Embed Size (px)
Citation preview
Specialized, same-day or ongoing treatment for a range of conditions.
A staff of compassionate, highly trained physicians, nurses and technicians provide timely, personal treatment in a convenient outpatient setting.
HEAL ING CENTER
MERCY HEALING CENTER
Hours:• Monday through Friday » Infusion related patient care needs 7 a.m. to 5:30 p.m. » Wound Clinic physician visits from 8 a.m. to 4:30 p.m; some openings earlier if physician available
• Saturday and Sunday 7 a.m. to 7:30 p.m.
• Holidays 7 a.m. to 3:30 p.m.
About the Healing Center:• For non-urgent/emergent care• Specially-trained nursing staff providing healing center care and physician oversight provided for wound treatments• We accept same-day add-ons based on availability of appointments
Authorizations• Ordering physician’s office must obtain any insurance prior authorizations for services or medications administered• The Healing Center will obtain authorizations for services we order directly for patients or those managed by a wound care physician
See reverse for our list of services.
Phone: (319) 398-6400Fax: (319) 221-8496
MERCY HEALING CENTER – OUR SERVICES:Infusion Clinic
• Hydration infusions• Blood transfusions• Antibiotic infusions• Wound dressings• Wound vac dressing changes• Specialty infusions related to certain disease processes• Urinary catheterizations• Specialty injections related to certain disease processes• Port flushes• PICC line dressing changes• PICC line laboratory draws• Total contact casting application/removal• Outpatient wound/ostomy nurse evaluations• Phlebotomy
Wound Clinic
• Physician initial visits• Physician follow up visits• Hyperbaric Oxygen therapy work up• Hyperbaric Oxygen therapy treatments• Compression garment application• Lower extremity non- invasive circulation testing• Lower extremity/foot assessments• Total Contact Casting application• Wound vac application and management• Must have an open wound• Focus is on chronic non-healing wounds not acute wounds
Physician referral required for these services.
R. Matthew Smith, MD
Nathaly François, MD
Jeremiah Murphy, MD
Mercy Urology Clinic has moved to the Hall-Perrine Cancer Center
Mercy’s Urology Clinic provides medical and surgical care for male and female patients, and selected services for pediatric patients, who suffer from problems of the urinary tract, as well as diseases and conditions of the male genital and reproductive organs.
Meet Our Urologists:
How To Schedule In EPICProviders with EPIC ambulatory available in your clinic, please make your referral within EPIC under: Amb Referral to UROLOGY
Providers without EPIC, please call Mercy Urology Clinic at (319) 398-6865 or fax referral to (319) 398-6635.
R. Matthew Smith, MDUrologist
Nathaly François, MDUrologist
Jeremiah Murphy, MDUrologist
NEW
LOCA
TION
UROLOGIC CANCER TREATMENTü Prostate cancerü Bladder cancerü Kidney cancerü Testicular and penile cancerü Adrenal cancer
DISORDERS OF URINATIONü Urinary leakageü Overactive bladderü Prostatic enlargementü Recurrent urinary tract infections
PROSTATE DISORDERSü Benign Prostatic Hyperplasia (BPH)ü Prostatitis
KIDNEY STONESü Treatment and prevention
URINARY STRICTURE DISEASEü Ureteropelvic Junction Obstruction (UPJ)ü Ureteral strictureü Urethral stricture
INFERTILITY (MALE)SEXUAL DYSFUNCTION (MALE)ü Erectile Dysfunction (ED)ü Penile Curvature (Peyronie’s Disease)
VARICOCELE
HYDROCELE
CIRCUMCISIONS
HYPOGONADISM
568-1949 3/18
For more information please contact Stacy Pohlman, RN, Nurse Manager, at (319) 398-6865, email [email protected], or visit www.mercycare.org/Urology701 10th Street SE | Level 2 within Hall-Perrine Cancer Center | Cedar Rapids, IA 52403 Phone: (319) 398-6865 | Fax: (319) 398-6635 | www.mercycare.org/Urology
Conditions We Treat
ü Cystoscopyü Diagnosticü Bladder Biopsyü Bladder Fulgurationü Botox Injectionü Stent Removalü Urethral Dilationü Difficult Catheter Placementü Urethral Bulking Agents (macroplastique)ü Urodynamics
• Post Void Residual (PVR) testing• Uroflow• Cystometrogram (CMG)
UROLOGIC ULTRASOUNDü Prostate, kidney, scrotal and penile ultrasoundü Ultrasound guided biopsy of the prostate (TRUS biopsy)
CATHETER CHANGESü Urethral and supra pubic cathetersü Self-catheterization teaching
BLADDER INSTILLATIONSü Bladder cancerü Intersitial cystitis / Bladder pain syndromeü Antibiotic instillation
HORMONE INJECTIONS FOR PROSTATE CANCER
PENILE INJECTIONS
NERVE STIMULATIONü Percutaneous Tibial Nerve Stimulation (PTNS)ü Percutaneous Nerve Evaluation (PNE)
REMOVAL OF GENITAL LESIONS
VASECTOMY - MINIMALLY INVASIVE“NO-SCALPEL” IN OFFICE.
Clinic Procedures
Our urologists perform advanced robotic surgery including laparoscopic, endoscopic and lasers, providing patients with a minimally invasive approach and faster recovery time.
ENDOSCOPIC PROCEDURES ü Bladder, Prostate and Urethraü Cystosocopy – to diagnose cancers and
abnormalities of the lower urinary tractü Bladder and urethral biopsyü Removal of bladder tumors (TURBT)ü Destruction of bladder lesions (fulguration)ü Opening of narrow urethra (DVIU)ü Bladder chemotherapy instillation (Mitomycin)ü Removal of enlarged prostate tissue (TURP)
• Bipolar TURP• Laser TURP (Photovaporization)
ü Urethral bulking agentsü Botox injection
ü Ureteroscopy – visualizing the upper urinary tract (kidney and ureter) for stone procedures as well as to diagnose strictures or masses in these areas
STONE REMOVAL PROCEDURESü Removal of stones in bladder (cystolithalopaxy)ü Removal of stones in ureter and kidney
• Shock Wave treatment (ESWL)• Ureteroscopy – using a laser to break up and
remove stone• Percutaneous stone removal – using a small
hole in your back to remove larger stones
SCROTAL / PENILE PROCEDURESü Circumcision (young boys (older than 6 months)
through adulthood)ü Revision circumcision (typically in young boys with an
incomplete circumcision at birth)ü Penile exploration – for trauma to the penisü Testicular removal (orchiectomy) for cancer
ü Hydrocele removalü Removal of epididymal cysts or entire epididymisü Removal of tumors in spermatic cordü Varicocele repair
UROLOGIC IMPLANT SURGERYü Penile implants for erectile dysfunctionü Artificial sphincter for severe incontinenceü Sling surgery (men and women) for incontinence
CANCER SURGERYü Prostatectomy (prostate cancer)ü Nephrectomy (kidney cancer)
• Full removal (radical), as well as partial removal (kidney sparing surgery)
ü Adrenalectomy (removal of adrenal glands)ü Orchiectomy (removal of testicular tumor)
*** The above surgery can be performed robotically in most situations.
Surgical Procedures
Cedar Rapids Medical Education Foundation
Counting Medical Education Courses
April 2018
Page 1 of 1 4/3/2018
DATE TOPIC PRESENTOR(S)
Tues. 4/24 1200 – CRMEF – Visiting Professor Program
Topic: Pediatric and Adolescent Gynecology
Speaker: Joshua Kapfhamer, MD
University of Iowa
ACCREDITATION * The Cedar Rapids Medical Education Foundation is accredited by the Iowa Medical Society (IMS) to provide continuing medical education for physicians.
+ The Cedar Rapids Medical Education Foundation designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit ™. Physicians should only claim credit commensurate with their participation in the activity.
CONFLICT OF INTEREST As a sponsor accredited by the Iowa Medical Society, the Cedar Rapids Medical Education Program must assure balance, independence, objectivity and scientific rigor in all its individually sponsored or jointly sponsored educational activities. All faculty participating in a sponsored activity are expected to disclose to the activity audience any significant financial interest or other relationship (1) with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in an educational presentation and (2) with any commercial supporters of the activity (significant financial interest or other relationship can include such things as grants, or research support, employee, consultant, major stock holder, member of speakers bureau, etc.) The intent of this disclosure is not to prevent a speaker with a significant financial or other relationship from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for the audience to determine whether the speaker’s interests or relationship may influence the presentation with regard to exposition or conclusion. Disclosure forms for each presenter are on file in the CME office. Participants interested in viewing copies may write the CME Office, including a self-addressed, stamped envelope. Please write to: Continuing Medical Education Office, Cedar Rapids Medical Education Foundation, 1260 2nd Avenue, SE, Cedar Rapids, IA 52403. DURING PRESENTATIONS THERE ARE OCCASIONALLY DISCUSSIONS OF UNAPPROVED USE OF FDA APPROVED DRUGS, DEVICES OR
TREATMENTS. THIS MUST BE DISCLOSED TO THE AUDIENCE DURING THE LECTURE.
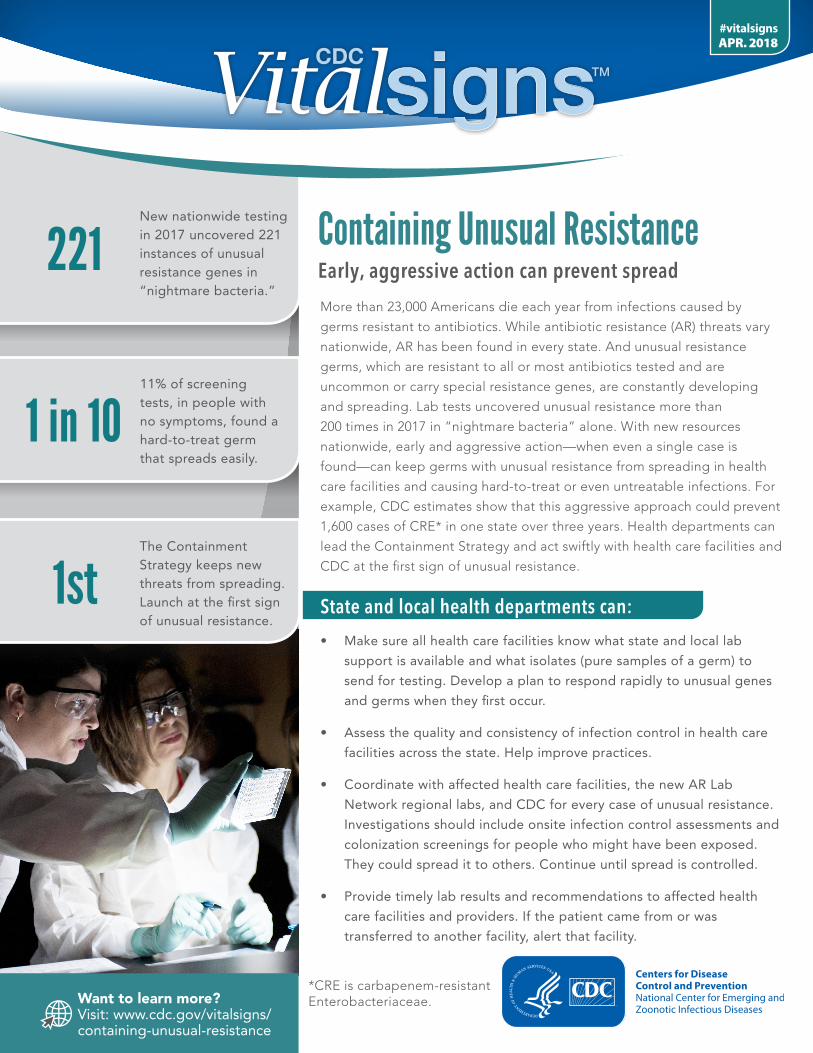
11% of screening tests, in people with no symptoms, found a hard-to-treat germ that spreads easily.
The Containment Strategy keeps new threats from spreading. Launch at the first sign of unusual resistance.
1 in 10
1st
221New nationwide testing in 2017 uncovered 221 instances of unusual resistance genes in “nightmare bacteria.”
Want to learn more? Visit: www.cdc.gov/vitalsigns/containing-unusual-resistance
APR. 2018#vitalsigns
Containing Unusual ResistanceEarly, aggressive action can prevent spread
More than 23,000 Americans die each year from infections caused by
germs resistant to antibiotics. While antibiotic resistance (AR) threats vary
nationwide, AR has been found in every state. And unusual resistance
germs, which are resistant to all or most antibiotics tested and are
uncommon or carry special resistance genes, are constantly developing
and spreading. Lab tests uncovered unusual resistance more than
200 times in 2017 in “nightmare bacteria” alone. With new resources
nationwide, early and aggressive action—when even a single case is
found—can keep germs with unusual resistance from spreading in health
care facilities and causing hard-to-treat or even untreatable infections. For
example, CDC estimates show that this aggressive approach could prevent
1,600 cases of CRE* in one state over three years. Health departments can
lead the Containment Strategy and act swiftly with health care facilities and
CDC at the first sign of unusual resistance.
State and local health departments can:
• Make sure all health care facilities know what state and local lab
support is available and what isolates (pure samples of a germ) to
send for testing. Develop a plan to respond rapidly to unusual genes
and germs when they first occur.
• Assess the quality and consistency of infection control in health care
facilities across the state. Help improve practices.
• Coordinate with affected health care facilities, the new AR Lab
Network regional labs, and CDC for every case of unusual resistance.
Investigations should include onsite infection control assessments and
colonization screenings for people who might have been exposed.
They could spread it to others. Continue until spread is controlled.
• Provide timely lab results and recommendations to affected health
care facilities and providers. If the patient came from or was
transferred to another facility, alert that facility.
*CRE is carbapenem-resistantEnterobacteriaceae.
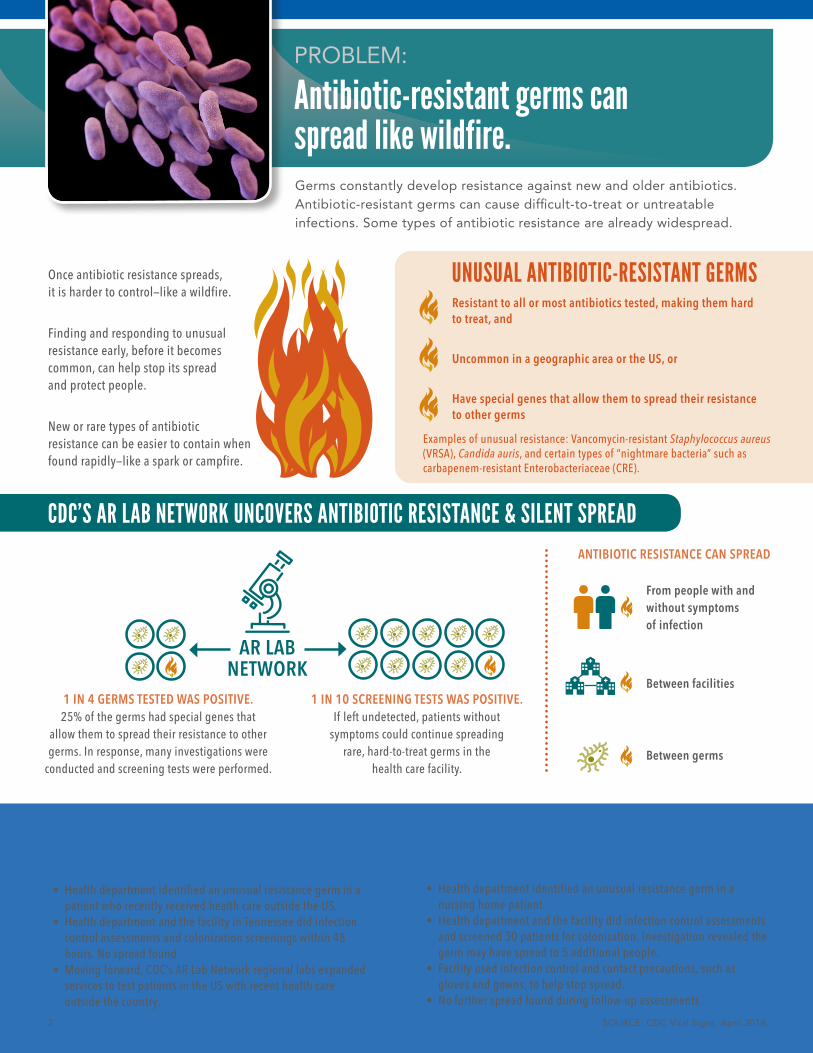
Germs constantly develop resistance against new and older antibiotics. Antibiotic-resistant germs can cause difficult-to-treat or untreatable infections. Some types of antibiotic resistance are already widespread.
PREVENTING AN UNUSUAL ANTIBIOTIC RESISTANCE WILDFIRE
CDC’S AR LAB NETWORK UNCOVERS ANTIBIOTIC RESISTANCE & SILENT SPREAD
UNUSUAL ANTIBIOTIC-RESISTANT GERMS
Rapid Response in Tennessee
AR LABNETWORK
Ongoing Vigilance in Iowa
PROBLEM:
Antibiotic-resistant germs can spread like wildfire.
SOURCE: CDC Vital Signs, April 2018.2
• Health department identified an unusual resistance germ in apatient who recently received health care outside the US.
• Health department and the facility in Tennessee did infectioncontrol assessments and colonization screenings within 48 hours. No spread found.
• Moving forward, CDC’s AR Lab Network regional labs expandedservices to test patients in the US with recent health care outside the country.
• Health department identified an unusual resistance germ in anursing home patient.
• Health department and the facility did infection control assessments and screened 30 patients for colonization. Investigation revealed thegerm may have spread to 5 additional people.
• Facility used infection control and contact precautions, such asgloves and gowns, to help stop spread.
• No further spread found during follow-up assessments.
Resistant to all or most antibiotics tested, making them hard to treat, and
Uncommon in a geographic area or the US, or
Have special genes that allow them to spread their resistance to other germs
Examples of unusual resistance: Vancomycin-resistant Staphylococcus aureus (VRSA), Candida auris, and certain types of “nightmare bacteria” such as carbapenem-resistant Enterobacteriaceae (CRE).
Once antibiotic resistance spreads, it is harder to control—like a wildfire.
Finding and responding to unusual resistance early, before it becomes common, can help stop its spread and protect people.
New or rare types of antibiotic resistance can be easier to contain when found rapidly—like a spark or campfire.
1 IN 4 GERMS TESTED WAS POSITIVE. 25% of the germs had special genes that
allow them to spread their resistance to other germs. In response, many investigations were
conducted and screening tests were performed.
1 IN 10 SCREENING TESTS WAS POSITIVE. If left undetected, patients without
symptoms could continue spreading rare, hard-to-treat germs in the
health care facility.
From people with and without symptoms of infection
Between facilities
Between germs
ANTIBIOTIC RESISTANCE CAN SPREAD
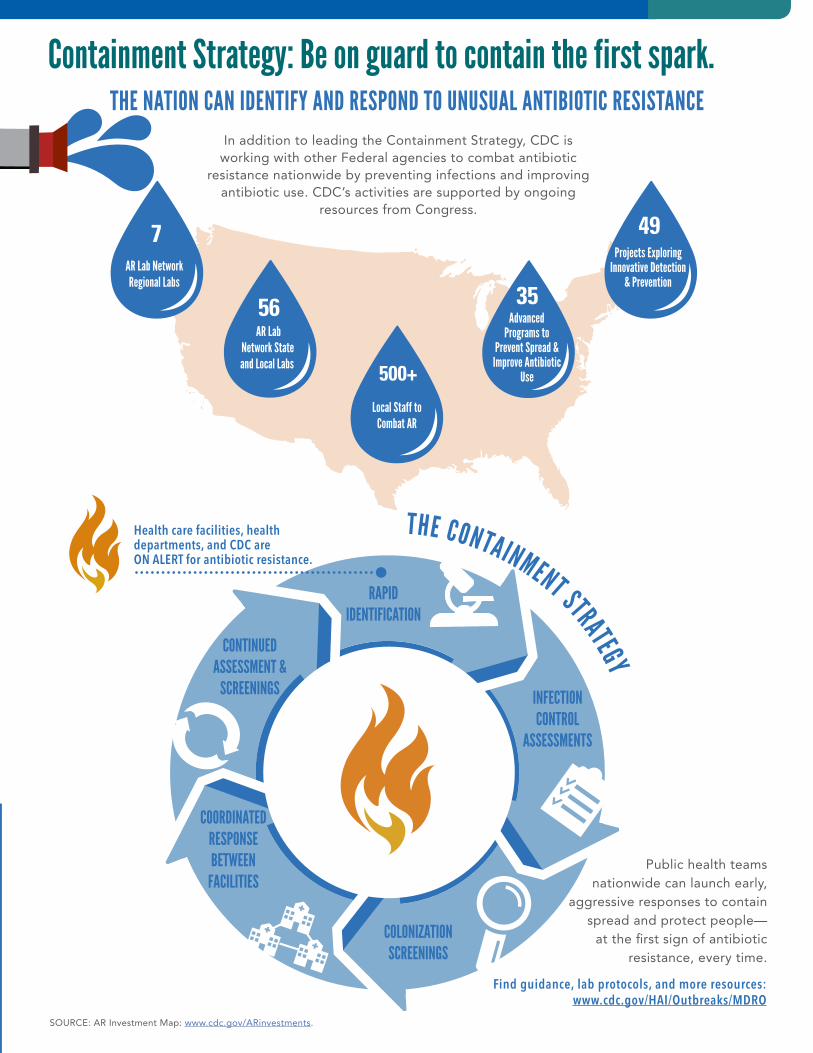
49Projects Exploring
Innovative Detection & Prevention
500+ Local Staff to
Combat AR
7AR Lab Network Regional Labs
56AR Lab
Network State and Local Labs
500+ 35Advanced
Programs to Prevent Spread &
Improve Antibiotic Use
Public health teams nationwide can launch early,
aggressive responses to contain spread and protect people—
at the first sign of antibiotic resistance, every time.
PREVENTING AN UNUSUAL ANTIBIOTIC RESISTANCE WILDFIRE
Containment Strategy: Be on guard to contain the first spark.THE NATION CAN IDENTIFY AND RESPOND TO UNUSUAL ANTIBIOTIC RESISTANCE
SOURCE: AR Investment Map: www.cdc.gov/ARinvestments.
Health care facilities, health departments, and CDC are ON ALERT for antibiotic resistance.
In addition to leading the Containment Strategy, CDC is working with other Federal agencies to combat antibiotic
resistance nationwide by preventing infections and improving antibiotic use. CDC’s activities are supported by ongoing
resources from Congress.
Find guidance, lab protocols, and more resources: www.cdc.gov/HAI/Outbreaks/MDRO
INFECTION CONTROL
ASSESSMENTS
COLONIZATION SCREENINGS
COORDINATED RESPONSE BETWEEN
FACILITIES
RAPID IDENTIFICATION
CONTINUED ASSESSMENT &
SCREENINGS
THE CONTAINMENT STRATEGY
THE FEDERAL GOVERNMENT IS:• Monitoring resistance and sounding the alarm when
threats emerge. CDC develops and provides new lab tests so health departments can quickly identify new threats.
• Improving identification through CDC’s new AR Lab Network in all 50 states, 5 large cities, and Puerto Rico, including 7 regional labs and a national tuberculosis lab for specialty testing.
• Supporting prevention experts and programs in every state, and providing data and recommendations for local prevention and response.
• Testing innovative infection control and prevention strategies with health care and academic partners.
STATE AND LOCAL HEALTH DEPARTMENTS AND LABS CAN:• Make sure all health care facilities know what state
and local lab support is available and what isolates (pure samples of a germ) to send for testing. Develop a plan to respond rapidly to unusual genes and germs when they first appear.
• Assess the quality and consistency of infection control in health care facilities across the state, especially in facilities with high-risk patients and long stays. Help improve practices.
• Coordinate with affected health care facilities, the new AR Lab Network regional lab, and CDC for every case of unusual resistance. Investigations should include onsite infection control assessments to find spread. Consider colonization screenings. Continue until spread is controlled.
• Provide timely lab results and recommendations to affected health care facilities and providers. If the patient came from or was transferred to another facility, alert that facility.
• Find resources: www.cdc.gov/hai/outbreaks/mdro
HEALTH CARE FACILITIES CAN:• Plan for unusual resistance arriving in your facility.
Find resources: www.cdc.gov/hai/outbreaks/mdro
• Leadership: Work with the health department to stop spread of unusual resistance. Review and support infection control in the facility.
• Clinical labs: Know what isolates to send for testing. Establish protocols that immediately notify the health department, healthcare provider, and infection control staff of unusual resistance. Validate new tests to identify the latest threats. If needed, use isolates from www.cdc.gov/ARIsolateBank.
• Healthcare providers, epidemiologists, and infection control staff: Place patients with unusual resistance on contact precautions, assess and enhance infection control, and work with the health department to screen others. Communicate about status when patients are transferred. Continue infection control assessments and colonization screenings until spread is controlled. Ask about any recent travel or health care to identify at-risk patients.
EVERYONE CAN:• Inform your healthcare provider if you recently
received health care in another country or facility.
• Talk to your healthcare provider about preventing infections, taking good care of chronic conditions and getting recommended vaccines.
• Practice good hygiene, such as keeping hands clean with handwashing or alcohol-based hand rubs, and keep cuts clean until healed.
CS286967A
For more information, please contact Telephone: 1-800-CDC-INFO (232-4636) TTY: 1-888-232-6348 | Web: www.cdc.gov
Centers for Disease Control and Prevention1600 Clifton Road NE, Atlanta, GA 30333Publication date: April 3, 2018
www.cdc.gov/vitalsigns/containing-unusual-resistancewww.cdc.gov/mmwr
WHAT CAN BE DONE
MERCY– INTERPRETIVE SERVICES
Hospitals are required by both law and regulation to ensure effective communication with our patient and visitors. Communication expectations:
• Patients and their companions will not be excluded, denied services, segregated or otherwise treated differently than other individuals because of the absence of auxiliary aids or services
• Patients and/or companions shall be offered auxiliary aids and services, including interpretive services free of charge
• The use of family members and other companions as interpreters shall be prohibited in non-emergency situations and discouraged in all situations
• Interpretive services are available 24/7 • Interpretive services should be provided by a qualified medical interpreter
o Bilingual or multilingual staff or providers should not serve as a medical interpreter without formal training
Please document when an interpretive service is used to communicate with your patient. • “Health history obtained using MARTTI.” • “In-person interpreter used to communicate with patient.”
What does Mercy Medical Center have available for interpretive services?
• MARTTI – video remote interpretive service • In person interpreters • Over- the- phone interpretive service • Limited number of translated documents
What does MercyCare Community Physicians have available for interpretive services?
• In person interpreters • Working on availability of over-the-phone interpretive service
What are the top languages requested through one of Mercy’s interpretive services?
1. Spanish 2. American Sign Language 3. French 4. Swahili 5. Arabic 6. Mandarin
In 2017, there were over 30 languages spoken at Mercy Medical Center and approximately 1900 calls or visits through one of Mercy’s interpretive services offerings