-
REVIEWAND PERSPECTIVES
Mesenchymal tumours of the mediastinumpart II
Michael A. den Bakker1,2 & Alexander Marx3 & Kiyoshi
Mukai4 & Philipp Strbel5
Received: 24 June 2015 /Revised: 6 August 2015 /Accepted: 11
August 2015# The Author(s) 2015. This article is published with
open access at Springerlink.com
Abstract This is the second part of a two-part review on
softtissue tumours whichmay be encountered in the mediastinum.This
review is based on the 2013 WHO classification of softtissue
tumours and the 2015WHO classification of tumours ofthe lung,
pleura, thymus and heart and provides an updatedoverview of
mesenchymal tumours that have been reported inthe mediastinum.
Keywords Mediastinum .Mesenchymal tumours .Soft
tissuetumours
Introduction
In this second part of a two-part review, the 2013 WHO
clas-sification of soft tissue tumours and the 2015 WHO
classifi-cation of tumours of the thymus form the basis to
summarizecurrent knowledge about soft tissue tumours in the
mediasti-num. This comprehensive review covers published
reportsfrom the English and Japanese literature. In the first of
thesereviews, general aspects, adipocytic, fibroblastic/
myofibroblastic, fibrohistiocytic tumours and soft tissue
tu-mours arising as somatic components in germ cell tumours,were
discussed. We now turn to mediastinal smooth muscle,skeletal
muscle, vascular, chondro-osseous, nerve sheath andmiscellaneous
tumours of uncertain differentiation, includingundifferentiated
sarcomas. Since most of the tumours de-scribed here closely
resemble soft tissue tumours elsewherein the body, we will focus
our review on defining criteria,epidemiology, clinical findings and
prognosis, rather than his-tological descriptions. For in-depth
coverage of the histologi-cal aspects of these tumours, the reader
is referred to specificliterature.
Smooth muscle tumours
Smooth muscle cell tumours resemble normal smooth muscleand
retain many of their immunohistochemical markers. Few-er benign
smooth muscle cell tumours (leiomyomas) than ma-lignant smooth
muscle tumours (leiomyosarcomas) have beenreported in the
mediastinum.
To qualify as a primary mediastinal leiomyoma, tumoursshould
arise from the somatic soft tissue of the mediastinum,whilst
esophageal and large vessel primaries should be ex-cluded. If these
criteria are applied, primary mediastinalleiomyoma is very rare
with approximately 20 reported casesin the literature [14, 19, 136,
139, 149, 162, 180, 205, 227].Mediastinal leiomyoma is twice as
common in females as inmales and is mainly seen in the posterior
mediastinum of olderadults (age range 2375 years; median age 50
years). Thesetumours may remain asymptomatic, or patients may
complainof dyspnea or chest pain. The tumours may grow to a
largesize (up to 1,600 g). The morphology of mediastinalleiomyoma
is similar to its counterparts elsewhere in the bodyand is defined
as a neoplasm resembling normal smooth mus-cle cells and devoid of
pleomorphism and necrosis and with a
* Michael A. den [email protected]
1 Department of Pathology, Maasstad Ziekenhuis, PO Box
9100,3007, AC Rotterdam, The Netherlands
2 Department of Pathology, ErasmusMC, Rotterdam, The
Netherlands3 Institute of Pathology, University Medical Center
Mannheim,
University of Heidelberg, Heidelberg, Germany4 Department of
Diagnostic Pathology, Saiseikai Central Hospital,
Tokyo, Japan5 Department of Pathology, Universittsmedizin
Gttingen,
Gttingen, Germany
Virchows ArchDOI 10.1007/s00428-015-1832-6
- very low mitotic rate (
-
The differential diagnosis of the rare primary
mediastinalrhabdomyosarcoma is the much more common
rhabdomyo-sarcoma as a component of a germ cell tumour [23, 35,
69,120]. In germ cell tumours with somatic-type malignancy,
theprognosis is determined by the somatic (i.e.
sarcomatous)component and in the setting of rhabdomyosarcoma is
dismal.Rhabdomyoblastic differentiation has been reported in
bothlow-grade (thymoma) [29, 129, 174] and high-grade
(thymiccarcinoma, carcinosarcoma) [41, 48, 145] thymic
epithelialtumours and thus enters the differential diagnosis of
rhabdo-myosarcoma [29, 41, 48, 129, 145, 174]. Identification of
anepithelial component by appropriate immunohistochemicalstaining
will aid the accurate diagnosis. Rhabdomyoblasticdifferentiation
may also occur in MPNST, which are thencalled malignant Triton
tumours. Nine cases have been report-ed in the mediastinum
(reviewed by Ren et al. [166]). Thetypical spindle cell
MPSNTcomponent usually predominates,whilst cells with
rhabdomyoblastic differentiation commonlyform a minor component of
the tumour. These tumours carry avery poor prognosis.
Vascular tumours
Amongst mesenchymal neoplasms in the mediastinum, vas-cular
(endothelial) tumours are not uncommon with well over100 cases
reported in the literature.
Benign and intermediate-grade vascular tumours
Benign blood vessel tumours (hemangioma variants) havebeen
reported as individual cases and have been summarizedin several
reviews [32, 39, 127, 130]. Endothelial tumours ofintermediate
grade (hemangioendotheliomas) are character-ized by local
infiltrative growth and rare metastases.
Mediastinal hemangiomamay originate in the soft tissue ofthe
mediastinum or may arise in the thymus [5, 32, 154].Mediastinal
hemangiomas span a wide age range, from thenewborn to the elderly,
with most cases occurring in youngadults. Of the reported cases,
5075 % were located in theanterior mediastinum [32, 130]. Up to 50
% of cases wereasymptomatic. Patients with symptomatic tumours
presentedwith pain, cough and rarely with signs of compression of
vitalstructures by the tumour, such as Horners syndrome,
neuro-logical signs and superior vena cava obstruction [32].
Tumoursize ranged from a few centimetres to 20 cm [32, 130]
andincluded both capillary and cavernous hemangioma subtypes.In the
series by Moran and Suster, associated histological fea-tures
included fatty metaplasia, fibrosis, smooth muscle over-growth and
inflammation [130]. Surgical resection is curativein most cases,
although recurrence may rarely occur [32].
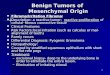
Lymphangioma has been reported as a cystic mass in
themediastinum of children and is very uncommon in adults
(Fig. 1) [61, 147, 156]. Lymphangiomas are not considered
trueneoplasms but rather malformations of the lymphatic
vasculaturewith progressive cystic change resulting from
obstruction of lym-phatic drainage [80]. The progressive growth of
these lesionscauses dyspnea. Surgical resection is curative in most
cases, al-though recurrences may require repeated surgery
[156].
Vascular endothelial tumours of intermediate malignancy(with
local aggressive behaviour and/or rare metastases) havebeen
reported in the mediastinum as case reports and caseseries. These
include kaposiform hemangioendothelioma(KHE) and a single case of
composite hemangioendothelioma[24].
Less than 15 cases of exclusively mediastinal KHE havebeen
reported, in addition to a number of cases where largeKHEs extended
contiguously from the neck into the medias-tinum [51, 77, 81, 89,
114, 140, 210, 211, 220, 226, 234]. Thereported mediastinal KHE
cases were exclusively seen in in-fants (016 months of age) with
almost equal sex distribution.Thrombocytopenic consumptive
coagulopathy (Kasabach-Merritt syndrome) was present in almost all
of the reportedcases and is a major cause of fatality in this
tumour. Medias-tinal KHE is histologically similar to its soft
tissue counter-parts and is characterized by poorly circumscribed
nodules oftightly packed small capillary-sized vessels, Kaposi
sarcoma-like areas with spindled cells and absence of HHV-8
immuno-reactivity. A component of larger lymphatic vessels is
oftenpresent. The prognosis of KHE is variable. Complete
surgicalremoval may provide a cure but may not be possible in
caseswith extensive infiltration. Variable success has been
achievedby medical treatment with interferon and chemotherapy.
Theprognosis is often determined by the haematological
compli-cations rather than the local tumour effects. In the
mediastinalcases with follow-up information, six patients were
alive with-out evidence of disease, two patients were alive with
diseaseand two patients died of disease.
A single case of composite hemangioendothelioma, a rarevascular
neoplasm of intermediate grade with variable histo-logical
components, was described in the central mediastinalarea of a
50-year-old female. There was evidence of disease13 months after
surgical resection [24].
Malignant vascular tumours
Malignant vascular tumours comprising
epithelioidhemangioendothelioma (EHE) and angiosarcoma (AS)
havebeen reported in the mediastinum.
Mediastinal EHE is a malignant endothelial neoplasm
withapproximately 30 cases published mostly as case reports [7,
16,25, 27, 56, 60, 88, 103, 109, 115, 121, 143, 151, 191, 202,
215,216, 229] and a single series of 12 primary mediastinal
casesdescribed by Suster et al. [191] All cases occurred in
adults(median age 46 years, age range 1969 years) with twice asmany
cases reported in males as in females. A considerable
Virchows Arch
-
proportion of EHE was discovered incidentally on imagingstudies
for other indications. Symptomatic patients complainedof chest
pain, cough and dyspnea. All reported cases were lo-cated in the
anterior or anteriorsuperior mediastinum and anumber of reports
document involvement of or an origin fromlarge veins (superior vena
cava and innominate vein in partic-ular). The tumours were often
partially encapsulated but oftenat least focally contained
infiltrative areas. Mediastinal EHEshowed the typical histology
with epithelioid endothelial cells,often with intra-cytoplasmic
lumina (blister cells), set in avariable hyalinizedmyxo-collagenous
or chondroidmatrix. Os-teoclastic giant cells and metaplastic bone
were reported inseveral cases [191]. Intra-nuclear cytoplasmic
inclusions areanother feature typically observed in EHE. A
recurrent geneticaberration in EHE, including mediastinal cases, is
translocationof the CAMTA1 gene on chromosome 1p and fusion with
theWWTR1 gene on chromosome 3q [7, 53]. A subset of EHEharbour a
different genetic abnormality in which a YAP1-TFE3 fusion gene is
generated from YAP1 sequences on chro-mosome 11 and TFE1 sequences
from the X-chromosome [9].To date, the YAP1-TFE3 fusion gene has
not been reported inmediastinal EHE.
The differential diagnosis of EHE includes
epithelioidangiosarcoma (EAS) and metastatic adenocarcinoma.
Theintra-cytoplasmic lumina in EHE may easily be mistaken
forglandular differentiation, which in conjunction with
thecytokeratin expression seen in up to 40 % of EHE may leadto an
erroneous diagnosis of metastatic carcinoma. The diag-nosis of EHE
can be established by recognition of the vascular
differentiation by immunohistochemistry (with CD31, CD34,ERG or
FLI staining) (Fig. 2).
Epithelioid angiosarcoma shows high-grade cytologyand usually
lacks the typical myxoid, hyaline or chondroidstroma of EHE.
Features more commonly associated withEAS include capillary
vessels, vascular lakes and papillarygrowth [7]. The genetic
changes identified in the EHEhave only been identified in a single
case of EAS andthus may serve to distinguish the two entities. The
prog-nosis of mediastinal EHE is not unfavourable; of the 15cases
with follow-up, 13 patients showed no evidence ofdisease following
surgical removal, one patient died ofcomplications of the surgical
procedure, and one patientdied of the tumour 9 years after initial
presentation (nosurgery was performed). A subdivision into low- and
high-grade EHE on the basis of cytonuclear features has
beensuggested [7].
Mediastinal AS has almost exclusively been reported inthe
anterior mediastinum. Less than 40 cases are on record[7, 42, 67,
69, 93, 151, 195, 217, 230]. Although olderreports frequently
described a favourable outcome evenafter marginal resection, it
should be noted that many ofthese did not include
immunohistochemical confirmation,raising the possibility that the
reports may have incorpo-rated entities that would currently not be
diagnosed as AS.Furthermore, the prognosis and the demographics of
thepatients in older series are in marked contrast with
morerecently described cases. In a recent series of mediastinalEAS,
12 of 13 patients succumbed to the disease [7], whilst
Fig. 1 Lymphangioma. Anteriormediastinal mass considered to bea
benign cystic lesion wasdiscovered during routine check-up in an
81-year-old male. Themass increased in size from 16 to22 mm in a
period of 8 years. Norecurrence 1 year after thesurgery.
aNon-enhanced CTaxialimage shows a smallhomogeneous mass
withattenuation. b Axial fat-saturatedT2-weighted MR image shows
ahyperintense signal with smallinternal septations. c HE stain
ofresected tumour. Irregular thin-walled vascular structures
inadipose tissue. d D2-40 stain,supporting the
lymphaticdifferentiation of the liningendothelium
Virchows Arch
-
in older reports with follow-up data, no evidence of diseasewas
documented in seven of ten patients after surgical remov-al
(follow-up 636 months) [42, 67, 69, 93, 195, 217]. Simi-larly, in a
more recent series, there was a distinct male pre-dominance with a
median age of 67.5 years, whilst in the olderreports, an equal
gender distribution with a median age of42 years was recorded. The
demographic and prognostic dataof the recent series are more
concordant with the high tumour-related mortality reported for AS
in other organs [57]. In con-trast to EHE, all cases of AS were
symptomatic with painbeing the most common presenting symptom. Most
AS mea-sured less than 10 cm in largest dimension and showed
aninfiltrative growth pattern. There are too few well-documented
cases to draw firm conclusions on treatmentand prognosis. The main
differential diagnoses are other vas-cular neoplasms, in particular
EHE. However, AS is an infil-trative neoplasm with high-grade
cytology and usually lacksthe peculiar fibro-myxoid stroma of EHE.
It is not uncommonto observe AS as a component of somatic type
malignancy in
mediastinal germ cell tumours [35, 47, 69, 120, 131,
171,230].
Chondro-osseous tumours
To qualify as a primarymediastinal osteo- or chondrosarcoma,an
origin from bony structures, chest wall soft tissue,
tracheo-bronchial structures and a putative relationship with a
germcell tumour must be excluded. Bearing these restrictions
inmind, about ten cases of primary extraskeletal
mediastinalosteosarcoma cases occurring in all compartments of the
me-diastinum have been reported [28, 70, 84, 86, 110, 186, 196,208,
221]. However, similar to neoplasms described in previ-ous
paragraphs, several reports predate current concepts andideally
would require substantiation. Although reported casesspanned a wide
age range (1977 years), six cases occurred inyoung adults (1930
years). Four patients were females, andsix were males. A single
case was most likely a radiation
Fig. 2 Epithelioid hemangioendothelioma. Anterior mediastinal
mass in56-year-old female. Angiosarcoma was diagnosed on needle
biopsy. Thetumour was subsequently excised and diagnosed as
epithelioidhemangioendothelioma. The presence of a
CAMTA1-WWTR1translocation was confirmed by RT-PCR. The patient
remains free of
recurrence 23 years post-surgery. a The HE stain shows
myxo-collagenous matrix with epithelioid cells with
intra-cytoplasmicvascular spaces consistent with so-called blister
cells. b MembranousCD31 staining confirming the vascular nature of
the tumour cells
Fig. 3 Ganglioneuroma. Paraspinal tumour in the mediastinum of a
45-year-old female, extending from the cervical region to the
diaphragm. Themass was excised, the patient remained disease free.
a CT image showing
the cervical aspect of the paraspinal mass. b HE stain of the
tumour,revealing a schwannian background with scattered ganglion
cells. cNeurofilament stain revealing elongated slender cytoplasmic
extensions
Virchows Arch
-
induced osteosarcoma following radiotherapy for Hodgkinsdisease
[28]. Most patients presented with chest pain or dys-pnea.
Synchronous secondary deposits were reported in sev-eral cases
[110, 186, 196, 221]. Tumours ranged in size from4.5 to 16 cm and
were often partially encapsulated. Of eightpatients with follow-up
data, five died of disease, one patientwas alive with disease and
two patients showed no evidenceof disease after therapy, including
one patient who developeda recurrence, which was treated with
radiotherapy. Osteosar-coma has only rarely been reported as
somatic type malignan-cy in germ cell tumours [131, 204].
Less than ten cases of extraskeletal mediastinalchondrosarcoma
have been reported, six cases were describedin a single series
[189] and the remaining cases as case reports.Tumour location in
the anterior as well as in the posteriormediastinum was described
for both conventional and mesen-chymal chondrosarcomas. Patients
ranged from 11 to 36 yearswith no obvious sex predilection [91,
189]. Tumours ranged insize from 5 to 15 cm and were mostly
encapsulated. Themesenchymal chondrosarcomas contained areas of
primitivesmall cells and more mature cartilaginous areas, whilst
theconventional chondrosarcomas were composed of hyalinecartilage
with increased cellularity and atypical chondrocytes.In the cases
with follow-up, recurrences occurred in five pa-tients, two
patients died of disease (one after a recurrence) andtwo patients
were alive without disease (one after a recur-rence).
Chondrosarcoma arising in a germ cell tumour appearsto be extremely
uncommon with only a single reported case inthe mediastinum
[125].
The histological differential diagnosis of mediastinal
oste-osarcoma and chondrosarcoma is very limited. Osseous
meta-plasia may occur in other tumours including thymoma [183]but
is unlikely to be confused with the atypical cells of
oste-osarcoma. Bone or cartilage tissue of variable maturity may
bea component of a mediastinal teratoma but does also not showthe
irregular texture and cellular atypia of osteo- andchondrosarcomas.
Osteosarcomatous differentiation has alsobeen reported in malignant
peripheral nerve sheath tumours[44].
Ewing sarcoma/primitive neuroectodermal tumour(PNET)
In the WHO classification, Ewing sarcoma (ES)/PNET is in-cluded
in the classification of bone tumours despite the factthat up to
20% of cases are extraskeletal (extra-osseous Ewingsarcoma, eES)
and are located in various soft tissue sites andeven in parenchymal
organs. Furthermore, the cell of originand differentiation of
ES/PNET remain currently unknown.As stated above for
chondro-osseous tumours, an origin frombony structures such as
vertebrae and chest wall must be ex-cluded in order to qualify as
primary mediastinal eES/PNET,leading to the exclusion of several
reported cases where
tumours extended to these structures or where
insufficientdetails were given [112, 231]. Less than 20 convincing
casesof eES/PNET have been reported in the mediastinum [3, 50,74,
75, 100, 102, 119, 153, 164, 169, 178, 231]. The casesmostly
occurred in young individuals (median age 28 years,range 566 years)
with equal gender distribution and in allcompartments of the
mediastinum. The presenting symptomswere non-specific; pain and
dyspnea were frequent. Sometumours extended through the foramina
and caused nervecompression symptoms [100, 119, 169]. The
characteristicgenetic translocation involving the EWSR1 gene on
chromo-some 22was confirmed in several cases [75,
119].Multimodaltherapy was given in a number of cases with variable
results.Long-term cure was achieved in isolated cases.
The differential diagnosis is broad and includes eES/PNET with
variant translocations and eES-like tumours un-related to EWS
(small blue round cell tumours), as well assynovial sarcomas and
undifferentiated pleomorphic sarco-mas with a small cell
morphology. In the anterior medias-tinum, T lymphoblastic lymphoma
(TLBL) is a major dif-ferential diagnostic consideration,
especially since both tu-mours express CD99. Immunohistochemical
staining forlymphocyte markers and TdT will exclude lymphoma.Small
cell neuroendocrine carcinoma (both primary medi-astinal and
metastatic) can be excluded by its high-gradecytologic features and
expression of neuroendocrine and(sometimes weak) epithelial markers
and TTF1. In the pos-terior mediastinum, neuroblastoma must be
excluded,which is usually CD99 negative and does not show EWSR1gene
translocations.
Nerve sheath tumours and tumours derivedfrom the autonomic
nervous system
Neural tumours are the most common mesenchymal tumoursin the
mediastinumwith an estimated incidence of 1219% ofall mediastinal
tumours. Aspects of these tumours have beenthe subject of several
comprehensive reviews [65, 116, 122,165, 167]; the various entities
will therefore only be coveredin general terms in this review, for
specific details the reader isreferred to these reviews. Neural
mediastinal tumours may becategorized into tumours of nerve
sheathschwannian deri-vation, which are predominantly seen in
adults and those ofthe autonomic
(neuronalganglionic/sympatheticparasym-pathetic) nervous system,
which are much more common inthe paediatric age group. Tumours
which are thought to ariseform embryonic remnants of the neural
tube, such as rareexamples of ependymoma (Table 1), constitute a
third catego-ry [43, 54, 222].
Schwannomas are the most common of the mediastinalneural tumours
and are considered to arise from spinalnerves. They are therefore
mainly seen in the posterior
Virchows Arch
-
mediastinum, although cases located in the anterior medi-astinum
are also on record [193, 206]. A significant pro-portion of cases
are asymptomatic and discovered inciden-tally by routine imaging
investigations. Symptomatic casespresent with chest pain, cough or
compression symptoms,in particular in tumours extending through
spinal foramina.There is no gender predilection for schwannoma;
they aremost common in young- to middle-aged adults. Similar
toother locations, these are circumscribed encapsulated tu-mours,
which may undergo cystic degeneration and degen-erative (ancient)
changes. Surgical removal is curativewith extremely low recurrence
rates.
The cellular variant of schwannoma, which may be mistak-en for a
malignant tumour owing to its increased cellularityand lack of
Verocay bodies, is particularly common in themediastinum. Its
benign behaviour has been confirmed in sev-eral series [58, 113,
218, 223]. A more aggressive variant ofschwannoma, previously
designated melanotic schwannoma,has been shown to have a high
recurrence and metastatic ratewith associated 27 % mortality in a
single series, promptingthe prefix malignant to its name [201].
Malignant melanoticschwannoma may be associated with the Carney
complex and
typically originates from spinal nerves in the posterior
medi-astinum or retroperitoneum.
A single hybrid nerve sheath tumour sharing features
ofperineurioma and schwannoma has been reported in the pos-terior
mediastinum. These hybrid tumours are commonlyfound in superficial
soft tissues and require immunohisto-chemistry to confirm their
hybrid nature [157]. Because oftheir coexpression of vimentin and
EMA, they need to bedistinguished from meningioma, type A thymoma
and follic-ular dendritic cell sarcoma. A single case of
myxoidneurothekeoma/nerve sheath myxoma in the superior
medias-tinum was recently reported [176].
Neurofibroma, similar to schwannoma, occurs mainly inthe
posterior mediastinum. Up to 45 % of neurofibromas oc-cur in
patients with neurofibromatosis type I (vonRecklinghausens disease;
NF1), in this setting, the tumoursoccur at a younger age and are
often multiple [116]. Plexiformneurofibroma is pathognomonic for
NF1 and carries a risk oftransformation to MPNST. The anatomical
location and ill-defined borders (in contrast to schwannoma) of
plexiformneurofibroma hamper removal resulting in a higher
recurrencerate.
Table 1 Summary of mediastinal neural tumours
Neural tumours
Derivation Type Behaviour Location in mediastinum/age of
onset
Nerve sheath/schwannian Schwannoma Benign Post./adult
Cellular schwannoma Benign Post./adult
Malignant melanoticpsammomatous schwannoma
Malignant Post./adult
Nerve sheath myxoma Benign NA
Hybrid schwannomaperineurioma Benign NA
Neurofibroma Benign Post./all ages
Plexiform neurofibroma Benign Post./young adult
MPNST Malignant Post./all ages
Malignant Triton tumour Malignant Post./all ages
Granular cell tumour Benign Post./young adult
Malignant granular cell tumour Malignant Post./adult
Ganglionic/autonomousnervous system
Sympathetic ganglia, neuronal/neuroblastic
Ganglioneuromas Benign Post./ped./young adult
Neuroblastoma Malignant Post./ped.
Ganglioneuroblastoma Malignant Post./ped.
Paraganglioma Anterior mediastinalbranchiomericchemodectoma
Benign/malignant
Ant./adult
Posterior mediastinal paraganglioma(50 %
functional/adrenergic)
Benign/malignant
Post./young adult(male)
Embryonal neural tube remnants Ependymoma Low-grademalignant
Post./na
Neuroectodermal Melanotic neuroectodermal tumour
Low-grademalignant
Ped.
Virchows Arch
-
Malignant peripheral nerve sheath tumours are high-gradesarcomas
which typically arise in association with larger nervetrunks and
carry a poor prognosis. MPNST, in particular thosearising in
NF1-associated neurofibromas, can occur in youngpatients [45, 46].
Similar to other nerve sheath tumours, me-diastinal MPNST is
typically located in the posterior compart-ment, although cases may
also arise in the anterior mediasti-num [92, 99, 148, 166, 232].
Complete surgical resection mayprovide a cure [105, 124], but
overall, these are aggressiveneoplasms with high rates of local
recurrence and metastases.Variants of MPNST, which have also been
reported in themediastinum, may show divergent mesenchymal
differentia-tion with components of skeletal muscle
(rhabdomyosarcoma,the so-called Triton tumour) [105], osteosarcoma
andchondrosarcoma [44]. MPNST, including the Triton tumourvariant,
has been reported as a somatic component of medias-tinal germ cell
tumours [33, 118, 131].
Granular cell tumour (GrCT) shows differentiation
alongneuroectodermal lines and shares similarities with
Schwanncells. GrCT occurs in the posterior mediastinum, in
keepingwith its proposed neuroectodermal/neural derivation.
Lessthan 20 cases of GrCT have been reported in the mediastinum[1,
4, 8, 15, 40, 76, 87, 95, 98, 117, 137, 159, 168, 170, 179,184,
185, 224], including cases with malignant behaviour oratypical
features suggestive of malignant GrCT [40, 76, 137,185]. Benign
mediastinal GrCT occurred twice as frequentlyin females as in
males; malignant GrCT (four cases) wereequally distributed in males
and females. Benign GrCT wereseen in young- to middle-aged adults
(range 1153 years, me-dian age 27 years) with an average size of 4
cm and oftendiscovered incidentally. Malignant GrCTs were
symptomaticand occurred in older individuals (range 5966 years,
medianage 63 years) and were larger (range 5.415 cm, average
size10.3 cm).
A very rare tumour with proposed neuroectodermaldifferentiation
based on electron microscopic compara-tive studies, melanotic
neuroectodermal tumour of infan-cy (retinal anlage tumour,
melanotic progronoma),which most commonly occurs in the jaws of
infantshas twice been reported in the mediastinum [36, 128].These
tumours show a biphasic morphology with smallcells of supposed
neural origin which are immunoreac-tive for neuronal/neuroendocrine
markers such assynaptophysin and chromogranin, surrounded by
largercells with (neuro)ectodermal differentiation evidencedby
staining reactions with EMA, cytokeratin andHMB45. Two cases have
been reported in the mediasti-num; one case presented in a
7-month-old infant andsecond case was reported in a 23-year-old
female whodied of metastases [36, 128].
Neuroblastic tumours with variable ganglionic differenti-ation
originating from sympathetic ganglia range from be-nign
ganglioneuromas through to malignant neuroblastoma
and the intermediate form, ganglioneuroblastoma [116]. Inline
with their postulated cell of origin, most of these tu-mours
develop in the posterior mediastinum.
Malignantneuroblasticganglionic tumours (neuroblastoma
andganglioneuroblastoma) are very rarely encountered in theadult
population [11], whilst ganglioneuroma is seen inchildren and young
adults and is a benign and oftenasymptomatic tumour (Fig. 3) [116].
Whilst a significantproportion of neuroblastomas present in the
mediastinum,it has been suggested that these tumours differ from
themore common adrenal neuroblastomas by their pathogene-sis and a
more favourable prognosis [116]. A single case ofneuroblastoma as a
somatic component of a mediastinalgerm cel l tumour was repor ted ,
in which theneuroblastemous component metastasized and resulted
inthe demise of the patient [144].
Mediastinal paraganglionic tumours of the autonomousnervous
system have not infrequently been reported in themediastinum as
case series and single case reports, many ofwhich have been
included in recent reviews [66, 104, 132,141, 142, 146, 150].
Mediastinal paragangliomas may occurin the anterior mediastinum,
where they are associated withaorticopulmonary, vagal, subclavian,
carotid and coronaryvessel (branchiomeric) paraganglia.
Branchiomeric(aorticopulmonary) paraganglia (chemodectomas) are
rarelyfunctional [219].
Paragangliomas located in the posterior compartmentderive from
the sympathetic chain and are located in thecostovertebral sulcus
and secrete catecholamines in up to50 % of cases, resulting in
systemic symptoms (extra-adrenal pheochromocytoma). Mediastinal
paragangliomaoccurs over a wide age range; those located in the
ante-rior mediastinum are slightly more common in females,whilst
paravertebral paraganglioma has slightly more fre-quently been
reported in young adult males [66, 132].The biological behaviour of
these tumours cannot reli-ably be predicted based on morphological
features. Upto a quarter of cases may metastasize [104]. Owing
tothe close vicinity of branchomeric paraganglia to medi-astinal
vessels and organs and associated surgical consid-erations, the
prognosis of this subgroup is worse than forparavertebral
paraganglioma.
Remnants of the embryonic neural tube may on very rareoccasions
give rise to tumours located in the mediastinum. Sixcases of
mediastinal ependymoma, including one case ofmyxopapillary
ependymoma, have been published, whichwere summarized in a case
report by Estrozi et al. [54]. Allcases occurred in the posterior
mediastinum of adult females(age range 3571 years; median age 40.5
years). The tumoursranged in size from 5.0 to 9.0 cm. Of four cases
with follow-up, three patients were alive without disease after
surgicalresection, and one patient suffered metastases to the
pleuraand mediastinal lymph nodes.
Virchows Arch
-
Tumours of uncertain differentiation
The WHO classification of soft tissue tumours includes achapter
on neoplasms with unclear histogenesis, some ofwhich have been
reported to occur in the mediastinum(Table 2) and are described in
the following section. It isconceivable that a number of these
tumours may not actuallyhave a normal tissue counterpart but
instead reflect the conse-quence of genetic aberrations in which
translocations and oth-er genetic errors culminate in histological
patterns, which arenot encountered in normal tissue. A number of
the entitiesincluded in this section of the WHO classification are
site-specific, such as intra-muscular myxoma, and are not
encoun-tered in the mediastinum; those that have been reported in
themediastinum are listed in Table 2 and are described in
thefollowing section. The term malignant mesenchymomawhich was used
in the past for sarcomas with two or moretypes of differentiation
is no longer recommended since therespective tumours are now
classified as sarcomas with areasof divergent differentiation (e.g.
dedifferentiated liposarcomaor Triton tumour).
Angiomatoid fibrous histiocytoma
Despite its name, angiomatoid fibrous histiocytoma is gener-ally
considered a tumour of uncertain histogenesis rather thana true
fibrohistiocytic tumour (see part I of this review). Twocases of
angiomatoid fibrous histiocytoma, which were bothresected without
further disease activity, have been reported inthe mediastinum [12,
38].
Ossifying fibromyxoid tumour
Two cases of ossifying fibromyxoid tumour (OFT) havebeen
reported in the mediastinum, both in the anterior
compartment [49, 197]. One case presented as a large mass(1,052
g) in a 50-year-old female who complained of chestpain [197]. No
evidence of recurrence or metastasis wasnoted 1-year after surgery
on follow-up. The second casepresented as an 11-cm tumour in a
59-year-old female; nofollow-up data was provided [49].
Myoepithelial tumours including parachordoma
There have been no convincing reports of myoepithelial tu-mours
in the mediastinum. A single case of a myoepthelialtumour located
in the inferior mediastinum in close associa-tion with the carina
was suggested to originate from heartmuscle and thus cannot be
considered a bona fide tumour ofmediastinal soft tissue [10].
Synovial sarcoma
Synovial sarcoma (SySa) is a high-grade spindle cell sarcomaof
uncertain histogenesis, often with epithelial differentiation,most
commonly occurring in deep soft tissue of the extremi-ties in young
adults. SySa is one of the more frequently en-countered sarcomas in
the mediastinum.
Salah et al. performed a literature survey of mediastinalSySa
and identified 40 cases in the English language withappropriate
descriptive details [173], including 15 patientsdescribed in a
series by Suster et al. [190]. The majority ofcases occurred in
young adults (age range 383 years; medianage 30.5 years) with a
male predominance (2.9:1). Seventypercent of cases were reported in
the anterior mediastinumwith tumour size ranging from 5 to 20 cm
(median size11 cm). Pain and dyspnea were the most common
presentingsymptoms.
Most cases were monophasic spindle cell SySa on histolo-gy. A
specific chromosomal translocation, t(X;18)(p11;q11),involving the
SS18 (SYT, SSXT) gene on chromosome 18 andthe SSX1, SSX2 or SSX4
gene on the X-chromosome is acharacteristic feature of SySa and has
been demonstrated inmediastinal SySa [94, 172, 203].
Complete surgical resection was achieved in 57.5 % ofpatients,
which was combined with either radiation or chemo-therapy in eight
patients. Progression occurred in 67 % ofpatients. Eleven of 30
(37%) patients with follow-up data diedof disease, nine (30 %) were
alive with disease and nine(27%) patients were alive with no
evidence of disease; diseasestatus was unknown for two patients.
Complete resection wasidentified as the sole factor influencing
survival.
The differential diagnosis of mediastinal SySa comprisesother
spindle cell sarcomas, in particular MPNST, malignantsolitary
fibrous tumour (SFT) and pleomorphic sarcoma NOS.Type A thymoma and
sarcomatoid carcinoma may also enterthe differential diagnosis.
Table 2 Mediastinal mesenchymal tumours of uncertain
differentiation
Tumour type N
Angiomatoid fibrous histiocytoma [12, 38] 2
Ossifying fibromyxoid tumour [49, 197] 2
Myoepithelioma/myoepithelial carcinoma/mixed tumour/parachordoma
[10]
1a
Synovial sarcoma
-
Type A thymoma is usually composed of uniform non-hyperchromatic
epithelial spindle cells, whilst the cells in sy-novial sarcoma are
hyperchromatic andmitotically active. Theglandular and epithelial
components in biphasic synovial sar-coma may be mistaken for
elements of type A thymoma.
Immunohistochemistry is very useful. Although synovialsarcoma is
usually positive for cytokeratin and EMA, stainingis typically weak
and/or focal, whilst type A thymoma is typ-ically diffusely
cytokeratin positive. TLE1 and CD56 arecommonly expressed in SySa
and not found in type Athymoma, whilst bcl2 expression is found in
both. Demon-stration of the t(X;18) translocation by FISH is
diagnostic ofSySa, and this genetic abnormality has not been
identified inother tumours.
MPNST may be very difficult to distinguish from synovialsarcoma
without molecular analysis, as these tumours sharesome
morphological and immunohistochemical features.S-100 staining may
be seen synovial sarcoma, and converselyMPNST is frequently
completely negative for S-100. Similar-ly, staining for TLE1 may
also be positive in MPNST andSFT. SFT may be distinguished from
SySa by CD34 andSTAT-6 immunohistochemistry, as both markers are
notexpressed in SySa.
Epithelioid sarcoma
A single case of mediastinal epithelioid sarcoma was identi-fied
in the literature. The tumour was located in the
posteriormediastinum of a 1-year-old male infant. After
radiotherapyand chemotherapy, no evidence of disease was recorded
aftera follow-up period of 44 months [71].
Alveolar soft part sarcoma (ASPS)
Two well-documented cases of primary mediastinal ASPShave been
reported to date. ASPS is a rare tumour with adistinctive histology
and characteristic genetic translocationwhich arises in the deep
soft tissue of the lower limb girdle,most commonly in young
individuals. ASPS ultimatelycarries a poor prognosis, and
metastases may occur after longtime intervals. The two mediastinal
cases described in a reportby Flieder et al. were located in the
anterior mediastinum of a23-year-old male and in the posterior
mediastinum of a 22-year-old male [59]. One of these patients
presented with syn-chronous metastatic disease in the lungs and
brain, and thesecond patient was lost to follow-up after 14 years
withoutevidence of recurrence or metastasis. A third putative case
ofprimary mediastinal ASPS was reported in the anterior
medi-astinum of a 13-year-old female. However, during work-up,
atumour was later identified in the thigh, which most
likelyrepresents the primary location [177].
Clear cell sarcoma of soft tissue
Two cases of clear cell sarcoma (CCS;melanoma of soft parts)have
been reported as primary tumours in the mediastinum[194, 199]. A
15-cm tumour was excised from the superiormediastinum of a
59-year-old female in the report byTirabosco et al. [199]. Although
the histology was represen-tative for CCS, immunohistochemical
staining for HMB45and Melan-A was negative. The diagnosis was
supported bydemonstration of a translocation involving the EWSR1
geneby FISH analysis; the partner gene was not identified.
Meta-static disease developed 16 months post-surgery; no
furtherfollow-up was provided. A second case of CCS was
resectedbyVATS from the superior mediastinum of a
63-year-oldmale[194]. A tumour of 8.5 cm was removed and showed
thetypical histology for CCS with positive staining for HMB45and
S-100 protein. Melan-Awas negative and no genetic anal-ysis was
performed. At 15 months of follow-up, there was noevidence of
disease.
Extraskeletal myxoid chondrosarcoma
One case o f med ia s t i na l ex t r a ske l e t a l myxo
idchondrosa r coma was inc luded in the se r i e s o
fchondrosarcoma of Suster et al. [189].
Extrarenal rhabdoid tumour
Extrarenal rhaboid (ERRT) tumour is an exceedingly rare tu-mour,
which is histologically similar to its renal and centralnervous
system counterparts. ERRToccurs typically in younginfants and
carries an exceptionally poor prognosis. TheSMARCB1 (INI1) gene,
located on chromosome 22q11, ismutated or deleted in ERRT. Despite
its rarity in somatic softtissue, several cases, mainly included in
series, have beenreported in the mediastinum [73, 155, 158, 198].
All fivepatients with sufficient clinical details died of disease.
Onefemale patient was diagnosed at the age of 26 years, and
twopaediatric patients were infants (8 months and a
congenitalcase).
PEComa
Tumours with assumed perivascular differentiation and an
ep-ithelioid morphology (PEComa) include angiomyolipoma,which
contains a variable component of mature fat and mostcommonly arises
in the kidney. PEComa cells have a distinctmorphology and
immunophenotype with evidence of smoothmuscle and melanocytic
differentiation with variable stainingfor smooth muscle actin,
desmin and melanocytic markerssuch as Melan-A and HMB45. Since
their first description,PEComas have been described in many
anatomical locations.
Virchows Arch
-
PEComa may arise in the setting of tuberous sclerosis
andlymphangioleiomyomatosis.
To date, less than 15 cases of PEComa have been reportedin the
mediastinum, which have all behaved in a benign fash-ion [6, 18,
26, 63, 78, 96, 97, 134, 200, 212214]. Threequarters of the
reported cases were discovered incidentallyby imaging studies for
other reasons, symptomatic casesmainly presented with shortness of
breath. The marked femalepredominance seen in non-mediastinal cases
was less pro-nounced in the mediastinal tumours (2:1). The cases
werereported over a wide age range (2263 years; median age54.4
years). Anatomically, the cases were evenly distributedin the
anterior (n=5) and posterior (n=4) mediastinum withsingle cases in
other compartments, with sizes ranging from 4to 15 cm (average size
7.8 cm). Three of reported cases arelikely to have arisen in
association with tuberous sclerosis/lymphangioleiomyomatosis [134,
200, 212].
Desmoplastic small round cell tumour
A single case of desmoplastic small round cell tumour(DSRCT) was
reported in the anterior mediastinum of a 22-year-old male
[138].
Unclassified/undifferentiated sarcoma
High-grade undifferentiated sarcomas were previously
oftenclassified as malignant fibrous histiocytoma (MFH). Follow-ing
the current understanding that there is insufficient supportfor
histiocytic (or any other specific) differentiation, these tu-mours
are now categorized as undifferentiated sarcomas in theWHO
classification. So-called MFH cases have been de-scribed in the
mediastinum but do not show any further char-acteristic features. A
series of 34 so-called MFH cases in themediastinum were reviewed by
Murakawa et al. [135], andfurther individual case reports haven
been published. As inother soft tissue sites, these tumours are
seen over a wideage range but mainly in older adults, with an equal
genderdistribution. As would be expected, these tumours have a
verypoor prognosis despite therapeutic intervention.
Acknowledgments The authors wish to thank Dr. Satoshi
Kaneda(Department of Radiology, Saiseikai Central Hospital, Tokyo,
Ja-pan) for providing radiological images, Dr. Ieneke Hartmann
(De-partment of Radiology, Maasstad Ziekenhuis, Rotterdam,The
Netherlands) for reviewing the radiological images and for
pro-viding suggestions for the figure legends. The molecular
analysis ofthe epithelioid hemangioendothelioma (Fig. 2) was kindly
per-formed by Dr. Uta Flucke (Department of Pathology, Radboud
Uni-versity Medical Center, Nijmegen, The Netherlands).
Compliance with Ethical Standards
Conflict of interest The authors declare that they have no
competinginterests.
Human and Animal Rights and Informed Consent There was
noresearch involving human participants and/or animals performed
for thismanuscript.
Open Access This article is distributed under the terms of the
CreativeCommons At t r ibut ion 4 .0 In te rna t ional License (h t
tp : / /creativecommons.org/licenses/by/4.0/), which permits
unrestricted use,distribution, and reproduction in any medium,
provided you give appro-priate credit to the original author(s) and
the source, provide a link to theCreative Commons license, and
indicate if changes were made.
References
1. Abenoza P, Sibley RK (1987) Granular cell myoma
andschwannoma: fine structural and immunohistochemical
study.Ultrastruct Pathol 11:1928
2. Abiko T, Sato S, Futamata T, Kato R (2005) A case of
pleomor-phic leiomyosarcoma of the posterior mediastinum.
NipponKokyukigeka Gakkai Zasshi 19:819822
3. Ahmad R, Mayol B, Davis M, Rougraff B (1999)
ExtraskeletalEwings sarcoma. Cancer 85:725731
4. Aisner SC, Chakravarthy AK, Joslyn JN, Coughlin TR
(1988)Bilateral granular cell tumors of the posterior mediastinum.
AnnThorac Surg 46:688689
5. Akiba T, Morikawa T, Hirayama S, Ohki T (2012)
Thymichaemangioma presenting with a left innominate vein
aneurysm:insight into the aetiology. Interact Cardiovasc Thorac
Surg 15:925927. doi:10.1093/icvts/ivs340
6. Amir AM, Zeebregts CJ, Mulder HJ (2004) Anterior
mediastinalpresentation of a giant angiomyolipoma. Ann Thorac Surg
78:21612163. doi:10.1016/S0003-4975(03)01512-1
7. Anderson T, Zhang L, Hameed M, Rusch V, Travis WD,Antonescu
CR (2015) Thoracic epithelioid malignant vasculartumors: a
clinicopathologic study of 52 cases with emphasis onpathologic
grading and molecular studies of WWTR1-CAMTA1fusions. Am J Surg
Pathol 39:132139. doi:10.1097/PAS.0000000000000346
8. Angeles RM, Papari M, Malecki Z (2005) Pathologic quiz case:
a43-year-old woman with an incidentally detected posterior
medi-astinal mass. Granular cell tumor of the posterior
mediastinum.Arch Pathol Lab Med 129:e27e28.
doi:10.1043/1543-2165(2005)1292.0.CO;2
9. Antonescu CR, Le Loarer F, Mosquera JM, Sboner A, Zhang
L,Chen CL, Chen HW, Pathan N, Krausz T, Dickson BC,Weinreb I,Rubin
MA, Hameed M, Fletcher CD (2013) Novel YAP1-TFE3f u s i o n d e f i
n e s a d i s t i n c t s u b s e t o f e p i t h e l i o i
dhemangioendothelioma. Genes Chromosomes Cancer 52:775784.
doi:10.1002/gcc.22073
10. Arab M, Danel C, dAttellis N, Juvin K, Hernigou A, Fabiani
JN,Riquet M (2005) A rare inferior middle mediastinal tumor
resec-tion under extra-corporeal circulation. Ann Thorac Surg
79:14131415. doi:10.1016/j.athoracsur.2003.10.019
11. Argani P, Erlandson RA, Rosai J (1997) Thymic neuroblastoma
inadults: report of three cases with special emphasis on its
associa-tion with the syndrome of inappropriate secretion of
antidiuretichormone. Am J Clin Pathol 108:537543
12. Asakura S, Tezuka N, Inoue S, Kihara N, Fujino S
(2001)Angiomatoid fibrous histiocytoma in mediastinum. Ann
ThoracSurg 72:283285
13. Auliac JB, Cuvelier A, Peillon C, Louvel JP, Metayer J, Muir
JF(1999) Mediastinal leiomyosarcoma. RevMal Respir 16:210213
Virchows Arch
-
14. Baldo X, Sureda C, Gimferrer JM, Belda J (1997) Primary
medi-astinal leiomyoma: an angiographic study and embolisation of
thefeeding vessels to improve the surgical approach. Eur
JCardiothorac Surg 11:574576
15. Bean SM, Eloubeidi MA, Eltoum IA, Cerfolio RJ, Jhala
DN(2005) Preoperative diagnosis of a mediastinal granular cell
tumorby EUS-FNA: a case report and review of the
literature.Cytojournal 2:8. doi:10.1186/1742-6413-2-8
16. Begbie SD, Bell DR, Nevell DF (1997) Mediastinal
epithelioidhemangioendothelioma in a patient with type IV
Ehlers-Danlossyndrome: a case report and review of the literature.
Am J ClinOncol 20:412415
17. Begin LR, Schurch W, Lacoste J, Hiscott J, Melnychuk DA
(1994)Glycogen-rich clear cell rhabdomyosarcoma of the
mediastinum.Potential diagnostic pitfall. Am J Surg Pathol
18:302308
18. Bertrand G, Bidabe MC, George P, Dubin P, Touzard C
(1984)Angiomyolipoma of the central mediastinum. An
apparentlyundescribed entity. Ann Chir 38:679681
19. Bhagotra R, Kapoor R, Singhal VS (1990) Leiomyoma of
themediastinum. Indian J Chest Dis Allied Sc 32:133136
20. Boor A, Jurkovic I, Janik M, Vajo J, Kocan P, Ponist J,
DudrikovaK, Krajcar R, Stubna J (2000) Benign glomus tumor of the
supe-rior posterior mediastinum. Cesk Patol 36:156159
21. Box JC, Newman CL, Anastasiades KD, Lucas GW, Latouff
OM(1995) Adult rhabdomyoma: presentation as a
cervicomediastinalmass (case report and review of the literature).
AmSurg 61:271276
22. Brindley GV Jr (1949) Glomus tumor of the mediastinum.
JThorac Surg 18:417420
23. Caballero C, Gomez S, Matias-Guiu X, Prat J
(1992)Rhabdomyosarcomas developing in association with
mediastinalgerm cell tumours. Virchows Arch A Pathol Anat
Histopathol420:539543
24. Cakir E, Demirag F, Gulhan E, Oz G, Tastepez I
(2009)Mediastinal composite hemangioendothelioma. A rare tumor atan
unusual location. Tumori 95:98100
25. Campos J, Otero E, Dominguez MJ, Gonzalez-Quintela A
(2007)Epithelioid hemangioendothelioma in the posterior
mediastinum.Eur J Intern Med 18:331332.
doi:10.1016/j.ejim.2006.11.010
26. Candas F, Berber U, Yildizhan A, Yiyit N, Gorur R,
Isitmangil T(2013) Anterior mediastinal angiomyolipoma. Ann Thorac
Surg95:14311432. doi:10.1016/j.athoracsur.2012.07.066
27. Carassai P, Caput M (2010) Report of a case of
epithelioidhemangioendothelioma of the anterior mediastinum
metastatic topleura. Pathologica 102:112114
28. Catanese J, Dutcher JP, Dorfman HD, Andres DF, Wiernik
PH(1988) Mediastinal osteosarcoma with extension to lungs in
apatient treated for Hodgkins disease. Cancer 62:22522257
29. Chetty R, Reddi A (2003) Rhabdomyomatousmultilocular
thymiccyst. Am J Clin Pathol 119:816821.
doi:10.1309/QDJC-A1HX-QLHL-CFTM
30. Choi YJ, YangKH, Gang SJ, KimBK, Kim SM
(1991)Malignantglomus tumor originating in the superior
mediastinuman immu-nohistochemical and ultrastructural study. J
Korean Med Sci 6:157163
31. ChuWP (2013) Anterior mediastinal alveolar
rhabdomyosarcomain an infant: rare site for a common paediatric
tumour. Hong KongMed J 19:458459. doi:10.12809/hkmj133714
32. Cohen AJ, Sbaschnig RJ, Hochholzer L, Lough FC, Albus
RA(1987) Mediastinal hemangiomas. Ann Thorac Surg 43:656659
33. Comiter CV, Kibel AS, Richie JP, NucciMR, RenshawAA
(1998)Prognostic features of teratomas with malignant
transformation: aclinicopathological study of 21 cases. J Urol
159:859863
34. Conner WC, Fink GW, McGinnis KM, Alfieris GM (2004)Surgical
management of leiomyosarcoma of the mediastinum.Ann Thorac Surg
77:334336
35. Contreras AL, Punar M, Tamboli P, Tu SM, Pisters L, Moran
C,Czerniak BA, Guo CC (2010) Mediastinal germ cell tumors withan
angiosarcomatous component: a report of 12 cases. Hum
Pathol41:832837. doi:10.1016/j.humpath.2009.11.008
36. DAbrera VS, Burfitt-Williams W (1973) A
melanoticneuroectodermal neoplasm of the posterior mediastinum.
JPathol 111:165172. doi:10.1002/path.1711110304
37. DAiuto M, Veronesi G, Pompilio G, Gasparri R, Presicci
F,Galetta D, Biglioli P, Spaggiari L (2005) Extended right
pneumo-nectomy with partial left atrial resection for
primaryleiomyosarcoma of the mediastinum. J Thorac Cardiovasc
Surg129:694695. doi:10.1016/j.jtcvs.2004.07.057
38. Davies KA, Cope AP, Schofield JB, Chu CQ, Mason JC, KrauszT,
Smith P, Denman AM, Walport MJ (1995) A rare mediastinaltumour
presenting with systemic effects due to IL-6 and tumournecrosis
factor (TNF) production. Clin Exp Immunol 99:117123
39. Davis JM, Mark GJ, Greene R (1978) Benign blood
vasculartumors of the mediastinum. Report of four cases and review
ofthe literature. Radiology 126:581587. doi:10.1148/126.3.581
40. De Luca G, Luciano A, Benincasa G, Sessa R, Petteruti F
(2013)Giant malignant granular cell tumor (GCT) of the posterior
medi-astinum. J Thorac Oncol 8:11071108.
doi:10.1097/JTO.0b013e318299ad62
41. de Queiroga EM, Chikota H, Bacchi CE, Moran CA, Suster
S(2004) Rhabdomyomatous carcinoma of the thymus. Am J SurgPathol
28:12451250
42. Deroux A, Destors M, Coudurier M, Lantuejoul S, Aubert
M,Girard N, Moro-Sibilot D (2012) A case of
mediastinalangiosarcoma. Rev Mal Respir 29:11201123.
doi:10.1016/j.rmr.2012.04.009
43. Doglioni C, Bontempini L, Iuzzolino P, Furlan G, Rosai J
(1988)Ependymoma of the mediastinum. Arch Pathol Lab Med
112:194196
44. Ducatman BS, Scheithauer BW (1984) Malignant peripheralnerve
sheath tumors with divergent differentiation. Cancer
54:10491057
45. Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM,Ilstrup
DM (1986) Malignant peripheral nerve sheath tumors.
Aclinicopathologic study of 120 cases. Cancer 57:20062021
46. Ducatman BS, Scheithauer BW, Piepgras DG, ReimanHM
(1984)Malignant peripheral nerve sheath tumors in childhood. J
Neuro-Oncol 2:241248
47. Ehrenreich T, Freund AJ, Shapiro HN (1953)
Hemangio-endothelioma arising in a mediastinal teratoma. Dis Chest
23:294303
48. Eimoto T, Kitaoka M, Ogawa H, Niwa H, Murase T, Tateyama
H,Inagaki H, Soji T, Wang HJ (2002) Thymic sarcomatoid carcino-ma
with skeletal muscle differentiation: report of two cases, onewith
cytogenetic analysis. Histopathology 40:4657
49. Ekfors TO, Kulju T, Aaltonen M, Kallajoki M (1998)Ossifying
fibromyxoid tumour of soft parts: report of fourcases including one
mediastinal and one infantile. APMIS106:11241130
50. El Weshi A, Allam A, Ajarim D, Al Dayel F, Pant R,
Bazarbashi S,MemonM (2010) Extraskeletal Ewings sarcoma family of
tumoursin adults: analysis of 57 patients from a single
institution. ClinOncol(R Coll Radiol) 22:374381.
doi:10.1016/j.clon.2010.02.010
51. Enjolras O, Wassef M,Mazoyer E, Frieden IJ, Rieu PN, Drouet
L,Taieb A, Stalder JF, Escande JP (1997) Infants with
Kasabach-Merritt syndrome do not have true hemangiomas. J
Pediatr130:631640
52. Eroglu A, Kurkcuoglu C, Karaoglanoglu N, Gursan N
(2002)Primary leiomyosarcoma of the anterior mediastinum. Eur
JCardiothorac Surg 21:943945
53. Errani C, Zhang L, Sung YS, Hajdu M, Singer S, Maki
RG,Healey JH, Antonescu CR (2011) A novel WWTR1-CAMTA1
Virchows Arch
-
gene fusion is a consistent abnormality in
epithelioidhemangioendothelioma of different anatomic sites.
GenesChromosomes Cancer 50:644653. doi:10.1002/gcc.20886
54. Estrozi B, Queiroga E, Bacchi CE, Faria Soares de Almeida
V,Lucas de Carvalho J, Lageman GM, Rosado-de-Christenson M,Suster S
(2006) Myxopapillary ependymoma of the posterior me-diastinum. Ann
Diagn Pathol 10:283287. doi:10.1016/j.anndiagpath.2006.03.015
55. Fergeson JO, Clagett OT, Mc DJ (1954) Glomus tumor of
themediastinum; review of the literature and report of case.
Surgery36:320326
56. Ferretti GR, Chiles C, Woodruff RD, Choplin RH
(1998)Epithelioid hemangioendothelioma of the superior vena
cava:computed tomography demonstration and review of the
literature.J Thorac Imaging 13:4548
57. Fletcher C, Bridge J, Lee J-C (2013) Extra-pleural solitary
fibroustumour, 4th edn, WHO classification of tumours of soft
tissue andbone. IARC Press, Lyon, pp 8082
58. Fletcher CD, Davies SE, McKee PH (1987) Cellularschwannoma:
a dis t inct pseudosarcomatous ent i ty.Histopathology 11:2135
59. Flieder DB, Moran CA, Suster S (1997) Primary alveolar
soft-partsarcoma of the mediastinum: a clinicopathological and
immuno-histochemical study of two cases. Histopathology
31:469473
60. Flucke U, Vogels RJ, de Saint Aubain Somerhausen N,
CreytensDH, Riedl RG, van Gorp JM, Milne AN, Huysentruyt CJ,
VerdijkMA, van Asseldonk MM, Suurmeijer AJ, Bras J, Palmedo G,G r o
e n e n P J , M e n t z e l T ( 2 0 1 4 ) E p i t h e l i o i
dhemangioendothelioma: clinicopathologic, immunohistochemi-cal, and
molecular genetic analysis of 39 cases. Diagn Pathol 9:131.
doi:10.1186/1746-1596-9-131
61. Fokkema JP, Paul MA, Vrouenraets BC (2014)
Mediastinallymphangioma in an adult. Ann R Coll Surg Engl
96:e24e25.doi:10.1308/003588414X13946184901209
62. Folpe AL, Weiss SW (2002) Lipoleiomyosarcoma
(well-differen-tiated liposarcoma with leiomyosarcomatous
differentiation): aclinicopathologic study of nine cases including
one with dediffer-entiation. Am J Surg Pathol 26:742749
63. Fukuzawa J, Shimizu T, Sakai E, Ido A, Fujita Y, Tsuji T,
Ohki Y,Kimura T, Fujita M, Onodera S (1992) Case report
ofangiomyolipoma of the posterior upper mediastinum. NihonKyobu
Shikkan Gakkai Zasshi 30:464467
64. Gaertner EM, Steinberg DM, Huber M, Hayashi T, Tsuda N,Askin
FB, Bell SW, Nguyen B, Colby TV, Nishimura SL,Miettinen M, Travis
WD (2000) Pulmonary and mediastinal glo-mus tumorsreport of five
cases including a pulmonaryglomangiosarcoma: a clinicopathologic
study with literature re-view. Am J Surg Pathol 24:11051114
65. Gale AW, Jelihovsky T, Grant AF, Leckie BD, Nicks R
(1974)Neurogenic tumors of themediastinum. Ann Thorac Surg
17:434443
66. Gallivan M, Chun B, Rowden G, Lack E (1980)
Intrathoracicparavertebral malignant paraganglioma. Arch Pathol Lab
Med104:4651
67. Gibbs AR, Johnson NF, Giddings JC, Powell DE, Jasani B
(1984)Primary angiosarcoma of the mediastinum: light and electron
mi-croscopic demonstration of factor VIII-related antigen in
neoplas-tic cells. Hum Pathol 15:687691
68. Gomez-Roman JJ, Val-Bernal JF (1997) Lipoleiomyosarcoma
ofthe mediastinum. Pathology 29:428430
69. Gonzalez-Vela JL, Savage PD, Manivel JC, Torkelson
JL,Kennedy BJ (1990) Poor prognosis of mediastinal germ cell
can-cers containing sarcomatous components. Cancer 66:11141116
70. Greenwood SM, Meschter SC (1989) Extraskeletal
osteogenicsarcoma of the mediastinum. Arch Pathol Lab Med
113:430433
71. Gross E, Rao BN, Pappo A, Bowman L, Shearer P, Kaste
S,Greenwald C, Michalkiewicz E, Pratt C (1996) Epithelioid sarco-ma
in children. J Pediatr Surg 31:16631665
72. Gupta S, Jindal SK, Vashisht R, Singh H, Malik SK
(1983)Leiomyosarcoma of the mediastinum. Eur J Respir Dis
64:6971
73. Gururangan S, Bowman LC, Parham DM, Wilimas JA, Rao B,Pratt
CB, Douglass EC (1993) Primary extracranial rhabdoid tu-mors.
Clinicopathologic features and response to ifosfamide.Cancer
71:26532659
74. Halefoglu AM (2013) Extraskeletal Ewings sarcoma
presentingas a posterior mediastinal mass. Arch Bronconeumol
49:8284.doi:10.1016/j.arbres.2012.02.020
75. Halliday J, Soon SY, Monaghan H,Walker WS, Zamvar V
(2010)Extraskeletal Ewings sarcoma presenting as a mediastinal
mass.Ann Thorac Surg 90:10161017.
doi:10.1016/j.athoracsur.2010.01.083
76. Harrer WV, Patchefsky AS (1972) Malignant
granular-cellmyoblastoma of the posterior mediastinum. Chest
61:9596
77. Hartman KR, Moncur JT, Minniti CP, Creamer KM
(2009)Mediastinal Kaposiform hemangioendothelioma and
Kasabach-Merritt phenomenon in an infant: treatment with
interferon. JPediatr Hematol Oncol 31:690692.
doi:10.1097/MPH.0b013e3181a1c291
78. Hayashi K, Yamamoto M, Nishimura H, Inou N
(1994)Angiomyolipoma of the anterior mediastinuma case report.Nihon
Kyobu Geka Gakkai Zasshi 42:584587
79. Herlitzka AJ, Gale JW (1958) Tumors and cysts of the
mediasti-num; survey of one hundred seventy-four mediastinal
tumorstreated surgically during the past eighteen years at the
Universityof Wisconsin Hospitals. AMA Arch Surg 76:697706
80. Hilliard RI, McKendry JB, Phillips MJ (1990) Congenital
abnor-malities of the lymphatic system: a new clinical
classification.Pediatrics 86:988994
81. Hiraiwa H, Hamazaki M, Tsuruta S, Hattori H, Mimaya
J,Hasegawa S , Kohno S , Aok i K (1998) In f an t i l
ehemangioendothelioma of the thymus with massive pleural effu-sion
and KasabachMerritt syndrome: histopathological, flowcytometrical
analysis of the tumor. Acta Paediatr Jpn 40:604607
82. Hirano H, Kizaki T, Sashikata T, Maeda T, Yoshii Y
(2003)Leiomyosarcoma arising from soft tissue tumor of the
mediasti-num. Med Electron Microsc 36:5258.
doi:10.1007/s007950300007
83. Hirose T, Hasegawa T, Seki K, Yang P, Sano T, Morizumi
H,Tsuyuguchi M (1996) Atypical glomus tumor in the mediastinum:a
case report with immunohistochemical and ultrastructural stud-ies.
Ultrastruct Pathol 20:451456
84. Hishida T, Yoshida J, Nishimura M, Ishii G, Nakao M, Nagai
K(2009) Extraskeletal osteosarcoma arising in anterior
mediasti-num: brief report with a review of the literature. J
Thorac Oncol4:927929. doi:10.1097/JTO.0b013e3181a52c63
85. Hoseok I, Jeong YJ, Choi KU, Kim YD (2008)
Symptomaticposterior mediastinal angioleiomyoma. Yonsei Med J
49:666668. doi:10.3349/ymj.2008.49.4.666
86. Ikeda T, Ishihara T, Yoshimatsu H, Kikuchi K, Murakami
M(1974) Primary osteogenic sarcoma of the mediastinum.
Thorax29:582588
87. Ishibashi H, Ota S, Hirose M, Tanio N, Fukuchi K, Muro
H,Nakajima N (2010) Granular cell tumor in themediastinum; reportof
a case. Kyobu Geka 63:496499
88. Isowa N, Hasegawa S, Mino M, Morimoto K, Wada H
(2002)Mediastinal epithelioid hemangioendothelioma resected
byhemi-plastron window technique. Ann Thorac Surg 74:567569
89. Iwami D, Shimaoka S, Mochizuki I, Sakuma T (2006)Kaposiform
hemangioendothelioma of the mediastinum in a 7-
Virchows Arch
-
month-old boy: a case report. J Pediatr Surg 41:14861488.
doi:10.1016/j.jpedsurg.2006.04.013
90. Iwata T, Miura T, Inoue K, Hanada S, Inoue H, Miyamoto
Y(2012) Primary leiomyosarcoma of the anterior mediastinumencasing
the aortic arch, left common carotid and left subclavianarteries.
Ann Thorac Cardiovasc Surg 18:140143
91. Jeong SS, Choi PJ, Kim DW, Son C, Roh MS (2013)
Primaryextraskeletal mesenchymal chondrosarcoma of the anterior
medi-astinum. Korean J Pathol 47:492494.
doi:10.4132/KoreanJPathol.2013.47.5.492
92. Kalra B, Kingsley PA, Bedi HS, Kwatra KS, Negi P
(2014)Malignant peripheral nerve sheath tumor of the anterior
mediasti-num: a rare presentation. Rare Tumors 6:5528.
doi:10.4081/rt.2014.5528
93. Kardamakis D, Bouboulis N, Ravazoula P, Dimopoulos
P,Dougenis D (1996) Primary hemangiosarcoma of the mediasti-num.
Lung Cancer 16:8186
94. Katakura H, Fukuse T, Shiraishi I, Hayatsu E, Nishijo
K,Toguchida J, Nakashima Y, Wada H (2009) Mediastinal
synovialsarcoma. Thorac Cardiovasc Surg 57:183185.
doi:10.1055/s-2006-955886
95. Kim do Y, Jeon HW, Kim KS, Park JK, Sung SW (2014) A
rarecase of mediastinal granular cell tumor. Korean J
ThoracCardiovasc Surg 47:494496.
doi:10.5090/kjtcs.2014.47.5.494
96. Kim YH, Kwon NY, Myung NH, Kim EJ, Choi YH, Yoon SY,Choi EK,
Park JS, Kim KY, Lee KY (2001) A case of mediastinalangiomyolipoma.
Korean J Intern Med 16:277280
97. Knight CS, Cerfolio RJ, Winokur TS (2008) Angiomyolipoma
ofthe anterior mediastinum. Ann Diagn Pathol 12:293295.
doi:10.1016/j.anndiagpath.2006.12.007
98. Kocatas A, Dural AC, Sever N, Kankaya B, Dogan M, Yegen
G,Gonenc M, Bilgic BM, Bedirhan MA, Alis H (2014) Minimalinvasive
endoscopic management of synchronous granular celltumours in the
colon and posterior mediastinum. J MinimAccess Surg 10:3436.
doi:10.4103/0972-9941.124469
99. Koezuka S, Hata Y, Sato F, Otsuka H,Makino T, Tochigi N,
IyodaA (2014) Malignant peripheral nerve sheath tumor in the
anteriormediastinum: a case report. Mol Clin Oncol 2:987990.
doi:10.3892/mco.2014.343
100. Koizumi K, Haraguchi S, Mikami I, Kubokura H, Okada
D,Yamagishi S, Kinoshita H, Enomoto Y, Shimizu K, Maeda M(2005)
Video-assisted thoracic surgery for Ewings sarcoma ofthe
mediastinum in a 3-year-old girl. Ann Thorac CardiovascSurg
11:117120
101. Kuschill-Dziurda J, Mastalerz L, Grzanka P,
Nizankowska-Mogilnicka E (2009) Rhabdomyoma as a tumor of the
posteriormediastinum. Pol Arch Med Wewn 119:599602
102. Kuzucu A, Erkal HS, Soysal O, Serin M (2006)
ExtraskeletalEwings sarcoma presenting with multifocal
intrathoracic masslesions associated with mediastinal shift. Ann
Thorac Surg 81:14871488. doi:10.1016/j.athoracsur.2005.03.116
103. Lamovec J, Sobel HJ, Zidar A, Jerman J (1990)
Epithelioidhemangioendothelioma of the anterior mediastinum
withosteoclast-like giant cells. Light microscopic,
immunohistochemi-cal, and electron microscopic study. Am J Clin
Pathol 93:813817
104. Lamy AL, Fradet GJ, Luoma A, Nelems B (1994) Anterior
andmiddle mediastinum paraganglioma: complete resection is
thetreatment of choice. Ann Thorac Surg 57:249252
105. Lang-Lazdunski L, Pons F, Jancovici R (2003)Malignant
Tritontumor of the posterior mediastinum: prolonged survival
afterstaged resection. Ann Thorac Surg 75:16451648
106. Lazure T, Essamet W, Palazzo L, Epardeau B, Fabre M
(2001)Cytological findings of a primary
mediastino-pulmonaryleiomyosarcoma. Report of a case diagnosed by
endoscopicultrasonography-guided fine needle aspiration.
Cytopathology12:410413
107. Lee DH, Park CK, Keum DY, Kim JB, Hwang I
(2012)Leiomyosarcoma of the posterior mediastinum extending intothe
adjacent spinal canal. Korean J Thorac Cardiovasc Surg 45:192195.
doi:10.5090/kjtcs.2012.45.3.192
108. Lee TJ, Reddy GP, Leung JW, Gotway MB (2008)
Mediastinalglomangioma: CT and octreotide scintigraphy appearance,
andreview of the literature. J Thorac Imaging 23:289291.
doi:10.1097/RTI.0b013e31817eee70
109. Li XM, Lin XY, XuHT, Yu JH,Wang L, Fan CF, Liu Y,Wang
EH(2013) Mediastinal epithelioid hemangioendothelioma with
abun-dant spindle cells and osteoclast-like giant cells mimicking
malig-nant fibrous histiocytoma. Diagn Pathol 8:103.
doi:10.1186/1746-1596-8-103
110. Lin J, Ho J, Chan A, Yeo W, Yip KM, Johnson PJ
(1995)Extraosseous osteogenic sarcoma of the mediastinum
occurringin a Chinese patient. Clin Oncol (R Coll Radiol)
7:200201
111. Lincoln JC (1965) Leiomyosarcoma of the anterior
mediastinum.Thorax 20:362366
112. Linnoila RI, Tsokos M, Triche TJ, Marangos PJ, Chandra
RS(1986) Evidence for neural origin and PAS-positive variants ofthe
malignant small cell tumor of thoracopulmonary region(Askin tumor).
Am J Surg Pathol 10:124133
113. Lodding P, Kindblom LG, Angervall L, Stenman G
(1990)Cellular schwannoma. A clinicopathologic study of 29cases.
Virchows Arch A Pathol Anat Histopathol 416:237248
114. Lyons LL, North PE, Mac-Moune Lai F, Stoler MH, Folpe
AL,Weiss SW (2004) Kaposiform hemangioendothelioma: a study of33
cases emphasizing its pathologic, immunophenotypic, and bi-ologic
uniqueness from juvenile hemangioma. Am J Surg Pathol28:559568
115. Maamouri F, Ennaifer Jerbi E, Tounsi Guettiti H, Boussen
H,Dellagi K, Boubaker S (2008) Multicentric
epithelioidhemangioendothelioma involving lung, mediastinum and
liver.Tunis Med 86:616617
116. Macchiarini P, Ostertag H (2004) Uncommon primary
mediastinaltumours. Lancet Oncol 5:107118.
doi:10.1016/S1470-2045(04)01385-3
117. Machida E, HaniudaM, Eguchi T, KuraiM,Yamanda T, Amano
J,Ota H (2003) Granular cell tumor of the mediastinum. Intern
Med42:178181
118. Malagon HD, Valdez AM, Moran CA, Suster S (2007) Germ
celltumors with sarcomatous components: a clinicopathologic
andimmunohistochemical study of 46 cases. Am J Surg Pathol
31:13561362. doi:10.1097/PAS.0b013e318033c7c4
119. Manduch M, Dexter DF, Ellis PM, Reid K, Isotalo PA
(2008)Extraskeletal Ewings sarcoma/primitive neuroectodermal
tumorof the posterior mediastinum with t(11;22)(q24;q12). Tumori
94:888891
120. Manivel C, Wick MR, Abenoza P, Rosai J (1986) The
occurrenceof sarcomatous components in primary mediastinal germ
cell tu-mors. Am J Surg Pathol 10:711717
121. Mansour Z, Neuville A, Massard G (2010)Mediastinal
epithelioidhaemangioendothelioma: a rare mediastinal tumour.
InteractCardiovasc Thorac Surg 10:122124.
doi:10.1510/icvts.2009.216978
122. Marchevsky AM (1999) Mediastinal tumors of peripheral
nervoussystem origin. Semin Diagn Pathol 16:6578
123. Matsuoka H, Nishio W, Sakamoto T, Harada H, Sashikata
T,Tsubota N (2002) Mediastinal angioleiomyoma. Ann ThoracSurg
73:16531654
124. McConnell YJ, Giacomantonio CA (2012) Malignant triton
tu-morscomplete surgical resection and adjuvant radiotherapy
as-sociated with improved survival. J Surg Oncol 106:5156.
doi:10.1002/jso.23042
Virchows Arch
-
125. Michel M, Pratt JW (2004) Anterior mediastinal
nonseminomatousgerm cell tumor with malignant transformation: a
case report. CurrSurg 61:576579.
doi:10.1016/j.cursur.2004.05.021
126. Miller R, Kurtz SM, Powers JM (1978)Mediastinal
rhabdomyoma.Cancer 42:19831988
127. Mineo TC, Biancari F, Cristino B, DAndrea V (1995)
Benignvascular tumours of the mediastinum: presentation of three
casesand review of the literature. Thorac Cardiovasc Surg
43:361364.doi:10.1055/s-2007-1013811
128. Misugi K, Okajima H, NewtonWA Jr, Kmetz DR, Delorimier
AA(1965) Mediastinal origin of a melanotic progonoma or
retinalanlage tumor: ultrastructural evidence for neural crest
origin.Cancer 18:477484
129. Moran CA, Koss MN (1993) Rhabdomyomatous thymoma. Am JSurg
Pathol 17:633636
130. Moran CA, Suster S (1995) Mediastinal hemangiomas: a study
of18 cases with emphasis on the spectrum of morphological
fea-tures. Hum Pathol 26:416421
131. Moran CA, Suster S (1997) Primary germ cell tumors of the
me-diastinum: I. Analysis of 322 cases with special emphasis
onteratomatous lesions and a proposal for histopathologic
classifica-tion and clinical staging. Cancer 80:681690
132. Moran CA, Suster S, Fishback N, Koss MN (1993)
Mediastinalparagangliomas. A clinicopathologic and
immunohistochemicalstudy of 16 cases. Cancer 72:23582364
133. Moran CA, Suster S, Perino G, Kaneko M, Koss MN
(1994)Malignant smooth muscle tumors presenting as mediastinal
softtissue masses. A clinicopathologic study of 10 cases. Cancer
74:22512260
134. Morita K, Shida Y, Shinozaki K, Uehara S, Seto T, Sugio
K,Ichinose Y, Nishiyama K, Matsuo Y, Hatakenaka M, Honda H(2012)
Angiomyolipomas of the mediastinum and the lung. JTho ra c Imag ing
27 :W21W23. do i : 10 . 1097 /RTI .0b013e31823150c7
135. Murakawa T, Nakajima J, Fukami T, Tanaka M, Takeuchi
E,Takamoto S (2001) Malignant fibrous histiocytoma in the
anteriormediastinum. Jpn J Thorac Cardiovasc Surg 49:722727
136. Nakamura M, Tachibana H, Mukaeyama T (1996) A case
ofleiomyoma of the posterior mediastinum. Nihon Kyobu GekaGakkai
Zasshi 44:20822086
137. Nakao M, Hishida T, Ishii G, Yoshida J, Nishimura M, Nagai
K(2012)Malignant granular cell tumor of the posterior
mediastinumwith dissemination. Asian Cardiovasc Thorac Ann 20:7173.
doi:10.1177/0218492311421453
138. Nayak HK, Vangipuram DR, Sonika U, Kar P, Kumar N, KapoorN
(2011) Mediastinal massa rare presentation of desmoplasticsmall
round cell tumour. BMJ Case Rep 2011. doi:
10.1136/bcr.10.2011.5042
139. Niwa H, Kondou K, Sekiguchi K (1988) A case of
mediastinalleiomyoma associated with cystic change and
calcificationa re-view of 7 cases in Japanese literatures.
NihonKyobu Geka GakkaiZasshi 36:21362139
140. ORegan GM, IrvineAD, YaoN, OMarcaigh A, Sheridan-PereiraM,
Phelan E, McDermott MB, Twomey A, Russell J, Watson R(2009)
Mediastinal and neck kaposiform hemangioendothelioma:report of
three cases. Pediatr Dermatol 26:331337.
doi:10.1111/j.1525-1470.2009.00913.x
141. Odze R, Begin L (1990)Malignant paraganglioma of the
posteriormediastinum. Cancer 65:667694
142. Odze R, Begin LR (1990) Malignant paraganglioma of the
poste-rior mediastinum. A case report and review of the
literature.Cancer 65:564569
143. Ohebsion J, OConnor WN, Attili AK, Diaz-Guzman E (2010)
A30-year-old man with facial flushing and a mediastinal mass.Chest
138:746749. doi:10.1378/chest.09-2847
144. Ohtsuka M, Satoh H, Inoue M, Yazawa T, Yamashita
YT,Sekizawa K, Hasegawa S (2000) Disseminated metastasis
ofneuroblastomatous component in immature mediastinal teratoma:a
case report. Anticancer Res 20:527530
145. Okudela K, Nakamura N, Sano J, Ito T, Kitamura H (2001)
Thymiccarcinosarcoma consisting of squamous cell carcinomatous and
em-bryonal rhabdomyosarcomatous components. Report of a case
andreview of the literature. Pathol Res Pract 197:205210
146. Olson J, Sayler W (1978) Mediastinal paragangliomas
(aorticbody tumor): a report of four cases and a review of the
literature.Cancer 41:24052412
147. Oshikiri T, Morikawa T, Jinushi E, Kawakami Y, Katoh H
(2001)Five cases of the lymphangioma of the mediastinum in adult.
AnnThorac Cardiovasc Surg 7:103105
148. Otani Y, Morishita Y, Yoshida I, Ishikawa S, Otaki A,
Aihara T,Nakajima T (1996) A malignant Triton tumor in the anterior
me-diastinum requiring emergency surgery: report of a case.
SurgToday 26:834836
149. Ouadnouni Y, Achir A, Bekarsabein S, Bouchikh M, Smahi
M,Msougar Y, Mahassini N, Benosman A (2009) Primary mediasti-nal
leiomyoma: a case report. Cases J 2:8555.
doi:10.4076/1757-1626-2-8555
150. Pachter MR (1963) Mediastinal nonchromaffin paraganglioma.
Aclinicopathologic study based on eight cases. J Thorac
CardiovascSurg 45:152160
151. Pachter MR, Lattes R (1963) Mesenchymal tumors of the
medi-astinum II. Tumors of blood vascular origin. Cancer
16:95107
152. Panasuk DB, Bauer TL, Davies AL, Schneider C, Flynn C
(2003)Commonmalignancies with uncommon sites of presentation:
case1. Anterior mediastinal rhabdomyosarcoma. J Clin Oncol
21:44554456. doi:10.1200/JCO.2003.03.149
153. Pandit S, Mukherjee S, Bhattacharya S, Dattachaudhuri
A,Bhuniya S, Deb J, Bhanja P (2012) A rare mediastinal tumourin a
young male mimicking massive pleural effusion. Lung India29:6669.
doi:10.4103/0970-2113.92368
154. Papagiannopoulos K, Sheppard MN, Goldstraw P (2000)
Thymichemangioma presenting with recurrent pleural effusion.
AnnThorac Surg 70:297299
155. Parham DM, Weeks DA, Beckwith JB (1994) The
clinicopatho-logic spectrum of putative extrarenal rhabdoid tumors.
An analysisof 42 cases studied with immunohistochemistry or
electron mi-croscopy. Am J Surg Pathol 18:10101029
156. Park JG, AubryMC, Godfrey JA,Midthun DE
(2006)Mediastinallymphangioma: Mayo Clinic experience of 25 cases.
Mayo ClinProc 81:11971203. doi:10.4065/81.9.1197
157. Park JY, Park NJ, Kim SP, Kwon KY, Lee SS (2012) A soft
tissueperineurioma and a hybrid tumor of perineurioma
andschwannoma. Korean J Pathol 46:7578.
doi:10.4132/KoreanJPathol.2012.46.1.75
158. Perlman EJ, Ali SZ, Robinson R, Lindato R, Griffin CA
(1998)Infantile extrarenal rhabdoid tumor. Pediatr Dev Pathol
1:149152
159. Ponce FA, Killory BD, Wait SD, Theodore N, Dickman CA(2011)
Endoscopic resection of intrathoracic tumors: experiencewith and
long-term results for 26 patients. J Neurosurg Spine 14:377381.
doi:10.3171/2010.11.SPINE09718
160. Qi Y, Chang B, Pang L, Liu C, Li F (2011) Solid alveolar
rhab-domyosarcoma with spindle-shaped cells and epithelial
differenti-ation of the mediastinum in a 68-year-old man: a case
report andliterature review. J Cancer Res Ther 7:353356.
doi:10.4103/0973-1482.87009
161. Quan GM, Irons S, Scripcaru G, Tang SK (2014) Posterior
medi-astinal paraspinal angioleiomyoma causing
thoracicradiculopathy. ANZ J Surg. doi:10.1111/ans.12639
162. Rajasingham AS, Cooray GH (1954) A large leiomyoma of
themediastinum. Br J Surg 41:446447
Virchows Arch
-
163. Rasaretnam R, Panabokke RG (1975) Leiomyosarcoma of
themediastinum. Br J Dis Chest 69:6369
164. Reali A, Mortellaro G, Allis S, Trevisiol E, Anglesio
SM,Bartoncini S, Ruo Redda MG (2013) A case of primary medias-tinal
Ewings sarcoma/primitive neuroectodermal tumor present-ing with
initial compression of superior vena cava. Ann ThoracMed 8:121123.
doi:10.4103/1817-1737.109834
165. Reeder LB (2000) Neurogenic tumors of the mediastinum.
SeminThorac Cardiovasc Surg 12:261267
166. RenW, XuX, Yan J, Qian X, Liu B (2014) Malignant triton
tumorof the anterior mediastinum: a case report. Oncol Lett
7:807810.doi:10.3892/ol.2014.1787
167. Ribet ME, Cardot GR (1994) Neurogenic tumors of the
thorax.Ann Thorac Surg 58:10911095
168. Robinson JM, Knoll R, Henry DA (1988) Intrathoracic
granularcell myoblastoma. South Med J 81:14531457
169. Romano R, Cesario A, Lococo F, Petrone G, Margaritora
S,Granone P (2013) Successful multidisciplinary management of
aprimary mediastinal Ewings sarcoma. Minerva Chir 68:121124
170. Rosenbloom PM, Barrows GH, Kmetz DR, Canty TG
(1975)Granular cell myoblastoma arising from the thoracic
sympatheticnerve chain. J Pediatr Surg 10:819822
171. Saito A, Watanabe K, Kusakabe T, Abe M, Suzuki T
(1998)Mediastinal mature teratoma with coexistence of
angiosarcoma,granulocytic sarcoma and a hematopoietic region in the
tumor: arare case of association between hematological malignancy
andmediastinal germ cell tumor. Pathol Int 48:749753
172. Salah S, Al-Ibraheem A, Daboor A, Al-Hussaini M
(2013)Synovial sarcoma presenting with huge mediastinal mass: a
casereport and review of the literature. BMC Res Notes 6:240
173. Salah S, Salem A (2014) Primary synovial sarcomas of the
medi-astinum: a systematic review and pooled analysis of the
publishedliterature. ISRN Oncol 2014:412527.
doi:10.1155/2014/412527
174. Salih Deveci M, Ceyhan K, Deveci G, Finci R (2001)
Pericardialrhabdomyomatous spindle cell thymoma with mucinous
cysticdegeneration. Histopathology 38:479481
175. Sartelet H, Lantuejoul S, Armari-Alla C, Pin I, Delattre
O,Brambilla E (1998) Solid alveolar rhabdomyosarcoma of the tho-rax
in a child. Histopathology 32:165171
176. Sayan M, Celik A, Ertunc O, Uluoglu O, Tastepe AI
(2014)Mediastinal neurothekeoma: a rare tumor. Asian
CardiovascThorac Ann. doi:10.1177/0218492314552857
177. Schenning R, Vajtai P, Troxell M, Pollock J, Hopkins K
(2013)Alveolar soft part sarcoma: unusual etiology of mediastinal
massin an adolescent. Clin Pract 3:e26. doi:10.4081/cp.2013.e26
178. Schulman H, Newman-Heinman N, Kurtzbart E, Maor E, ZirkinH,
Laufer L (2000) Thoracoabdominal peripheral
primitiveneuroectodermal tumors in childhood: radiological
features. EurRadiol 10:16491652. doi:10.1007/s003300000367
179. Segawa M, Kusajima Y, Senda K, Saito K (2007)
Mediastinalgranular cell tumor arising from the left recurrent
nerve; reportof a case. Kyobu Geka 60:595598
180. Shaffer K, Pugatch RD, Sugarbaker DJ (1990) Primary
mediasti-nal leiomyoma. Ann Thorac Surg 50:301302
181. Short M, Dramis A, Ramani P, Parikh DH (2008) Mediastinal
andpulmonary infantile myofibromatosis: an unusual surgical
presen-tation. J Pediatr Surg 43:e29e31.
doi:10.1016/j.jpedsurg.2008.06.046
182. Sidhu JS, NicolasMM,TaylorW (2002)Mediastinal rhabdomyoma:a
case report and review of the literature. Int J Surg Pathol
10:313318
183. Siraj F, Dhawan S, Jain D (2011) Invasive thymoma with
osseousmetaplasia and cystic change in a case of myasthenia gravis:
a rarepresentation. Gen Thorac Cardiovasc Surg 59:583586.
doi:10.1007/s11748-010-0726-4
184. Smith AR, Gilbert CF, Strausbauch P, Silverman JF (1998)
Fineneedle aspiration cytology of a mediastinal granular cell
tumorwith histologic confirmation and ancillary studies. A case
report.Acta Cytol 42:10111016
185. Soh WM, Yeong ML, Wong KP (2014) Malignant granular
celltumour of the mediastinum. Malays J Pathol 36:149151
186. Stark P, Smith DC, Watkins GE, Chun KE (1990) Primary
intra-thoracic extraosseous osteogenic sarcoma: report of three
cases.Radiology 174:725726. doi:10.1148/radiology.174.3.2305056
187. Steen BC, Florez Martin S, Fernandez Fau L, Garcia Tirado
J,Jareno Esteban J, Ancochea Bermudez J (1993)
Mediastinalleiomyosarcoma. An Med Interna 10:8385
188. Sunderrajan EV, Luger AM, Rosenholtz MJ, Maltby JD
(1984)Leiomyosarcoma in the mediastinum presenting as superior
venacava syndrome. Cancer 53:25532556
189. Suster S, Moran CA (1997) Malignant cartilaginous tumors of
themediastinum: clinicopathological study of six cases presenting
asextraskeletal soft tissue masses. Hum Pathol 28:588594
190. Suster S, Moran CA (2005) Primary synovial sarcomas of
themediastinum: a clinicopathologic, immunohistochemical, and
ul-trastructural study of 15 cases. Am J Surg Pathol 29:569578
191. Suster S, Moran CA, Koss MN (1994) Epithelioid
hemangio-endothelioma of the anterior mediastinum.
Clinicopathologic, im-munohistochemical, and ultrastructural
analysis of 12 cases. Am JSurg Pathol 18:871881
192. Suster S, Moran CA, KossMN (1994) Rhabdomyosarcomas of
theanterior mediastinum: report of four cases unassociated with
germcell, teratomatous, or thymic carcinomatous components.
HumPathol 25:349356
193. Tajima H, Tajima N, Yamamoto K,Maeda S, Koizumi K,
KumazakiT, Yoshida H, Egami K (1995) Anterior mediastinal
schwannoma: acase report. Radiat Med 13:175177
194. Tanaka Y, Yoshimasu T, Oura S, Hirai Y, Kawago M, Okamura
Y(2014) Primary clear-cell sarcoma in the mediastinum. Case
RepOncol 7:306309. doi:10.1159/000363180
195. Tane S, Tanaka Y, Tauchi S, Uchino K, Nakai R, Yoshimura
M(2011) Radically resected epithelioid angiosarcoma that
originatedin the mediastinum. Gen Thorac Cardiovasc Surg
59:503506.doi:10.1007/s11748-010-0710-z
196. Tarr RW, Kerner T, McCook B, Page DL, Nance EP, Kaye
JJ(1988) Primary extraosseous osteogenic sarcoma of the
mediasti-num: clinical, pathologic, and radiologic correlation.
South Med J81:13171319
197. Teh BM, Nickless D, Seevanayagam S (2011) Malignant
ossify-ing fibromyxoid tumour: a large anterior mediastinal
mass.Pathology 43:749751. doi:10.1097/PAT.0b013e32834c72b1
198. Thomson TA, Klijanienko J, Couturier J, Brisse H, Pierron
G,Freneaux P, Sastre-Garau X, Lagace R, Bourdeaut F
(2011)Fine-needle aspiration of renal and extrarenal rhabdoid
tumors:the experience of the Institut Curie regarding 20 tumors in
13patients. Cancer Cytopathol 119:4957. doi:10.1002/cncy.20121
199. Tirabosco R, Lang-Lazdunski L, Diss TC, AmaryMF,
Rodriguez-Justo M, Landau D, Lorenzi W, Flanagan AM (2009) Clear
cellsarcoma of the mediastinum. Ann Diagn Pathol 13:197200.
doi:10.1016/j.anndiagpath.2008.02.014
200. Torigian DA, Kaiser LR, Soma LA, Tomaszewski JE, Kotloff
R,Siegelman ES (2002) Symptomatic dysrhythmia caused by a
pos-terior mediastinal angiomyolipoma. AJR Am J Roentgenol
178:9396. doi:10.2214/ajr.178.1.1780093
201. Torres-Mora J, Dry S, Li X, Binder S, Amin M, Folpe AL
(2014)Malignant melanotic schwannian tumor: a clinicopathologic,
im-munohistochemical, and gene expression profiling study of
40cases, with a proposal for the reclassification of
melanoticschwannoma. Am J Surg Pathol 38:94105.
doi:10.1097/PAS.0b013e3182a0a150
Virchows Arch
-
202. Toursarkissian B, OConnor WN, Dillon ML (1990)
Mediastinalepithelioid hemangioendothelioma. Ann Thorac Surg
49:680685
203. Trupiano JK, Rice TW, Herzog K, Barr FG, Shipley J, Fisher
C,Goldblum JR (2002) Mediastinal synovial sarcoma: report of
twocases with molecular genetic analysis. Ann Thorac Surg
73:628630
204. Ulusakarya A, Terrier P, Regnard JF, de Montpreville V,
MunckJN (1999) Extraskeletal osteosarcoma of the mediastinum
aftertreatment of a mediastinal germ-cell tumor. Am J Clin Oncol
22:609614
205. Uno A, Sakurai M, Onuma K, Yamane Y, Kurita K, Hayashi
I,Ikeda M, Hagiwara N, Tominaga K, Hakozaki H (1988) A case ofgiant
mediastinal leiomyoma with long-term survival. Tohoku JExp Med
156:16
206. Vaish AK, Verma SK, Shakya S, Goel MM (2012) Schwannomain
anterior mediastinum with massive pericardial effusion. BMJCase Rep
2012. doi: 10.1136/bcr-2012-007867
207. Van Schil PE, Colpaert CG, Van Look R, Van OosteromAT,
EAVm, Reher SW, Schoofs EL (1993) Primary
mediastinalleiomyosarcoma. Thorac Cardiovasc Surg 41:377378.
doi:10.1055/s-2007-1013895
208. Venuta F, Pescarmona EO, Rendina EA, Ciriaco P, De Giacomo
T,Ricci C (1993) Primary osteogenic sarcoma of the posterior
me-diastinum. Case report. Scand J Thorac Cardiovasc Surg
27:169173
209. Vrtik M, Larbalestier RI, Cameron D, Gupta A, Sinniah R
(2004)Giant superior mediastinal angioleiomyoma. J Thorac
CardiovascSurg 128:786788. doi:10.1016/j.jtcvs.2004.03.035
210. Wallenstein MB, Hole MK, McCarthy C, Fijalkowski N, Jeng
M,Wo n g W B ( 2 0 1 4 ) M e d i a s t i n a l K a p o s i f o r
mhemangioendothelioma and Kasabach-Merritt phenomenon in apatient
with no skin changes and a normal chest CT. PediatrHematol Oncol.
doi:10.3109/08880018.2013.825356
211. Walsh MA, Carcao M, Pope E, Lee KJ (2008)
Kaposiformhemangioendothelioma presenting antenatally with a
pericardialeffusion. J Pediatr Hematol Oncol 30:761763.
doi:10.1097/MPH.0b013e318175c244
212. Warth A, Herpel E, Schmahl A, Hoffmann H, Herth
FJ,Schirmacher P, Dienemann H, Schnabel PA (2008)
Mediastinalangiomyolipomas in a male patient affected by tuberous
sclerosis.Eur Respir J 31:678680. doi:10.1183/09031936.00021207
213. Watanabe S, Sato H, Tawaraya K, Tsubota M, Endo M, Seki
M(1997) A case of mediastinal angiomyolipoma. Nihon KyobuGeka
Gakkai Zasshi 45:18891892
214. Watts KA, Watts JR Jr (2007) Incidental discovery of an
anteriormediastinal angiomyolipoma. J Thorac Imaging 22:180181.
doi:10.1097/01.rti.0000213571.09280.f8
215. Weidner N (1991) Atypical tumor of the mediastinum:
epithelioidhemangioendothelioma containing metaplastic bone
andosteoclastlike giant cells. Ultrastruct Pathol 15:481488
216. Weiss SW, Enzinger FM (1982) Epithelioid
hemangioendothelioma:a vascular tumor oftenmistaken for a
carcinoma. Cancer 50:970981
217. Weissferdt A, Kalhor N, Suster S, Moran CA (2010)
Primaryangiosarcomas of the anterior mediastinum: a
clinicopathologicand immunohistochemical study of 9 cases. Hum
Pathol 41:17111717. doi:10.1016/j.humpath.2010.05.003
218. White W, Shiu MH, Rosenblum MK, Erlandson RA, WoodruffJM
(1990) Cellular schwannoma. A clinicopathologic study of 57patients
and 58 tumors. Cancer 66:12661275
219. Wick MR, Rosai J (1991) Neuroendocrine neoplasms of the
me-diastinum. Semin Diagn Pathol 8:3551
220. Wilken JJ, Meier FA, Kornstein MJ (2000)
Kaposiformhemangioendothelioma of the thymus. Arch Pathol Lab
Med124 : 1 5 4 2 154 4 . d o i : 1 0 . 1 0 4 3 / 0 0 0 3 - 9 9 8 5
( 2 0 0 0 )1242.0.CO;2
221. Wilson H (1941) Extraskeletal ossifying tumors. Ann Surg
113:95112
222. Wilson RW, Moran CA (1998) Primary ependymoma of the
me-diastinum: a clinicopathologic study of three cases. Ann
DiagnPathol 2:293300
223. Woodruff JM, Godwin TA, Erlandson RA, Susin M, Martini
N(1981) Cellular schwannoma: a variety of schwannoma some-times
mistaken for a malignant tumor. Am J Surg Pathol 5:733744
224. Yanagawa N, Sasou S, Sato T, Shiono S, Kato H
(2006)Mediastinal granular cell tumor: report of a case. Kyobu
Geka59:418421
225. Yasuda A, Mizuno A, Mishima A, Sasaki S, Ochi N, Wakasugi
T,Sawai H, Takeyama H, Manabe T (2007) Posterior
mediastinalangioleiomyoma: report of a case. J Thorac Imaging
22:363365. doi:10.1097/RTI.0b013e31813fabb5
226. Yasui N, Koh K, Kato M, Park MJ, Tomizawa D, Oshima
K,Uchisaka N, Gocho Y, Arakawa A, Seki M, Oguma E,Kishimoto H,
Watanabe S, Kikuchi A, Hanada R (2013)Kasabach-Merritt phenomenon:
a report of 11 cases from a singleinstitution. J Pediatr Hematol
Oncol 35:554558. doi:10.1097/MPH.0b013e318281558e
227. Yazici U, Gulhan E, Yazici U, Yaran P, Cakir E, Tastepe I
(2011) Acase of giant mediastinal leiomyoma. Turk J Gastroenterol
22:656657
228. Younker D, Boozalis JE (1991) A thoracic leiomyosarcoma
pro-ducing tracheal obstruction. J Clin Anesth 3:344346
229. Yousem SA, Hochholzer L (1987) Unusual thoracic
manifesta-tions of epithelioid hemangioendothelioma. Arch Pathol
LabMed 111:459463
230. Zehani A, Ayadi-Kaddour A, Daghfous H, Ridene I, Marghli
A,Kilani T, El Mezni F (2011) Primary mediastinal sarcomas. RevMal
Respir 28:1424. doi:10.1016/j.rmr.2010.05.015
231. Zhang WD, Zhao LL, Huang XB, Cai PQ, Xu GX (2010)Computed
tomography imaging of anterior and middle mediasti-nal Ewing
sarcoma/primitive neuroectodermal tumors. J ThoracImaging
25:168172. doi:10.1097/RTI.0b013e3181a99117
232. Zisis C, Fragoulis S, Rontogianni D, Stratakos G, Bellenis
I (2006)Malignant triton tumour of the anterior mediastinum as
incidentalfinding. Monaldi Arch Chest Dis 65:222224
233. Zolota V, Tzelepi V, Charoulis N, Apostolakis E, Dougenis
D(2006) Mediastinal rhabdomyoma: case report and review of
theliterature. Virchows Arch 449:124128.
doi:10.1007/s00428-006-0211-8
234. Zukerberg LR, Nickoloff BJ, Weiss SW (1993)
Kaposiformhemangioendothelioma of infancy and childhood. An
aggressiveneoplasm associated with Kasabach-Merritt syndrome
andlymphangiomatosis. Am J Surg Pathol 17:321328
Virchows Arch
Mesenchymal tumours of the mediastinumpart
IIAbstractIntroductionSmooth muscle tumours
Pericytic (perivascular) tumoursSkeletal muscle tumoursVascular
tumoursBenign and intermediate-grade vascular tumoursMalignant
vascular tumours
Chondro-osseous tumoursEwing sarcoma/primitive neuroectodermal
tumour (PNET)
Nerve sheath tumours and tumours derived from the autonomic
nervous systemTumours of uncertain differentiationAngiomatoid
fibrous histiocytomaOssifying fibromyxoid tumourMyoepithelial
tumours including parachordomaSynovial sarcomaEpithelioid
sarcomaAlveolar soft part sarcoma (ASPS)Clear cell sarcoma of soft
tissueExtraskeletal myxoid chondrosarcomaExtrarenal rhabdoid
tumourPEComaDesmoplastic small round cell
tumourUnclassified/undifferentiated sarcoma
References










![Mesenchymal tumours of the mediastinum part I · mediastinal liposarcomas are large, and tumours up to 7 kg havebeenreported[105].Tumoursmayremainasymptomatic for long periods. Shortness](https://img.pdfslide.net/doc/110x75/5f7d0297e752d81f3415c77c/mesenchymal-tumours-of-the-mediastinum-part-i-mediastinal-liposarcomas-are-large.jpg)