Embed Size (px)
Citation preview

OUTBREAK MANAGEMENT IN
RESIDENTIAL CARE FACILITIES
(RCFS)
Metro South Public Health Unit
Dr Bhakti Vasant (Public Health Physician) and Deb Judd (Public Health Nurse)
LEARNING OUTCOMES
1.Definition of an outbreak
2.Potential causes
3.Outbreak recognition
4.Outbreak management
5.Resources
Image source: http://nursing-issues.com/nursing-issues/aged-care-facilities/attachment/elderly-people-2/
Outbreak Management Guidelines

DEFINITION OF AN OUTBREAK
“Occurrence of more cases of disease than expected in a given area among a specific
group of people over a particular period of time”
“Two or more linked cases of the same illness”
NHMRC Australian Guidelines for the Prevention and Control of Infection in Healthcare
(2010) pp. 121

POTENTIAL CAUSES OF OUTBREAKS IN
RCFS• Viruses, bacteria and parasites
– Viruses are most common
• Respiratory virus infection
– Influenza, Parainfluenza, HMPV, RSV, Rhinovirus
• Gastrointestinal infection
– Viruses: Norovirus, Sapovirus, Adenovirus, Rotavirus
– Bacteria: Salmonella, Camplyobacter, E. coli
– Parasites: Giardia, Cryptosporidium
• Can only be definitively identified by laboratory testing
Slide: West Morton Public Health Unit
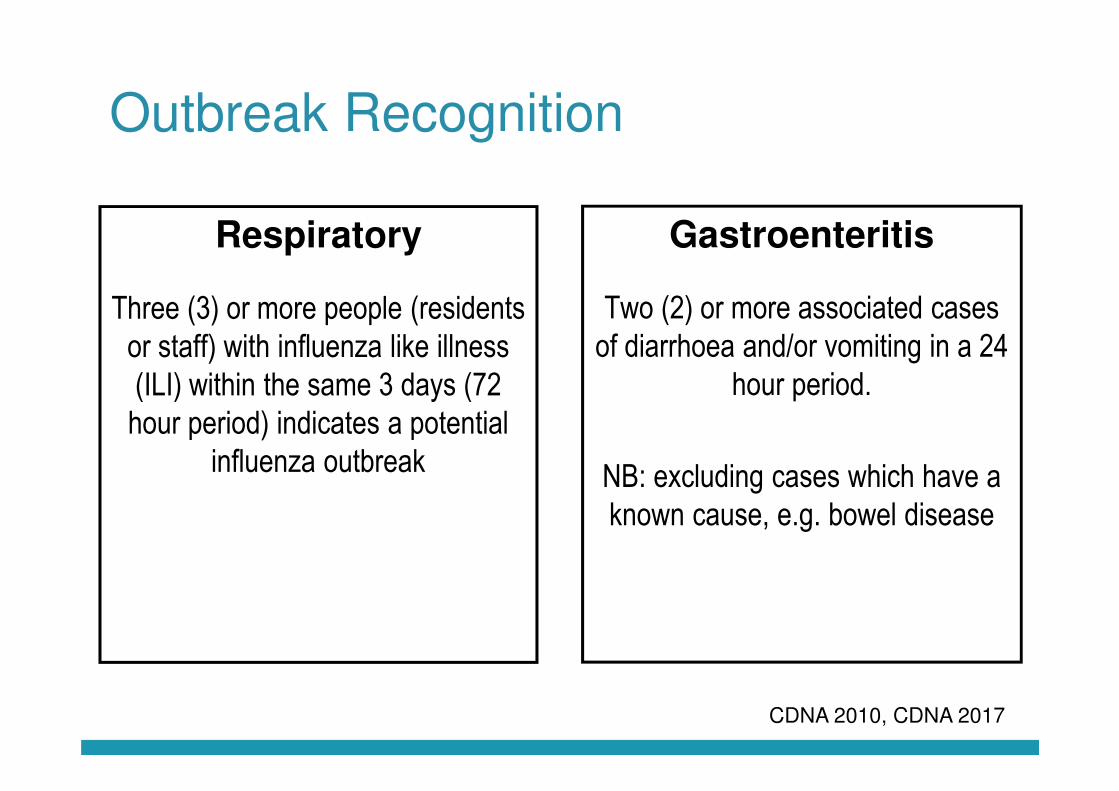
Outbreak Recognition
Respiratory
Three (3) or more people (residents or staff) with influenza like illness (ILI) within the same 3 days (72 hour period) indicates a potential
influenza outbreak
Gastroenteritis
Two (2) or more associated cases of diarrhoea and/or vomiting in a 24
hour period.
NB: excluding cases which have a known cause, e.g. bowel disease
CDNA 2010, CDNA 2017

CASE DEFINITIONS
Respiratory (influenza like illness (ILI))
•Sudden onset of symptoms
•And at least one of the following three respiratory symptoms
– Cough (new or worsening)
– Sore throat
– Shortness of breath
•And at least one of the following four systemic symptoms
– Fever or feverishness - Headache
– Malaise - MyalgiaCDNA 2017

CASE DEFINITIONS
Gastroenteritis (Suspected)
•Three or more loose stools or bowel movements in a 24 hour period that are different from normal
and/or
•Two or more episodes of vomiting in a 24 hour period
CDNA 2010
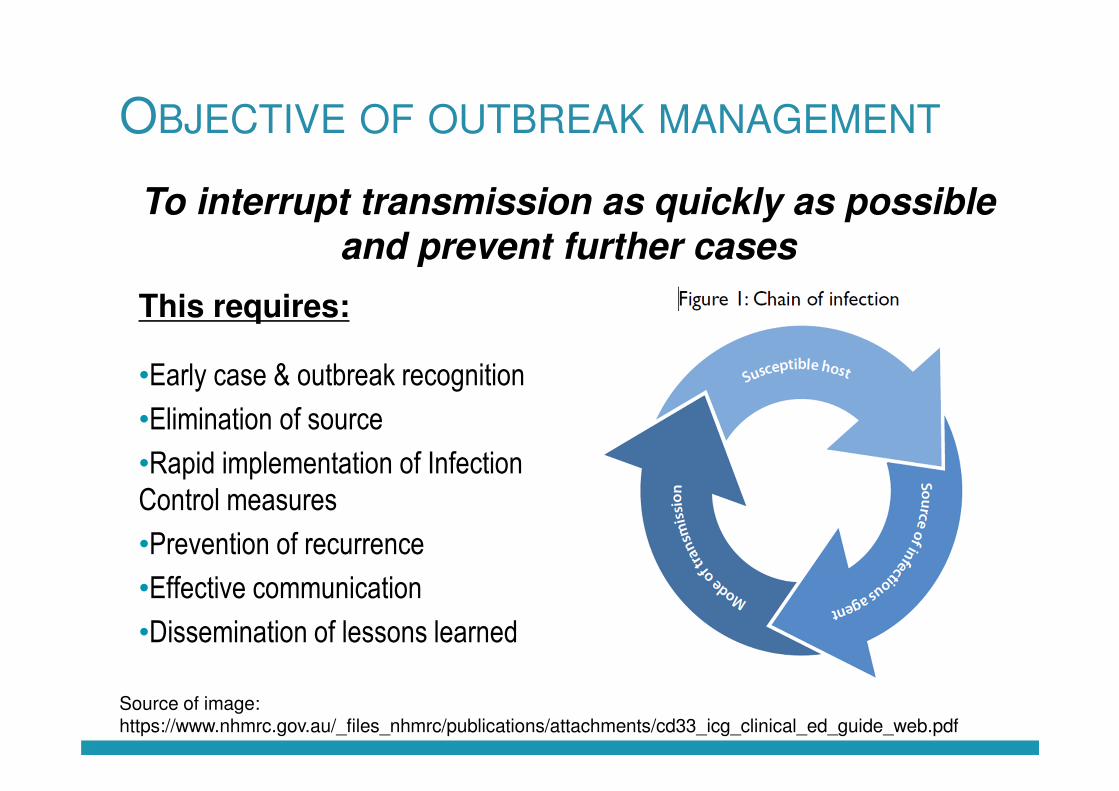
OBJECTIVE OF OUTBREAK MANAGEMENT
This requires:
•Early case & outbreak recognition
•Elimination of source
•Rapid implementation of Infection Control measures
•Prevention of recurrence
•Effective communication
•Dissemination of lessons learned
Source of image: https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/cd33_icg_clinical_ed_guide_web.pdf
To interrupt transmission as quickly as possible
and prevent further cases

MANAGEMENT OF SINGLE CASES
• Isolate resident or exclude staff member
• Apply appropriate infection control measures (e.g PPE)
• Review outbreak management plan and vaccination status
of residents and staff (influenza)
• Be vigilant for further cases

Outbreak Management
Four Phases of Outbreak Management
1. PREPARATION – Outbreak Management Plan
2. RESPONSE – Activation of the plan
3. MONITORING – Assess and modify the plan
4. CONCLUSION – Declare outbreak over, debrief and update Outbreak Management Plan
CDNA 2017

PHASE 1: PREPARATION
Resources
•Develop/Update Outbreak Management Plan (OMP)•Develop/Update IC Policies•Include a medical practitioner in the development of the OMP – antivirals
Tools
•Ensure adequate stock of Personal protective equipment (PPE) – how will you obtain further stock•Cleaning materials •Pathology collection onsite – swabs, faecal pots are in date•Outbreak kit
Early Detection
•Develop/Maintain system for detection of staff/resident illnesses•Consider active surveillance for cases •Develop a tool for recording cases
Communication•Consider how you will communicate to staff, residents, relatives, …•Consider how you will communicate and notify your GPs, service providers, hospitals, QAS, …

PHASE 1: PREPARATION
Vaccination
•RCFs should aim to achieve 95% Influenza vaccination rates for staff and residents annually…think how is your facility going to achieve this? (Education/communication strategies, vaccination clinics on-site..)•Compile vaccination register for staff and residents•Encourage visitors to have annual influenza vaccination
Antivirals
•Develop processes with attending GPs for antiviral prescriptions/standing orders prior to flu season•Consider GP assessment of renal function prior to Influenza season •Prepare for logistics of mass Tamiflu distribution (liaison with community pharmacy, staff training…)•Establish if GPs will be happy to prescribe tamiflu to unvaccinated staff members if required.
Staffing•Develop a staffing strategy•Consider the additional staffing will you required during an outbreak (cleaning, support, nursing)
Training
•Ensure staff receive training in outbreak management, are aware of relevant resources, and that these resources are readily accessible•Ensure that there are contingencies in place in case staff in outbreak management roles are absent/ill
Strategies for a successful RCF staff
vaccination program
• Provision of free or subsidised influenza vaccines
• Staff vaccination clinics at workplace
• Education to improve knowledge, help dispel vaccine
misconceptions – emphasis individual benefits
• Participation of local staff leaders and vaccine advocates
• Inclusion of recognition, rewards and incentives for
vaccinated staff
• RCF vaccination policies linked to broader infection
control policies and staff health programs
Share you experiences of what has worked
Image source: https://www.agedcareguide.com.au/talking-aged-care/better-flu-vaccines-wanted-for-the-vulnerable-elderly

PHASE 2: RESPONSE
•Notify GPs of suspected outbreak
•Implement infection control
•Request appropriate laboratory tests to confirm the diagnosis
•Collate a line listing
•Notify Public Health Unit
•Form an Outbreak Management Team (OMT)
IMMEDIATE

PHASE 2: RESPONSE
•Most important hygiene measure in
preventing spread
•Gloves are not a substitute for hand
washing
•Wash hands with soap and water
before and after contact with each
client, if hand washing facilities are
not available – use alcohol based
hand rub
Hand hygiene
Infection Control

PHASE 2: RESPONSE
Gloves
•When in direct contact with ill persons or
potentially contaminated surfaces likely.
•Change gloves and wash hands after each client
Masks
•When entering room or working within one metre
(flu). If risk aerosolisation vomit/faeces (gastro)
•Remove when leaving – Dispose - Wash hands
Gowns
•When soiling of clothes with respiratory secretions,
vomit, or faeces is possible
Eye Protection
•Where potential for splattering/spraying blood,
body fluids, secretions or excretions
Compliance with Precautions
Infection Control

PHASE 2: RESPONSE
What tests should I request?
•Gastroenteritis
– Faeces multiplex, MCS, Viral PCR including Rotavirus, Norovirus and Adenovirus
– Vomitus – Norovirus
•Respiratory
– Respiratory virus PCR
Ensure correct swabs used– check with pathology company
•How many specimens need to be collected?
– Generally - 7 – 8 specimens over the course of outbreak, public health may request additional specimens from time to time
Laboratory Testing
Image source: https://www.agedcareguide.com.au/talking-aged-care/better-flu-vaccines-wanted-for-the-vulnerable-elderly

PHASE 2: RESPONSE
Direct and oversee management of the outbreak
• Communication, dissemination of
information
• Staff support
• Resource allocation
• Monitor outbreak progress and initiate
changes in response, as required
Liaise with GPs and PHU
Evaluation
Outbreak Management Team (OMT)
Source of image: http://usattorneysblog.blogspot.com.au/2016/08/northern-illinois-nursing-home-receives.html

Phase 2: Response
Members:
Chairperson – co-ordinating Outbreak Control team meetings, setting times, agenda, delegating tasks
Secretary – organises meetings, notifies of changes, records and distributes minutes
Outbreak Co-ordinator – IC decisions of OMT carried out, coordinates actives to contain and investigate outbreak
Media spokesperson – provide information to the media
Visiting General Practitioner – identified during the planning phase
Outbreak Management Team (OMT)
PHASE 2: RESPONSE
Step One – Clean
Step Two – Disinfect
•Increase cleaning frequency – twice daily
•High touch areas may require more frequent cleaning after high usage times
•Clean with
– Neutral detergent followed by a bleach solution
(1000 ppm)
•In order for bleach to be effective:
– Sufficient contact time (10 minutes)
– Surfaces free of vomit/faeces or organic matter
– Dilution of bleach to made up fresh, just before
using (CDNA 2010)
EnvironmentalCleaning
Infection Control

PHASE 2: RESPONSE
Equipment
•Should be dedicated for use of an individual
resident
•If shared, items must be cleaned and disinfected
between each resident use.
Linen
•Soiled linen and clothing should be removed
immediately, placed in collection bag or leak proof
plastic bag at source – Alginate bags
•Laundered in hot water and detergent
•Dried on a hot setting in a dryer
•Use appropriate PPE when handling
Crockery and cutlery
•Idealy in dishwasher or with detergent + hot water and
dried
Environmental
Infection Control

PHASE 2: RESPONSE
Isolation and Cohorting
•Isolate ill residents to single rooms where
possible
•Attempt to separate ill people from well
(‘Cohorting’)
•Ensure ill residents - > 1 metre apart (draw
privacy screens where necessary)
•Separate toilet facilities (ill from well)
•Close common areas such as dining rooms,
communal living areas
•Cease group activities such as day trips...
Environmental
Infection Control
PHASE 2: RESPONSE
Staff
•Dedicated staff to look after ill persons
•Staff should not move between wings or other
areas
•Self monitor for symptoms – exclude if unwell
Respiratory illness
Unvaccinated staff
•Work only if well
•Care for well residents ONLY
•Wear a mask when attending to any resident
care (within 1 metre and change between
residents) OR asymptomatic and taking antiviral medication
•if staff have been working in an outbreak affected
area – should not be moved to other wings
Staff
Infection Control
Image source http://firetrainingcourse.com/residential-care-home-fire-training-course/
PHASE 2: RESPONSE
New admissions
Should be restricted – depending on extent of the
outbreak – maybe applied one floor or wing or
entire facility
Re-admission of affected residents
Require provision of appropriate accommodation,
care and infection control.
Re-admission of residents non affected residents
•Generally not recommended HOWEVER maybe
required once outbreak under control
•Consider factors - appropriate accommodation,
vaccination status, ability to protect returning
resident, IC measures, provision of antivirals…
Admission and Readmission
Infection Control

PHASE 2: RESPONSE
Visitors
•Suspend group social activities that involve visitors
such as musicians
•Postpone visits from non-essential external
providers
•Inform regular visitors and families – request
essential visits only – discourage unnecessary
visitors
Request visitors
•Visit one person only
•Enter and leave directly without spending time in
communal areas
•Hand hygiene and PPE
Visitor restriction and signage
Infection Control

PHASE 2: RESPONSE
• Should only be used in addition to other outbreak control measures –Infection Control
• Decision to administer antivirals as prophylaxis should be made by the OMT in collaboration with local public health unit.
Uses
• Treatment
• Prophylaxis
Antiviral Medication

PHASE 3: MONITORING
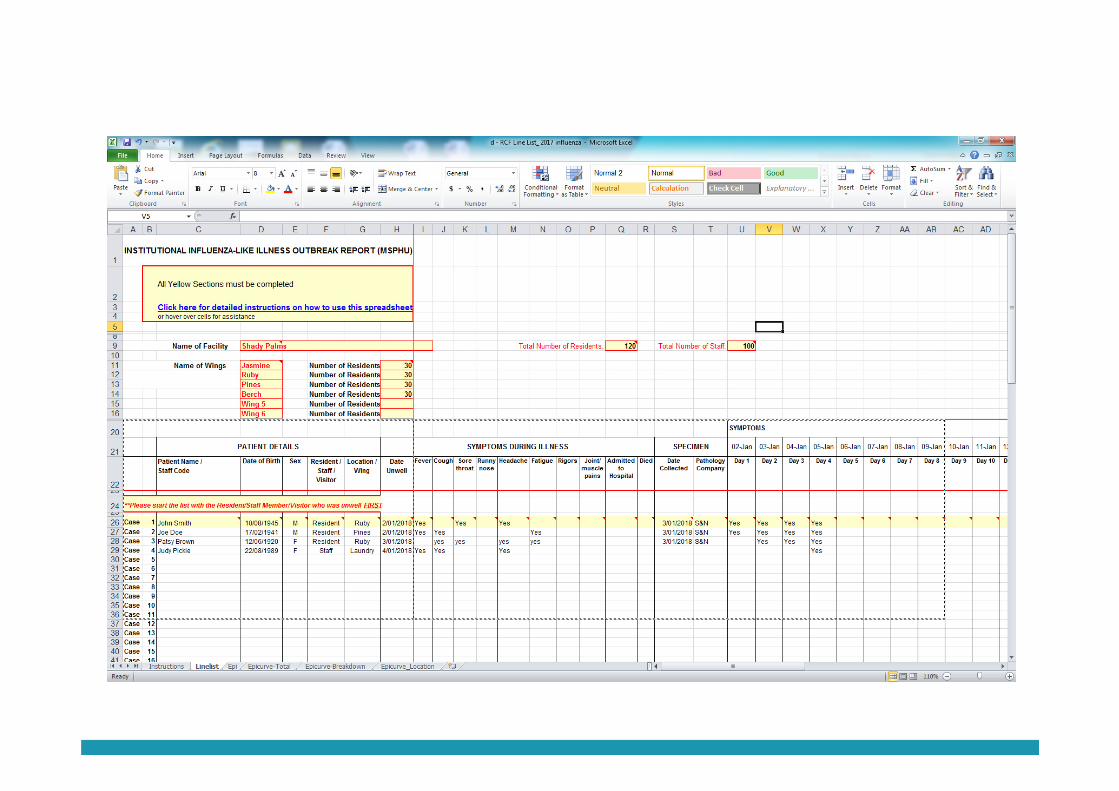
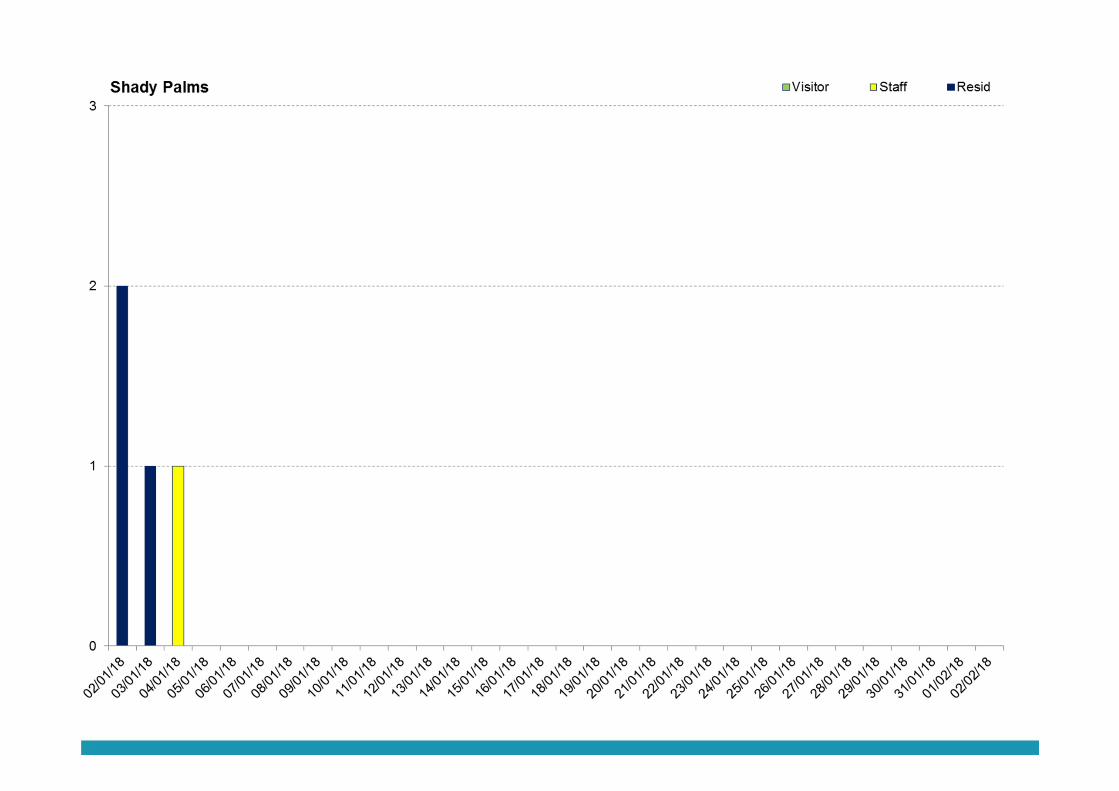
Line lists capture ongoing:
Resident surveillance
• Cases – initial and new
• Resident symptoms
• Status of ill residents – hospitalisations, recovered, deceased
• Record of antiviral usage
• Pathology results
Staff surveillance
• Cases – initial and new
• Status of ill staff – recovered, hospitalised
• Pathology results

Potential Challenges
• Implementation of Public Health recommendations difficult and expensive
for facility
• Building design not ideal to successful Infection Control
• Some RCF reluctant to move residents
• Residents with dementia
• Record keeping
• Transfer of residents, new admissions……
Source: Slide from West Morton Public Health Unit May 2017

Phase 3: Monitoring
PHASE 4: CONCLUSION• The OMT (with approval from public health) has the responsibility of declaring the
outbreak is over, and to communicate this to the RCF community
• Influenza - can be declared over if no new cases occur within 8 days following the onset of symptoms in the last resident case [8 days is the sum of the usual infectious period (5 days) plus maximum incubation period (3 days)].
• Gastroenteritis – can be declared over once the facility has reached 72 hours with no new cases, and no episodes of vomiting or diarrhoea at the facility.

PHASE 4: CONCLUSION
The Debrief:
• Identifies strengths and weakness of outbreak response
• Allows investigations of processes to ensure management of future outbreaks is improved
• Provides a formal avenue for resident and staff feedback
• Should involve all members of the OMT
• Lessons learnt can help to PREVENT future outbreaks

Outbreak management issues identified by
PHUs
• Lack of outbreak preparation and planning
• Late detection of outbreak within the facility
• Delays in implementing appropriate outbreak infection control practices
• Delays in cohorting staff and residents
• Inability to identify ongoing cases due to lack of knowledge of case definition
• Incorrectly collected specimens delaying diagnosis
• Delayed notification to public health
• Delayed return of request paperwork – line listing
• Tamiflu – lack of knowledge and timeliness in implementation
• Lack of notification to hospital of outbreak at RACF
• Lack of knowledge of appropriate cleaning products for gastroenteritis outbreak management

Infection Control issues
• Lack of appropriate Hand Hygiene
• Inappropriate use of PPE, especially masks
• Inappropriate storage of waste and ppe – bags
tied to/stored on banisters
• Inappropriately cleaning of shared equipment
• Lack of knowledge on the requirement for masks
to be worn by unvaccinated staff whilst attending
to patient care during outbreaks.

GUIDELINES
Guidelines for the public health management of gastroenteritis outbreaks due to norovirus or
suspected viral agents in Australia (CDNA 2010)
http://www.health.gov.au/internet/main/publishing.nsf/content/cda-cdna-norovirus.htm/$File/norovirus-guidelines.pdf
Guidelines for the Prevention, Control and Public Health Management of Influenza Outbreaks in
Residential Care Facilities in Australia (CDNA 2017)
http://www.health.gov.au/internet/main/publishing.nsf/Content/27BE697A7FBF5AB5CA257BF0001D3AC8/$File/RCF_Guidelines.pdf
Influ-info – Influenza kit for home care (Department of Social Services
2017)https://agedcare.health.gov.au/publications-articles/resources-learning-training/influ-info-influenza-kit-for-home-care
Australian Guidelines for the Prevention and Control of Infection in Healthcare (NHMRC 2010)
https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/cd33_infection_control_healthcare_140616.pdf
RESOURCES
Influenza in residential care facilities (QLD Health)
https://www.health.qld.gov.au/public-health/industry-environment/care-facilities/prevention/influenza-in-residential-care-facilities
Outbreak control measures for non-influenza respiratory viral illnesses in residential care facilities
(QLD Health)
https://www.health.qld.gov.au/public-health/industry-environment/care-facilities/prevention/non-influenza-respiratory-viral-illness
Influenza vaccination guidelines (QLD Health)
https://www.health.qld.gov.au/clinical-practice/guidelines-procedures/diseases-infection/immunisation/service-providers/influenza
The Australian Immunisation Handbook (Australian Govt)
http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/Handbook10-home~handbook10part4~handbook10-4-10
Hand washing for hygiene (QLD Health)
https://www.qld.gov.au/health/conditions/all/prevention/hand-hygiene

RESOURCES
Hand Hygiene Australia
Online learning package
http://www.hha.org.au/

QUESTIONS??

























