Embed Size (px)
Citation preview
1
Metabolic Activation and Idiosycratic Drug Toxicity: By Avoiding Structural
Alerts, Do We Mitigate Risks?
Amit S. Kalgutkar, Ph.D. Pfizer Global Research and Development
Groton, CT 06340, USA
2
Cause(s) of Attrition in Drug Discovery
• In the early 90’s, major cause of attrition was poor pharmacokinetics1,2
– Largely resolved via involvement of DM/PK groups at early stages of drug discovery (Exploratory/Lead development/candidate-seeking)
• Of late: lack of efficacy (achieving POM for novel targets) and drug safety are the leading causes of candidate attrition – Pharmacology tactics to counterbalance attrition
• Better understanding of pharmacological targets • Incorporation of translational pharmacology (PK/PD, disease
biomarkers, etc) • Probe concept (exploratory INDs, etc)
– Tactics to counterbalance safety-related attrition arising from IADRs • ?
1Roberts SA (2003) Drug metabolism and pharmacokinetics in drug discovery. Curr Opin Drug Discov Devel. 6(1):66-80. 2Kola I and Landis J (2004) Can the pharmaceutical industry reduce attrition rates? Nat Rev Drug Discov. 3(8):711-5
3
Safety-Related Attrition: Adverse Drug Reactions (ADRs)
• ADRs Contribute to patient morbidity and mortality – One of the most common causes for drug recalls or black box warning labels
• Of a total of 548 drugs approved in the period from 1975-1999, 45 drugs (8.2%) acquired 1 or more black box warnings, 16 (2.9%) were withdrawn from the market
• ADR Classification – Type A ADRs: ~ 80% of ADRs fall in this category
• Type A ADRs can be predicted from known drug pharmacology (e.g. Hemorrhage with anticoagulants)
• Dose dependent – can be reversed with dose reduction • Generally identified in preclinical species (animal models of pharmacology)
– Type B (Bizarre) or Idiosyncratic ADRs (e.g., hepatotoxicity, skin rashes, aplastic anaemia, agranulocytosis) – e.g., black box warning for “sulfonamides”
• Unrelated to primary pharmacology • Dose independent (with the exception of some drugs) – can occur at any dose within the
therapeutic range • Temporal relationship - Symptoms subsides after cessation of treatment; rapid onset upon
re-challenge • Can be severe - maybe fatal - most common cause for drug withdrawal • Cannot be predicted from traditional toxicological studies in animals • Rare - frequency of occurrence - 1 in 10,000 to 1 in 100,000
– Normally not observed until phase III or post launch
4
Associating a Functional Group with Adverse Drug Reactions – Sulfonamides have achieved notoriety with respect to
hypersensitivity (e.g., skin rashes)
See - Kalgutkar, A. S., Jones, R. and Sawant, A. ”Sulfonamide as an Essential Functional Group in Drug Design” In Metabolism, Pharmacokinetics and Toxicity of Functional Groups: Impact of the Building Blocks of Medicinal Chemistry on ADMET (Royal Society of Chemistry), [Dennis A. Smith, Editor], 2010, Chapter 5, pp. 210 – 273.
5
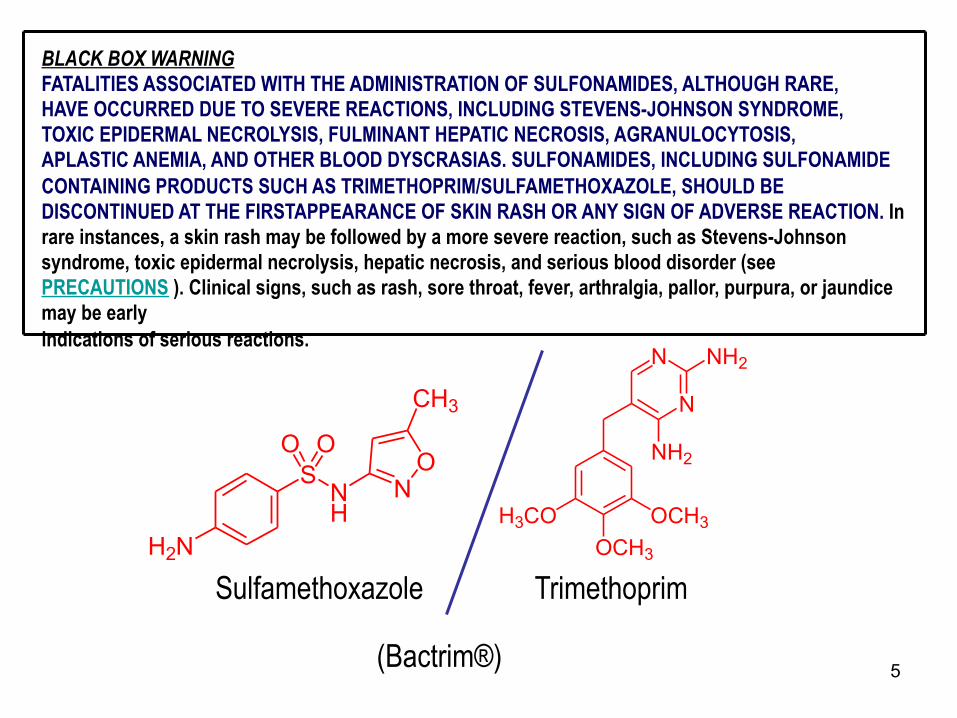
BLACK BOX WARNING FATALITIES ASSOCIATED WITH THE ADMINISTRATION OF SULFONAMIDES, ALTHOUGH RARE, HAVE OCCURRED DUE TO SEVERE REACTIONS, INCLUDING STEVENS-JOHNSON SYNDROME, TOXIC EPIDERMAL NECROLYSIS, FULMINANT HEPATIC NECROSIS, AGRANULOCYTOSIS, APLASTIC ANEMIA, AND OTHER BLOOD DYSCRASIAS. SULFONAMIDES, INCLUDING SULFONAMIDE CONTAINING PRODUCTS SUCH AS TRIMETHOPRIM/SULFAMETHOXAZOLE, SHOULD BE DISCONTINUED AT THE FIRSTAPPEARANCE OF SKIN RASH OR ANY SIGN OF ADVERSE REACTION. In rare instances, a skin rash may be followed by a more severe reaction, such as Stevens-Johnson syndrome, toxic epidermal necrolysis, hepatic necrosis, and serious blood disorder (see PRECAUTIONS ). Clinical signs, such as rash, sore throat, fever, arthralgia, pallor, purpura, or jaundice may be early indications of serious reactions.
H2N
SNH
O O
NO
CH3
H3CO OCH3OCH3
N
N
NH2
NH2
Sulfamethoxazole Trimethoprim
(Bactrim®)

6
7
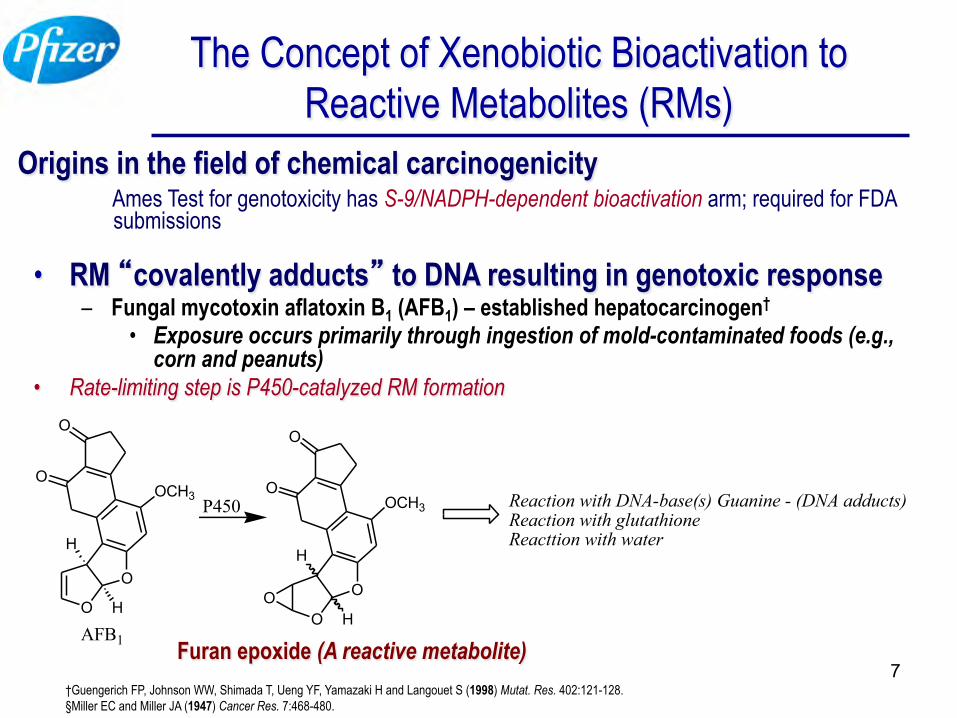
The Concept of Xenobiotic Bioactivation to Reactive Metabolites (RMs)
Origins in the field of chemical carcinogenicity Ames Test for genotoxicity has S-9/NADPH-dependent bioactivation arm; required for FDA submissions
• RM “covalently adducts” to DNA resulting in genotoxic response – Fungal mycotoxin aflatoxin B1 (AFB1) – established hepatocarcinogen†
• Exposure occurs primarily through ingestion of mold-contaminated foods (e.g., corn and peanuts)
• Rate-limiting step is P450-catalyzed RM formation
O
O
H
H
OCH3O
O
AFB1O
O
H
H
OCH3O
O
P450
O
Reaction with DNA-base(s) Guanine - (DNA adducts)Reaction with glutathioneReacttion with water
†Guengerich FP, Johnson WW, Shimada T, Ueng YF, Yamazaki H and Langouet S (1998) Mutat. Res. 402:121-128. §Miller EC and Miller JA (1947) Cancer Res. 7:468-480.
Furan epoxide (A reactive metabolite)
8
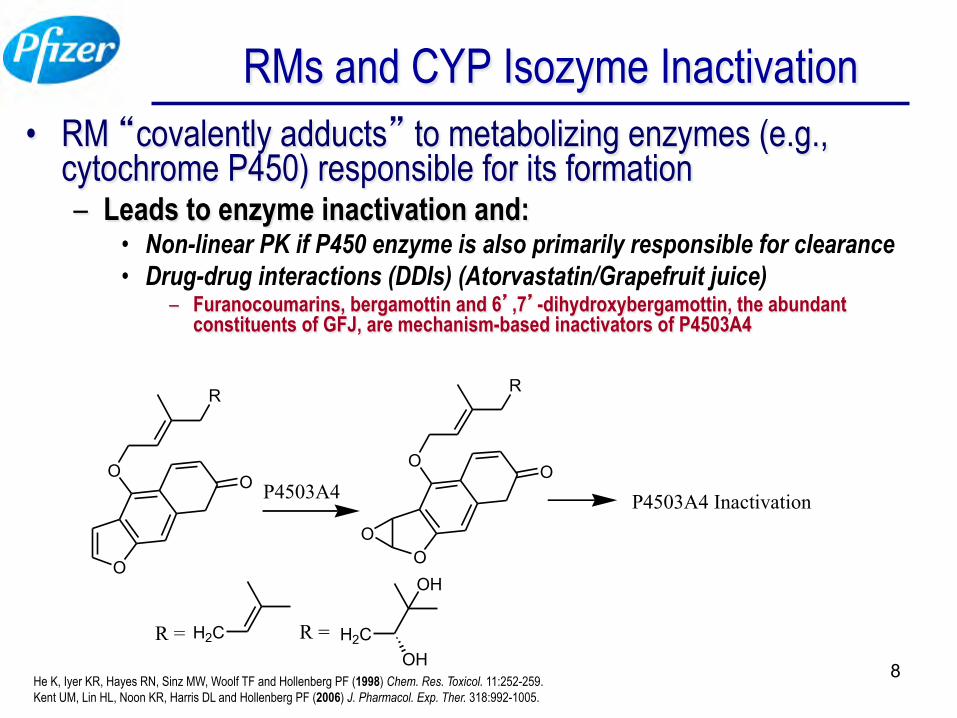
RMs and CYP Isozyme Inactivation • RM “covalently adducts” to metabolizing enzymes (e.g.,
cytochrome P450) responsible for its formation – Leads to enzyme inactivation and:
• Non-linear PK if P450 enzyme is also primarily responsible for clearance • Drug-drug interactions (DDIs) (Atorvastatin/Grapefruit juice)
– Furanocoumarins, bergamottin and 6’,7’-dihydroxybergamottin, the abundant constituents of GFJ, are mechanism-based inactivators of P4503A4
O
OO
R
R = H2C R =
OH
OHH2C
P4503A4
O
OO
R
O
P4503A4 Inactivation
He K, Iyer KR, Hayes RN, Sinz MW, Woolf TF and Hollenberg PF (1998) Chem. Res. Toxicol. 11:252-259. Kent UM, Lin HL, Noon KR, Harris DL and Hollenberg PF (2006) J. Pharmacol. Exp. Ther. 318:992-1005.
9
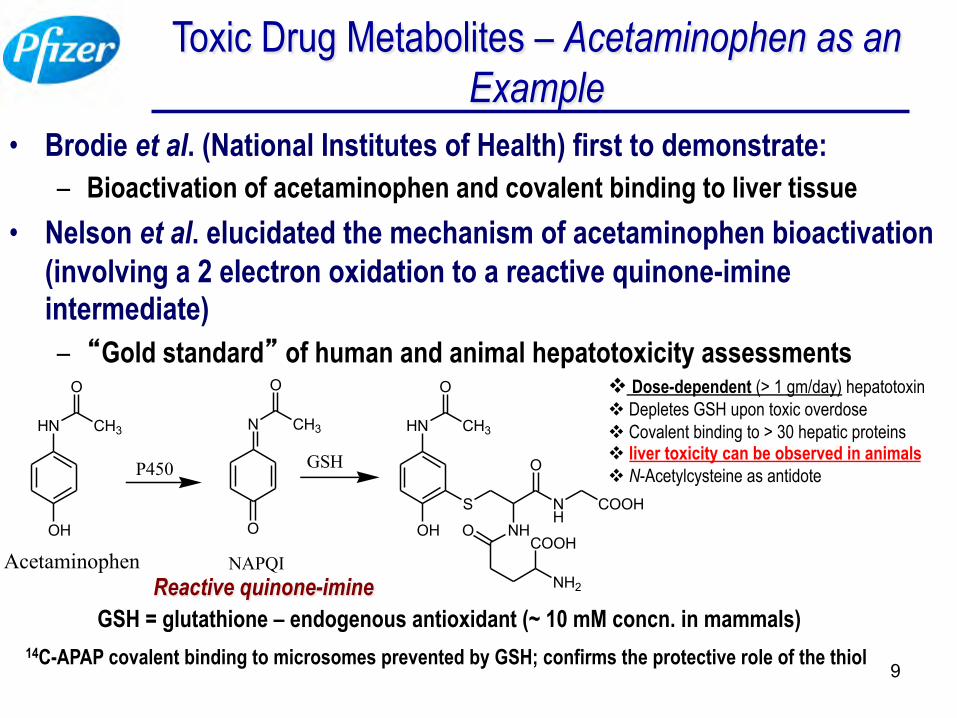
Toxic Drug Metabolites – Acetaminophen as an Example
• Brodie et al. (National Institutes of Health) first to demonstrate: – Bioactivation of acetaminophen and covalent binding to liver tissue
• Nelson et al. elucidated the mechanism of acetaminophen bioactivation (involving a 2 electron oxidation to a reactive quinone-imine intermediate) – “Gold standard” of human and animal hepatotoxicity assessments
v Dose-dependent (> 1 gm/day) hepatotoxin v Depletes GSH upon toxic overdose v Covalent binding to > 30 hepatic proteins v liver toxicity can be observed in animals v N-Acetylcysteine as antidote
HN
OH
CH3
O
Acetaminophen
P450
N
O
CH3
O
NAPQI
GSH
HN
OH
CH3
O
S
NH
NH
O
COOH
O
NH2
COOH
GSH = glutathione – endogenous antioxidant (~ 10 mM concn. in mammals) 14C-APAP covalent binding to microsomes prevented by GSH; confirms the protective role of the thiol
Reactive quinone-imine
10
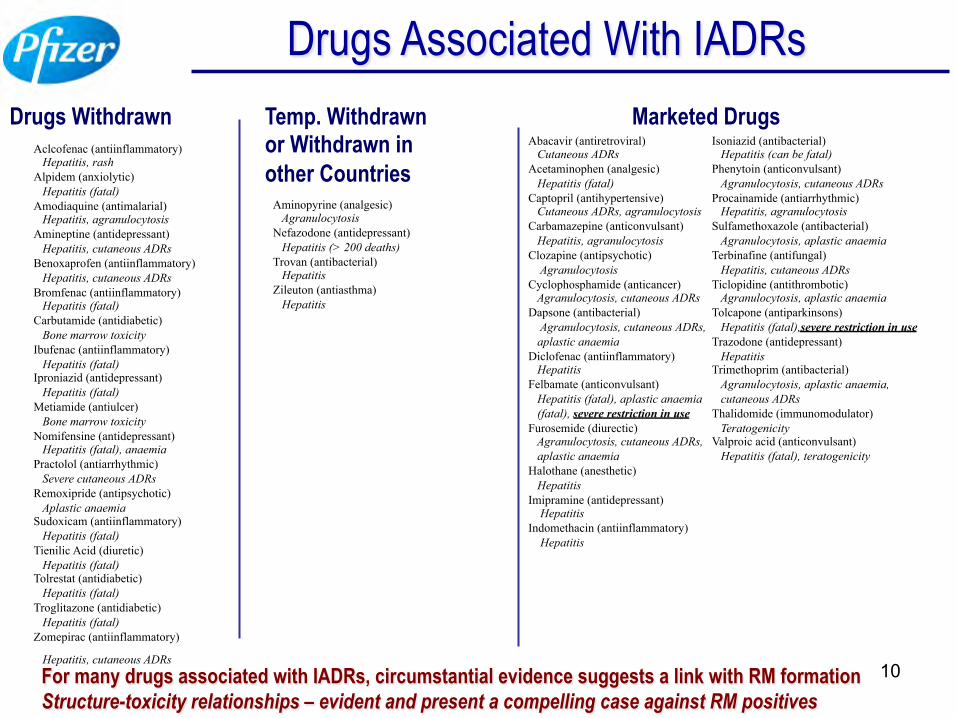
Drugs Associated With IADRs Drugs Withdrawn
Aclcofenac (antiinflammatory) Hepatitis, rash Alpidem (anxiolytic) Hepatitis (fatal) Amodiaquine (antimalarial) Hepatitis, agranulocytosis Amineptine (antidepressant) Hepatitis, cutaneous ADRs Benoxaprofen (antiinflammatory) Hepatitis, cutaneous ADRs Bromfenac (antiinflammatory) Hepatitis (fatal) Carbutamide (antidiabetic) Bone marrow toxicity Ibufenac (antiinflammatory) Hepatitis (fatal) Iproniazid (antidepressant) Hepatitis (fatal) Metiamide (antiulcer) Bone marrow toxicity Nomifensine (antidepressant) Hepatitis (fatal), anaemia Practolol (antiarrhythmic) Severe cutaneous ADRs Remoxipride (antipsychotic) Aplastic anaemia Sudoxicam (antiinflammatory) Hepatitis (fatal) Tienilic Acid (diuretic) Hepatitis (fatal) Tolrestat (antidiabetic) Hepatitis (fatal) Troglitazone (antidiabetic) Hepatitis (fatal) Zomepirac (antiinflammatory)
Hepatitis, cutaneous ADRs
Marketed Drugs Abacavir (antiretroviral) Cutaneous ADRs Acetaminophen (analgesic) Hepatitis (fatal) Captopril (antihypertensive) Cutaneous ADRs, agranulocytosis Carbamazepine (anticonvulsant) Hepatitis, agranulocytosis Clozapine (antipsychotic) Agranulocytosis Cyclophosphamide (anticancer) Agranulocytosis, cutaneous ADRs Dapsone (antibacterial) Agranulocytosis, cutaneous ADRs, aplastic anaemia Diclofenac (antiinflammatory) Hepatitis Felbamate (anticonvulsant) Hepatitis (fatal), aplastic anaemia (fatal), severe restriction in use Furosemide (diurectic) Agranulocytosis, cutaneous ADRs, aplastic anaemia Halothane (anesthetic) Hepatitis Imipramine (antidepressant) Hepatitis Indomethacin (antiinflammatory) Hepatitis
Isoniazid (antibacterial) Hepatitis (can be fatal) Phenytoin (anticonvulsant) Agranulocytosis, cutaneous ADRs Procainamide (antiarrhythmic) Hepatitis, agranulocytosis Sulfamethoxazole (antibacterial) Agranulocytosis, aplastic anaemia Terbinafine (antifungal) Hepatitis, cutaneous ADRs Ticlopidine (antithrombotic) Agranulocytosis, aplastic anaemia Tolcapone (antiparkinsons) Hepatitis (fatal),severe restriction in use Trazodone (antidepressant) Hepatitis Trimethoprim (antibacterial) Agranulocytosis, aplastic anaemia, cutaneous ADRs Thalidomide (immunomodulator) Teratogenicity Valproic acid (anticonvulsant) Hepatitis (fatal), teratogenicity
Temp. Withdrawn or Withdrawn in other Countries
Aminopyrine (analgesic) Agranulocytosis Nefazodone (antidepressant) Hepatitis (> 200 deaths) Trovan (antibacterial) Hepatitis Zileuton (antiasthma) Hepatitis
For many drugs associated with IADRs, circumstantial evidence suggests a link with RM formation Structure-toxicity relationships – evident and present a compelling case against RM positives
11
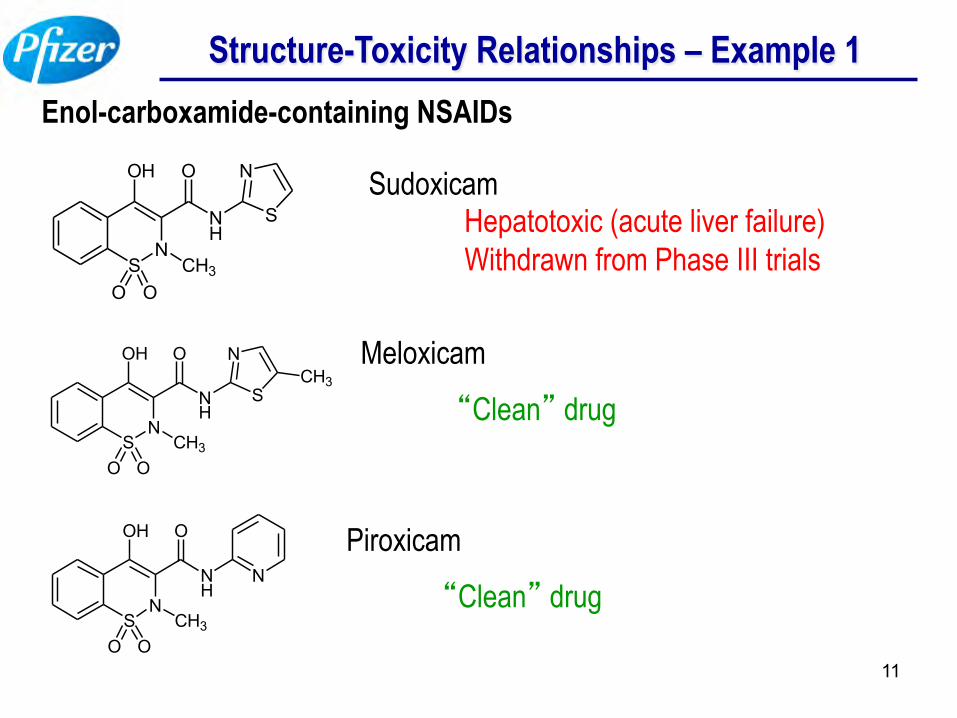
Structure-Toxicity Relationships – Example 1 Enol-carboxamide-containing NSAIDs
Sudoxicam Hepatotoxic (acute liver failure) Withdrawn from Phase III trials
Meloxicam
“Clean” drug
Piroxicam
“Clean” drug
SN
OH
CH3O O
NH
O
S
N
SN
OH
CH3O O
NH
O
S
NCH3
SN
OH
CH3O O
NH
O
N
12
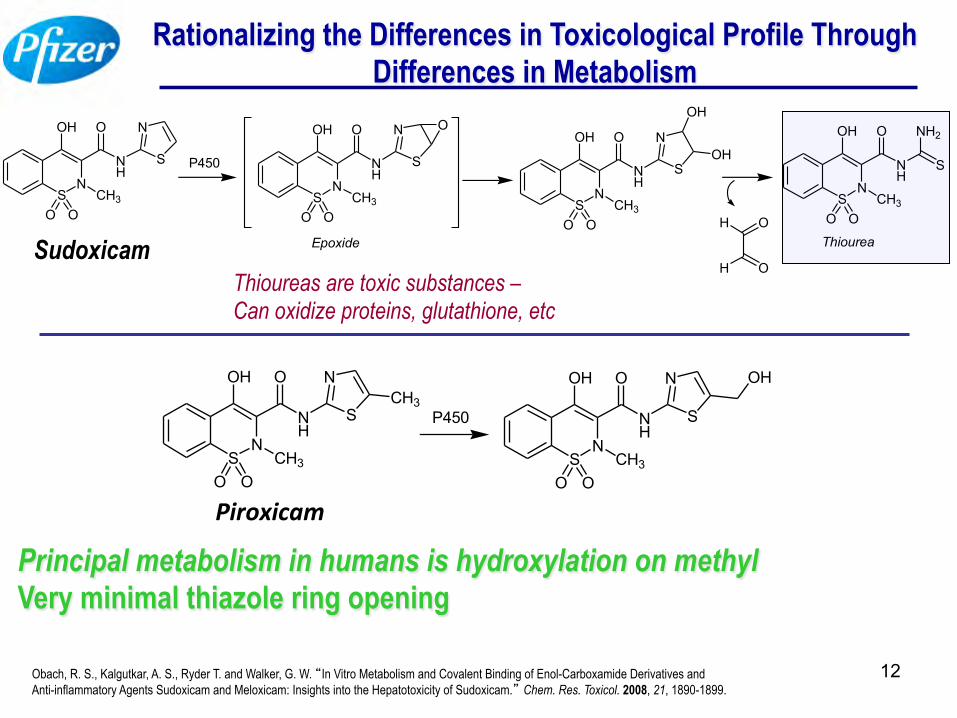
Rationalizing the Differences in Toxicological Profile Through Differences in Metabolism
SN
OH
CH3O O
NH
O
S
N
P450
SN
OH
CH3O O
NH
O
S
N O
SN
OH
CH3O O
NH
O
S
N
OH
OH
SN
OH
CH3O O
NH
O NH2
S
Epoxide ThioureaOH
OHThioureas are toxic substances – Can oxidize proteins, glutathione, etc
SN
OH
CH3O O
NH
O
S
NCH3
P450
SN
OH
CH3O O
NH
O
S
N OH
Sudoxicam
Piroxicam
Principal metabolism in humans is hydroxylation on methyl Very minimal thiazole ring opening
Obach, R. S., Kalgutkar, A. S., Ryder T. and Walker, G. W. “In Vitro Metabolism and Covalent Binding of Enol-Carboxamide Derivatives and Anti-inflammatory Agents Sudoxicam and Meloxicam: Insights into the Hepatotoxicity of Sudoxicam.” Chem. Res. Toxicol. 2008, 21, 1890-1899.
13
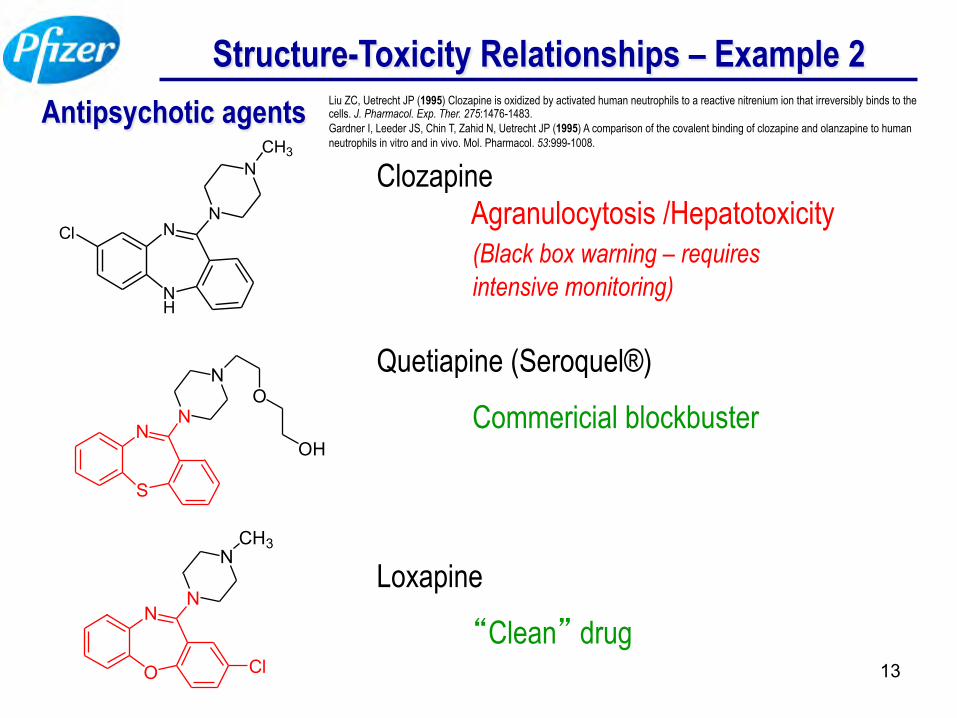
Structure-Toxicity Relationships – Example 2 Antipsychotic agents
NH
NClN
NCH3
S
NN
NO
OH
O
NN
NCH3
Cl
Clozapine Agranulocytosis /Hepatotoxicity (Black box warning – requires intensive monitoring)
Quetiapine (Seroquel®)
Commericial blockbuster
Loxapine
“Clean” drug
Liu ZC, Uetrecht JP (1995) Clozapine is oxidized by activated human neutrophils to a reactive nitrenium ion that irreversibly binds to the cells. J. Pharmacol. Exp. Ther. 275:1476-1483. Gardner I, Leeder JS, Chin T, Zahid N, Uetrecht JP (1995) A comparison of the covalent binding of clozapine and olanzapine to human neutrophils in vitro and in vivo. Mol. Pharmacol. 53:999-1008.
14
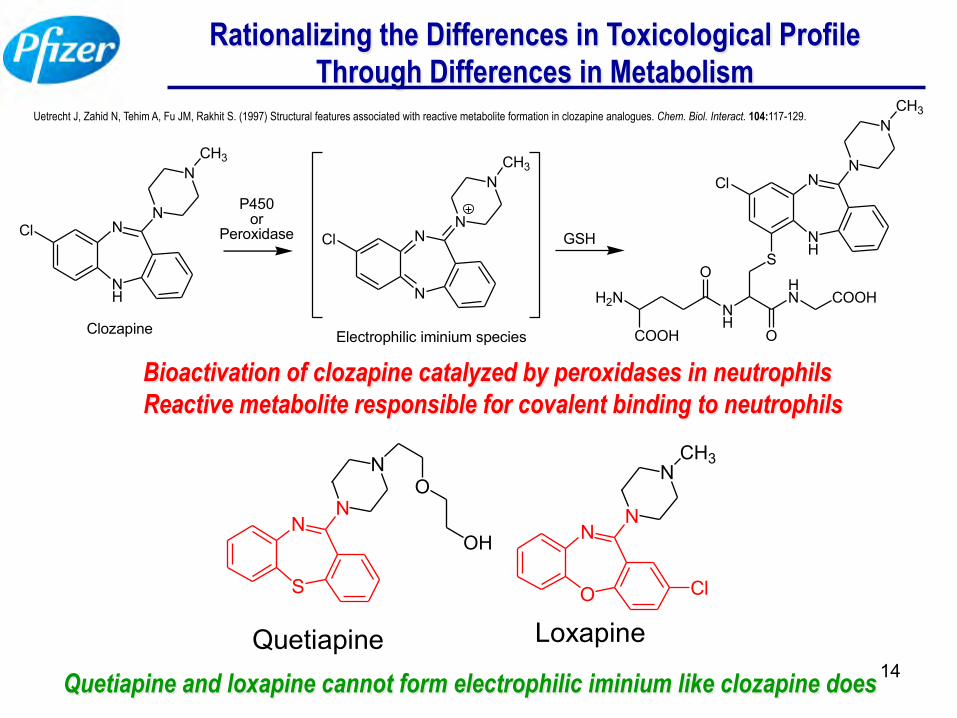
Rationalizing the Differences in Toxicological Profile Through Differences in Metabolism
NH
NClN
NCH3
Clozapine
P450 or
Peroxidase
N
NClN
NCH3
Electrophilic iminium species
GSH NH
NClN
NCH3
S
NH
HN
O
COOH
O
H2N
COOH
Bioactivation of clozapine catalyzed by peroxidases in neutrophils Reactive metabolite responsible for covalent binding to neutrophils
O
NN
NCH3
Loxapine
ClS
NN
N
Quetiapine
O
OH
Quetiapine and loxapine cannot form electrophilic iminium like clozapine does
Uetrecht J, Zahid N, Tehim A, Fu JM, Rakhit S. (1997) Structural features associated with reactive metabolite formation in clozapine analogues. Chem. Biol. Interact. 104:117-129.
15
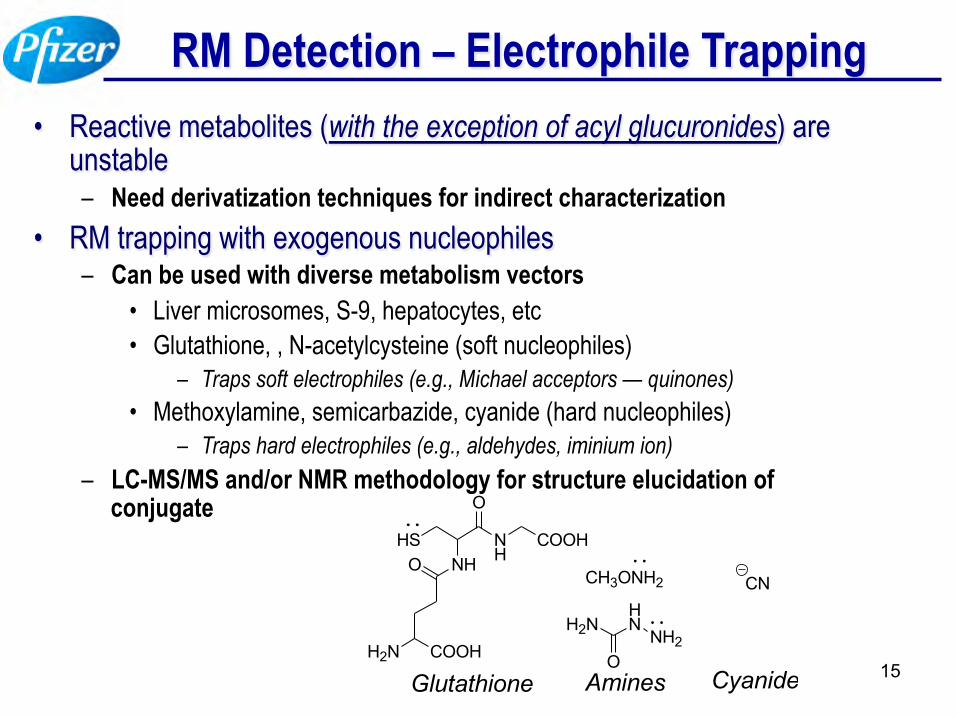
RM Detection – Electrophile Trapping • Reactive metabolites (with the exception of acyl glucuronides) are
unstable – Need derivatization techniques for indirect characterization
• RM trapping with exogenous nucleophiles – Can be used with diverse metabolism vectors
• Liver microsomes, S-9, hepatocytes, etc • Glutathione, , N-acetylcysteine (soft nucleophiles)
– Traps soft electrophiles (e.g., Michael acceptors — quinones) • Methoxylamine, semicarbazide, cyanide (hard nucleophiles)
– Traps hard electrophiles (e.g., aldehydes, iminium ion) – LC-MS/MS and/or NMR methodology for structure elucidation of
conjugate HS
NHNH
O
COOHO
H2N COOH
Glutathione
CN
Cyanide
CH3ONH2
Amines
NH2
HNH2N
O
16
RM Detection – Covalent Binding • Limited to availability of radiolabeled drug candidate
– May not be suitable in early discovery
• In Vitro covalent binding can be assessed with diverse metabolism vectors – Effect of competing/detoxicating drug metabolizing enzymes on
covalent binding can also be examined • In vivo covalent binding can be assessed in
preclinical species • Covalent binding data is quantitative
– No information on nature of proteins modified
17
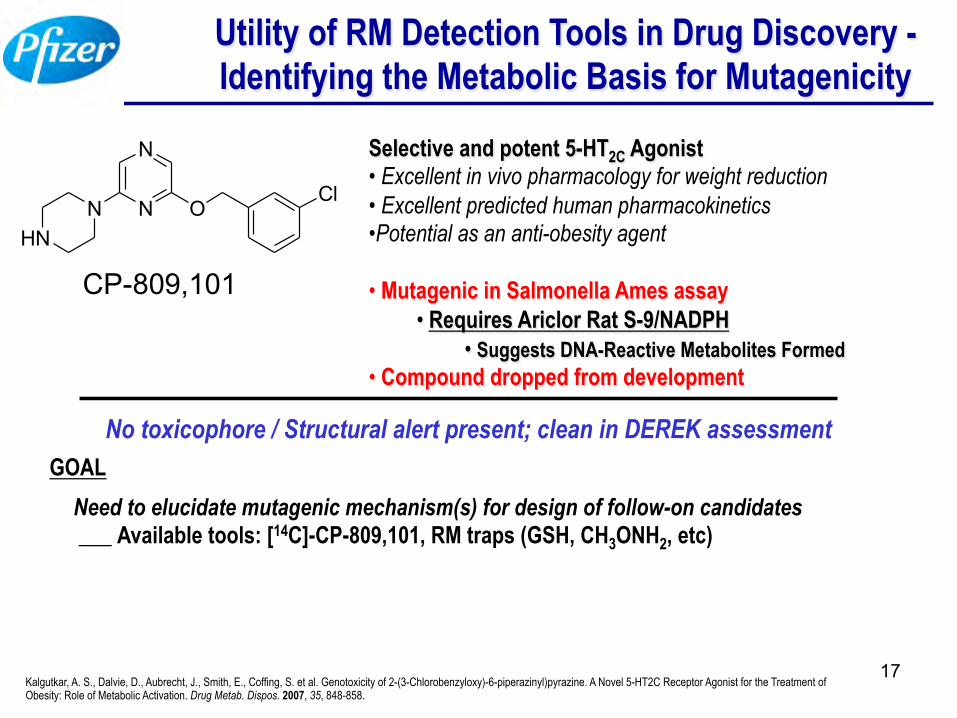
Utility of RM Detection Tools in Drug Discovery - Identifying the Metabolic Basis for Mutagenicity
N
N
NHN
OCl
CP-809,101
Selective and potent 5-HT2C Agonist • Excellent in vivo pharmacology for weight reduction • Excellent predicted human pharmacokinetics • Potential as an anti-obesity agent • Mutagenic in Salmonella Ames assay
• Requires Ariclor Rat S-9/NADPH • Suggests DNA-Reactive Metabolites Formed
• Compound dropped from development
Need to elucidate mutagenic mechanism(s) for design of follow-on candidates ___ Available tools: [14C]-CP-809,101, RM traps (GSH, CH3ONH2, etc)
GOAL
Kalgutkar, A. S., Dalvie, D., Aubrecht, J., Smith, E., Coffing, S. et al. Genotoxicity of 2-(3-Chlorobenzyloxy)-6-piperazinyl)pyrazine. A Novel 5-HT2C Receptor Agonist for the Treatment of Obesity: Role of Metabolic Activation. Drug Metab. Dispos. 2007, 35, 848-858.
No toxicophore / Structural alert present; clean in DEREK assessment
18
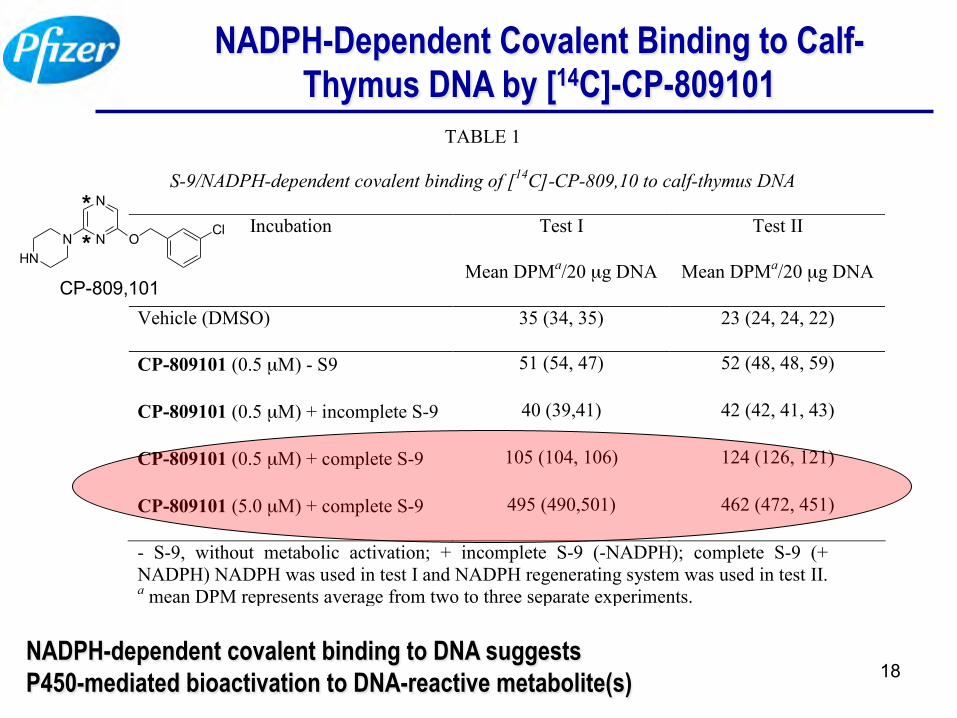
NADPH-Dependent Covalent Binding to Calf-Thymus DNA by [14C]-CP-809101
TABLE 1
S-9/NADPH-dependent covalent binding of [14C]-CP-809,10 to calf-thymus DNA
Incubation Test I
Mean DPMa/20 µg DNA
Test II
Mean DPMa/20 µg DNA
Vehicle (DMSO) 35 (34, 35) 23 (24, 24, 22)
CP-809101 (0.5 µM) - S9 51 (54, 47) 52 (48, 48, 59)
CP-809101 (0.5 µM) + incomplete S-9 40 (39,41) 42 (42, 41, 43)
CP-809101 (0.5 µM) + complete S-9 105 (104, 106) 124 (126, 121)
CP-809101 (5.0 µM) + complete S-9 495 (490,501) 462 (472, 451)
- S-9, without metabolic activation; + incomplete S-9 (-NADPH); complete S-9 (+ NADPH) NADPH was used in test I and NADPH regenerating system was used in test II. a mean DPM represents average from two to three separate experiments.
NADPH-dependent covalent binding to DNA suggests P450-mediated bioactivation to DNA-reactive metabolite(s)
N
N
NHN
OCl
CP-809,101
* *
19
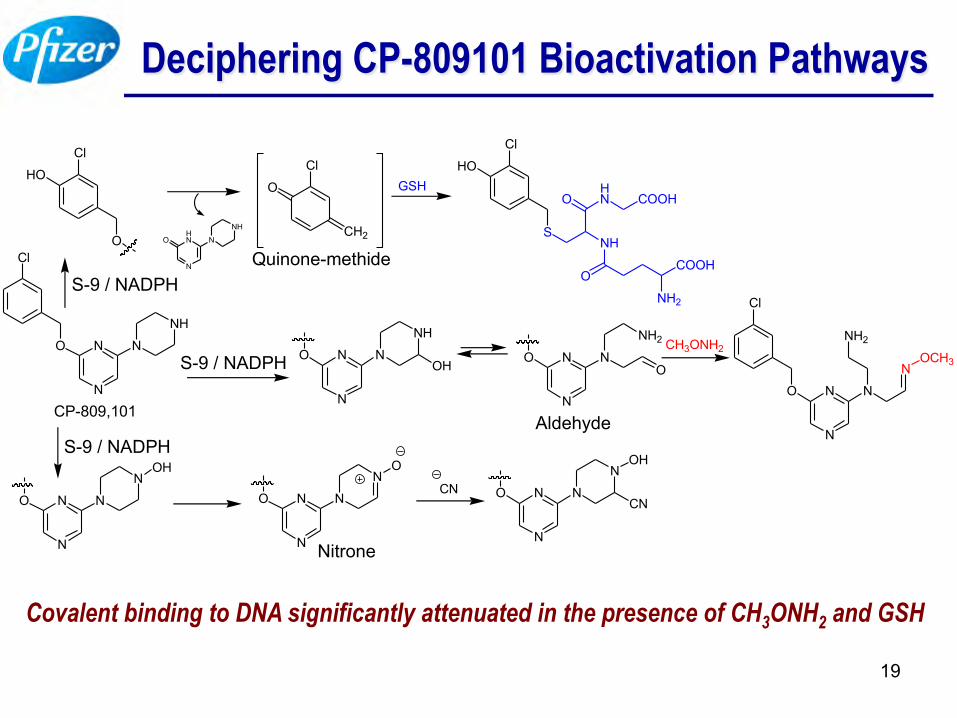
Deciphering CP-809101 Bioactivation Pathways
Covalent binding to DNA significantly attenuated in the presence of CH3ONH2 and GSH
Cl
O
N
N N
NH
CP-809,101
Cl
O
HOCl
CH2
O
Quinone-methideO
N
HN N
NH
S-9 / NADPH
GSH
Cl
S
HO
NH
OHN COOH
OCOOH
NH2
S-9 / NADPH O
N
N N
NH
OH O
N
N N
NH2
O
CH3ONH2
Cl
O
N
N N
NH2
NOCH3
S-9 / NADPH
O
N
N N
NOH
O
N
N N
NO
CN O
N
N N
NOH
CN
Aldehyde
Nitrone
20
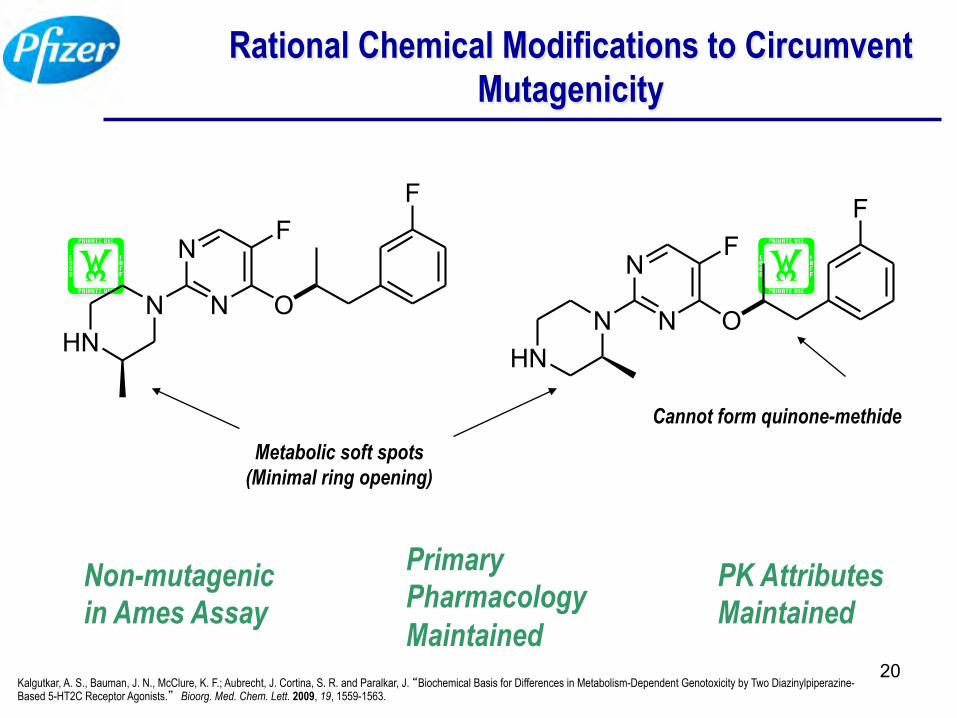
Metabolic soft spots (Minimal ring opening)
Cannot form quinone-methide
Non-mutagenic in Ames Assay
HN
N N
N
O
FF
HNN N
N
O
FF
Primary Pharmacology Maintained
PK Attributes Maintained
Rational Chemical Modifications to Circumvent Mutagenicity
Kalgutkar, A. S., Bauman, J. N., McClure, K. F.; Aubrecht, J. Cortina, S. R. and Paralkar, J. “Biochemical Basis for Differences in Metabolism-Dependent Genotoxicity by Two Diazinylpiperazine- Based 5-HT2C Receptor Agonists.” Bioorg. Med. Chem. Lett. 2009, 19, 1559-1563.
21
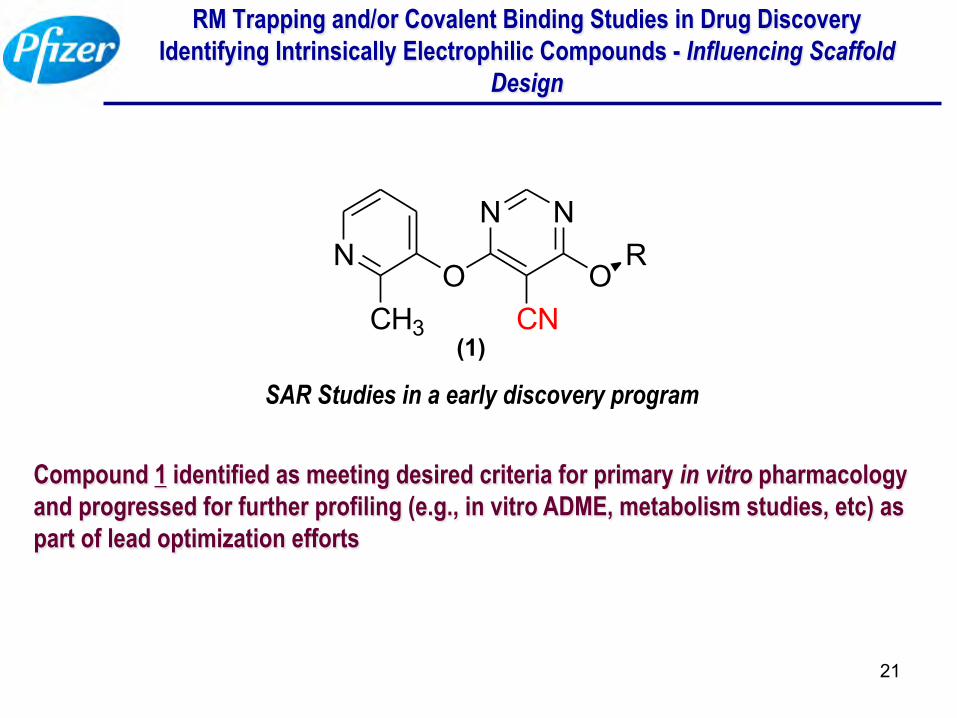
RM Trapping and/or Covalent Binding Studies in Drug Discovery Identifying Intrinsically Electrophilic Compounds - Influencing Scaffold
Design
SAR Studies in a early discovery program
Compound 1 identified as meeting desired criteria for primary in vitro pharmacology and progressed for further profiling (e.g., in vitro ADME, metabolism studies, etc) as part of lead optimization efforts
OR
NN
CNO
N
CH3(1)
22
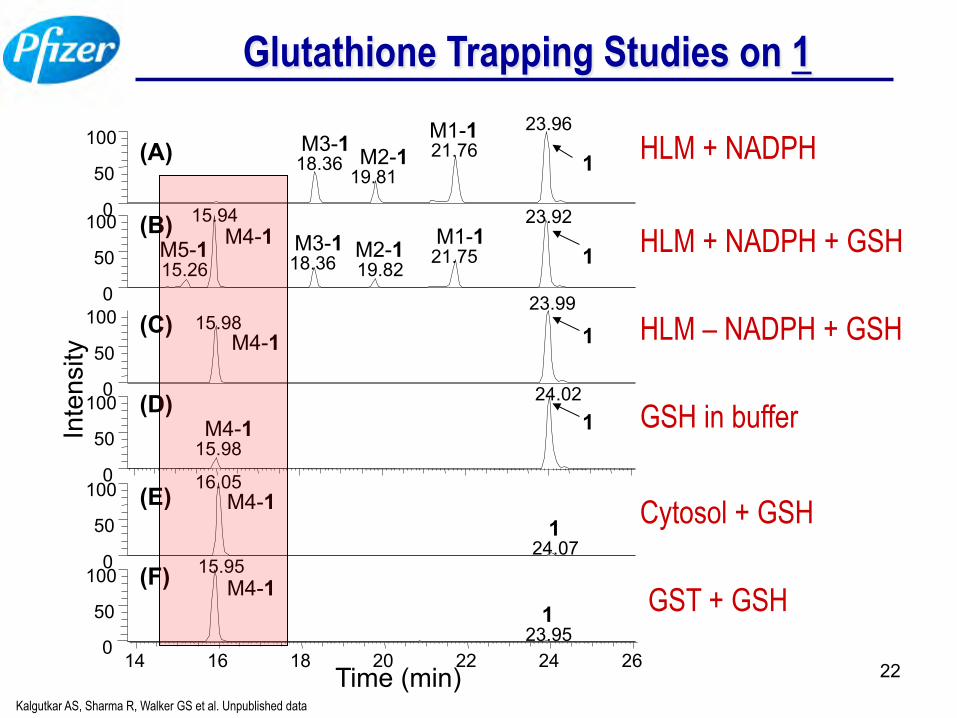
Glutathione Trapping Studies on 1
0
50
100 0
50
100
Inte
nsity
23.96 21.76
18.36 19.81
15.94 23.92
21.75 18.36 19.82 15.26
1 M1-1
M2-1 M3-1
M5-1 M4-1 1
0
50
100 23.99
15.98 M4-1 1
0
50
100
15.98 M4-1 1
24.02
0
50
100 16.05
24.07
M4-1 1
0
50
100
23.95
M4-1 1
15.95
Time (min) 14 16 18 20 22 24 26
(A)
(B)
(C)
(D)
(E)
(F)
M3-1 M2-1 M1-1
HLM + NADPH
HLM + NADPH + GSH
HLM – NADPH + GSH
GSH in buffer
Cytosol + GSH
GST + GSH
Kalgutkar AS, Sharma R, Walker GS et al. Unpublished data
23
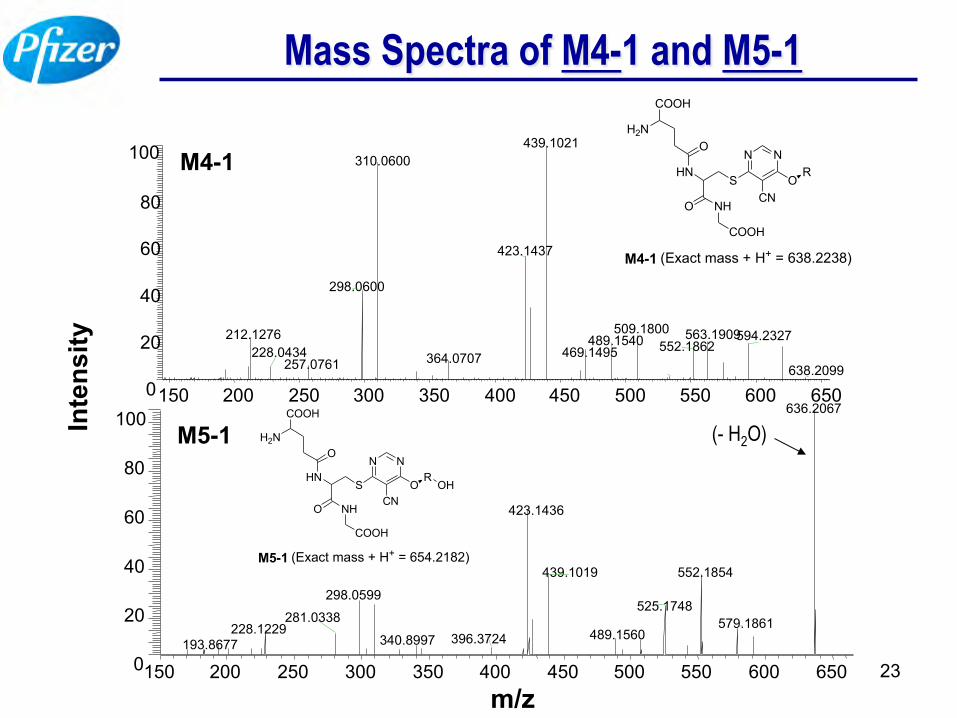
Mass Spectra of M4-1 and M5-1 In
tens
ity
m/z
150 200 250 300 350 400 450 500 550 600 650 0
20
40
60
80
100 439.1021 310.0600
423.1437
298.0600
509.1800 212.1276 563.1909 594.2327 552.1862 469.1495
489.1540 364.0707 257.0761
228.0434 638.2099
M4-1
150 200 250 300 350 400 450 500 550 600 650 0
20
40
60
80
100 636.2067
423.1436
552.1854 439.1019
298.0599 525.1748
579.1861 228.1229 281.0338
489.1560 193.8677 340.8997 396.3724
M5-1
N N
OCN
RS
HN
NHO
COOH
O
COOH
H2N
M4-1 (Exact mass + H+ = 638.2238)
N N
OCN
RS
HN
NHO
COOH
O
COOH
H2N
M5-1 (Exact mass + H+ = 654.2182)
OH
(- H2O)
24
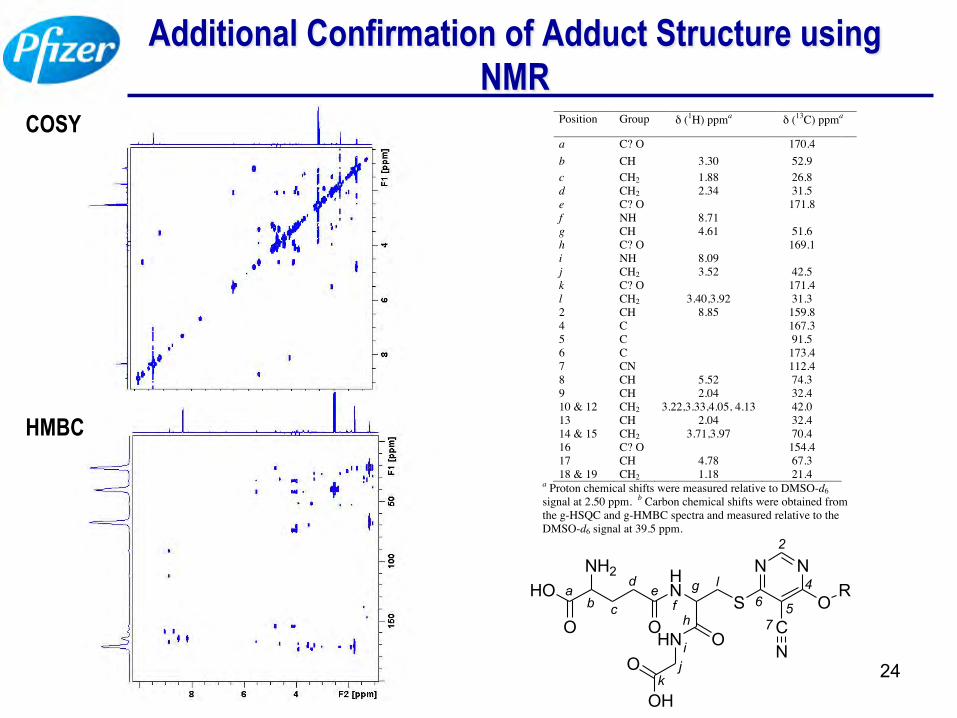
Additional Confirmation of Adduct Structure using NMR
COSY
HMBC
N N
CN
SHN
HN O
OH
O
O
NH2HO
OO
ad
fg
kji
h
ecb
l6 5
4
2
7
R
Position Group δ (1H) ppma δ (13C) ppma
a C? O 170.4 b CH 3.30 52.9 c CH2 1.88 26.8 d CH2 2.34 31.5 e C? O 171.8 f NH 8.71 g CH 4.61 51.6 h C? O 169.1 i NH 8.09 j CH2 3.52 42.5 k C? O 171.4 l CH2 3.40,3.92 31.3 2 CH 8.85 159.8 4 C 167.3 5 C 91.5 6 C 173.4 7 CN 112.4 8 CH 5.52 74.3 9 CH 2.04 32.4 10 & 12 CH2 3.22,3.33,4.05, 4.13 42.0 13 CH 2.04 32.4 14 & 15 CH2 3.71,3.97 70.4 16 C? O 154.4 17 CH 4.78 67.3 18 & 19 CH2 1.18 21.4
a Proton chemical shifts were measured relative to DMSO-d6 signal at 2.50 ppm. b Carbon chemical shifts were obtained from the g-HSQC and g-HMBC spectra and measured relative to the DMSO-d6 signal at 39.5 ppm.
25
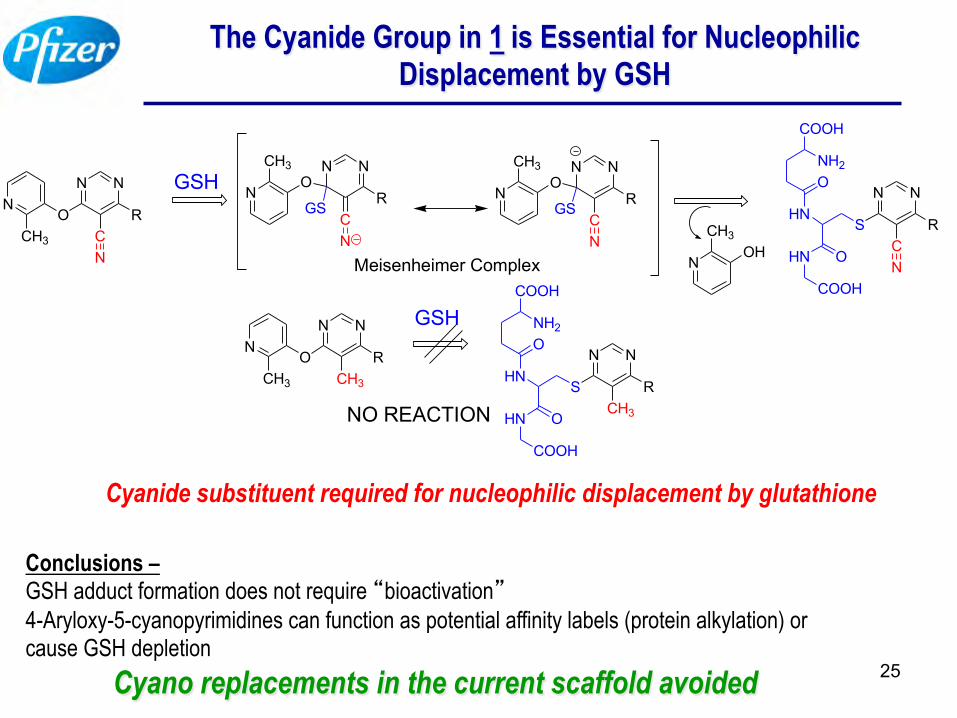
The Cyanide Group in 1 is Essential for Nucleophilic Displacement by GSH
Cyanide substituent required for nucleophilic displacement by glutathione
Conclusions – GSH adduct formation does not require “bioactivation” 4-Aryloxy-5-cyanopyrimidines can function as potential affinity labels (protein alkylation) or cause GSH depletion Cyano replacements in the current scaffold avoided
N N
RC
ON
CH3
GSHN N
RC
O
GS
N
N
CH3
Meisenheimer Complex
N N
RC
O
GS
N
N
CH3
N
N N
RC
S
N
HN
OHN
COOH
ONH2
COOH
OHN
CH3
N N
RCH3
ON
CH3
NO REACTION
N N
RCH3
SHN
OHN
COOH
ONH2
COOH
GSH
26
Eliminating Toxicity Risks in Drug Discovery Setting
• Structure-toxicity analyses teaches us that avoiding RM formation with drug candidates represents one potential solution to preventing drug toxicity
• Avoid chemical functionalities known to be susceptible to reactive metabolites – Tall order but avoids risk
27
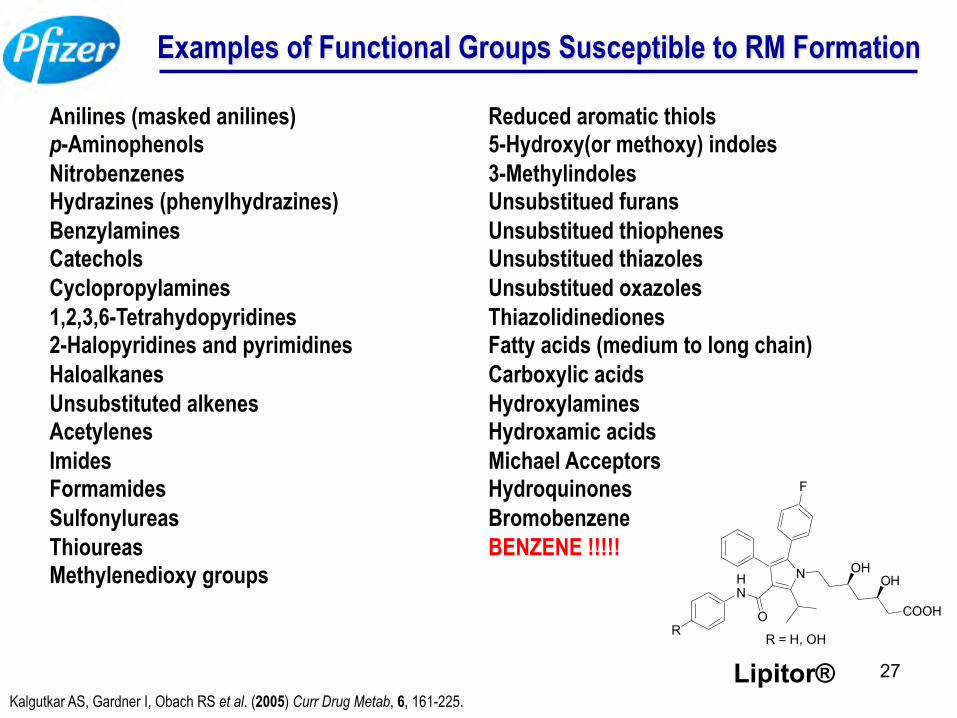
Examples of Functional Groups Susceptible to RM Formation
Anilines (masked anilines) p-Aminophenols Nitrobenzenes Hydrazines (phenylhydrazines) Benzylamines Catechols Cyclopropylamines 1,2,3,6-Tetrahydopyridines 2-Halopyridines and pyrimidines Haloalkanes Unsubstituted alkenes Acetylenes Imides Formamides Sulfonylureas Thioureas Methylenedioxy groups
Reduced aromatic thiols 5-Hydroxy(or methoxy) indoles 3-Methylindoles Unsubstitued furans Unsubstitued thiophenes Unsubstitued thiazoles Unsubstitued oxazoles Thiazolidinediones Fatty acids (medium to long chain) Carboxylic acids Hydroxylamines Hydroxamic acids Michael Acceptors Hydroquinones Bromobenzene BENZENE !!!!!
Kalgutkar AS, Gardner I, Obach RS et al. (2005) Curr Drug Metab, 6, 161-225.
N
F
HN
O
OHOH
COOHR
R = H, OH
Lipitor®
28
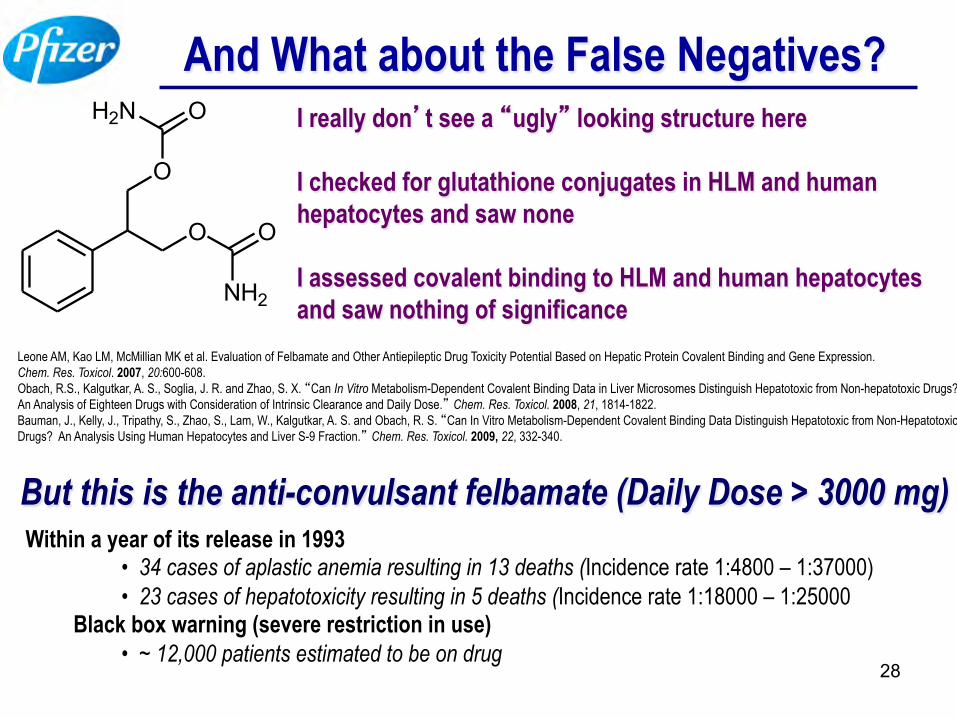
And What about the False Negatives?
O
OH2N
O O
NH2
I really don’t see a “ugly” looking structure here I checked for glutathione conjugates in HLM and human hepatocytes and saw none I assessed covalent binding to HLM and human hepatocytes and saw nothing of significance
Within a year of its release in 1993 • 34 cases of aplastic anemia resulting in 13 deaths (Incidence rate 1:4800 – 1:37000) • 23 cases of hepatotoxicity resulting in 5 deaths (Incidence rate 1:18000 – 1:25000
Black box warning (severe restriction in use) • ~ 12,000 patients estimated to be on drug
But this is the anti-convulsant felbamate (Daily Dose > 3000 mg)
Leone AM, Kao LM, McMillian MK et al. Evaluation of Felbamate and Other Antiepileptic Drug Toxicity Potential Based on Hepatic Protein Covalent Binding and Gene Expression. Chem. Res. Toxicol. 2007, 20:600-608. Obach, R.S., Kalgutkar, A. S., Soglia, J. R. and Zhao, S. X. “Can In Vitro Metabolism-Dependent Covalent Binding Data in Liver Microsomes Distinguish Hepatotoxic from Non-hepatotoxic Drugs? An Analysis of Eighteen Drugs with Consideration of Intrinsic Clearance and Daily Dose.” Chem. Res. Toxicol. 2008, 21, 1814-1822. Bauman, J., Kelly, J., Tripathy, S., Zhao, S., Lam, W., Kalgutkar, A. S. and Obach, R. S. “Can In Vitro Metabolism-Dependent Covalent Binding Data Distinguish Hepatotoxic from Non-Hepatotoxic Drugs? An Analysis Using Human Hepatocytes and Liver S-9 Fraction.” Chem. Res. Toxicol. 2009, 22, 332-340.
29
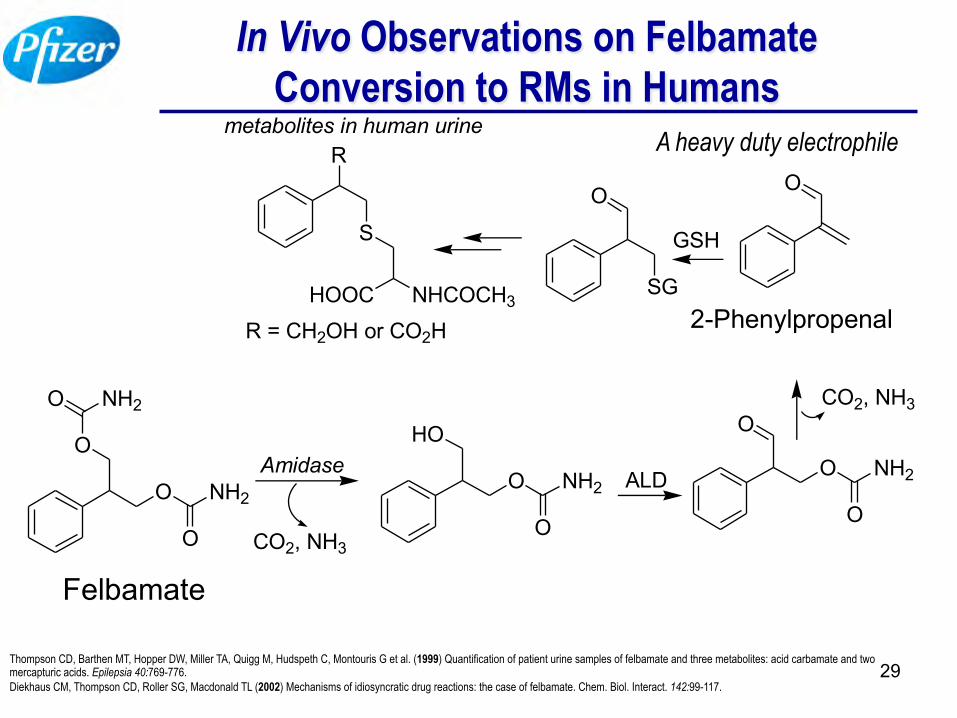
In Vivo Observations on Felbamate Conversion to RMs in Humans
O
O NH2
O
O NH2
Felbamate
CO2, NH3
HO
O NH2
O
O
O NH2
O
AmidaseALD
OO
SG
CO2, NH3
GSH
R
S
NHCOCH3HOOCR = CH2OH or CO2H
metabolites in human urine
2-Phenylpropenal
A heavy duty electrophile
Thompson CD, Barthen MT, Hopper DW, Miller TA, Quigg M, Hudspeth C, Montouris G et al. (1999) Quantification of patient urine samples of felbamate and three metabolites: acid carbamate and two mercapturic acids. Epilepsia 40:769-776. Diekhaus CM, Thompson CD, Roller SG, Macdonald TL (2002) Mechanisms of idiosyncratic drug reactions: the case of felbamate. Chem. Biol. Interact. 142:99-117.
30
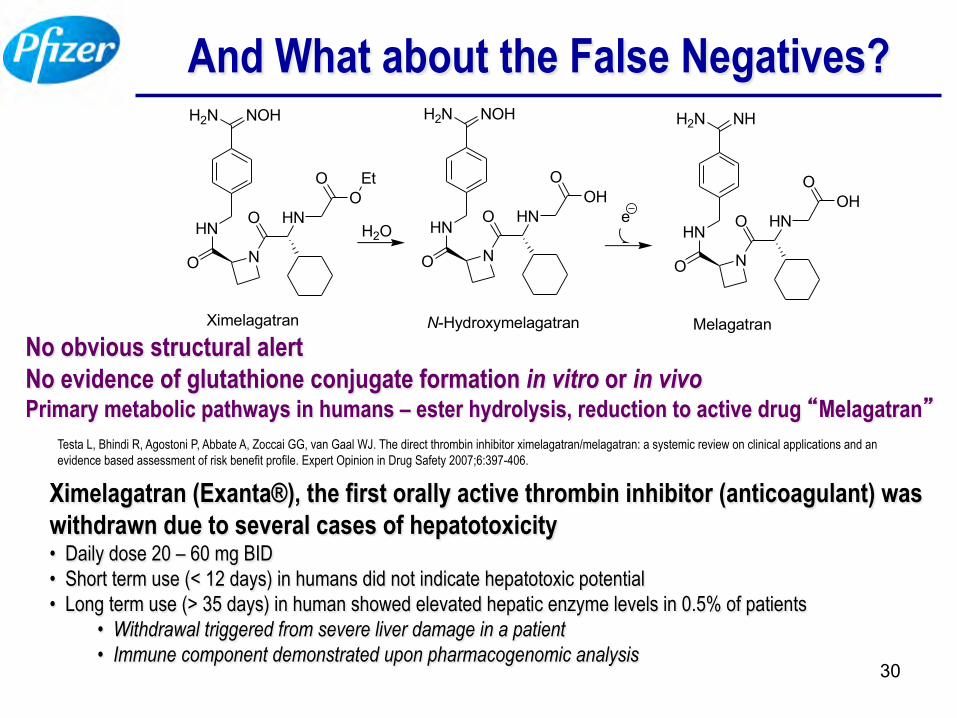
And What about the False Negatives? H2N NOH
HN
O N
O HNO
O Et
Ximelagatran
H2N NOH
HN
O N
O HNOH
O
N-Hydroxymelagatran
H2Oe
H2N NH
HN
O N
O HNOH
O
MelagatranNo obvious structural alert No evidence of glutathione conjugate formation in vitro or in vivo Primary metabolic pathways in humans – ester hydrolysis, reduction to active drug “Melagatran”
Ximelagatran (Exanta®), the first orally active thrombin inhibitor (anticoagulant) was withdrawn due to several cases of hepatotoxicity • Daily dose 20 – 60 mg BID • Short term use (< 12 days) in humans did not indicate hepatotoxic potential • Long term use (> 35 days) in human showed elevated hepatic enzyme levels in 0.5% of patients
• Withdrawal triggered from severe liver damage in a patient • Immune component demonstrated upon pharmacogenomic analysis
Testa L, Bhindi R, Agostoni P, Abbate A, Zoccai GG, van Gaal WJ. The direct thrombin inhibitor ximelagatran/melagatran: a systemic review on clinical applications and an evidence based assessment of risk benefit profile. Expert Opinion in Drug Safety 2007;6:397-406.
31
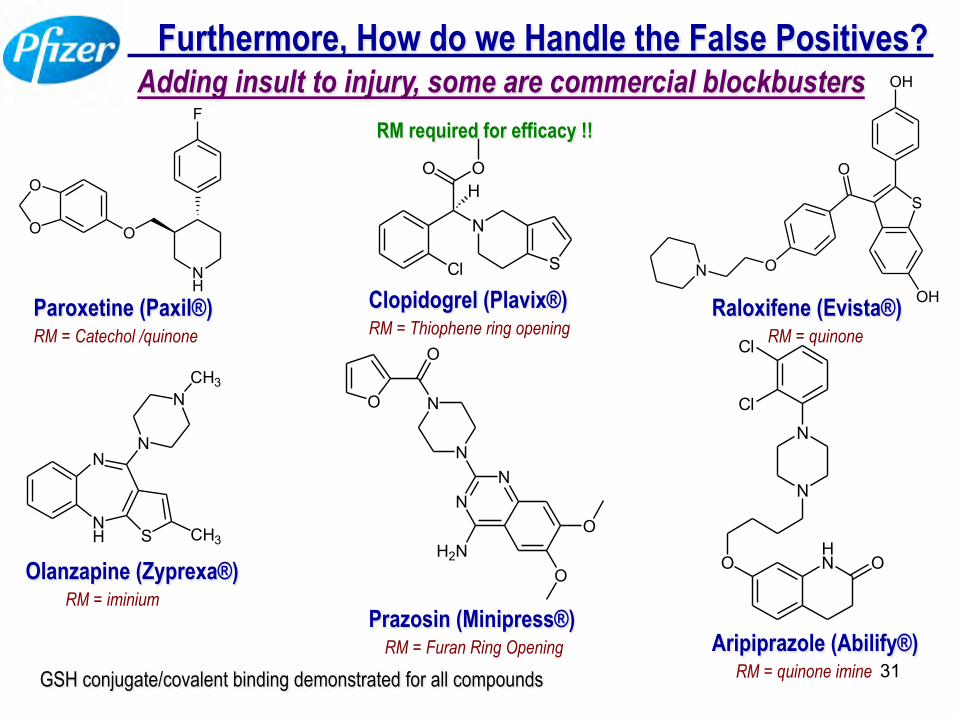
Furthermore, How do we Handle the False Positives?
Paroxetine (Paxil®)
NH
N
S CH3
N
NCH3
F
NH
O
O
O
Olanzapine (Zyprexa®)
OH
S
OH
O
ON
Raloxifene (Evista®)
O
O
N
N
NN
H2NO
O
Prazosin (Minipress®)
Cl
Cl
N
N
OHN O
Aripiprazole (Abilify®)
RM = Catechol /quinone
RM = Furan Ring Opening RM = quinone imine
RM = iminium
RM = quinone
Adding insult to injury, some are commercial blockbusters
Cl
N
O OH
S
Clopidogrel (Plavix®) RM = Thiophene ring opening
RM required for efficacy !!
GSH conjugate/covalent binding demonstrated for all compounds
32
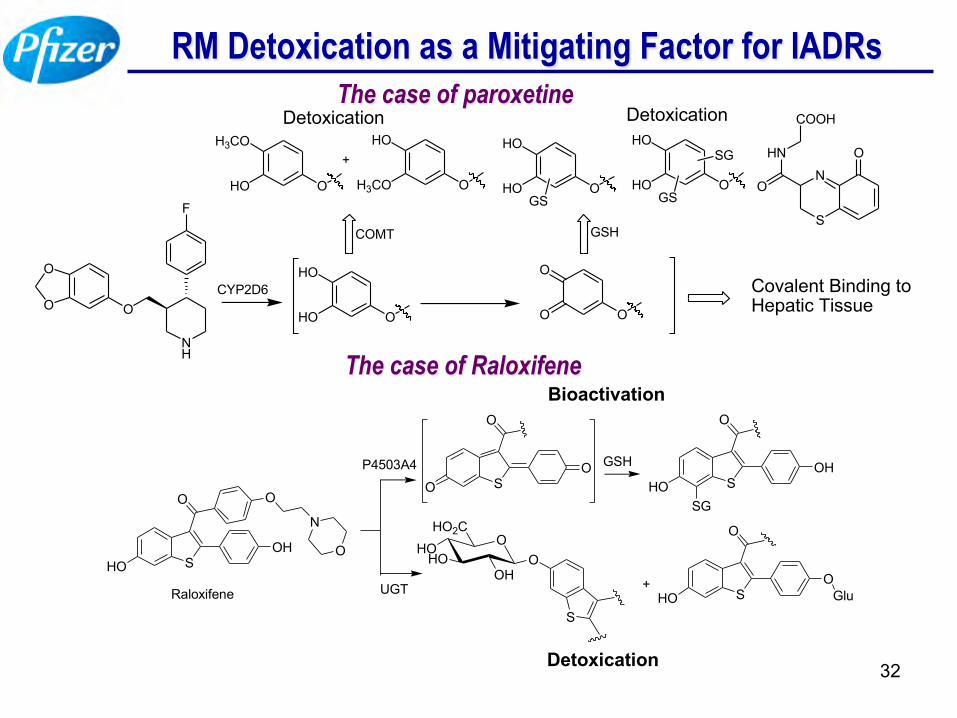
RM Detoxication as a Mitigating Factor for IADRs The case of paroxetine
O
O O
NH
F
CYP2D6
O
HO
HO O
O
O
O
H3CO
HO O
HO
H3CO
+
COMT
Detoxication
Covalent Binding to Hepatic Tissue
O
HO
HOGS
O
HO
HOGS
SG
GSH
N
S
O
O
HN
COOHDetoxication
The case of Raloxifene
SHO
O
OH
O
N
O
Raloxifene
P4503A4SO
O
O GSHSHO
O
OH
SG
HO OHO O
HO2C
OH
S
+UGT SHO
O
OGlu
Detoxication
Bioactivation
33
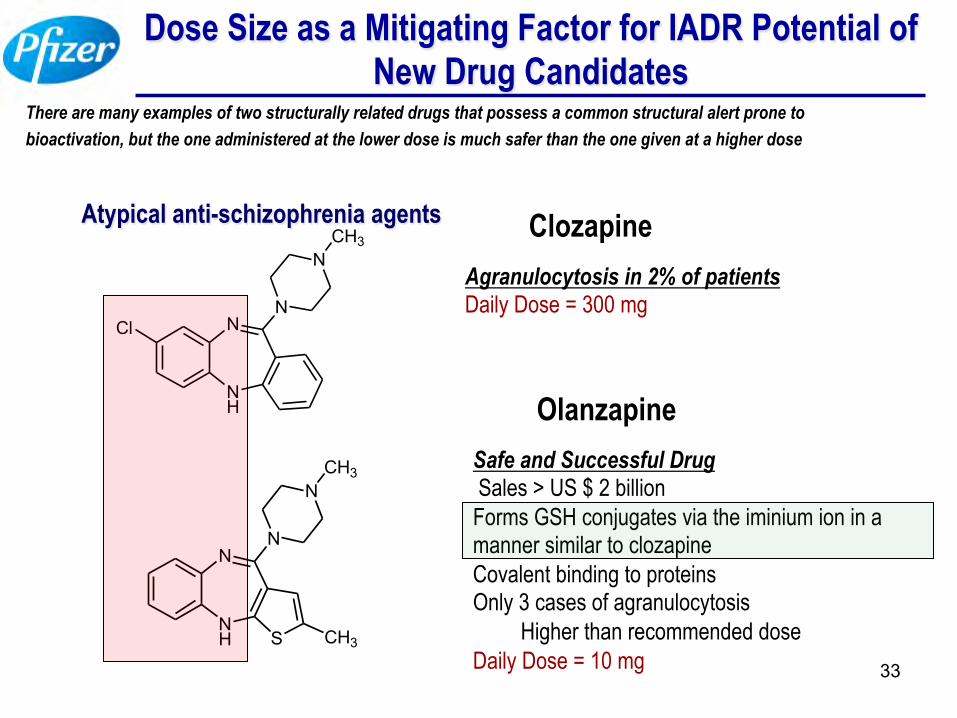
Dose Size as a Mitigating Factor for IADR Potential of New Drug Candidates
Atypical anti-schizophrenia agents
Agranulocytosis in 2% of patients Daily Dose = 300 mg
Safe and Successful Drug Sales > US $ 2 billion Forms GSH conjugates via the iminium ion in a manner similar to clozapine Covalent binding to proteins Only 3 cases of agranulocytosis
Higher than recommended dose Daily Dose = 10 mg
NH
NClN
NCH3
NH
N
S CH3
N
NCH3
Clozapine
Olanzapine
There are many examples of two structurally related drugs that possess a common structural alert prone to bioactivation, but the one administered at the lower dose is much safer than the one given at a higher dose
34
Bioactivation Data Needs to be Placed in Proper Context — Risk/Benefit Assessments (Qualifying Considerations)
• Nature of the medical need – Life-threatening disease / unmet medical need – First in class
• Target population – Underlying disease state (immune-compromised patients)
• Is the drug candidate intended to provide proof of a novel mechanism?
• What % of clearance mechanism involves bioactivation – Existence of detoxication pathways; renal excretion, etc
• What is the daily dose of the drug? – IADRs are rare for drugs dosed below 20 mg QD
35
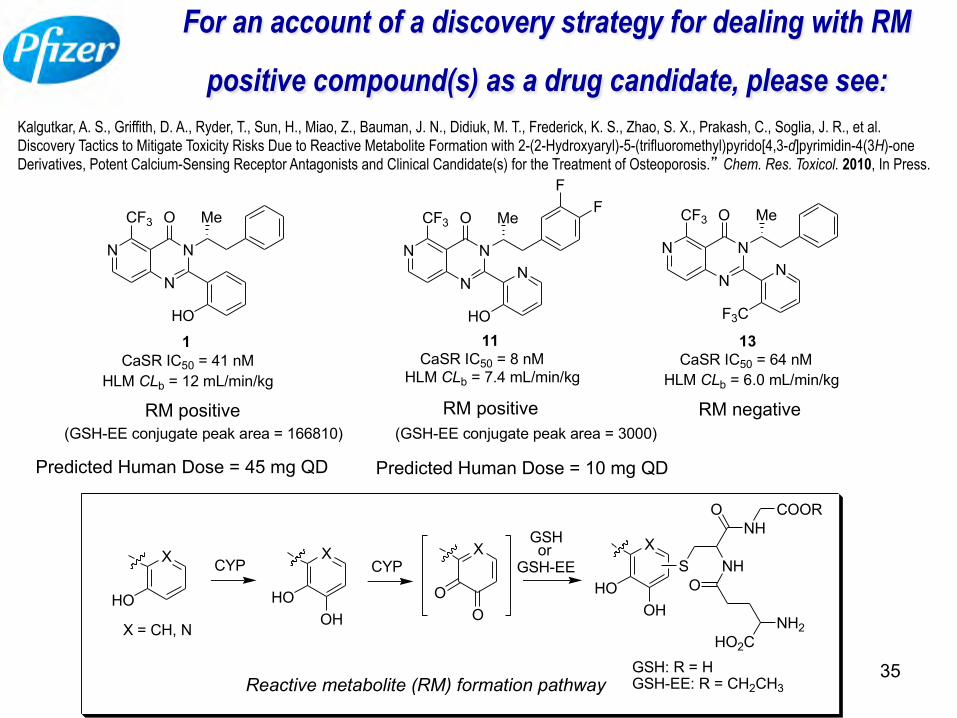
For an account of a discovery strategy for dealing with RM
positive compound(s) as a drug candidate, please see: Kalgutkar, A. S., Griffith, D. A., Ryder, T., Sun, H., Miao, Z., Bauman, J. N., Didiuk, M. T., Frederick, K. S., Zhao, S. X., Prakash, C., Soglia, J. R., et al. Discovery Tactics to Mitigate Toxicity Risks Due to Reactive Metabolite Formation with 2-(2-Hydroxyaryl)-5-(trifluoromethyl)pyrido[4,3-d]pyrimidin-4(3H)-one Derivatives, Potent Calcium-Sensing Receptor Antagonists and Clinical Candidate(s) for the Treatment of Osteoporosis.” Chem. Res. Toxicol. 2010, In Press.
N
N
N
CF3 O
HO
Me
1
RM negative
CaSR IC50 = 41 nM
N
N
N
CF3 O
N
HO
Me
11CaSR IC50 = 8 nM
FF
N
N
N
CF3 O
N
F3C
Me
13CaSR IC50 = 64 nM
HLM CLb = 12 mL/min/kg HLM CLb = 7.4 mL/min/kg HLM CLb = 6.0 mL/min/kg
X
HO
X = CH, N
CYPX
HOOH
CYPX
OO
GSHor
GSH-EEX
HOOH
S NH
ONH
COOR
O
NH2HO2C
GSH: R = HGSH-EE: R = CH2CH3Reactive metabolite (RM) formation pathway
RM positive RM positive
Predicted Human Dose = 45 mg QD Predicted Human Dose = 10 mg QD
(GSH-EE conjugate peak area = 166810) (GSH-EE conjugate peak area = 3000)





























