Embed Size (px)
Citation preview

RESEARCH Open Access
Metabolomic change due to combinedtreatment with myo-inositol, D-chiro-inositol and glucomannan in polycysticovarian syndrome patients: a pilot studyJacopo Troisi1,2,3*† , Claudia Cinque1†, Luigi Giugliano1, Steven Symes4,5, Sean Richards5,6, David Adair5,Pierpaolo Cavallo7,11, Laura Sarno8, Giovanni Scala2,9, Maria Caiazza10 and Maurizio Guida1,2
Abstract
Background: Polycystic ovarian syndrome (PCOS) is a highly variable syndrome and one of the most commonfemale endocrine disorders. Although the association inositols-glucomannan may represent a good therapeuticstrategy in the treatment of PCOS women with insulin resistance, the effect of inositols on the metabolomic profileof these women has not been described yet.
Results: Fifteen PCOS-patients and 15 controls were enrolled. Patients were treated with myo-inositol (1.75 g/day),D-chiro-inositol (0.25 g/day) and glucomannan (4 g/day) for 3 months. Blood concentrations of glucose, insulin,triglycerides and cholesterol, and ovary volumes and antral follicles count, as well as metabolomic profiles, wereevaluated for control subjects and for cases before and after treatment.PCOS-patients had higher BMI compared with Controls, BMI decreased significantly after 3 months of treatmentalthough it remained significantly higher compared to controls. 3-methyl-1-hydroxybutyl-thiamine-diphosphate,valine, phenylalanine, ketoisocapric, linoleic, lactic, glyceric, citric and palmitic acid, glucose, glutamine, creatinine,arginine, choline and tocopherol emerged as the most relevant metabolites for distinguishing cases from controls.
Conclusion: Our pilot study has identified a complex network of serum molecules that appear to be correlatedwith PCOS, and with a combined treatment with inositols and glucomannan.
Trial registration: ClinicalTial.gov, NCT03608813. Registered 1st August 2018 - Retrospectively registered, .
Keywords: Polycystic ovary syndrome, Inositols-glucomannan association, Metabolomics
BackgroundPolycystic ovary syndrome (PCOS) is a heterogeneoussyndrome and one of the most common femaleendocrine disorders, affecting 5–20% of women inreproductive age [1, 2]. Clinical expression is highlyvariable, but typically includes oligo-ovulation or anovu-lation, hyperandrogenism and polycystic ovaries [3].PCOS is associated with an increased risk of type 2 dia-betes, cardiovascular events [4] and endometrial cancer
[5]. Insulin Resistance (IR) plays a central role inapproximately 70–80% of obese women and in 15–30%of lean women with PCOS [3], and represents the patho-genic link between metabolic and reproductive disordersin PCOS [6].The last decade has seen the introduction of inositols
for the treatment of PCOS and a recent review suggeststhat inositol therapy can reduce insulin resistance,improve ovarian function, and reduce androgen levels inwomen with PCOS [7]. The two inositol isomers ofinterest are myo-inositol (MI) and D-chiro-inositol(DCI) which often have a physiological ratio of 40:1 inmost healthy tissues [8]. Importantly, the MI:DCI ratiodoes vary between healthy and disease state [9–11] thus
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected]†Both authors contributed equally to this work.1Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana”,University of Salerno, Baronissi, SA, Italy2Theoreo srl, Via degli Ulivi 3, 84090 Montecorvino Pugliano, SA, ItalyFull list of author information is available at the end of the article
Troisi et al. Journal of Ovarian Research (2019) 12:25 https://doi.org/10.1186/s13048-019-0500-x

strengthening the hypothesis that inositol therapy maybe beneficial for maintaining metabolic, endocrine, andreproductive health in women with PCOS.Glucomannan is a water-soluble fiber that is derived
from the konjac root [12]. It has been reported as beingable to suppress hepatic cholesterol synthesis andincrease the elimination of cholesterol-containing bileacids [13]. Some authors have suggested that glucoman-nan ingestion could also increase the gastric emptyingtime [14–16]. This effect may be related to the increasedfeeling of satiety reported in some studies [17]. The Euro-pean Food and Safety Authority (EFSA) in 2010 reporteda scientific opinion supporting the anti-cholesterol andweight reduction claims for glucomannan-containingdrugs [18].The association inositols-glucomannan may represent a
good therapeutic strategy in the treatment of PCOS womenwith insulin resistance [19].The use of metabolomics for the study of disease mecha-
nisms is increasing. Metabolites are low-molecular-weightorganic and inorganic chemicals that are the substrates, in-termediates, and byproducts of enzyme-mediated biochem-ical reactions in the cell [20]. Several thousand metabolitesin human serum have been identified so far, and the applica-tion of metabolomics has allowed the development of bio-markers which provides new insight for many diseases [21].Metabolomic analysis in gynecology has been extended
to studies of various malignancies, such as ovariancancer [22] and endometrial cancer [23, 24]. Moreover,many studies have incorporated a metabolomic approachto better define the pathophysiology of PCOS [25–31]and to describe how different therapies can modifymetabolic profiles [32–34].However, the effect of inositols on the metabolomic
profile of women with a diagnosis of PCOS has not beendescribed yet. Thus, the aim of this study is to analyzethe metabolic profiles in women with PCOS before andafter 3 months of therapy with a combination of MI,DCI and glucomannan, and compare these data with agroup of healthy control women.
ResultsBased on serum metabolomic signatures of PCOS pa-tients and controls a statistical power of 80% resultedfrom the analysis of at least 15 subjects for each class(See Additional file 1: Figure S1). The demographic andclinical–biochemical characteristics of PCOS patients atbaseline (PCOS-T0) and after 3 treatment months(PCOS-T1) and controls (CTRL) are reported in Table 1.All PCOS patients met both the Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop GroupCriteria [4] and the adolescent criteria [35] for thediagnosis of PCOS. All subjects in this study were un-married, not interested in soon becoming pregnant, and
were not currently taking hormonal contraceptives.None of them had previously given birth or hadundergone voluntary interruption of pregnancy. Noneof the controls displayed any biochemical orgynecological abnormalities. Women with PCOS hadhigher Body Mass Index (BMI) compared with Con-trols (mean ± standard deviation, 28.4 ± 1.7 vs. 21.6 ±1.6 [kg/m2], p < 0.05) and BMI decreased significantly(p < 0.05) after 3 months of treatment even if itremained significantly higher compared to controls(26.4 ± 1.7 vs. 21.6 ± 1.6 [kg/m2], p < 0.05). Averageblood Glucose, Insulin and Homeostatic Model As-sessment for Insulin Resistance (HOMA-IR) valueswere not significantly different, although the meanvalues for each parameter were greater in PCOS sam-ples. These values did not significantly change after 3months of treatment. Menstrual cycle regularity im-proved significantly after treatment. The number of antralfollicles and the ovary volume were higher in PCOS pa-tients (6.8 ± 1.2 vs. 15.4 ± 1.7, p < 0.05 and 7.4 ± 0.7 vs. 12.2± 2.2 [mL], p < 0.05, respectively) but both decreased aftertreatment (13.2 ± 2.3 and 10.2 ± 1.9 [mL], p < 0.05, respect-ively). The same trend was observed for theFerriman-Galleway and the acne score (see Table 1).As shown in Fig. 1a, the partial least square-discrimin-
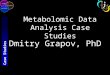
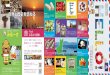
ant analysis (PLS-DA) score plots clearly differentiatedthree groups consisting of controls, PCOS patients be-fore treatment, and PCOS patients after treatment. The15 highest scoring VIP variables (VIP score > 1.5) identi-fied by PLS-DA are shown in Fig. 1b. The metaboliteconcentration changes induced by the therapy alloweddivision of the metabolites into three classes: those withhigher concentrations than the controls and which in-creased further after therapy, those which have higherconcentrations than the controls and whose concentra-tion decreased after therapy and, those with lower con-centrations compared to controls that did not changeafter therapy.As shown in Fig. 2, the concentrations of
3-methyl-1-hydroxybutyl-thiamine diphosphate (FC =6.94, p < 0.001), valine (FC = 4.87, p = 0.001) and phenyl-alanine (FC = 10.91, p < 0.001) were higher in PCOS-T0patients compared to the control and increased even fur-ther after the treatments (FC = 1.13, p = 0.001; FC = 1.71,p = 0.002; FC = 1.17, p < 0.001, comparing PCOS-T1 toPCOS-T0, respectively).Ketoisocapric acid (FC = 3.12, p < 0.001), linoleic acid
(FC = 14.76, p < 0.001), lactic acid (FC = 5.31, p < 0.001),palmitic acid (FC = 6.22, p < 0.001) and glucose (FC =19.92, p < 0.001), were also higher in PCOS patients atenrollment time but they decreased after treatments(FC = 0.93, p < 0.001; FC = 0.90, p < 0.001; FC = 0.93,p < 0.001; FC = 0.93, p < 0.001; FC = 0.89, p = 0.001,respectively).
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 2 of 11

Glutamine (FC = 0.41, p > 0.05), glyceric acid (FC =0.85, p > 0.05), creatinine (FC = 0.71, p > 0.05), arginine(FC = 0.50, p > 0.05), citric acid (FC = 0.45, p > 0.05),choline (FC = 0.55, p > 0.05) and tocopherol (FC = 0.59,p > 0.05) were all lower in PCOS patients and had verylow concentrations after treatment although thesevalues were not significantly different.The metabolic pathway analysis of the selected
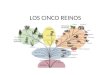
metabolites is summarized in the metabolic systemsmap shown in Fig. 3. There is a definite interactionof several pathways involving Biopterin metabolism;De novo fatty acid biosynthesis; Di-unsaturatedfatty acid beta-oxidation; Glycerophospholipid me-tabolism; Glycine, serine, alanine and threoninemetabolism; Linoleate metabolism; Saturated fattyacids beta-oxidation; TCA cycle; Tyrosine metabol-ism; Urea cycle and metabolism of arginine, proline,
glutamate, aspartate and asparagine; Valine, leucineand isoleucine degradation; Vitamin B3 (nicotinateand nicotinamide) metabolism; Vitamin E metabolism.
DiscussionThis is a prospective case-control study conducted in asingle center at University Hospital “San Giovanni diDio e Ruggi D’Aragona” of Salerno.The studied population included only young/adoles-
cent women. We have chosen to investigate this specificage group, since younger women may benefit the mostfrom an early treatment in terms of future pregnancychances and possibly avoiding comorbidities develop-ment [36]. Furthermore, the PCOS-inositols treatmentsdo not contraindicate other concomitant therapeuticoptions [7].
Table 1 Anamnestic and anthropometric characteristics of controls and cases at enrollment (PCOS-T0) and after 3-monthstreatment (PCOS-T1)
Control (n = 15) PCOS-T0 (n = 15) PCOS -T1 (n = 15) Reference values
Age (years) 21.9 ± 2.9 19.7 ± 1.9 –
Height (cm) 158.0 ± 6.4 159.2 ± 7.2 –
Weight (Kg) 53.9 ± 6.0 71.9 ± 6.7* 67.0 ± 7.3* –
BMI (Kg/m2) 21.6 ± 1.6 28.4 ± 1.7* 26.4 ± 1.7*,§ < 18.5 Underweight18.5–25.0 Normal weight25.1–29.9 Overweight> 30 Obese
Menstrual flux
Normal 12 (80%) 5 (33%) 9 (60%) < 20 mL
hypo- 2 (13%) 9 (60%) 5 (33%) 20–80 mL
hyper- 1 (7%) 1 (7%) 1 (10%) > 80 mL
Blood Glucose (mg/dL) 79.3 ± 6.9 83.9 ± 7.5 88.0 ± 8.5* 70–110
Insulin (μU/mL) 6.2 ± 1.2 8.0 ± 3.1 7.9 ± 3.8 2–25
HOMA-IR index 1.30 ± 0.22 1.68 ± 0.64 1.76 ± 0.99 0.2–2.2
Total Cholesterol (mg/dL) 150.7 ± 17.3 169.7 ± 34.9 152.1 ± 21.5 < 200
Triglycerides (mg/dL) 67.0 ± 17.1 77.6 ± 26.0 62.5 ± 12.3 < 150
Total Testosterone (ng/dL) 32.7 ± 9.88 42.7 ± 9.91* 34.98 ± 8.11 21–49
Free Testosterone (pg/mL) 2.49 ± 0.81 2.50 ± 0.98 2.48 ± 1.06 < 3.0
Menstrual cycle regularity
Yes 15 (100%) 0 (0%)* 4 (27%)* Regularity: loss between 20–80mL;cycle lasting 25–36 days
No 0 (0%) 15 (100%)* 11 (73%)*
Number of menstrual cycles in previous 3 months 3.0 ± 0.0 1.6 ± 0.5* 2.0 ± 0.7*
Number of antral follicles 6.8 ± 1.2 15.4 ± 1.7* 13.2 ± 2.3*,§ < 12
Acne score 1.4 ± 0.5 2.1 ± 1.2 1.8 ± 1.1 –
Ovary volumes (mL) 7.4 ± 0.7 12.2 ± 2.2* 10.2 ± 1.9*,§ < 10
Ferriman-Gallwey score 5.1 ± 2.1 15.5 ± 5.0* 15.0 ± 4.9* < 8
Patient characteristics are reported as mean ± standard deviation or number (percentage). * p-value < 0.05 PCOS-T0 or PCOS-T1 vs Control, §p-value < 0.05PCOS-T1vs PCOS-T0
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 3 of 11

The aim of this study was, firstly, to identify discrimin-ant metabolites in serum of women with a diagnosis ofPCOS and, secondly, to define if treatment with inositolscan improve metabolomic pathways and metabolicprofiles of women with PCOS. Multi-variate statistical
analysis identified fifteen metabolites as being particu-larly important in separating cases from controls:3-methyl-1-hydroxybutyl-thiamine diphosphate, valine,phenylalanine, ketoisocapric acid, linoleic acid, lacticacid, palmitic acid and glucose were increased in PCOS
Fig. 1 a Partial least square discriminant analysis (PLS-DA) models to discriminate Controls (CTRL, yellow circles), PCOS patients at enrolment(PCOS-T0, green circles) and PCOS patients after 3-months treatment (PCOS-T1, purple circles). The explained variance of each component isshown in parentheses on the corresponding axis. b The 15 top-scoring VIP metabolites (VIP-score≥ 1.5) are shown. The colored boxes on theright indicate the relative amount of the corresponding metabolite in each group under study
Fig. 2 Box and Whisker plot of the VIP metabolites in the cohort of patients and controls. Boxes represent controls (CTRL) n = 15; PCOS patientsat the basal enrolment time (PCOS-T0), n = 15; and PCOS patients after 3-months treatment (PCOS-T1), n = 15). The vertical axis reports the log ofthe GC-MS value of the normalized area of each metabolite. Abbreviations: Gas Chromatography-Mass Spectrometry (GC-MS), Polycystic OvarySyndrome (PCOS), Thiamine Phosphate (ThPP)
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 4 of 11

patients compared to controls, while glutamine, glycericacid, creatinine, arginine, citric acid, choline and tocoph-erol were decreased.According to these results, different metabolic
pathways appear to be involved in PCOS pathology. Inthe serum of PCOS patients at enrollment time in com-parison with control group, several metabolites, closelyassociated with carbohydrate and lipid metabolisms, aresignificantly dysregulated.Increased levels of lactic acid have been previously
reported in PCOS patients [27, 37] and can be related toan increased muscular gluconeogenesis or can indicatean uptake and consumption of glucose by muscles, sug-gesting an important role for insulin resistance in thesepatients [25].As previously reported [27], linoleic acid and palmitic
acid are also increased, likely the result of increasedlipolysis that might be related to presence of insulinresistance in fatty tissue [25]. PCOS is associated withincreased lipolysis due to presence of IR in adiposetissue [38]. However, IR does not occur in all tissues ofall women with PCOS, and different mechanisms maycontribute to hyperinsulinemia [39].Moreover, high abundances of linoleic acid appear to
inhibit the maturation and development of oocytes [40].Due to proinflammatory activity, elevated linoleic acidlevels can lead to the chronic inflammation associatedwith PCOS [41, 42].Several amino acids and other metabolites associ-
ated with the tricarboxylic acid cycle (TCA) arealtered in PCOS patients: the levels of arginine, cho-line, glutamine and citric acid were decreased and
those of phenylalanine and valine were increased,compared to the controls. Such alterations to theTCA cycle are also related to insulin resistance [43]and alterations in oocyte maturation [44].Valine was increased in PCOS patients as previously
reported [29] and it might be associated with othermetabolic alterations not related with insulin resistance[25]. As with the present study, creatinine has beenreported to be reduced in PCOS patients [37].Nevertheless, our specific cohort showed a low
incidence of insulin resistance, according to previousreported data on adolescent population [35, 45], there-fore the proposed theories/explanation may not fullyapply to the cohort of patients evaluated in this study.We found a reduction of tocopherol in PCOS patients,
consistent with previous work [39]. This metabolite hasan anti-oxidant effect and the reduction in concentrationmight be explained by the increased oxidative stressobserved in PCOS.According to recent guidelines, insulin-sensitizer drugs
are the first-line therapy in women with metabolic ab-normalities and irregular menstrual cycle with the pur-pose to improve fertility, whereas a lifestyle change withweight loss and physical activity is the first step in over-weight and obese PCOS patients [46]. Inositols belongto a sugar alcohol family comprising nine stereoisomersand two of them, MI and DCI, are involved in the patho-physiology and treatment of PCOS [47]. Inositols workas second messengers of insulin: MI improves oocytequality mediating glucose uptake and follicle stimulatinghormone (FSH) signaling, while the supplementation ofDCI, is involved in insulin-mediated androgen synthesis,
Fig. 3 Metabolic systems map summarizing the shortest route that may explain the interactions among the 15 selected metabolites. There is aclear interplay of several pathways involving: Biopterin metabolism; De novo fatty acid biosynthesis; Di-unsaturated fatty acid beta-oxidation;Glycerophospholipid metabolism; Glycine, serine, alanine and threonine metabolism; Linoleate metabolism; Saturated fatty acids beta-oxidation;TCA cycle; Tyrosine metabolism; Urea cycle and metabolism of arginine, proline, glutamate, aspartate and asparagine; Valine, leucine andisoleucine degradation; Vitamin B3 (nicotinate and nicotinamide) metabolism; Vitamin E metabolism
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 5 of 11

replenishing stores of the mediator and improving insu-lin sensitivity [7, 47, 48]. A recent review has shown theefficacy of inositols treatment in the management ofPCOS [49], while an Italian study [19] has shown thesynergistic action of inositols-glucomannan in thetreatment of PCOS women with insulin resistance (IR).So, we can suggest a central but not peripheral role ofIR in the present cohort. In another study, aftercombined treatment with inositols-glucomannan, PCOSpatient showed decreased levels of free fatty acids, andpatients experienced weight reduction [50]. In addition,the reduction of linoleic acid was also reported after 30months of polytherapy with pioglitazone-flutamide-met-formin and hormonal medication in an adolescent pa-tient group with PCOS [32]. Moreover, a recent study[33] has shown how, in metabolic terms,3-iodothyronamine administration in a mouse modelof PCOS may serve as a promising endogenous sup-plement in the treatment of dysfunctional lipidmetabolism.It would be reasonable to expect a trend towards
normalization of the metabolome upon weight reductionand clinical improvement due to the treatment. Indeed,after 3 months of treatment with a combination of MI,DCI and glucomannan, the clinical symptoms didimprove. However, the metabolic profiles of patientsafter 3 months of treatment were less close to those ofcontrols compared to initial metabolomes. Indeed, me-tabolites with lower abundances in PCOS-T0 patients ei-ther stayed the same or decreased even more aftertreatment, while those metabolites with higher abun-dances generally increased after treatment. We offer twopotential explanations for these observations: 1) themetabolome is more strongly affected by therapeuticallyinduced rapid weight loss (approximately 400 g/week) inoverweight patients compared to PCOS condition; 2) themetabolome of patients with PCOS may adapt to thiscondition, thus rendering the differences between con-trols and not-treated patients less prominent. This effectwas observed in anorexic women treated with a foodtherapy [51]. Similarly, it can be argued that the stronglyaltered metabolome of weight loss patients wouldnormalize if the achieved body weight is maintained. Ingeneral terms, we conclude that metabolic processes areseemingly susceptible to changes generated by beingoverweight and even more so by subsequent weight loss.The modest improvement in menstrual cycle regularityfollowing treatment (Table 1) is statistically consistentwith that reported by Pundir’s meta-analysis [52]. Thiscan be related to the lower incidence of IR in our cohort;indeed a large amount of evidence indicates that lower-ing insulin levels with insulin-sensitizing drugs inIR-PCOS women can reduce circulating androgen levels,increase SHBG levels, and restore ovulatory menstrual
cycles [53]. Moreover, although only 27% of thepost-treatment subjects reported menstrual cycle charac-teristics consistent with a “regular” definition (i.e., acycle lasting between 25 and 36 days and menstrualblood loss between 20 and 80mL), all the patientsreported some kind of improvement in menstrual cycleregularity.Our study has a few limitations. The first is the lack of
a metabolomic comparison among PCOS patientsundergoing inositols-only treatment. As a result, wecannot address which changes were due to the com-bined treatment and which ones were due to inositols. Afurther limitation is the small number of patientsenrolled, although acceptable statistical power [54] isstill achieved. Our PCOS patients did not show higherfree and total testosterone levels compared with refer-ence values of the Italian population. However, manyfactors are considered for diagnosis of hyperandrogen-ism. The Androgen Excess Society criteria for diagnosisof PCOS requires clinical or biochemical evidence ofhyperandrogenism [55].Clinical diagnosis of hyperandrogenism is identified by
hirsutism (as scored by the Ferriman-Gallwey exam), acne,and alopecia [56]. Biochemical diagnosis of hyperandro-genism includes measuring serum total testosterone, freetestosterone, free androgen index, androstenedione, anddehydroepiandrosterone sulfate [57]. Amirie et al. [58],conducted a meta-analysis of 6593 PCOS patients andconfirmed that the Ferriman-Gallwey clinical diagnosticcriteria significantly correlates with biochemical diagnosticcriteria. Concentrations of androstenedione anddehydroepiandrosterone sulfate correlated with theFerriman-Gallwey diagnosis of PCOS; while, as with ourstudy, a significant correlation was not found withtestosterone and free testosterone [58]. Indeed, the mostcommonly quantified biochemical parameters of hyperan-drogenism are free testosterone and free androgen index;however, the increased levels of androstenedione or otherandrogen precursors are, for many patients, the onlyindicators of hyperandrogenism [55, 58, 59]. Thus, the factthat free testosterone and total testosterone was nothigher in our PCOS cases does not indicate the patientdid not have PCOS. Therefore, all of our PCOS cases metthe clinical criteria for hyperandrogenism, which is con-sidered the cornerstone of PCOS [55]. Finally, our PCOScases were also well defined by ultrasonography and Acnescores.Despite the limitations, the present pilot study allowed
us to follow the patients over a 3-month treatmentregimen. Indeed, our pilot study is an ideal model be-cause it allows metabolomic analysis of pre- andpost-treatment serum taken from the same patient. Thisin turn allows comparative analysis of metabolite profilesfrom subjects for which the genetic, hormonal and
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 6 of 11

environmental backgrounds have remained constant. Inthis way, changes in metabolome occurring during thetreatment can be traced independently from the physio-logical inter-variability among people.Large functional and prospective studies, including
clinical trials, are needed to verify our preliminaryresults and to separate the role of inositols and of thecombined treatment with inositol and glucomannan.Such studies will continue to shed further insights intothese metabolite profiles and determine whether someof them are biomarkers or actual mediators of PCOS. Abetter understanding of the role of these biomarkers inobesity and obesity-related PCOS pathogenesis mightfinally lead to novel targets for therapeutic/preventiveintervention. Furthermore, this kind of study can con-tribute to understanding the role of weight reduction inPCOS patients.
ConclusionsIn summary, our pilot study has identified a complexnetwork of serum molecules that appear to be correlatedwith PCOS, and with a combined treatment withinositols and glucomannan. Future studies with largersamples sizes involving PCOS patients identified throughclinical and biochemical criteria are needed to furthervalidate our findings.
MethodsPopulation and study designThe study was designed as a prospective case-controlconducted at the University of Salerno from September2016 to July 2017. Women with a diagnosis of PCOS(according to the European Society of HumanReproduction and Embryology [4] and to adolescentPCOS diagnostic criteria [35]) were recruited, along withmatched healthy controls.Both cases and controls were enrolled at the
University Hospital “San Giovanni di Dio e Ruggid’Aragona” of Salerno, during routine visits to thegynecological clinic, whenever inclusion criteria werepresent. Inclusion criteria for the case group were: agebetween 18 and 35 years, overweight/obesity (BMI > 25kg/m2), a positive diagnosis of PCOS, and absence ofany other acute intercurrent or chronic illness. Healthycontrols were patients between 18 and 35 years old with-out acute intercurrent or chronic illness.Women using hormonal medications or drugs that
affect insulin sensitivity (e.g., inositols or metformin) be-fore enrollment were excluded.An informed consent form was signed by each partici-
pant at enrollment. The study was carried out in accord-ance with the ethical principles of the declaration ofHelsinki and approved by the ethics committee CEI“Comitato etico Campania Sud” (IRB N. 78/2016).
Subjects were recruited in the framework of a multi-centric registered study. The study was registered in theclinicaltrial.gov portal on August 2018 with the number:NCT03608813. Only patients recruited in the Salernohospital were used for this pilot study.
Data collection and pharmacological treatmentAt enrollment, anamnestic and demographic characteris-tics were collected. Specific data collected include: BMI,frequency and characteristics of menstrual cycle.To evaluate the degree of hirsutism, the modified
score of Ferriman-Gallwey [60] was used. It gives a scorefrom 0 (no growth of terminal area) to 4 (extensive hairgrowth) for each of the nine body areas. An overall valueof Ferriman-Gallwey score greater than, or equal to, 8was considered as indicative of hirsutism according tothe American Association of Clinical EndocrinologistsMedical Guidelines for Clinical Practice for the Diagno-sis and Treatment of Hyperandrogenic Disorders [61].The degree of acne was evaluated according to the
Global evaluation scale proposed in 2002 by FDA [62].In clinical practice, menstrual cycle is considered normalwhen it lasts between 25 and 36 days (28 on average)with a blood loss between 28 and 80 ml; menstrual lossof modest size (< 20ml) is considered hypomenorrhea,while, abundant menstrual loss (> 80ml) is characteristicof hypermenorrhea condition [63]. To evaluate men-strual loss, we used the menstrual pictogram proposedby Magnay et al. [64].Blood concentration of glucose, insulin, triglycerides
and cholesterol were evaluated for control subjects andfor cases at baseline (PCOS-T0) and after 3 months oftreatment (PCOS-T1). HOMA-IR was also calculated.Ovary volumes and the antral follicles count wereevaluated by a vaginal ultrasound performed by a trainedgynecologist.Enrolled cases were treated with myo-inositol 1.75 g/
day, D-chiro-inositol 0.25 g/day and glucomannan 4 g/day using the Realim (AG Pharma, Rome, Italy) formula-tion. The drugs were divided into two equal parts andtaken before the two principal meals for three consecu-tive months. After this time, the patients werere-evaluated regarding the anthropometric, biochemicaland ultrasound parameters. Both groups were recom-mended to not change any life standards during thestudy period, except for the use of medications.
Ultrasonographic evaluationAll patients underwent transvaginal ultrasonography(US) performed by four experienced gynecologists (C.C.,M.C., L.G. and M.G.) using a MyLab Seven ultrasoundmachine (Esaote, Genova, Italy) with a 5MHz convexprobe using a transvaginal approach. This approachmade it possible to accurately evaluate the internal
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 7 of 11

structure, even in obese patients, in whom thetrans-abdominal scan was not sufficiently reliable.Transvaginal ultrasonography was performed with thewoman in the lithotomy position and empty bladder. Tocorrectly visualize the annexes, we moved the probe tothe right for the right adnexal region and to the left forthe left adnexal region; furthermore, by rotating theprobe and making movements in the anterior-posteriordirection, both on the right and on the left, we obtainedoblique-longitudinal scans that allowed us to evaluatethe entire adnexal region. The position, the echostruc-ture, the size of the ovaries and the number of folliclesfor each of them were evaluated. In particular, for thedimensions, we measured three orthogonal diametersfor each ovary (defined D1, D2 and D3) and then the USmachine software applied the ellipsoid formula: π/6 X(D1 X D2 X D3). For the number of follicles, thecalculation included all the follicles present on eachovary, from margin more internal to the outermost one,regardless of their arrangement, and, for a more exhaust-ive study. According to the Rotterdam ESHRE/ASRM--Sponsored PCOS Consensus Workshop Group, presenceof 12 or more follicles in each ovary, measuring 2–9 mmin diameter, and/or increased ovarian volume (> 10mL)are the criteria with sufficient specificity and sensitivityfor the diagnosis of PCOS.
Samples collectionHuman tissue collection strictly adhered to the guide-lines outlined in the Declaration of Helsinki IV edition[65]. Blood samples were collected at enrollment fromcontrols and at enrollment and three months after thetreatment for cases, using a BD vacutainer (BectonDickinson, Oxfordshire, UK) blood collection red tube(with no additives). After centrifugation, the sample wasimmediately frozen to − 80 °C until the time of analysis.All patients were asked to respect a 12-h fast beforeblood collection.
Metabolite extraction and derivatizationMetabolome extraction, purification and derivatizationwas carried out with the MetaboPrep GC kit (Theo-reo srl, Montecorvino Pugliano [SA], Italy) accordingto the manufacturer’s instructions. Details regardingmetabolite extraction and the overall analyticalscheme, including QA/QC sample analyses, werereported in Troisi et al. [24, 66, 67].
GC-MS analysisTwo μL samples of the derivatized solution wereinjected into the GC-MS system (GC-2010 Plus gaschromatograph coupled to a 2010 Plus single quadru-pole mass spectrometer; Shimadzu Corp., Kyoto, Japan).Chromatographic separation was achieved with a 30
m × 0.25 mm CP-Sil 8 CB fused silica capillary GCcolumn with 1.00 μm film thickness (Agilent, J&WScientific, Folsom, CA, USA). High-purity helium wasused as carrier gas. The initial oven temperature of 100 °Cwas maintained for 1min and then raised by 4 °C/min to320 °C with a further 4min of hold time. The gas flow wasset to obtain a constant linear velocity of 39 cm/s and thesplit flow was set at 1:5. The mass spectrometer was oper-ated with electron impact ionization (70 eV) in full scanmode in the interval of 35–600m/z with a scan velocity of3333 amu/sec and a solvent cut time of 4.5 min. Thecomplete GC program duration was 60min. Untargetedmetabolites were identified by comparing the massspectrum of each chromatographic peak with the NISTlibrary collection (NIST, Gaithersburg, MD, USA). Over250 signals were observed in each sample, but several werenot investigated further because they were either not con-sistently found in other sets of samples or were too low inconcentration to be confirmed as metabolites due to poorspectral quality. A total of 243 endogenous metabolites in-volved in energy metabolism, lipid metabolism and aminoacid metabolism were consistently detected and positivelyidentified. To identify peaks, the linear index differencemax tolerance was set at 10, while the minimum matchingfor the NIST library search was set at 85%.
Statistical analysis
Sample size evaluation Based on the GC-MS serummetabolomic profiles of PCOS patients and controls, wehave evaluated the minimum sample size to include inthis pilot study to reach an 80% statistical power. Samplesize was evaluated using the average power of all metab-olites corrected for multiple testing using the falsediscovery rate (FDR = 0.20) by means of the SSPA pack-age implemented in BioConductor [68] based onFerreira and Zwinderman algorithms [69].
Anthropometric parameters Data are reported asmean ± standard deviation for continuous variables andnumber (percentage) for categorical variables.Statistical analysis was performed using Statistica soft-
ware (StatSoft, Oklahoma, USA) and Minitab (MinitabInc., Pennsylvania, USA). Normal distribution of datawas verified using the Shapiro-Wilks test. Since the datawere normally distributed, the t-test was used forinter-group (CTRL/PCOS-T0 and CTRL/PCOS-T1) andintra-group (PCOS-T0/PCOS-T1) comparisons. Thealpha (ɑ) value was set to 0.05. Pearson’s chi-squared testwas used to determine differences among groups for thecategorical variables.
Multivariate data analysis The chromatographic datawere tabulated with one sample per row and one
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 8 of 11

variable (metabolite) per column. Data pre-treatmentconsisted of normalizing each metabolite peak area tothat of the internal standard followed by generalized logtransformation and data scaling by autoscaling(mean-centered and divided by standard deviation ofeach variable). PLS-DA [70] was performed using thestatistical software package R (Foundation for StatisticalComputing, Vienna, Austria). Class separation wasachieved by PLS-DA, which is a supervised method thatuses multivariate regression techniques to extract, vialinear combinations of original variables (X), the infor-mation that can predict class membership (Y). PLSregression was performed using the plsr functionincluded in the R pls package [71]. Classification andcross-validation was performed using the correspondingwrapper function included in the caret package [72]. Apermutation test was performed to assess the signifi-cance of class discrimination. In each permutation, aPLS-DA model was built between the data (X) and thepermuted class labels (Y) using the optimal number ofcomponents determined by cross validation for themodel based on the original class assignment. Two typesof test statistics were used to measure class discrimin-ation. The first is based on prediction accuracy duringtraining. The second made use of separation distancebased on the ratio Between group sum of the squaresand the Within group sum of squares (B/W-ratio). If theobserved test statistics was part of the distribution basedon the permuted class assignments, class discriminationcannot be considered significant from a statistical pointof view [73]. Variable Importance in Projection (VIP)scores were calculated for each metabolite. The VIPscore is a weighted sum of squares of the PLS loadings,taking into account the amount of explained Y-variationin each dimension. The highest scoring VIP metaboliteswere compared in terms of fold changes (FC). FC is theratio of the mean abundances between any two classesand is a measure describing how much a quantitychanges going from an initial to a final value.The metabolic pathway was constructed using MetS-
cape application [74] of the software Cytoscape [75].
Additional file
Additional file 1: Predicted power and sample size relationship plot.(TIFF 215 kb)
AbbreviationsBMI: Body Mass Index; CTRL: Control Subjects; DCI: D-chiro-inositol; FC: FoldChange; FDA: Food and Drug Administration; FDR: False Discovery Rate;HOMA-IR: Homeostatic Model Assessment for Insulin Resistance; IR: InsulinResistance; IRB: Institutional Review Board; IST: National Institute of Standardand Technology; MI: Myo-inositol; PCOS: Polycystic ovary syndrome; PCOS-T0: Polycystic ovary syndrome patients at baseline; PCOS-T1: Polycystic ovarysyndrome patients after 3-months; PLS-DA: Partial Least Square DiscriminantAnalysis; QA/QC: Quality assurance and Quality Controls; SSPA: Sample Size
and Power Analysis; TCA: Tricarboxylic Acid Cycle; VIP: Variable Importanceon Projection
AcknowledgementsNot applicable.
FundingThis project was funded by POR CAMPANIA FESR 2014/2020 Asse 1 -Obiettivo specifico 1.2 - Azione1 .2. Progetto: Campania Onco Terapie CUP:B61G18000470007.
Availability of data and materialsThe datasets generated during and/or analyzed during the current study areavailable from the corresponding author on reasonable request.
Authors’ contributionsJT, CC, LG and LS wrote the main manuscript text, SS, SR, DA and MG editthe text. JT, GS and PC performed the metabolomics and the biochemicalanalysis. JT, GS, SS, SR, performed the statistical evaluation and built themachine learning algorithms. CC, MC, LG and MG enrolled the patients andperformed the clinical evaluations. All authors reviewed the manuscript.All authors read and approved the final manuscript.
Ethics approval and consent to participateThe study was carried out in accordance with the ethical principles of thedeclaration of Helsinki and approved by the ethics committee CEI “Comitatoetico Campania Sud” (IRB N. 78/2016).
Consent for publicationThe manuscript describes anonymized data.
Competing interestsJT and GS work for companies (Theoreo srl and Hosmotic srl, respectively)dealing with the development and marketing of diagnostic tests based onmetabolomics. All other authors declare no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana”,University of Salerno, Baronissi, SA, Italy. 2Theoreo srl, Via degli Ulivi 3, 84090Montecorvino Pugliano, SA, Italy. 3European Biomedical Research Institute ofSalerno (EBRIS), Via S. de Renzi, 3, 84125 Salerno, SA, Italy. 4Department ofChemistry and Physics, University of Tennessee at Chattanooga, 615 McCallieAve., Chattanooga, TN 37403, USA. 5Department of Obstetrics andGynecology, University of Tennessee College of Medicine, Chattanooga, TN,USA. 6Department of Biology, Geology and Environmental Sciences,University of Tennessee at Chattanooga, 615 McCallie Ave., Chattanooga, TN37403, USA. 7Department of Physics, University of Salerno, Fisciano, SA, Italy.8Department of Neurosciences and Reproductive and Dentistry Sciences,University of Naples Federico II, Naples, Italy. 9Hosmotic srl, Via Raffale Bosco78, 80069 Vico Equense, NA, Italy. 10Azienda Sanitaria Locale, distrettosanitario 66, via Vernieri, 14, 84124 Salerno, SA, Italy. 11Istituto SistemiComplessi – Consiglio Nazionale delle Ricerche, Rome, Italy.
Received: 18 October 2018 Accepted: 7 March 2019
References1. Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF,
Futterweit W, et al. The androgen excess and PCOS society criteria for thepolycystic ovary syndrome: the complete task force report. Fertil Steril.2009;91:456–88.
2. Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO. Theprevalence and features of the polycystic ovary syndrome in an unselectedpopulation. J Clin Endocrinol Metab. 2004;89:2745–9.
3. Fauser BCJM, Tarlatzis BC, Rebar RW, Legro RS, Balen AH, Lobo R, et al.Consensus on women’s health aspects of polycystic ovary syndrome
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 9 of 11

(PCOS): the Amsterdam ESHRE/ASRM-sponsored 3rd PCOS consensusworkshop group. Fertil Steril. 2012;97:28–38 e25.
4. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group.Revised 2003 consensus on diagnostic criteria and long-term health risksrelated to polycystic ovary syndrome. Fertil Steril. 2004;81:19–25.
5. Galazis N, Pang Y-L, Galazi M, Haoula Z, Layfield R, Atiomo W. Proteomicbiomarkers of endometrial cancer risk in women with polycystic ovarysyndrome: a systematic review and biomarker database integration.Gynecol Endocrinol Off J Int Soc Gynecol Endocrinol. 2013;29:638–44.
6. Sortino MA, Salomone S, Carruba MO, Drago F. Polycystic ovary syndrome: insightsinto the therapeutic approach with Inositols. Front Pharmacol. 2017;8:341.
7. Kalra B, Kalra S, Sharma J. The inositols and polycystic ovary syndrome.Indian J Endocrinol Metab. 2016;20:720–4.
8. Bizzarri M, Carlomagno G. Inositol: history of an effective therapy forpolycystic ovary syndrome. Eur Rev Med Pharmacol Sci. 2014;18:1896–903.
9. Heimark D, McAllister J, Larner J. Decreased myo-inositol to chiro-inositol(M/C) ratios and increased M/C epimerase activity in PCOS theca cellsdemonstrate increased insulin sensitivity compared to controls. Endocr J.2014;61:111–7.
10. Larner J. D-chiro-inositol--its functional role in insulin action and its deficit ininsulin resistance. Int J Exp Diabetes Res. 2002;3:47–60.
11. Sun T, Heimark DB, Nguygen T, Nadler JL, Larner J. Both myo-inositol tochiro-inositol epimerase activities and chiro-inositol to myo-inositol ratiosare decreased in tissues of GK type 2 diabetic rats compared to Wistarcontrols. Biochem Biophys Res Commun. 2002;293:1092–8.
12. Lyon MR, Reichert RG. The effect of a novel viscous polysaccharide alongwith lifestyle changes on short-term weight loss and associated risk factorsin overweight and obese adults: an observational retrospective clinicalprogram analysis. Altern Med Rev J Clin Ther. 2010;15:68–75.
13. Doi K. Effect of konjac fibre (glucomannan) on glucose and lipids. Eur J ClinNutr. 1995;49(Suppl 3):S190–7.
14. Shima K, Tanaka A, Ikegami H, Tabata M, Sawazaki N, Kumahara Y. Effect ofdietary fiber, glucomannan, on absorption of sulfonylurea in man. HormMetab Res Horm Stoffwechselforschung Horm Metab. 1983;15:1–3.
15. Scalfi L, Coltorti A, D’Arrigo E, Carandente V, Mazzacano C, Di Palo M, et al.Effect of dietary fibre on postprandial thermogenesis. Int J Obes.1987;11(Suppl 1):95–9.
16. Cairella M, Marchini G. Evaluation of the action of glucomannan onmetabolic parameters and on the sensation of satiation in overweight andobese patients. Clin Ter. 1995;146:269–74.
17. Au-Yeung F, Jovanovski E, Jenkins AL, Zurbau A, Ho HVT, Vuksan V. The effects ofgelled konjac glucomannan fibre on appetite and energy intake in healthyindividuals: a randomised cross-over trial. Br J Nutr. 2018;119:109–16.
18. (NDA) EP on DPN and A. Scientific Opinion on the substantiation of healthclaims related to konjac mannan (glucomannan) and reduction of bodyweight (ID 854, 1556, 3725), reduction of post-prandial glycaemic responses(ID 1559), maintenance of normal blood glucose concentrations (ID 835,3724), maintenance of normal (fasting) blood concentrations of triglycerides(ID 3217), maintenance of normal blood cholesterol concentrations (ID3100, 3217), maintenance of normal bowel function (ID 834, 1557, 3901)and decreasing potentially pathogenic gastro-intestinal microorganisms(ID 1558) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J.2010;8 Available from: https://doi.org/10.2903/j.efsa.2010.1798.
19. De Leo V, Tosti C, Cappelli V, Morgante G, Cianci EA. Combinationinositol and glucomannan in PCOS patients. Minerva Ginecol. 2014;66:527–33.
20. Dunn WB, Broadhurst DI, Atherton HJ, Goodacre R, Griffin JL.Systems level studies of mammalian metabolomes: the roles of massspectrometry and nuclear magnetic resonance spectroscopy. ChemSoc Rev. 2011;40:387–426.
21. Gowda GAN, Zhang S, Gu H, Asiago V, Shanaiah N, Raftery D. Metabolomics-basedmethods for early disease diagnostics. Expert Rev Mol Diagn. 2008;8:617–33.
22. Turkoglu O, Zeb A, Graham S, et al. Metabolomics of biomarker discovery inovarian cancer: a systematic review of the current literature. Metabolomics.2016;12(4):60.
23. Bahado-Singh RO, Lugade A, Field J, Al-Wahab Z, Han B, Mandal R, et al.Metabolomic prediction of endometrial cancer. Metabolomics. 2017;14:6.
24. Troisi J, Sarno L, Landolfi A, Scala G, Martinelli P, Venturella R, et al. Metabolomicsignature of endometrial Cancer. J Proteome Res. 2018;17:804–12.
25. Murri M, Insenser M, Escobar-Morreale HF. Metabolomics in polycystic ovarysyndrome. Clin Chim Acta Int J Clin Chem. 2014;429:181–8.
26. Zhang Y, Liu L, Yin T-L, Yang J, Xiong C-L. Follicular metabolic changes andeffects on oocyte quality in polycystic ovary syndrome patients. Oncotarget.2017;8:80472–80.
27. Zhao Y, Fu L, Li R, Wang L-N, Yang Y, Liu N-N, et al. Metabolicprofiles characterizing different phenotypes of polycystic ovarysyndrome: plasma metabolomics analysis. BMC Med. 2012;10:153.
28. Couto Alves A, Valcarcel B, Makinen V-P, Morin-Papunen L, Sebert S, KangasAJ, et al. Metabolic profiling of polycystic ovary syndrome revealsinteractions with abdominal obesity. Int J Obes (Lond). 2017;41:1331–40.
29. Zhang C, Zhao Y, Li R, Yu Y, Yan L, Li L, et al. Metabolic heterogeneity offollicular amino acids in polycystic ovary syndrome is affected by obesityand related to pregnancy outcome. BMC Pregnancy Childbirth. 2014;14:11.
30. Whigham LD, Butz DE, Dashti H, Tonelli M, Johnson LK, Cook ME, et al.Metabolic evidence of diminished lipid oxidation in women with polycysticovary syndrome. Curr Metabolomics. 2014;2:269–78.
31. Samino S, Vinaixa M, Diaz M, Beltran A, Rodriguez MA, Mallol R, et al.Metabolomics reveals impaired maturation of HDL particles in adolescentswith hyperinsulinaemic androgen excess. Sci Rep. 2015;5:11496.
32. Vinaixa M, Rodriguez MA, Samino S, Diaz M, Beltran A, Mallol R, et al.Metabolomics reveals reduction of metabolic oxidation in women withpolycystic ovary syndrome after pioglitazone-flutamide-metforminpolytherapy. PLoS One. 2011;6:e29052.
33. Selen Alpergin ES, Bolandnazar Z, Sabatini M, Rogowski M, Chiellini G,Zucchi R, et al. Metabolic profiling reveals reprogramming of lipid metabolicpathways in treatment of polycystic ovary syndrome with 3-iodothyronamine. Physiol Rep. 2017;5:e13097.
34. Karakas SE, Perroud B, Kind T, Palazoglu M, Fiehn O. Changes in plasmametabolites and glucose homeostasis during omega-3 polyunsaturatedfatty acid supplementation in women with polycystic ovary syndrome. BBAClin. 2016;5:179–85.
35. Rosenfield RL. The diagnosis of polycystic ovary syndrome in adolescents.Pediatrics. 2015;136:1154–65.
36. Gilbert EW, Tay CT, Hiam DS, Teede HJ, Moran LJ. Comorbidities andcomplications of polycystic ovary syndrome: an overview ofsystematic reviews. Clin Endocrinol (Oxf). 2018;0 Available from:https://doi.org/10.1111/cen.13828.
37. Sun L, Hu W, Liu Q, Hao Q, Sun B, Zhang Q, et al. Metabonomics revealsplasma metabolic changes and inflammatory marker in polycystic ovarysyndrome patients. J Proteome Res. 2012;11:2937–46.
38. Landin K, Lonnroth P, Krotkiewski M, Holm G, Smith U. Increased insulinresistance and fat cell lipolysis in obese but not lean women with a highwaist/hip ratio. Eur J Clin Investig. 1990;20:530–5.
39. Escobar-Morreale HF, Samino S, Insenser M, Vinaixa M, Luque-Ramirez M,Lasuncion MA, et al. Metabolic heterogeneity in polycystic ovary syndromeis determined by obesity: plasma metabolomic approach using GC-MS.Clin Chem. 2012;58:999–1009.
40. Marei WF, Wathes DC, Fouladi-Nashta AA. Impact of linoleic acid on bovineoocyte maturation and embryo development. Reprod Camb Engl.2010;139:979–88.
41. Escobar-Morreale HF, Luque-Ramirez M, Gonzalez F. Circulatinginflammatory markers in polycystic ovary syndrome: a systematic reviewand metaanalysis. Fertil Steril. 2011;95:1048–58 e1-2.
42. Ojeda-Ojeda M, Murri M, Insenser M, Escobar-Morreale HF. Mediators oflow-grade chronic inflammation in polycystic ovary syndrome (PCOS).Curr Pharm Des. 2013;19:5775–91.
43. Gaster M, Nehlin JO, Minet AD. Impaired TCA cycle flux in mitochondria inskeletal muscle from type 2 diabetic subjects: marker or maker of thediabetic phenotype? Arch Physiol Biochem. 2012;118:156–89.
44. Jimenez PT, Frolova AI, Chi MM, Grindler NM, Willcockson AR,Reynolds KA, et al. DHEA-mediated inhibition of the pentosephosphate pathway alters oocyte lipid metabolism in mice.Endocrinology. 2013;154:4835–44.
45. Witchel SF, Oberfield S, Rosenfield RL, Codner E, Bonny A, Ibáñez L, et al.The diagnosis of polycystic ovary syndrome during adolescence.Horm Res Paediatr. 2015;83:376–89.
46. Legro RS, Arslanian SA, Ehrmann DA, Hoeger KM, Murad MH, Pasquali R, etal. Diagnosis and treatment of polycystic ovary syndrome: an EndocrineSociety clinical practice guideline. J Clin Endocrinol Metab. 2013;98:4565–92.
47. Laganà AS, Rossetti P, Buscema M, La Vignera S, Condorelli RA, Gullo G, etal. Metabolism and ovarian function in PCOS women: a therapeuticapproach with Inositols. Int J Endocrinol. 2016;2016:6306410.
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 10 of 11

48. Unfer V, Nestler JE, Kamenov ZA, Prapas N, Facchinetti F. Effects of inositol(s)in women with PCOS: a systematic review of randomized controlled trials.Int J Endocrinol. 2016;2016:1849162.
49. Gateva A, Unfer V, Kamenov Z. The use of inositol(s) isomers in themanagement of polycystic ovary syndrome: a comprehensive review.Gynecol Endocrinol Off J Int Soc Gynecol Endocrinol. 2018;34:545–50.
50. Dong F, Deng D, Chen H, Cheng W, Li Q, Luo R, et al. Serum metabolomicsstudy of polycystic ovary syndrome based on UPLC-QTOF-MS coupled witha pattern recognition approach. Anal Bioanal Chem. 2015;407:4683–95.
51. Focker M, Timmesfeld N, Scherag S, Knoll N, Singmann P, Wang-Sattler R, etal. Comparison of metabolic profiles of acutely ill and short-term weightrecovered patients with anorexia nervosa reveals alterations of 33 out of163 metabolites. J Psychiatr Res. 2012;46:1600–9.
52. Pundir J, Psaroudakis D, Savnur P, Bhide P, Sabatini L, Teede H, et al. Inositoltreatment of anovulation in women with polycystic ovary syndrome: a meta-analysis of randomised trials. BJOG Int J Obstet Gynaecol. 2018;125:299–308.
53. Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-sensitising drugs(metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women withpolycystic ovary syndrome, oligo amenorrhoea and subfertility. CochraneDatabase Syst Rev. 2009;11:CD003053.
54. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations forplanning pilot studies in clinical and translational research.Clin Transl Sci. 2011;4:332–7.
55. Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF,Futterweit W, et al. Positions statement: criteria for defining polycystic ovarysyndrome as a predominantly hyperandrogenic syndrome: an androgenexcess society guideline. J Clin Endocrinol Metab. 2006;91:4237–45.
56. Panidis D, Tziomalos K, Papadakis E, Chatzis P, Kandaraki EA, Tsourdi EA, etal. The clinical significance and primary determinants of hirsutism inpatients with polycystic ovary syndrome. Eur J Endocrinol. 2013;168:871–7.
57. Coskun A, Ercan O, Arikan DC, Ozer A, Kilinc M, Kiran G, et al. ModifiedFerriman-Gallwey hirsutism score and androgen levels in Turkish women.Eur J Obstet Gynecol Reprod Biol. 2011;154:167–71.
58. Amiri M, Ramezani Tehrani F, Nahidi F, Bidhendi Yarandi R, Behboudi-Gandevani S, Azizi F. Association between biochemical hyperandrogenismparameters and Ferriman-Gallwey score in patients with polycystic ovarysyndrome: a systematic review and meta-regression analysis.Clin Endocrinol. 2017;87:217–30.
59. Cibula D, Hill M, Starka L. The best correlation of the new index ofhyperandrogenism with the grade of increased body hair. Eur J Endocrinol.2000;143:405–8.
60. Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women.J Clin Endocrinol Metab. 1961;21:1440–7.
61. Goodman NF, Bledsoe MB, Cobin RH, Futterweit W, Goldzieher JW, PetakSM, Smith KD, Steinberger E, American Association of ClinicalEndocrinologists Hyperandrogenic Disorders Task Force. AmericanAssociation of Clinical Endocrinologists Medical Guidelines for ClinicalPractice for the Diagnosis and Treatment of Hyperandrogenic Disorders.Endocr Pract. 2001;7:120–34.
62. Lehmann HP, Robinson KA, Andrews JS, Holloway V, Goodman SN. Acnetherapy: a methodologic review. J Am Acad Dermatol. 2002;47:231–40.
63. Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual blood loss--apopulation study. Variation at different ages and attempts to definenormality. Acta Obstet Gynecol Scand. 1966;45:320–51.
64. Magnay JL, Nevatte TM, Seitz C, O’Brien S. A new menstrual pictogram foruse with feminine products that contain superabsorbent polymers. FertilSteril. 2013;100:1715–21 e1-4.
65. World Medical Association. World medical association declaration ofHelsinki: Ethical principles for medical research involving human subjects.JAMA. 2013;310:2191–4.
66. Troisi J, Sarno L, Martinelli P, Di Carlo C, Landolfi A, Scala G, et al. Ametabolomics-based approach for non-invasive diagnosis of chromosomalanomalies. Metabolomics. 2017;13:140.
67. Troisi J, Landolfi A, Sarno L, Richards S, Symes S, Adair D, et al. Ametabolomics-based approach for non-invasive screening of fetal centralnervous system anomalies. Metabolomics. 2018;14:77.
68. van Iterson M, ‘t Hoen PAC, Pedotti P, Hooiveld GJEJ, den Dunnen JT, vanOmmen GJB, et al. Relative power and sample size analysis on geneexpression profiling data. BMC Genomics. 2009;10:439.
69. Ferreira JA, Zwinderman A. Approximate sample size calculations withmicroarray data: an illustration. Stat Appl Genet Mol Biol. 2006;5:Article25.
70. Wold S, Sjöström M, Eriksson L. PLS-regression: a basic tool ofchemometrics. PLS Methods. 2001;58:109–30.
71. Mevik B-H, Wehrens R. The pls package: principal component and partialleast squares regression in R. J Stat Softw. 2007;1 Available from: https://www.jstatsoft.org/v018/i02.
72. Kuhn M. Building predictive models in R using the caret package. J StatSoftw. 2008;1 Available from: https://www.jstatsoft.org/v028/i05.
73. Bijlsma S, Bobeldijk I, Verheij ER, Ramaker R, Kochhar S, Macdonald IA, et al.Large-scale human metabolomics studies: a strategy for data (pre-)processing and validation. Anal Chem. 2006;78:567–74.
74. Karnovsky A, Weymouth T, Hull T, Tarcea VG, Scardoni G, Laudanna C, et al.Metscape 2 bioinformatics tool for the analysis and visualization ofmetabolomics and gene expression data. Bioinforma Oxf Engl.2012;28:373–80.
75. Nishida K, Ono K, Kanaya S, Takahashi K. KEGGscape: a Cytoscape app forpathway data integration. F1000Research. 2014;3:144.
Troisi et al. Journal of Ovarian Research (2019) 12:25 Page 11 of 11