Embed Size (px)
Citation preview
CHAPTER III
METHODOLOGY
3.1 Research Design:
A research design is the arrangement of conditions for collection and analysis of data in a
manner that aims to combine relevance to the research purpose with economy in
procedure (Kumar, 2008).
The purpose of the present study was:
1. To analyze the gait pattern in post stroke hemiparetic patients
2. To correct the gait pattern in post stroke hemiparetic patients
Accordingly, the study was carried out in two phases:
Phase I: Analysis of gait pattern in post stroke hemiparetic patients
In this phase of study, gait parameters were analyzed in post stroke hemiparetic patients
and then compared with healthy asymptomatic subjects (control group).
Phase II: Correction of gait pattern in post stroke hemiparetic patients
In the 2nd
phase of study, four different types of interventional programs namely, NDT
based gait training; strengthening exercises of lower limb musculature; static cycling; and
conventional physiotherapy were administered for 8 weeks and then compared to
examine their efficacy on the correction of gait pattern in post stroke hemiparetic
patients.

3.2 Nature of study:
Figure 3.1: Flowchart showing the nature of study
Nature of Study
Interventional in
nature Descriptive in
nature
Phase I Phase II
Descriptive research is a most basic type
of enquiry that aims to observe certain
phenomena, typically at a single point in
time.
The aim is to examine a situation by
describing important factors associated
with that situation, such as
demographic, socio-economic, and
health characteristics, events, behaviors,
attitudes, experiences, and knowledge
(Kelley, et al., 2003).
In an intervention study, the subjects are
selected from one population with a
particular characteristic present; then,
immediately after baseline, the total study
group is split up into a group that
receives the intervention and a group that
does not receive that intervention (control
group).
The comparison of the outcomes of the
two groups at the end of the study period
is an evaluation of the intervention
(Everitt & Howell, 2005).
3.3 Research setting:
The study was performed at Ur Physio Physiotherapy Clinic, Jalandhar
3.4 Ethical approval and Consent:
The study was approved by the Board of Post Graduate Studies and Research (Faculty of
Medicine), Punjabi University, Patiala vide letter No. 553/ Research dated 15th
January,
2008 (Annexure I). The subjects were thoroughly explained about the procedure prior to
participation in the study and their informed written consent was taken (Annexure II).
3.5 Duration of study:
For phase I, the duration of the study was from August 2007 to December 2009.
For phase II, the study started in September 2007 and completed in January 2013.

3.6 Sample selection:
Figure 3.2: Flowchart showing the sample selection of study
Participants
Non paretic healthy
asymptomatic controls
Post stroke hemiparetic
patients
Residential colonies
Guru Gobind Singh Nagar
Guru Teg Bahadur Nagar
Model House
Model Town
Doordarshan enclave
Bhargav Nagar
Residential colonies
Guru Gobind Singh Nagar
Guru Teg Bahadur Nagar
Door Darshan Enclave
Model Town
Model House
Basti Sheikh
Basti Guzan
Bhargav Nagar
Urban estate
Tagore Nagar
Saraswati Vihar
Raja Garden
Rose Park
Sant Nagar
Clinics and Hospitals
Ur Physio Physiotherapy Clinic, Jalandhar
Department of Physiotherapy, Lovely
Professional University, Phagwara
Lovely Physiotherapy OPD, Lovely
Autos, Phagwara.
Guru Teg Bahadur Charitable Hospital,
Jalandhar
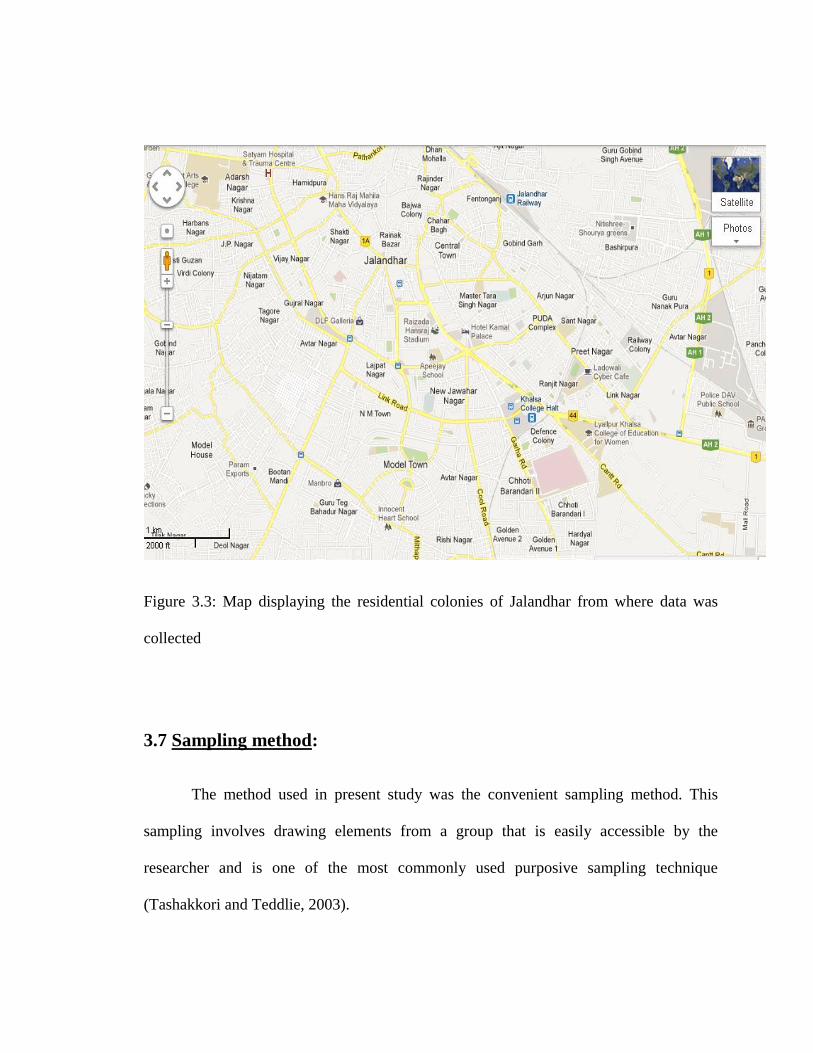
Figure 3.3: Map displaying the residential colonies of Jalandhar from where data was
collected
3.7 Sampling method:
The method used in present study was the convenient sampling method. This
sampling involves drawing elements from a group that is easily accessible by the
researcher and is one of the most commonly used purposive sampling technique
(Tashakkori and Teddlie, 2003).

3.8 Sample size:
For Phase I, the sample size was of 30 in patient group and 30 in control group.
For Phase II, the sample size was of 20 in each interventional group (The sample
size was calculated as per the formula given in Annexure IV).
Thus, eighty post stroke hemiparetic patients in total.
3.9 Sampling criteria:
The subjects were included acoording to the inclusion criteria described in Figure 3.4.
Figure 3.4: Flowchart showing the inclusion criteria
Non paretic healthy
asymptomatic subjects
Post stroke hemiparetic
patients
1. Age 40-70 years
2. Both males and females
3. Alert and able to follow
commands
4. Able to walk independently
5. Cooperative and compliant
in gait analysis
1. Affected for a period of 4-6 weeks
2. Both males and females
3. Aged 40-70 years
4. Hemiparesis secondary to CVA
5. Having no more than one CVA prior
to testing
6. Able to walk more than 10 meters
with or without gait aid
7. Cooperative and compliant in gait
analysis
8. Alert and able to follow commands
Inclusion criteria
The subjects were excluded according to the following exclusion criteria as described in
Figure 3.5
Figure 3.5: Flowchart showing the exclusion criteria
Non paretic healthy
asymptomatic subjects
Post stroke hemiparetic
patients
Exclusion criteria
1. Comorbid conditions such as disabling
arthritis, amputation, limb length
discrepancy or severe cardiovascular
disease
2. Acute illness
3. Active inflammatory or pathological
changes in the joints of the lower limbs,
or foot deformities (such as pes valgus,
pes cavus, hallux valgus or hallux
rigidus) in the previous 6 months; and
4. History of syncope.
1. Hemiplegia due to trauma, brain tumor
or secondary etiology
2. Completely recovered from the stroke
3. Comorbid conditions such as disabling
arthritis, Parkinson’s disease,
amputation, patients with limb length
discrepancy or severe cardiovascular
disease
4. Acute illness
5. Active inflammatory or pathological
changes in the joints of the lower limbs,
or foot deformities (such as pes valgus,
pes cavus, hallux valgus or hallux
rigidus) in the previous 6 months
6. History of syncope
7. Non-ambulatory
8. Severe visual spatial dysfunction.
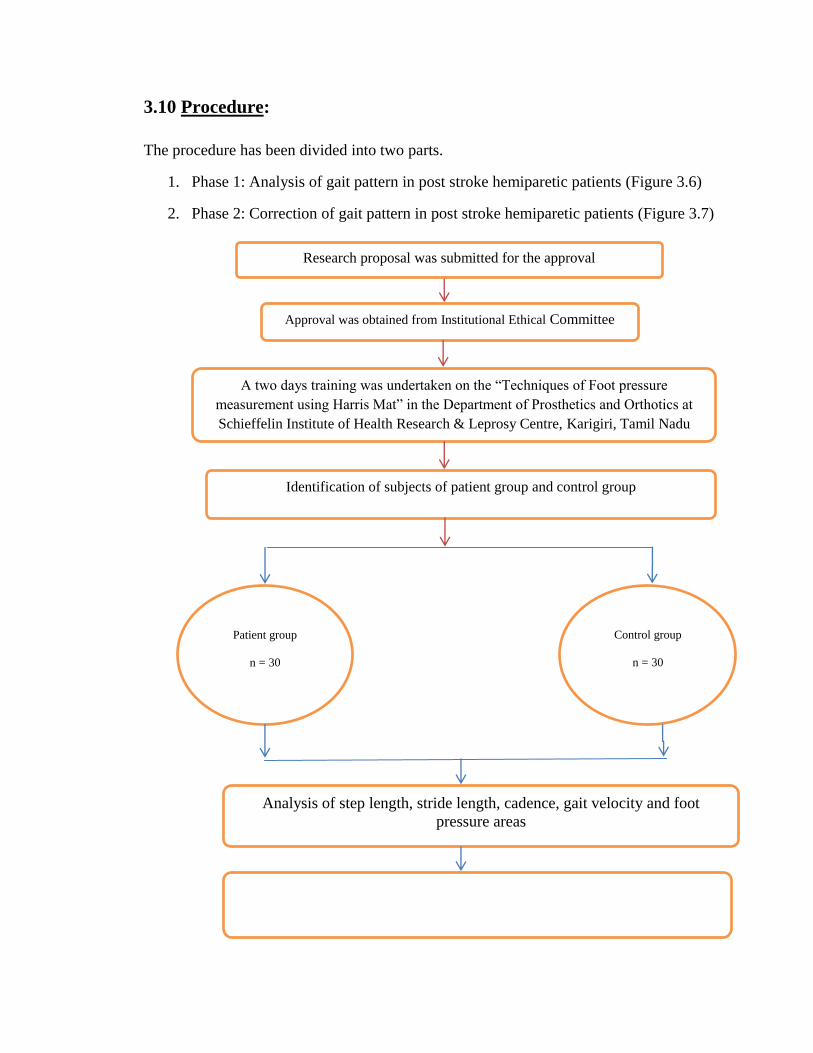
3.10 Procedure:
The procedure has been divided into two parts.
1. Phase 1: Analysis of gait pattern in post stroke hemiparetic patients (Figure 3.6)
2. Phase 2: Correction of gait pattern in post stroke hemiparetic patients (Figure 3.7)
Identification of subjects of patient group and control group
Analysis of step length, stride length, cadence, gait velocity and foot
pressure areas
Comparison of gait pattern of patient group and control group
Approval was obtained from Institutional Ethical Committee
Patient group
n = 30
Control group
n = 30
A two days training was undertaken on the “Techniques of Foot pressure
measurement using Harris Mat” in the Department of Prosthetics and Orthotics at
Schieffelin Institute of Health Research & Leprosy Centre, Karigiri, Tamil Nadu
Research proposal was submitted for the approval

Figure 3.6: Flowchart showing the procedure of analysis of gait pattern of post stroke
hemiparetic patients of the present study
All thirty patients of Phase I gave their consent to
participate further in the interventional study
Group A (n= 20) NDT
Based Gait Training with
conventional
physiotherapy (Annexure
6)
Group B (n= 20) Lower
limb Strengthening
exercises with
conventional
physiotherapy (Annexure
7)
Group C (n = 20)
Static Cycling along
with conventional
Physiotherapy
(Annexure 8)
Group D (n = 20)
Conventional
physiotherapy
alone
(Annexure 9)
Intervention was carried out for eight weeks at a frequency of 5 days per week
Another 50 patients were identified to n = 80
Group A Started on
8th Sep 2007 and
ended on 23rd Dec
2012
Group B Started on
15th March 2008 and
ended on 27th Dec
2012
Group C started on
20th Nov 2008 and
ended on 14th Jan
2013
Group D started on
10th Nov 2007 and
ended on 4th Nov
2012
All 80 patients were evaluated thoroughly
Then divided into four groups
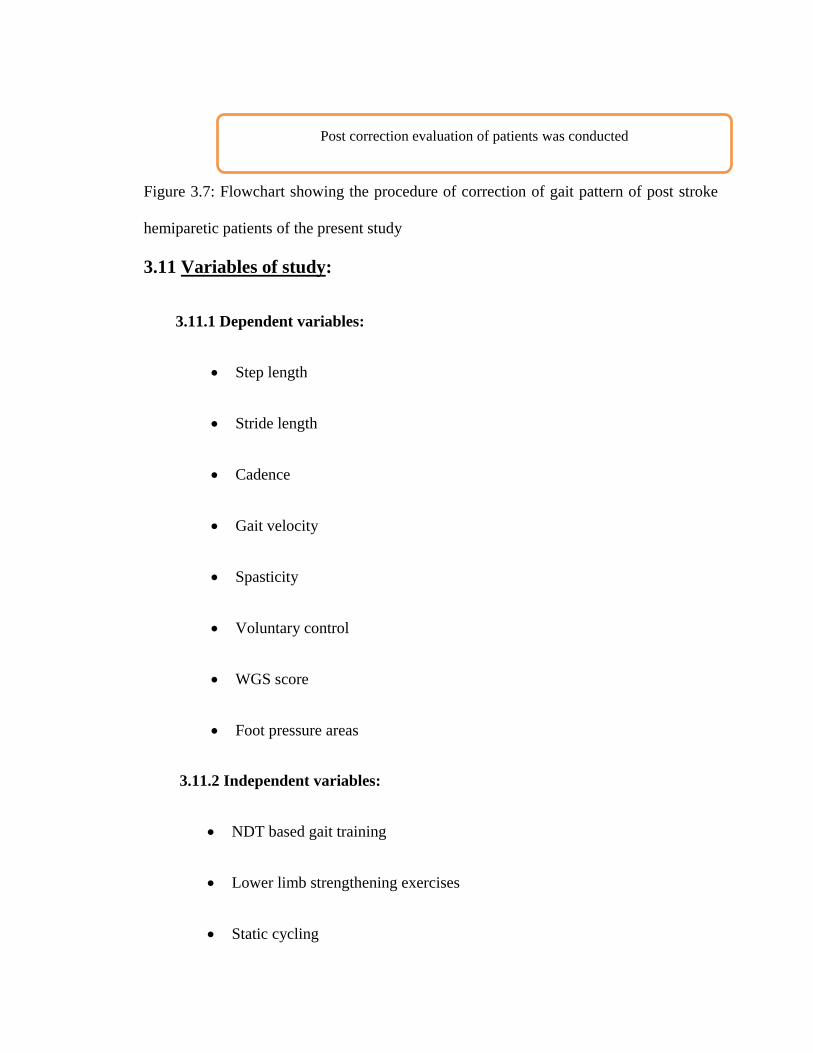
Figure 3.7: Flowchart showing the procedure of correction of gait pattern of post stroke
hemiparetic patients of the present study
3.11 Variables of study:
3.11.1 Dependent variables:
Step length
Stride length
Cadence
Gait velocity
Spasticity
Voluntary control
WGS score
Foot pressure areas
3.11.2 Independent variables:
NDT based gait training
Lower limb strengthening exercises
Static cycling
Post correction evaluation of patients was conducted
Conventional physiotherapy
3.12 Tools used:
Harris mat
Ink, roller and chart paper
Marker
Measuring tape
Stop watch
WGS Scale
MAS
Brunnstrom stages of motor recovery classification
3.13 Description of tools:
3.13.1 Harris Mat:
The Harris mat was developed by R.I. Harris and is a rubber mat stretched
across a support frame. The mat has a rough side which consists of ridges of three
different heights lined up in two planes. A light pressure is indicated by only the
large ridges printing, whereas a heavier pressure will progressively print the
smaller and then the smallest ridges in addition to the large ridges (Silvino et al.,
1980). Thus, this mat prints light foot pressure in large, light squares (formed by
tall grid ridges) and heavier pressures in dark, smaller squares (deep ridges). At a
very high pressure, a blotting of ink will obliterate the squares formed by the
ridges. The darker areas are areas of high pressure. It gives a grid analysis of
pressure distribution at a relatively low cost per patient and can be used for static
and dynamic assessment (Sussnan and Batesensen, 2007). This foot printing
technique has been used in clinical studies. The mat is inexpensive, easily used,
and very practical for the clinician. It provides a permanent record of the
distribution of pressure under the foot in an analog mode (Silvino et al., 1980).
For the purpose of taking foot imprints, a portable wooden platform was
constructed in which the Harris mat could be placed. The patient walks on the
platform and steps over the Harris mat which is embedded into the platform so
that there is no height difference between the mat and platform. The patient is thus
able to walk without being conscious.
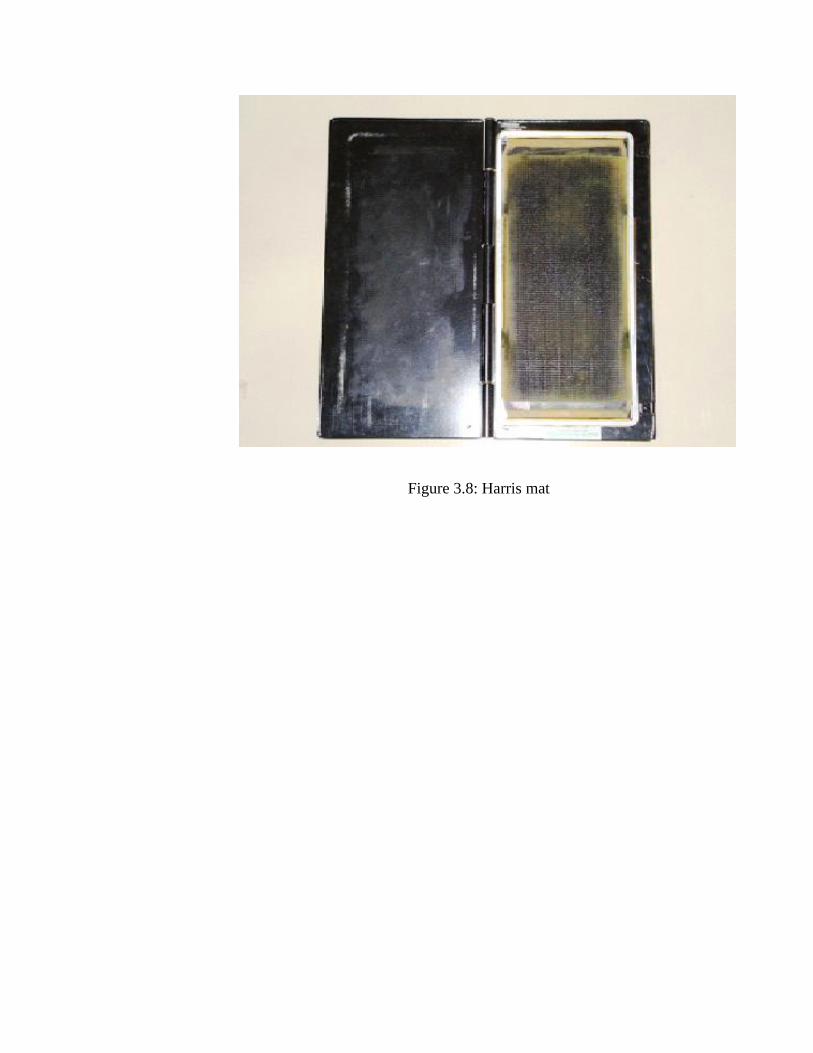
Figure 3.8: Harris mat
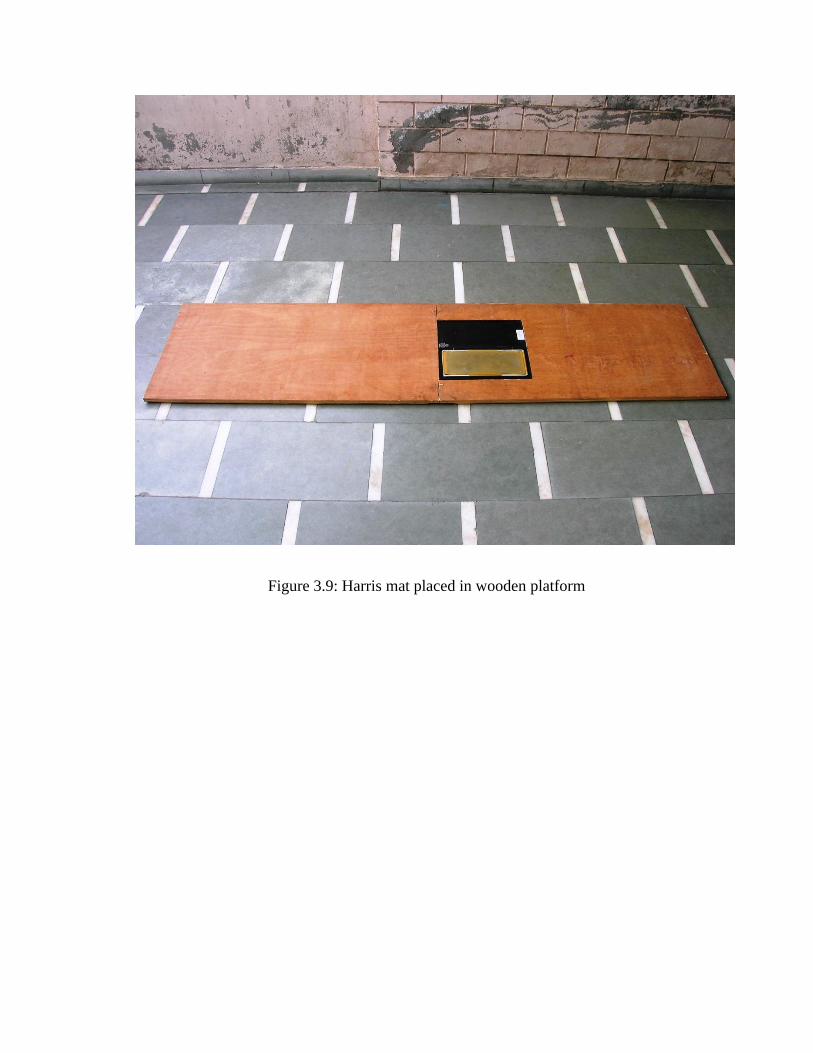
Figure 3.9: Harris mat placed in wooden platform

3.13.2 Ink, roller and chart paper:
The ink was used for application over the Harris mat for the purpose of taking the
foot imprints. The ink was also used for taking the foot prints of the subjects while
walking over the floor in order to calculate step length and stride length. A roller
was required to apply the ink over the Harris mat. The white chart papers were
used for taking the foot imprints using Harrris mat.
3.13.3 Marker:
A marker was used to mark the points over the floor in order to calculate the step
length, stride length and gait velocity.
3.13.4 Measuring tape:
A measuring tape having units of measurement in centimeters was used to
measure the step length, stride length and walking distance for calculation of gait
velocity.
3.13.5 Stop watch:
A stop watch was used in order to calculate the time taken to walk the required
distance for calculation of gait velocity in seconds.
3.13.6 Wisconsin Gait Scale (WGS):
The Wisconsin Gait Scale (WGS), developed in 1996, is a 14-item scale intended
to measure clinically relevant components of gait in persons with stroke
(Annexure V). The WGS uses an ordinal scale to categorize the findings from

Observational Gait Analysis (OGA). WGS can be used to evaluate the gait
problems experienced by a patient with hemiplegia following stroke. This can be
used to monitor the effectiveness of rehabilitation training. WGS proved to have
high intra-rater and inter-rater reliability when administered by physiatrists with
neuro-rehabilitative expertise (Rubertone, et al., 2000; Wellmon, et al., 2003).
The scale consists of four basic measures: -
1. Stance phase of the affected leg.
2. Toe off the affected leg.
3. Swing phase of the affected leg.
4. Heel strike of the affected leg.
The subject is made to walk as observations of the subject are done:
(1) Walking towards the observer
(2) Walking away from the observer
(3) From the side
Each of these measures further consisted of sub-measures as follows: -
I. Stance phase of the affected leg has five sub- measures:
(1) Use of hand held gait aid.
(2) Stance time on impaired side.
(3) Step length of the unaffected side.
(4) Weight shift to the affected side with or without gait aid.
(5) Stance width.
II. Toe off the affected leg has 2 sub-measures: -
(6) Guardedness.
(7) Hip extension of affected side.
III. Swing phase of the affected leg has six sub measures:
(8) External rotation during initial swing.
(9) Circumduction at mid swing.
(10) Hip hiking at mid swing.
(11) Knee flexion from toe off to mid swing.
(12) Toe clearance.
(13) Pelvic rotation.
IV. Heel strike of the affected leg has one sub-measure:
(14) Initial foot contact.
Interpretation:
Minimum score: 13.35
Maximum score: 42
The higher the score the more seriously affected the gait.
3.13.7 Modified Ashworth Scale (MAS):
The Modified Ashworth Scale is a 6-point rating scale that is used to measure
muscle tone. It is a widely used qualitative scale for the assessment of spasticity;
measures resistance to passive stretch (Elovic et al., 2004). The measurements
obtained with the MAS, when a standardized procedure is used in the lower limbs
of people with stroke, have acceptable intrarater reliability on the grade of 0
(Blackburn et al., 2002). This scale has a minimum score of 0 indicating no
increase in tone and maximum score of 4 indicating severe spasticity (Annexure
VI).
3.13.4 Brunnstrom stages of motor recovery:
The voluntary motor control of the lower limb was assessed using the Brunnstrom
stages of motor recovery (Annexure VII).
3.14 Procedure of quantification of gait parameters:
The gait pattern was assessed within a week after the patient had resumed
walking, which was defined as the ability to walk ten to fifteen meters without the
assistance of another individual, with or without gait aid. All subjects, post stroke
hemiparetic patients as well as controls, were instructed to walk along a smooth,
horizontal 10 m long walkway at a comfortable speed.

3.14.1 Quantification of foot pressures using Harris mat:
A wooden platform was constructed in which the Harris mat could be placed and
the subject could step over the Harris mat smoothly without any constraint. The Harris
mat was positioned in the center of the wooden platform and the subject was made to
walk over the platform and instructed to place the foot over the mat while walking. In this
way the foot imprint was taken for both the paretic and non-paretic sides. Later the foot
imprints were analyzed and high pressure and low pressure areas were calculated by
dividing the foot imprint into three parts – Upper part, middle part and lower part.
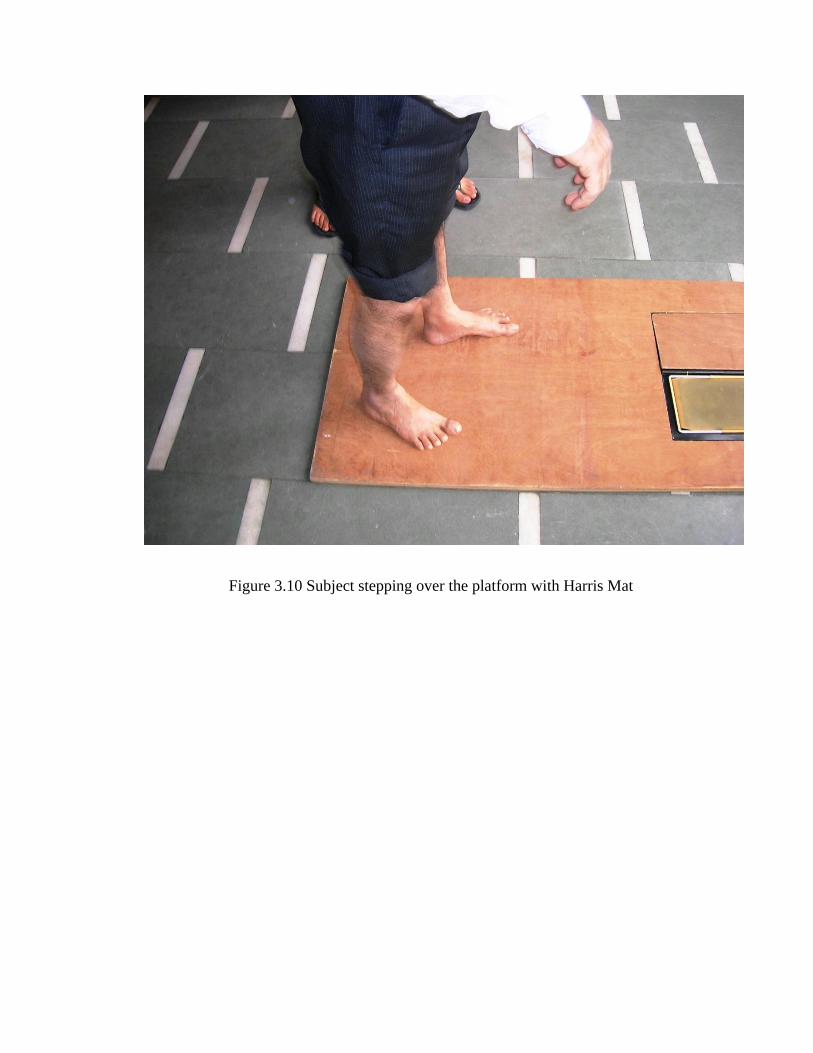
Figure 3.10 Subject stepping over the platform with Harris Mat
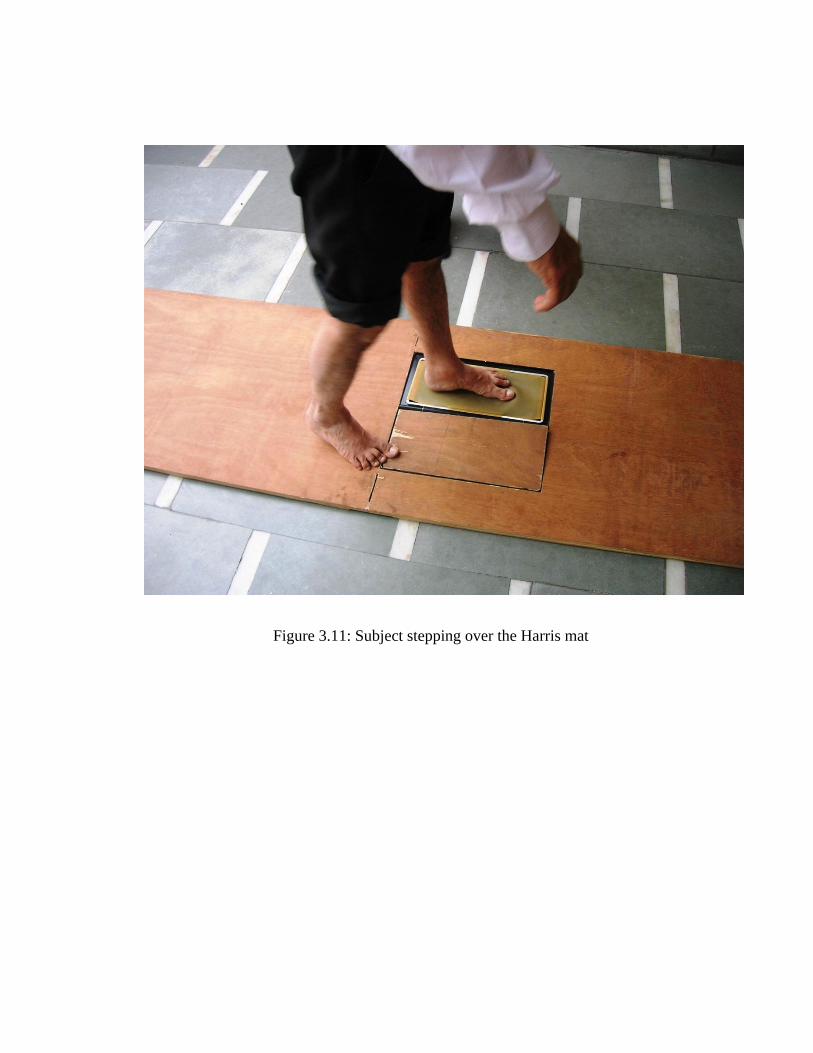
Figure 3.11: Subject stepping over the Harris mat
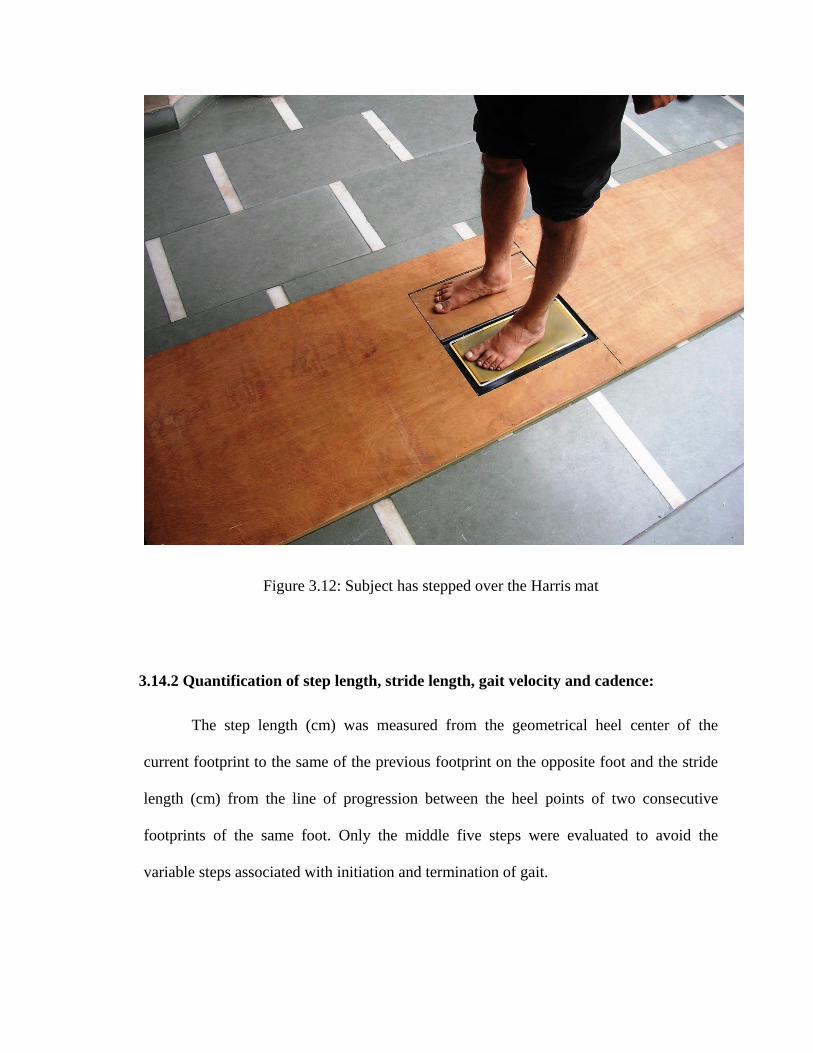
Figure 3.12: Subject has stepped over the Harris mat
3.14.2 Quantification of step length, stride length, gait velocity and cadence:
The step length (cm) was measured from the geometrical heel center of the
current footprint to the same of the previous footprint on the opposite foot and the stride
length (cm) from the line of progression between the heel points of two consecutive
footprints of the same foot. Only the middle five steps were evaluated to avoid the
variable steps associated with initiation and termination of gait.
For calculation of gait velocity, the subject was instructed to walk in a straight
pathway and the middle 10 meters distance was considered for calculation of gait
velocity. A line was marked indicating the start of the 10 meters and termination of the
10 meters. The time taken to cover this 10 meters distance was recorded. The walking
velocity (cm/s) was obtained after dividing the recorded 10 meters distance by the
ambulation time recorded for this distance.
The cadence was calculated by asking the subject to walk for one minute through
a straight pathway with self-selected speed and then calculating the number of steps taken
during one minute. This distance walked was independent of the 10 m walkway.
3.14.3 Assessment of Wisconsin Gait Scale (WGS) score:
The post stroke hemiparetic patients were examined while walking without the
assistance of orthotic devices, but were allowed to use a gait aid. Each subject was
observed walking towards, walking away from the investigator and from the side.
The parameters were scored in comparison to the normal side. For example, one
of the patients used no gait aid. So he was given 1 point for the first sub measure use of
hand held gait aid. For the second sub measure of stance time on impaired side, he was
given 2 points as his time spent on affected side was unequal as compared to time spent
on unaffected side during single leg stance. Similarly, he was given 3 points for the
seventh sub measure as there was marked hip extension of affected side. For the ninth sub
measure, he was given 2 points, as there was moderate circumduction at mid swing.
However, there was no knee flexion from toe off to mid swing. Therefore, he was given 4
points for the eleventh sub measure. As he was having foot flat on initial foot contact, he
was given 2 points for the fourteenth sub measure. In this way, the scoring was done
using the WGS.
3.14.4 Assessment of spasticity of lower limb musculature:
The spasticity was assessed in Hip adductors, Knee extensors and ankle plantar
flexor muscles. Each subject was put in a resting position for 5 minutes, with socks and
shoes removed. The handling and positioning of the subject’s limbs by the investigator
are described in Annexure VIII. Each test movement was performed over a duration of
about 1 second (by counting “one thousand one”), as described by Bohannon and Smith
(1987). The movement was repeated 3 times because once may not be sufficient for a
rater to attribute a score. After performing the 3 test movements, the investigator graded
the resistance felt, with a single score, according to the MAS.
3.14.5 Assessment of voluntary control of lower limb musculature:
Voluntary control of lower limbs was assessed by using the stages of motor
recovery classification given by Brunnstrom (Annexure VII).
3.15 Gait correction interventions:
3.15.1 NDT based gait training:
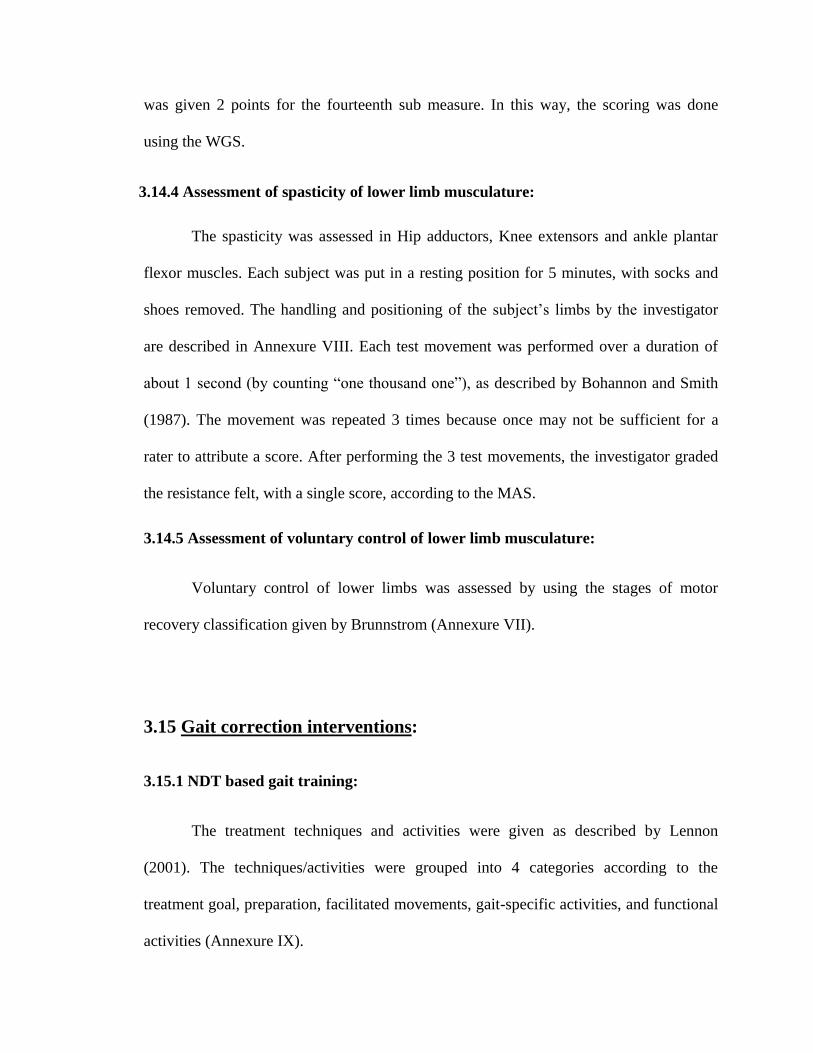
The treatment techniques and activities were given as described by Lennon
(2001). The techniques/activities were grouped into 4 categories according to the
treatment goal, preparation, facilitated movements, gait-specific activities, and functional
activities (Annexure IX).
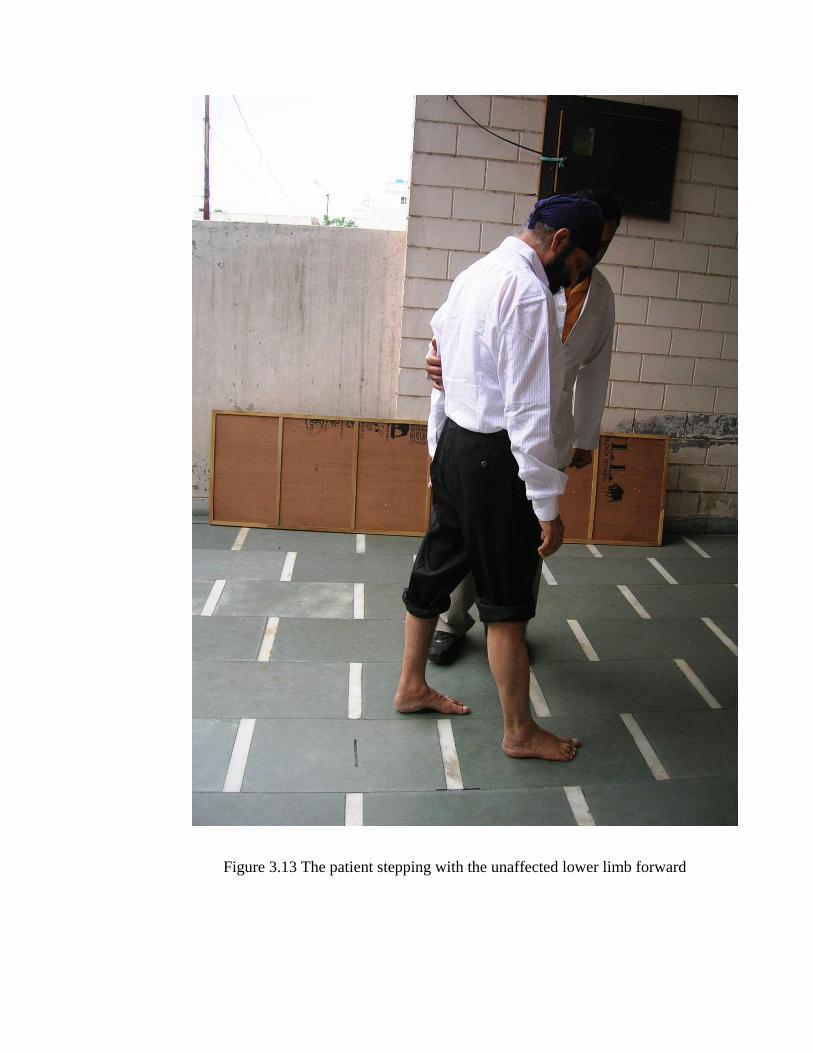
Figure 3.13 The patient stepping with the unaffected lower limb forward

Figure 3.14 The patient stepping with the unaffected lower limb on and off a step

3.15.2 Lower limb strengthening:
The lower limb strengthening protocol required each patient to isotonically exercise the
affected LE using external resistance (Sullivan et al., 2007). The strengthening was done
for six specific muscle groups (hip flexors, hip extensors, knee flexors, knee extensors,
ankle dorsiflexors, and ankle plantar flexors) (Annexure X).
Figure 3.15 The patient being given strengthening exercises for knee flexors
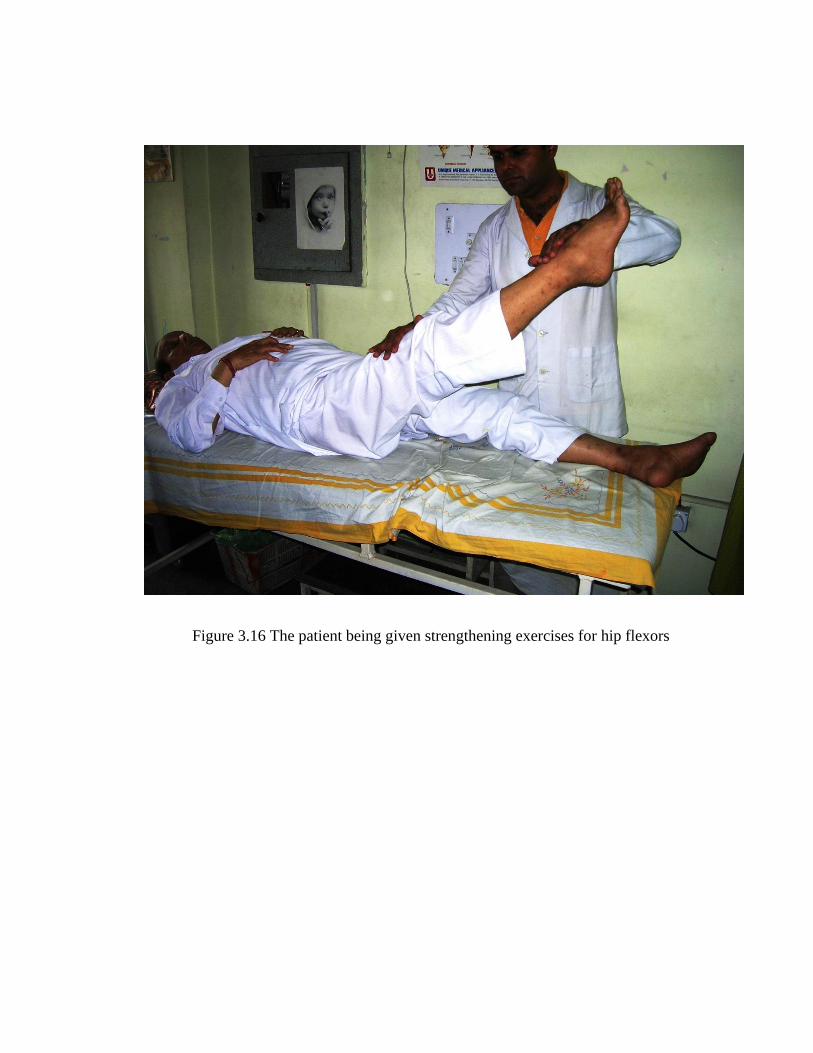
Figure 3.16 The patient being given strengthening exercises for hip flexors

3.15.3 Static cycling:
A static cycler was used for providing gait correction to the group C. The patients were
seated on a static cycle and were asked to complete 10 sets of 15 to 20 revolutions in each
session. They were given at least 2 minutes to rest between sets (Sullivan et al., 2007)
(Annexure XI).
Fig 3.17 The patient performing static cycling

Fig 3.18 The patient performing static cycling
3.15.4 Conventional physiotherapy:
The conventional physiotherapy gait correction program comprised of the exercises in
anatomical planes, passive movements, active movements, passive stretching exercises
etc. (Dickstein et al., 1986). (Annexure XII).
Figure 3.19 The subject being given stretching of hamstrings (Conventional
physiotherapy)
Figure 3.20 The patient being given passive movements (Conventional physiotherapy)
3.16 Dropouts:
The following is the detail about the dropouts in each group:
Group A Group B Group C Group D
1 2 2 3





























