Embed Size (px)
Citation preview

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8
Metal Stents in the Urinary Tract
Evangelos N. Liatsikos a,*, Dimitrios Karnabatidis b, George C. Kagadis c,Paraskevi F. Katsakiori a, Jens-Uwe Stolzenburg d, George C. Nikiforidis c,Petros Perimenis a, Dimitrios Siablis b
aDepartment of Urology, University of Patras, School of Medicine, Patras, GreecebDepartment of Radiology, University of Patras, School of Medicine, Patras, GreececDepartment of Medical Physics, University of Patras, School of Medicine, Patras, GreecedDepartment of Urology, University of Leipzig, Germany
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Article info
Keywords:Metal stentsUreterUrethra
Abstract
Introduction: The successful use of metal stents (MSs) in the vascular andbiliary systems led several investigators to propose their use in urology.Methods: In the present study, we review the current literature andpresent the latest developments with the application of MSs in theurinary tract.Results: The application of MSs in the urinary tract has improved clinicaloutcome in the treatment of urinary tract strictures and is currentlythought to be a useful tool in urology practice.Conclusions: Considerable efforts are being made to optimise stentbiomaterial, the coating, and, in general, the ureteral stent design.Continuing the research interest seems to be essential for further clinicalimprovement, aiming to minimise stent-related morbidity.
# 2006 European Association of Urology and European Board of Urology.
Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Urology, University of Patras, School of Medicine,Patras, GR 265 00 Greece. Tel. +1130 2610 999386; Fax: +1130 2610 993981.E-mail address: [email protected] (E.N. Liatsikos).
1. Introduction
The successful use of metal stents (MSs) in thevascular and biliary systems led several investiga-tors to propose their use in urology. In 1988, Milroyimplanted the first stent in the urinary tract for thetreatment of urethral stricture [1]. Over recent years,their use has been expanded in the managementof benign conditions, such as benign prostatichyperplasia, urethral stricture, and detrusor sphinc-ter dyssynergia [2,3]. Urologists initially implantedureteral stents as a palliative intervention in
1871-2592/$ – see front matter # 2006 European Association of UrologyPublished by Elsevier B.V. All rights reserved.
end-stage malignant disease [4–9]. Treating uretero-intestinal strictures is another application thatseems to be challenging. The use of MSs in thissituation shows promising results but still has manyuntoward effects such as tissue ingrowth andrecurrent obstruction [10–12].
Urothelial hyperplasia through the stent mesh,encrustation, infection, stent migration, and inter-action between stent and ureteral peristalsis areimportant issues that influence the short-term andespecially long-term results after stent insertion in astrictured ureter. Urologists have used various
and European Board of Urology. doi:10.1016/j.eeus.2006.11.003

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 878
experimental models to approach these issues andhave proposed the use of metal mesh stents coatedor covered with biocompatible materials to mini-mise these side-effects. Still, the ideal MS withradiopacity, low cost, long-term patency as well asresistance to encrustation, infection, and migrationis yet to come.
In the present study, we review the currentliterature and present the latest developments withthe application of MSs in the urinary tract.
2. Urethral MSs
2.1. Types and history of urethral stents
The urethra was the first anatomic site of theurinary tract stented by Milroy et al to treat recurrentbulbar urethral stricture after optical urethrotomy[1]. Since then, permanent stents, made from
Table 1 – Clinical experience with the use of urethral metal st
Investigators No. of patients
Self-expanding, woven stent
Milroy et al [1] 8 The first anatomic site stente
period: 8 mo (6–12 mo).
At mean follow-up of 8 mo,
covering of the implant at 4–
ASI titanium stent
Kirby et al [2] 30 Aim: treat intravesical obstru
25 patients. Urinary tract inf
epithelisation of the stent su
Self-reinforced bioabsorbable stents
Laaksovirta et al [41] 39 Aim: prevent postoperative u
A lactic and glycolic acid copo
the stent was degraded into s
prostatic urethra. In 2 patient
Isotalo et al [44,45] 22 Aim: treat recurrent urethral
double-spiral stent was used
voiding: all patients. Urinary
all patients, except 1. Degrad
At 46 mo: successful treatme
Covered retrievable expandable nitinol stent
Song et al [25] 12 Aim: treat traumatic urethra
Mean follow-up: 20 mo; 4/12
with the insertion of the firs
Temperature-based memory-shape metal stent
Kamata et al [22] 1 Aim: treat ischuria after repa
A nickel-titanium alloy stent
into the bladder was observe
VanDijk et al [21] 108 Aim: treat severe lower urina
The bell-shaped nitinol prost
Spontaneous voiding: all pat
and migration. This stent do
VanDijk et al [20] 35 Aim: treat lower urinary trac
nitinol prostatic stent was us
voiding: all patients. Main re
towards the bladder. Uneven
various materials or nondegradable polymers, havebeen applied in the urethra. Several problems suchas encrustation, hyperplasia of the epithelium, andpostvoiding dribbling have been reported, leading tothe development of temporary urethral stents [13].The clinical experience with the use of urethral MSsis shown in Table 1.
Three types of MSs have been used to treatrecurrent urethral strictures: the self-expandingmesh, the ASI titanium stent, which is a short rigidmesh of titanium wire, and the nitinol stent, whichis a flexible spring in one or two parts connected by asteel wire remaining endoluminal [14]. There aresome anatomic limitations of the prostatic urethrathat may influence the clinical outcome after stentplacement. The prostatic urethra does not alwaysconform to the cylindrical shape of the insertedstent. In addition, the bladder neck/urethral angle isnot a right angle, thus leading to difficult positioningand probably inadequate epithelial covering of the
ents
Description
d in the urinary tract. Aim: treat urethral strictures. Follow-up
good calibre urethra. Ureteroscopy revealed complete epithelial
6 mo.
ction due to benign prostatic hyperplasia. Effective micturition:
ection: 10 patients, without need for stent removal. Partial
rface: in a proportion of patients.
rinary retention after procedures that induce prostatic edema.
lymer prostatic spiral stent was used in all cases. At 4 mo,
mall pieces. At 6 mo, no piece of the stent was found in the
s, a stent portion was found at the bottom of the bladder.
strictures. A self-expandable, self-retaining poly-L-lactic acid
in combination with optical urethrotomy in all cases. Free
infection: 2 patients. Total epithelialisation of the stent after 6 mo:
ation at 12 mo: all patients. Stricture recurrence: 10 patients.
nt in 8/22 patients.
l strictures near the external sphincter.
patients, 5/8 patients, and 2/2 patients were successfully treated
t, the second, and the third stent, respectively.
ired cloacal anomaly with a temporary stent.
was implanted in a 2-yr-old girl. Asymptomatic stent migration
d in 2 mo.
ry tract symptoms due to benign prostatic enlargement.
atic stent was inserted in all cases. Successful insertion: 97%.
ients. Main complications: haematuria, urge incontinence,
es not seem suitable for clinical use.
t symptoms due to bladder outlet obstruction. An hourglass-shaped
ed in all cases. Failure of insertion: 5 patients. Spontaneous
ason for stent removal: stent migration (93%), in most cases
tful removal: in all, except for 1.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8 79
stent [15]. However, the advantage of stent place-ment over the conventional urethral catheter, toovercome the urethral stricture, has already beenreported with regard to the risk for urinary tractinfection [16].
The removal of the urethral stent is still an issueof concern. The permanent stents remain on theurethral wall and keep the lumen permanentlyopen, leading to uncontrolled dribbling after voiding[1]. Besides, they induce mucosal hyperplasiathrough the stent openings, with the potential riskof stent obstruction. If stent obstruction occurs,repeat endoscopic resection, stent replacement, oreven surgical removal may be needed. To resolvethese problems, several types of temporarily placedor bioabsorbable urethral stents were introduced[17,18]. Currently, urologists tend to temporarilystent the urethra with the use of bioabsorbable orthermoexpandable memory shape stents. The firstones are biodegraded, leading to self-remotion. Thesecond ones are relatively easily removed due totheir nature. They soften at a specific temperatureand regain their shape in a different one.
The first bioabsorbable urethral stent was intro-duced in an experimental animal study by Kemp-painen et al in 1993 [18]. Bioabsorbable materialsused in urology are polyactic acid, polyglycolic acid,and copolymers of lactide and glycoside. Thebiodegradation time depends on the stent materialand processing methods and ranges from 2 to 12 mo.Isotalo et al compared a new braided self-reinforcedpoly-L-lactic acid (SR-PLLA) urethral stent with thespiral biodegradable SR-PLLA stent and a stainlesssteel stent in rabbits [19]. The results of thisexperimental study were encouraging because thedegradation of the new stent seemed more con-trolled and more favourable compared to thedisintegration of the previous stent forms. Butclinical studies are needed to prove the efficacy ofthis new stent in the strictured urethra in humans.
Several thermoexpandable shape-memory stentshave been used in urethral strictures. Van Dijk et alused a hourglass-shaped nitinol prostatic stent inthe management of bladder outlet obstruction.Improvement of the symptoms was observed, butthe application of this stent was limited due to highmigration rate and, consequently, the need for itsremoval [20]. The same authors also introduced theuse of bell-shaped nitinol stent (Endocare) withpromising results [21]. Memokath 028 (Engineers &Doctors A/S, Hombaek, Denmark) was placed byKamata et al for 6 mo in a 2-yr-old girl with ischuriaafter repaired cloacal anomaly. Their observationsshow that the temporary application of this memorymetal stent in paediatric patients with functional
obstruction can be a safe and effective alternative[22].
The ideal urethral stent is still under develop-ment. Its predominance over the urethral catheterin the treatment of urethral strictures has alreadybeen described, but the complications that mayoccur after stent placement in the urethra minimiseits use and prompts a more appropriate urethralstent design.
2.2. The stent influence on the urethra
The interaction between the stent material and theendothelium of the urethra is a significant issue thatinfluences the long-term outcome and the patient’squality of life after stent placement. Stent obstruc-tion or migration, encrustation, injury of urethra,and formation of granulation tissue are some ofthese issues. Experimental studies are being con-ducted to evaluate the possible effects of the stentinsertion to the urethra and develop a moreappropriate urethral stent (Table 2).
MSs can easily migrate and cause local pain,discomfort, and hyperplasia of the mucosa. Encrus-tation has been described while using permanenturethral stents [2]. When the MS is fully incorpo-rated into the periurethral tissues, it is difficult to beremoved and even surgical procedures may beneeded. For this reason, bioabsorbable or tempera-ture-based shape-memory stents are being investi-gated [18–22]. However, with use of these kinds ofstents, migration is more possible. In addition, thesudden breakdown of the bioabsorbable stent maycause urethral obstruction from the broken pieces.Currently, there is a continuous search for thedevelopment of bioabsorbable urethral stents with areduced possibility for migration and urethralobstruction.
Restenosis or blockage of the stent may occur dueto either tissue hyperplasia or to formation ofgranulation tissue. Tissue hyperplasia at eitherend of a covered stent is usual, leading to difficultstent removal. For this reason, reduction or preven-tion of the development of tissue hyperplasia isnecessary [23]. Granulation tissue formation usuallyresolves after stent removal [24].
To evaluate the possible interactions betweenstent and urethral endothelium, Ko et al conductedan experimental study in normal canine urethras[24]. They used a polyurethane-covered retrievablenitinol stent. Migration of the stent (partial orcomplete) was reported and therefore confined itsuse. Granulation tissue was observed at both ends ofthe stent in 17 of 20 dogs. The potential migrationand the disruption of the polyurethane membrane

Table 2 – Experimental studies in urethral stenting
Investigators Issue Description
Ko et al [24] Evaluate the use of a retrieval stent and estimate if
granulation tissue resolves after stent removal in
a canine urethra
Technically successful stent placement: all dogs.
Granulation tissue at both ends of stent: 17/20 dogs.
Stent removal failure: 2 cases. Diminished granulation
tissue: 2 wk after stent removal.
Kemppainen et al [18] Examine the suitability of biodegradable polymers
for a urethral stent in rabbits after urethrotomy
A biodegradable self-reinforced poly-L-lactic acid (SR-PLLA)
was implanted in 16 male rabbits. Within 6 mo, minimal
tissue reaction around the stent material. This stent
seems a promising material for a urethral stent with
regard to prevention of restenosis.
Isotalo et al [19] Compare a biodegradable SR-PLLA urethral stent to
the former spiral biodegradable SR-PLLA stent and
stainless steel stent in the rabbit urethra.
Metal stents caused the strongest inflammatory reaction
and induced epithelial hyperplasia and polyposis earlier
than the biodegradable stents.
Shin et al [23] Evaluate a paclitaxel-eluting covered stent in a
canine urethral model.
Local delivery of paclitaxel from covered stents reduced
tissue hyperplasia after stent placement.
Isotalo et al [17] Evaluate the biocompatibility of a caprolactone,
copolymer-coated, SR-PLLA urethral stent by a
rabbit muscle implantation test.
Acute tissue reactions attributable to operative trauma
in all specimens at 1 wk. After 6 mo, chronic
inflammatory changes and foreign-body reactions
only in positive controls (rods made of latex).
Isotalo et al [46] Evaluate the biocompatibility of a bioabsorbable
x-ray–positive SR-PLA 96/4 urethral stent by a
rabbit muscle implantation test.
The stent worked well, with good biocompatibility and less
encrustation than in metal stents. After 6 mo, chronic
inflammatory changes and foreign body reaction only in
positive controls (rods made from latex).
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 880
were also some of its limitations. Because of theseinteractions, the authors concluded that this stentmay be suitable for urethral use only after makingtechnical modifications.
Finally, the influence of the stent on the externalsphincter when applied to treat nearby strictures isan important issue because it can lead to incon-tinence after stenting. Song et al proposed the use ofa covered, retrievable, expandable nitinol stent topreserve continence after stent placement [25].
Table 3 – Basic properties of the ideal ureteral stent [47]
Property Description
Memory Maintenance of its position within the
ureter
Durometer Strength of memory
Elasticity Manipulation of its shape
Tensile strength Crystallisation and cross-linking in the
biomaterials
Elongation capacity Elongation at stent breakage
Biodurability Ability to exist within the body without
degradation of its structure and function
Biocompatibility No significant effect of the stent to the
urothelium
Coefficient of friction Facility of its passage or exchange
Radiopacity Facility of stent visualisation during
fluoroscopy
3. Ureteral MSs
3.1. Types and history of ureteral stents
The aim of ureteral stent implantation is to ensurethe unobstructed drainage of urine from the renalpelvis to the bladder. The ideal stent should be inert,resistant to encrustation, and suitable for long-termuse; in addition, its implantation in the organ shouldnot cause any pain. The basic characteristics thatureteral stents should have to ensure safe and long-term effective urine drainage are summarised inTable 3.
There are four general types of MSs for ureteraluse: the self-expandable, the balloon-expandable,the covered, and the thermoexpandable shape-memory stents. The most commonly used MSs inthe ureter are the self-expanding stents althoughurologists’ interest has recently reoriented to cov-ered stents, in an effort to minimise tissue ingrowth,
which eventually threatens to compromise ureteralpatency. The ability of covered stents to reducetissue ingrowth initially appeared promising butfailed to prove efficacy when used in the ureterdue to a high rate of migration [26]. The overallexperience with the use of ureteral MSs is shown inTable 4.
The Wallstent (Microvasive, Natick, MA) is a self-expandable endoprosthesis and is composed ofbraided biomedical cobalt-based alloy monofila-ments. It is available in a diameter of 7 or 10 mmand in a length of 4, 6, and 8 cm [12].
Memokath 051 (Engineers & Doctors A/S) is athermoexpandable shape-memory stent, composedof a nickel and titanium alloy [27]. It has a unique

Table 4 – Types of metal stent (MS) and experience
Type of MS No. of patients/strictures
Description
Self-expanding and balloon-expandable MS
Lugmayr and Pauer [8] 23/30 Follow-up period: 31 wk (3–75 wk), type of obstruction: malignant. Self-expanding
MS were used in all strictures. Primary patency was 83% after 30 wk. Macrohaematuria
was observed in 1 patient and incrustation in 2 patients.
Pauer and Lugmayr [9] 12/15 Follow-up period: 3–31 wk, type of obstruction: malignant. Self-expanding MSs were
used in all strictures. Haemorrhagia was reported in 1 patient, incrustation in
2 patients, and obstruction distal to the stent in 3 patients.
Pollak et al [48] 8/11 Type of obstruction: malignant and benign. Two of 5 malignant strictures was occluded
within 1 mo and 1/6 benign strictures remained patent in 11 mo.
Lugmayr and Pauer [5] 40/44 Follow-up period: 10.5 mo (1–44 mo), type of obstruction: malignant. Self-expanding
MSs were used in all strictures. 49% needed reintervention and 3 ureters finally had to
be abandoned.
Barbalias et al [4] 12/14 Follow-up period: 9 mo (8–16 mo), type of obstruction: malignant. In 6 patients,
we used self-expanding and in the other 6, balloon-expandable MSs. Second
intervention was necessary in 3 cases due to urothelial hyperplasia, tumour
ingrowth, and local recurrence of primary cancer invading the upper end of the stent.
Barbalias et al [10] 14/14 Follow-up period: 15 mo (9–24 mo), type of obstruction: malignant. Self-expanding
MSs were used in all strictures. Only 2 patients needed further intervention.
Rapp et al [12] 4/6 Follow-up period: 10 mo (7–12 mo), type of obstruction: malignant. Self-expanding
MSs were used in all strictures. No recurrence was observed.
Covered MS
Barbalias et al [26] 16/20 Follow-up period: 8 mos (6–16 mo), type of obstruction: malignant. Thirteen of
16 patients needed second intervention due to stent migration. At the end of
the follow-up period, patency was 100%.
Trueba Arguinarena et al [29] 20/29 Follow-up period: 3 mo for 3 patients, 6 mo for 4 patients, 12 mo for 4 patients,
24 mo for 7 patients; type of obstruction: malignant and benign. In 3 patients,
insertion of second stent was needed because of migration of the first stent.
At the end of the follow-up period, patency was 100%.
Thermoexpandable shape-memory MS
Kulkarni and Bellamy [27] 15/22 Follow-up period: 10.6 mo (2–21 mo), type of obstruction: malignant and benign. In 3/15
stent migration occurred and a shorter Memokath 051 (Engineers & Doctors A/S) was
inserted because of bladder irritation. At the end of the follow-up period, patency
was 100%.
Kulkarni and Bellamy [28] 28/37 Follow-up period: 19.3 mo (3–35 mo), type of obstruction: malignant and benign.
Nine stents in 7 patients were removed, 4 of them requiring no more intervention,
1 led to nephrectomy, 1 to renal failure, and 1 to cystectomy with nephroureterectomy.
Klarskov et al [49] 33/37 Follow-up period: 14 mo (3–30 mo), type of obstruction: malignant and benign.
A total of 22 nonfunctioning stents in approximately 5 mo: 10 of them migrated and
12 malfunctioning. Four stents were occluded by stone after 1–10 mo.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8 81
tight spiral structure that prevents endothelialgrowth. This endoprosthesis softens below 10 8Cand regains its shape when reheated to 50 8C.Because of its thermal shape memory, it is easilyremovable if indicated. Kulkarni and Bellamy usedthis MS in managing both benign and malignantureteral obstruction and showed that this stent hasvery good long-term results in the management ofmalignant stricture or recurrent benign strictures.In addition, no stent migration or infection wasreported [27,28].
Trueba Arguinarena and Fernandez del Busto useda self-expanding polytetrafluoroethylene-coverednitinol stent (Hemobahn Endoprosthesis, W. L. Goreand Associates, Flagstaff, AZ) to treat both benign andmalignant ureteral stenosis [29]. This stent proved tobe safe and effective in managing ureteral stenosis
and showed high resistance to calcification. Hyper-plasia was observed only at the stent ends and only ina few cases and it did not cause obstruction.Migration of the stent occurred in 3 of 20 patients.Long-term follow-up is needed to prove that thiscovered nitinol stent inhibits ureteral hyperplasia.
Recently, Borin et al published data on a womanwith intractable ureteral obstruction due to retro-peritoneal fibrosis after metastatic breast cancer.They used a newly developed all-metal double-pigtailResonance stent (Cook Ireland, Limerick, Ireland),which is constructed of MP35N alloy, a compositeof nonmagnetic nickel-cobalt-chromium-molybde-num. The obstruction had previously resisted theinsertion of two 6F double-pigtail stents. The ureterwas found to be patent in the renal scan at a 4-mofollow-up [30].

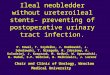
Fig. 1 – Balloon dilation of the stenotic ureteral segment.
Fig. 2 – Excretory urography: patent stented ureteral
segment.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 882
The insertion technique (antegrade or retrograde)has been previously described in detail [4,31]. Briefly,a standard percutaneous nephrostomy, followed bynephropyeloureterography, is done to exactly definethe obstructed segment. The stenosed segment isthen passed with the use of a 0.018-, 0.035-, or 0.038-inch guidewire. Dilatation is performed with the useof a high-pressure balloon catheter (8–10 mmdiameter; Fig. 1). The space for stent passage isthen adequate and the endoprosthesis is insertedover the guidewire. It is placed in such a positionthat the upper end bypasses the stricture by at least3–4 cm while the lower end extends intravesicallyfor 0.5–1 cm from the ureteral orifice. Two or moreMSs can be placed in sequence if necessary, over-lapping by at least 2–3 cm to bridge longerobstructed ureteral segments. If the MS does notexpand to the desired diameter, supplementaryballoon dilatations may be performed.
After the stent placement is completed, a plainradiograph of kidneys-ureters-bladder, ultrasono-graphy, and antegrade nephrotomography areobtained to confirm ureteral patency. The nephros-tomy tube can then be removed. Urinalysis, urineculture, serum creatinine measurement, transab-dominal ultrasonography, and excretory urographyare performed in scheduled order (Fig. 2). Renogra-phy with diethylenetriamine pentaacetic acid(DTPA) can be performed if indicated and uretero-scopy may be necessary to assess and treat eventualencrustations. Virtual endoscopy (VE) has also beenproposed as a noninvasive method to evaluatepatency of the stented ureter [32–34] (Fig. 3).
Since the first stent implantation in the ureter,considerable efforts have been made to improvestentdesign, aiming to facilitate insertion, prevent migra-tion, and permit maximum flow of urine into thebladder. Nevertheless, the ideal stent does not exist.
3.2. The stent influence on the ureter
Urothelial hyperplasia of the stent lumen has beenthe principal problem after the insertion of a metalprothesis in the ureter (Fig. 4). It is a commonphenomenon that may influence patency of thestented ureter and has been verified endoscopically.Thijssen et al have shown that the grade ofurothelial hyperplasia seems to depend on thedegree of the force exerted on the ureteral wall aswell as on the extent of the ureteral overstretchingand the resulting urothelial trauma [35]. Desgrand-champs et al conducted an experimental study inpigs, inserting eight stents. Only one of them wasobserved to be patent 35 d after the insertion [36].Careful insertion of the stent with avoidance ofoverextending the strictured area of the ureteris needed. Urothelial hyperplasia usually regresses4–6 wk after the insertion of the stent, avoiding thenarrowing of the ureteral lumen [4,5,8–10]. Flueck-iger et al reported that during the first 2 wk after thestent insertion reactive swelling of the urothelium,but not hyperplasia, occurs, leading to constrictionof the ureteral lumen [7].

Fig. 3 – Virtual endoscopy. (a) Patent stented ureteral lumen
and (b) stenotic distal part of the endoprosthesis.
Fig. 4 – Excretory urography: urothelial hyperplasia
jeopardising luminal patency.
Fig. 5 – Computed tomography/three-dimensional
reconstruction: trumpet-like configuration adjacent to the
proximal end of the metal stent.
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8 83
The concept of a covered MS was introduced toovercome the problem of hyperplasia growth.Nevertheless, migration of a coated MS may occur,with a frequency of 81.2% observed in one of ourprevious publications [26]. Migration may be cor-rected by coaxial insertion of another prothesis. In aprevious study, we implanted coated MSs in 16patients with malignant ureteral stricture. Thirteenof the 16 showed migration of the endoprosthesis,which caused ureteral obstruction and sub-sequently ipsilateral lumbar pain. The floatingstents were removed cystoscopically from thebladder and bare MSs were then implanted, achiev-ing ureteral patency for a mean follow-up of 8 mo[26]. The high and fast migration rate of the coatedstents into the bladder, the confirmed ‘‘non-anchor-age’’ of the coated stents into the ureteral wall due
to the presence of the coating material, and, finally,the enhanced ureteral peristalsis are consideredstrong arguments against the use of coated stentsfor the management of ureteral strictures.
In our previous publications, we described atrumpet-like configuration of the ureter adjacent tothe upper extremity of the MS, which did not hinderureteral patency [10,26] (Fig. 5). The autopsy findingsin a patient with malignant ureteral stricture, whodied 2 mo after MS implantation, revealed a fibroticreaction in the lumen of the balloon expandable

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 884
stent, probably due to an overextension of theureteral wall causing urothelial trauma [4].
The effect of the MS on ureteral dynamics is anissue of controversy. The presence of foreignmaterial in a peristaltic organ increases the peri-stalsis of the organ aiming to ascertain lumenpatency. Hemikoglu et al suggested that the aper-istaltic segment of the stented ureter in conjunctionwith urothelial peristalsis causes urinary stasis andthus encrustation of the uncovered areas of the MS[37].
Encrustation of the MS is a significant factor thatmay limit the long-term use of the ureteralendoprosthesis. Both the biomaterial and thepatient’s history influence the risk of encrustation.Tunney et al compared the resistance of differentstent biomaterials to encrustation and concludedthat a stent resistant to encrustation should beformed from a biomaterial resistant to bacterialinfection and subsequent biofilm formation [38].Pauer and Lugmayr reported the presence ofencrustations in a small area of Wallstents thatwas not covered by endothelium because it did notembrace the ureteral wall [9].
Experimental studies are being conducted toinvestigate the microscopic urothelial changes thatoccur after stent implantation as well as to develop acovered or coated endoprosthesis that will minimisecomplications (Table 5). Greater understanding of
Table 5 – Experimental studies in ureteral stenting
Investigators Issue
Wrigth et al [50] Placement of self- and balloon-expand
stents (MSs) in normal/stenotic canine
Desgrandchamps et al [36] Placement of self-expanding MS in pig
Liatsikos et al [39] Placement of bare MS and internally o
coated MS in normal pig ureters
Thijssen et al [35] Placement of self-expanding MS in his
normal canine ureters
Antimisiaris et al [51] Simulation of in vivo conditions after t
placement of a liposome-covered MS,
slowly releases dexamethasone
Leveillee et al [52] Bare MS and MS lined with porous bio
polymer in canine ureters
Liatsikos et al [40] Placement of bare MS and paclitaxel d
stent (DES) in normal pig ureters
the interaction between the stent material andurine, with improvements in biomedical engineer-ing, may reduce some of the undesirable eventsassociated with ureteral stenting.
4. Our experience
Our experience with MSs dates back to 1997 whenwe applied self- and balloon-expandable MSs in themanagement of malignant disease in 12 patients. Asecondary intervention was necessary in three ofthem due to urothelial hyperplasia, tumouringrowth, or recurrence of primary tumour in theupper end of stent [4]. Consequently, we applied MSsin the treatment of benign anastomotic stricturesdeveloped after ureteroileal diversion and after-wards in ureteropelvic junction obstruction withencouraging results [10,33].
MSs covered with various biocompatible materi-als have already been used with success in thevascular arena and with better clinical outcomecompared to bare MSs. The aim was to limit theingrowth of intimal hyperplasia along the length ofthe treated arterial segment and thereby to improvepatency as compared to conventional angioplastyand stenting. This observation in the vascularsystem has led urologists to experimentally use thiskind of stent in the urinary tract. Their main
Description
able metal
ureters
Complete occlusion in all stented ureters due
to mucosal hyperplasia in 4–8 wk.
ureters Distal narrowing was observed, due to functional
discrepancy between adynamic stented ureter
and normal underlying ureter.
Urothelial hyperplasia was another feature, but it
did not play an important role in obstructing
porcine ureters.
r externally Coated stents cause minimal tissue ingrowth
but tend to migrate towards bladder, whereas
bare MSs cause less inflammation of
surrounding tissues.
tologically Ureters remained patent. MS was not
incorporated within the ureter wall.
Penetration of epithelium/submucosa between
wire struts and areas of fibrosis in submucosal
layer were observed.
he
which
May be an efficient method of treating ureteral
stent obstruction.
compatible MSs lined with a biocompatible material help
prevent tissue ingrowth, whereas bare MSs
cause ureteral obstruction and hydronephrosis.
rug-eluting Paclitaxel-DES generated less inflammation and
less hyperplasia of surrounding tissues, thus
maintaining ureteral patency.

Fig. 6 – Section of the pig stented ureteral lumen. The fine
epithelial lining is evident covering the metal mesh (a).
The patency of the ureteral lumen is documented
ureteroscopically (b).
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8 85
disadvantage is the high rate of migration, theintense inflammatory reaction of the urotheliumdue to the presence of the lining material, and,finally, the easier infection of this kind of stentcompared to the indigenous grafts. The moreintensive inflammatory reaction generates fibroustissue that is compressed beneath the prosthesis.Still, clinical experience is limited and furtherexperimental as well as clinical investigation isdeemed necessary for their evaluation in the urinarytract.
To find a more appropriate MS and improve ourresults, we conducted an experimental study in pigs,using internally and externally coated MSs, andcompared the results between coated and bareMSs. The follow-up led to controversial outcomes.The bare MSs generated less inflammation of thesurrounding tissues but coated stents had theadvantage of minimal tissue ingrowth. Additionally,coated stents tended to migrate into the bladder,jeopardising ureteral patency [39]. Consequently, we
placed covered MSs in 16 patients with malignantureteral obstruction but unfavourable clinicalresults were observed. No local or systemic infectionwas described, but a high and fast migration rate ofthe MS into the bladder occurred due to ‘‘non-anchorage’’ of the implanted stent into the ureteralwall. This finding was considered to be a strongargument against their use in the ureter [26].
Recently, we published our experience with theuse of a drug-eluting stent (DES) in an experimentalpig model. The results seem promising. DESs areused in the treatment of strictures of coronaryvessels, aiming to minimise the risk of restenosis. Ithas been shown that they reduce inflammation andsmooth muscle proliferation. We thus postulatedthat they may have similar tissue effects in theurinary tract and reduce potential luminal occlusionin the stented ureter. Less inflammation and lesshyperplasia of surrounding tissues were observedwith DESs compared to bare MSs, thereby main-taining ureteral patency (Fig. 6). Still, long-termanimal and human trials are needed to furthervalidate these promising initial results [40].
5. New perspectives
Since the first stent implantation in the field ofurology, efforts have been made to improve stentdesign but still the ideal MS has not been developed.
The use of coated or covered MSs as well asbioabsorbable stents seems promising in minimis-ing stent-related morbidity and improving long-term urine drainage into the bladder [23,40–43].Pharmacologically active agents can be incorporatedonto covered or coated MSs. The agent may beplaced either directly to the polymeric surface of thestent (coated MS) or into the core of the stent’spolymeric structure (DES). In the first case, the agentis pharmacologically active at the surface and canprevent infection or encrustation, whereas in thesecond case, the pharmacologic agent is deliveredlocally in a sustained-release fashion and may havepotential activity at the urothelium.
Experimental studies with the application of DESshave already been initiated in both the urethra andthe ureter. DESs tend to reduce neointimal hyper-plasia by inhibiting vascular smooth muscle cellproliferation and migration. We used a paclitaxel-eluting covered stent in the pig ureter model withpromising results [40]. Shin et al applied a similarstent in a canine urethral model and described lesstissue hyperplasia reaction compared to polyur-ethane-covered stents [23]. DESs are being used inthe treatment of strictures in coronary vessels to

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 886
minimise the risk of restenosis because they reduceinflammation and smooth muscle proliferation. Wetend to believe that the application of DESs will solvemany of the problems of stenting in the urinarytract, but more long-term animal and human trialsare needed to prove their efficacy in this field.However, a retrievable stent design is needed inDESs to make the removal easier [23].
Bioabsorbable stents are still being developed.Little is known about their behaviour in the urinarytract but the first results seem promising. Isotalo et alevaluated the use ofa bioabsorbable SR-PLLA urethralstent combined with optical urethrotomy in thetreatment of recurrent urethral stricture in 22patients [44]. Thirteen recurrent strictures werereported within 15 mo. At 6 mo, the stent was totallyepithelialised in almost all patients and at 12 mo, thestents were totally degraded in all patients. Theirlong-term results showed that in most of the patientswith stricture recurrence at the stent site, therecurrence was discovered during the weakening ofthe stent [45]. The stent seems to collapse, leading topermanent urethral obstruction, if sudden heavycompression happens during the early degradationperiod. The biocompatibility of the bioabsorbablestents has been reported to be good [17,18,46].
6. Conclusions
The application of MSs in the urinary tract hasimproved clinical outcome in the treatment ofurinary tract strictures and is currently thought tobe a useful tool in urology practice. Considerableefforts are being made to optimise stent biomaterial,the coating, and, in general, the ureteral stentdesign. Continuing the research interest seemsto be essential for further clinical improvement,aiming to minimise stent-related morbidity.
References
[1] Milroy EJ, Chapple CR, Cooper JE, et al. A new treatment for
urethral strictures. Lancet 1988;1:1424–7.
[2] Kirby RS, Heard SR, Miller P, et al. Use of the ASI titanium
stent in the management of bladder outflow obstruction
due to benign prostatic hyperplasia. J Urol 1992;148:1195–7.
[3] MacMillan RD, El Harram M. Urethral stents as an alter-
native to sphincterotomy in high pressure bladders. Read
at annual meeting of International Continence Society,
Halifax, Nova Scotia, Canada, September 1992, p. 111
(abstract).
[4] Barbalias GA, Siablis D, Liatsikos EN, et al. Metal stents: a
new treatment of malignant ureteral obstruction. J Urol
1997;158:54–8.
[5] Lugmayr HF, Pauer W. Wallstents for the treatment of
extrinsic malignant ureteral obstruction: midterm
results. Radiology 1996;198:105–8.
[6] VanSonnenberg E, D’Agostino HB, O’Laoide R, et al. Malig-
nant ureteral obstruction: treatment with metal stents—
technique, results, and observations with percutaneous
intraluminal US. Radiology 1994;191:765–8.
[7] Flueckiger F, Lammer J, Klein GE, et al. Malignant ureteral
obstruction: preliminary results of treatment with metal-
lic self-expandable stents. Radiology 1993;186:169–73.
[8] Lugmayr H, Pauer W. Self-expanding metal stents for
palliative treatment of malignant ureteral obstruction.
AJR Am J Radiol 1992;159:1091–4.
[9] Pauer W, Lugmayr H. Metallic Wallstents: a new therapy
for extrinsic ureteral obstruction. J Urol 1992;148:281–4.
[10] Barbalias GA, Liatsikos EN, Kalogeropoulou C, Karnabati-
dis D, Siablis D. Metallic stents in gynecologic cancer: an
approach to treat extrinsic ureteral obstruction. Eur Urol
2000;38:35–40.
[11] Kurzer E, Leveillee RJ. Endoscopic management of ureter-
ointestinal strictures after radical cystectomy. J Endourol
2005;19:677–82.
[12] Rapp DE, Laven BA, Steinberg GD, Gerber GS. Percuta-
neous placement of permanent metal stents for treat-
ment of ureteroenteric anastomotic strictures. J Endourol
2004;18:677–81.
[13] Badlani GH. Role of permanent stents. J Endourol
1997;11:473–5.
[14] Yachia D. The use of urethral stents for the treatment of
urethral strictures. Ann Urol (Paris) 1993;27:245–52.
[15] Milroy EJ, Rickards D. Anatomic limitations of prostatic
urethra in using cylindrical stents. J Endourol 1997;11:455–
8.
[16] Egilmez T, Aridogan IA, Yachia D, Hassin D. Comparison
of nitinol urethral stent infections with indwelling cathe-
ter-associated urinary-tract infections. J Endourol
2006;20:272–7.
[17] Isotalo T, Halasz A, Talja A, Tammela TL, Paasimaa S,
Tormala P. Tissue biocompatibility of a new caprolactone
coated self-reinforced self-expandable poly-L-lactic acid
(SR-PLLA) bioabsorbable urethral stent. J Endourol
1999;13:525–30.
[18] Kemppainen E, Talja M, Riihela M, Pohjonen T, Tormala P,
Alfthan O. A bioresorbable urethral stent. An experimen-
tal study. Urol Res 1993;21:235–8.
[19] Isotalo TM, Nuutine J-P, Vaajanen A, et al. Biocompat-
ibility properties of a new braided biodegradable urethral
stent: a comparison with a biodegradable spiral and a
braided metallic stent in the rabbit urethra. BJU Int
2006;97:856–9.
[20] Van Dijk MM, Mochtar CA, Wijkstra H, Laguna P, de la
Rosette JJMCH. Hourglass-shaped nitinol prostatic stent
in treatment of patients with lower urinary tract symp-
toms due to bladder outlet obstruction. Urology
2005;66:845–9.
[21] van Dijk MM, Mochtar CA, Wijkstra H, Laguna MP, de la
Rosette JJMCH. The bell-shaped nitinol prostatic stent in
the treatment of lower urinary tract symptoms: experi-
ence in 108 patients. Eur Urol 2006;49:353–9.

e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 8 87
[22] Kamata S, Usui N, Kamiyama M, Yoneda A, Tazuke Y, Ooue
T. Application of memory metallic stents to urinary tract
disorders in pediatric patients. J Pediatr Surg 2005;40:E43–5.
[23] Shin JH, Song HY, Choi CG, et al. Tissue hyperplasia:
influence of a paclitaxel-eluting covered stent—prelimin-
ary study in a canine urethral model. Radiology 2005;234:
438–44.
[24] Ko G-Y, Kim G-C, Seo T-S, et al. Covered, retrievable,
expandable urethral nitinol stent: feasibility study in
dogs. Radiology 2002;223:83–90.
[25] Song HY, Park H, Suh TS, et al. Recurrent traumatic
urethral strictures near the external sphincter: treatment
with a covered, retrievable, expandable nitinol stent-
initial results. Radiology 2003;226:433–40.
[26] Barbalias GA, Liatsikos EN, Kalogeropoulou C, et al. Exter-
nally coated ureteral metallic stents: an unfavorable clin-
ical experience. Eur Urol 2002;42:276–80.
[27] Kulkarni RP, Bellamy EA. A new thermo-expandable
shape-memory nickel-titanium alloy stent for the man-
agement of ureteric strictures. BJU Int 1999;83:755–9.
[28] KulkarniR,Bellamy E.Nickel-titaniumshapememoryalloy
Memokath 051 ureteral stent for managing long-term uret-
eral obstruction: 4-year experience. J Urol 2001;166:1750–4.
[29] Trueba Arguinarena FJ, Fernandez Del Busto E. Self-
expanding polytetrafluoroethylene covered nitinol stents
for the treatment of ureteral stenosis: preliminary report.
J Urol 2004;172:620–3.
[30] Borin JF, Melamud O, Clayman RV. Initial experience with
full-length metal stent to relieve malignant ureteral
obstruction. J Endourol 2006;20:300–4.
[31] Liatsikos EN, Kagadis GC, Barbalias GA, Siablis D. Ureteral
metal stents: a tale or a tool? J Endourol 2005;19:934–9.
[32] Siablis D, Kagadis GC, Liatsikos EN, et al. Ureteral metallic
stents: application of virtual endoscopy for ureteral
patency control. Int Urol Nephrol 2003;35:327–30.
[33] Barbalias GA, Liatsikos EN, Kagadis GC, et al. Uretero-
pelvic junction obstruction: an innovative approach com-
bining metallic stenting and virtual endoscopy. J Urol
2002;168:2383–6.
[34] Kagadis GC, Siablis D, Liatsikos EN, Petsas T, Nikiforidis
GC. Virtual endoscopy of the urinary tract. Asian J Androl
2006;8:31–8.
[35] Thijssen AM, Millward SF, Mai KT. Ureteral response to
the placement of metallic stents: an animal model. J Urol
1994;151:268–70.
[36] Desgrandchamps F, Tuchschmid Y, Cochand-Priollet B,
Therin M, Teillac P, Le Duc A. Experimental study of
Wallstent self-expandable metal stent in ureteral implan-
tation. J Endourol 1995;9:477–81.
[37] Hemikoglu B, Men S, Pinar A, et al. Urothelial hyperplasia
complicating use of metal stents in malignant ureteral
obstruction. Eur Radiol 1996;6:675–81.
[38] Tunney MM, Keane PF, Jones DS, Gorman SP. Comparative
assessment of ureteral stent biomaterial encrustation.
Biomaterials 1996;17:1541–6.
[39] Liatsikos EN, Siablis D, Kalogeropoulou C, et al. Coated v
noncoated ureteral metal stents: an experimental model.
J Endourol 2001;15:747–51.
[40] Liatsikos EN, Karnabatidis D, Kagadis GC, et al. Applica-
tion of paclitaxel-eluting metal mesh stents within the
pig ureter: an experimental study. Eur Urol 2007;51:217–
23.
[41] Laaksovirta S, Talja M, Valimaa T, Isotalo T, Tormala P,
Tammela TL. Expansion and bioabsorption of the self-
reinforced lactic and glycolic acid copolymer prostatic
spiral stent. J Urol 2001;166:919–22.
[42] Lumiaho J, Heino A, Pietilainen T, et al. The morphological
in situ effects of a self-reinforced bioabsorbable polyac-
tide (SR-PLA 96) ureteric stent: an experimental study.
J Urol 2000;164:1360–3.
[43] Lumiaho J, Heino A, Tunninen V, et al. New bioabsorbable
polyactide ureteral stent in the treatment of ureteral
lesions: an experimental study. J Endourol 1999;13:107–12.
[44] Isotalo T, Tammela TL, Talja M, Valimaa T, Tormala P. A
bioabsorbable, self-expandable, self-reinforced poly-L-
lactic acid urethral stent for recurrent urethral strictures:
a preliminary report. J Urol 1998;160:2033–6.
[45] Isotalo T, Talja M, Valimaa T, Tormala P, Tammela TL. A
bioabsorbable self-expandable, self-reinforced poly-L-
lactic acid urethral stent for recurrent urethral strictures:
long-term results. J Endourol 2002;16:759–62.
[46] Isotalo T, Alarakkola E, Talja M, Tammela TL, Valimaa T,
Tormala P. Biocompatibility testing of a new bioabsorb-
able X-ray positive SR-PLA 96/4 urethral stent. J Urol
1999;162:1764–7.
[47] Lam JS, Gupta M. Update on ureteral stents. Urology
2004;64:9–15.
[48] Pollak JS, Rosenblatt MM, Egglin TK, Dikey KW, Glickman
M. Treatment of ureteral obstructions with the Wallstent
endoprosthesis: preliminary results. J Vasc Interv Radiol
1995;6:417–25.
[49] Klarskov P, Nordling J, Nielsen JB. Experience with Mem-
okath 051 ureteral stent. Scand J Urol Nephrol
2005;39:169–72.
[50] Wright KC, Dobben RL, Magal C, Ogawa K, Wallace S,
Gianturco C. Occlusive effect of metallic stents on canine
ureters. Cardiovasc Intervent Radiol 1993;16:230–4.
[51] Antimisiaris SG, Siablis D, Liatsikos E, et al. Liposome-
coated metal stents: an in vitro evaluation of controlled-
release modality in the ureter. J Endourol 2000;14:743–7.
[52] Leveillee RJ, Pinchuk L, Wilson GJ, Block NL. A new self-
expanding lined stent-graft in the dog ureter: radiological,
gross, histopathological and scanning electron micro-
scopic findings. J Urol 1998;160:1877–82.
CME questions
Please visit www.eu-acme.org/europeanurologyto answer these CME questions on-line. The CMEcredits will then be attributed automatically.
1. T
he clinical outcome after insertion of a urethralMS may be influenced by:A. Anatomic limitation of the prostatic urethraB. Stent materialC. Insertion techniqueD. None of the above
e a u - e b u u p d a t e s e r i e s 5 ( 2 0 0 7 ) 7 7 – 8 888
2. T
he biodegradation time of the biodegradablematerials used in urology is:A. 1 moB. 13–18 moC. 2–12 moD. None of the above3. T
he main limitation of ureteral MS insertion is:A. MigrationB. Urothelial hyperplasiaC. EncrustationD. None of the above4. C
overed MSs were used:A. To overcome the problem of hyperplasticreactionB. For better anchorage
C. To reduce encrustationD. None of the above
5. D
rug-eluting MSs have been shown to:A. Be toxic on the tissueB. Reduce migrationC. Reduce inflammation and hyperplastic reac-tionD. Increase inflammation and hyperplastic reac-
tion
6. I
nsertion of a ureteral MS:A. Can be performed in an antegrade fashionB. Can be performed in a retrograde fashionC. Combination of A and BD. Can be performed with ureteroscopic gui-dance