health and Merced County Accountable Community For Health (ongoing); and cooperative efforts to improve access to health care as well as quality health care delivery through MCDPH’s Whole Health Partnership and Merced County Accountable Community For Health efforts (ongoing).
February 2017 | 12

Merced County Community Health Improvement Plan
Section 3: Community Engagement Approach
To ensure that a broad representation of county residents had an opportunity to contribute to the CHIP, MCDPH planned a series of community meetings and identified outreach events where the top 10 health conditions and social determinants of health issues from the CHA would be presented.
MCDPH contracted with RDA to develop visually appealing graphics and materials depicting the 10 priority health issues. RDA created representative icons for each health issue to allow for quick and easy identification by community members, taking into account concerns about literacy and cultural differences among Merced County’s diverse residents (see example in Figure 3 and full materials in Appendix A). RDA then developed PowerPoint presentations for the community meetings. MCDPH and RDA used these materials to facilitate the prioritization of health issues at two types of community engagement events: 1) community meetings; and 2) a traveling booth. Each of these approaches is described below.
Merced County Community Health Improvement Planning Session October 27, 2016
Figure 2. CHIP Participatory Strategy Sessions - September and October 2016
Merced County Community Health Improvement Planning Session September 22, 2016
February 2017 | 13
Merced County Community Health Improvement Plan
Community Meetings
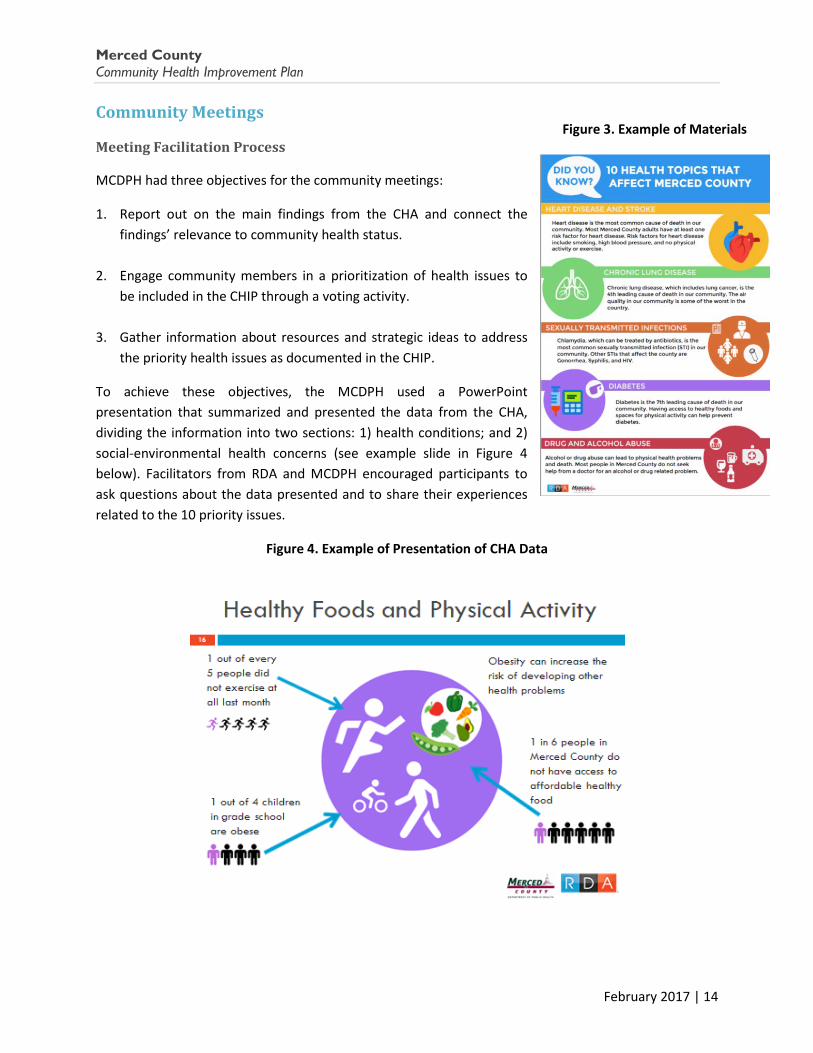
MCDPH had three objectives for the community meetings:
1. Report out on the main findings from the CHA and connect the findings’ relevance to community health status.
2. Engage community members in a prioritization of health issues to be included in the CHIP through a voting activity.
3. Gather information about resources and strategic ideas to address
the priority health issues as documented in the CHIP.
To achieve these objectives, the MCDPH used a PowerPoint presentation that summarized and presented the data from the CHA, dividing the information into two sections: 1) health conditions; and 2) social-environmental health concerns (see example slide in Figure 4 below). Facilitators from RDA and MCDPH encouraged participants to ask questions about the data presented and to share their experiences related to the 10 priority issues.
Figure 4. Example of Presentation of CHA Data
Figure 3. Example of Materials
February 2017 | 14

Merced County Community Health Improvement Plan
Next, participants had the opportunity to vote for their first and second priorities in each section: health conditions and social determinants of health. The facilitators used an electronic voting tool, iclicker, to allow for an interactive and real-time voting process. (see Figure 5).
Figure 5. Voting Exercise with iclicker
Following the voting activity, the facilitators led a discussion about: 1) services and resources that currently exist or could be expanded upon to effectively address the priority health issues; and 2) services and resources that do not exist but would be beneficial in addressing the priority health issues.
Through the community meetings, MCDPH aimed to gather feedback from stakeholders at various locations across the widespread geographic area of Merced County, as well as from vulnerable populations and the county’s major ethnic communities. For geographic representation, MCDPH held one or two meetings in each of the five county supervisorial districts. Additionally, five population-specific meetings and two meetings with health care professionals were also held (see Figure 6 below).
February 2017 | 15
Merced County Community Health Improvement Plan
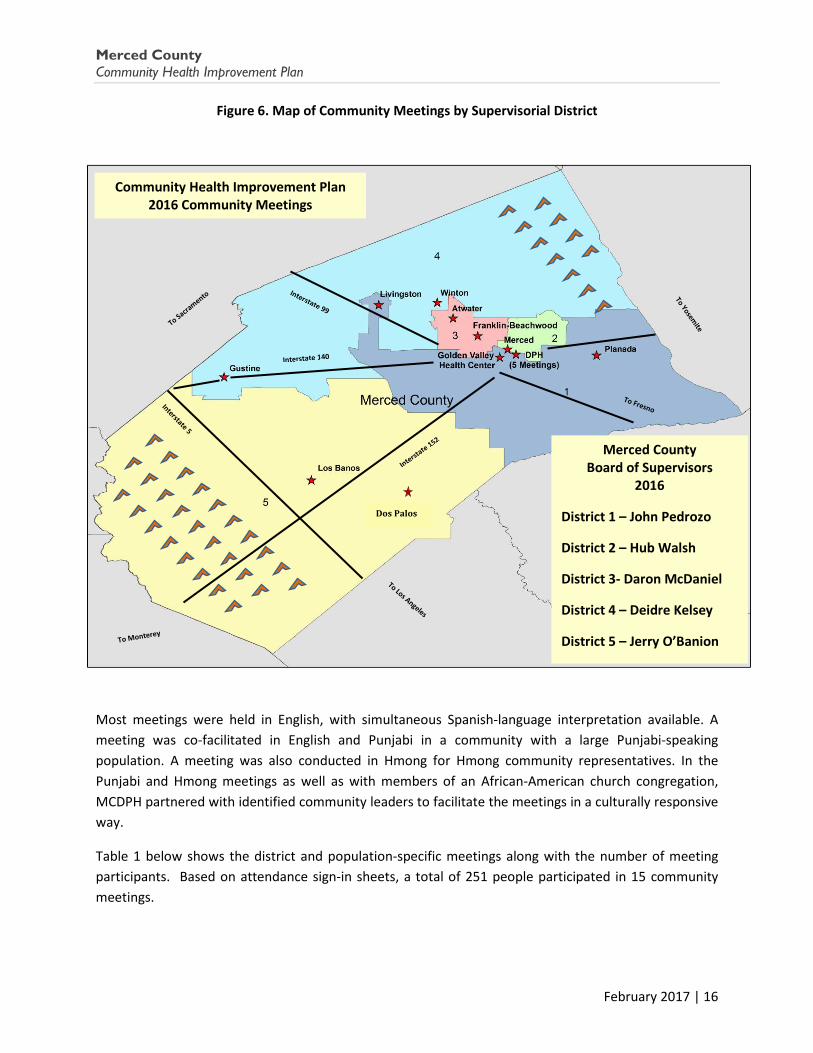
Figure 6. Map of Community Meetings by Supervisorial District
Most meetings were held in English, with simultaneous Spanish-language interpretation available. A meeting was co-facilitated in English and Punjabi in a community with a large Punjabi-speaking population. A meeting was also conducted in Hmong for Hmong community representatives. In the Punjabi and Hmong meetings as well as with members of an African-American church congregation, MCDPH partnered with identified community leaders to facilitate the meetings in a culturally responsive way.
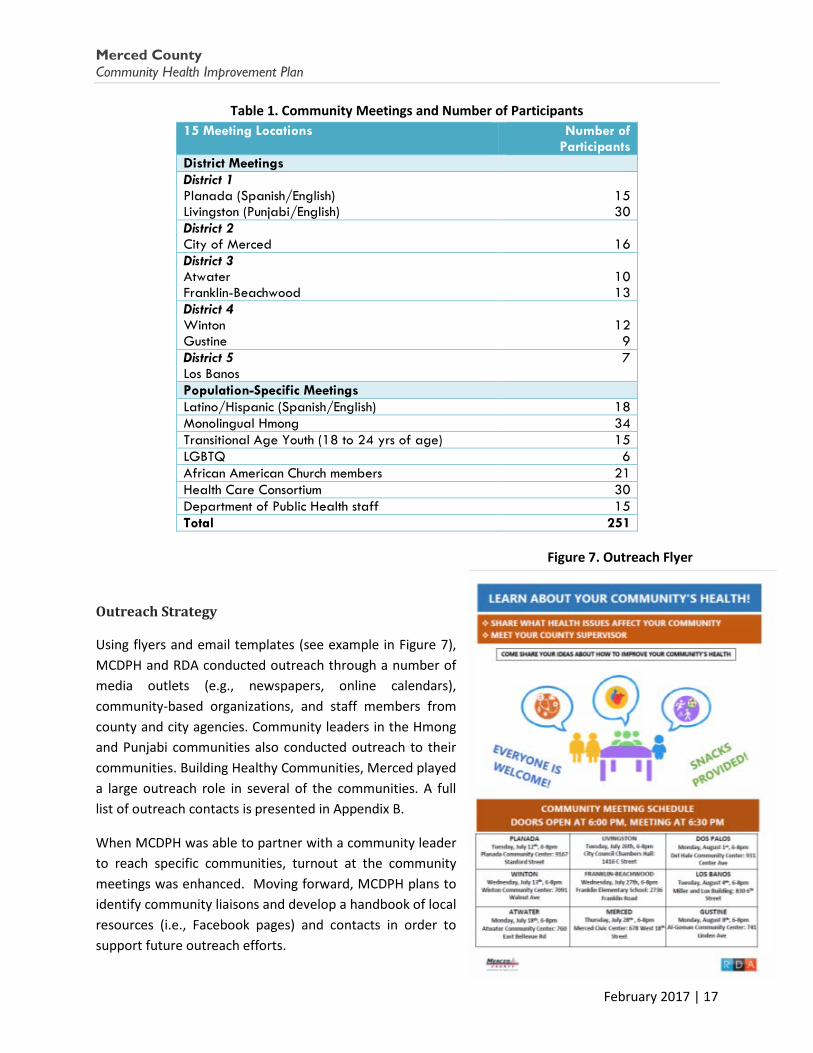
Table 1 below shows the district and population-specific meetings along with the number of meeting participants. Based on attendance sign-in sheets, a total of 251 people participated in 15 community meetings.
Merced County Board of Supervisors
2016
District 1 – John Pedrozo
District 2 – Hub Walsh
District 3- Daron McDaniel
District 4 – Deidre Kelsey
District 5 – Jerry O’Banion
Community Health Improvement Plan 2016 Community Meetings
Dos Palos
February 2017 | 16
Merced County Community Health Improvement Plan
Table 1. Community Meetings and Number of Participants 15 Meeting Locations Number of
Participants District Meetings District 1 Planada (Spanish/English) Livingston (Punjabi/English)
15 30
District 2 City of Merced
16
District 3 Atwater Franklin-Beachwood
10 13
District 4 Winton Gustine
12 9
District 5 Los Banos
7
Population-Specific Meetings Latino/Hispanic (Spanish/English) 18 Monolingual Hmong 34 Transitional Age Youth (18 to 24 yrs of age) 15 LGBTQ 6 African American Church members 21 Health Care Consortium 30 Department of Public Health staff 15 Total 251
Outreach Strategy
Using flyers and email templates (see example in Figure 7), MCDPH and RDA conducted outreach through a number of media outlets (e.g., newspapers, online calendars), community-based organizations, and staff members from county and city agencies. Community leaders in the Hmong and Punjabi communities also conducted outreach to their communities. Building Healthy Communities, Merced played a large outreach role in several of the communities. A full list of outreach contacts is presented in Appendix B.
When MCDPH was able to partner with a community leader to reach specific communities, turnout at the community meetings was enhanced. Moving forward, MCDPH plans to identify community liaisons and develop a handbook of local resources (i.e., Facebook pages) and contacts in order to support future outreach efforts.
Figure 7. Outreach Flyer
February 2017 | 17
Merced County Community Health Improvement Plan
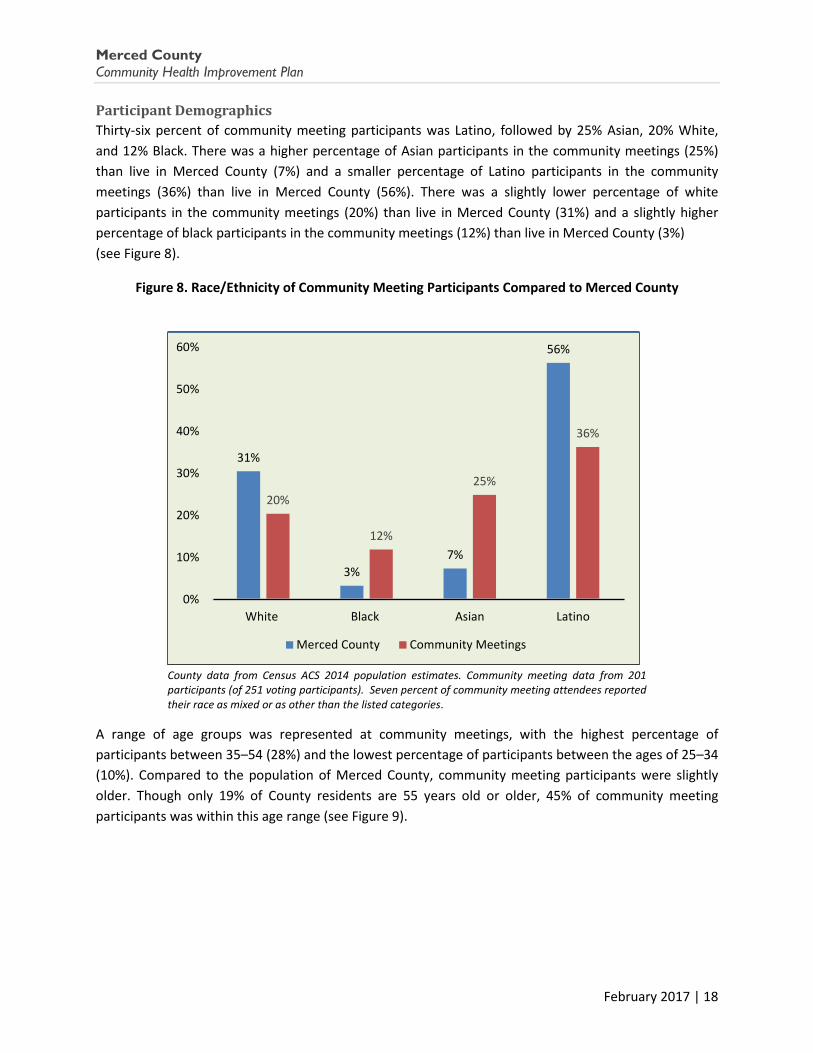
Thirty-six percent of community meeting participants was Latino, followed by 25% Asian, 20% White, and 12% Black. There was a higher percentage of Asian participants in the community meetings (25%) than live in Merced County (7%) and a smaller percentage of Latino participants in the community meetings (36%) than live in Merced County (56%). There was a slightly lower percentage of white participants in the community meetings (20%) than live in Merced County (31%) and a slightly higher percentage of black participants in the community meetings (12%) than live in Merced County (3%) (see Figure 8).
Figure 8. Race/Ethnicity of Community Meeting Participants Compared to Merced County
County data from Census ACS 2014 population estimates. Community meeting data from 201 participants (of 251 voting participants). Seven percent of community meeting attendees reported their race as mixed or as other than the listed categories.
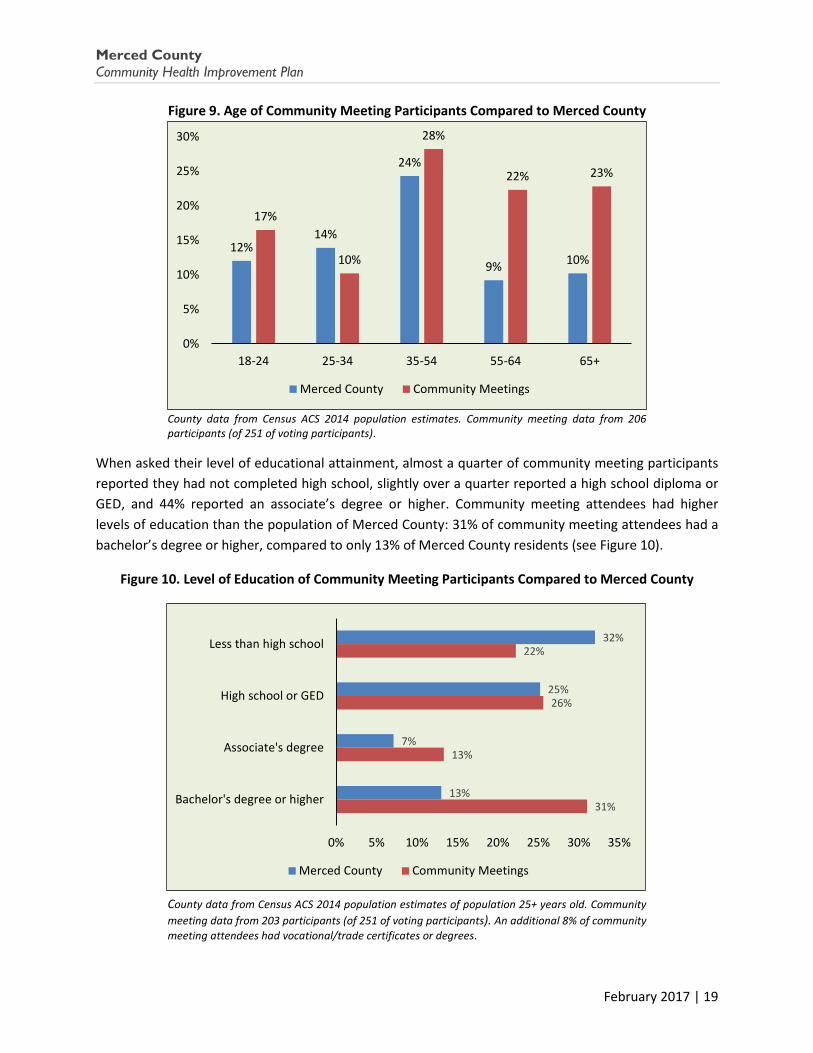
A range of age groups was represented at community meetings, with the highest percentage of participants between 35–54 (28%) and the lowest percentage of participants between the ages of 25–34 (10%). Compared to the population of Merced County, community meeting participants were slightly older. Though only 19% of County residents are 55 years old or older, 45% of community meeting participants was within this age range (see Figure 9).
31%
3% 7%
56%
20%
12%
25%
36%
0%
10%
20%
30%
40%
50%
60%
White Black Asian Latino
Merced County Community Meetings
February 2017 | 18
Merced County Community Health Improvement Plan
Figure 9. Age of Community Meeting Participants Compared to Merced County
County data from Census ACS 2014 population estimates. Community meeting data from 206 participants (of 251 of voting participants).
When asked their level of educational attainment, almost a quarter of community meeting participants reported they had not completed high school, slightly over a quarter reported a high school diploma or GED, and 44% reported an associate’s degree or higher. Community meeting attendees had higher levels of education than the population of Merced County: 31% of community meeting attendees had a bachelor’s degree or higher, compared to only 13% of Merced County residents (see Figure 10).
Figure 10. Level of Education of Community Meeting Participants Compared to Merced County
County data from Census ACS 2014 population estimates of population 25+ years old. Community meeting data from 203 participants (of 251 of voting participants). An additional 8% of community meeting attendees had vocational/trade certificates or degrees.
12% 14%
24%
9% 10%
17%
10%
28%
22% 23%
0%
5%
10%
15%
20%
25%
30%
18-24 25-34 35-54 55-64 65+
Merced County Community Meetings
32%
25%
7%
13%
22%
26%
13%
31%
0% 5% 10% 15% 20% 25% 30% 35%
Less than high school
High school or GED
Associate's degree
Bachelor's degree or higher
Merced County Community Meetings
February 2017 | 19

Merced County Community Health Improvement Plan
Traveling Booth
In order to gather feedback from as many diverse community members as possible, including hard-to-reach populations in more remote locations, MCDPH set up a “traveling booth” at 14 community events and locations throughout the County (see text box below). At each location, the community engagement materials depicting the 10 health issues were presented in English and Spanish on large posters and on handouts for community members. MCDPH representatives staffed the booth and were available to answer questions and provide additional information about the health issues.
Figure 12. Community Meeting in Planada, July 12, 2016
Figure 11. Community Meeting in Livingston, July 26, 2016
February 2017 | 20
Merced County Community Health Improvement Plan
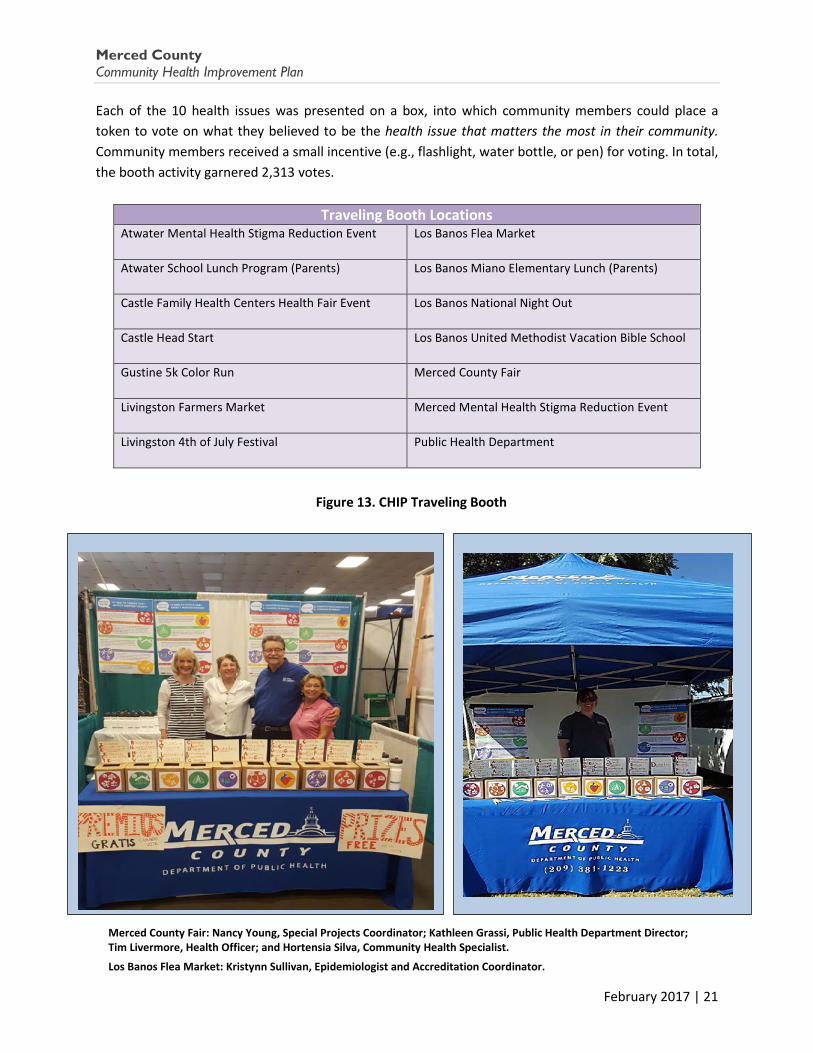
Each of the 10 health issues was presented on a box, into which community members could place a token to vote on what they believed to be the health issue that matters the most in their community. Community members received a small incentive (e.g., flashlight, water bottle, or pen) for voting. In total, the booth activity garnered 2,313 votes.
Traveling Booth Locations Atwater Mental Health Stigma Reduction Event
Los Banos Flea Market
Atwater School Lunch Program (Parents)
Los Banos Miano Elementary Lunch (Parents)
Castle Family Health Centers Health Fair Event
Los Banos National Night Out
Castle Head Start
Los Banos United Methodist Vacation Bible School
Gustine 5k Color Run
Merced County Fair
Livingston Farmers Market
Merced Mental Health Stigma Reduction Event
Livingston 4th of July Festival
Public Health Department
Figure 13. CHIP Traveling Booth
Merced County Fair: Nancy Young, Special Projects Coordinator; Kathleen Grassi, Public Health Department Director; Tim Livermore, Health Officer; and Hortensia Silva, Community Health Specialist.
Los Banos Flea Market: Kristynn Sullivan, Epidemiologist and Accreditation Coordinator.
February 2017 | 21

Merced County Community Health Improvement Plan
Section 4: Ranked Health Priorities
A tally of the votes collected across the 15 community meetings and the 14 traveling booth locations revealed community members’ health priorities. Figure 14 displays the number of votes each health issue received across all community meetings, and whether the issue was voted as the first or second priority. Adding the total number of votes, including participants’ first and second top priorities, the top five priority areas were: Income, Education, and Employment; Heart Disease and Stroke; Diabetes; Access to Health Care; and Drug and Alcohol Abuse (see
Appendix C for priority votes from individual meetings).
Figure 14. Community Meeting Votes by Health Issues
Table 2 lists the total votes received by each health issue at the traveling booth.
Table 2. Tally of Traveling Booth Votes by Health Issue
Health Topic Number of Votes Income, Education, Employment 438 Alcohol & Drug Abuse 433 Housing & Homelessness 329 Diabetes 276 Injury & Violence 203 Healthy Food & Physical Activity 190 Access to Medical Care 160 Heart Disease & Stroke 109 Sexually Transmitted Infections 91 Chronic Lung Disease 74 Overall Total 2,313
February 2017 | 22
1
6
1
2
7
13
1
1
2
2
4
4
9
8
5
2
SEXUALLY TRANSMITTED INFECTIONS
INJURY & VIOLENCE
HOUSING & HOMELESSNESS
CHRONIC LUNG DISEASE
HEALTHY FOODS & PHYSICAL ACTIVITY
DRUG & ALCOHOL ABUSE
ACCESS TO CARE
DIABETES
HEART DISEASE & STROKE
INCOME, EDUCATION, & EMPLOYMENT
First Priority Second Priority
(15)
(12)
(10)
(10)
(10)
(5)
Merced County Community Health Improvement Plan
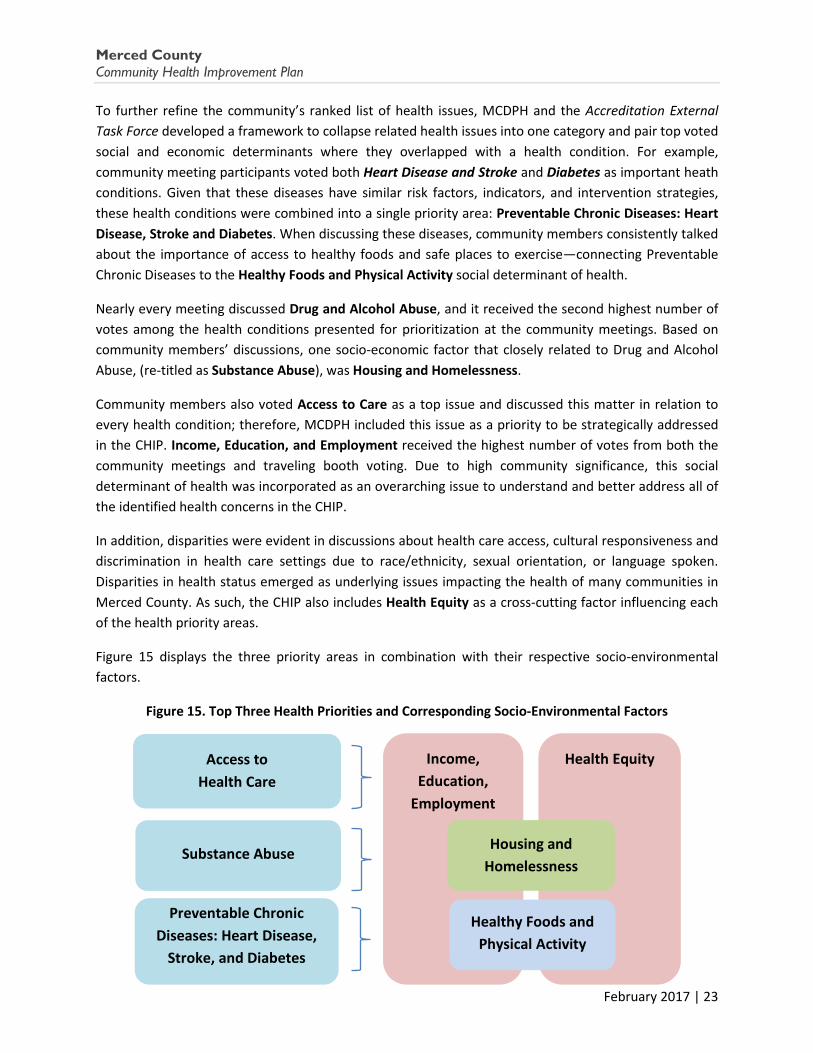
To further refine the community’s ranked list of health issues, MCDPH and the Accreditation External Task Force developed a framework to collapse related health issues into one category and pair top voted social and economic determinants where they overlapped with a health condition. For example, community meeting participants voted both Heart Disease and Stroke and Diabetes as important heath conditions. Given that these diseases have similar risk factors, indicators, and intervention strategies, these health conditions were combined into a single priority area: Preventable Chronic Diseases: Heart Disease, Stroke and Diabetes. When discussing these diseases, community members consistently talked about the importance of access to healthy foods and safe places to exercise—connecting Preventable Chronic Diseases to the Healthy Foods and Physical Activity social determinant of health.
Nearly every meeting discussed Drug and Alcohol Abuse, and it received the second highest number of votes among the health conditions presented for prioritization at the community meetings. Based on community members’ discussions, one socio-economic factor that closely related to Drug and Alcohol Abuse, (re-titled as Substance Abuse), was Housing and Homelessness.
Community members also voted Access to Care as a top issue and discussed this matter in relation to every health condition; therefore, MCDPH included this issue as a priority to be strategically addressed in the CHIP. Income, Education, and Employment received the highest number of votes from both the community meetings and traveling booth voting. Due to high community significance, this social determinant of health was incorporated as an overarching issue to understand and better address all of the identified health concerns in the CHIP.
In addition, disparities were evident in discussions about health care access, cultural responsiveness and discrimination in health care settings due to race/ethnicity, sexual orientation, or language spoken. Disparities in health status emerged as underlying issues impacting the health of many communities in Merced County. As such, the CHIP also includes Health Equity as a cross-cutting factor influencing each of the health priority areas.
Figure 15 displays the three priority areas in combination with their respective socio-environmental factors.
Figure 15. Top Three Health Priorities and Corresponding Socio-Environmental Factors
Health Equity Access to Health Care
Substance Abuse
Preventable Chronic Diseases: Heart Disease,
Stroke, and Diabetes
Income, Education,
Employment
Healthy Foods and Physical Activity
Housing and Homelessness
February 2017 | 23
Merced County Community Health Improvement Plan
Section 5: Summary of Community Discussions on the Health Priorities
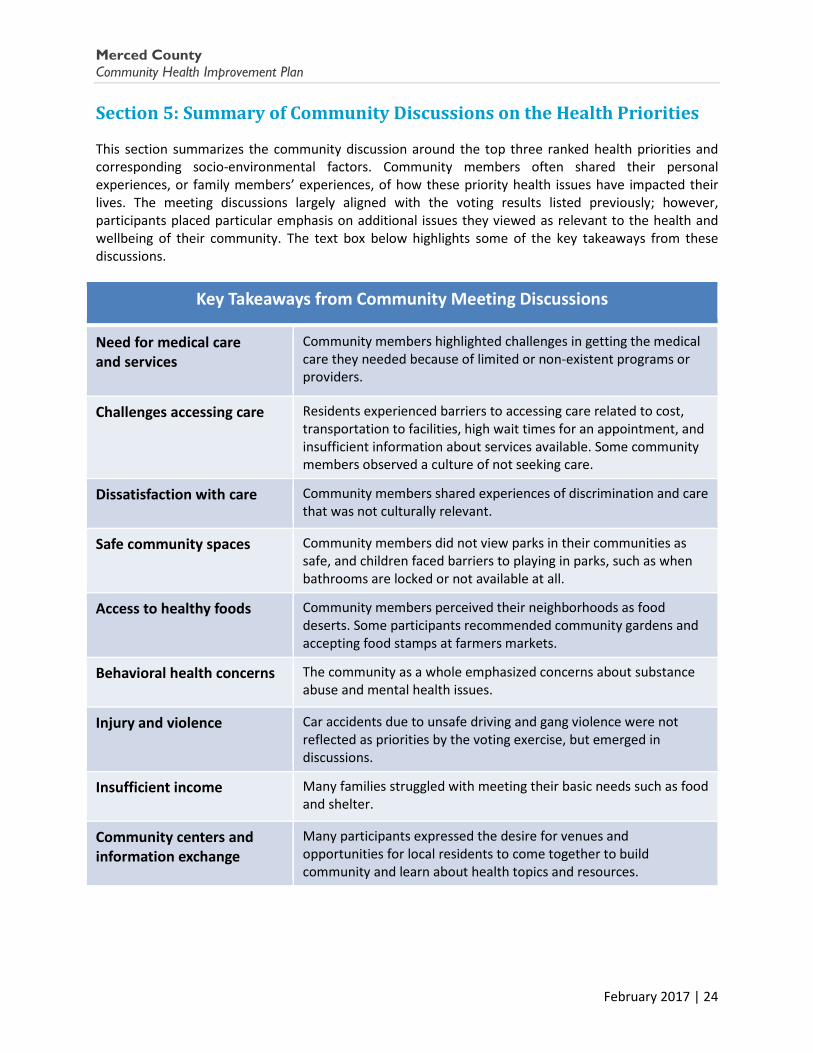
This section summarizes the community discussion around the top three ranked health priorities and corresponding socio-environmental factors. Community members often shared their personal experiences, or family members’ experiences, of how these priority health issues have impacted their lives. The meeting discussions largely aligned with the voting results listed previously; however, participants placed particular emphasis on additional issues they viewed as relevant to the health and wellbeing of their community. The text box below highlights some of the key takeaways from these discussions.
Key Takeaways from Community Meeting Discussions
Need for medical care and services
Community members highlighted challenges in getting the medical care they needed because of limited or non-existent programs or providers.
Challenges accessing care Residents experienced barriers to accessing care related to cost, transportation to facilities, high wait times for an appointment, and insufficient information about services available. Some community members observed a culture of not seeking care.
Dissatisfaction with care Community members shared experiences of discrimination and care that was not culturally relevant.
Safe community spaces Community members did not view parks in their communities as safe, and children faced barriers to playing in parks, such as when bathrooms are locked or not available at all.
Access to healthy foods Community members perceived their neighborhoods as food deserts. Some participants recommended community gardens and accepting food stamps at farmers markets.
Behavioral health concerns The community as a whole emphasized concerns about substance abuse and mental health issues.
Injury and violence Car accidents due to unsafe driving and gang violence were not reflected as priorities by the voting exercise, but emerged in discussions.
Insufficient income Many families struggled with meeting their basic needs such as food and shelter.
Community centers and information exchange
Many participants expressed the desire for venues and opportunities for local residents to come together to build community and learn about health topics and resources.
February 2017 | 24

Merced County Community Health Improvement Plan
Access to Health Care
Community meeting participants across all districts and population-specific groups expressed numerous challenges in accessing the various types of health care services and programs they need. Since the rollout of the Affordable Care Act, more people in Merced County have health care coverage; however, according to community participants, many people remain uninsured, specifically Merced’s undocumented adults. Participants stated that undocumented residents experience disproportionate challenges in getting the care they need. Additionally, even insured residents are not having their medical needs met. Residents reported struggles with the cost, availability, location, quality of care, and wait time for services. Participants in the Health Care Consortium community meeting voiced that there continues to be an extremely high utilization of emergency services for primary care needs, as well as a shortage of all types of health care providers across the county. A summary of the barriers to care most frequently mentioned in the community meetings follows.
Many community members stated that there is not enough primary care, specialist, or mental health providers to adequately serve their community. Some attributed the shortage of doctors and health care providers in general to challenges with retention and noted that, currently, many providers are retiring at a high rate.
The availability of mental health providers and services, especially counseling services, was of particular concern in most population-specific and several district community meetings. One community participant expressed frustration about the need for more services and observed that many who seek care in a hospital setting would be better served by targeted mental health treatment.
Additionally, many community members identified issues of drug and alcohol abuse as well as injury and violence as important health concerns related to the perceived lack of access to mental health care services and the limited availability of providers.
Multiple community meetings discussed strengthening the University of California, Merced medical education track to create a strategic career pipeline of medical professionals to serve the community from within and address the shortage of physicians.
Participants in Districts 1, 2, 3, and 5 and all population-specific group participants stated that cost was a major barrier to obtaining medical services. Many described financial challenges
“Income and unemployment is a major problem in our community; people don’t come to the hospital because of the bill—they can’t pay it.”
-Franklin-Beachwood Community Meeting Participant
“We need more help with mental health problems - they don’t need to go to the hospital, but they need mental health treatment. Often people stay in the hospital and there is no mental health evaluation there, so they sit there.”
–African American CommunityMeeting Participant
February 2017 | 25

Merced County Community Health Improvement Plan
making it difficult to meet their basic needs and impeding their ability to pay for medical care, even when medical services are offered on a sliding scale.
Meetings in all districts discussed concerns with transportation. For some, not having access to a car made it difficult for them to get to medical appointments. Additionally, participants mentioned having to travel great distances to seek out services they needed because those services are not available in their immediate area or even within Merced County. Many voiced spending a whole day on one appointment, including traveling to the doctor and then waiting to be seen. One participant also described this challenge related to accessing mental health treatment.
At almost all of the population-specific community meetings, participants mentioned experiencing discrimination during their health care interactions and in the community at large, or described a friend or family member’s experiences with discrimination. Community members shared experiences of being discriminated against based on their race, ethnicity, or sexual orientation in medical settings. Participants noted that ongoing discrimination decreases the likelihood that they will seek care, and causes them to lose confidence in the health care system. They question whether their health care providers genuinely have their best interests in mind.
“In Los Banos, on the west side of Merced [County], we have nothing…. We have transportation issues. In order to come to Merced, it’s 35 miles. If someone is in need [of medical care] they are not going to go.”
–Health Care Consortium MeetingParticipant
“There are not enough doctors and those who are available are not necessarily willing to serve the [Black] community. They may be available, but not available to the Black community. The disparities in health care access are significant. We are not talked to with respect… We do not trust the medical community.”
-African American Community Meeting Participant
“In the family health clinic it’s very discriminatory; if you are gay you are looked down upon. The doctors need better training and education. Doctors and health care providers need to be more respectful about how we are spoken to. We are people too. It’s not a crime to be queer and to be sexually active.”
–LGBTQ CommunityMeeting Participant
“Discrimination happens constantly; doctors do not value our community… [Doctors] assume that we don’t have insurance, a job, or speak English.”
-Hmong Community Meeting Participant
February 2017 | 26

Merced County Community Health Improvement Plan
Community members also stated that in order to provide better care and more effective health education, there is a need for an improved understanding of their cultures within the medical community. Participants from the Punjabi community, the Hmong community, and the Latino community mentioned a culturally appropriate approach is particularly relevant when a provider recommends diet modifications for improved nutrition and/or disease prevention. Rather than a one-size-fits-all model, community members desire health care interactions where they feel understood and health education classes that are applicable in their daily lives.
Participants in Districts 1, 3, and 5 agreed that better dissemination of information is needed regarding the health services available, including hours of operation. For example, one participant stated that people in the community are not aware of what services are available to them and when they are available.
Preventable Chronic Diseases: Health Disease, Stroke, and Diabetes
The discussion in community meetings and the voting results showed that participants are aware of diabetes and heart disease as serious health issues. However, community members expressed that they want more support in understanding disease management, particularly with diabetes. Additionally, when participants discussed how to lead healthy lifestyles with a balanced diet and exercise, they described challenges around access to healthy foods and safe places for physical activity.
“In my experience, Latino men will not come to nutritional classes, but if we have an educator go to them on their front porch it totally changes the dynamic...”
–Health Care ConsortiumMeeting Participant
“Any solution for diabetes regulation that is proposed has to be culturally appropriate. Doctors can’t make the same suggestions that they would for an American family… Doctors have to make suggestions that are appropriate for a Hmong diet, and be aware that in the Hmong community there is no word for diabetes. They call it ‘sweet blood’.”
-Hmong Community Meeting Participant
“No one knows what services are available in Merced County. Lists of resources including days and hours open, location, who is eligible, hours available, would be helpful.”
- Los Banos Community Meeting Participant
February 2017 | 27

Merced County Community Health Improvement Plan
In community meetings held in Districts 1, 2, and 5, participants discussed challenges in grasping the complexities of managing diabetes. Some participants commented that insufficient or inaccessible explanations are provided to patients about what is required to manage their diabetes. An additional barrier mentioned was the cost of testing strips. Some participants also mentioned that they used home remedies instead of seeking medical care due to affordability.
Community member discussions pointed to a clear recognition of the interconnectivity between chronic diseases, (heart disease, stroke, and diabetes) and obesity and access to healthy foods and safe places to exercise.
Meetings in Districts 1, 2, 3, and 4, and the Transition Age Youth and Hmong meetings greatly
emphasized the need for clean and safe parks with unlocked bathrooms that would encourage people to be more active and allow them to better enjoy their community. In addition to safer parks, the Hmong community meeting pointed to a need for parks with shade and without loose dogs, so that they can comfortably exercise.
Community meeting participants shared their observations that the physical education classes at schools do not provide adequate physical activity for their children. Some parents enrolled their children in other activities like boxing, but other parents stated that they could not afford auxiliary programs.
Access to healthy foods was another concern expressed in many community meetings. Similar to the challenges expressed in accessing health care, many participants observed that they lived in a food desert and would need a car in order to get to the full-service grocery stores in the City of Merced. Additionally, the cost of healthy food was highlighted as a barrier. To address this barrier, participants from the community meeting in Gustine indicated that they have a weekly Farmers Market during the warmer seasons; however, on the off seasons, they must travel to Turlock or Los Banos to obtain fresh produce. In the Transition Age
Youth meeting, one participant noted the differences in food access even between the South and North sides of the City of Merced itself, noting that there are more opportunities for making healthy food decisions for residents in North Merced, a higher income neighborhood, than for residents in South Merced, a lower income neighborhood. Culturally relevant nutrition classes were also suggested in several community meetings.
“There is a problem with not having any food stores. Most people don’t have a car and the only good stores are in [the City of] Merced.”
-Planada Community Meeting Participant
“The concept of [blood] sugars is very complicated, and many doctors and other medical professionals don't explain it well at the patient level.”
- City of Merced Community Participant
“Many men drink and smoke in the park and use the restroom [outdoors] because the park’s restrooms are locked….I don’t take my kids to the park for this reason. The picnic tables are used by the older guys doing their thing [drinking]”
- Planada Community Meeting Participant
“There is only one park in Winton, and people get shot there.”
–Winton Community Meeting Youth Participant
February 2017 | 28

Merced County Community Health Improvement Plan
Substance Abuse
Many community members spoke with emphatic concern and urgency about the perceived high visibility of substance use in their neighborhoods. For example, in all district meetings and in most population-specific meetings, residents mentioned that their families could not utilize their community parks because that is where substance users congregate. When discussing substance abuse, often the discussion intertwined with community members’ acknowledgement of the related
issues of homelessness and the perceived lack of mental health support across the county. Community members expressed concern for both adults and youth with substance abuse issues, but were particularly concerned about youth having easy access to substances, especially at their schools.
Community meeting participants stated the need for educational resources to identify drug and alcohol abuse and how to avoid addiction and peer pressure. Participants also expressed the importance of providing engaging activities for Merced County’s youth as a way to prevent drug and alcohol abuse. Participants also mentioned that there is often stigma associated with substance abuse problems, and that some people are afraid or do not know how to ask for help. Additionally, a number of participants voiced a perception that the county does not have the necessary services to treat
those with drug and alcohol abuse issues.
Participants at the District 3 and the African American community meetings also discussed the negative impacts that criminalization of substances has had in their community. Overall, most community participants agreed that drug and alcohol abuse severely affected and fragmented their community.
Income, Education, and Employment
The large domain of Income, Education, and Employment had the highest votes of all the 10 health topics. This multifaceted topic was identified at nearly every community meeting as an all-encompassing factor that impacted the community’s health. Additionally, many participants indicated that addressing disparities that exist in income, education, and employment would improve the prevention, management, and treatment of each of the health conditions which affect county residents.
“Alcohol and drug abuse is a big issue and [drugs] are cheap at schools.” -Winton Community Meeting Youth Participant
“Drug and alcohol inpatient and outpatient programs are all gone [they were defunded].”
- Atwater Community Meeting Participant
“I have seen the community [change]. It was thriving…and now because of the drugs there are so many homeless people.... There were [substance abuse] programs that are now underfunded… Youth need to have access to other activities. Otherwise it’s, ‘Let’s drink, let’s get high, there’s nothing else to do!’”
–LGBTQ Community Member Participant
February 2017 | 29
Merced County Community Health Improvement Plan
As mentioned in the section on Access to Care, many community meeting participants spoke about having limited access to health care services and shared that their income affected their ability to access services. Participants also highlighted that their income levels corresponded to their education and their ability to get the job or housing they desired, which some observed affected their mental health and contributed to substance abuse issues. Many participants stated that the opportunity to receive an education, and subsequently get a job with a steady income,
was not equitable across the different populations in Merced County. For example, one community member pointed out that those who are undocumented face challenges due to the limited availability of financial assistance for basic needs.
Section 6: Introduction to the Work Plan - Goals, Objectives, & Strategies This section presents the CHIP Work Plan which includes goals and objectives specifically designed to address each health priority area – Access to Health Care; Preventable Chronic Diseases: Heart Disease, Stroke, and Diabetes; Substance Abuse; and Health Equity and Social Determinants of Health. Each objective delineates strategies that fall into the following broad categories which cover a continuum of activities from planning to implementation to evaluation:
Each objective also contains a list of potential indicators that may be used to assess progress toward implementing the CHIP strategies. These indicators will be further defined in the annual implementation plan. A list of responsible agencies/partners, not linked to specific strategies, but rather, more broadly, to each objective, is also included.
CHIP Action Categories Partnerships Evaluation
Communication Assessment
Policy Development/Implementation Youth/Adult Engagement
Resource Development Stakeholder/Consumer Education
Practice Enhancement Other
“How do we change the cycle? When you are poor you can’t afford a house, then you’re looked down upon because you are poor; this can then lead to mental health issues, so I drink or smoke to take the edge off.”
-African American Community Meeting Participant
“For undocumented adults, assistance is not available; people have to choose whether to pay for housing or buy food. You can do more things with a higher income.”
-Youth Community Meeting Participant
February 2017 | 30
Merced County Community Health Improvement Plan
Merced County Community Health Improvement
Work Plan
2017 - 2022
February 2017 | 31
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: A
cces
s to
Hea
lth C
are
PRIO
RITY
ARE
A 1:
ACC
ESS
TO H
EALT
H C
ARE
Goal
: All
indi
vidu
als
in M
erce
d Co
unty
hav
e ac
cess
to q
ualit
y he
alth
car
e.
Obj
ectiv
e 1.
1: B
y 20
22, i
ncre
ase
the
num
ber o
f hea
lth c
are
prov
ider
s, in
all
field
s, in
Mer
ced
Coun
ty.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Part
ners
hips
Iden
tify
and
shar
e ex
ampl
es o
f hea
lth c
are
orga
niza
tion
part
ners
hips
succ
essf
ully
leve
ragi
ng c
linic
al p
erso
nnel
, and
im
plem
ent w
here
feas
ible
.
Reso
urce
Dev
elop
men
t
Incr
ease
locu
m te
nens
.2
In
crea
se te
lehe
alth
opp
ortu
nitie
s.
Esta
blish
med
ical
resid
ency
pro
gram
s in
part
ners
hip
with
ed
ucat
iona
l ins
titut
ions
and
med
ical
org
aniza
tions
.
Prac
tice
Enha
ncem
ent
Incr
ease
recr
uitm
ent i
ncen
tives
for p
rovi
ders
.
Educ
atio
n
Crea
te h
ealth
car
eer p
ipel
ine
prog
ram
s at p
rimar
y,
seco
ndar
y, a
nd p
ost-
seco
ndar
y sc
hool
s.
Com
mun
ity E
nhan
cem
ents
Incr
ease
des
irabi
lity
of c
omm
unity
by
prov
idin
g m
ore
inco
me,
edu
catio
n, e
mpl
oym
ent,
and
recr
eatio
nal
oppo
rtun
ities
for h
ealth
pro
fess
iona
ls an
d th
eir f
amili
es.
• N
umbe
r of p
rovi
ders
in M
erce
d Co
unty
•
Rese
arch
repo
rt o
f suc
cess
ful h
ealth
car
e or
gani
zatio
ns p
artn
ersh
ips
• N
umbe
r of g
roup
s with
whi
ch
part
ners
hip
repo
rt is
shar
ed
• Pa
rtne
rshi
p m
eetin
g ag
enda
s and
m
inut
es
• N
umbe
r of n
ew lo
cum
tene
ns
• N
umbe
r of n
ew te
lehe
alth
opp
ortu
nitie
s •
Esta
blish
men
t and
/or e
xpan
sion
of o
ne
med
ical
resid
ency
pro
gram
•
Num
ber o
f new
ince
ntiv
es o
ffere
d to
pr
ovid
ers
• N
umbe
r of n
ew h
ealth
car
eer p
rogr
ams
at lo
cal s
choo
ls •
Incr
ease
d em
ploy
men
t opp
ortu
nitie
s •
Incr
ease
d sc
hool
per
form
ance
•
Num
ber o
f new
recr
eatio
nal a
ctiv
ities
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• Ca
lifor
nia
Uni
vers
ity a
nd C
olle
ge sy
stem
s an
d lo
cal c
omm
unity
col
lege
syst
ems
• Sc
hool
Dist
ricts
•
Busin
esse
s •
City
/Cou
nty
Plan
ning
Dep
artm
ents
•
City
/Cou
nty
Park
s and
Rec
reat
ion
Depa
rtm
ents
•
Econ
omic
Dev
elop
men
t Dep
artm
ents
•
Mer
ced
Coun
ty D
epar
tmen
t of P
ublic
He
alth
2 Hea
lth c
are
faci
litie
s ca
n hi
re lo
cum
tene
ns p
hysic
ians
whe
n a
heal
th c
are
empl
oyer
face
s te
mpo
rary
sta
ffing
sho
rtag
es d
ue to
vac
anci
es, i
llnes
s, o
r oth
er c
ause
s. L
ocum
te
nens
phy
sicia
ns c
an h
elp
fill t
hose
vac
anci
es to
mai
ntai
n pa
tient
car
e qu
ality
.
Febr
uary
201
7 |
32
Mer
ced
Cou
nty
Com
mun
ity H
ealth
Impr
ovem
ent P
lan:
Acc
ess
to H
ealth
Car
e
Obj
ectiv
e 1.
2: B
y 20
22, e
nsur
e co
mpr
ehen
sive
, cul
tura
lly re
spon
sive
, and
qua
lity
heal
th c
are
for a
ll.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Prac
tice
Enha
ncem
ent
En
sure
app
ropr
iate
leve
l of c
are
as a
par
t of q
ualit
y ca
re.
U
se c
are
base
d in
cent
ives
to im
prov
e an
d m
aint
ain
qual
ityan
d co
mpe
tenc
y.
Incr
ease
num
ber a
nd p
artic
ipat
ion
of c
onsu
mer
s in
patie
ntca
re a
dviso
ry c
omm
ittee
s.
R eso
urce
Dev
elop
men
t
In
crea
se in
volv
emen
t of i
nter
pret
ers a
nd c
ultu
r al
brok
ers/
com
mun
ity h
ealth
wor
kers
(CHW
)/pr
omot
oras
inpa
tient
nav
igat
ion.
Educ
atio
n
In
crea
se p
rovi
der e
duca
tion
abou
t cul
tura
l com
pete
ncy.
•N
umbe
r of n
ew p
atie
nt le
vel t
riage
prog
ram
s and
staf
f•
Redu
ctio
n in
inap
prop
riate
ER
visit
s•
Num
ber o
f hig
h-ris
k pa
tient
s rec
eivi
n gco
ordi
nate
d ca
re th
roug
h He
alth
Hom
eso r
sim
ilar p
rogr
am•
Incr
ease
d us
e of
car
e ba
sed
ince
ntiv
es•
Incr
ease
d qu
ality
and
com
pete
ncy
inc a
re•
Num
ber o
f con
sum
ers i
n pa
tient
car
ead
viso
ry c
omm
ittee
s•
Num
ber o
f int
erpr
eter
s, cu
ltura
l bro
kers
,CH
Ws
•N
umbe
r of n
ew p
rovi
der c
ultu
ral
com
pete
ncy
educ
atio
n op
port
uniti
es
•He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
,ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lthpr
ovid
ers)
•Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth(C
CAH)
•M
erce
d Co
unty
Dep
artm
ent o
f Pub
li cH e
alth
•Co
mm
unity
Bas
ed O
rgan
izatio
ns
Obj
ectiv
e 1.
3: B
y 20
22, b
uild
dat
a re
posi
tory
and
dat
a sh
arin
g re
sour
ces a
cros
s sys
tem
s of c
are
to in
crea
se c
ontin
uity
and
qua
lity
of c
are.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
De
velo
p He
alth
Info
rmat
ion
Exch
ange
(HIE
) cap
acity
and
expa
nd h
ealth
car
e or
gani
zatio
n pa
rtic
ipat
ion.
Bu
ild 2
11 c
apac
ity to
adv
ertis
e id
entif
ied
com
mun
ityre
sour
ces a
nd su
ppor
t com
mun
ity c
linic
al li
nkag
es.
Cr
eate
e-r
efer
ral p
athw
ays t
o ap
prop
riate
clin
ical
and
non
-cl
inic
al se
rvic
es.
•N
umbe
r of n
ew p
artic
ipat
ing
heal
thca
re o
rgan
izatio
ns in
HIE
•N
umbe
r of n
ew re
sour
ces i
n 21
1•
Num
ber o
f 211
cal
ls re
ceiv
ed a
bout
heal
th re
sour
ces
•O
ne n
ew li
nkag
e pa
thw
ay c
reat
ed
•He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
,ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lthpr
ovid
ers)
•Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth (C
CAH)
•M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic H
ealth
•U
nite
d W
ay (2
11)
Febr
uary
201
7 |
33
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: A
cces
s to
Hea
lth C
are
Obj
ectiv
e 1.
4: B
y 20
22, c
reat
e co
mm
unity
-bas
ed h
ealth
supp
ort s
ervi
ces i
nten
ded
to e
nhan
ce c
linic
al c
are.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Stak
ehol
der/
Cons
umer
Edu
catio
n
Cond
uct o
utre
ach
to a
nd e
duca
tion
of c
onsu
mer
s to
incr
ease
app
ropr
iate
hea
lth in
sura
nce
utili
zatio
n.
Educ
ate
cons
umer
s abo
ut th
e im
port
ance
of p
reve
ntat
ive
care
.
Reso
urce
Dev
elop
men
t
Build
Com
mun
ity H
ealth
Wor
ker (
CHW
) net
wor
k to
im
prov
e co
mm
unity
-clin
ical
link
ages
.
Es
tabl
ish F
amily
Res
ourc
e Ce
nter
s and
incr
ease
cap
acity
of
scho
ol li
aiso
ns to
impr
ove
com
mun
ity-r
esou
rce
linka
ges.
In
crea
se m
edic
al tr
ansp
orta
tion
reso
urce
s.
Prac
tice
Enha
ncem
ent
Prom
ote
prov
ider
util
izatio
n of
uni
vers
al, s
tand
ardi
zed
0-5
year
dev
elop
men
tal s
cree
ning
s.
• N
umbe
r of n
ew c
onsu
mer
edu
catio
n op
port
uniti
es
• N
umbe
r of n
ew c
onsu
mer
pre
vent
ativ
e ca
re o
ppor
tuni
ties
• N
umbe
r of C
HWs
• Es
tabl
ish o
ne F
amily
Res
ourc
e Ce
nter
•
Num
ber o
f new
reso
urce
s for
scho
ol
liaiso
ns
• O
ne n
ew m
edic
al tr
ansp
orta
tion
reso
urce
•
Num
ber o
f pro
vide
rs u
tilizi
ng
stan
dard
ized
deve
lopm
enta
l scr
eeni
ngs
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• He
alth
Hom
e O
rgan
izatio
ns
• Co
ntin
uum
of C
are
• Sc
hool
Dist
ricts
•
Mer
ced
Coun
ty O
ffice
of E
duca
tion
• Fi
rst 5
Mer
ced
Coun
ty
Obj
ectiv
e 1.
5: B
y 20
22, s
uppo
rt in
tegr
atio
n of
prim
ary
care
and
beh
avio
ral h
ealth
with
in th
e he
alth
car
e sy
stem
.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Prac
tice
Enha
ncem
ent/
Asse
ssm
ent
Anal
yze
the
path
way
s for
refe
rral
s acr
oss p
rovi
der s
yste
ms
and
stra
tegi
ze m
etho
ds to
incr
ease
con
tinui
ty o
f pat
ient
ca
re.
Incr
ease
prim
ary
care
pro
vide
rs’ u
tiliza
tion
of b
ehav
iora
l he
alth
and
subs
tanc
e ab
use
scre
enin
g to
ols.
Educ
atio
n
Incr
ease
aw
aren
ess a
mon
g co
nsum
ers o
f rol
e of
prim
ary
care
pro
vide
rs a
s a re
sour
ce in
mild
to m
oder
ate
beha
vior
al
heal
th c
once
rns a
nd su
bsta
nce
abus
e.
• O
ne n
ew li
nkag
e pa
thw
ay c
reat
ed
• N
umbe
r of n
ew p
rovi
ders
usin
g be
havi
oral
hea
lth a
nd su
bsta
nce
abus
e sc
reen
ing
tool
s •
Num
ber c
onsu
mer
s see
king
beh
avio
ral
heal
th se
rvic
es a
t prim
ary
care
site
s
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• M
erce
d Co
unty
Dep
artm
ent o
f Beh
avio
ral
Heal
th a
nd R
ecov
ery
Serv
ices
Febr
uary
201
7 |
34
Mer
ced
Cou
nty
Com
mun
ity H
ealth
Impr
ovem
ent P
lan:
Pre
vent
able
Chr
onic
Dise
ases
: Hea
rt D
iseas
e, S
troke
, and
Dia
bete
s PR
IORI
TY A
REA
2: P
REVE
NTA
BLE
CHRO
NIC
DIS
EASE
S: H
EART
DIS
EASE
, STR
OK
E, A
ND
DIA
BETE
S
Goal
: Mer
ced
Coun
ty w
ill o
ptim
ize
the
soci
al a
nd p
hysi
cal e
nvir
onm
ents
to s
uppo
rt h
ealt
hy li
fest
yles
and
red
uce
the
risk
of c
hron
ic d
isea
se fo
r al
l res
iden
ts.
Obj
ectiv
e 2.
1: B
y 20
22, a
ddre
ss p
olic
y, sy
stem
, and
env
ironm
enta
l fac
tors
inte
nded
to p
rom
ote
and
impr
ove
com
mun
ity h
ealth
.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t/Pa
rtne
rshi
ps
In
crea
se n
umbe
r of s
hare
d us
e ag
reem
ents
.
Impr
ove
qual
ity a
nd sa
fety
of p
arks
.
Incr
ease
fund
ing
for p
arks
.
Incr
ease
opp
ortu
nitie
s to
obta
in h
ealth
y fo
ods
thro
ugh
farm
ers m
arke
t, co
mm
unity
gar
dens
, and
groc
ery
stor
es.
In
crea
se to
bacc
o-fr
ee p
lace
s and
rest
rict a
cces
s to
toba
cco
prod
ucts
(inc
ludi
ng e
-cig
aret
tes)
.
•N
umbe
r of n
ew sh
ared
use
agr
eem
ents
.•
New
fund
ing
for p
arks
•In
cide
nce
of c
rime
at p
arks
•N
umbe
r of n
ew fa
rmer
s mar
kets
,co
mm
unity
mar
kets
, and
hea
lthy
food
outle
ts•
Num
ber o
f tob
acco
reta
ilers
(mai
ntai
n or
decr
ease
cur
rent
num
bers
)•
Num
ber o
f new
smok
e-fr
ee p
olic
ies
•Sc
hool
Dist
ricts
•Co
mm
unity
-Bas
ed O
rgan
izatio
ns•
City
/Cou
nty
Park
s and
Rec
reat
ion
Depa
rtm
ents
•La
w e
nfor
cem
ent
•M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic H
ealth
•Ci
ty C
ounc
ils/ B
oard
of S
uper
viso
rs•
Busin
ess C
omm
unity
•Ci
ty/C
ount
y Pl
anni
ng D
epar
tmen
ts•
Farm
ers/
Grow
ers/
Prod
ucer
s•
Faith
-Bas
ed O
rgan
izatio
ns
Obj
ectiv
e 2.
2: B
y 20
22, i
ncre
ase
com
mun
ity a
cces
s to
soci
al n
etw
orks
and
supp
ort s
yste
ms t
o re
duce
and
man
age
prev
enta
ble
chro
nic
dise
ases
.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
De
velo
p CH
W/p
rom
otor
a ne
twor
k to
exp
and
peer
-le
d or
pee
r-to
-pee
r pro
gram
s (e.
g. C
hron
ic D
iseas
eSe
lf-M
anag
emen
t Pro
gram
, Pee
rs fo
r Pro
gres
s, m
icro
clin
ics)
and
con
nect
com
mun
ity m
embe
rs to
serv
ices
.
Prac
tice
Enha
ncem
ent
Id
entif
y op
port
uniti
es fo
r rei
mbu
rsem
ent o
fCH
Ws/
prom
otor
as (e
.g. C
CAH
and
stat
e le
vel).
•N
umbe
r of C
HWs
•N
umbe
r new
of p
eer-
led
clas
ses o
ffere
d•
Num
ber o
f 211
refe
rral
s to
clas
ses
•De
velo
ped
stra
tegy
for r
eim
burs
emen
t•
Perc
ent o
f CHW
wor
k th
at is
reim
burs
ed
•He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, hos
pita
ls,cl
inic
s, b
ehav
iora
l hea
lth p
rovi
ders
)•
Cent
ral C
alifo
rnia
Alli
ance
for H
ealth
(CCA
H)•
Mer
ced
Coun
ty D
epar
tmen
t of P
ublic
Hea
lth•
Com
mun
ity-B
ased
Org
aniza
tions
•U
nite
d W
ay (2
11)
•Fa
ith-B
ased
Org
aniza
tions
Febr
uary
201
7 |
35
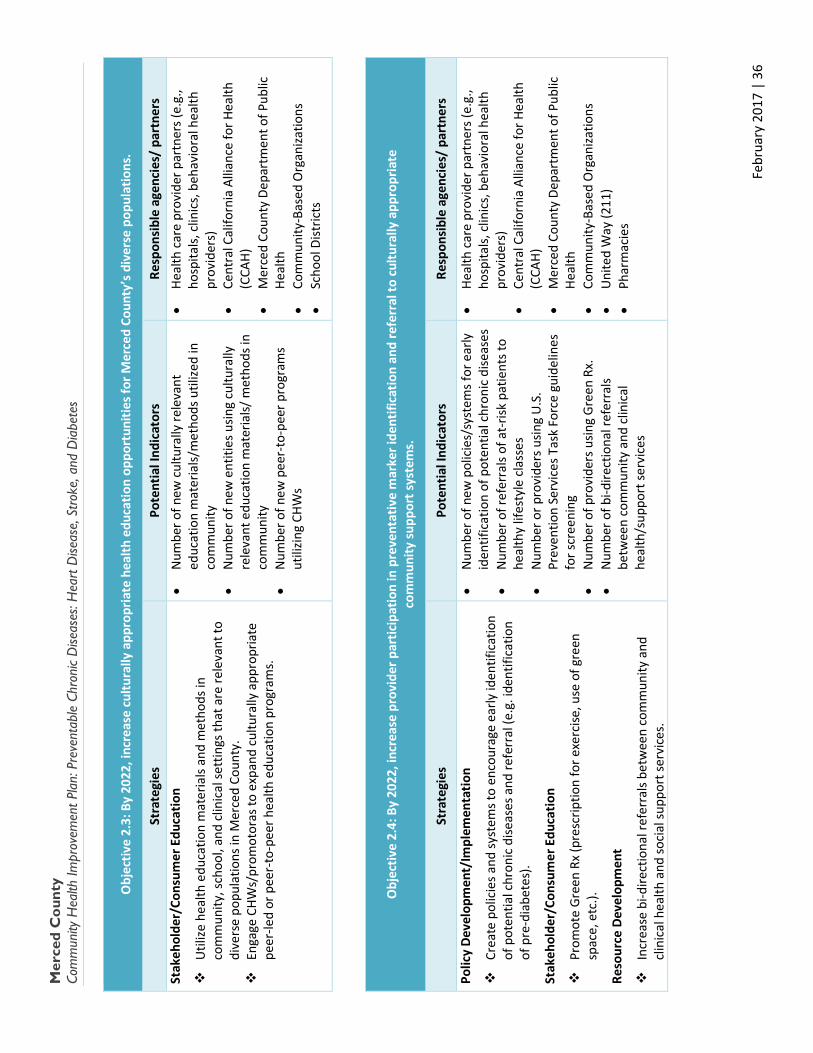
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: P
reve
ntab
le C
hron
ic D
iseas
es: H
eart
Dise
ase,
Stro
ke, a
nd D
iabe
tes
Obj
ectiv
e 2.
3: B
y 20
22, i
ncre
ase
cultu
rally
app
ropr
iate
hea
lth e
duca
tion
oppo
rtun
ities
for M
erce
d Co
unty
’s d
iver
se p
opul
atio
ns.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Stak
ehol
der/
Cons
umer
Edu
catio
n
Util
ize h
ealth
edu
catio
n m
ater
ials
and
met
hods
in
com
mun
ity, s
choo
l, an
d cl
inic
al se
ttin
gs th
at a
re re
leva
nt to
di
vers
e po
pula
tions
in M
erce
d Co
unty
.
En
gage
CHW
s/pr
omot
oras
to e
xpan
d cu
ltura
lly a
ppro
pria
te
peer
-led
or p
eer-
to-p
eer h
ealth
edu
catio
n pr
ogra
ms.
• N
umbe
r of n
ew c
ultu
rally
rele
vant
ed
ucat
ion
mat
eria
ls/m
etho
ds u
tilize
d in
co
mm
unity
•
Num
ber o
f new
ent
ities
usin
g cu
ltura
lly
rele
vant
edu
catio
n m
ater
ials/
met
hods
in
com
mun
ity
• N
umbe
r of n
ew p
eer-
to-p
eer p
rogr
ams
utili
zing
CHW
s
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• Sc
hool
Dist
ricts
Obj
ectiv
e 2.
4: B
y 20
22, i
ncre
ase
prov
ider
par
ticip
atio
n in
pre
vent
ativ
e m
arke
r ide
ntifi
catio
n an
d re
ferr
al to
cul
tura
lly a
ppro
pria
te
com
mun
ity su
ppor
t sys
tem
s.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Polic
y De
velo
pmen
t/Im
plem
enta
tion
Crea
te p
olic
ies a
nd sy
stem
s to
enco
urag
e ea
rly id
entif
icat
ion
of p
oten
tial c
hron
ic d
iseas
es a
nd re
ferr
al (e
.g. i
dent
ifica
tion
of p
re-d
iabe
tes)
.
Stak
ehol
der/
Cons
umer
Edu
catio
n
Prom
ote
Gree
n Rx
(pre
scrip
tion
for e
xerc
ise, u
se o
f gre
en
spac
e, e
tc.).
Reso
urce
Dev
elop
men
t
Incr
ease
bi-d
irect
iona
l ref
erra
ls be
twee
n co
mm
unity
and
cl
inic
al h
ealth
and
soci
al su
ppor
t ser
vice
s.
• N
umbe
r of n
ew p
olic
ies/
syst
ems f
or e
arly
id
entif
icat
ion
of p
oten
tial c
hron
ic d
iseas
es
• N
umbe
r of r
efer
rals
of a
t-risk
pat
ient
s to
heal
thy
lifes
tyle
cla
sses
•
Num
ber o
r pro
vide
rs u
sing
U.S
. Pr
even
tion
Serv
ices
Tas
k Fo
rce
guid
elin
es
for s
cree
ning
•
Num
ber o
f pro
vide
rs u
sing
Gre
en R
x.
• N
umbe
r of b
i-dire
ctio
nal r
efer
rals
betw
een
com
mun
ity a
nd c
linic
al
heal
th/s
uppo
rt se
rvic
es
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• U
nite
d W
ay (2
11)
• Ph
arm
acie
s
Febr
uary
201
7 |
36

Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: S
ubst
ance
Abu
se PR
IORI
TY A
REA
3: S
UBS
TAN
CE A
BUSE
Goal
: Inc
reas
e w
elln
ess
in M
erce
d Co
unty
by
addr
essi
ng th
e co
ndit
ions
that
lead
to d
rug
and
alco
hol a
buse
.
Obj
ectiv
e 3.
1: B
y 20
22, i
ncre
ase
trea
tmen
t cap
acity
and
acc
essi
bilit
y to
subs
tanc
e ab
use
reso
urce
s.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
Incr
ease
trea
tmen
t opp
ortu
nitie
s in
alte
rnat
ive
com
mun
ity
sett
ings
(e.g
., sc
hool
s, c
hurc
hes,
etc
.)
Prac
tice
Enha
ncem
ent
Asse
ss d
epre
ssio
n in
you
th in
alte
rnat
ive
com
mun
ity se
ttin
gs.
• N
umbe
r of c
lass
es in
alte
rnat
ive
loca
tions
•
Num
ber o
f clie
nts s
erve
d in
alte
rnat
ive
loca
tions
•
Num
ber o
f you
th sc
reen
ed fo
r dep
ress
ion
in a
ltern
ativ
e lo
catio
ns
• De
part
men
t of B
ehav
iora
l Hea
lth a
nd
Reco
very
Ser
vice
s •
Scho
ol D
istric
ts
• Fa
ith-B
ased
Org
aniza
tions
•
Com
mun
ity-B
ased
Org
aniza
tions
•
Boys
and
Girl
s Clu
b an
d ot
her
com
mun
ity p
lace
s
Febr
uary
201
7 |
37
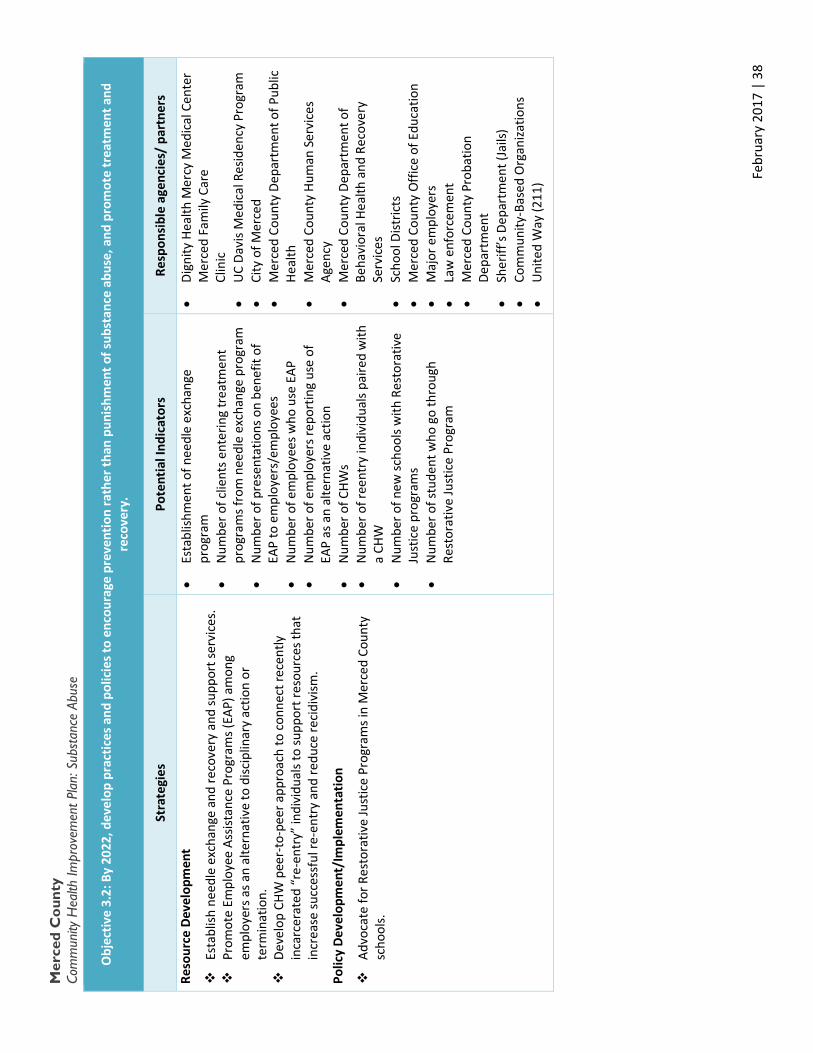
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: S
ubst
ance
Abu
se
Obj
ectiv
e 3.
2: B
y 20
22, d
evel
op p
ract
ices
and
pol
icie
s to
enco
urag
e pr
even
tion
rath
er th
an p
unis
hmen
t of s
ubst
ance
abu
se, a
nd p
rom
ote
trea
tmen
t and
re
cove
ry.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
Esta
blish
nee
dle
exch
ange
and
reco
very
and
supp
ort s
ervi
ces.
Pr
omot
e Em
ploy
ee A
ssist
ance
Pro
gram
s (EA
P) a
mon
g em
ploy
ers a
s an
alte
rnat
ive
to d
iscip
linar
y ac
tion
or
term
inat
ion.
De
velo
p CH
W p
eer-
to-p
eer a
ppro
ach
to c
onne
ct re
cent
ly
inca
rcer
ated
“re
-ent
ry”
indi
vidu
als t
o su
ppor
t res
ourc
es th
at
incr
ease
succ
essf
ul re
-ent
ry a
nd re
duce
reci
divi
sm.
Polic
y De
velo
pmen
t/Im
plem
enta
tion
Advo
cate
for R
esto
rativ
e Ju
stic
e Pr
ogra
ms i
n M
erce
d Co
unty
sc
hool
s.
• Es
tabl
ishm
ent o
f nee
dle
exch
ange
pr
ogra
m
• N
umbe
r of c
lient
s ent
erin
g tr
eatm
ent
prog
ram
s fro
m n
eedl
e ex
chan
ge p
rogr
am
• N
umbe
r of p
rese
ntat
ions
on
bene
fit o
f EA
P to
em
ploy
ers/
empl
oyee
s •
Num
ber o
f em
ploy
ees w
ho u
se E
AP
• N
umbe
r of e
mpl
oyer
s rep
ortin
g us
e of
EA
P as
an
alte
rnat
ive
actio
n •
Num
ber o
f CHW
s •
Num
ber o
f ree
ntry
indi
vidu
als p
aire
d w
ith
a CH
W
• N
umbe
r of n
ew sc
hool
s with
Res
tora
tive
Just
ice
prog
ram
s •
Num
ber o
f stu
dent
who
go
thro
ugh
Rest
orat
ive
Just
ice
Prog
ram
• Di
gnity
Hea
lth M
ercy
Med
ical
Cen
ter
Mer
ced
Fam
ily C
are
Cl
inic
•
UC
Davi
s Med
ical
Res
iden
cy P
rogr
am
• Ci
ty o
f Mer
ced
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• M
erce
d Co
unty
Hum
an S
ervi
ces
Agen
cy
• M
erce
d Co
unty
Dep
artm
ent o
f Be
havi
oral
Hea
lth a
nd R
ecov
ery
Serv
ices
•
Scho
ol D
istric
ts
• M
erce
d Co
unty
Offi
ce o
f Edu
catio
n •
Maj
or e
mpl
oyer
s •
Law
enf
orce
men
t •
Mer
ced
Coun
ty P
roba
tion
Depa
rtm
ent
• Sh
eriff
’s D
epar
tmen
t (Ja
ils)
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• U
nite
d W
ay (2
11)
Febr
uary
201
7 |
38
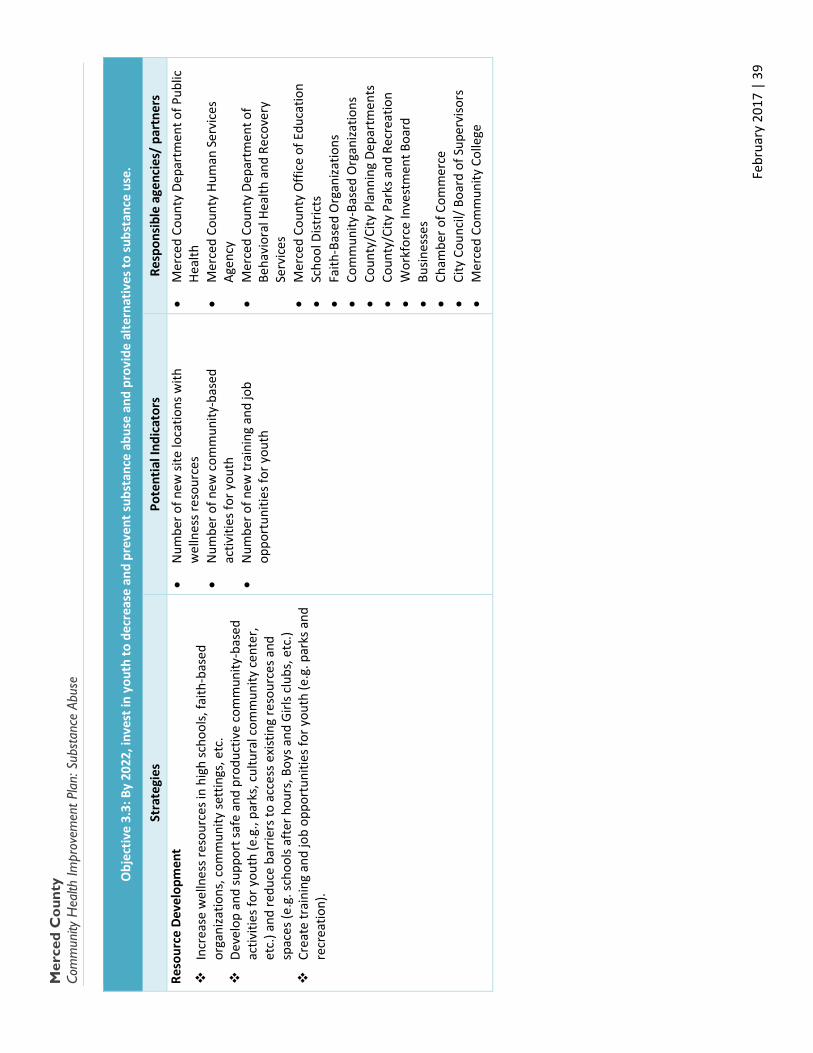
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: S
ubst
ance
Abu
se
Obj
ectiv
e 3.
3: B
y 20
22, i
nves
t in
yout
h to
dec
reas
e an
d pr
even
t sub
stan
ce a
buse
and
pro
vide
alte
rnat
ives
to su
bsta
nce
use.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
Incr
ease
wel
lnes
s res
ourc
es in
hig
h sc
hool
s, fa
ith-b
ased
or
gani
zatio
ns, c
omm
unity
sett
ings
, etc
.
De
velo
p an
d su
ppor
t saf
e an
d pr
oduc
tive
com
mun
ity-b
ased
ac
tiviti
es fo
r you
th (e
.g.,
park
s, c
ultu
ral c
omm
unity
cen
ter,
etc.
) and
redu
ce b
arrie
rs to
acc
ess e
xist
ing
reso
urce
s and
sp
aces
(e.g
. sch
ools
afte
r hou
rs, B
oys a
nd G
irls c
lubs
, etc
.)
Cr
eate
trai
ning
and
job
oppo
rtun
ities
for y
outh
(e.g
. par
ks a
nd
recr
eatio
n).
• N
umbe
r of n
ew si
te lo
catio
ns w
ith
wel
lnes
s res
ourc
es
• N
umbe
r of n
ew c
omm
unity
-bas
ed
activ
ities
for y
outh
•
Num
ber o
f new
trai
ning
and
job
oppo
rtun
ities
for y
outh
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• M
erce
d Co
unty
Hum
an S
ervi
ces
Agen
cy
• M
erce
d Co
unty
Dep
artm
ent o
f Be
havi
oral
Hea
lth a
nd R
ecov
ery
Serv
ices
•
Mer
ced
Coun
ty O
ffice
of E
duca
tion
• Sc
hool
Dist
ricts
•
Faith
-Bas
ed O
rgan
izatio
ns
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• Co
unty
/City
Pla
nnin
g De
part
men
ts
• Co
unty
/City
Par
ks a
nd R
ecre
atio
n •
Wor
kfor
ce In
vest
men
t Boa
rd
• Bu
sines
ses
• Ch
ambe
r of C
omm
erce
•
City
Cou
ncil/
Boa
rd o
f Sup
ervi
sors
•
Mer
ced
Com
mun
ity C
olle
ge
Febr
uary
201
7 |
39

Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: S
ubst
ance
Abu
se
Obj
ectiv
e 3.
4: B
y 20
22, e
duca
te a
nd e
ngag
e co
mm
unity
mem
bers
and
stak
ehol
ders
aro
und
fact
ors t
hat c
ontr
ibut
e to
the
initi
atio
n an
d pe
rpet
uatio
n of
su
bsta
nce
abus
e (e
.g. A
CEs)
.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Asse
ssm
ent
Asse
ss w
hich
Adv
erse
Chi
ldho
od E
xper
ienc
es
(ACE
s) a
re m
ost p
reva
lent
in M
erce
d Co
unty
th
roug
h da
ta c
olle
ctio
n (e
.g.,
Head
Sta
rt fa
mili
es).
Prac
tice
Enha
ncem
ent
Educ
ate
prov
ider
s on
impo
rtan
ce a
nd in
crea
se
utili
zatio
n of
ACE
scre
enin
g to
ols.
Ed
ucat
e pr
ovid
ers o
n in
fluen
ce o
f and
incr
ease
sc
reen
ing
for r
isk fa
ctor
s tha
t cou
ld le
ad to
su
bsta
nce
abus
e (e
.g. j
ob lo
ss, r
ecen
t los
s,
syst
emic
raci
sm, p
over
ty).
• N
umbe
r of A
CE e
valu
atio
ns c
ompl
eted
•
Perc
ent o
f chi
ldre
n w
ith h
igh
ACEs
•
Num
ber o
f ACE
edu
catio
nal o
ppor
tuni
ties
for p
rovi
ders
•
Num
ber o
f pro
vide
rs re
gula
rly a
sses
sing
ACEs
•
Num
ber o
f pro
vide
rs u
tilizi
ng su
bsta
nce
abus
e ris
k fa
ctor
scre
enin
gs
• M
erce
d Co
unty
Dep
artm
ent o
f Beh
avio
ral H
ealth
an
d Re
cove
ry S
ervi
ces
• M
erce
d Co
unty
Offi
ce o
f Edu
catio
n •
Mer
ced
Coun
ty H
ead
Star
t •
Heal
th c
are
prov
ider
par
tner
s (e.
g., h
ospi
tals,
cl
inic
s, b
ehav
iora
l hea
lth p
rovi
ders
) •
Cent
ral C
alifo
rnia
Alli
ance
for H
ealth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic H
ealth
•
Com
mun
ity-B
ased
Org
aniza
tions
Obj
ectiv
e 3.
5: B
y 20
22, s
uppo
rt H
ousi
ng F
irst a
nd o
ther
sobe
r liv
ing
effo
rts,
co-
loca
ted
with
subs
tanc
e ab
use
prev
entio
n an
d tr
eatm
ent p
rogr
ams,
to c
reat
e st
able
env
ironm
ents
for t
he h
omel
ess.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Polic
y De
velo
pmen
t/Im
plem
enta
tion
Enco
urag
e be
st p
ract
ice
hous
ing
mod
els.
Su
ppor
t qua
lity
cont
rol m
easu
res f
or so
ber l
ivin
g en
viro
nmen
ts.
• As
sess
men
t of s
elec
ted
hous
ing
mod
els
agai
nst b
est p
ract
ices
•
Num
ber o
f sob
er li
ving
env
ironm
ents
with
qu
ality
con
trol
mea
sure
s in
plac
e
• Av
erag
e qu
ality
con
trol
scor
e of
sobe
r liv
ing
envi
ronm
ents
•
Num
ber o
f org
aniza
tions
impl
emen
ting
Heal
th H
ome
mod
el
• M
erce
d Co
unty
Dep
artm
ent o
f Beh
avio
ral H
ealth
an
d Re
cove
ry S
ervi
ces
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic H
ealth
•
Com
mun
ity-B
ased
Org
aniza
tions
•
Cont
inuu
m o
f Car
e •
Cent
ral C
alifo
rnia
Alli
ance
for H
ealth
(CCA
H)
• M
erce
d Co
unty
Hou
sing
Auth
ority
•
City
Cou
ncil/
Boa
rd o
f Sup
ervi
sors
Febr
uary
201
7 |
40
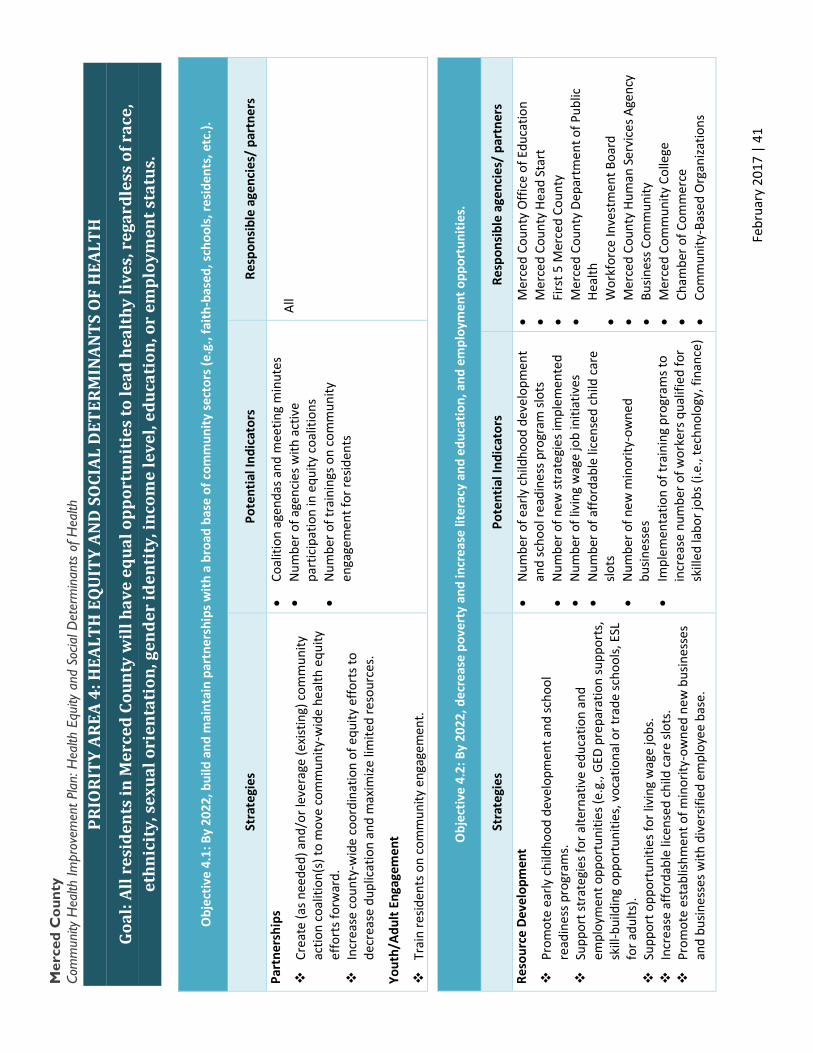
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: H
ealth
Equ
ity a
nd S
ocia
l Det
erm
inan
ts o
f Hea
lth
PRIO
RITY
ARE
A 4:
HEA
LTH
EQ
UIT
Y AN
D S
OCI
AL D
ETER
MIN
ANTS
OF
HEA
LTH
Goal
: All
resi
dent
s in
Mer
ced
Coun
ty w
ill h
ave
equa
l opp
ortu
niti
es to
lead
hea
lthy
live
s, r
egar
dles
s of
rac
e,
ethn
icit
y, s
exua
l ori
enta
tion
, gen
der
iden
tity
, inc
ome
leve
l, ed
ucat
ion,
or
empl
oym
ent s
tatu
s.
Obj
ectiv
e 4.
1: B
y 20
22, b
uild
and
mai
ntai
n pa
rtne
rshi
ps w
ith a
bro
ad b
ase
of c
omm
unity
sect
ors (
e.g.
, fai
th-b
ased
, sch
ools
, res
iden
ts, e
tc.).
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Part
ners
hips
Crea
te (a
s nee
ded)
and
/or l
ever
age
(exi
stin
g) c
omm
unity
ac
tion
coal
ition
(s) t
o m
ove
com
mun
ity-w
ide
heal
th e
quity
ef
fort
s for
war
d.
Incr
ease
cou
nty-
wid
e co
ordi
natio
n of
equ
ity e
ffort
s to
decr
ease
dup
licat
ion
and
max
imize
lim
ited
reso
urce
s.
Yout
h/Ad
ult E
ngag
emen
t
Trai
n re
siden
ts o
n co
mm
unity
eng
agem
ent.
• Co
aliti
on a
gend
as a
nd m
eetin
g m
inut
es
• N
umbe
r of a
genc
ies w
ith a
ctiv
e pa
rtic
ipat
ion
in e
quity
coa
litio
ns
• N
umbe
r of t
rain
ings
on
com
mun
ity
enga
gem
ent f
or re
siden
ts
All
Obj
ectiv
e 4.
2: B
y 20
22, d
ecre
ase
pove
rty
and
incr
ease
lite
racy
and
edu
catio
n, a
nd e
mpl
oym
ent o
ppor
tuni
ties.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Reso
urce
Dev
elop
men
t
Prom
ote
early
chi
ldho
od d
evel
opm
ent a
nd sc
hool
re
adin
ess p
rogr
ams.
Supp
ort s
trat
egie
s for
alte
rnat
ive
educ
atio
n an
d em
ploy
men
t opp
ortu
nitie
s (e.
g., G
ED p
repa
ratio
n su
ppor
ts,
skill
-bui
ldin
g op
port
uniti
es, v
ocat
iona
l or t
rade
scho
ols,
ESL
fo
r adu
lts).
Supp
ort o
ppor
tuni
ties f
or li
ving
wag
e jo
bs.
Incr
ease
affo
rdab
le li
cens
ed c
hild
car
e slo
ts.
Prom
ote
esta
blish
men
t of m
inor
ity-o
wne
d ne
w b
usin
esse
s an
d bu
sines
ses w
ith d
iver
sifie
d em
ploy
ee b
ase.
• N
umbe
r of e
arly
chi
ldho
od d
evel
opm
ent
and
scho
ol re
adin
ess p
rogr
am sl
ots
• N
umbe
r of n
ew st
rate
gies
impl
emen
ted
• N
umbe
r of l
ivin
g w
age
job
initi
ativ
es
• N
umbe
r of a
fford
able
lice
nsed
chi
ld c
are
slots
•
Num
ber o
f new
min
ority
-ow
ned
busin
esse
s •
Impl
emen
tatio
n of
trai
ning
pro
gram
s to
incr
ease
num
ber o
f wor
kers
qua
lifie
d fo
r sk
illed
labo
r job
s (i.e
., te
chno
logy
, fin
ance
)
• M
erce
d Co
unty
Offi
ce o
f Edu
catio
n •
Mer
ced
Coun
ty H
ead
Star
t •
Firs
t 5 M
erce
d Co
unty
•
Mer
ced
Coun
ty D
epar
tmen
t of P
ublic
He
alth
•
Wor
kfor
ce In
vest
men
t Boa
rd
• M
erce
d Co
unty
Hum
an S
ervi
ces A
genc
y •
Busin
ess C
omm
unity
•
Mer
ced
Com
mun
ity C
olle
ge
• Ch
ambe
r of C
omm
erce
•
Com
mun
ity-B
ased
Org
aniza
tions
Febr
uary
201
7 |
41
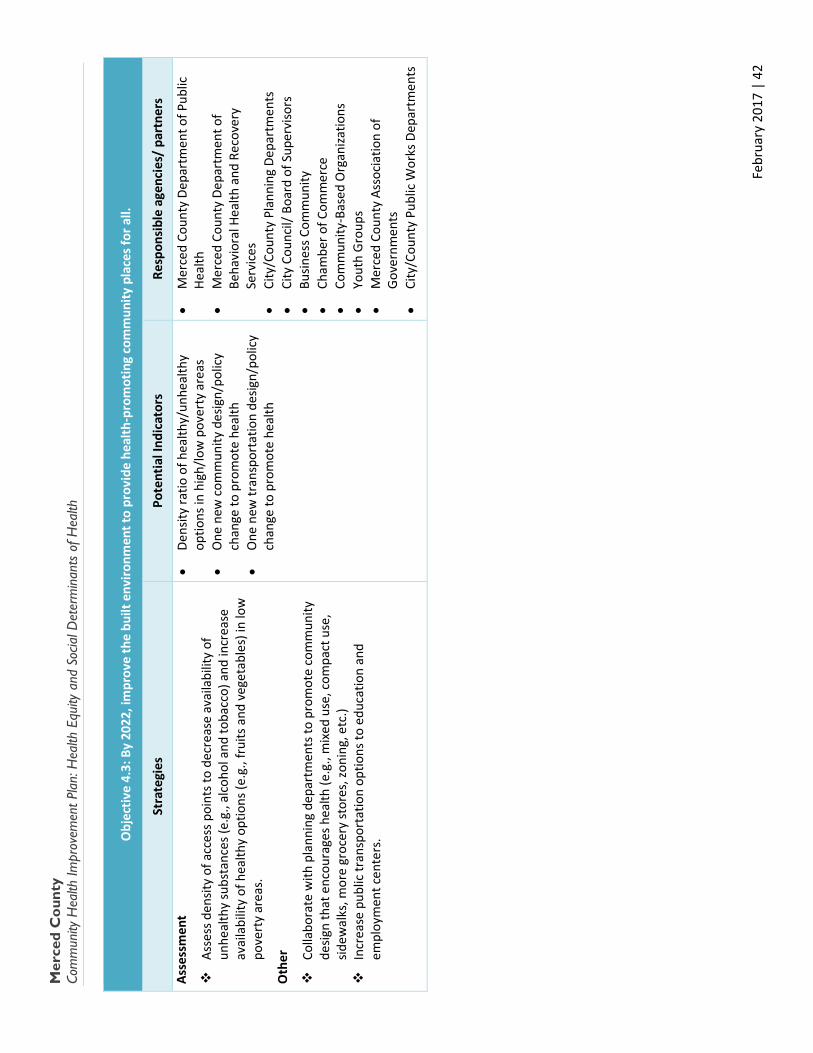
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: H
ealth
Equ
ity a
nd S
ocia
l Det
erm
inan
ts o
f Hea
lth
Obj
ectiv
e 4.
3: B
y 20
22, i
mpr
ove
the
built
env
ironm
ent t
o pr
ovid
e he
alth
-pro
mot
ing
com
mun
ity p
lace
s for
all.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Asse
ssm
ent
Asse
ss d
ensit
y of
acc
ess p
oint
s to
decr
ease
ava
ilabi
lity
of
unhe
alth
y su
bsta
nces
(e.g
., al
coho
l and
toba
cco)
and
incr
ease
av
aila
bilit
y of
hea
lthy
optio
ns (e
.g.,
frui
ts a
nd v
eget
able
s) in
low
po
vert
y ar
eas.
Oth
er
Colla
bora
te w
ith p
lann
ing
depa
rtm
ents
to p
rom
ote
com
mun
ity
desig
n th
at e
ncou
rage
s hea
lth (e
.g.,
mix
ed u
se, c
ompa
ct u
se,
sidew
alks
, mor
e gr
ocer
y st
ores
, zon
ing,
etc
.)
In
crea
se p
ublic
tran
spor
tatio
n op
tions
to e
duca
tion
and
empl
oym
ent c
ente
rs.
• De
nsity
ratio
of h
ealth
y/un
heal
thy
optio
ns in
hig
h/lo
w p
over
ty a
reas
•
One
new
com
mun
ity d
esig
n/po
licy
chan
ge to
pro
mot
e he
alth
•
One
new
tran
spor
tatio
n de
sign/
polic
y ch
ange
to p
rom
ote
heal
th
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• M
erce
d Co
unty
Dep
artm
ent o
f Be
havi
oral
Hea
lth a
nd R
ecov
ery
Serv
ices
•
City
/Cou
nty
Plan
ning
Dep
artm
ents
•
City
Cou
ncil/
Boa
rd o
f Sup
ervi
sors
•
Busin
ess C
omm
unity
•
Cham
ber o
f Com
mer
ce
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
• Yo
uth
Gro
ups
• M
erce
d Co
unty
Ass
ocia
tion
of
Gov
ernm
ents
•
City
/Cou
nty
Publ
ic W
orks
Dep
artm
ents
Febr
uary
201
7 |
42
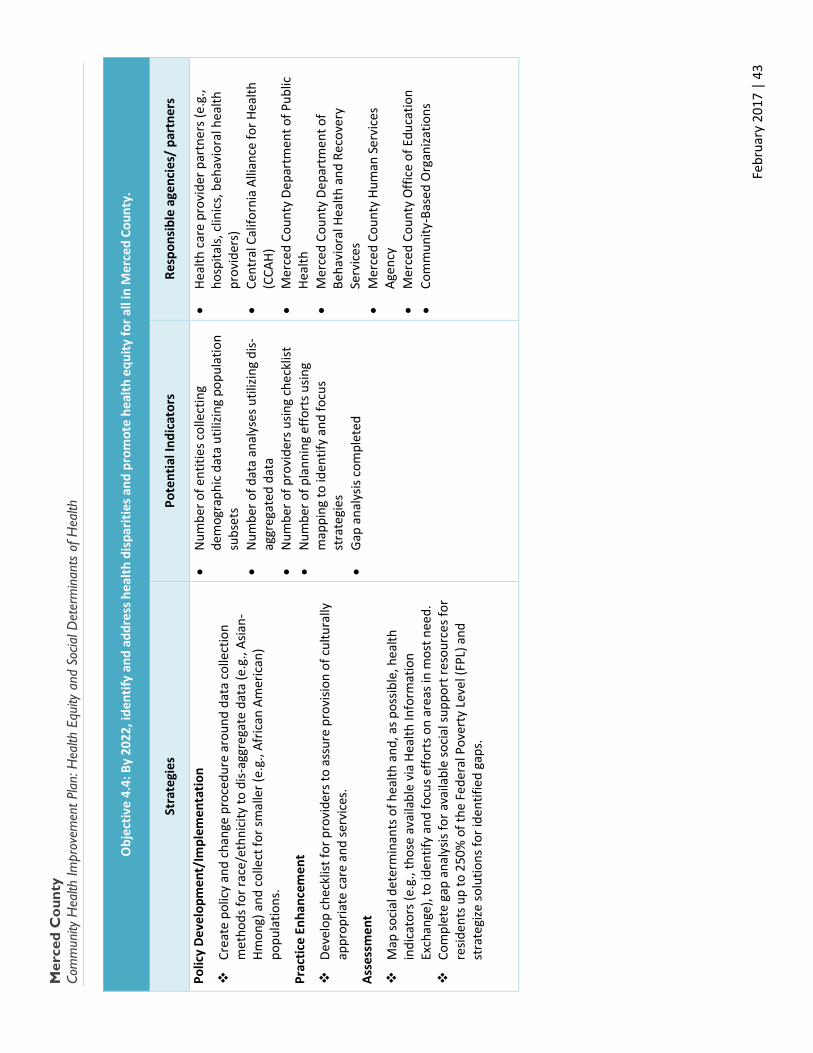
Mer
ced
Cou
nty
Co
mm
unity
Hea
lth Im
prov
emen
t Pla
n: H
ealth
Equ
ity a
nd S
ocia
l Det
erm
inan
ts o
f Hea
lth
Obj
ectiv
e 4.
4: B
y 20
22, i
dent
ify a
nd a
ddre
ss h
ealth
dis
parit
ies a
nd p
rom
ote
heal
th e
quity
for a
ll in
Mer
ced
Coun
ty.
Stra
tegi
es
Pote
ntia
l Ind
icat
ors
Resp
onsi
ble
agen
cies
/ pa
rtne
rs
Polic
y De
velo
pmen
t/Im
plem
enta
tion
Crea
te p
olic
y an
d ch
ange
pro
cedu
re a
roun
d da
ta c
olle
ctio
n m
etho
ds fo
r rac
e/et
hnic
ity to
dis-
aggr
egat
e da
ta (e
.g.,
Asia
n-Hm
ong)
and
col
lect
for s
mal
ler (
e.g.
, Afr
ican
Am
eric
an)
popu
latio
ns.
Prac
tice
Enha
ncem
ent
Deve
lop
chec
klist
for p
rovi
ders
to a
ssur
e pr
ovisi
on o
f cul
tura
lly
appr
opria
te c
are
and
serv
ices
.
Asse
ssm
ent
Map
soci
al d
eter
min
ants
of h
ealth
and
, as p
ossib
le, h
ealth
in
dica
tors
(e.g
., th
ose
avai
labl
e vi
a He
alth
Info
rmat
ion
Exch
ange
), to
iden
tify
and
focu
s effo
rts o
n ar
eas i
n m
ost n
eed.
Co
mpl
ete
gap
anal
ysis
for a
vaila
ble
soci
al su
ppor
t res
ourc
es fo
r re
siden
ts u
p to
250
% o
f the
Fed
eral
Pov
erty
Lev
el (F
PL) a
nd
stra
tegi
ze so
lutio
ns fo
r ide
ntifi
ed g
aps.
• N
umbe
r of e
ntiti
es c
olle
ctin
g de
mog
raph
ic d
ata
utili
zing
popu
latio
n su
bset
s •
Num
ber o
f dat
a an
alys
es u
tilizi
ng d
is-ag
greg
ated
dat
a •
Num
ber o
f pro
vide
rs u
sing
chec
klist
•
Num
ber o
f pla
nnin
g ef
fort
s usin
g m
appi
ng to
iden
tify
and
focu
s st
rate
gies
•
Gap
ana
lysis
com
plet
ed
• He
alth
car
e pr
ovid
er p
artn
ers (
e.g.
, ho
spita
ls, c
linic
s, b
ehav
iora
l hea
lth
prov
ider
s)
• Ce
ntra
l Cal
iforn
ia A
llian
ce fo
r Hea
lth
(CCA
H)
• M
erce
d Co
unty
Dep
artm
ent o
f Pub
lic
Heal
th
• M
erce
d Co
unty
Dep
artm
ent o
f Be
havi
oral
Hea
lth a
nd R
ecov
ery
Serv
ices
•
Mer
ced
Coun
ty H
uman
Ser
vice
s Ag
ency
•
Mer
ced
Coun
ty O
ffice
of E
duca
tion
• Co
mm
unity
-Bas
ed O
rgan
izatio
ns
Febr
uary
201
7 |
43
Merced County Community Health Improvement Plan
This Page Left Intentionally
Blank
February 2017 | 44
Merced County Community Health Improvement Plan
Merced County Community Health Improvement Plan
Appendices
2017 – 2022
February 2017 | 45

Merced County Community Health Improvement Plan
Appendix A: Community Engagement Handouts
February 2017 | 46
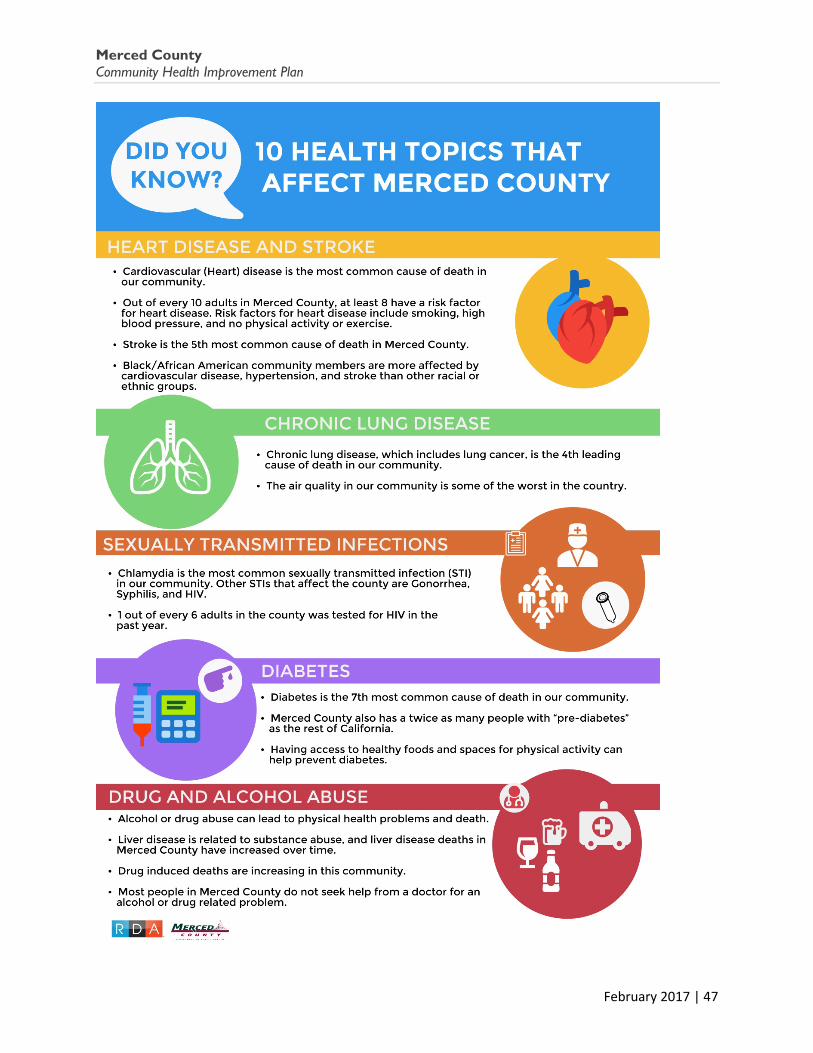
Merced County Community Health Improvement Plan
February 2017 | 47
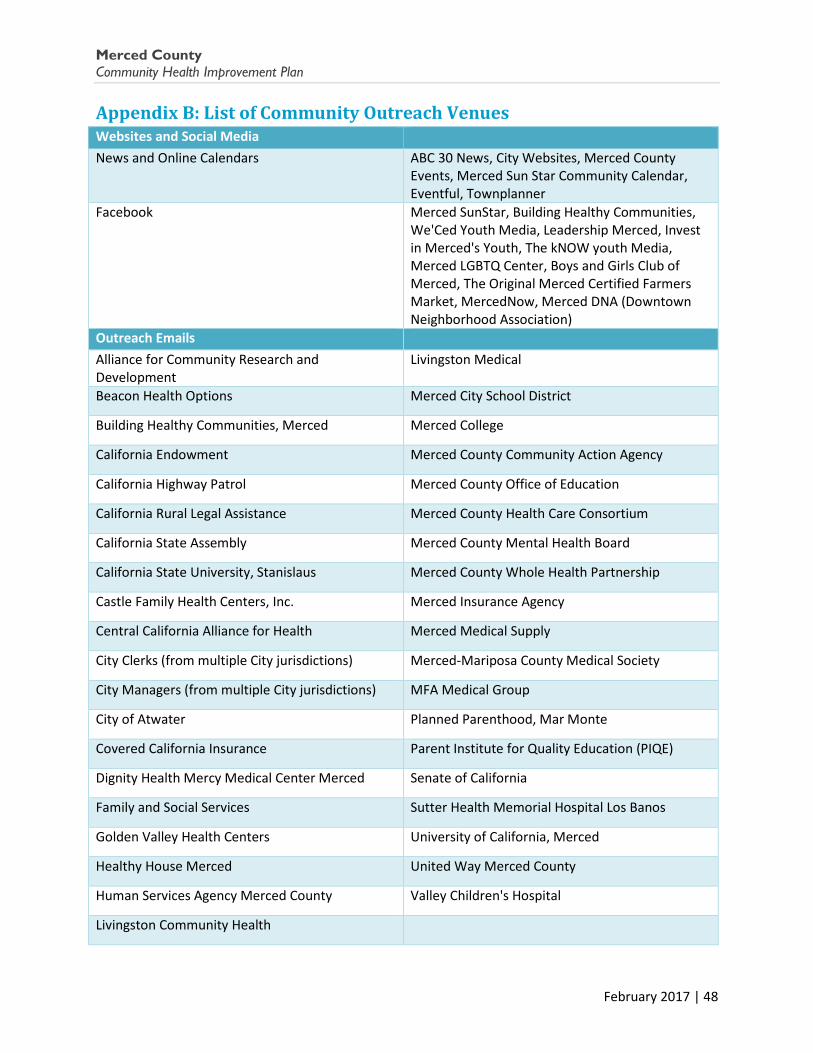
Merced County Community Health Improvement Plan
Appendix B: List of Community Outreach Venues Websites and Social Media
News and Online Calendars ABC 30 News, City Websites, Merced County Events, Merced Sun Star Community Calendar, Eventful, Townplanner
Facebook Merced SunStar, Building Healthy Communities, We'Ced Youth Media, Leadership Merced, Invest in Merced's Youth, The kNOW youth Media, Merced LGBTQ Center, Boys and Girls Club of Merced, The Original Merced Certified Farmers Market, MercedNow, Merced DNA (Downtown Neighborhood Association)
Outreach Emails Alliance for Community Research and Development
Livingston Medical
Beacon Health Options Merced City School District
Building Healthy Communities, Merced Merced College
California Endowment Merced County Community Action Agency
California Highway Patrol Merced County Office of Education
California Rural Legal Assistance Merced County Health Care Consortium
California State Assembly Merced County Mental Health Board
California State University, Stanislaus Merced County Whole Health Partnership
Castle Family Health Centers, Inc. Merced Insurance Agency
Central California Alliance for Health Merced Medical Supply
City Clerks (from multiple City jurisdictions) Merced-Mariposa County Medical Society
City Managers (from multiple City jurisdictions) MFA Medical Group
City of Atwater Planned Parenthood, Mar Monte
Covered California Insurance Parent Institute for Quality Education (PIQE)
Dignity Health Mercy Medical Center Merced Senate of California
Family and Social Services Sutter Health Memorial Hospital Los Banos
Golden Valley Health Centers University of California, Merced
Healthy House Merced United Way Merced County
Human Services Agency Merced County Valley Children's Hospital
Livingston Community Health
February 2017 | 48
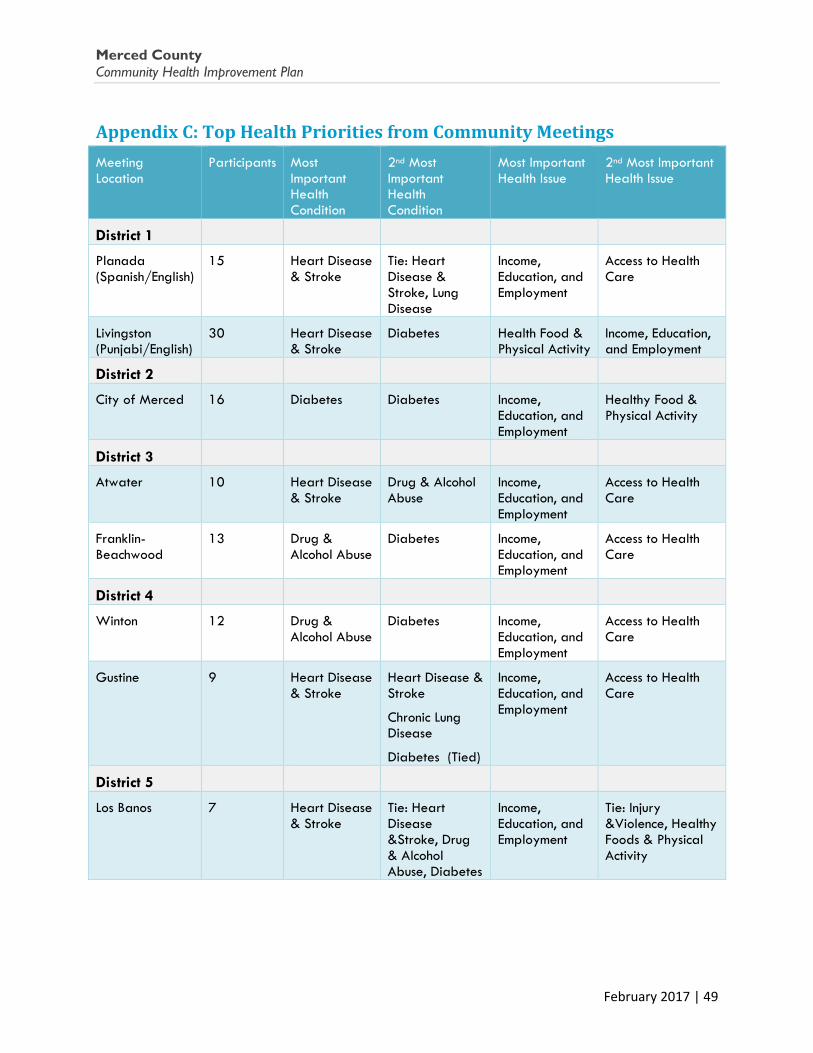
Merced County Community Health Improvement Plan
Appendix C: Top Health Priorities from Community Meetings Meeting Location
Participants Most Important Health Condition
2nd Most Important Health Condition
Most Important Health Issue
2nd Most Important Health Issue
District 1
Planada (Spanish/English)
15 Heart Disease & Stroke
Tie: Heart Disease & Stroke, Lung Disease
Income, Education, and Employment
Access to Health Care
Livingston (Punjabi/English)
30 Heart Disease & Stroke
Diabetes Health Food & Physical Activity
Income, Education, and Employment
District 2
City of Merced 16 Diabetes Diabetes Income, Education, and Employment
Healthy Food & Physical Activity
District 3
Atwater 10 Heart Disease & Stroke
Drug & Alcohol Abuse
Income, Education, and Employment
Access to Health Care
Franklin-Beachwood
13 Drug & Alcohol Abuse
Diabetes Income, Education, and Employment
Access to Health Care
District 4
Winton 12 Drug & Alcohol Abuse
Diabetes
Income, Education, and Employment
Access to Health Care
Gustine 9 Heart Disease & Stroke
Heart Disease & Stroke
Chronic Lung Disease
Diabetes (Tied)
Income, Education, and Employment
Access to Health Care
District 5
Los Banos 7 Heart Disease & Stroke
Tie: Heart Disease &Stroke, Drug & Alcohol Abuse, Diabetes
Income, Education, and Employment
Tie: Injury &Violence, Healthy Foods & Physical Activity
February 2017 | 49
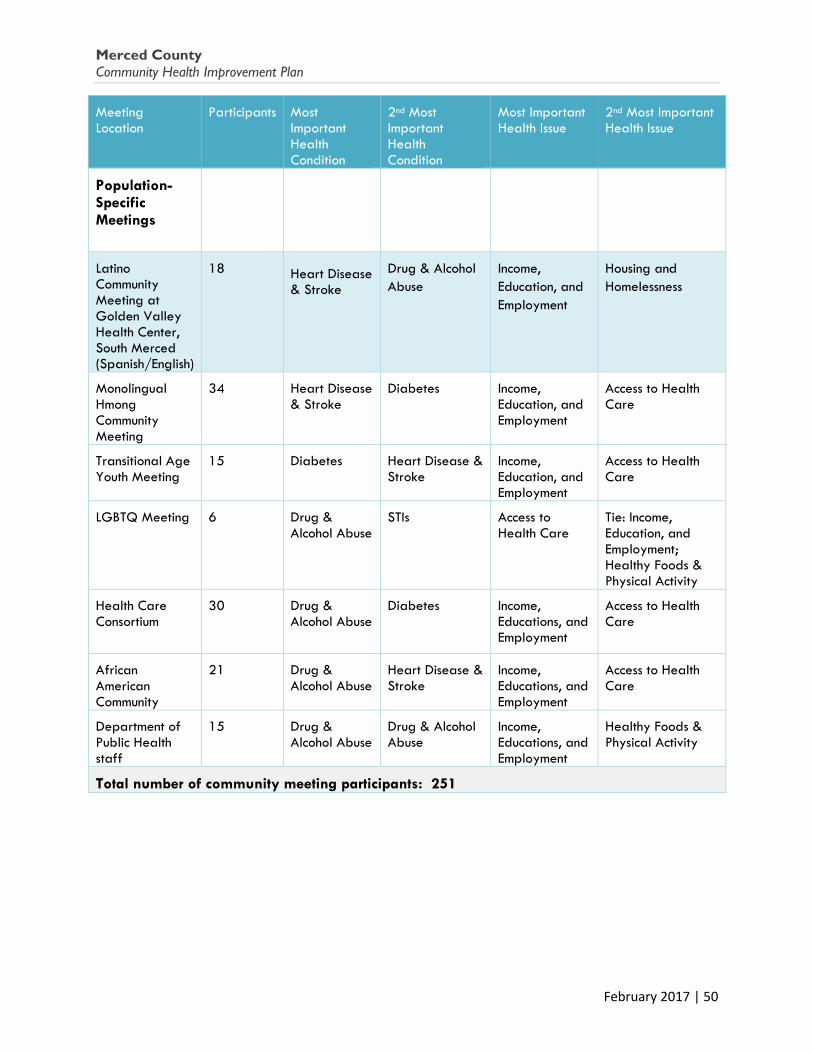
Merced County Community Health Improvement Plan
Meeting Location
Participants Most Important Health Condition
2nd Most Important Health Condition
Most Important Health Issue
2nd Most Important Health Issue
Population-Specific Meetings
Latino Community Meeting at Golden Valley Health Center, South Merced (Spanish/English)
18 Heart Disease & Stroke
Drug & Alcohol Abuse
Income, Education, and Employment
Housing and Homelessness
Monolingual Hmong Community Meeting
34 Heart Disease & Stroke
Diabetes Income, Education, and Employment
Access to Health Care
Transitional Age Youth Meeting
15 Diabetes Heart Disease & Stroke
Income, Education, and Employment
Access to Health Care
LGBTQ Meeting 6 Drug & Alcohol Abuse
STIs Access to Health Care
Tie: Income, Education, and Employment; Healthy Foods & Physical Activity
Health Care Consortium
30 Drug & Alcohol Abuse
Diabetes Income, Educations, and Employment
Access to Health Care
African American Community
21 Drug & Alcohol Abuse
Heart Disease & Stroke
Income, Educations, and Employment
Access to Health Care
Department of Public Health staff
15 Drug & Alcohol Abuse
Drug & Alcohol Abuse
Income, Educations, and Employment
Healthy Foods & Physical Activity
Total number of community meeting participants: 251
February 2017 | 50
Merced County Community Health Improvement Plan
This Page Left Intentionally
Blank
February 2017 | 51
The Many Faces of Merced County
Merced County
Community Health Improvement Plan
www.countyofmerced.com/publichealth Resource Development Associates