Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
JSM Clinical Case Reports
Cite this article: Busch T, Bayram E, Sheplay K, Aziz M (2018) Metaplastic Breast Carcinoma with Metastasis to Small Bowel: A Case Report with Review of the Literature. JSM Clin Case Rep 6(3): 1154.
*Corresponding authorThomas Busch, Department of Pathology, American University of the Caribbean, 11530 Upland Way, Cupertino CA, USA, Tel: (408) 893 - 9407; Email:
Submitted: 30 July 2018
Accepted: 17 August 2018
Published: 20 August 2018
Copyright © 2018 Busch et al.
ISSN: 2373-9819
OPEN ACCESS
Keywords•Metaplastic breast carcinoma; Metastasis; Sarcoma;
Extranodal; Distant; Bowel; Lung; Myoepithelial
Case Report
Metaplastic Breast Carcinoma with Metastasis to Small Bowel: A Case Report with Review of the LiteratureThomas Busch*, Esra Bayram, Kirk Sheplay, and Mohamad AzizDepartment of Pathology, American University of the Caribbean, USA
Abstract
A 69-year-old female with history of breast carcinoma presented with a large non-obstructive soft tissue mass in the small bowel radiologically suggestive of sarcoma. She also had multiple hepatic cystic lesions, bilateral adrenal masses, a blastic iliac bone lesion and a left lung mass consistent with metastases. The lung mass was biopsied and revealed a spindle cell tumor positive for vimentin, smooth muscle actin (SMA) and BCL-2. History of prior breast carcinoma was investigated and it was found to have been reported as metaplastic carcinoma with prominent spindle cell sarcomatous component. Pathological analysis of the small bowel tumor was consistent with multiple metastases. Metaplastic breast carcinoma is more aggressive than ductal carcinoma, with larger tumor size, higher grade, more distant metastases and poor prognosis. These tumors are usually negative for mucin, estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER-2), complicating diagnosis and management. It is important to distinguish metaplastic breast carcinoma and initiate an individualized treatment protocol to avoid a devastating outcome.
ABBREVIATIONSMBC: Metaplastic Breast Carcinoma; IDC: Invasive Ductal
Carcinoma; ER: Estrogen Receptor; PR: Progesterone Receptor; Her-2: Human Epidermal Growth Factor Receptor; SMA: Smooth Muscle Actin
INTRODUCTIONMetaplastic breast carcinoma (MBC) was recognized as
a distinct diagnosis in 2000. It is characterized by admixture of invasive epithelial elements and mesenchymal elements in addition to a transitional state [1,2]. Data reported to the National Cancer Database from 2001 to 2004 identified 892 cases of MBC compared to 255,164 cases of invasive ductal carcinoma (IDC). Statistically significant trends revealed that MBC cases were older, were represented by an increased percentage of African-Americans and Hispanics, had fewer T1 tumors (small tumor size), more N0 tumors (node-negative), more poorly or undifferentiated tumors, and fewer ER positive tumors compared to the IDC group. Additionally, breast conserving surgery was used less often in the MBC group because of larger tumor size, and chemotherapy was used more often because of advanced stage [3]. MBC is considered aggressive compared to other IDC, with larger tumor size, higher grade/stage at presentation and poor prognosis. MBC tends to spread hematogenously and is typically negative for mucin, ER, PR and HER-2, which presents challenges for management and continued surveillance. Here, we report the case of a female patient with a prior history of MBC that presented six years later with metastatic tumors clinically and histomorphologically compatible with spindle cell sarcoma.
CASE PRESENTATIONA 69-year-old female with history of breast carcinoma six
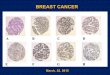
years prior presented with a 5.7 cm non-obstructive soft tissue mass in the small bowel radiologically suggestive of sarcoma. Whole body imaging studies revealed multiple hepatic cystic lesions, bilateral adrenal masses, a blastic iliac bone lesion and many lung masses clinically consistent with metastases. Biospies of the bowel and largest lung mass (6.0 x 5.0 cm) revealed malignant spindle cell tumors with a leiomyosarcoma-like morphology positive for vimentin, SMA and BCL-2 and negative for cytokeratin AE1/AE3, S-100, desmin, CD34, EMA, CD31, CAM 5.2, TTF-1, ER, PR, mammaglobin, GCDFP-15, MOC 31, calretinin, CD117, CK7 and CK20 (Figure 1A, 1B, 1C). History of a 2.5 cm left breast mass was investigated, and it was found to have been reported six years earlier as metaplastic breast carcinoma arising in a background of ER- and PR-positive solid papillary carcinoma. Lumpectomy of the mass was followed by breast radiation. There was no clinical suspicion of lymph node involvement, and the patient declined axillary lymph node dissection. Margins of resection were negative >3 mm. in all directions except superiorly, which was <1 mm. The metaplastic component contained a spectrum of patterns including leiomyosarcoma-like areas with spindle cells, which accounted for >80% of the tumor mass (Figure 1D). Cytokeratin immunostains (CK, CAM5.2, CK7, CK19) were positive only in the papillary epithelium. By reviewing the slides and report, we concluded that the diagnosis was stage 1 metaplastic breast carcinoma, spindle cell type. Though the bowel mass was resected (Figure 1E, 1F, 1G, 1H, 1I)

CentralBringing Excellence in Open Access
Busch et al. (2018)Email:
JSM Clin Case Rep 6(3): 1154 (2018) 2/4
and the patient initiated on a sarcoma chemotherapy protocol, she unfortunately expired from multiple organ failure six months later. Hospital policy required no patient consent for this case report since identification information is completely masked.
DISCUSSION Metaplastic breast carcinoma comprises less than 1% of
invasive breast cancers, and presents with larger tumor size, lower rate of lymph node involvement, and higher percentage of triple-negativity (HR-, PR-, Her-2 negative) [4]. In MBC, it is hypothesized that sarcoma arises de novo from carcinomatous epithelium through reprogramming to a stem-cell-like state, subsequent acquisition of genetic mutations facilitating detachment and overt blood borne dissemination; however a subset may also arise from basal myoepithelium [5].
Our patient presented initially with a breast mass suspicious for IDC, which was later diagnosed as MBC. Analysis of core biopsies revealed a spectrum of solid papillary carcinoma, fibrohistiocytic-like areas, liposarcoma-like areas, and leiomyosarcoma-like areas in addition to areas of overlapping
features. The expert pathologist noted his impression that the spindle cell component likely arose from myoepithelial cells in addition to the possibility of ductal cell origin. There have been a few reports indicating that malignant basal-like tumors of the breast metastasize regionally and distantly 50% of the time [6]. Six years after initial treatment for breast malignancy, our patient presented with a large intestinal lesion and no sign of primary neoplasm elsewhere in the abdomen. Small intestinal metastasis of primary breast cancer is estimated by the World Health Organization to occur in only 1.7% of cases. Pathological analysis of the tumor resected from the small bowel and a large lung nodule showed a predominantly leiomyosarcomaous morphology with positivity for SMA and Bcl-2 but negative for a cytokeratin cocktail and CD34, identifying these tumors as pure sarcoma. Primary leiomyoscarcoma of the small intestine is extremely rare. Many benign and malignant spindle cell tumors strongly co-express Bcl-2 and CD34, however the Bcl-2+/CD34- phenotype observed in our patient excludes gastrointestinal stromal tumor (GIST) and metastatic malignant phyllode [7]. Considered together, these findings supported a diagnosis of late-manifesting metastatic sarcoma originating from MBC.
Figure 1 Pathological Analysis of Tumors in Breast, Small Bowel, and Lung. A: Breast biopsy, original tumor shows intermediately-differentiated, invasive epithelial and mesenchymal elements, hematoxylin & eosin at x10 magnificationB: Breast biopsy, original tumor shows cigar-shaped spindle cell morphology, H&E x 50 magnificationsC: Breast biopsy, original tumor shows pleomorphic and hyperchromatic nuclei, and mitoses (indicated by arrows), H&E x100 magnificationD: Small bowel tumor with ink present at excisional margins, gross specimenE, F: Small bowel biopsy shows malignant spindle cells, H&E x50 and x100 magnification respectivelyG: Lung biopsy immunohistochemistry shows strong Vimentin positivity, x10 magnificationH: Lung biopsy immunohistochemistry of shows focal Bcl-2 positivity, x 50 magnificationsI: Lung biopsy shows malignant spindle cells, H&E x100 magnification

CentralBringing Excellence in Open Access
Busch et al. (2018)Email:
JSM Clin Case Rep 6(3): 1154 (2018) 3/4
All tumors from the breast, bowel, and lung were identical histomorphologically and immunohistochemically.
The clinical timeline of events and the morphological similarities discovered upon review of the pathological analysis suggest a remarkable natural history of disease in this patient. The late, distant metastases we observed illustrate the unpredictable and potentially aggressive behavior of MBC. Comparative tumor genome analysis and fusion-gene expression profiling at the time of discovery would lend increased support for our conclusion by resolving specific tumorigenic molecular mechanisms that facilitated dissemination. GATA3 has arisen as a sensitive tissue marker of breast or bladder origin, which can be useful when considering a diagnosis of metastatic MBC where mammaglobin and luminal markers have been lost [8-10]. Unfortunately, such studies which are contemporary methods were not available at the time of presentation, and the tissue and patient are not available for such further confirming analysis. Notably, GATA3 expression in the purely sarcomatous extra-mammary tumors in our patient is expected to be inconclusive.
Treatment of metaplastic breast carcinoma can be very challenging. It has historically been managed similarly to epithelial malignancy with TNM staging and surgical resection with optional adjunctive radiotherapy and chemotherapy [11,12]. Hormone therapies have a very minimal role since the tumor is typically ER-/PR-. In our patient, the breast tumor was predominantly sarcomatous (>80% tumor mass), and in hindsight we wondered if early initiation of sarcoma-specific therapy would have provided benefits beyond mastectomy with confirmation of cancer-free lymph nodes. Retrospective studies suggest that breast sarcoma behaves comparably to other soft tissue sarcomas, therefore proposed treatment regimens have been extrapolated from meta-analyses which detect a moderate survival advantage (11% increase in 10-year overall survival compared to resection alone) of short-course intra-arterial or intravenous infusion of doxorubicin +/- iphosphamide; however, marginal efficacy and significant morbidity highlights the need for development of better pharmacologic options [13-16]. Due to the paucity of reports and lack of prospective clinical trials, there is currently no consensus on the optimal treatment protocol. Thus, specialists have utilized highly individualized strategies based on performance of the patient as well as expertise and preferences of the providers. Ideally, management should be conducted by a multidisciplinary team at a major cancer center with enrollment in a clinical trial. The best evidence from case-control studies is that the most important factor impacting overall and disease-free survival is resection with negative margins, preferably greater than 1 cm. in all dimensions (if muscle or fat, 5 mm is sufficient when there is an unbroken facial barrier) confirmed by pathological analysis; since frozen section may be falsely negative, delayed closure may be required while definitive confirmation is obtained [4,17-19]. Metaplastic breast carcinoma with a significant sarcomatous component may be equated to a high grade primary breast sarcoma for staging: when tumor size is greater than 5 cm, the risk of distant metastasis to lungs, liver, and bone by the hematogenous route is greatly increased. Perioperative radiotherapy should be considered for shrinking the tumor before resection and suppressing any micro-metastases after resection [20]. Fluorodeoxyglucose (FDG)-PET
or dynamic contrast-enhanced magnetic resonance imaging (MRI) have been proposed for following treatment response, but this has not been validated by clinical trials.
It is our hope that this report raises awareness of what remains an unmet need in breast cancer management and that continued investigation drives further development of efficacious and safe treatments for improving patient outcomes.
REFERENCES1. Lakhani SR, International Agency for Research on Cancer. World
Health Organization. WHO Classification of Tumours of the Breast.
2. Catroppo JF, Lara JF. Metastatic metaplastic carcinoma of the breast (MCB): an uncharacteristic pattern of presentation with clinicopathologic correlation. Diagn Cytopathol. 2001; 25: 285-291.
3. Pezzi CM, Patel-Parekh L, Cole K, Franko J, Klimberg VS, Bland K. Characteristics and treatment of metaplastic breast cancer: analysis of 892 cases from the National Cancer Data Base. Ann Surg Oncol. 2007; 14: 166-173.
4. Song Y, Liu X, Zhang G, Hongtao Song, Yanlv Ren, Xiaoguang He, et al. Unique clinicopathological features of metaplastic breast carcinoma compared with invasive ductal carcinoma and poor prognostic indicators. World J Surg Oncol. 2013; 11: 129.
5. Zhang Y, Toy KA, Kleer CG. Metaplastic breast carcinomas are enriched in markers of tumor-initiating cells and epithelial to mesenchymal transition. Mod Pathol. 2012; 25: 178-184.
6. Trepp R, Padberg BC, Varga Z, Cathomas R, Inauen R, Reinhart WH. Extensive extranodal metastases of basal-like breast cancer with predominant myoepithelial spindle cell differentiation. Pathol Res Pract. 2010; 206: 334-337.
7. Gustafsson BI, Siddique L, Chan A, Dong M, Drozdov I, Kidd M, et al. Uncommon cancers of the small intestine, appendix and colon: an analysis of SEER 1973-2004, and current diagnosis and therapy. Int J Oncol. 2008; 33: 1121-1131.
8. Gown AM, Fulton RS, Kandalaft PL. Markers of metastatic carcinoma of breast origin. Histopathology. 2016; 68: 86-95.
9. Cimino-Mathews A, Subhawong AP, Illei PB, Sharma R, Halushka MK, Vang R, et al. GATA3 expression in breast carcinoma: utility in triple-negative, sarcomatoid, and metastatic carcinomas. Hum Pathol. 2013; 44: 1341-1349.
10. Cimino-Mathews A, Verma S, Figueroa-Magalhaes MC, et al. A Clinicopathologic Analysis of 45 Patients with Metaplastic Breast Carcinoma. Am J Clin Pathol. 2016; 145: 365-372.
11. Ünal B, Erdogan G, Karaveli FS. Step by step approach to rare breast lesions containing spindle cells. Springerplus. 2015; 4: 678.
12. Rakha EA, Chan S. Metastatic triple-negative breast cancer. Clin Oncol (R Coll Radiol). 2011; 587-600.
13. Gultekin M, Eren G, Babacan T, Yildiz F, Altundag K, Guler N, et al. Metaplastic breast carcinoma: a heterogeneous disease. Asian Pac J Cancer Prev. 2014; 15: 2851-2586.
14. Shah DR, Tseng WH, Martinez SR. Treatment options for metaplastic breast cancer. ISRN Oncol. 2012; 2012: 706162.
15. Martin-Liberal J. Leiomyosarcoma: Principles of management. Intractable rare Dis Res. 2013; 2: 127-129.
16. Hudis CA, Gianni L. Triple-negative breast cancer: an unmet medical need. Oncologist. 2011; 16: 1-11.
17. Pandey M, Mathew A, Abraham EK, Rajan B. Primary sarcoma of the breast. J Surg Oncol. 2004; 87: 121-125.

CentralBringing Excellence in Open Access
Busch et al. (2018)Email:
JSM Clin Case Rep 6(3): 1154 (2018) 4/4
Busch T, Bayram E, Sheplay K, Aziz M (2018) Metaplastic Breast Carcinoma with Metastasis to Small Bowel: A Case Report with Review of the Literature. JSM Clin Case Rep 6(3): 1154.
Cite this article
18. Zelek L, Llombart-Cussac A, Terrier P, Pivot X, Guinebretiere JM, Le Pechoux C, et al. Prognostic factors in primary breast sarcomas: a series of patients with long-term follow-up. J Clin Oncol. 2003; 21: 2583-2588.
19. Shabahang M, Franceschi D, Sundaram M, Castillo MH, Moffat FL,
Frank DS, et al. Surgical management of primary breast sarcoma. Am Surg. 2002; 68: 673-677.
20. Yin M, Mackley HB, Drabick JJ, Harvey HA. Primary female breast sarcoma: clinicopathological features, treatment and prognosis. Sci Rep. 2016; 6: 31497.