Embed Size (px)
Citation preview

1
Metastatic Breast Cancer Updated June 2017 by Dr. Veitch (Tom Baker Cancer Centre) Reviewed by Dr. Eitan Amir (Staff Medical Oncologist, University of Toronto) DISCLAIMER: The following are study notes compiled by the above PGY-5 medical oncology residents and reviewed by a staff medical oncologist. They reflect what we feel is relevant knowledge for graduating medical oncology residents preparing for their final examination. The information has not been surveyed or ratified by the Royal College. Diagnosis and Workup ASCO 2015 guideline: Use of Biomarkers to Guide Decisions on Systemic Therapy for Women with Metastatic Breast Cancer
- Patients with accessible, newly diagnosed metastases from primary breast cancer should be offered biopsy for confirmation of disease process and testing of ER, PR, and HER2 status. They should also be informed that if discordances are found, evidence is lacking to determine whether outcomes are better with treatment regimens based on receptor status in the metastases or the primary tumor.
- With discordance of results between primary and metastatic tissues, the Panel consensus is to preferentially use the ER, PR, and HER2 status from the metastasis to direct therapy, if supported by the clinical scenario and the patient's goals for care.
- Recommendations for tissue biomarkers: There is no evidence at this time that changing therapy based solely on biomarker results beyond ER, PR, and HER2 improves health outcomes, quality of life, or cost effectiveness.
- Recommendations for circulating tumor markers: There is no evidence at this time that changing therapy based solely on circulating biomarker results improves health outcomes, quality of life, or cost effectiveness.
- CEA, CA 15-3, and CA 27-29 may be used as adjunctive assessments to contribute to decisions regarding therapy for metastatic breast cancer. Data are insufficient to recommend use of CEA, CA 15-3, and CA 27-29 alone for monitoring response to treatment.
Treatment ** Principles of treatment (ASCO 2016)
- Sequential hormone therapy is the preferential treatment for most women with HR-positive MBC. Except in cases of immediately life-threatening disease, hormone therapy, alone or in combination, should be used as initial treatment. Patients whose tumors express any level of hormone receptors should be offered hormone therapy. Treatment recommendations should be based on type of adjuvant treatment, disease-free interval, and organ function.
- Tumor markers should not be the sole criteria for determining tumor progression; use of additional biomarkers remains experimental. Assessment of menopausal status is critical; ovarian suppression or ablation should be included in premenopausal women.
- For postmenopausal women, aromatase inhibitors (AIs) are the preferred first-line endocrine therapy, with or without the cyclin-dependent kinase inhibitor palbociclib. As second-line therapy, fulvestrant should be administered at 500 mg with a loading schedule and may be administered with palbociclib.
- The mammalian target of rapamycin inhibitor everolimus may be administered with exemestane to postmenopausal women with MBC whose disease progresses while receiving nonsteroidal AIs. Among patients with HR-positive, human epidermal growth factor receptor 2–positive MBC, human epidermal growth factor receptor 2–targeted therapy plus an AI can be effective for those who are not chemotherapy candidates.
- Patients with brain metastases should receive appropriate local therapy and systemic therapy, if indicated.

2
Ø Local therapies include surgery, whole-brain radiotherapy, and stereotactic radiosurgery. Ø Treatments depend on factors such as patient prognosis, presence of symptoms,
resectability, number and size of metastases, prior therapy, and whether metastases are diffuse.
Ø Other options include systemic therapy, best supportive care, enrollment onto a clinical trial, and/or palliative care.
Ø Clinicians should not perform routine magnetic resonance imaging (MRI) to screen for brain metastases, but rather should have a low threshold for MRI of the brain because of the high incidence of brain metastases among patients with HER2-positive advanced breast cancer.
I. Chemotherapy Overview
• Endocrine Rx indications: HR+, long disease remission, bony mets / aSx visceral mets • Chemo Indications: ER/PR neg, endocrine resistant dz, rapidly progressive, symptomatic
visceral crisis Response rates of chemotherapy regimens (monotherapy): First line (%) Second line (%) Anthracyclines 35-50 30 Taxanes 30-50 20-60 Nab-paclitaxel 30-70 Capecitabine 15-35 20-30 Gemcitabine 15-40 15-40 Vinorelbine 25-50 20-35 Response rates of chemotherapy regimens (combination therapy): generally 50-70% Anthracyclines
• Anthracycline monotherapy: o Response rates (RR) are 35-50% in pts who are anthracycline-naive or who
develop metastases >12 months after anthracycline-based adjuvant therapy o Efficacy in women with an anthracycline-free interval <12 months is uncertain
• Multidrug anthracycline-containing regimens o Eg. CAF (cyclo 500mg/m2, doxo 50mg/m2, 5-FU 500mg/m2 all on d1 q 21d), FEC
(5’FU 500mg/m2, epi 60mg/m2, cyclo 500mg/m2 all on d1 q 28d) o RR 20-60% in previously untreated patients with MBC o Generally more active but also more toxic than single agent regimen /
monotherapy • With the taxane containing regimens, it is very rare to use doxorubicin >450mg/m2 or epirubicin >900mg/m2 lifetime cumulative dose.
Taxanes
• Hypersensitivity reactions: o Paclitaxel –due to Cremophor solvent; risk decreased by pre-treatment with dex
and anti-histamines, and slowing infusion o Docetaxel –still occur albeit less common o Nab-paclitaxel – nano-particle albumin-bound formulation of paclitaxel; lower
incidence of reactions and no steroid pre-meds required • Toxicity profile:
o Paclitaxel § Alopecia (~ 100% esp. with 3-weekly regimen, lower with weekly
treatment) § Grade 3 / 4 myalgias and arthralgias (5-15%)
3
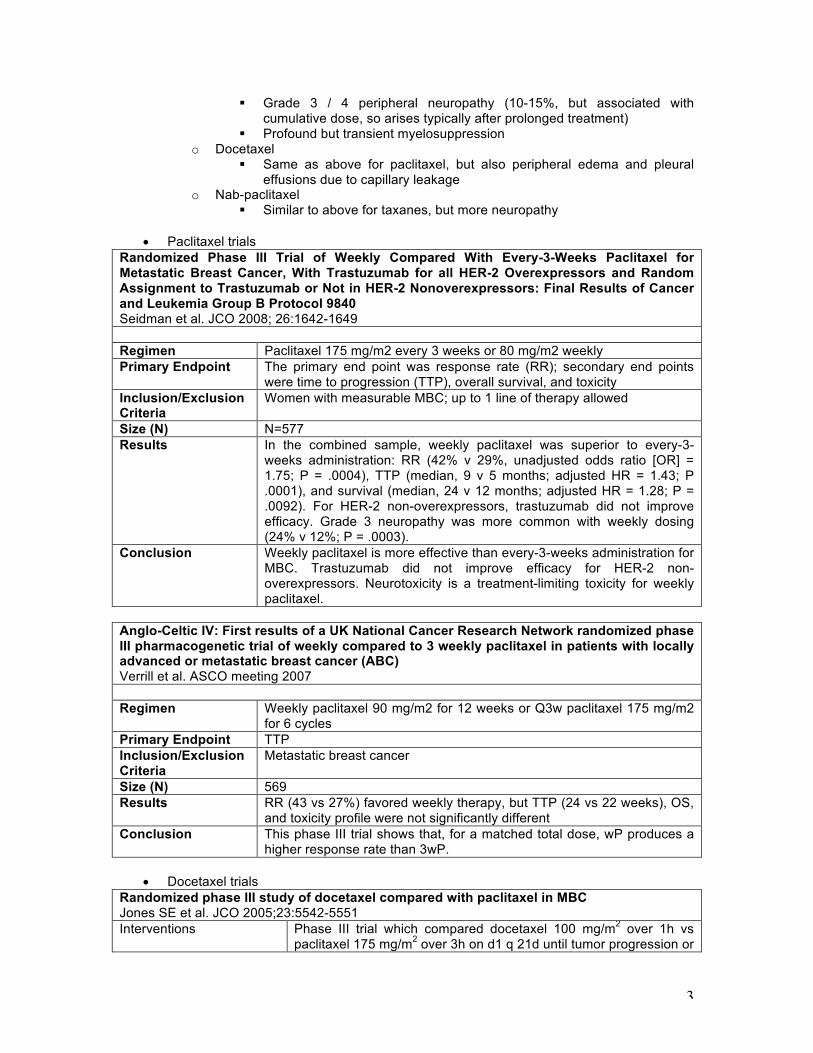
§ Grade 3 / 4 peripheral neuropathy (10-15%, but associated with cumulative dose, so arises typically after prolonged treatment)
§ Profound but transient myelosuppression o Docetaxel
§ Same as above for paclitaxel, but also peripheral edema and pleural effusions due to capillary leakage
o Nab-paclitaxel § Similar to above for taxanes, but more neuropathy
• Paclitaxel trials
Randomized Phase III Trial of Weekly Compared With Every-3-Weeks Paclitaxel for Metastatic Breast Cancer, With Trastuzumab for all HER-2 Overexpressors and Random Assignment to Trastuzumab or Not in HER-2 Nonoverexpressors: Final Results of Cancer and Leukemia Group B Protocol 9840 Seidman et al. JCO 2008; 26:1642-1649 Regimen Paclitaxel 175 mg/m2 every 3 weeks or 80 mg/m2 weekly Primary Endpoint The primary end point was response rate (RR); secondary end points
were time to progression (TTP), overall survival, and toxicity Inclusion/Exclusion Criteria
Women with measurable MBC; up to 1 line of therapy allowed
Size (N) N=577 Results In the combined sample, weekly paclitaxel was superior to every-3-
weeks administration: RR (42% v 29%, unadjusted odds ratio [OR] = 1.75; P = .0004), TTP (median, 9 v 5 months; adjusted HR = 1.43; P .0001), and survival (median, 24 v 12 months; adjusted HR = 1.28; P = .0092). For HER-2 non-overexpressors, trastuzumab did not improve efficacy. Grade 3 neuropathy was more common with weekly dosing (24% v 12%; P = .0003).
Conclusion Weekly paclitaxel is more effective than every-3-weeks administration for MBC. Trastuzumab did not improve efficacy for HER-2 non-overexpressors. Neurotoxicity is a treatment-limiting toxicity for weekly paclitaxel.
Anglo-Celtic IV: First results of a UK National Cancer Research Network randomized phase III pharmacogenetic trial of weekly compared to 3 weekly paclitaxel in patients with locally advanced or metastatic breast cancer (ABC) Verrill et al. ASCO meeting 2007 Regimen Weekly paclitaxel 90 mg/m2 for 12 weeks or Q3w paclitaxel 175 mg/m2
for 6 cycles Primary Endpoint TTP Inclusion/Exclusion Criteria
Metastatic breast cancer
Size (N) 569 Results RR (43 vs 27%) favored weekly therapy, but TTP (24 vs 22 weeks), OS,
and toxicity profile were not significantly different Conclusion This phase III trial shows that, for a matched total dose, wP produces a
higher response rate than 3wP.
• Docetaxel trials Randomized phase III study of docetaxel compared with paclitaxel in MBC Jones SE et al. JCO 2005;23:5542-5551 Interventions Phase III trial which compared docetaxel 100 mg/m2 over 1h vs
paclitaxel 175 mg/m2 over 3h on d1 q 21d until tumor progression or
4
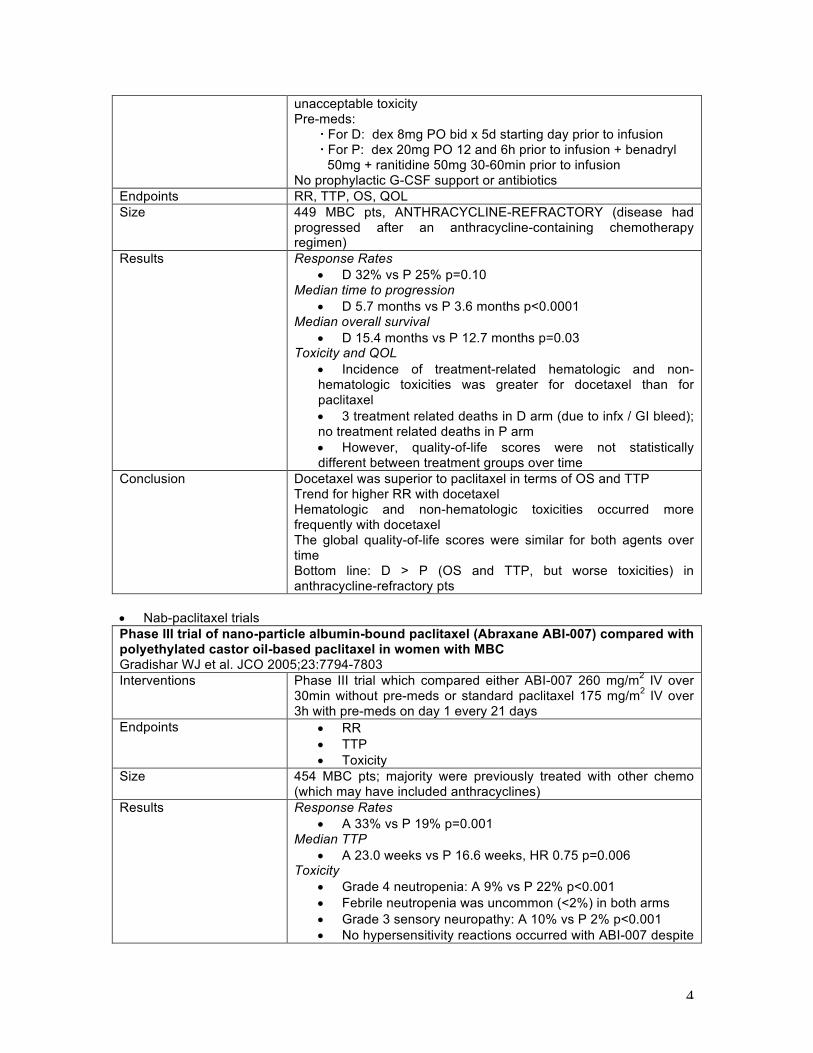
unacceptable toxicity Pre-meds: For D: dex 8mg PO bid x 5d starting day prior to infusion For P: dex 20mg PO 12 and 6h prior to infusion + benadryl 50mg + ranitidine 50mg 30-60min prior to infusion No prophylactic G-CSF support or antibiotics
Endpoints RR, TTP, OS, QOL Size 449 MBC pts, ANTHRACYCLINE-REFRACTORY (disease had
progressed after an anthracycline-containing chemotherapy regimen)
Results Response Rates • D 32% vs P 25% p=0.10
Median time to progression • D 5.7 months vs P 3.6 months p<0.0001
Median overall survival • D 15.4 months vs P 12.7 months p=0.03
Toxicity and QOL • Incidence of treatment-related hematologic and non-hematologic toxicities was greater for docetaxel than for paclitaxel • 3 treatment related deaths in D arm (due to infx / GI bleed); no treatment related deaths in P arm • However, quality-of-life scores were not statistically different between treatment groups over time
Conclusion Docetaxel was superior to paclitaxel in terms of OS and TTP Trend for higher RR with docetaxel Hematologic and non-hematologic toxicities occurred more frequently with docetaxel The global quality-of-life scores were similar for both agents over time Bottom line: D > P (OS and TTP, but worse toxicities) in anthracycline-refractory pts
• Nab-paclitaxel trials Phase III trial of nano-particle albumin-bound paclitaxel (Abraxane ABI-007) compared with polyethylated castor oil-based paclitaxel in women with MBC Gradishar WJ et al. JCO 2005;23:7794-7803 Interventions Phase III trial which compared either ABI-007 260 mg/m2 IV over
30min without pre-meds or standard paclitaxel 175 mg/m2 IV over 3h with pre-meds on day 1 every 21 days
Endpoints • RR • TTP • Toxicity
Size 454 MBC pts; majority were previously treated with other chemo (which may have included anthracyclines)
Results Response Rates • A 33% vs P 19% p=0.001
Median TTP • A 23.0 weeks vs P 16.6 weeks, HR 0.75 p=0.006
Toxicity • Grade 4 neutropenia: A 9% vs P 22% p<0.001 • Febrile neutropenia was uncommon (<2%) in both arms • Grade 3 sensory neuropathy: A 10% vs P 2% p<0.001 • No hypersensitivity reactions occurred with ABI-007 despite

5
absence of pre-meds and shorter administration time (30min) Conclusion ABI-007 demonstrated better RR and TTP, and a favorable safety
profile compared with standard paclitaxel The improved therapeutic index and elimination of corticosteroid pre-meds required for solvent-based taxanes make the novel albumin-bound paclitaxel ABI-007 an important advance in the treatment of MBC Bottom line: ABI-007 > P (RR, TTP, toxicity, convenience)
- However, given the three-arm trial comparing paclitaxel, nab-paclitaxel and ixabepilone (see below), there is no evidence that nab-paclitaxel is particularly more effective in terms of survival compared with weekly paclitaxel.
• Taxane combination trials Phase III trial of doxorubicin, paclitaxel, and combination of doxorubicin and paclitaxel as front-line chemotherapy for MBC: ECOG 1193 Intergroup Trial Sledge GW et al. JCO 2003;21:588-592 Regimen Doxorubicin 60 mg/m2, paclitaxel 175 mg/m2, or combination of
doxorubicin and paclitaxel (AT, 50 mg/m2 and 150 mg/m2, plus GCSF 5 mg/kg) as 1st-line therapy Crossed over to the other agent at progression if monotherapy
Primary Endpoint TTF, OS Inclusion/Exclusion Criteria
First-line therapy for metastatic breast cancer, anthracycline naïve
Size (N) N=739 Results Response rates
• Doxo 36% vs Paclitaxel 34% vs AT 47% • P =0.84 for Doxo vs Paclitaxel, P =0.007 for Doxo vs AT, P =0.004 for Paclitaxel vs AT)
Median time to treatment failure • Doxo 5.8 months, Paclitaxel 6.0 months, AT 8.0 months • P =0.68 for Doxo vs Paclitaxel, P =0.003 for Doxo vs AT, P =0.009 for Paclitaxel vs AT)
Median overall survival • Doxo 18.9 months, Paclitaxel 22.2 months, AT 22.0 months • All P = non-significant • Responses were seen in 20% of pts crossing from doxorubicin à paclitaxel and 22% of pts crossing from paclitaxel à doxorubicin (P = non-significant)
QOL • Changes in global quality-of-life measurements from on-study to
week 16 of treatment were similar in all three groups Conclusion Doxorubicin and paclitaxel have equivalent activity in anthracycline-naive
MBC pts The combination of AT results in superior overall RR and TTF However, combination AT did not improve either OS or QOL compared to sequential single-agent therapy Bottom line: Doxo = paclitaxel < AT (RR, TTF) in anthracycline naïve pts, but OS and QOL not different
Other comments Predictors of poor OS: TN, short relapse interval (1-24mos), >3sites of disease, prior therapy.
Doxorubicin and paclitaxel vs doxorubicin and cyclophosphamide as first-line chemo in MBC: EORTC 10961 Multicenter Phase III Trial Biganzoli L et al. JCO 2002;20:3114-3121
6
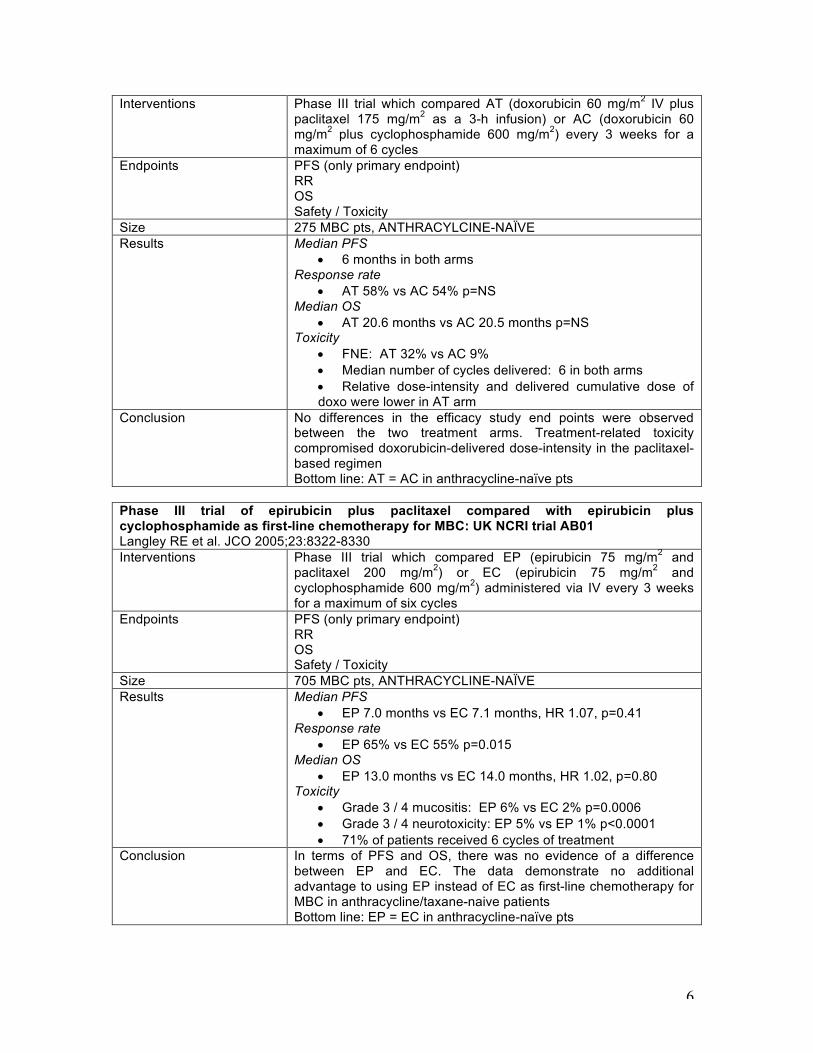
Interventions Phase III trial which compared AT (doxorubicin 60 mg/m2 IV plus paclitaxel 175 mg/m2 as a 3-h infusion) or AC (doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2) every 3 weeks for a maximum of 6 cycles
Endpoints PFS (only primary endpoint) RR OS Safety / Toxicity
Size 275 MBC pts, ANTHRACYLCINE-NAÏVE Results Median PFS
• 6 months in both arms Response rate
• AT 58% vs AC 54% p=NS Median OS
• AT 20.6 months vs AC 20.5 months p=NS Toxicity
• FNE: AT 32% vs AC 9% • Median number of cycles delivered: 6 in both arms • Relative dose-intensity and delivered cumulative dose of doxo were lower in AT arm
Conclusion No differences in the efficacy study end points were observed between the two treatment arms. Treatment-related toxicity compromised doxorubicin-delivered dose-intensity in the paclitaxel-based regimen Bottom line: AT = AC in anthracycline-naïve pts
Phase III trial of epirubicin plus paclitaxel compared with epirubicin plus cyclophosphamide as first-line chemotherapy for MBC: UK NCRI trial AB01 Langley RE et al. JCO 2005;23:8322-8330 Interventions Phase III trial which compared EP (epirubicin 75 mg/m2 and
paclitaxel 200 mg/m2) or EC (epirubicin 75 mg/m2 and cyclophosphamide 600 mg/m2) administered via IV every 3 weeks for a maximum of six cycles
Endpoints PFS (only primary endpoint) RR OS Safety / Toxicity
Size 705 MBC pts, ANTHRACYCLINE-NAÏVE Results Median PFS
• EP 7.0 months vs EC 7.1 months, HR 1.07, p=0.41 Response rate
• EP 65% vs EC 55% p=0.015 Median OS
• EP 13.0 months vs EC 14.0 months, HR 1.02, p=0.80 Toxicity
• Grade 3 / 4 mucositis: EP 6% vs EC 2% p=0.0006 • Grade 3 / 4 neurotoxicity: EP 5% vs EP 1% p<0.0001 • 71% of patients received 6 cycles of treatment
Conclusion In terms of PFS and OS, there was no evidence of a difference between EP and EC. The data demonstrate no additional advantage to using EP instead of EC as first-line chemotherapy for MBC in anthracycline/taxane-naive patients Bottom line: EP = EC in anthracycline-naïve pts
7
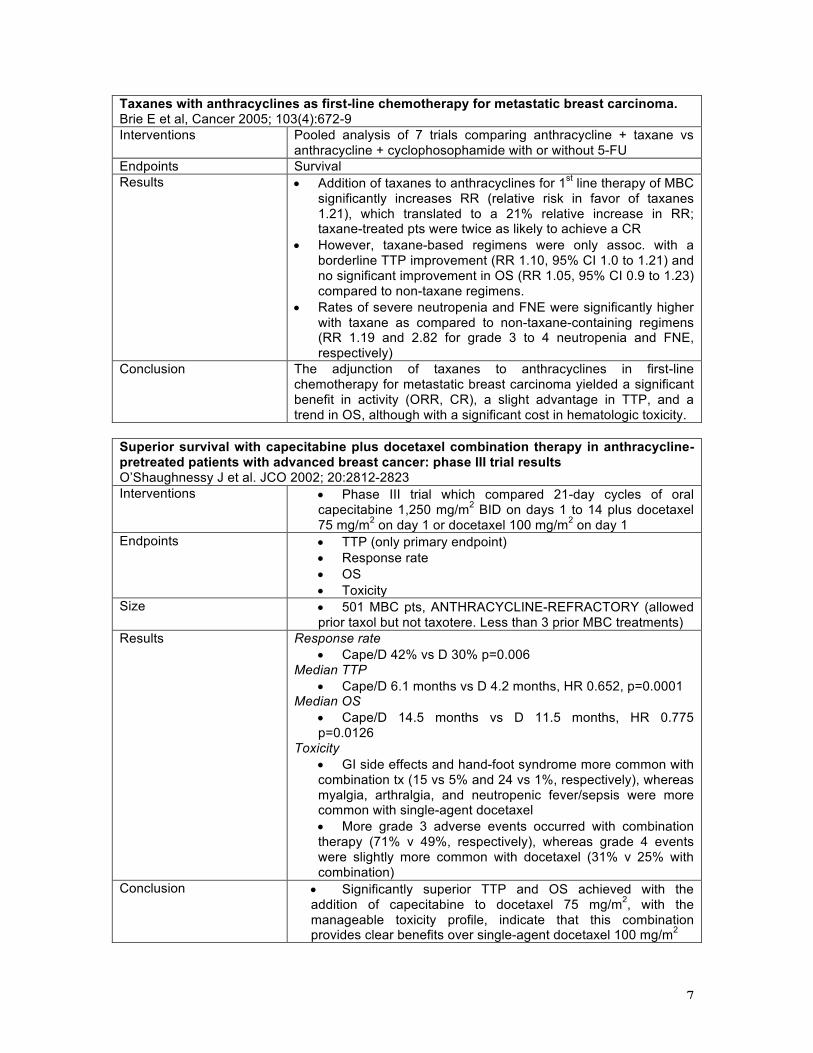
Taxanes with anthracyclines as first-line chemotherapy for metastatic breast carcinoma. Brie E et al, Cancer 2005; 103(4):672-9 Interventions Pooled analysis of 7 trials comparing anthracycline + taxane vs
anthracycline + cyclophosophamide with or without 5-FU Endpoints Survival Results • Addition of taxanes to anthracyclines for 1st line therapy of MBC
significantly increases RR (relative risk in favor of taxanes 1.21), which translated to a 21% relative increase in RR; taxane-treated pts were twice as likely to achieve a CR
• However, taxane-based regimens were only assoc. with a borderline TTP improvement (RR 1.10, 95% CI 1.0 to 1.21) and no significant improvement in OS (RR 1.05, 95% CI 0.9 to 1.23) compared to non-taxane regimens.
• Rates of severe neutropenia and FNE were significantly higher with taxane as compared to non-taxane-containing regimens (RR 1.19 and 2.82 for grade 3 to 4 neutropenia and FNE, respectively)
Conclusion The adjunction of taxanes to anthracyclines in first-line chemotherapy for metastatic breast carcinoma yielded a significant benefit in activity (ORR, CR), a slight advantage in TTP, and a trend in OS, although with a significant cost in hematologic toxicity.
Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: phase III trial results O’Shaughnessy J et al. JCO 2002; 20:2812-2823 Interventions • Phase III trial which compared 21-day cycles of oral
capecitabine 1,250 mg/m2 BID on days 1 to 14 plus docetaxel 75 mg/m2 on day 1 or docetaxel 100 mg/m2 on day 1
Endpoints • TTP (only primary endpoint) • Response rate • OS • Toxicity
Size • 501 MBC pts, ANTHRACYCLINE-REFRACTORY (allowed prior taxol but not taxotere. Less than 3 prior MBC treatments)
Results Response rate • Cape/D 42% vs D 30% p=0.006
Median TTP • Cape/D 6.1 months vs D 4.2 months, HR 0.652, p=0.0001
Median OS • Cape/D 14.5 months vs D 11.5 months, HR 0.775 p=0.0126
Toxicity • GI side effects and hand-foot syndrome more common with combination tx (15 vs 5% and 24 vs 1%, respectively), whereas myalgia, arthralgia, and neutropenic fever/sepsis were more common with single-agent docetaxel • More grade 3 adverse events occurred with combination therapy (71% v 49%, respectively), whereas grade 4 events were slightly more common with docetaxel (31% v 25% with combination)
Conclusion • Significantly superior TTP and OS achieved with the addition of capecitabine to docetaxel 75 mg/m2, with the manageable toxicity profile, indicate that this combination provides clear benefits over single-agent docetaxel 100 mg/m2
8
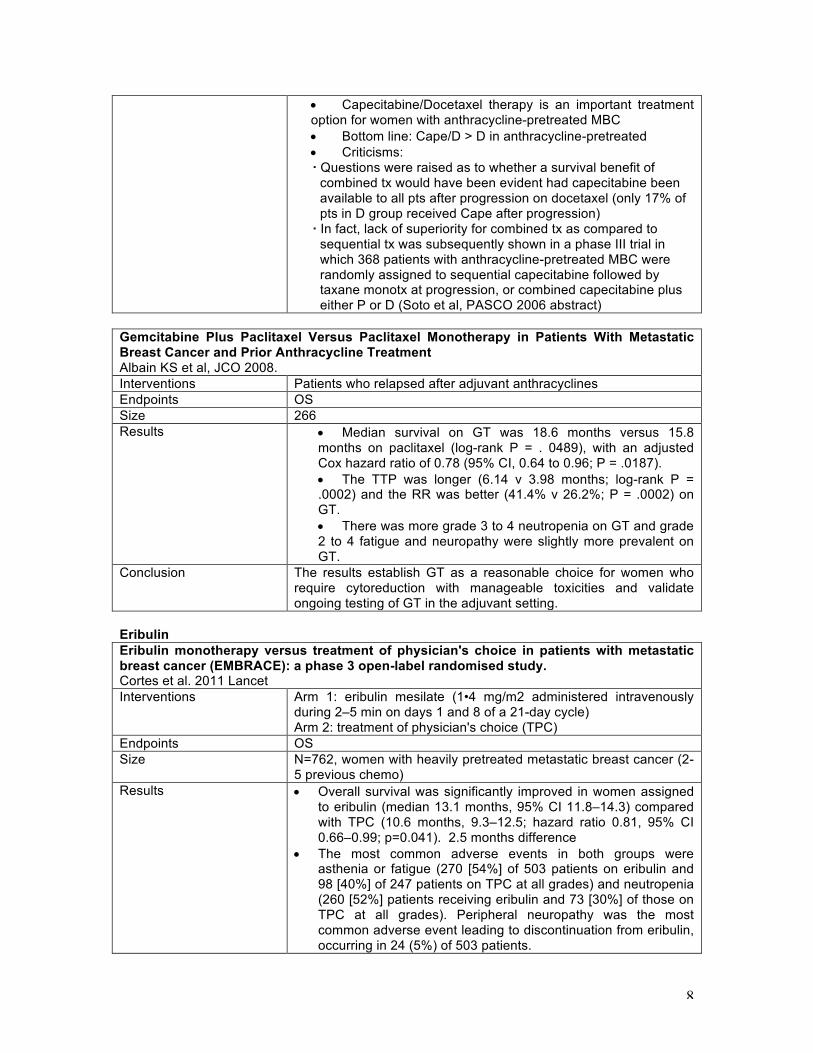
• Capecitabine/Docetaxel therapy is an important treatment option for women with anthracycline-pretreated MBC • Bottom line: Cape/D > D in anthracycline-pretreated • Criticisms:
Questions were raised as to whether a survival benefit of combined tx would have been evident had capecitabine been available to all pts after progression on docetaxel (only 17% of pts in D group received Cape after progression) In fact, lack of superiority for combined tx as compared to sequential tx was subsequently shown in a phase III trial in which 368 patients with anthracycline-pretreated MBC were randomly assigned to sequential capecitabine followed by taxane monotx at progression, or combined capecitabine plus either P or D (Soto et al, PASCO 2006 abstract)
Gemcitabine Plus Paclitaxel Versus Paclitaxel Monotherapy in Patients With Metastatic Breast Cancer and Prior Anthracycline Treatment Albain KS et al, JCO 2008. Interventions Patients who relapsed after adjuvant anthracyclines Endpoints OS Size 266 Results • Median survival on GT was 18.6 months versus 15.8
months on paclitaxel (log-rank P = . 0489), with an adjusted Cox hazard ratio of 0.78 (95% CI, 0.64 to 0.96; P = .0187). • The TTP was longer (6.14 v 3.98 months; log-rank P = .0002) and the RR was better (41.4% v 26.2%; P = .0002) on GT. • There was more grade 3 to 4 neutropenia on GT and grade 2 to 4 fatigue and neuropathy were slightly more prevalent on GT.
Conclusion The results establish GT as a reasonable choice for women who require cytoreduction with manageable toxicities and validate ongoing testing of GT in the adjuvant setting.
Eribulin Eribulin monotherapy versus treatment of physician's choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Cortes et al. 2011 Lancet Interventions Arm 1: eribulin mesilate (1•4 mg/m2 administered intravenously
during 2–5 min on days 1 and 8 of a 21-day cycle) Arm 2: treatment of physician's choice (TPC)
Endpoints OS Size N=762, women with heavily pretreated metastatic breast cancer (2-
5 previous chemo) Results • Overall survival was significantly improved in women assigned
to eribulin (median 13.1 months, 95% CI 11.8–14.3) compared with TPC (10.6 months, 9.3–12.5; hazard ratio 0.81, 95% CI 0.66–0.99; p=0.041). 2.5 months difference
• The most common adverse events in both groups were asthenia or fatigue (270 [54%] of 503 patients on eribulin and 98 [40%] of 247 patients on TPC at all grades) and neutropenia (260 [52%] patients receiving eribulin and 73 [30%] of those on TPC at all grades). Peripheral neuropathy was the most common adverse event leading to discontinuation from eribulin, occurring in 24 (5%) of 503 patients.
9
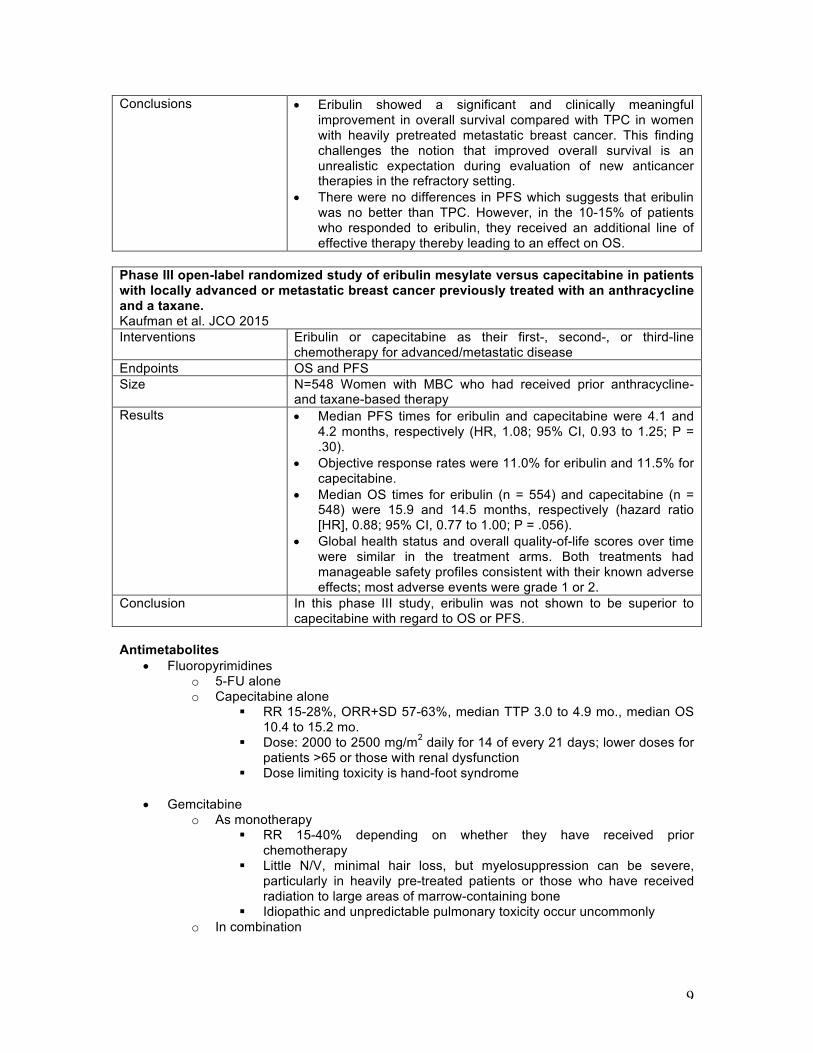
Conclusions • Eribulin showed a significant and clinically meaningful improvement in overall survival compared with TPC in women with heavily pretreated metastatic breast cancer. This finding challenges the notion that improved overall survival is an unrealistic expectation during evaluation of new anticancer therapies in the refractory setting.
• There were no differences in PFS which suggests that eribulin was no better than TPC. However, in the 10-15% of patients who responded to eribulin, they received an additional line of effective therapy thereby leading to an effect on OS.
Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. Kaufman et al. JCO 2015 Interventions Eribulin or capecitabine as their first-, second-, or third-line
chemotherapy for advanced/metastatic disease Endpoints OS and PFS Size N=548 Women with MBC who had received prior anthracycline-
and taxane-based therapy Results • Median PFS times for eribulin and capecitabine were 4.1 and
4.2 months, respectively (HR, 1.08; 95% CI, 0.93 to 1.25; P = .30).
• Objective response rates were 11.0% for eribulin and 11.5% for capecitabine.
• Median OS times for eribulin (n = 554) and capecitabine (n = 548) were 15.9 and 14.5 months, respectively (hazard ratio [HR], 0.88; 95% CI, 0.77 to 1.00; P = .056).
• Global health status and overall quality-of-life scores over time were similar in the treatment arms. Both treatments had manageable safety profiles consistent with their known adverse effects; most adverse events were grade 1 or 2.
Conclusion In this phase III study, eribulin was not shown to be superior to capecitabine with regard to OS or PFS.
Antimetabolites
• Fluoropyrimidines o 5-FU alone o Capecitabine alone
§ RR 15-28%, ORR+SD 57-63%, median TTP 3.0 to 4.9 mo., median OS 10.4 to 15.2 mo.
§ Dose: 2000 to 2500 mg/m2 daily for 14 of every 21 days; lower doses for patients >65 or those with renal dysfunction
§ Dose limiting toxicity is hand-foot syndrome
• Gemcitabine o As monotherapy
§ RR 15-40% depending on whether they have received prior chemotherapy
§ Little N/V, minimal hair loss, but myelosuppression can be severe, particularly in heavily pre-treated patients or those who have received radiation to large areas of marrow-containing bone
§ Idiopathic and unpredictable pulmonary toxicity occur uncommonly o In combination
10
§ Can be combined occasionally to taxanes (refer to above), cisplatin, vinorelbine
§ RR 36-70% even in heavily pre-treated patients § Acceptable toxicity
Alkylating agents
• Cyclophosphamide o Most widely used alkylating agent o Old studies suggest single agent activity of 10-60% in previously untreated MBC o Side effects: nausea, vomiting, alopecia, myelosuppression as well as bladder
inflammation and hematuria (reduce risk by adequate hydration and urination) o Increased risk of secondary AML, related drug exposure and cumulative dose o In contrast to melphalan which increases risk of AML 30-fold, increased risk from
cyclophosphamide is less than 3-fold, especially at doses below 20 g/m2 Vinca alkaloids
• Vinorelbine o Prevent assembly of microtubules, thereby inhibiting DNA replication o Monotherapy particularly useful for the treatment of MBC in older women who
have significant comorbidity o Side effects: mild nausea, vomiting and hair loss o RR 25-53%, median TTP 2.8 to 3.0 mo., median OS 6.0 to 7.0 mo., even in
heavily pre-treated patients o Combination regimens that contain a vinca alkaloid are often associated with
higher RR but no better OS when compared to anthracycline or a taxane alone Platinum
• Cisplatin and carboplatin o Combinations with other drugs, including taxanes, capecitabine, etoposide,
vinorelbine, and gemcitabine may be considered for 3rd/4th-line (or beyond) therapy in pts who maintain a good ECOG and adequate marrow reserve
o Some interests especially in triple negative disease.
o TNT trial (Tutt et al SABCS 2014) - showed that carboplatin was similar to docetaxel as first line therapy in TNBC, but was better in BRCA mutation carriers.
o Anti-Cancer Drugs (Guan 2015) Meta-analysis (8 RCT’s, 1142 patients) evaluating palliative and neoadjuvant patients (separate analyses)showed that platinum based regimens were significantly better RR = 2.42 in metastatic TNBC.
Others
• Etoposide o RR 25-50%, even in heavily pre-treated patients o Continuous oral administration (50 mg/m2 daily) permits dose titration to toxicity,
which is principally hematologic and gastrointestinal o Oral etoposide is a reasonable 3rd/4th-line (or beyond) regimen.
Combination vs. sequential therapy Multicenter randomized trial comparing sequential with concomitant administration of doxorubicin (A) and docetaxel (T) as first-line treatment of metastatic breast cancer: a Spanish Breast Cancer Research Group (GEICAM-9903) phase III study Alba E et al. JCO 2004;22:2587-2593 Interventions Phase III trial which compared 3 cycles of A 75 mg/m2 every 21
days followed by 3 cycles of T 100 mg/m2 every 21 days (sequential
11
AàT) or 6 cycles of A 50 mg/m2 and T 75 mg/m2 every 21 days (combined AT), as 1st line chemotherapy in MBC
Endpoints Toxicity RR PFS OS
Size • 144 MBC pts Results Toxicity
• FNE: AàT 29.3% vs AT 47.8% p=0.02 • Asthenia, diarrhea, and fever more frequent in AT arm
Response ate • AàT 61% vs AT 51% p=NS
Median duration of response • AàT 8.7 months vs AT 7.6 months p=NS
Median time to progression • AàT 10.5 months vs AT 9.2 months p=NS
Median overall survival • Aà 22.3 months vs AT 21.8 months (AT) p=NS
Conclusion AàT significantly reduced febrile neutropenia compared with AT in MBC patients, but maintains comparable antitumoral efficacy AàT represents a valid option for the treatment of MBC
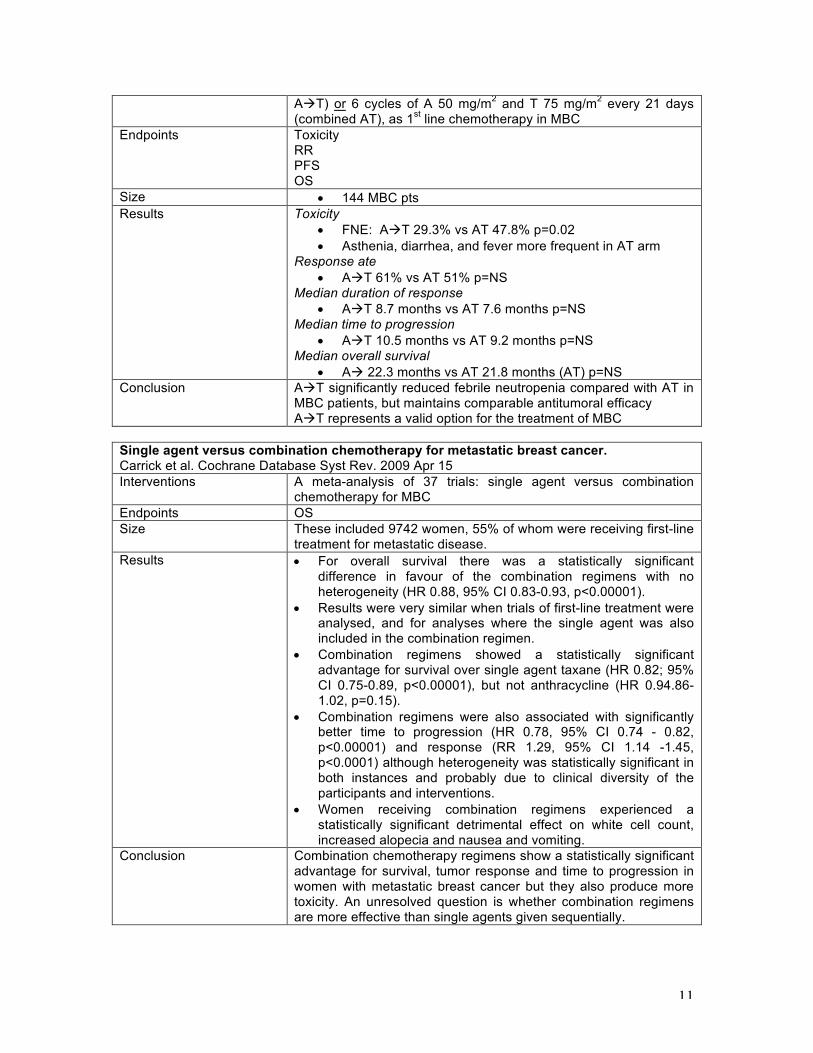
Single agent versus combination chemotherapy for metastatic breast cancer. Carrick et al. Cochrane Database Syst Rev. 2009 Apr 15 Interventions A meta-analysis of 37 trials: single agent versus combination
chemotherapy for MBC Endpoints OS Size These included 9742 women, 55% of whom were receiving first-line
treatment for metastatic disease. Results • For overall survival there was a statistically significant
difference in favour of the combination regimens with no heterogeneity (HR 0.88, 95% CI 0.83-0.93, p<0.00001).
• Results were very similar when trials of first-line treatment were analysed, and for analyses where the single agent was also included in the combination regimen.
• Combination regimens showed a statistically significant advantage for survival over single agent taxane (HR 0.82; 95% CI 0.75-0.89, p<0.00001), but not anthracycline (HR 0.94.86-1.02, p=0.15).
• Combination regimens were also associated with significantly better time to progression (HR 0.78, 95% CI 0.74 - 0.82, p<0.00001) and response (RR 1.29, 95% CI 1.14 -1.45, p<0.0001) although heterogeneity was statistically significant in both instances and probably due to clinical diversity of the participants and interventions.
• Women receiving combination regimens experienced a statistically significant detrimental effect on white cell count, increased alopecia and nausea and vomiting.
Conclusion Combination chemotherapy regimens show a statistically significant advantage for survival, tumor response and time to progression in women with metastatic breast cancer but they also produce more toxicity. An unresolved question is whether combination regimens are more effective than single agents given sequentially.

12
- Soto et al. ASCO abstract 2006: Anthracycline pretreated MBC: xeloda (X) à Taxotere (T) versus XT, versus XP (paclitaxel). RR higher with combo (60-70% vs 40% for sequential) but after 15mos f/u, median OS similar (about 30 mos all arms.)
- 2010 Investigational New Drugs Park: N=82, MBC pretreated with anthracyclines and paclitaxel Combination of gemcitabine and vinorelbine or gemcitabine until disease progression followed by vinorelbine monotherapy. Median overall survival for the combination and sequential arms was 10.6 months and 8.9 months, respectively (P = 0.436). Combined gemcitabine and vinorelbine therapy appears comparable to sequential monotherapy for heavily pretreated patients with metastatic breast cancer as demonstrated by improved quality of life outcomes with similar therapeutic efficacies and incidences of adverse events
Bottom line
• Despite slightly better RR and TTF for multi-drug regimens, QOL and toxicity analyses favor single agent therapy in women with MBC, esp. since no difference in OS and goal of treatment in MBC is really palliative • However, for very symptomatic patients or those with rapidly progressive visceral metastases, combination therapy may be a more appropriate choice because of the greater likelihood of an objective response (Recommended by ASCO)
Endocrine therapy Overview
• Rapidly progressive / symptomatic visceral metastases is generally considered a contraindication to primary endocrine Rx à these women should receive chemotherapy
• Predictors of Response to Endocrine Rx in the Metastatic Setting:
o ER/PR positivity Phenotype Frequency RR (1st line) ER+ / PR+ 40% 75-80% ER+ / PR- 30% 20-25% ER- / PR+ 2% 40-45% ER- / PR- 28% 5-10%
o Long relapse free interval o Isolated bone and soft-tissue involvement o Prior response to endocrine therapy
• Premenopausal Women:
o 1st Line – Ov ablation (oophrect or GnRH agonist) + AI + CDK4/6 o 2nd Line – Ov ablation if not given 1st line; tam if not given 1st line
• Postmenopausal Women:
o For women who do not have visceral crisis, hormonal therapy with CDK4/6 inhibition is considered first line therapy for metastatic HR+/HER2- disease
o Primary Hormone Sensitive (i.e. no prior endocrine Rx, relapse >12mo post adjuvant endocrine Rx, relapse while receiving adjuvant tamoxifen)
§ 1st Line – Aromatase Inhibition with CDK4/6 inhibition § 2nd Line – Fulvestrant +/- CDK 4/6 inhibition OR Exemestane +/-
everolimus § 3rd Line – Tamoxifen, Exemestane, Fulvestrant (demonstrated benefit in
Bone only disease – FALCON)
13
Ovarian ablation • Oophrectomy / Ovarian Radiation:
o ORR = ~33% o No difference in OS or PFS with LHRH agonist vs. Tam
• GnRH Agonists: o Groserelin / Leuprolide – peptide analogues of LHRH, 50-100x more potent o Act on the pituitary; initially stimulate LH/FSH, then profoundly supress pituitary –
ovarian axis, causing fall of estrogen to menopausal levels o Effectiveness GnRH Agonist vs. Oophrectomy as 1st Line Endocrine Rx (Taylor,
JCO 1998; 16:994) - 136 pts randomized; no difference in FFS or OS
• Ovarian Ablation / Suppression Plus Tamoxifen: o Meta-analysis of 4 trials w. 506 premenopausal women treated 1st line with
Tam+GnRH vs. GnRH alone (Klijn, JCO 2001; 19:343) - Combination Rx provided modest DFS and OS benefit vs. GnRH alone - Compared w ovarian suppression alone, combined therapy signficinatly improved both
PFS (HR 0.70, p=0.0003) and OS (HR 0.78, p=0.02) - Whether treatment is superior to single agent tam is unknown. - RR combination 39% vs. monoRx 30% - Similar toxicity: hot flashes, vaginal discharge, sexual function impact
• Ovarian Ablation / Suppression Plus AI:
o Only phase II trials, but some promising results § Park IH, et al JCO 2010: 35 premenopausal pts received goserelin (3.6
mg sc every 28 days) plus letrozole (2.5 mg orally daily), and 38 postmenopausal pts received letrozole alone as 1st line endocrine therapy in the metastatic setting
• Clinical benefit rates comparable b/w the 2 groups (77 vs 74%, p=0.77)
• No difference in TTP (9.5 vs 8.9 mo, CI 6.4 – 13.3 mo) • In pts who didn’t receive bisphosphonates, letrozole +/- goserelin
caused a greater loss of bone mineral density @ 6 mo’s compared w that of pts receiving bisphosphonate treatment
• Aromatase Inhibition w/o Ovarian Ablation:
o Contraindicated in premenopausal women o Reduced feedback of estrogen to the hypothalamus and pituitary leads to an
increase in GnRH secretion à Estrogen surge & possible breast CA flare Tamoxifen
• Tamoxifen Benefit: o ER/PR positive = 50-60% RR o ER/PR negative = 5-10% RR o Duration of benefit – median 12 to 18 months o Viable option in both pre and post-menopausal populations
• Tamoxifen Resistance:
o 1/3 of women with secondary tam resistance will respond to other endrocrine Rx o 15% of women with primary tam resistance will respond to other endocrine Rx
Aromatase inhibitor
• Anastrozole (1mg PO OD): - Nabholtz, EJC 2003: combined analysis of 2 phase 3 trials, 1st line ANA vs TAM; ORR
33%, TTP 8.2m (same)
14
- Budzar, Cancer 1998: combined analysis of 2 phase 3 trials, 2nd line ANA for patients progressing on TAM; ORR 10.3%, mOS 27m
• Letrozole (2.5 mg PO OD): - Mouridsen, JCO 2003: phase 3 trial of LET vs TAM, 1st line; RR 32 vs 21%, TTP 9.4 vs
6m, time until chemo 15 vs 9m, OS 24 vs 30 (NS). - 2nd line: RR 24%, OS 25m
• Exemestane (25 mg PO OD): - Paridaens, ASCO meeting 2004: phase 3 trial of EXE vs TAM, 1st line; RR 44 vs 29%,
PFS 10.9 vs 6.7m - 2nd line: TTP 20 weeks - Phase II trials have shown Exemestane is effective in patients who never responded to
tamoxifen (primary refractory), as well as patients who have failed non-steroidal AIs (secondary refractory)
• Meta-Analysis of 1st line AI vs. Tam in Met Br CA: - Mauri D, JNCI 2006; 98:1285; 23 published trials comparing any AI to tam in advanced breast CA (8504) Ø Significant survival benefits w third-generation AI’s and inactivators (vorozole, letrozole,
exemestane, anastrozole) (RH=0.87, p<0.001), but not with first generation (aminoglutethimide) or 2nd generation (formestane and fadrozole) agents.
Ø The difference in the summary effects between these 2 groups of trials was significant (p=0.04)
Ø Survival benefit w 3rd generation agents in first line trials, in which these agents were compared w tamoxifen (11% RH reduction, p=0.03) was identical to their benefit in 2nd and subsequent line trials in which these agents were compared w other treatments (14% RH reduction, p<0.001)
Fulvestrant
• ER antagonist that blocks ER dimerization and DNA binding, increases ER turnover, and inhibits nuclear uptake of the receptor - Because it blocks ER function before estrogen can bind the receptor, Fulvestrant can
theoretically overcome resistance that is driven by the agonist properties of tamoxifen - IM injection 500mg loading dose d1,14 then monthly
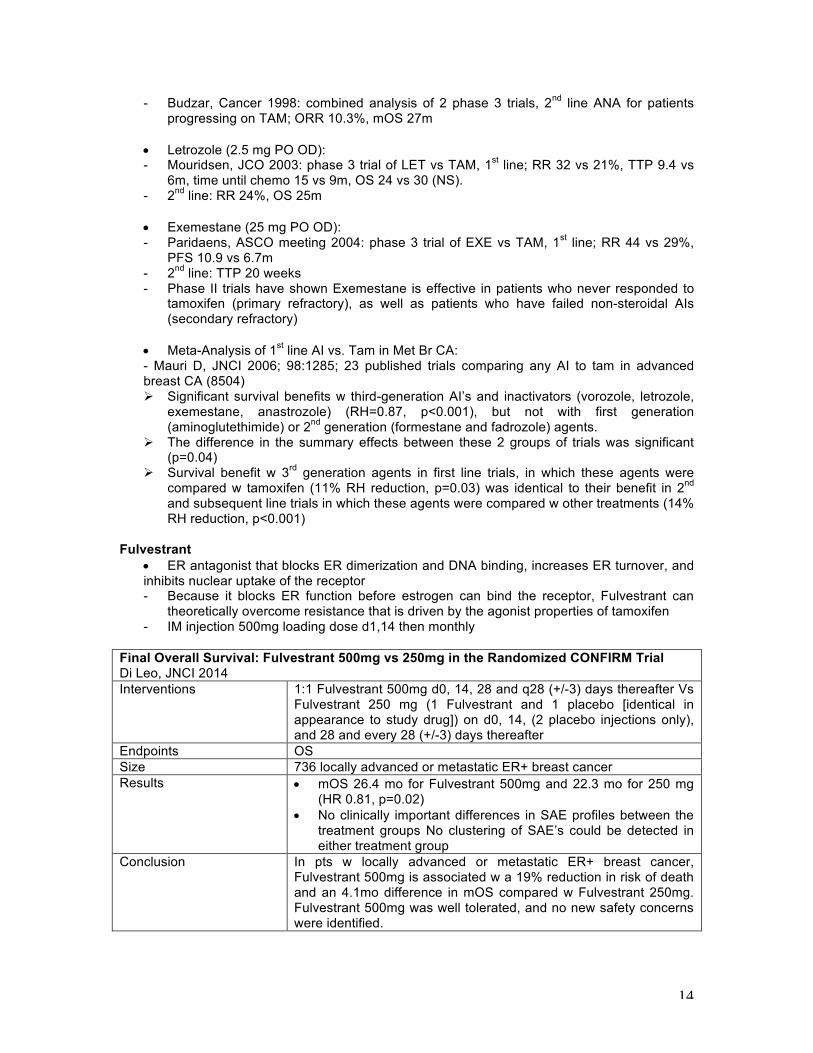
Final Overall Survival: Fulvestrant 500mg vs 250mg in the Randomized CONFIRM Trial Di Leo, JNCI 2014 Interventions 1:1 Fulvestrant 500mg d0, 14, 28 and q28 (+/-3) days thereafter Vs
Fulvestrant 250 mg (1 Fulvestrant and 1 placebo [identical in appearance to study drug]) on d0, 14, (2 placebo injections only), and 28 and every 28 (+/-3) days thereafter
Endpoints OS Size 736 locally advanced or metastatic ER+ breast cancer Results • mOS 26.4 mo for Fulvestrant 500mg and 22.3 mo for 250 mg
(HR 0.81, p=0.02) • No clinically important differences in SAE profiles between the
treatment groups No clustering of SAE’s could be detected in either treatment group
Conclusion In pts w locally advanced or metastatic ER+ breast cancer, Fulvestrant 500mg is associated w a 19% reduction in risk of death and an 4.1mo difference in mOS compared w Fulvestrant 250mg. Fulvestrant 500mg was well tolerated, and no new safety concerns were identified.

15
Fulvestrant 500mg versus anastrazole 1mg for hormone receptor-positive advanced breast cancer (FALCON): an international, randomized, double-blind, phase 3 trial Robertson et. al Lancet 2016 Interventions 1:1 assignment, Fulvestrant (HD 500mg on day 1 and 14 of month
1 & q28 days therafter) vs Anastrazole 1mg. ITT analysis Endpoints PFS, Intervention by surgery or RT, or death from any cause. Size 462 postmenopausal, HR+, HER2-ve, endocrine therapy naïve Results - mPFS 16.6 vs 13.8 months in Fulvestrant vs Anastrazole
respectively. OS not yet reached. - Patients with Non-visceral disease HR=0.59, mPFS =22.3
vs 13.8 mths for Fulvestrant vs Anastrazole - Patients with Visceral disease HR = 0.99, mPFS 13.8 vs
15.9 mths for Fulvestrant vs Anastrazole Conclusion - For patients with endocrine naïve disease, Fulvestrant
shows superior PFS compared with Anastrazole. - In subgroup analysis, patients with Non-visceral disease
(not specifically bone-only) have a superior mPFS compared with those who have visceral disease.
Combination trials
Ø 1st line - Mehta 2012 NEJM (SWOG S0226): FULV/ANA vs ANA, mPFS 15 vs 13.5m (significant), OS 47.87 vs 42.3m (p=0.05)
Ø 2nd line - Bergh 2012 JCO (FACT): FULV/ANA vs ANA, no difference in TTP and OS Ø 2nd line – Johnston 2013 Lancet Oncol (SoFEA): FULV/ANA vs FULV vs EXE, PFS same
Overcoming hormone refractoriness • No known overall survival benefit with secondary manipulations of hormone therapy with the
additional agents, but PFS benefit when combined with AI • Everolimus – mTOR inhibitor
Everolimus in Postmenopausal Hormone-Receptor–Positive Advanced Breast Cancer Baselga et al. NEJM 2012; Ann Oncol 2014 Interventions 2:1 Everolimus 10mg/d and Exemestane 25mg/d Vs Exemestane
and placebo Endpoints PFS Size 724 women w HR+ advanced breast cancer who had recurrence or
progression while receiving previous therapy w a NSAI in the adjuvant setting or to treat advanced disease (or both)
Results • Interim analysis mPFS 6.9 vs 2.8 mo, according to assessments by local investigators(HR 0.43, p<0.001) mPFS 10.6 vs 4.1 mo according to central assessment (HR0.36, p<0.001)
• mOS 31.0mo vs 26.6 mo (HR 0.89 p=0.14) • Most common gd 3 or 4 AE’s were stomatitis (8 vs 1%), anemia
(6 vs <1%), dyspnea (4 vs 1%), hyperglycemia (4% vs <1%), fatigue (4 vs 1%), and pneumonitis (3 vs 0%).
• ~25% of patients discontinued treatment without progression due to toxicity.
Conclusion Adding EVE to EXE did not confer a statistically significant improvement in the secondary endpoint OS despite producing a clinically meaningful and statistically significant improvement in the primary endpoint PFS (4.6 mo prolongation in mPFS, p<0.0001). Ongoing translational research should further refine the benefit of mTOR inhibition and related pathways in this treatment setting.
Comments Post-study treatments were received by 84% of pts in the
16
EVE+EXE vs 90% in the PBO+EXE The problem with this trial is that there was informative censoring which when accounted for makes the difference in PFS a lot less clinically meaningful.
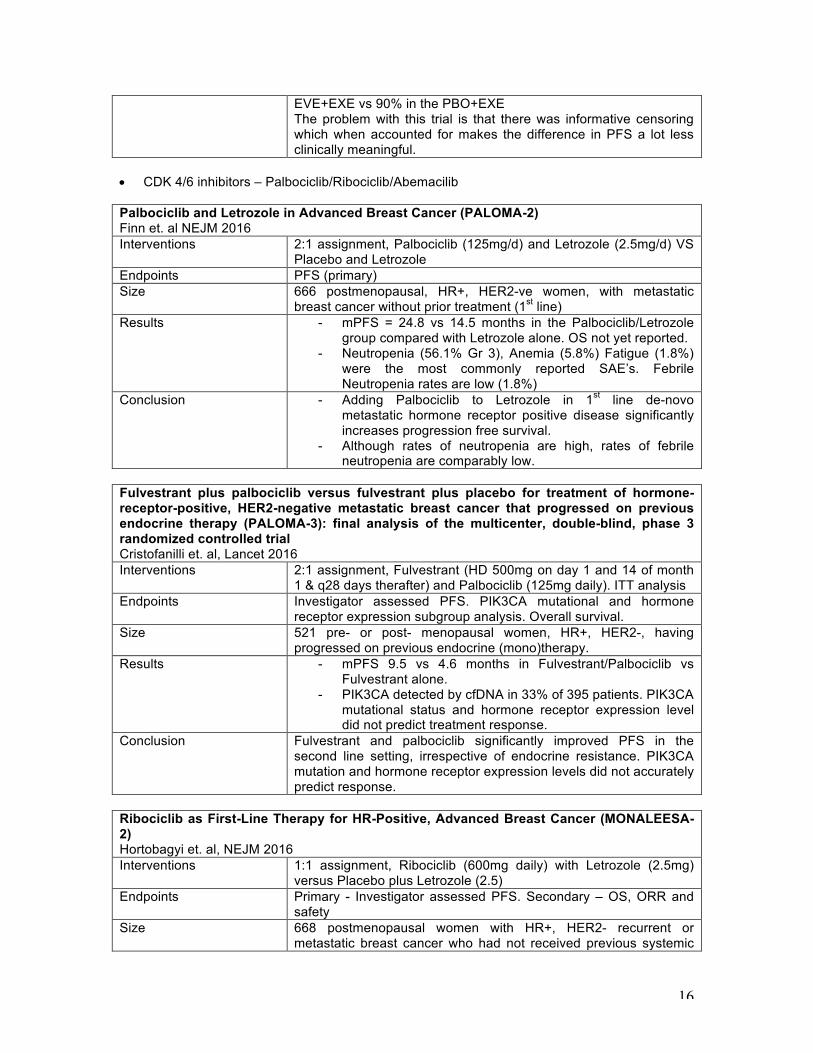
• CDK 4/6 inhibitors – Palbociclib/Ribociclib/Abemacilib Palbociclib and Letrozole in Advanced Breast Cancer (PALOMA-2) Finn et. al NEJM 2016 Interventions 2:1 assignment, Palbociclib (125mg/d) and Letrozole (2.5mg/d) VS
Placebo and Letrozole Endpoints PFS (primary) Size 666 postmenopausal, HR+, HER2-ve women, with metastatic
breast cancer without prior treatment (1st line) Results - mPFS = 24.8 vs 14.5 months in the Palbociclib/Letrozole
group compared with Letrozole alone. OS not yet reported. - Neutropenia (56.1% Gr 3), Anemia (5.8%) Fatigue (1.8%)
were the most commonly reported SAE’s. Febrile Neutropenia rates are low (1.8%)
Conclusion - Adding Palbociclib to Letrozole in 1st line de-novo metastatic hormone receptor positive disease significantly increases progression free survival.
- Although rates of neutropenia are high, rates of febrile neutropenia are comparably low.
Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicenter, double-blind, phase 3 randomized controlled trial Cristofanilli et. al, Lancet 2016 Interventions 2:1 assignment, Fulvestrant (HD 500mg on day 1 and 14 of month
1 & q28 days therafter) and Palbociclib (125mg daily). ITT analysis Endpoints Investigator assessed PFS. PIK3CA mutational and hormone
receptor expression subgroup analysis. Overall survival. Size 521 pre- or post- menopausal women, HR+, HER2-, having
progressed on previous endocrine (mono)therapy. Results - mPFS 9.5 vs 4.6 months in Fulvestrant/Palbociclib vs
Fulvestrant alone. - PIK3CA detected by cfDNA in 33% of 395 patients. PIK3CA
mutational status and hormone receptor expression level did not predict treatment response.
Conclusion Fulvestrant and palbociclib significantly improved PFS in the second line setting, irrespective of endocrine resistance. PIK3CA mutation and hormone receptor expression levels did not accurately predict response.
Ribociclib as First-Line Therapy for HR-Positive, Advanced Breast Cancer (MONALEESA-2) Hortobagyi et. al, NEJM 2016 Interventions 1:1 assignment, Ribociclib (600mg daily) with Letrozole (2.5mg)
versus Placebo plus Letrozole (2.5) Endpoints Primary - Investigator assessed PFS. Secondary – OS, ORR and
safety Size 668 postmenopausal women with HR+, HER2- recurrent or
metastatic breast cancer who had not received previous systemic
17
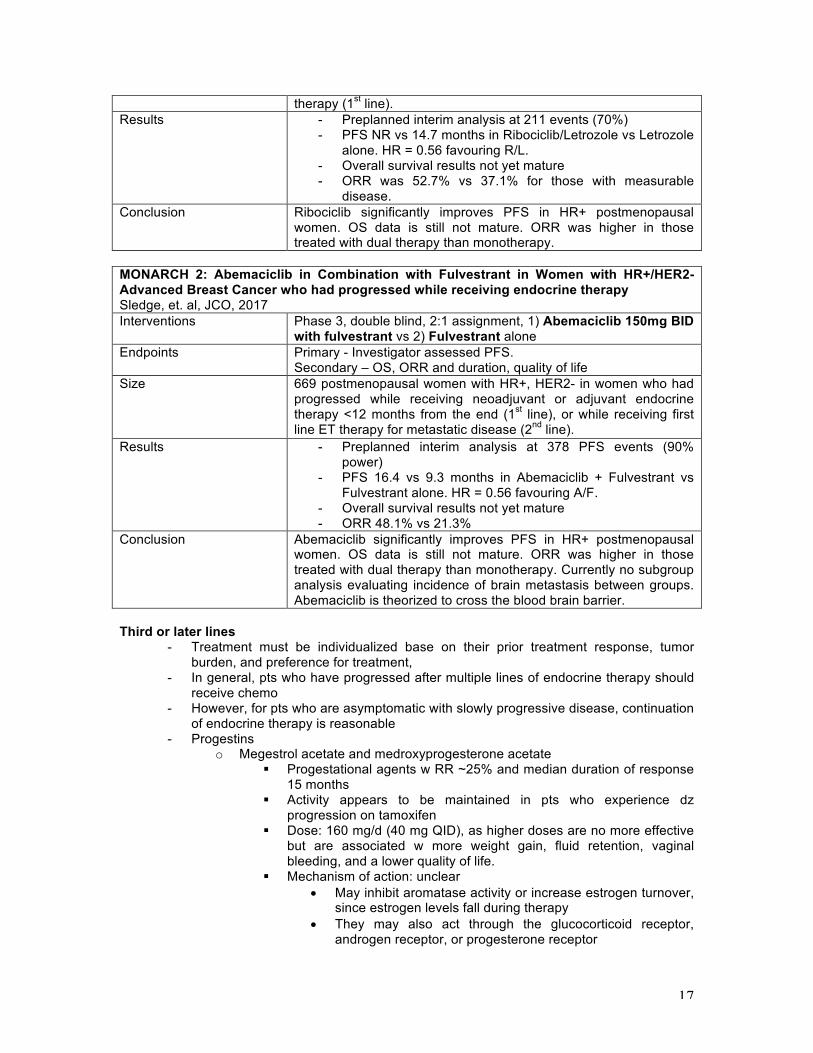
therapy (1st line). Results - Preplanned interim analysis at 211 events (70%)
- PFS NR vs 14.7 months in Ribociclib/Letrozole vs Letrozole alone. HR = 0.56 favouring R/L.
- Overall survival results not yet mature - ORR was 52.7% vs 37.1% for those with measurable
disease. Conclusion Ribociclib significantly improves PFS in HR+ postmenopausal
women. OS data is still not mature. ORR was higher in those treated with dual therapy than monotherapy.
MONARCH 2: Abemaciclib in Combination with Fulvestrant in Women with HR+/HER2- Advanced Breast Cancer who had progressed while receiving endocrine therapy Sledge, et. al, JCO, 2017 Interventions Phase 3, double blind, 2:1 assignment, 1) Abemaciclib 150mg BID
with fulvestrant vs 2) Fulvestrant alone Endpoints Primary - Investigator assessed PFS.
Secondary – OS, ORR and duration, quality of life Size 669 postmenopausal women with HR+, HER2- in women who had
progressed while receiving neoadjuvant or adjuvant endocrine therapy <12 months from the end (1st line), or while receiving first line ET therapy for metastatic disease (2nd line).
Results - Preplanned interim analysis at 378 PFS events (90% power)
- PFS 16.4 vs 9.3 months in Abemaciclib + Fulvestrant vs Fulvestrant alone. HR = 0.56 favouring A/F.
- Overall survival results not yet mature - ORR 48.1% vs 21.3%
Conclusion Abemaciclib significantly improves PFS in HR+ postmenopausal women. OS data is still not mature. ORR was higher in those treated with dual therapy than monotherapy. Currently no subgroup analysis evaluating incidence of brain metastasis between groups. Abemaciclib is theorized to cross the blood brain barrier.
Third or later lines
- Treatment must be individualized base on their prior treatment response, tumor burden, and preference for treatment,
- In general, pts who have progressed after multiple lines of endocrine therapy should receive chemo
- However, for pts who are asymptomatic with slowly progressive disease, continuation of endocrine therapy is reasonable
- Progestins o Megestrol acetate and medroxyprogesterone acetate
§ Progestational agents w RR ~25% and median duration of response 15 months
§ Activity appears to be maintained in pts who experience dz progression on tamoxifen
§ Dose: 160 mg/d (40 mg QID), as higher doses are no more effective but are associated w more weight gain, fluid retention, vaginal bleeding, and a lower quality of life.
§ Mechanism of action: unclear • May inhibit aromatase activity or increase estrogen turnover,
since estrogen levels fall during therapy • They may also act through the glucocorticoid receptor,
androgen receptor, or progesterone receptor

18
- Estrogens o Estrogenic compounds can be used as a treatment for MBC but there are no
data on the impact on outcomes of treatment compared w placebo. § Evidence was from a NEJM trial in 1981!
- Androgens o Including testosterone, fluoxymesterone, and danazol, are inferior to high
dose estrogens and are rarely used to treat MBC o Though RR 10-20%, side effects include virilization, edema, and jaundice.
Investigational Approaches
- Targeting mutations in the estrogen receptor o ESR1, the gene that encodes estrogen receptor 1
§ Found to have recurrent mutations – works as an acquired resistance mechanisms to endocrine therapy, particularly AI’s.
§ In contrast to the rare occurrence in primary breast tumor, ESR1 mutation was found in 11 to 55% of metastatic biopsies
§ These mutations cluster in the ligand binding domain of ER, with Y537S, C, or N and D538G being the most common, leading to a constitutive agonist conformation, and therefore resistance to AI treatment
§ In addition, in preclinical studies, a higher dose of tam or fulvestrant was needed to suppress tumor cell proliferation in the presence of ESR1 mutations
- Exemestane plus entinostat (HDAC inhibitor) - Endocrine therapy plus PI3K pathway inhibitors - Endocrine therapy plus androgen receptor blockade - The pan-PI3K + endocrine therapy trials are either negative (e.g. FERGI) or
statistically positive, but clinically unmeaningful (BELLE-2). - The RCT of exemestane +/- abiraterone was negative.
Her-2 directed therapy
First-line therapy: Pertuzumab + trastuzumab + docetaxel
- Pertuzumab binds to subdomain 2 of Her-2 and prevents heterodimerization of Her-2 with Her-3.
Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. 2012 NEJM Baselga; 2015 NEJM Swain (CLEOPATRA) Interventions 1st line Treatment of: Placebo + Trastuzumab + Docetaxel (control
group) Vs Pertuzumab + Trastuzumab + Docetaxel (Pertuzumab group) Until time of disease progression or development of intolerable toxic effects
Endpoints OS Size 808 pts w HER2-positive MBC Results 12.4 mo vs 18.5 mo HR for progression or death, 0.62, p<0.001)
Update: mPFS for Pertuzumab group 6.3 months (HR 0.68) Pertuzumab extended the median duration of response by 7.7 mo. The objective response rate was 69.3% in the control group, as compared with 80.2% in the pertuzumab group. Update: mOS 40.8 mo vs 56.5mo (HR favoring Pertuzumab group, 0.68, p<0.001), a difference of 15.7 months. (This analysis was not adjusted for crossover to the Pertuzumab group, and is therefore conservative) Most AE’s occurred during admin of docetaxel in the 2 groups, w
19
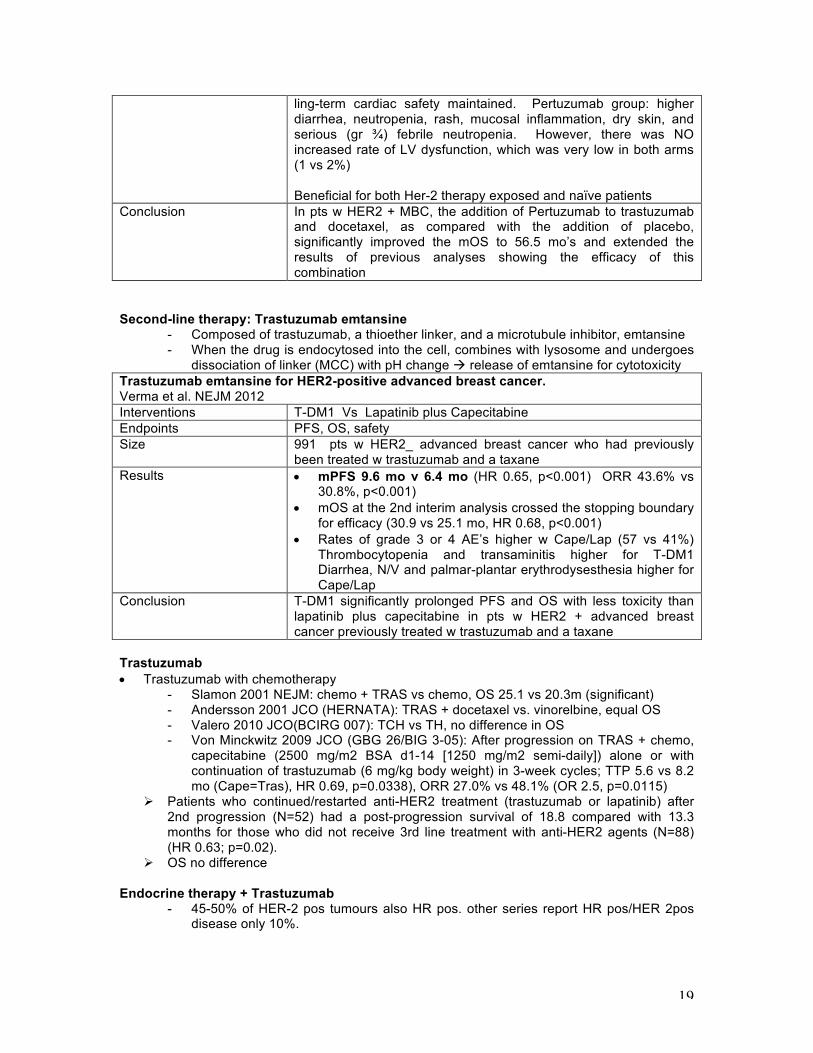
ling-term cardiac safety maintained. Pertuzumab group: higher diarrhea, neutropenia, rash, mucosal inflammation, dry skin, and serious (gr ¾) febrile neutropenia. However, there was NO increased rate of LV dysfunction, which was very low in both arms (1 vs 2%) Beneficial for both Her-2 therapy exposed and naïve patients
Conclusion In pts w HER2 + MBC, the addition of Pertuzumab to trastuzumab and docetaxel, as compared with the addition of placebo, significantly improved the mOS to 56.5 mo’s and extended the results of previous analyses showing the efficacy of this combination
Second-line therapy: Trastuzumab emtansine
- Composed of trastuzumab, a thioether linker, and a microtubule inhibitor, emtansine - When the drug is endocytosed into the cell, combines with lysosome and undergoes
dissociation of linker (MCC) with pH change à release of emtansine for cytotoxicity Trastuzumab emtansine for HER2-positive advanced breast cancer. Verma et al. NEJM 2012 Interventions T-DM1 Vs Lapatinib plus Capecitabine Endpoints PFS, OS, safety Size 991 pts w HER2_ advanced breast cancer who had previously
been treated w trastuzumab and a taxane Results • mPFS 9.6 mo v 6.4 mo (HR 0.65, p<0.001) ORR 43.6% vs
30.8%, p<0.001) • mOS at the 2nd interim analysis crossed the stopping boundary
for efficacy (30.9 vs 25.1 mo, HR 0.68, p<0.001) • Rates of grade 3 or 4 AE’s higher w Cape/Lap (57 vs 41%)
Thrombocytopenia and transaminitis higher for T-DM1 Diarrhea, N/V and palmar-plantar erythrodysesthesia higher for Cape/Lap
Conclusion T-DM1 significantly prolonged PFS and OS with less toxicity than lapatinib plus capecitabine in pts w HER2 + advanced breast cancer previously treated w trastuzumab and a taxane
Trastuzumab • Trastuzumab with chemotherapy
- Slamon 2001 NEJM: chemo + TRAS vs chemo, OS 25.1 vs 20.3m (significant) - Andersson 2001 JCO (HERNATA): TRAS + docetaxel vs. vinorelbine, equal OS - Valero 2010 JCO(BCIRG 007): TCH vs TH, no difference in OS - Von Minckwitz 2009 JCO (GBG 26/BIG 3-05): After progression on TRAS + chemo,
capecitabine (2500 mg/m2 BSA d1-14 [1250 mg/m2 semi-daily]) alone or with continuation of trastuzumab (6 mg/kg body weight) in 3-week cycles; TTP 5.6 vs 8.2 mo (Cape=Tras), HR 0.69, p=0.0338), ORR 27.0% vs 48.1% (OR 2.5, p=0.0115)
Ø Patients who continued/restarted anti-HER2 treatment (trastuzumab or lapatinib) after 2nd progression (N=52) had a post-progression survival of 18.8 compared with 13.3 months for those who did not receive 3rd line treatment with anti-HER2 agents (N=88) (HR 0.63; p=0.02).
Ø OS no difference Endocrine therapy + Trastuzumab
- 45-50% of HER-2 pos tumours also HR pos. other series report HR pos/HER 2pos disease only 10%.

20
Ø Mackey 2006 (TAMDEM): HR+/HER2 by ihc 3+/FISH randomized to anastrazole 1mg od +/- herceptin (4mg/kg load, 2mg wkl). PFS improved with combo 4.8 vs 2.7 mos, ss. ORR 20% vs 6%, ss. OS 28 vs 25 mos, NS (more than 50% crossover). Central confirmed HR pos n = 150: even longer PFS 5.8 vs 3.8 mos ss. If NO LIVER METS: OS improved with combo: 41 vs 32 mos, significant.
Ø Huober 2009 (ELECTRA): HR+/HER2+ first line, randomized to letrozole+/- Herceptin. HR+/Her2 negative letrozole alone (arm c). N=92, closed early. Combo arm TTP: 14 mos vs 3 mos (15 mos in arm c). CBR was 65% vs 40% (77% arm C). no sig change in cardiac function.
Lapatinib
- Orally active dual erbB-1/2 TK inhibitor. - Inhibits HER 2 (erb2) and EGFR (erb1). Erb 2likely most impt in breast ca growth.
Crosses BBB. Reported side effects include diarrhea, acneiform rash most commonly (NOT associated with efficacy like other egfri), cardiotoxicity and rarely ILD.
- Nth LINE: Lapatinib + Capcitabine Lapatinib plus capecitabine for HER2-positive advanced breast cancer.. Geyer et al. N Engl J Med. 2006 Interventions Capcitabine alone (1250 mg/m2 BID 14dys out of 21) or
Capcitabine (1000mg/m2 BID) + Labatinib (1250mg OD continuous)
Primary Endpoint TTP Inclusion Criteria HER2 Positive MBC
Progression with previous anthracycline, taxane and trastuzumab Results • Interim analysis revealed significant TTP benefit favouring
combination therapy (8 vs. 4 months) and RR (22 vs 14%). No OS benefit. • 08 Update: TTP better with combo: HR 0.57, ss. OS: trend (HR 0.78, p=0.1) Less CNS relapse with lapatanib (4 vs 13, ss). Serum Her 2 extracellular domain did not predict for response. Response limited to IHC 3+/FISH pos. • Similar adverse event profile in two arms
Conclusion Lapatinib improves RR and TTP in patients with refractory HER2+ metastatic breast cancer
HER-2 NEGATIVE: NOVEL TARGETED AGENTS BRCA1/2 Mutation Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA mutation Robson, et. al. N Engl J Med. 2017 Interventions PARP inhibition using 1) Olaparib (300mg BID) or 2) TPC
(standard single agent chemotherapy – cape, eribulin, vinorelbine) Primary Endpoint 1) PFS
2) OS Inclusion Criteria Metastatic HR+/- and /HER2-, BRCA1/2 mutation positive breast
cancer Results • Randomized Phase 3, 2:1 ITT analysis, n=302
• PFS = 7.0 vs 4.2 mths (HR=0.58) • RR = 59.9% vs 28.8% • Rate of toxic discontinuation was 4.9 vs 7.7% • No difference in Overall survival (HR = 0.9)
Conclusion Olaparib increases median PFS but does not increase overall survival. Critisicism – BRCA1 patients seemed to benefit more with the 95% confidence

21
intervals for BRCA2 crossing over 1. – HR+ vs TNBC patients also did not benefit to the same
degree (HR= 0.82 vs 0.43) Immune therapy in triple negative cancer Phase Ia trial
Ø Involved 54 women with metastatic triple-negative breast cancer who were treated every 3 weeks with MPDL3280A (PD-L1 inhibitor) 15 or 20 mg/kg or with a flat dose of 1200 mg. The level of PD-L1 expression on tumor-infiltrating immune cells was assessed using a proprietary assay.
Ø All 21 patients evaluable for efficacy had levels of PD-L1 on immune cells of 5% or greater. The overall response rate was 19% (95% confidence interval [CI], 5% - 42%), and 24-week progression-free survival was 27% (95% CI, 7% - 47%). There were two complete responses and two partial responses.
Ø 3 patients appeared to experience the phenomenon of "pseudoprogression" — an atypical response pattern seen in some patients treated with this class of agent — and were considered to have progressive disease.
Ø The median duration of response has not yet been reached (range, 18 to at least 56 weeks), and the median duration of survival follow-up is approximately 40 weeks (range, 2 to at least 85 weeks).
Ø In the 54 patients evaluable for safety, MPDL3280A was generally well tolerated. Fatigue, nausea, fever, decreased appetite, and asthenia were the most common treatment-related adverse events, Dr Emens reported. Grade 3 treatment-related adverse events were seen in 11% of patients. There was one case of grade 4 pneumonitis. The cause of two deaths is currently being investigated. - However, so far, the immunotherapy trials reported at SABCS were not particularly
impressive.