Embed Size (px)
Citation preview
Metro West Ambulance – Dispatch Operational Guidelines
Washington County, Oregon
2011 – Progressive Document Version: 1
Issued: April 12, 2011
2
TO: Metro West Ambulance – Dispatch Center FROM: Jonathan Chin, EMS Program Supervisor DATE: April 12, 2011 SUBJECT: Metro West Ambulance – Dispatch Operational Guidelines 2011 – Progressive Document
The culture of the Washington County EMS Community and the operational approach to EMS within the County have dramatically changed over the past four years. The current Control Center Protocols from 2007 are dated, and reflect a rigid and authoritarian infrastructure for providing oversight to the system. This is not the current environment or the future of EMS in Washington County. Dispatch operational guidelines will be developed collaboratively by the WCEO. As guidelines, they allow for flexibility in their application as determined by situational and operational needs. Acknowledging the need to update and convert the current protocols to guidelines, along with ongoing system enhancements which require support and direction from Metro West Ambulance Dispatch (MWA-D), the 2007 protocols have been reformatted and deemed guidelines. Reformatting and utilizing this document as an operational guide will accommodate progressive updating of each section independently. As a progressive document, it is a dynamic document which continually changes as individual sections are updated and revised, approved, and then implemented. Version 1, dated April 12, 2011, is the original reformatted document and contains no content changes. The Table of Contents has been restructured to track revisions, i.e., which sections have been updated and those remaining to be done. This progressive format will be used until the entire document has been updated. Thank you in advance for your cooperation and participation in this process.
3
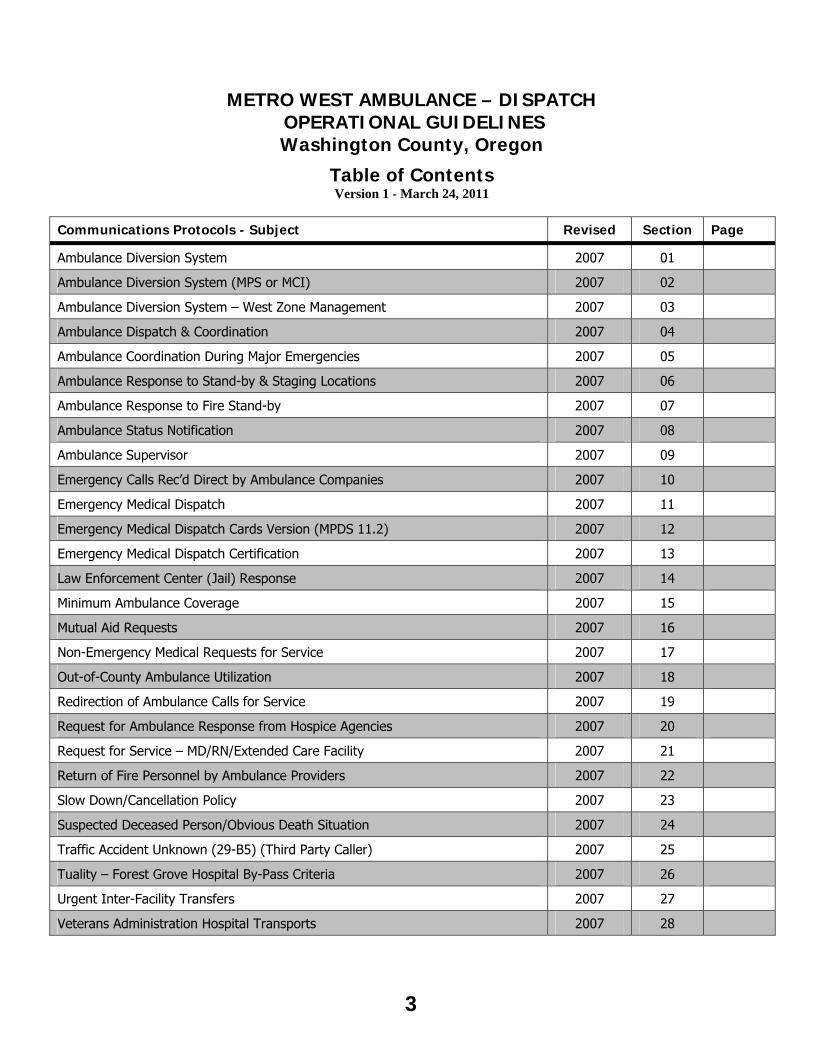
METRO WEST AMBULANCE – DISPATCH OPERATIONAL GUIDELINES Washington County, Oregon
Table of Contents Version 1 - March 24, 2011
Communications Protocols - Subject Revised Section Page
Ambulance Diversion System 2007 01
Ambulance Diversion System (MPS or MCI) 2007 02
Ambulance Diversion System – West Zone Management 2007 03
Ambulance Dispatch & Coordination 2007 04
Ambulance Coordination During Major Emergencies 2007 05
Ambulance Response to Stand-by & Staging Locations 2007 06
Ambulance Response to Fire Stand-by 2007 07
Ambulance Status Notification 2007 08
Ambulance Supervisor 2007 09
Emergency Calls Rec’d Direct by Ambulance Companies 2007 10
Emergency Medical Dispatch 2007 11
Emergency Medical Dispatch Cards Version (MPDS 11.2) 2007 12
Emergency Medical Dispatch Certification 2007 13
Law Enforcement Center (Jail) Response 2007 14
Minimum Ambulance Coverage 2007 15
Mutual Aid Requests 2007 16
Non-Emergency Medical Requests for Service 2007 17
Out-of-County Ambulance Utilization 2007 18
Redirection of Ambulance Calls for Service 2007 19
Request for Ambulance Response from Hospice Agencies 2007 20
Request for Service – MD/RN/Extended Care Facility 2007 21
Return of Fire Personnel by Ambulance Providers 2007 22
Slow Down/Cancellation Policy 2007 23
Suspected Deceased Person/Obvious Death Situation 2007 24
Traffic Accident Unknown (29-B5) (Third Party Caller) 2007 25
Tuality – Forest Grove Hospital By-Pass Criteria 2007 26
Urgent Inter-Facility Transfers 2007 27
Veterans Administration Hospital Transports 2007 28
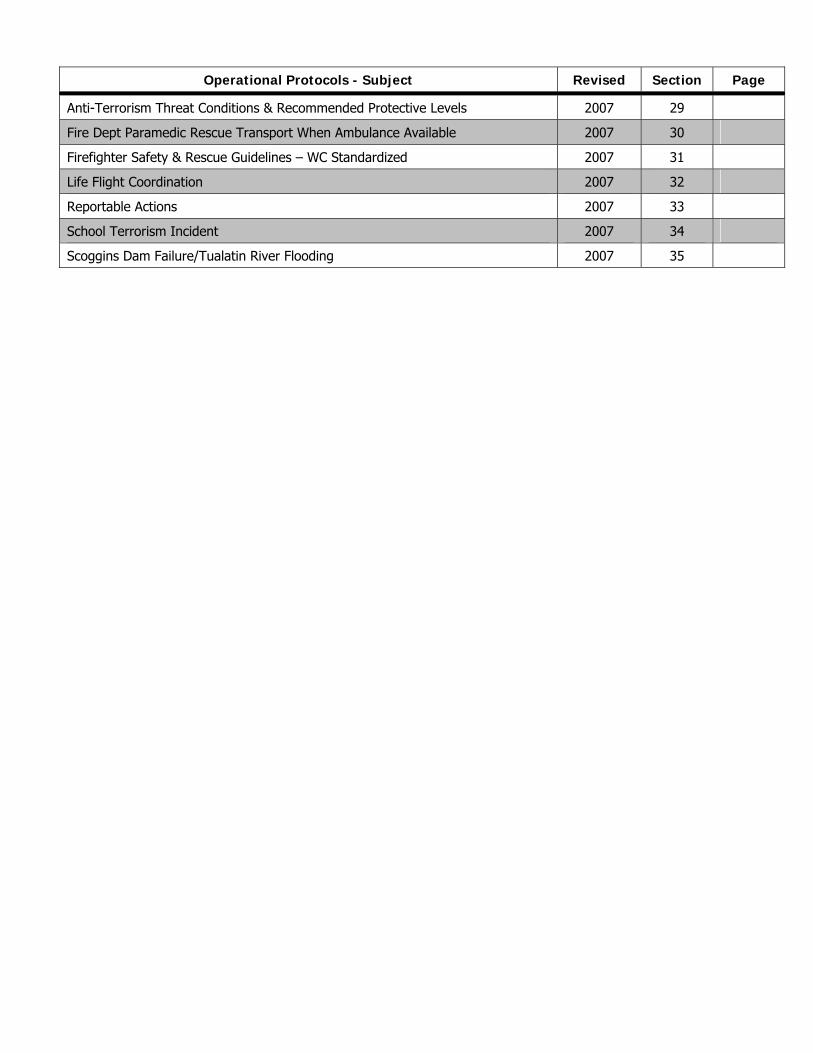
Operational Protocols - Subject Revised Section Page
Anti-Terrorism Threat Conditions & Recommended Protective Levels 2007 29
Fire Dept Paramedic Rescue Transport When Ambulance Available 2007 30
Firefighter Safety & Rescue Guidelines – WC Standardized 2007 31
Life Flight Coordination 2007 32
Reportable Actions 2007 33
School Terrorism Incident 2007 34
Scoggins Dam Failure/Tualatin River Flooding 2007 35
COMMUNICATIONS PROTOCOLS
5
AMBULANCE DIVERSION SYSTEM GUIDELINES Approved: Oregon ED Managers and EMS Providers Group 5/26/00
Revised: 7/11/02, 4/29/03, 11/11/05, and 06/09/06 I. OVERVIEW
The Greater Portland Metropolitan Area has experienced steady growth patterns over the past several years. Ambulance providers, emergency departments, and hospitals struggle with increasing patient volumes and acuity at times reaching crisis proportions. As a result, the emergency health care system is being challenged to provide access and service to the community. The Ambulance Diversion Guidelines exist to provide guidance for emergency departments and ambulance providers during capacity times. The guidelines are a collaborative effort between affected hospital emergency departments, ambulance providers, County Emergency Medical Services (EMS) agencies, and the Oregon Association of Hospitals and Health Systems (OAHHS).
II. PURPOSE
To effectively manage situations in the Greater Portland Metropolitan Area where the diversion of a 9-1-1 EMS ambulance may be necessary due to temporary shortages of hospital emergency department (ED) resources and when such diversions may have an adverse effect on patient care or the EMS system as a whole.
III. PHILOSOPHY
To promote the underlying philosophy that the Greater Portland Metropolitan Area hospitals will make every effort to avoid the diversion of 9-1-1 EMS ambulances because ambulance diversion may result in: - Transporting patients away from their hospital or physician of choice. - Prolonged pre-hospital care for unstable or critically ill patients. - Unacceptably prolonged transport times. - Attempts by field personnel to predict the specific diagnostic and therapeutic resources needed by
individual patients. - Reduced ED availability to the community. - Reduced ambulance availability to the community.
IV. OBJECTIVES
A. To promote efficient and effective provision of 9-1-1 EMS ambulance services in accordance with County Codes, as well as State and Federal Regulations.
B. To provide definitions and agreed upon procedures if ambulance diversion is determined to be
necessary.
C. To identify hospitals utilizing these guidelines and their respective geographical zones in the Greater Portland Metropolitan Area that may be impacted by ambulance diversion.
D. To identify a zone management system when multiple hospitals attempt ambulance diversion simultaneously.
E. To identify a system of accountability and quality improvement by providing ambulance diversion
data to all participants on a monthly basis. V. DEFINITIONS A. 9-1-1 EMS Ambulance Diversion – The diversion of a 9-1-1 EMS ambulance from an intended receiving
facility to an alternate receiving facility due to a temporary lack of emergency department resources such as staffing or space.
B. Inter-Facility Transfers – Hospital destination is pre-determined by physician-to-physician communication
as a formal transfer. C. Regional Hospital – A medical facility designated to coordinate MCI or disaster situations co-located with
Trauma Center Communications (TCC) and Medical Resource Hospital (MRH) which provides online
6
medical control for Multnomah and Clackamas counties. This is currently located at OHSU.
D. Zone Manager - a medical agency or facility authorized to provide coordination to pre-hospital care providers and hospitals during times of zone wide diversion.
E. Advanced Diversion System (ADS) – computerized system that the hospitals and ambulance providers use
to designate emergency department status. F. Hoscap (www.oregonhospitals.org) - Region-wide web-site for distribution of hospital status information
and incident management. G. Diversion Status Categories
1. GREEN - The ED is able to accept patients transported from 9-1-1 EMS calls and unscheduled EMS transports, except those patients they do not normally treat.
2. YELLOW - The ED is unable to accept patients transported from 9-1-1 EMS calls which require the following resources:
a. CT SCAN – The ED is unable to take patients who may need a CT scan, examples include, but are not limited to:
Any brain CT (i.e. stroke, acute neurological deficit,) Suspected aortic aneurysm (Including abdominal and/or thoracic) Isolated abdominal injury which would not otherwise meet criteria for
Trauma System entry.
b. ED CRITICAL CARE – The ED is unable to take unstable patient(s). Examples of chief complaints include, but are not limited to: Acute abdomen, non-traumatic Chest pain Coma/Sustained Altered Mental Status Respiratory distress Shock Status seizures Acute Neurologic Deficit A patient with a 12 Lead ECG that indicates a STEMI. (Contact Hospital to
determine ability to accept patient.)
3. RED – The ED is unable to accept patient(s) transported from a 9-1-1 EMS call, except: Uncontrolled airway Non-trauma patient too unstable to transport to another facility Patient refuses alternate facility Prearranged inter-facility transfer Pregnant patients >20 weeks gestation or illness or injury which could have a potential life
threatening effect on the mother and/or the fetus. A patient with a 12 Lead ECG that indicates a STEMI. (Contact Hospital to determine ability
to accept patient.)
4. Trauma Red – A designated trauma hospital will divert to another trauma hospital when it has exceeded its capacity of personnel, equipment, or facilities to assess and care for trauma patients.
H. Life Flight Network Status
• Green – Available • Yellow – On stand-by for another patient • Red – Unavailable
7
I. Destination Hospital/Services Abbreviations
1. DC Doernbecher Children’s Hospital (located within OHSU ED) Portland 2. EM Legacy Emanuel Hospital Portland 3. EC Legacy Emanuel Children’s Hospital (located in Emanuel’s ED) Portland 4. FG Tuality Forest Grove Hospital Forest Grove 5. GS Legacy Good Samaritan Hospital Portland 6. MH Legacy Mt. Hood Medical Center Gresham 7. MP Legacy Meridian Park Hospital Tualatin 8. SC Legacy Salmon Creek Hospital Vancouver 9. PA Adventist Medical Center Portland 10. PM Providence Milwaukie Hospital Milwaukie 11. PR Providence Portland Medical Center Portland 12. SK Kaiser Sunnyside Hospital Clackamas 13. SV Providence St. Vincent Medical Center Portland 14. SW Southwest Washington Medical Center Vancouver 15. TH Tuality Hospital Hillsboro 16. UH Oregon Health Sciences University Hosp. Portland 17. VA Veterans Administration Hospital Portland 18. WF Willamette Falls Hospital Oregon City 19. LF Life Flight Network Hillsboro and Aurora 20. MW Metro West Ambulance Hillsboro 21. EMS Washington County EMS Office
Hillsboro
VI. AMBULANCE DIVERSION POLICY
A. Ambulance diversion is not initiated because of: • Lack of in-patient staffing or beds • Key resources being reserved for anticipated elective patient care, i.e. elective
surgical cases or radiological studies.
B. The ED staff and ED physician determines that the emergency department is reaching capacity and attempts to accommodate by following their internal plan.
C. The ED staff and ED physician determines that ambulance diversion is necessary in order to safely
take care of patients in the emergency department because: • Critical/unstable patients occupy all suitable ED beds. • There is not enough staff to safely care for additional unstable patients in the ED. • There is a loss of CT scanner capability. • There is an in-house disaster, i.e. fire, flooding, electrical power outage, etc. which
compromises patient care/safety. • Trauma resources are unavailable (for designated trauma centers).
D. The objective of the Trauma System is that only one of the designated Level 1 Trauma Centers
may divert at a time: OHSU or Legacy Emanuel.
E. When one of the Level 1 Trauma Centers goes on ambulance diversion status, notification of divert status to the other designated trauma center must occur. Trauma patients will then be diverted to the other Trauma Center.
F. When both Level 1 Trauma Centers are at capacity the Trauma Center Communications will be
notified to begin rotating trauma patients between the two trauma hospitals until the situation has stabilized or either hospital is able to return to standard operations. The Regional Hospital may also need to do an “All Call” to other community hospitals activating the MCI or disaster system in order to coordinate distribution of trauma patients.
8
G. Designated ED staff changes their status on the Ambulance Diversion System computer screen.
H. In the event a hospital is unable to change their status on the Ambulance Diversion System screen, i.e. connection problems, the hospital may contact the zone manager to authorize the zone manager to change the hospital status on the Ambulance Diversion System screen.
I. A hospital’s Ambulance Diversion System status at the time ambulance transport begins with a
loaded patient will determine the ability of the hospital to accept patients. To insure the up-to-the-minute ability of a hospital to accept a patient, a transporting unit will contact dispatch requesting the status of the preferred destination hospital when the patient has been loaded and as they are preparing to depart the scene. Diversion of an ambulance shall not occur after the transport has begun.
J. Every effort will be made to reopen to green status as soon as possible.
VII. ZONE MANAGEMENT
A. Occasionally, multiple hospitals will go on ambulance diversion at the same time. This poses a challenge to other hospitals trying to stay open to serve their community.
B. Hospitals are grouped into the following geographical zones:
West Zone Providence St. Vincent MC
Legacy Meridian Park Hospital Tuality Community Hospital
Tuality Forest Grove Hospital
Central Zone Oregon Health Sciences University
Providence Portland MC Legacy Good Samaritan Hospital Legacy Salmon Creek Hospital
Veteran’s Administration Hospital SW Washington Medical Center
Legacy Emanuel Hospital
East Zone Adventist Medical Center
Kaiser Sunnyside Legacy Mt. Hood Medical
Center Willamette Falls Hospital
Providence Milwaukie Hospital
Zone Manager: Metro West Ambulance
Zone Manager: Regional Hospital
Zone Manager: Regional Hospital
C. Management of the hospital resources for any zone may begin if there is only one green hospital in
the West or East Zones or two green hospitals in the Central Zone. Zone management may apply even when hospitals are closed to critical care.
D. Zone Management Steps: 1. If hospital resources meet the criteria for zone management as specified in item C, the
zone manager will initiate “Active Zone Management” for the zone(s) affected.
2. The zone manager will initiate an “all call” via the 800mHz radio to hospitals informing them of the “Active Zone Management” status.
3. Local transporting EMS agencies/ dispatch centers will notify their respective EMS units
that zone management is in effect for the defined zone(s) and that their units are to contact the zone manager to obtain hospital destination(s).
4. Under zone management, the zone manager will determine the destination of all EMS
transporting units within the affected zone(s). EMS may transport to any hospital outside of the affected zone if it is green status.
5. Ambulances may go outside their zone during Zone Management as long as their
destination hospital is green and as long as the transport does not significantly impact an ambulance provider's ability to provide coverage in their area. This includes honoring previously agreed upon destinations.
9
6. Rotation will continue with one patient per hospital as determined by the zone manager. Each zone has identified “small hospitals” (West – Tuality Forest Grove (FG); East – Providence Milwaukie (PM). These hospitals will be skipped in the rotation every other time. The VA will be included (for Veterans only) at the discretion of the zone manager. Note: the rotation will not apply to the trauma hospitals for trauma entry patients.
7. Prior to discontinuing zone management, the zone manager will monitor key area hospitals
and emergency transport agencies. When system resources are above the activation threshold the zone manager may discontinue zone management. When appropriate, the Multnomah County EMS Medical Director will participate in this discussion for the Central and East zones.
F. Disaster Management (Epidemic, Pandemic, Multiple Patient Incident or Mass Casualty Incident
Hospital destinations will be coordinated by Regional Hospital through HOSCAP and according to regionally and locally adopted emergency medical services protocols.
VIII. ACCOUNTABILITY AND QUALITY IMPROVEMENT A. The hospitals shall develop:
• An internal system and resources to avoid ambulance diversion. • An internal policy related to ambulance diversion. • Internal mechanisms to monitor ambulance diversion including number of hours and reasons why.
B. Hospitals are encouraged to track their own ambulance diversion hours via a report from the Ambulance
Diversion System. C. Multnomah County EMS will report number of hours and category of divert to all East and Central Zone
participants and Washington County EMS for the West Zone participants. D. A Greater Portland Metropolitan Area Ambulance Diversion Committee shall be established to address 9-1-
1 EMS ambulance diversion issues including monitoring diversion hours and categories. This committee will be a cooperative effort between involved EMS agencies, hospitals, and ambulance providers.
E. Problems related to the implementation of these guidelines should be forwarded to the Ambulance
Diversion Committee. IX. ORGANIZATIONS IN SUPPORT OF THESE GUIDELINES HOSPITALS Doernbecher Children’s Hospital Legacy Emanuel Children’s Hospital Legacy Emanuel Hospital Legacy Good Samaritan Hospital Legacy Meridian Park Hospital Legacy Mt. Hood Medical Center Legacy Salmon Creek Hospital Oregon Health Sciences University Portland Adventist Medical Center Providence Milwaukie Hospital Providence Portland Medical Center Providence St. Vincent Medical Center Southwest Washington Medical Center Sunnyside Kaiser Hospital Tuality Forest Grove Hospital Tuality Hospital Veterans Administration Hospital Willamette Falls Hospital
Oregon Association of Hospitals and Health Systems County EMS Agencies Washington County Clackamas County Clark County Multnomah County Ambulance Providers American Medical Response Canby Fire Department Camas Fire Department Molalla Fire Department Metro West Ambulance North Country Ambulance Life Flight Network
10
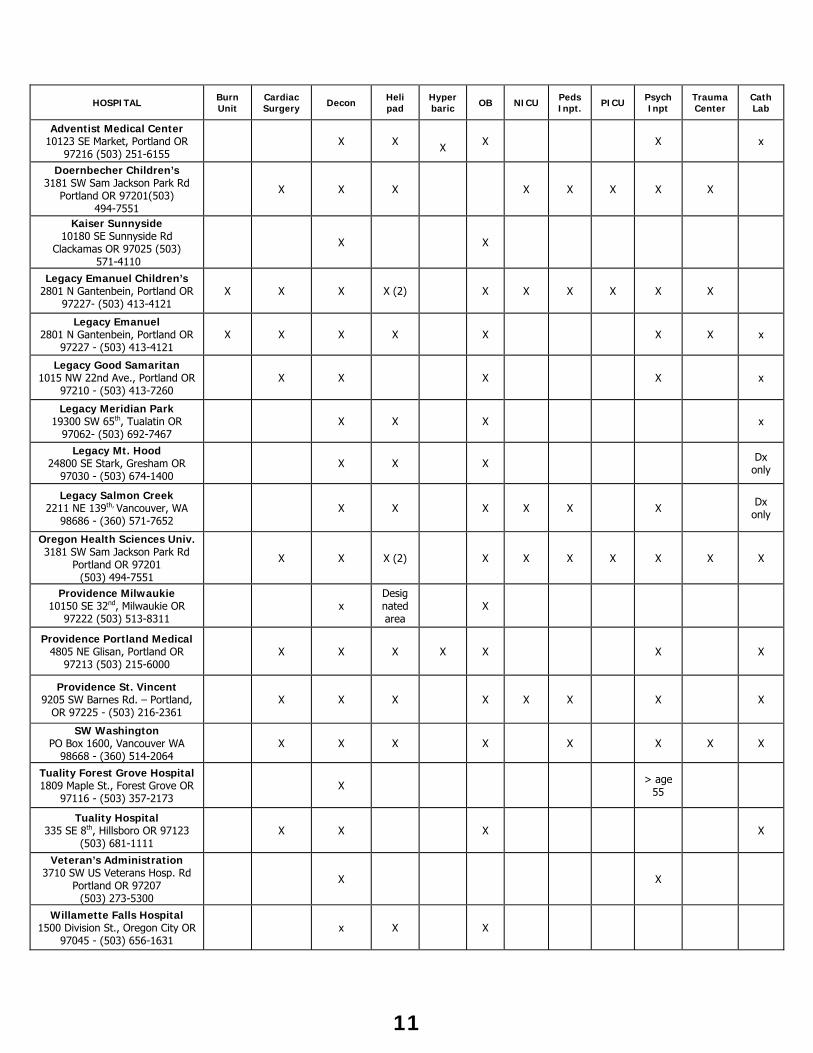
HOSPITAL Burn Unit
Cardiac Surgery
Decon
Heli pad
Hyper baric OB NICU Peds
Inpt. PICU Psych Inpt
Trauma Center
Cath Lab
Adventist Medical Center 10123 SE Market, Portland OR
97216 (503) 251-6155 X X
X X X x
Doernbecher Children’s 3181 SW Sam Jackson Park Rd
Portland OR 97201(503) 494-7551
X X X X X X X X
Kaiser Sunnyside 10180 SE Sunnyside Rd
Clackamas OR 97025 (503) 571-4110
X X
Legacy Emanuel Children’s 2801 N Gantenbein, Portland OR
97227- (503) 413-4121 X X X X (2) X X X X X X
Legacy Emanuel 2801 N Gantenbein, Portland OR
97227 - (503) 413-4121 X X X X X X X x
Legacy Good Samaritan 1015 NW 22nd Ave., Portland OR
97210 - (503) 413-7260 X X X X x
Legacy Meridian Park 19300 SW 65th, Tualatin OR
97062- (503) 692-7467 X X X x
Legacy Mt. Hood 24800 SE Stark, Gresham OR
97030 - (503) 674-1400 X X X Dx
only
Legacy Salmon Creek 2211 NE 139th, Vancouver, WA
98686 - (360) 571-7652 X X X X X X Dx
only
Oregon Health Sciences Univ. 3181 SW Sam Jackson Park Rd
Portland OR 97201 (503) 494-7551
X X X (2) X X X X X X X
Providence Milwaukie 10150 SE 32nd, Milwaukie OR
97222 (503) 513-8311 x
Desig nated area
X
Providence Portland Medical 4805 NE Glisan, Portland OR
97213 (503) 215-6000 X X X X X X X
Providence St. Vincent 9205 SW Barnes Rd. – Portland,
OR 97225 - (503) 216-2361 X X X X X X X X
SW Washington PO Box 1600, Vancouver WA
98668 - (360) 514-2064 X X X X X X X X
Tuality Forest Grove Hospital 1809 Maple St., Forest Grove OR
97116 - (503) 357-2173 X > age
55
Tuality Hospital 335 SE 8th, Hillsboro OR 97123
(503) 681-1111 X X X X
Veteran’s Administration 3710 SW US Veterans Hosp. Rd
Portland OR 97207 (503) 273-5300
X X
Willamette Falls Hospital 1500 Division St., Oregon City OR
97045 - (503) 656-1631 x X X
11
AMBULANCE DIVERSION SYSTEM (ADS) GUIDELINES FOR USE DURING A MULTIPLE
PATIENT SCENE (MPS) OR MASS CAUSALITY INCIDENT (MCI) When an MPS or MCI is declared in Washington County, the hospital destination, both medical and trauma, of patients shall be coordinated through ADS. The Ambulance Diversion System Coordinator, designated as the Metro West Ambulance Dispatch Center, shall be responsible for the notification of hospitals and the coordination of hospital destinations with the Medical Branch Director or Communication Supervisor at the scene. PROCEDURE Upon notification of an MPS or MCI, the ADS Coordinator shall notify all Washington County Hospitals and other receiving hospitals through the ADS program. As soon as possible after the initiation of the MPS or MCI the Triage/Treatment/Communications Supervisor shall notify the ADS Coordinator as to the number of immediate (red), delayed (yellow) and walking wounded (green) patients at the scene. This information will be updated to the receiving hospital(s) if not provided during the initial hospital notification. Working with the Triage/Treatment/Communications Supervisor, the ADS Coordinator shall determine which hospitals should expect to receive patients. The ADS Coordinator shall determine, based on the beds available from Washington County hospitals, if hospitals in Multnomah and Clackamas County’s will be receiving patients. If hospitals designated to receive patients are in Multnomah or Clackamas County’s or patients are to be entered into the trauma system, the Regional Hospital Coordinator, currently MRH shall be notified by the ADS Coordinator. The ADS Coordinator shall be responsible for coordinating hospital beds in Multnomah and Clackamas County’s with MRH.
The Triage/Treatment/Communications Supervisor shall notify the ADS Coordinator when an ambulance is loaded and ready for transport. The ADS Coordinator will determine the destination of the ambulance and notify the Triage/Treatment/Communications Supervisor. The Triage/Treatment/Communications Supervisor will notify the ADS Coordinator upon departure of the ambulance and will provide the ADS Coordinator with the number and types of injuries and the ETA of the ambulance to the hospital. The ADS Coordinator will be responsible for notifying the destination hospital of the ambulances ETA and the numbers and types of patients.
12
AMBULANCE DIVERSION SYSTEM – WEST ZONE MANAGEMENT Zone Management is a process consisting of a series of steps. Rotation of patients to closed (red) hospitals is one step in the Zone Management process.
West Zone Hospitals Providence St. Vincent Medical Center
Legacy Meridian Park Hospital Tuality Community Hospital
Tuality Forest Grove Hospital
Zone Management will begin if there is one green hospital remaining in the West Zone.
Step 1 (One Remaining Green Hospital in the West Zone) Metro West Ambulance Dispatch will call the Emergency Department Charge Nurse at each West Zone hospital and notify them that rotation of patients is pending and try to determine how much longer the hospital will be on divert.
Step 2 (All Hospitals in the West Zone are Red) Metro West Ambulance Dispatch will call the Emergency Department Charge Nurse at each West Zone hospital and notify them that the West Zone is in Zone Management and rotation of patients has begun.
Step 3 (All Hospitals in the West Zone are Red) Metro West Ambulance Dispatch will initiate a general broadcast on the Fire Dispatch channel that the West Zone is in Zone Management. The broadcast shall say, “All units, Medic Control, Washington County is now in hospital zone management until further notice.”
American Medical Response Portland Dispatch and Regional Hospital will be notified by phone that the West Zone is in Active Zone Management. On the ADS screen the West Zone will be changed to blinking to indicate Zone Management.
Step 4 (All Hospitals in the West Zone are Red) In Zone Management Metro West Ambulance will be responsible for rotating patients to West Zone Hospital in the following rotation: St. Vincent, Tuality-Hillsboro, Meridian Park, Forest Grove. Rotation to Forest Grove will be skipped every other cycle. This rotation will be for all patients transported by ambulance from any regional ambulance provider. A hospital’s status will not be changed by Metro West Ambulance. All hospital will remain red until changed by a hospital.
Step 5 (One or more hospitals returns to Green Status) Metro West Ambulance Dispatch will initiate a general broadcast on the Fire Dispatch channel that the West Zone is in no longer in Zone Management. The broadcast shall say, “All units, Medic Control, Washington County is no longer in hospital zone management.” American Medical Response Portland Dispatch and Regional Hospital will be notified by phone that the West Zone is no longer in Zone Management. On the ADS screen the West Zone will be changed from blinking to steady to indicate Zone Management has stopped.
13
AMBULANCE DISPATCH AND COORDINATION An emergency ambulance shall be dispatched according to the emergency medical dispatch cards approved by the EMS Office. Emergency means those medical or trauma conditions that manifests itself by symptoms of sufficient severity that a prudent lay person possessing an average knowledge of health and medicine would reasonably expect that failure to receive immediate medical attention would place the health of a person, or the fetus in the case of a pregnant woman, in serious jeopardy. An emergency condition also includes any condition specifically dealt with in the emergency medical dispatch system adopted by the Washington County or those conditions covered in 8.32.440 (G) of EMS Ordinance. Washington County Code 8.32.440 states:
Transport any individual requiring or with a high probability of requiring before or during transport the services of an emergency ambulance. Among examples of this are:
1. Persons with devices which prevent the rider from being able to protect their airway in the event of vomiting,
2. Persons requiring on-going treatment during transport which includes riders with IV infusions or oxygen except those riders on chronic supplemental oxygen, or other condition delineated by rule.
3. Persons not previously using a wheelchair whom are otherwise unable to move to the vehicle unassisted, unless the transport is at the express direction of a physician,
4. Persons with decompensation cardiovascular, respiratory or central nervous systems,
5. Persons with major bleeding from trauma, 6. Persons having a suspected major abdominal injury, 7. Persons with severe pain, 8. Persons with evidence of spinal cord injury unless previously examined by a
physician, 9. Any person with full thickness burns. PROCEDURE A. The Metro West Ambulance Communications Center shall coordinate emergency
ambulance response to calls that fall within the EMD card system. This coordination shall include ambulances on a mutual-aid basis both into and out of Washington County.
B. Metro West Ambulance shall retain the ability to reassess the triaging of EMS requests by WCCCA and when they feel appropriate modify the dispatch of an ambulance to include increasing or reducing the number of ambulance unit(s) responding and/or increasing or reducing the code response of the ambulance unit(s).
C. Calls for ambulance service that fall within the emergency medical dispatch card system and not defined by rule as “Inter-Facility” shall be immediately transferred to Metro West Ambulance for service.
14
AMBULANCE COORDINATION DURING MAJOR EMERGENCIES When a major emergency is declared in Washington County, these guidelines will help guide the coordination of ambulances. Metro West Ambulance's Control Center shall be designated as the ambulance control center for Washington County. Metro West Ambulance's Control Center shall be responsible for the coordination of ambulance resources to medical requests. This shall include ambulance response into and out of the county as well as requests originating from within the county. Dispatch of ambulance resources shall be done according to the major emergency version of the Emergency Medical Dispatch (EMD) cards. Note: WCCCA may or may not continue triaging all requests for medical assistance using the EMD cards. If WCCCA discontinues triaging calls, Metro West Ambulance may be asked to take over that responsibility.
COORDINATION OF AMBULANCE RESOURCES TO MEDICAL CALLS Patients shall be transported to the nearest emergency department. Exceptions to this are those patients requiring specialized medical care (burns, hyperbaric chamber, obstetrical emergencies.) The Washington County EMS Office shall suspend inter-facility transports until the lifting of the major emergency and/or authorization.
TRAUMA ENTRIES Patients requiring trauma system entry shall be transported to the OHSU/Emanuel Hospital only if transportation routes allow. If highways are congested or blocked, trauma patients shall be transported to St. Vincent Hospital. Under the most extreme conditions, trauma patients may have to be taken to the nearest hospital. Patients must still be entered into the trauma system as normal by contacting the Trauma Communications Center (TCC) and providing them with the necessary patient information, including trauma band number. If the patient is diverted to a non-trauma facility TCC must be notified of the diversion as soon as possible. If a patient meets trauma system entry criteria but must be diverted to a non-trauma hospital, the State EMS Office’s Trauma Division must be contacted immediately. Provided them with the patient’s name, trauma band # and destination hospital. Ambulance units will not be sent "stand-bys" unless there is the highest possibility that injuries may occur. Stand-by for non-medical events (i.e. fires, downed power lines) shall occur only if the county ambulance level is above three.
MAJOR EMERGENCY CHECKLIST 1. Confirm major emergency guideline activation at WCCCA on Fire dispatch channel or telephone. If activation of
guidelines for ambulance coordination during major emergencies came from the Washington County EMS Office, notify WCCCA on fire dispatch channel.
2. Notify field units that they are now operating under Major Emergency Guidelines. If roadways into and out of Portland are congested or blocked, trauma entry patients shall be transported to St. Vincent Hospital. If transport to St. Vincent Hospital is not possible, patients shall be transported to the nearest hospital.
4. Notify Washington County hospitals, including Meridian Park Hospital that patients will be transported to the nearest hospital.
5. Contact St. Vincent Hospital Emergency Department and request they be prepared to receive trauma patients. 6. Notify Washington County EMS Office by telephone/pager of Major Emergency Guideline activation. 7. Notify Metro West Ambulance management personnel of major emergency guideline activation so they can: a. Provide additional dispatch personnel as needed.
b. Staff additional ambulance units as needed or directed by EMS Office or company management or per Multiple Casualty Incident Plans.
8. Use Modified EMD Cards to establish priorities for ambulance response. Low Priority - Send ambulance only when County ambulance level is three (3) or above.
Medium Priority - Send ambulance only when County ambulance level is two (2) or above. High Priority - Send nearest ambulance immediately.
9. When operations under these Guidelines are terminated, notify: a. Field units that they can return to everyday activities. b. Washington County hospitals, including Meridian Park Hospital. c. Notify St. Vincent Hospital that they will no longer receive trauma patients. d. Washington County EMS Office, if activation came from WCCCA. e. WCCCA if activation came from Washington County EMS Office.
f. Metro West Management.
15
MAJOR EMERGENCY CHECKLIST
1. Confirm major emergency guideline activation at WCCCA on Fire dispatch channel or
telephone. If activation of guidelines for ambulance coordination during major emergencies came from the Washington County EMS Office, notify WCCCA on fire dispatch channel.
2. Notify field units that they are now operating under Major Emergency Guidelines. Tell them
if roadways into and out of Portland are congested or blocked, trauma entry patients shall be transported to St. Vincent Hospital. If transport to St. Vincent Hospital is not possible, patients shall be transported to the nearest hospital.
4. Notify Washington County hospitals, including Meridian Park Hospital that patients will be
transported to the nearest hospital. 5. Contact St. Vincent Hospital Emergency Department Duty Physician and ask them to
prepare to accept trauma entry patients. 6. Notify Washington County Emergency Medical Services Office by telephone or pager of
Major Emergency Guideline activation at WCCCA. 7. Notify Metro West Ambulance management personnel of major emergency guideline
activation so they can: a. Provide additional dispatch personnel as needed.
c. Staff additional ambulance units as needed or directed by EMS Office or company management or per Multiple Casualty Incident Plans.
9. Use Modified EMD Cards to establish priorities for ambulance response. Low Priority - Send ambulance only when County ambulance level is three (3) or above.
Medium Priority - Send ambulance only when County ambulance level is two (2) or above. High Priority - Send nearest ambulance immediately.
10. When operations under these Guidelines are terminated, notify: a. Field units that they can return to everyday activities. b. Washington County hospitals, including Meridian Park Hospital. c. Notify St. Vincent Hospital to deactivate as a back-up trauma center. d. Washington County EMS Office, if activation came from WCCCA. e. WCCCA if activation came from Washington County EMS Office.
f. Metro West Management as appropriate.
16
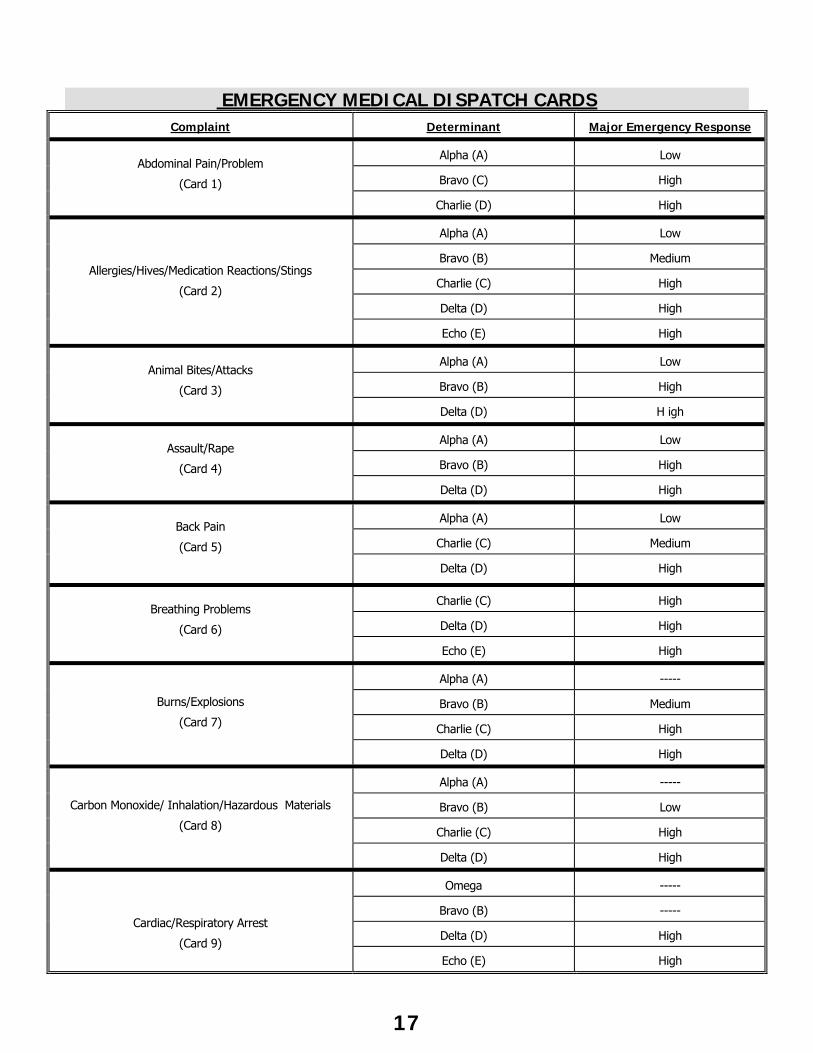
EMERGENCY MEDICAL DISPATCH CARDS Complaint Determinant Major Emergency Response
Alpha (A) Low
Bravo (C) High
Abdominal Pain/Problem
(Card 1)
Charlie (D) High
Alpha (A) Low
Bravo (B) Medium
Charlie (C) High
Delta (D) High
Allergies/Hives/Medication Reactions/Stings
(Card 2)
Echo (E) High
Alpha (A) Low
Bravo (B) High
Animal Bites/Attacks
(Card 3)
Delta (D) H igh
Alpha (A) Low
Bravo (B) High
Assault/Rape
(Card 4)
Delta (D) High
Alpha (A) Low
Charlie (C) Medium
Back Pain
(Card 5)
Delta (D) High
Charlie (C) High
Delta (D) High
Breathing Problems
(Card 6)
Echo (E) High
Alpha (A) -----
Bravo (B) Medium
Charlie (C) High
Burns/Explosions
(Card 7)
Delta (D) High
Alpha (A) -----
Bravo (B) Low
Charlie (C) High
Carbon Monoxide/ Inhalation/Hazardous Materials
(Card 8)
Delta (D) High
Omega -----
Bravo (B) -----
Delta (D) High
Cardiac/Respiratory Arrest
(Card 9) Echo (E) High
17
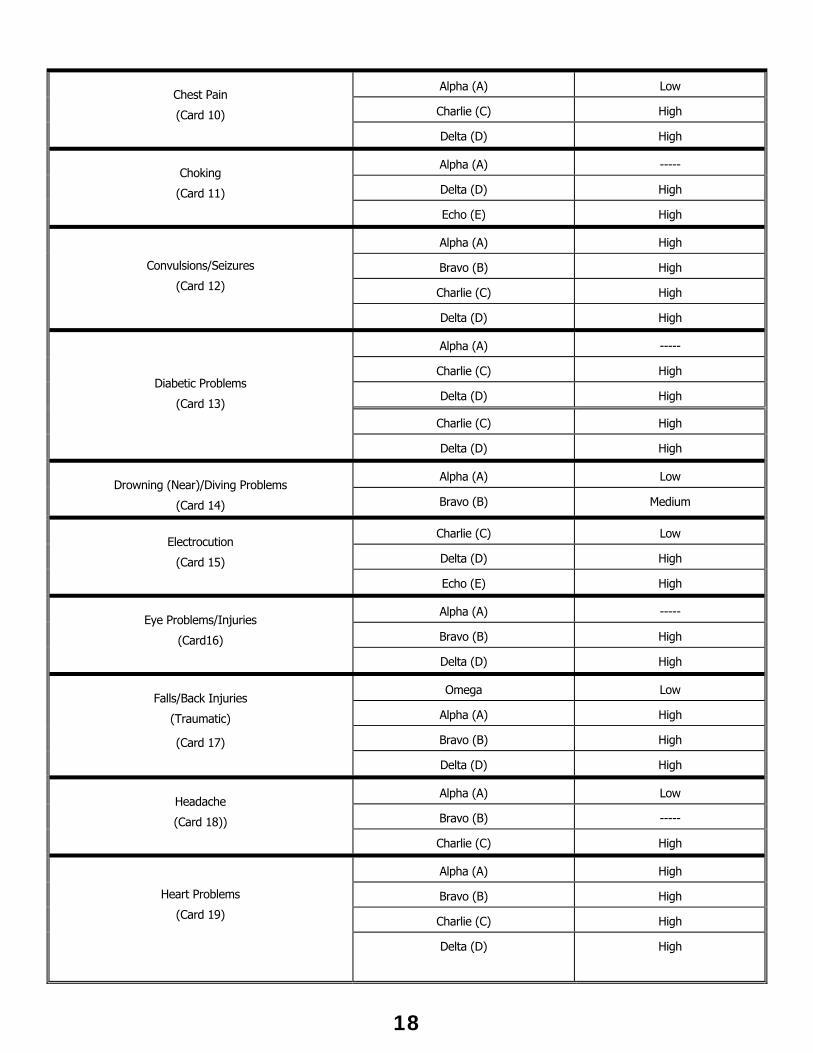
Alpha (A) Low
Charlie (C) High
Chest Pain
(Card 10)
Delta (D) High
Alpha (A) -----
Delta (D) High
Choking
(Card 11)
Echo (E) High
Alpha (A) High
Bravo (B) High
Charlie (C) High
Convulsions/Seizures
(Card 12)
Delta (D) High
Alpha (A) -----
Charlie (C) High
Delta (D) High
Charlie (C) High
Diabetic Problems
(Card 13)
Delta (D) High
Alpha (A) Low Drowning (Near)/Diving Problems
(Card 14) Bravo (B) Medium
Charlie (C) Low
Delta (D) High
Electrocution
(Card 15)
Echo (E) High
Alpha (A) -----
Bravo (B) High
Eye Problems/Injuries
(Card16)
Delta (D) High
Omega Low
Alpha (A) High
Bravo (B) High
Falls/Back Injuries
(Traumatic)
(Card 17)
Delta (D) High
Alpha (A) Low
Bravo (B) -----
Headache
(Card 18))
Charlie (C) High
Alpha (A) High
Bravo (B) High
Charlie (C) High
Heart Problems
(Card 19)
Delta (D) High
18
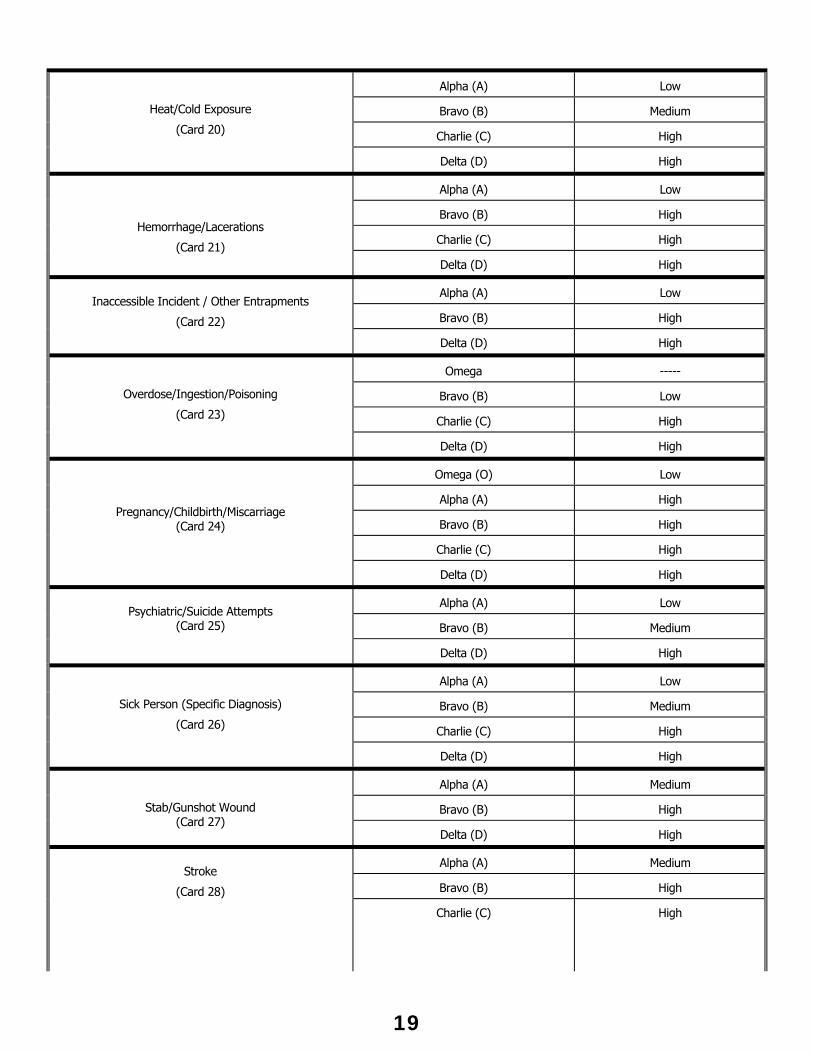
Alpha (A) Low
Bravo (B) Medium
Charlie (C) High
Heat/Cold Exposure
(Card 20)
Delta (D) High
Alpha (A) Low
Bravo (B) High
Charlie (C) High
Hemorrhage/Lacerations
(Card 21) Delta (D) High
Alpha (A) Low
Bravo (B) High
Inaccessible Incident / Other Entrapments
(Card 22)
Delta (D) High
Omega -----
Bravo (B) Low
Charlie (C) High
Overdose/Ingestion/Poisoning
(Card 23)
Delta (D) High
Omega (O) Low
Alpha (A) High
Bravo (B) High
Charlie (C) High
Pregnancy/Childbirth/Miscarriage (Card 24)
Delta (D) High
Alpha (A) Low
Bravo (B) Medium
Psychiatric/Suicide Attempts
(Card 25)
Delta (D) High
Alpha (A) Low
Bravo (B) Medium
Charlie (C) High
Sick Person (Specific Diagnosis)
(Card 26)
Delta (D) High
Alpha (A) Medium
Bravo (B) High
Stab/Gunshot Wound (Card 27)
Delta (D) High
Alpha (A) Medium
Bravo (B) High
Stroke
(Card 28)
Charlie (C) High
19
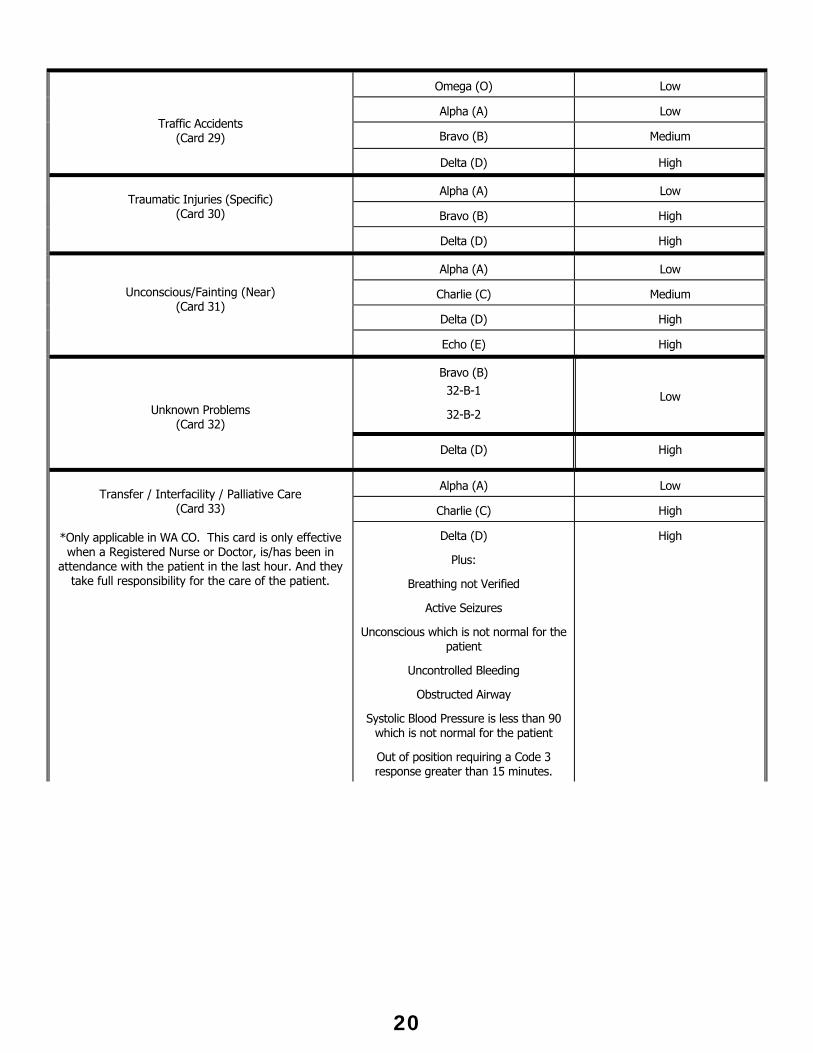
Omega (O) Low
Alpha (A) Low
Bravo (B) Medium
Traffic Accidents (Card 29)
Delta (D) High
Alpha (A) Low
Bravo (B) High
Traumatic Injuries (Specific)
(Card 30)
Delta (D) High
Alpha (A) Low
Charlie (C) Medium
Delta (D) High
Unconscious/Fainting (Near) (Card 31)
Echo (E) High
Bravo (B) 32-B-1
32-B-2
Low
Unknown Problems (Card 32)
Delta (D) High
Alpha (A) Low
Charlie (C) High
Transfer / Interfacility / Palliative Care
(Card 33)
*Only applicable in WA CO. This card is only effective when a Registered Nurse or Doctor, is/has been in
attendance with the patient in the last hour. And they take full responsibility for the care of the patient.
Delta (D)
Plus:
Breathing not Verified
Active Seizures
Unconscious which is not normal for the patient
Uncontrolled Bleeding
Obstructed Airway
Systolic Blood Pressure is less than 90 which is not normal for the patient
Out of position requiring a Code 3 response greater than 15 minutes.
High
20
AMBULANCE RESPONSE TO STANDBY AND STAGING LOCATIONS Stage - Committed until released. Used when ambulance is asked to delay approach to patient until police arrive. Used in situations where a patient is suspected to be present. Standby - Not committed to the incident and available for emergency call. PROCEDURE A. All responses to stage/stand-by requests shall be code-1. B. Response to stage shall be code-1 if ambulance is to wait for the arrival of law
enforcement, regardless of the code response dictated by the EMD cards. C. During the response to a stage/standby or while at the scene the ambulance unit shall
be available for any code-3 call. If an ambulance is removed from a stand-by WCCCA shall be notified as soon as possible. Ambulance responses to high acuity incidents (stabbing/shooting/hanging) shall not be diverted.
D. A replacement ambulance shall be sent to the stand-by as soon as possible.
21
AMBULANCE RESPONSE TO FIRE STAND-BYS
Metro West Ambulance will assign an ambulance to all fire assignments in Washington County as long as the ambulance level is above two (2). Ambulances will not be sent to Task Force assignments. If the County ambulance level is two (2) or below an ambulance will be assigned to the box as soon as the level rises above two (2). Fire-Com will be immediately notified of any delay in the assignment or response of a stand-by ambulance and the estimated time for the delay. The ambulance will respond code-1 to the box assignment and will be available for redirection to code-3 calls. If the assigned ambulance is redirected to a code-3 call, the next nearest ambulance will be immediately assigned to the box as long as the County ambulance level is above level two (2). Fire-Com shall be immediately notified of the switching of any unit. Upon arrival at the fire, the ambulance shall position themselves to be available to respond to code-3 calls and shall notify Fire-Com and Command of their arrival. If the ambulance needs to leave for a code-3 call, Command and Fire-Com must be notified. Metro West Dispatch will assign a replacement ambulance as soon as possible and notify Fire-Com of any delay in the assignment or response. If the County ambulance level drops to one (1), any ambulances on stand-by at box assignments shall immediately be put back in to the ambulance status plan and assigned to the appropriate ambulance post. If an ambulance assigned to a box causes a depletion in ambulance resources and causes longs ambulance responses to other calls during the assignment, Metro West Ambulance may petition the County for response time exemptions for those long responses.
22
AMBULANCE STATUS NOTIFICATION To develop a procedure for the notification of WCCCA when Metro West Ambulance unit availability reaches two (2) or less. Ambulance units at hospitals shall be considered available for emergency response.
This protocol shall not take the place of existing requirements that Metro West Ambulance Units notify WCCCA and fire users of their response to incidents and the location from where they are responding on the appropriate TAC channel.
PROCEDURE When Metro West Ambulance’s number of units available for emergency response reaches two (2), and in the estimation of Metro West dispatchers will remain at, or below two (2) for more than five (5) minutes, Metro West shall announce on the fire dispatch channel, “Information to all units, Washington County ambulance level is at X.”
Upon rising above Level 3 announce that on the fire dispatch channel, “Information to all units, Washington County ambulance level is at X.”
This notification shall take place only after the appropriate dispatching and coordination of ambulance units has been done. No delay in dispatching, coordination of response, movement of ambulance units to posting location(s) is expected. These take precedent over the requirements of this protocol.
23
AMBULANCE OPERATIONS SUPERVISOR
The MWA Operations Supervisor has the option to respond to all ambulance calls. In general, they may respond to unusual incidents, critical calls, air ambulance activation, multiple patient scenes and mass casualty incidents.
When a supervisor responds, WCCCA will be notified on the on the designated TAC channel. The Supervisor shall advise WCCCA if they are transport capable or not.
The Supervisor's presence is to directly oversee ambulance operations within the scope of the incident command system and MPS/MCI Protocol.
If responding as a non-transport unit, the Supervisor shall position their unit out of the flow of traffic as to not block other emergency vehicles. The Supervisor will report to Incident Command for assignment. If command does not have an assignment for the Supervisor, the Supervisor shall oversee ambulance operations to include the Transport and/or Communications Position.
If responding as a transport capable unit, but transport of patient(s) is not anticipated the Supervisor shall position their unit out of the flow of traffic as to not block other emergency vehicles. The Supervisor will report to Incident Command for assignment. If command does not have an assignment for the Supervisor, the Supervisor shall oversee ambulance operations to include the Transport and/or Communications function.
If responding as a transport capable unit and transport of patient(s) is anticipated the Supervisor will report to Incident Command/Medical Group for assignment.
24
EMERGENCY CALLS RECEIVED
DIRECTLY BY AMBULANCE COMPANIES
THIS PROTOCOL APPLIES TO ALL AMBULANCE PROVIDERS THAT ARE NOT DESIGNATED AS AN EMERGENCY AMBULANCE PROVIDER BY WASHINGTON COUNTY.
Ambulance company dispatchers will be responsible for handling incoming calls for medical assistance made directly to them according to the EMD cards with immediate notification of WCCCA.
When an ambulance company receives a request for medical assistance, the company shall use the EMD Card System to determine whether an emergency response is required. If the ambulance provider dispatcher is not emergency medical dispatch certified as required by these protocols, they shall immediately transfer the call to Metro West Ambulance.
An emergency means a medical or trauma condition that manifests itself by symptoms of sufficient severity that a prudent lay person possessing an average knowledge of health and medicine would reasonably expect that failure to receive immediate medical attention would place the health of a person, or the fetus in the case of a pregnant woman, in serious jeopardy. An emergency condition also includes any condition specifically dealt with in the emergency medical dispatch system adopted by the Washington County or those conditions covered in 8.32.440 (G) of EMS Ordinance.
Washington County Code 8.32.440 states: Transport of any individual requiring or with a high probability of requiring before or during transport the services of an emergency ambulance. Among examples of this are:
1. Persons with devices which prevent the rider from being able to protect their airway in the event of vomiting,
2. Persons requiring on-going treatment during transport which include riders with IV infusions or oxygen except those riders on chronic supplemental oxygen, or other condition delineated by rule.
3. Persons not previously using a wheelchair who are otherwise unable to move to the vehicle unassisted, unless the transport is at the express direction of a physician,
4. Persons with decompensation of cardiovascular, respiratory or central nervous systems, 5. Persons with major bleeding from trauma, 6. Persons having a suspected major abdominal injury, 7. Persons with severe pain,
8. Persons with evidence of spinal cord injury unless previously examined by a physician, 9. Any person with full thickness burns.
NON-EMERGENCY RESPONSE Non-emergency means those medical or trauma conditions that are not specifically dealt with in the emergency medical dispatch system adopted by the County. The County by rule shall further delineate categories contained in the emergency medical dispatch system that may be handled by a non-emergency ambulance provider. Unless specified by rule, those conditions that fall within the emergency medical dispatch system shall immediately be transferred to the emergency ambulance providers designated by Washington County. Administrative Rule 554-440-000 defines non-emergency to mean those medical conditions, that in the judgment of an individual certified or licensed at the emergency medical technician, registered nurse, physician assistant or physician level, are not expected to cause death, permanent disability or permanent harm within the next 24 hours and do not require a code-3 response as determined by the EMD card system.
25
If the response required by the EMD cards is code-3 or code-1 and the ambulance company dispatcher is EMD certified and the Ambulance Company is licensed to provide emergency ambulance service, the dispatcher shall complete the EMD process and dispatch an ambulance. As soon as possible WCCCA shall be notified of the location and the nature of the request as well as the telephone number of the person requesting aid and any other pertinent information received from the EMD process. EXCEPTION: Calls received directly from nursing homes and care facilities where there is a Registered Nurse in attendance of the patient, WCCCA does not need to be notified unless:
1. The patient’s breathing status can not be verified. 2. The patient is in active seizures. 3. The patient is unconscious which is not normal for the patient. 4. The patient has uncontrolled bleeding. 5. The patient has an obstructed airway. 6. The patient’s systolic blood pressure is less than 90mmHg, which is not normal for the
patient. 7. The ambulance is out of position requiring a code 3 response greater than fifteen (15)
minutes.
If the response required is not covered in the EMD cards and the ambulance company dispatcher is EMD certified and the Ambulance Company is licensed to provide emergency and/or non-emergency ambulance service, the dispatcher shall complete the EMD process and dispatch an ambulance. If the ambulance company dispatcher taking the call is not EMD certified they shall transfer the call immediately to Metro West Ambulance. Requests for ambulance service that do not fall within the EMD cards system can be handled by any licensed ambulance provider.
26
EMERGENCY MEDICAL DISPATCH
Emergency Medical Dispatch System The Medical Priority Dispatch System® (MPDS®) and Association of Public Safety Communicators Officials (APCO) have been approved as the standard for dispatch of emergency medical calls for Washington County. These card systems shall be utilized on every medical call unless otherwise directed by EMS protocols. The Washington County Emergency Medical Services Office shall be responsible for setting the ambulance response levels. Equipment Response Equipment response shall be according to EMD card and according to the capabilities of the jurisdiction. Quality Assurance/Quality Improvement The EMS Office shall develop and implement a Quality Assurance/Quality Improvement (QA/QI) program. This QA/QI Program will review and monitor the application of the MPDS® or APCO EMD Card system and assist with the training of emergency medical dispatchers.
27
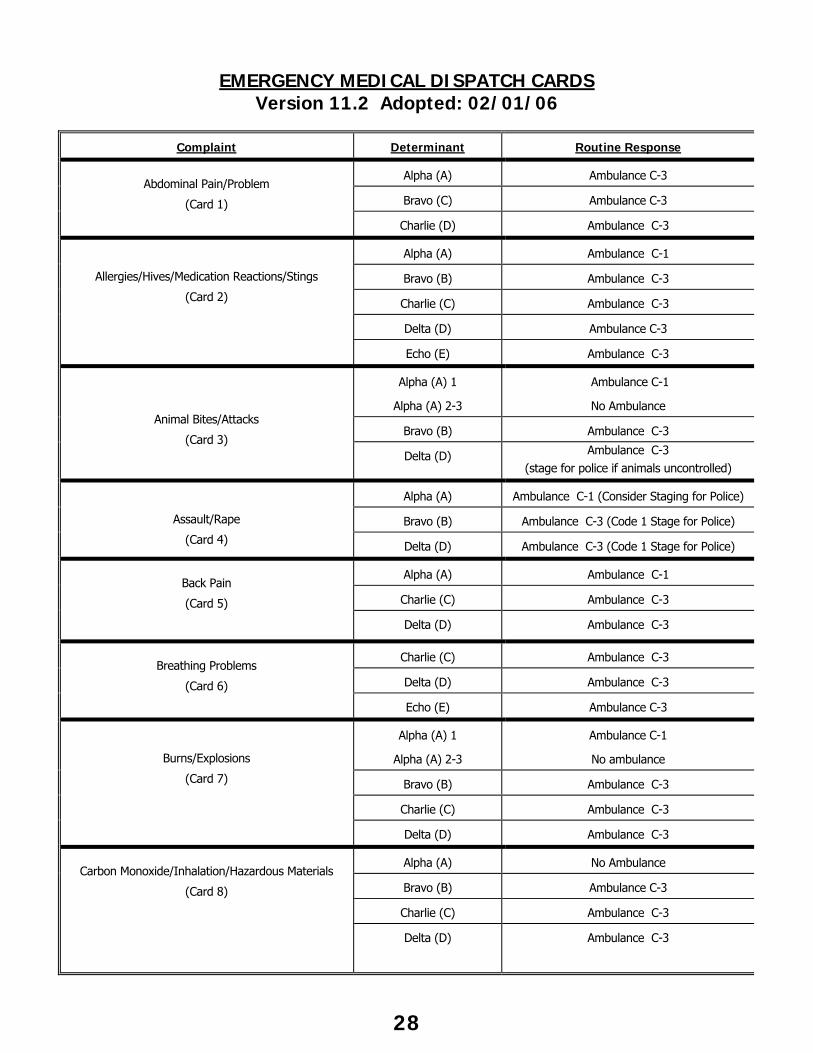
EMERGENCY MEDICAL DISPATCH CARDS
Version 11.2 Adopted: 02/01/06
Complaint Determinant Routine Response
Alpha (A) Ambulance C-3
Bravo (C) Ambulance C-3
Abdominal Pain/Problem
(Card 1)
Charlie (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Delta (D) Ambulance C-3
Allergies/Hives/Medication Reactions/Stings
(Card 2)
Echo (E) Ambulance C-3
Alpha (A) 1
Alpha (A) 2-3
Ambulance C-1
No Ambulance
Bravo (B) Ambulance C-3
Animal Bites/Attacks
(Card 3) Delta (D) Ambulance C-3
(stage for police if animals uncontrolled)
Alpha (A) Ambulance C-1 (Consider Staging for Police)
Bravo (B) Ambulance C-3 (Code 1 Stage for Police)
Assault/Rape
(Card 4) Delta (D) Ambulance C-3 (Code 1 Stage for Police)
Alpha (A) Ambulance C-1
Charlie (C) Ambulance C-3
Back Pain
(Card 5)
Delta (D) Ambulance C-3
Charlie (C) Ambulance C-3
Delta (D) Ambulance C-3
Breathing Problems
(Card 6)
Echo (E) Ambulance C-3
Alpha (A) 1
Alpha (A) 2-3
Ambulance C-1
No ambulance
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Burns/Explosions
(Card 7)
Delta (D) Ambulance C-3
Alpha (A) No Ambulance
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Carbon Monoxide/Inhalation/Hazardous Materials
(Card 8)
Delta (D) Ambulance C-3
28
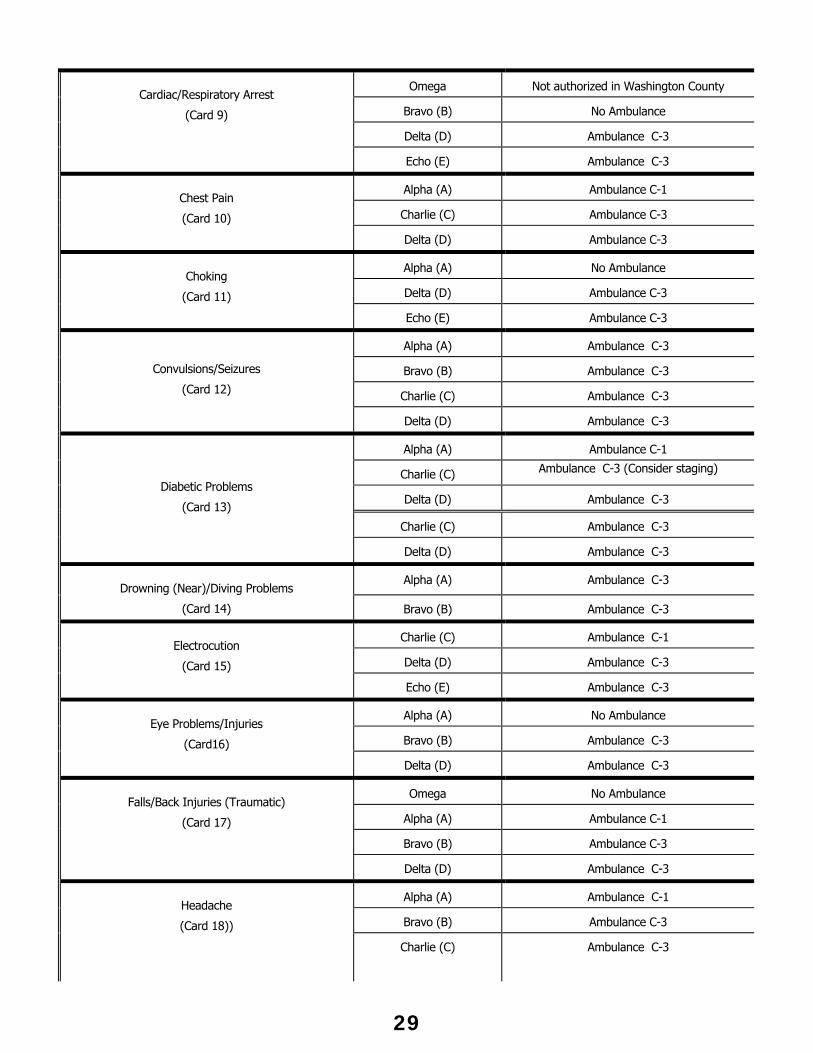
Omega Not authorized in Washington County
Bravo (B) No Ambulance
Delta (D) Ambulance C-3
Cardiac/Respiratory Arrest
(Card 9)
Echo (E) Ambulance C-3
Alpha (A) Ambulance C-1
Charlie (C) Ambulance C-3
Chest Pain
(Card 10)
Delta (D) Ambulance C-3
Alpha (A) No Ambulance
Delta (D) Ambulance C-3
Choking
(Card 11)
Echo (E) Ambulance C-3
Alpha (A) Ambulance C-3
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Convulsions/Seizures
(Card 12)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Charlie (C) Ambulance C-3 (Consider staging)
Delta (D) Ambulance C-3
Charlie (C) Ambulance C-3
Diabetic Problems
(Card 13)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-3 Drowning (Near)/Diving Problems
(Card 14) Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-1
Delta (D) Ambulance C-3
Electrocution
(Card 15)
Echo (E) Ambulance C-3
Alpha (A) No Ambulance
Bravo (B) Ambulance C-3
Eye Problems/Injuries
(Card16)
Delta (D) Ambulance C-3
Omega No Ambulance
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Falls/Back Injuries (Traumatic)
(Card 17)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Headache
(Card 18))
Charlie (C) Ambulance C-3
29
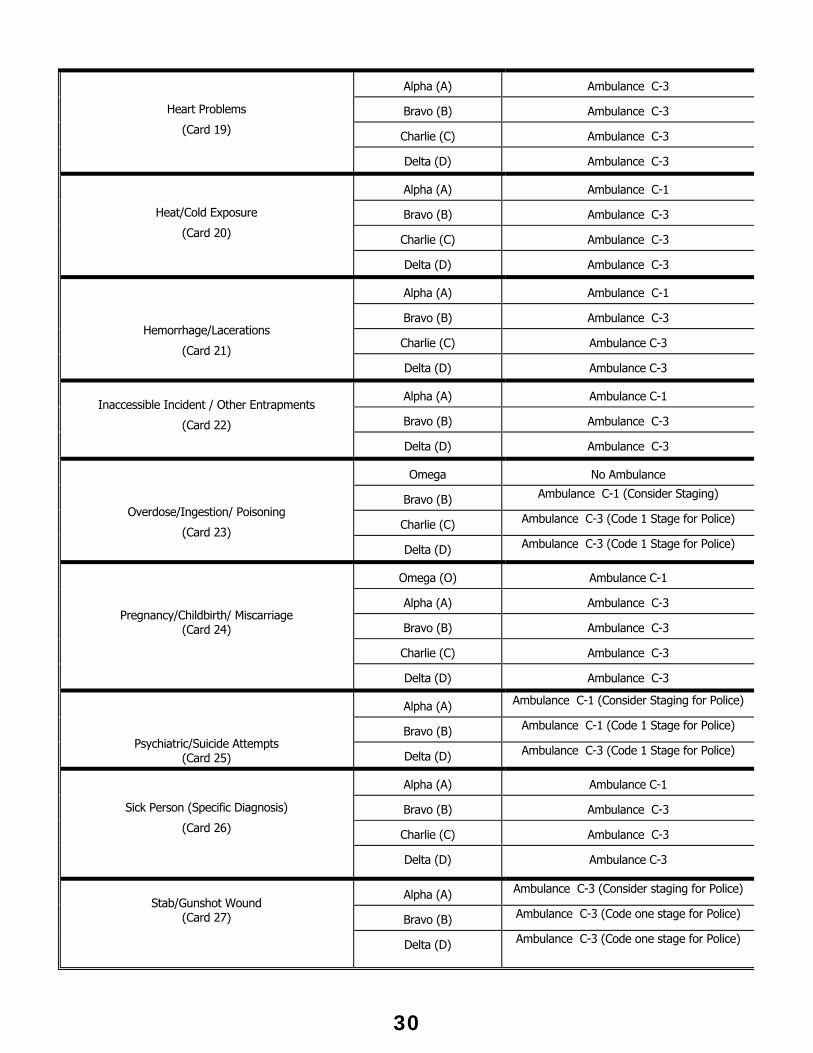
Alpha (A) Ambulance C-3
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Heart Problems
(Card 19)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Heat/Cold Exposure
(Card 20)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Hemorrhage/Lacerations
(Card 21) Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Inaccessible Incident / Other Entrapments
(Card 22)
Delta (D) Ambulance C-3
Omega No Ambulance
Bravo (B) Ambulance C-1 (Consider Staging)
Charlie (C) Ambulance C-3 (Code 1 Stage for Police)
Overdose/Ingestion/ Poisoning
(Card 23) Delta (D) Ambulance C-3 (Code 1 Stage for Police)
Omega (O) Ambulance C-1
Alpha (A) Ambulance C-3
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Pregnancy/Childbirth/ Miscarriage (Card 24)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1 (Consider Staging for Police)
Bravo (B) Ambulance C-1 (Code 1 Stage for Police)
Psychiatric/Suicide Attempts (Card 25) Delta (D) Ambulance C-3 (Code 1 Stage for Police)
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Charlie (C) Ambulance C-3
Sick Person (Specific Diagnosis)
(Card 26)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-3 (Consider staging for Police)
Bravo (B) Ambulance C-3 (Code one stage for Police)
Stab/Gunshot Wound
(Card 27)
Delta (D) Ambulance C-3 (Code one stage for Police)
30
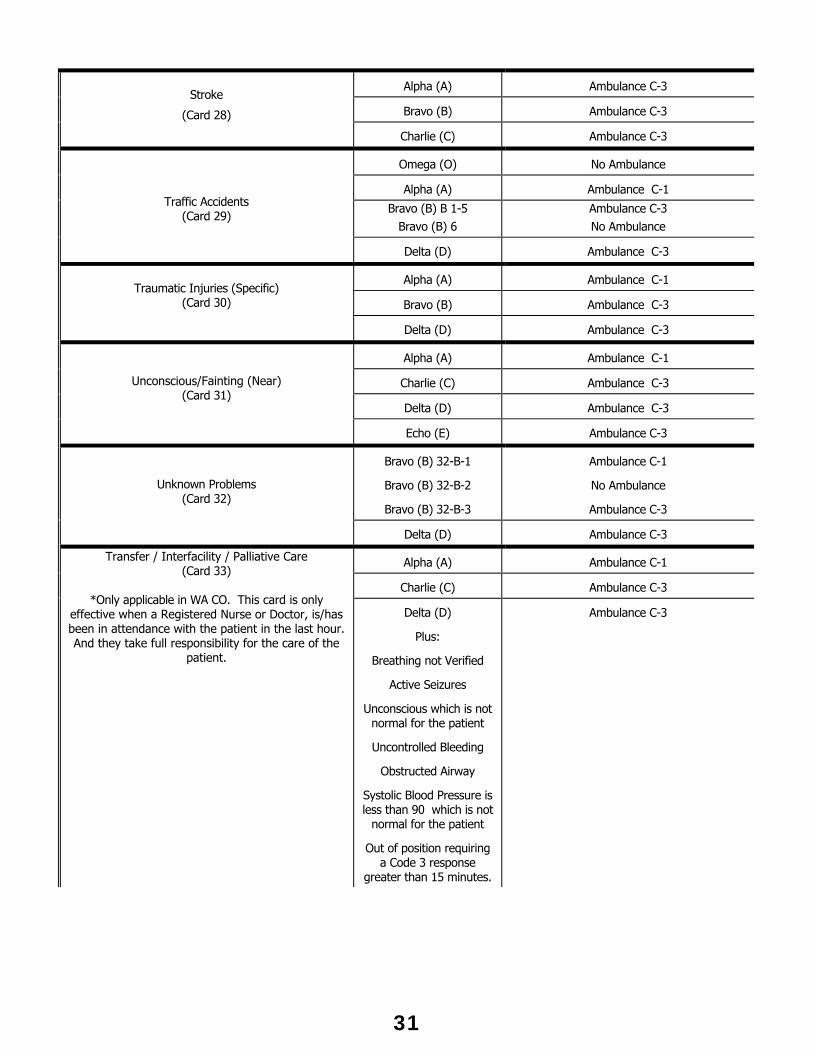
Alpha (A) Ambulance C-3
Bravo (B) Ambulance C-3
Stroke
(Card 28)
Charlie (C) Ambulance C-3
Omega (O) No Ambulance
Alpha (A) Ambulance C-1
Bravo (B) B 1-5 Bravo (B) 6
Ambulance C-3 No Ambulance
Traffic Accidents (Card 29)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Bravo (B) Ambulance C-3
Traumatic Injuries (Specific)
(Card 30)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Charlie (C) Ambulance C-3
Delta (D) Ambulance C-3
Unconscious/Fainting (Near) (Card 31)
Echo (E) Ambulance C-3
Bravo (B) 32-B-1
Bravo (B) 32-B-2
Bravo (B) 32-B-3
Ambulance C-1
No Ambulance
Ambulance C-3
Unknown Problems (Card 32)
Delta (D) Ambulance C-3
Alpha (A) Ambulance C-1
Charlie (C) Ambulance C-3
Transfer / Interfacility / Palliative Care (Card 33)
*Only applicable in WA CO. This card is only
effective when a Registered Nurse or Doctor, is/has been in attendance with the patient in the last hour. And they take full responsibility for the care of the
patient.
Delta (D)
Plus:
Breathing not Verified
Active Seizures
Unconscious which is not normal for the patient
Uncontrolled Bleeding
Obstructed Airway
Systolic Blood Pressure is less than 90 which is not
normal for the patient
Out of position requiring a Code 3 response
greater than 15 minutes.
Ambulance C-3
31
EMERGENCY MEDICAL DISPATCH (EMD) CERTIFICATION All ambulance dispatchers licensed to provide emergency or non-emergency ambulance service and 9-1-1 Center Call-Takers in Washington County shall become certified in CPR and EMD within 6 months of hire. CPR Certification The ambulance dispatcher or 9-1-1 call taker shall be recognized as proficient in American Heart Association CPR, level C or Red Cross equivalent prior to attending an Emergency Medical Dispatch Course. Emergency Medical Dispatch Certification The ambulance dispatcher or 9-1-1 call taker shall attend an Emergency Medical Dispatch course approved by the Washington County EMS Office and become certified in EMD within 6 months of hire. Each EMD certified EMS dispatcher or call-taker shall be required to successfully complete a four-hour re-certification course approved by the EMS Office every two years. Re-certification records shall be kept on file at the place of employment subject to EMS Office inspection on request.
32
LAW ENFORCEMENT CENTER (JAIL) RESPONSE
A request for EMS assistance at the Law Enforcement Center (LEC) may be made to WCCCA by LEC nursing staff or to Metro West Ambulance's Communications Center by the LEC on-duty physician. If the request for EMS assistance is made in the absence of a physician on-duty, the request shall be triaged against the emergency medical dispatch cards and the appropriate resources dispatched. If the on-duty physician requests an ambulance response only, they shall contact Metro West Ambulance Communications Center directly (503-648-6656) and request an ambulance under the direction of an on-scene physician. Metro West Ambulance shall dispatch an ambulance immediately. The request for EMS assistance does not need to be sent to WCCCA. Unless directed otherwise, access to the jail shall be through the Sally Port located on Adams St. Enter the Sally Port from the West. Once inside, position the ambulance so that other vehicles will not block you in. A guide will take you to the medical emergency. DO NOT ENTER THE JAIL WITHOUT A GUIDE OR WITHOUT THE PERMISSION OF JAIL STAFF. Take all equipment necessary to handle any type of adult medical call (e.g., monitor, oxygen, suction, medications, airway equipment, restraints, backboards, splints, c-collars etc.). Jail staff will assist in helping take equipment out of the jail. The jail is a large, very active, high security facility. Access to and from the Sally Port and ambulance will be time consuming and limited. KEEP AN EYE ON ALL EQUIPMENT. IF YOU MUST LEAVE SIGHT OF EQUIPMENT, NOTIFY JAIL STAFF AND HAVE SOMEONE WATCH IT. Request for ambulance transport may originate from the medical facility or from a jail pod. Nursing staff from the medical facility may not be in attendance if the medical emergency occurs within a pod. Upon arrival, determine if medical staff is present and interface with them for transfer of patient information. For medical-legal and security reasons the Sheriff's Department and Medical Staff request that all patients be transported from the facility if requested by jail staff. This includes patients in cardiac arrest that would normally fall into the Death in the Field Protocol.
33
MINIMUM AMBULANCE COVERAGE
This protocol does not effect units that are scheduled to go off-duty.
The minimum coverage level is the level of coverage for the County below which an emergency ambulance may not be removed from service for a non-emergency, (i.e. pre-scheduled, inter-facility, non-EMD card category) calls. The minimum coverage level is four (4) ambulances.
When the number of emergency ambulances reaches the minimum coverage level: 1. An emergency ambulance may not go out-of-service for an inter-facility request until the
number of available ambulance returns to the minimum coverage level. 2. Metro West Ambulance shall decline any out-of-county requests for mutual aid move ups
until more than four emergency ambulances are available for 9-1-1 dispatch in Washington County; however, code-3 mutual aid requests shall be honored. If the ambulance responding to the mutual aid request is canceled or does not provide transport, it shall immediately return to Washington County.
3. Inter-facility requests requiring a code-3 response, transport, or those for transfer to a trauma center as a trauma entry shall not be covered in the protocol.
34
MUTUAL AID REQUESTS
All requests for mutual aid shall be made through Metro West Ambulance and will be honored as long as the County ambulance coverage level is at least three (3).
Requests and coordination for mutual aid assistance shall be the responsibility of Metro West Ambulance. Metro West Ambulance will establish and maintain a mutual aid plan, which shall be approved by the EMS Office. Any request from outside Washington County for EMS mutual aid shall be handled as dictated by the Emergency Medical Dispatch and Minimum Ambulance Coverage Protocol for Washington County.
If Metro West requests mutual aid and then has a unit become available, Metro West shall contact the mutual aid provider and obtain the location of the mutual aid ambulance. If the Metro West unit is closer, the mutual aid ambulance shall be canceled. If the mutual aid ambulance is closer, Metro West shall cancel their response and let the mutual aid ambulance continue. The overall policy is that the nearest ambulance shall respond. All instances where a mutual aid ambulance is canceled shall be reported to the EMS Office.
If Metro West Ambulance receives a request to respond to a 9-1-1 call in: Multnomah County they must clear the response with AMR's dispatch center, unless AMR is
the caller. Clackamas County they must clear the response with AMR's dispatch center, unless AMR is
the caller. Yamhill County they must clear the response with Y-Com or Newberg Dispatch unless they
are the caller. Tillamook County they must clear the response with Tillamook 9-1-1, unless they are the
caller.
WCCCA or a local fire department does not have the authorization to request Metro West Ambulance’s response unless they clear it with the primary ambulance provider of that area.
WCCCA or a local fire department does not have the authorization to request an outside ambulance provider to respond to Washington County without first clearing it with the Metro West Ambulance Dispatch Center.
35
NON-EMERGENCY MEDICAL REQUESTS FOR SERVICE Non-emergency means those medical or trauma conditions that are not specifically dealt with in the emergency medical dispatch system adopted by the County. The County by rule shall further delineate categories contained in the emergency medical dispatch system that may be handled by a non-emergency ambulance provider. Unless specified by rule, those conditions that fall within the emergency medical dispatch system shall immediately be transferred to the emergency ambulance providers designated by Washington County. Administrative Rule 554-440-000 defines non-emergency as those medical conditions that, in the judgment of an individual certified or licensed at the emergency medical technician, registered nurse, physician assistant or physician level, are not expected to cause death, permanent disability or permanent harm within the next 24 hours and do not require a code-3 response as determined by the EMD card system. Ambulance Companies Requests for non-emergency ambulance transports occasionally are misdirected and come in as a 9-1-1 call. If, after going through the EMD card system, WCCCA determines the call is not specifically dealt with in the EMD card system, the caller shall be transferred to the ambulance company of the caller’s choice. Washington County Crisis Line If after examining a psychiatric patient, the patient is deemed not to have a medical condition, the Washington County Crisis Line (503-291-9111) should be contacted prior to transport. The following information is needed to determine where to transport the patient:
- Sex and age of patient - Date of birth - Presenting problem with precipitating events - Current and past medical history and current medications - Prior psychiatric history and current mental status - Voluntary vs. Involuntary status (a police or two physician hold is required) - Insurance status
The crisis worker may want to speak with the patient. They may be able to obtain further information, help calm the patient and facilitate an alternative option to transport. If crisis line personnel are unable to provide assistance in a timely manner (15 minutes), proceed to the nearest hospital. For patients who would go to Tuality Hospital - Forest Grove, transport the patient to Tuality Hospital -Hillsboro.
36
OUT-OF-COUNTY AMBULANCE UTILIZATION Metro West Ambulance is encouraged to develop mutual-aid plan, which shall be approved by the EMS Office. This protocol shall be used only when there are no available Washington County emergency ambulances. An out-of-county ambulance is any State licensed, paramedic staffed and equipped ambulance based outside of Washington County. For mutual aid purposes, any State licensed ambulance staffed and equipped to the paramedic level can be used in Washington County. Metro West shall coordinate of out-of-county ambulance response.
37
REDIRECTION OF AMBULANCE CALLS FOR SERVICE
Ambulance response districts do not match fire response districts. The dispatching of the correct ambulance provider to the Tualatin/Wilsonville, Gaston and Highway 99 area at the Yamhill/Washington County areas of the County has been a challenge. Fire Departments determines the fire response districts and they do not currently match ambulance provider responsibilities.
No changes will be made in the process for designation of an ambulance provider by WCCCA. Once WCCCA has designated an ambulance provider, WCCCA will send the dispatch information to Metro West or AMR. Metro West and AMR will further coordinate ambulance response between their dispatch centers. Once AMR and Metro West determine the correct ambulance, WCCCA will be notified of the ambulance dispatched.
If the ambulance recommended by WCCCA is incorrect based on the information provided the ambulance provider will immediately contact the correct ambulance provider and transfer the call information. The designated ambulance provider will immediately contact WCCCA and notify them of the change in ambulance providers.
The EMS Office will provide Metro West and AMR with fire management zone maps, which will contain the correct ambulance response to the borderline areas mentioned above. Metro West and AMR will be asked to verify that their computer aided dispatch system correctly recommends the appropriate ambulance response.
If there is disagreement between Metro West and AMR has to who the correct ambulance provider is, the ambulance provider initially designated by WCCCA will handle the call. In these situations the Washington County EMS Office shall be provided with the incident information.
38
REQUEST FOR AMBULANCE RESPONSE FROM HOSPICE AGENCIES When Metro West Ambulance receives a request from an authorized hospice agency, these requests do not need to be triaged against the approved Washington County EMD card system if the caller gives the information specified below. An authorized hospice agency is an agency on file with the EMS office. The ambulance response shall be Code 1 and no fire department response shall be sent. The individual who is making the request for ambulance service must provide the following information: The caller's name and title. That the patient is a hospice patient. The name of the hospice. That the request is for NON-EMERGENCY transportation. The hospice's EMS ID Number. The patient must be located in Washington County. Any request for "as soon as possible", "urgent", "right away" or any other terminology that would imply a degree of urgency shall be triaged against the approved Washington County EMD card system. Any request for transport received from a family member or third party shall be triaged according to the EMD card system.
AUTHORIZED HOSPICE AGENCIES Hopewell House Providence Medical Center Hospice Legacy Visiting Nurses Hospice 6171 SW Capitol Hwy. 1235 NE 47 Av., Suite 215 P.O. Box 3426 Portland, OR 97201 Portland, OR 97213 Portland, OR 97208 (503) 244-7890 (503) 331-4601 (503) 225-6370 EMS ID#: HOS/01 EMS ID#: HOS/06 EMS ID#: HOS/04 Hospice of St. Vincent VA Medical Center Washington County Hospice 9340 Barnes Rd P.O. Box 1035 (11V) 427 SE 8 Av. Portland, OR 97225 Portland, OR 97207 Hillsboro, OR 97123 (503) 297-6109 (503) 220-8262 X3378 (503) 648-9565 EMS ID#: HOS/02 EMS ID#: HOS/07 EMS ID#: HOS/09 Kaiser Permanente Hospice Mt. Hood Hospice Willamette Falls Hospice 2701 NW Vaughn St., #140 P.O. Box 835 1678 Beavercreek Rd, Suite K Portland, OR 97210 Sandy, OR 97055 Oregon City, OR 97045 (503) 499-5210 (503) 668-5545 (503) 655-0550 EMS ID#: HOS/03 EMS ID#: HOS/08 EMS ID#: HOS/10 Portland Adventist Hospice 10201 SE Main St., #1 Portland, OR 97216 (503) 251-6192 EMS ID#: HOS/05
39
REQUEST FOR SERVICE AT THE DIRECTION OF A PHYSICIAN OR NURSING HOME/EXTENDED
CARE FACILITY REGISTERED NURSE PHYSICIAN Any request for ambulance service made by, or at the direction of a physician shall receive the response requested if the physician is now on the scene or has been there to evaluate the patient within the last one (1) hour. This protocol shall not apply in the case of a suspected or confirmed cardiac arrest, if the patient is having seizure activity or an airway obstruction. Calls originated by all other medical personnel in the absence of a physician shall be handled according to the Emergency Medical Dispatch Card System. Before honoring the request for service the following information must be provided:
- The physician who made the request is identified by name. - They are a licensed M.D. or D.O., at the scene or have evaluated the patient
within the last one (1) hour. - They agree to take full responsibility for the care of the patient.
If a call is received from a person identifying himself/herself as a physician, the dispatcher will elicit the same patient information as if the caller were an untrained citizen. The purpose for this is to provide the maximum amount of information to responding units. If caller is unable to provide sufficient information to answer "key questions," response shall be as directed by the EMD card. NURSING HOME/EXTENDED CARE FACILITY REGISTERED NURSE Calls received from nursing homes and care facilities where there is a Registered Nurse in attendance of the patient do not require a fire response unless:
1. The patient’s breathing status can not be verified. 2. The patient is in active seizures. 3. The patient is unconscious which is not normal for the patient. 4. The patient has uncontrolled bleeding. 5. The patient has an obstructed airway. 6. The patient’s systolic blood pressure is less than 90mmHg, which is not normal for
the patient. 7. The ambulance response is greater than 15 minutes.
40
RETURN OF FIRE PERSONNEL BY AMBULANCE PROVIDERS Firefighters accompanying an ambulance may remain at the hospital until they are retrieved by their agency.
When the ambulance unit is ready to depart the destination hospital, if the ambulance provider is above a level four (4), the firefighter shall be returned to their station of origin or other location to meet a Supervisors Unit to finish the return.
When the ambulance unit is ready to depart the destination hospital, if the ambulance provider is below level four (4), the firefighter shall be returned to one of the following locations based on the ambulance’s next posting location: - Their department, district or station of origin.
- Tuality Hospital Emergency Department. - WCCCA. - St. Vincent Hospital
Upon leaving the destination hospital, ambulance personnel shall contact WCCCA and ask them to notify the fire fighter's department or district of the drop-off location and the estimated time of arrival to that location.
If an ambulance is responding to a drop-off location and is needed to respond to a code 3 call, the ambulance shall respond to the code 3 call. WCCCA shall notify the fire fighter's department or district that they will not be dropped off as previously planned. Once the ambulance arrives at the scene of the emergency, the firefighter should try to make arrangements with other fire personnel on scene, even if they are from different departments or districts, to be returned to their station.
At no time shall fire personnel be left in an unsecured location.
41
SLOW DOWN/CANCELLATION POLICY
First Responder Certified or certified law enforcement officer May slow an ambulance to Code 1 only after the patient has received a complete patient assessment and the person-in-charge determines that the patient's medical condition is stable. The ambulance will continue Code 1 and assess the patient.
EMT-Basic, Intermediate, Paramedic May slow or cancel other responders once the patient has been fully evaluated. Metro West Ambulance Communications Center Dispatchers have the right to substitute units on responses initially dispatched or reduced to Code 1 if the unit being substituted is diverted to a response initially dispatched or increased to Code 3. Metro West Communications Center will then assign the next closest, most appropriate unit to the initial Code 1 response. Metro West Communications Center will notify WCCCA of the substitution as soon as practical.
Metro West Ambulance Communications Center Dispatchers have the authority to modify the dispatch priority of an ambulance based on information provided by WCCCA or field units.
42
SUSPECTED DECEASED PERSON/OBVIOUS DEATH SITUATION
Upon receipt of a suspected deceased person or obvious death situation, all of the following questions shall be used to determine if a full EMS response is indicated: (NOTE: Declaring a person dead without a visual assessment can place a dispatcher in a difficult position. An incorrect assessment may result in liability exposure.) All of these questions shall be used in addition to the Key Questions required by MPDS© on EMD card #9. - Are you calling because you want the patient to receive medical care and resuscitation? If
the answer is yes, the call is to be dispatched as a Cardiac Arrest-Delta 1. - Is this an expected death? - Did a physician tell you the patient was dying? - Does the patient have a Do Not Resuscitate Order (DNR) Ambulance Directive? What does it
say? (The caller must have the DNR/Advance Directive in-hand.) - Is the patient involved in a Hospice program? Have you called them? - When was the last time you saw the patient conscious? - What happens when you gently shake the patient? - Does the patient's chest feel cold? - What does their skin look like? - What do the patient's eyes look like? (glazed/dry/unresponsive) Are they open?
If the patient is determined to be deceased, the call shall be dispatched as a Cardiac Arrest-Bravo 1. If in doubt as to the patient's condition, dispatch the call as a Cardiac Arrest-Delta 1. Calls triaged by WCCCA as an obvious death, do not include an ambulance.
43
TRAFFIC ACCIDENT UNKNOWN SITUATION (THIRD-PARY CALLER)
This guideline is for a traffic accident where the reporting party either heard or saw what they think is a traffic accident but is not present and cannot provide first hand information. This guideline shall not be used for situations where the reporting party is with people involved in the accident but does not think they are injured. Any suspicion that injuries are present, an ambulance shall be dispatched.
IF AN AMBULANCE IS IN A POSITION TO ARRIVE BEFORE THE FIRE RESPONDER, THEY ARE AUTHORIZED TO RESPOND EVEN IF THEY ARE NOT INITIALLY DISPATCHED.
TVF&R HILLSBORO FIRE DEPARTMENT CORNELIUS RFPD No ambulance is to be dispatched.
FOREST GROVE RFPD - Highway 6 North and West of Highway 6 and Gales Creek Road intersection: Stage at
intersection of Highway 6 and Gales Creek Road. - Gales Creek Road from Forest Grove City limits to intersection of Highway 6 and Gales
Greek Road: Stage at Gales Creek Road and Forest Gale Drive. - Highway 47 from Forest Grove to Highway 26: Stage at Highway 47 North and Forest
Grove City limits. - Wilson River Highway from Gales Creek Road to Highway 26: Stage at Highway 47 and
Forest Grove City Limits. - Highway 47 South from Forest Grove to Gaston: Stage at Highway 47 South at Forest
Grove City limits.
GASTON RFPD - Scoggins Valley Road: Stage at Highway 47 and Scoggins Valley Road.
BANKS FIRE DISTRICT #13 - Highway 26 west of Highway 47 to County line: Stage at Highway 47 and Highway 26.
WASHINGTON COUNTY RFPD #2 - Highway 26 between Highway 47 and 26 intersection and Hillsboro city limits: Stage at
Glencoe and Evergreen - North of Highway 26 in Washington County RFPD #2 response area: Stage at North
Plains Station. - Highway 219 from Hillsboro City limits to Highway 210 and all roads branching: Stage at
Farmington View School. - Highway 10 from Beaverton to Highway 219 and all roads branching: Stage at Highway
10 and Beaverton City limits. - Highway 210 and all roads branching: Stage at the intersection of Highway 210 and
Highway 10.
44
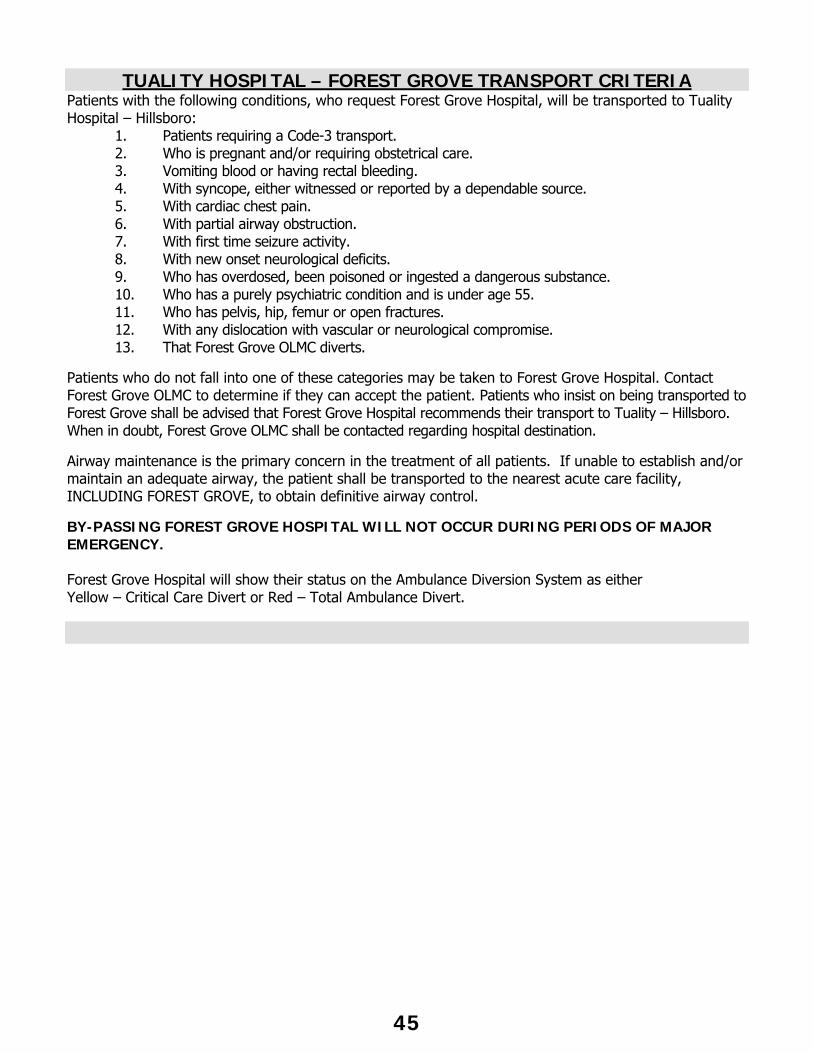
TUALITY HOSPITAL – FOREST GROVE TRANSPORT CRITERIA
Patients with the following conditions, who request Forest Grove Hospital, will be transported to Tuality Hospital – Hillsboro:
1. Patients requiring a Code-3 transport. 2. Who is pregnant and/or requiring obstetrical care. 3. Vomiting blood or having rectal bleeding. 4. With syncope, either witnessed or reported by a dependable source. 5. With cardiac chest pain. 6. With partial airway obstruction. 7. With first time seizure activity. 8. With new onset neurological deficits. 9. Who has overdosed, been poisoned or ingested a dangerous substance. 10. Who has a purely psychiatric condition and is under age 55. 11. Who has pelvis, hip, femur or open fractures. 12. With any dislocation with vascular or neurological compromise. 13. That Forest Grove OLMC diverts.
Patients who do not fall into one of these categories may be taken to Forest Grove Hospital. Contact Forest Grove OLMC to determine if they can accept the patient. Patients who insist on being transported to Forest Grove shall be advised that Forest Grove Hospital recommends their transport to Tuality – Hillsboro. When in doubt, Forest Grove OLMC shall be contacted regarding hospital destination.
Airway maintenance is the primary concern in the treatment of all patients. If unable to establish and/or maintain an adequate airway, the patient shall be transported to the nearest acute care facility, INCLUDING FOREST GROVE, to obtain definitive airway control. BY-PASSING FOREST GROVE HOSPITAL WILL NOT OCCUR DURING PERIODS OF MAJOR EMERGENCY. Forest Grove Hospital will show their status on the Ambulance Diversion System as either Yellow – Critical Care Divert or Red – Total Ambulance Divert.
45
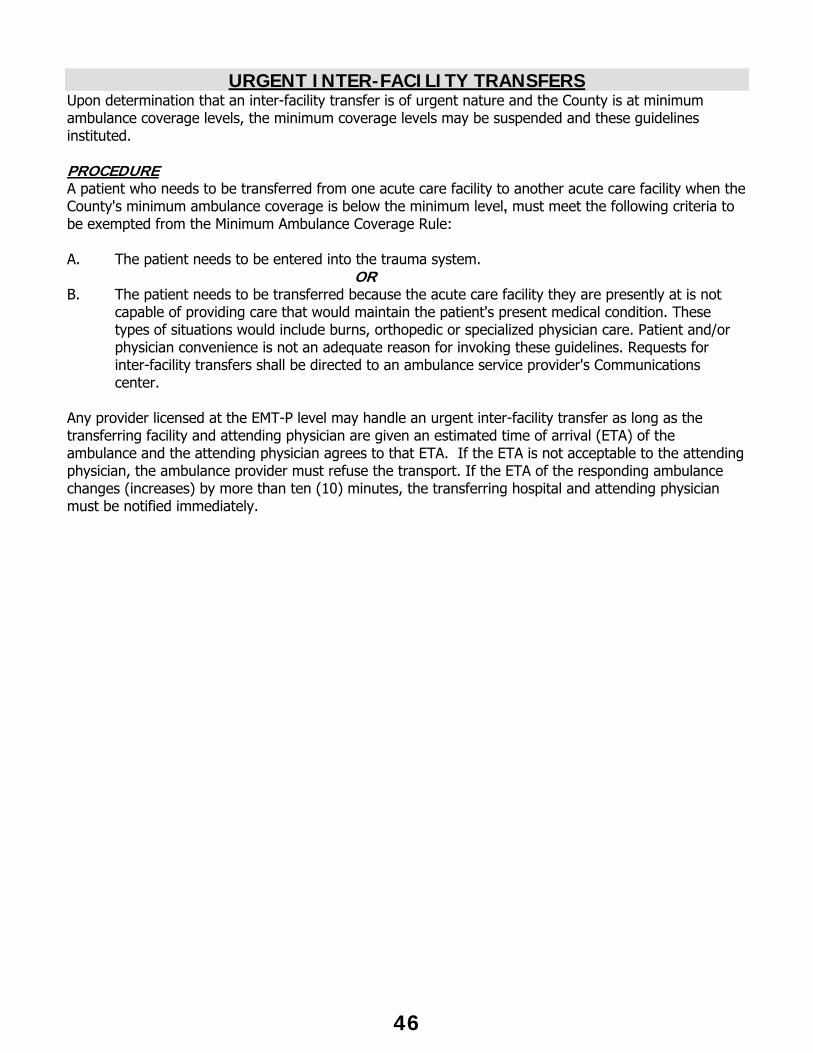
URGENT INTER-FACILITY TRANSFERS
Upon determination that an inter-facility transfer is of urgent nature and the County is at minimum ambulance coverage levels, the minimum coverage levels may be suspended and these guidelines instituted. PROCEDURE A patient who needs to be transferred from one acute care facility to another acute care facility when the County's minimum ambulance coverage is below the minimum level, must meet the following criteria to be exempted from the Minimum Ambulance Coverage Rule: A. The patient needs to be entered into the trauma system. OR B. The patient needs to be transferred because the acute care facility they are presently at is not
capable of providing care that would maintain the patient's present medical condition. These types of situations would include burns, orthopedic or specialized physician care. Patient and/or physician convenience is not an adequate reason for invoking these guidelines. Requests for inter-facility transfers shall be directed to an ambulance service provider's Communications center.
Any provider licensed at the EMT-P level may handle an urgent inter-facility transfer as long as the transferring facility and attending physician are given an estimated time of arrival (ETA) of the ambulance and the attending physician agrees to that ETA. If the ETA is not acceptable to the attending physician, the ambulance provider must refuse the transport. If the ETA of the responding ambulance changes (increases) by more than ten (10) minutes, the transferring hospital and attending physician must be notified immediately.
46

47
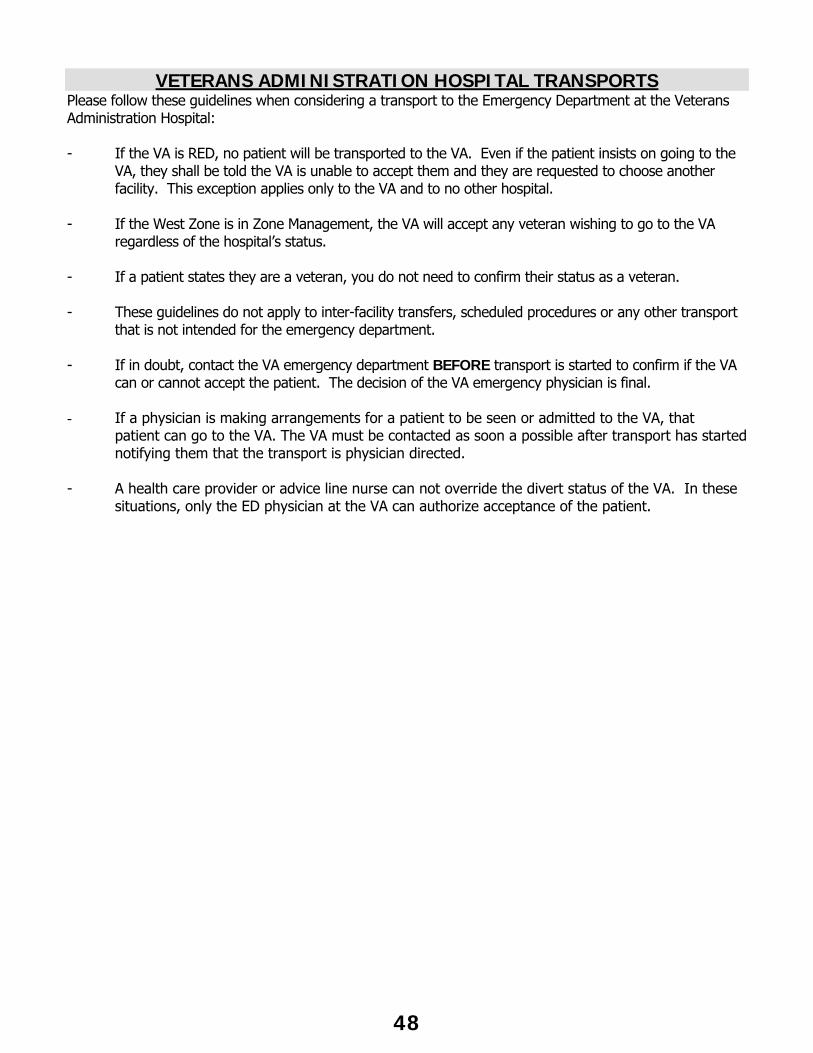
VETERANS ADMINISTRATION HOSPITAL TRANSPORTS
Please follow these guidelines when considering a transport to the Emergency Department at the Veterans Administration Hospital: - If the VA is RED, no patient will be transported to the VA. Even if the patient insists on going to the
VA, they shall be told the VA is unable to accept them and they are requested to choose another facility. This exception applies only to the VA and to no other hospital.
- If the West Zone is in Zone Management, the VA will accept any veteran wishing to go to the VA
regardless of the hospital’s status. - If a patient states they are a veteran, you do not need to confirm their status as a veteran. - These guidelines do not apply to inter-facility transfers, scheduled procedures or any other transport
that is not intended for the emergency department. - If in doubt, contact the VA emergency department BEFORE transport is started to confirm if the VA
can or cannot accept the patient. The decision of the VA emergency physician is final. - If a physician is making arrangements for a patient to be seen or admitted to the VA, that
patient can go to the VA. The VA must be contacted as soon a possible after transport has started notifying them that the transport is physician directed.
- A health care provider or advice line nurse can not override the divert status of the VA. In these
situations, only the ED physician at the VA can authorize acceptance of the patient.
48
OPERATIONAL PROTOCOLS
49
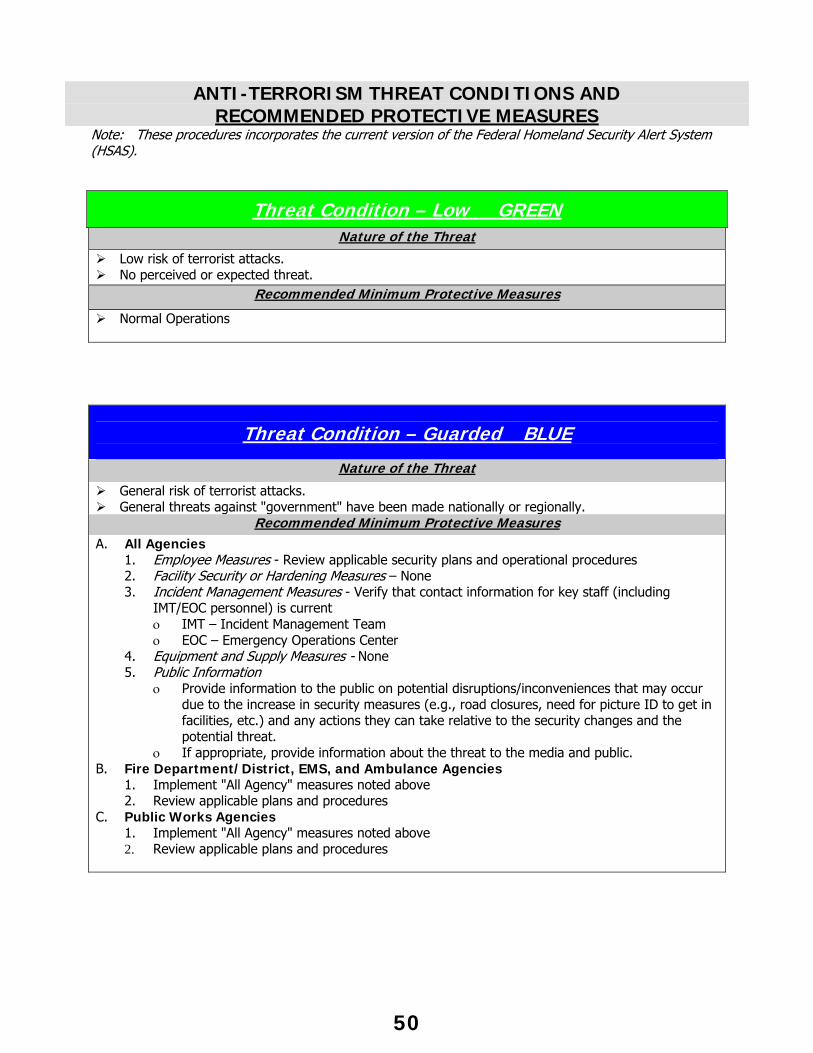
ANTI-TERRORISM THREAT CONDITIONS AND RECOMMENDED PROTECTIVE MEASURES
Note: These procedures incorporates the current version of the Federal Homeland Security Alert System (HSAS).
Threat Condition – Low GREEN Nature of the Threat
Low risk of terrorist attacks. No perceived or expected threat.
Recommended Minimum Protective Measures
Normal Operations
Threat Condition – Guarded BLUE
Nature of the Threat
General risk of terrorist attacks. General threats against "government" have been made nationally or regionally.
Recommended Minimum Protective Measures
A. All Agencies 1. Employee Measures - Review applicable security plans and operational procedures 2. Facility Security or Hardening Measures – None 3. Incident Management Measures - Verify that contact information for key staff (including
IMT/EOC personnel) is current IMT – Incident Management Team EOC – Emergency Operations Center
4. Equipment and Supply Measures - None 5. Public Information
Provide information to the public on potential disruptions/inconveniences that may occur due to the increase in security measures (e.g., road closures, need for picture ID to get in facilities, etc.) and any actions they can take relative to the security changes and the potential threat.
If appropriate, provide information about the threat to the media and public. B. Fire Department/District, EMS, and Ambulance Agencies
1. Implement "All Agency" measures noted above 2. Review applicable plans and procedures
C. Public Works Agencies 1. Implement "All Agency" measures noted above 2. Review applicable plans and procedures
50
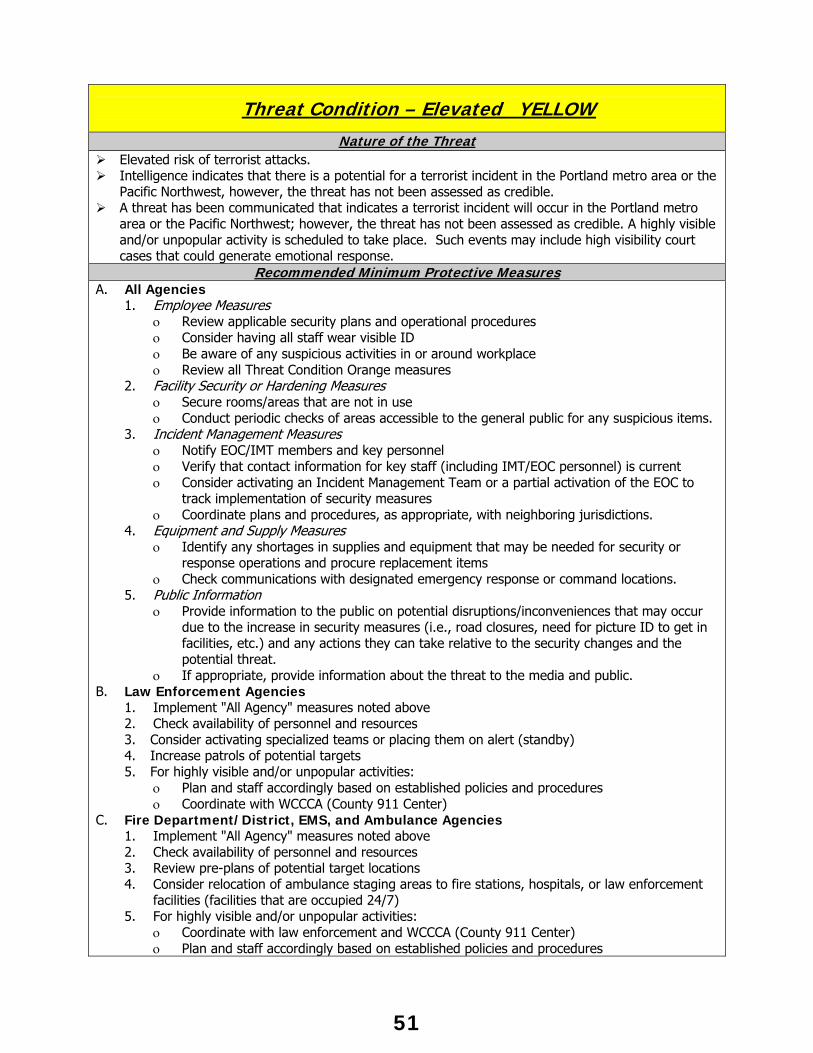
Threat Condition – Elevated YELLOW
Nature of the Threat Elevated risk of terrorist attacks. Intelligence indicates that there is a potential for a terrorist incident in the Portland metro area or the
Pacific Northwest, however, the threat has not been assessed as credible. A threat has been communicated that indicates a terrorist incident will occur in the Portland metro
area or the Pacific Northwest; however, the threat has not been assessed as credible. A highly visible and/or unpopular activity is scheduled to take place. Such events may include high visibility court cases that could generate emotional response.
Recommended Minimum Protective Measures A. All Agencies
1. Employee Measures Review applicable security plans and operational procedures Consider having all staff wear visible ID Be aware of any suspicious activities in or around workplace Review all Threat Condition Orange measures
2. Facility Security or Hardening Measures Secure rooms/areas that are not in use Conduct periodic checks of areas accessible to the general public for any suspicious items.
3. Incident Management Measures Notify EOC/IMT members and key personnel Verify that contact information for key staff (including IMT/EOC personnel) is current Consider activating an Incident Management Team or a partial activation of the EOC to
track implementation of security measures Coordinate plans and procedures, as appropriate, with neighboring jurisdictions.
4. Equipment and Supply Measures Identify any shortages in supplies and equipment that may be needed for security or
response operations and procure replacement items Check communications with designated emergency response or command locations.
5. Public Information Provide information to the public on potential disruptions/inconveniences that may occur
due to the increase in security measures (i.e., road closures, need for picture ID to get in facilities, etc.) and any actions they can take relative to the security changes and the potential threat.
If appropriate, provide information about the threat to the media and public. B. Law Enforcement Agencies
1. Implement "All Agency" measures noted above 2. Check availability of personnel and resources 3. Consider activating specialized teams or placing them on alert (standby) 4. Increase patrols of potential targets 5. For highly visible and/or unpopular activities:
Plan and staff accordingly based on established policies and procedures Coordinate with WCCCA (County 911 Center)
C. Fire Department/District, EMS, and Ambulance Agencies 1. Implement "All Agency" measures noted above 2. Check availability of personnel and resources 3. Review pre-plans of potential target locations 4. Consider relocation of ambulance staging areas to fire stations, hospitals, or law enforcement
facilities (facilities that are occupied 24/7) 5. For highly visible and/or unpopular activities:
Coordinate with law enforcement and WCCCA (County 911 Center) Plan and staff accordingly based on established policies and procedures
51
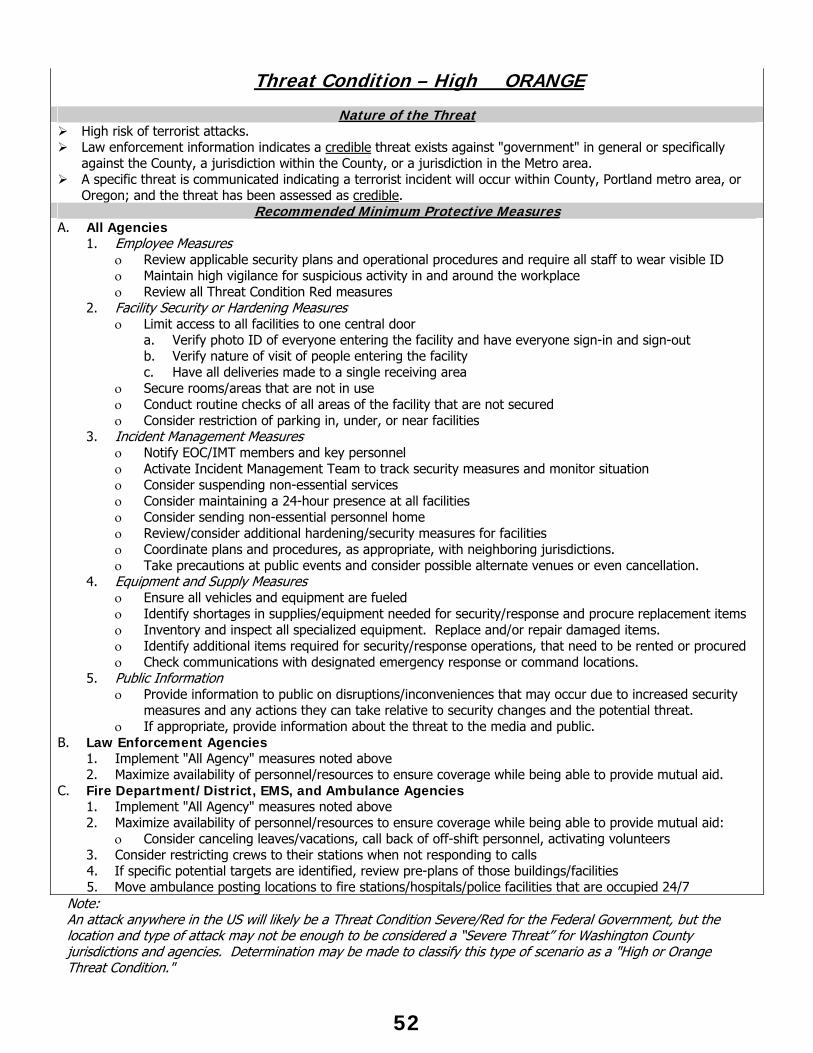
52
Threat Condition – High ORANGE
Nature of the Threat High risk of terrorist attacks. Law enforcement information indicates a credible threat exists against "government" in general or specifically
against the County, a jurisdiction within the County, or a jurisdiction in the Metro area. A specific threat is communicated indicating a terrorist incident will occur within County, Portland metro area, or
Oregon; and the threat has been assessed as credible. Recommended Minimum Protective Measures
A. All Agencies 1. Employee Measures
Review applicable security plans and operational procedures and require all staff to wear visible ID Maintain high vigilance for suspicious activity in and around the workplace Review all Threat Condition Red measures
2. Facility Security or Hardening Measures Limit access to all facilities to one central door
a. Verify photo ID of everyone entering the facility and have everyone sign-in and sign-out b. Verify nature of visit of people entering the facility c. Have all deliveries made to a single receiving area
Secure rooms/areas that are not in use Conduct routine checks of all areas of the facility that are not secured Consider restriction of parking in, under, or near facilities
3. Incident Management Measures Notify EOC/IMT members and key personnel Activate Incident Management Team to track security measures and monitor situation Consider suspending non-essential services Consider maintaining a 24-hour presence at all facilities Consider sending non-essential personnel home Review/consider additional hardening/security measures for facilities Coordinate plans and procedures, as appropriate, with neighboring jurisdictions. Take precautions at public events and consider possible alternate venues or even cancellation.
4. Equipment and Supply Measures Ensure all vehicles and equipment are fueled Identify shortages in supplies/equipment needed for security/response and procure replacement items Inventory and inspect all specialized equipment. Replace and/or repair damaged items. Identify additional items required for security/response operations, that need to be rented or procured Check communications with designated emergency response or command locations.
5. Public Information Provide information to public on disruptions/inconveniences that may occur due to increased security
measures and any actions they can take relative to security changes and the potential threat. If appropriate, provide information about the threat to the media and public.
B. Law Enforcement Agencies 1. Implement "All Agency" measures noted above 2. Maximize availability of personnel/resources to ensure coverage while being able to provide mutual aid.
C. Fire Department/District, EMS, and Ambulance Agencies 1. Implement "All Agency" measures noted above 2. Maximize availability of personnel/resources to ensure coverage while being able to provide mutual aid:
Consider canceling leaves/vacations, call back of off-shift personnel, activating volunteers 3. Consider restricting crews to their stations when not responding to calls
4. If specific potential targets are identified, review pre-plans of those buildings/facilities 5. Move ambulance posting locations to fire stations/hospitals/police facilities that are occupied 24/7
Note: An attack anywhere in the US will likely be a Threat Condition Severe/Red for the Federal Government, but the location and type of attack may not be enough to be considered a “Severe Threat” for Washington County jurisdictions and agencies. Determination may be made to classify this type of scenario as a "High or Orange Threat Condition."
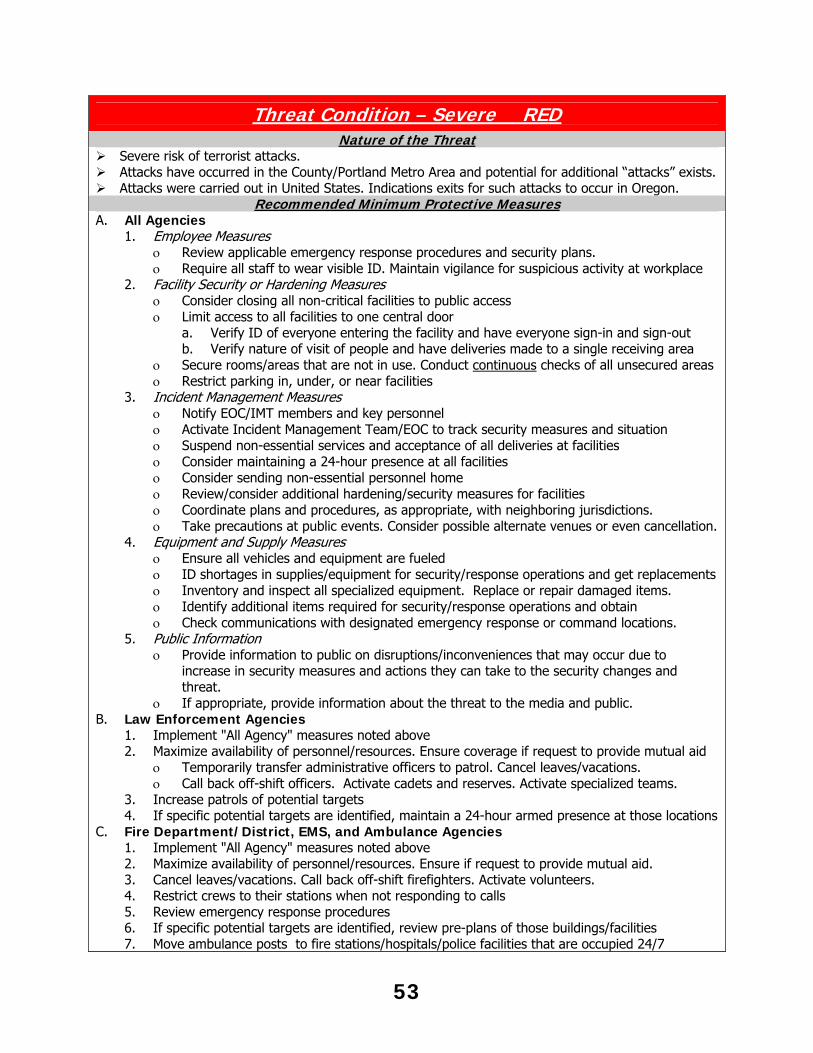
Threat Condition – Severe RED Nature of the Threat
Severe risk of terrorist attacks. Attacks have occurred in the County/Portland Metro Area and potential for additional “attacks” exists. Attacks were carried out in United States. Indications exits for such attacks to occur in Oregon.
Recommended Minimum Protective Measures A. All Agencies
1. Employee Measures Review applicable emergency response procedures and security plans. Require all staff to wear visible ID. Maintain vigilance for suspicious activity at workplace
2. Facility Security or Hardening Measures Consider closing all non-critical facilities to public access Limit access to all facilities to one central door
a. Verify ID of everyone entering the facility and have everyone sign-in and sign-out b. Verify nature of visit of people and have deliveries made to a single receiving area
Secure rooms/areas that are not in use. Conduct continuous checks of all unsecured areas Restrict parking in, under, or near facilities
3. Incident Management Measures Notify EOC/IMT members and key personnel Activate Incident Management Team/EOC to track security measures and situation Suspend non-essential services and acceptance of all deliveries at facilities Consider maintaining a 24-hour presence at all facilities Consider sending non-essential personnel home Review/consider additional hardening/security measures for facilities Coordinate plans and procedures, as appropriate, with neighboring jurisdictions. Take precautions at public events. Consider possible alternate venues or even cancellation.
4. Equipment and Supply Measures Ensure all vehicles and equipment are fueled ID shortages in supplies/equipment for security/response operations and get replacements Inventory and inspect all specialized equipment. Replace or repair damaged items. Identify additional items required for security/response operations and obtain Check communications with designated emergency response or command locations.
5. Public Information Provide information to public on disruptions/inconveniences that may occur due to
increase in security measures and actions they can take to the security changes and threat.
If appropriate, provide information about the threat to the media and public. B. Law Enforcement Agencies
1. Implement "All Agency" measures noted above 2. Maximize availability of personnel/resources. Ensure coverage if request to provide mutual aid
Temporarily transfer administrative officers to patrol. Cancel leaves/vacations. Call back off-shift officers. Activate cadets and reserves. Activate specialized teams.
3. Increase patrols of potential targets 4. If specific potential targets are identified, maintain a 24-hour armed presence at those locations
C. Fire Department/District, EMS, and Ambulance Agencies 1. Implement "All Agency" measures noted above 2. Maximize availability of personnel/resources. Ensure if request to provide mutual aid. 3. Cancel leaves/vacations. Call back off-shift firefighters. Activate volunteers. 4. Restrict crews to their stations when not responding to calls 5. Review emergency response procedures 6. If specific potential targets are identified, review pre-plans of those buildings/facilities 7. Move ambulance posts to fire stations/hospitals/police facilities that are occupied 24/7
53
FIRE DEPARTMENT PARAMEDIC RESCUE TRANSPORT WHEN AN AMBULANCE IS UNAVAILABLE
A licensed paramedic staffed/equipped fire unit may transport if after assessment, the patient requires a code-3 transport and the ambulance have not arrived.
CODE-3 TRANSPORT The following conditions are a non-exclusive list of when code 3 transport may be necessary: Inability to secure an adequate airway Inability to stabilize blood pressure (<90mmHg systolic). Trauma entry patients Cardiac or respiratory arrest Seizure, unresponsive to treatment Abnormal childbirth Severe respiratory distress unresponsive to treatment Cardiac chest pain with dysrhythmias or unrelieved by Nitroglycerin An MCI or MPS when transport will be delayed due to ambulance depletion
CODE-1 TRANSPORT If the patient's condition does not require a code-3 transport and the ETA of the code-3 ambulance is 15 or more minutes and the patient is ready for transport, (packaged and in the back of the rescue), transport is authorized. REQUIREMENTS FOR DETERMINING AMBULANCE E.T.A. The PIC must request the location and ETA of the ambulance when the patient is ready for transport. If the ambulance fails to respond, the PIC shall again request the information. If the ambulance fails to respond, PIC shall use their judgment in determining the ETA. The PIC attempt to communicate directly with the ambulance on the TAC channel. If ambulance fails to arrive within 15 minutes after the ETA is requested, transport is authorized. REVIEW The EMS Office shall review all transports by a paramedic fire unit. Based on the signs and symptoms listed on the PCF, the EMS Office will determine if the patient needed to be transported to the hospital Code-3. In the case of a non-critical patient, the EMS Office shall also determine if the ETA requirements were followed. The EMS Office shall make a finding if the protocol was followed and, at its discretion, take appropriate regulatory action. All units used to fulfill this protocol must have all State and Local licenses or variances. TRANSPORT BY EMT-I, EMT-B OR FIRST RESPONDER STAFFED UNITS The criteria for determining transport shall be the same as for a paramedic-staffed unit. Fire units staffed by EMT-Is, EMT-Bs or First Responders shall utilize all necessary means to have the patient transported by ambulance. This could mean meeting the ambulance mid-way and transfer the patient or providing all necessary care possible to minimize scene time when the ambulance arrives. An EMT-I, EMT-B or First Responder staffed unit must contact the responding ambulance with a report on the patient’s condition and seeking advice on transport prior to transport being authorized.
54
FIREFIGHTER SAFETY AND RESCUE GUIDELINES WASHINGTON COUNTY STANDARDIZED
COMMON TERMINOLOGY Abandon: Used to direct companies or crews operating in the hazard zone to immediately exit via escape routes to a safety zone. The order to “abandon the building” directs all companies or crews in the hazard zone to immediately exit to a safety zone. Companies or crews abandoning the hazard zone will take only the tools, equipment, and hose lines necessary to permit their emergency egress.
Safety Zone: An area of safe refuge located outside the hazard zone.
Withdraw: Used to order a controlled tactical movement from current operating positions to a safer location. Offensive operations at a structure fire could be shifted to defensive by ordering the companies to “withdraw from the building”. Companies or crews withdrawing from an operating position will remove tools, equipment, and hose.
Evacuate: Will be limited to removal of civilians who are exposed or potentially exposed to hazards presented by the incident, i.e. evacuation of exposures at a structure fire or evacuation conducted downwind of a hazardous materials release.
Emergency Traffic: Is the phrase used in radio communications to indicate a critical, life safety related message. Has priority over all other radio communications with the exception of a mayday message.
Mayday: Is the signal word used in radio communications to indicate a missing, trapped, or injured firefighter in need of assistance. Mayday messages have absolute priority over all other radio communications.
Emergency Button Activation: WCCCA will follow procedures as outlined in R-7 of their Operations Directives.
P.A.R.: Personnel Accountability Report is used to determine the status of all personnel on the scene. EMERGENCY CHANNEL The Incident Commander will monitor the assigned WORKING channel and the MAYDAY channel (position 16 on all portable radios), unless the Incident Commander assigns a designee (Safety Officer, RIT Officer, etc.) to monitor the MAYDAY channel if deemed more appropriate for the incident. Any member with an emergency traffic or mayday message will transmit that message on the WORKING channel. If they are unable to contact the Incident Commander on the WORKING channel, they will immediately retransmit the message on the MAYDAY channel. Finally, if unable to contact on the MAYDAY channel the member will try to transmit on the DISPATCH channel.
55
If Command receives an emergency traffic or mayday message via Dispatch, he or she must immediately retransmit the message over the assigned WORKING channel. If Command is notified of an Emergency Button Activation, they will call for a PAR.
EMERGENCY TRAFFIC “Emergency traffic” is used to request priority access for communications critical to life safety. Situations in which emergency traffic communications are indicated include (but are not limited to):
- Abandoning the hazard zone - Reporting extreme safety hazards such as imminent structural collapse - Changing strategy from offense to defense - Requesting additional resources in a critical situation
Emergency traffic has priority over all other radio communications (with the exception of a mayday message). All other radio traffic must cease and personnel must monitor the emergency traffic message. Emergency traffic communications follow the standard radio communications model as outlined in the following example:
“Command, Truck 67 with emergency traffic.” “Truck 67, Command, go ahead with your emergency traffic.”
“A large section of roof has collapsed on Side Bravo.” “Command copies, a large section of roof has collapsed on Side Bravo”.
TRANSMITTING THE MAYDAY “Mayday” is used to clearly communicate that a firefighter is missing, trapped, or injured and in need of assistance. It is used to differentiate this type of emergency from others that may be communicated using the “emergency traffic” signal phrase. Company Officers who suspect a Firefighter is missing must notify Command immediately. Command must always assume that the missing Firefighter is lost until the member is located.
When transmitting a mayday message, the location or last known location of the person or persons requiring assistance must be identified. For example:
“Mayday, Mayday, Command, Engine 813” “Engine 813, Command”
“Firefighter Smith off Engine 813 is missing, last known location on Floor 1, Side Delta” “Command copies…”
“Mayday, Mayday, Command, Engine 813” “Engine 813, Command”
“I have a firefighter trapped on Floor 1, Side Delta” “Command copies…”
The mayday message provides a heads up for the Rapid Intervention Team, who will receive specific tasking from Command.
56
ABANDONING THE HAZARD ZONE Rapidly developing hazardous conditions may require Command to order all companies and crews operating in the hazard zone to abandon that area of operation and immediately exit to a safe area. In a wildland/urban interface incident or other incident with a variable perimeter, safety zones must be defined by proclamation (i.e. the Safety Zone is located at…). In structure fires, safety zones are pre-defined at the corners of the structure and outside the collapse zone (others may be defined by proclamation).
Communicating the order to abandon the hazard zone is accomplished through both emergency traffic radio communication and an audible signal. An order to abandon the hazard zone deviates from the standard radio communications model as it is broadcast to all companies and crews (rather than specifically directed).
“All Companies, Command, with emergency traffic. Abandon the building, abandon the building.”
Upon receipt of an order to abandon the hazard zone, and if directed by the Incident Commander, all Apparatus Operators in the immediate area of the incident will sound their air horn with one long continuous blast lasting for a count of 10. This audible signal provides a backup to radio communications.
Following the order to abandon the hazard zone, Command must account for all resources operating at the incident by initiating personnel accountability report (PAR).
CALLING FOR A PAR Command should consider calling for a PAR when,
- There is a MAYDAY - Significant changes in fire behavior - Catastrophic event (roof or wall collapse) - Change from Offensive to Defensive attack - Following the order to abandon the hazard zone
- When the IC deems it appropriate
When a PAR is called for by Command, supervisors will report either, - PAR is complete and the resources present.
“PAR Complete, with Engines 62, 64, and 107” - PAR with resources present, those missing, and the missing resources last known
location. “PAR with Engine 62 and 64, missing Engine 107, last known location Floor 2, Bravo side”
- or PAR not completed, stand-by. “PAR not completed, stand-by”
57
LIFE FLIGHT COORDINATION Coordination of Life Flight shall be done by WCCCA. Standby Criteria Whenever an EMD card specifies, responding unit requests or dispatchers receives information which they feel may warrant its use, Life Flight shall be placed on "standby." Standby Procedure WCCCA shall be responsible for placing Life Flight on standby. Ground units should be notified when Life Flight has been placed on standby. Stand Down
As soon as a medical unit at the scene determines that Life Flight is not needed Life Flight should stand down. The decision to stand down Life Flight shall be made by the paramedic- (person)-in-charge (PIC). Cancellation Procedure
As soon as the PIC determines that Life Flight is not needed, WCCCA shall contact Life Flight and notify them to cancel. The decision should be made as soon as it is practical to free Life Flight for other calls. Activation Procedure As soon as the PIC on the scene determines that Life Flight is needed, WCCCA shall notify Life Flight to activate. Upon ordering activation, WCCCA will advise Life Flight of the following information:
- Unit number of the medical unit to contact and radio frequency on which to contact that unit.
- Any additional location information or updated incident information available. - Landing zone, if one has already been established.
58
REPORTABLE ACTIONS
TO BE REPORTED IMMEDIATELY Written incident report will be faxed to the Washington County EMS Office
within 24 hours. 1. Interface with WCCCA is off-line. 2. 9-1-1 call(s) are not imported from WCCCA. 3. Ambulance response in Washington County by provider other than Metro West Ambulance
to a 9-1-1 call.
59
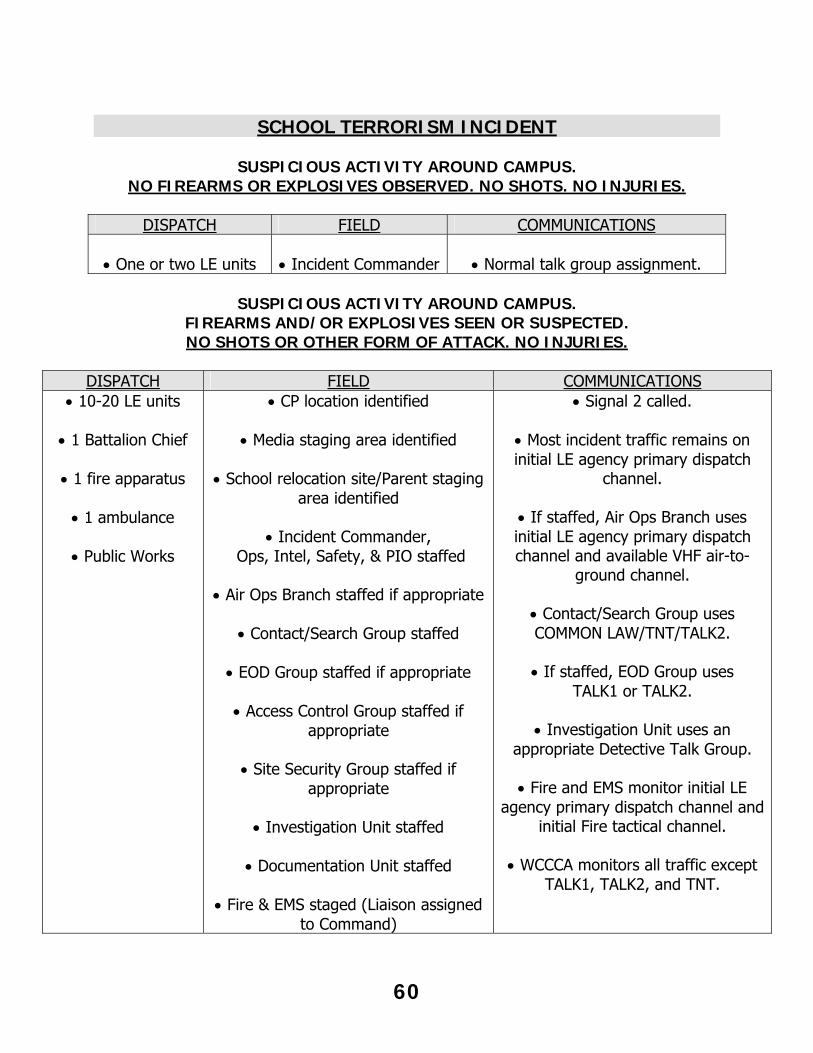
SCHOOL TERRORISM INCIDENT
SUSPICIOUS ACTIVITY AROUND CAMPUS. NO FIREARMS OR EXPLOSIVES OBSERVED. NO SHOTS. NO INJURIES.
DISPATCH FIELD COMMUNICATIONS
One or two LE units
Incident Commander
Normal talk group assignment.
SUSPICIOUS ACTIVITY AROUND CAMPUS.
FIREARMS AND/OR EXPLOSIVES SEEN OR SUSPECTED. NO SHOTS OR OTHER FORM OF ATTACK. NO INJURIES.
DISPATCH FIELD COMMUNICATIONS
10-20 LE units
1 Battalion Chief
1 fire apparatus
1 ambulance
Public Works
CP location identified
Media staging area identified
School relocation site/Parent staging area identified
Incident Commander,
Ops, Intel, Safety, & PIO staffed
Air Ops Branch staffed if appropriate
Contact/Search Group staffed
EOD Group staffed if appropriate
Access Control Group staffed if appropriate
Site Security Group staffed if
appropriate
Investigation Unit staffed
Documentation Unit staffed
Fire & EMS staged (Liaison assigned to Command)
Signal 2 called.
Most incident traffic remains on initial LE agency primary dispatch
channel.
If staffed, Air Ops Branch uses initial LE agency primary dispatch channel and available VHF air-to-
ground channel.
Contact/Search Group uses COMMON LAW/TNT/TALK2.
If staffed, EOD Group uses
TALK1 or TALK2.
Investigation Unit uses an appropriate Detective Talk Group.
Fire and EMS monitor initial LE
agency primary dispatch channel and initial Fire tactical channel.
WCCCA monitors all traffic except
TALK1, TALK2, and TNT.
60
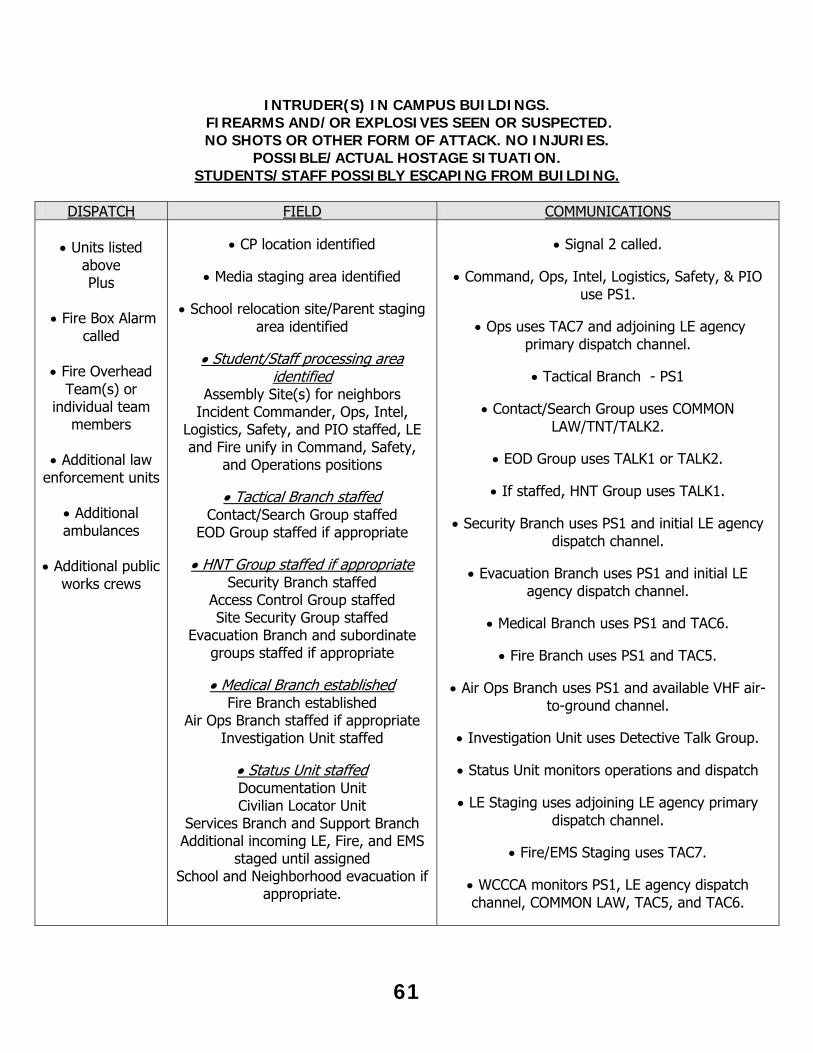
INTRUDER(S) IN CAMPUS BUILDINGS.
FIREARMS AND/OR EXPLOSIVES SEEN OR SUSPECTED. NO SHOTS OR OTHER FORM OF ATTACK. NO INJURIES.
POSSIBLE/ACTUAL HOSTAGE SITUATION. STUDENTS/STAFF POSSIBLY ESCAPING FROM BUILDING.
DISPATCH FIELD COMMUNICATIONS
Units listed
above Plus
Fire Box Alarm
called
Fire Overhead Team(s) or
individual team members
Additional law
enforcement units
Additional ambulances
Additional public
works crews
CP location identified
Media staging area identified
School relocation site/Parent staging
area identified
Student/Staff processing area identified
Assembly Site(s) for neighbors Incident Commander, Ops, Intel,
Logistics, Safety, and PIO staffed, LE and Fire unify in Command, Safety,
and Operations positions
Tactical Branch staffed Contact/Search Group staffed
EOD Group staffed if appropriate
HNT Group staffed if appropriate Security Branch staffed
Access Control Group staffed Site Security Group staffed
Evacuation Branch and subordinate groups staffed if appropriate
Medical Branch established
Fire Branch established Air Ops Branch staffed if appropriate
Investigation Unit staffed
Status Unit staffed Documentation Unit Civilian Locator Unit
Services Branch and Support Branch Additional incoming LE, Fire, and EMS
staged until assigned School and Neighborhood evacuation if
appropriate.
Signal 2 called.
Command, Ops, Intel, Logistics, Safety, & PIO
use PS1.
Ops uses TAC7 and adjoining LE agency primary dispatch channel.
Tactical Branch - PS1
Contact/Search Group uses COMMON
LAW/TNT/TALK2.
EOD Group uses TALK1 or TALK2.
If staffed, HNT Group uses TALK1.
Security Branch uses PS1 and initial LE agency dispatch channel.
Evacuation Branch uses PS1 and initial LE
agency dispatch channel.
Medical Branch uses PS1 and TAC6.
Fire Branch uses PS1 and TAC5.
Air Ops Branch uses PS1 and available VHF air-to-ground channel.
Investigation Unit uses Detective Talk Group.
Status Unit monitors operations and dispatch
LE Staging uses adjoining LE agency primary
dispatch channel.
Fire/EMS Staging uses TAC7.
WCCCA monitors PS1, LE agency dispatch channel, COMMON LAW, TAC5, and TAC6.
61
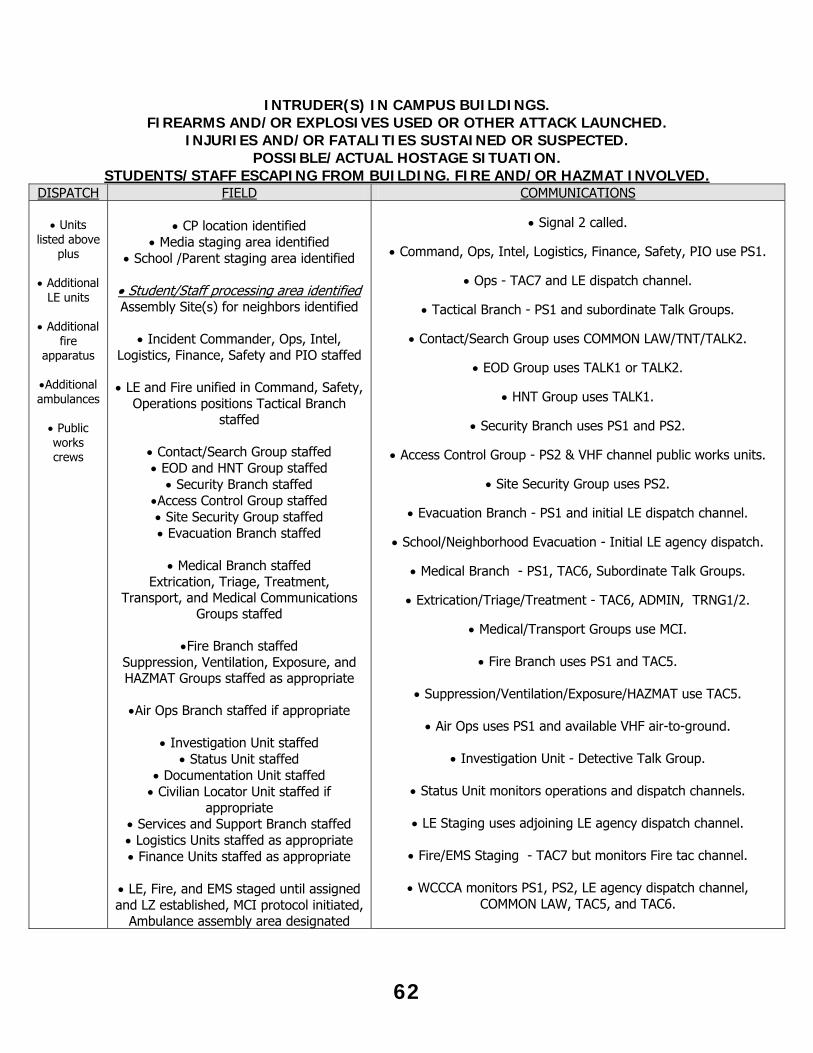
INTRUDER(S) IN CAMPUS BUILDINGS.
FIREARMS AND/OR EXPLOSIVES USED OR OTHER ATTACK LAUNCHED. INJURIES AND/OR FATALITIES SUSTAINED OR SUSPECTED.
POSSIBLE/ACTUAL HOSTAGE SITUATION. STUDENTS/STAFF ESCAPING FROM BUILDING. FIRE AND/OR HAZMAT INVOLVED.
DISPATCH FIELD COMMUNICATIONS
Units listed above
plus
Additional LE units
Additional
fire apparatus
Additional ambulances
Public works crews
CP location identified
Media staging area identified School /Parent staging area identified
Student/Staff processing area identified Assembly Site(s) for neighbors identified
Incident Commander, Ops, Intel,
Logistics, Finance, Safety and PIO staffed
LE and Fire unified in Command, Safety, Operations positions Tactical Branch
staffed
Contact/Search Group staffed EOD and HNT Group staffed
Security Branch staffed Access Control Group staffed Site Security Group staffed Evacuation Branch staffed
Medical Branch staffed
Extrication, Triage, Treatment, Transport, and Medical Communications
Groups staffed
Fire Branch staffed Suppression, Ventilation, Exposure, and HAZMAT Groups staffed as appropriate
Air Ops Branch staffed if appropriate
Investigation Unit staffed
Status Unit staffed Documentation Unit staffed Civilian Locator Unit staffed if
appropriate Services and Support Branch staffed Logistics Units staffed as appropriate Finance Units staffed as appropriate
LE, Fire, and EMS staged until assigned and LZ established, MCI protocol initiated,
Ambulance assembly area designated
Signal 2 called.
Command, Ops, Intel, Logistics, Finance, Safety, PIO use PS1.
Ops - TAC7 and LE dispatch channel.
Tactical Branch - PS1 and subordinate Talk Groups.
Contact/Search Group uses COMMON LAW/TNT/TALK2.
EOD Group uses TALK1 or TALK2.
HNT Group uses TALK1.
Security Branch uses PS1 and PS2.
Access Control Group - PS2 & VHF channel public works units.
Site Security Group uses PS2.
Evacuation Branch - PS1 and initial LE dispatch channel.
School/Neighborhood Evacuation - Initial LE agency dispatch.
Medical Branch - PS1, TAC6, Subordinate Talk Groups.
Extrication/Triage/Treatment - TAC6, ADMIN, TRNG1/2.
Medical/Transport Groups use MCI.
Fire Branch uses PS1 and TAC5.
Suppression/Ventilation/Exposure/HAZMAT use TAC5.
Air Ops uses PS1 and available VHF air-to-ground.
Investigation Unit - Detective Talk Group.
Status Unit monitors operations and dispatch channels.
LE Staging uses adjoining LE agency dispatch channel.
Fire/EMS Staging - TAC7 but monitors Fire tac channel.
WCCCA monitors PS1, PS2, LE agency dispatch channel,
COMMON LAW, TAC5, and TAC6.
62
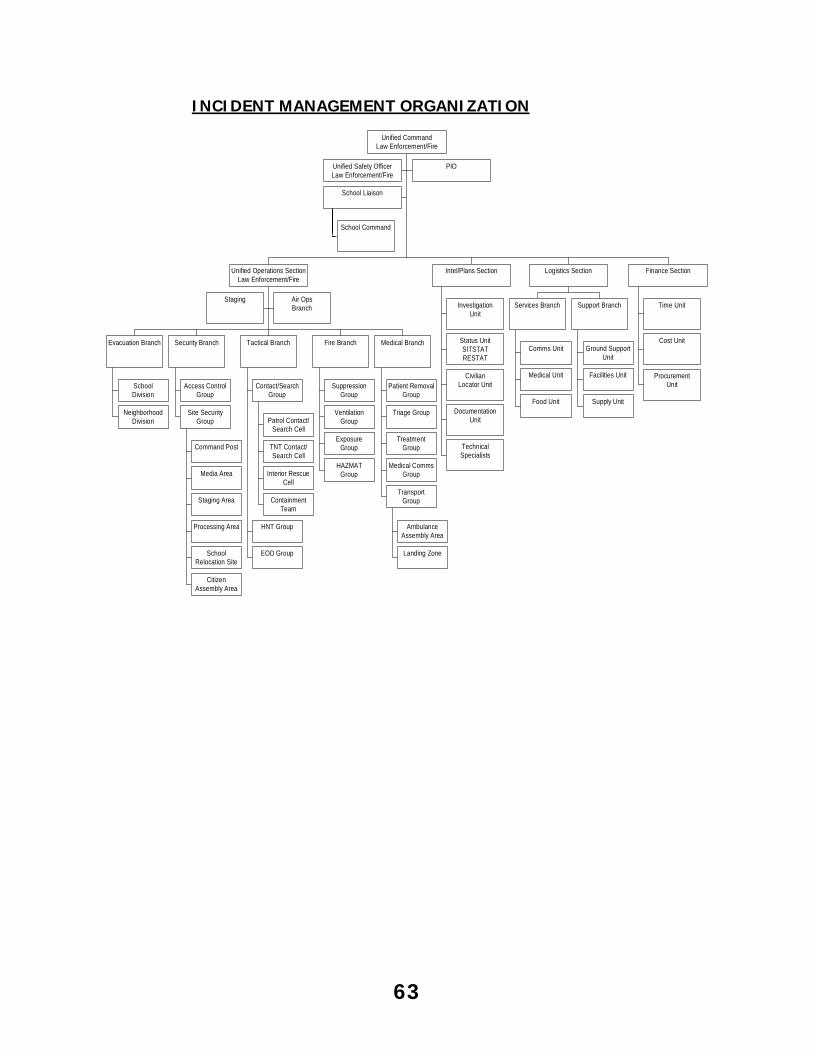
INCIDENT MANAGEMENT ORGANIZATION
Unified Safety OfficerLaw Enforcement/Fire
PIO
School Command
School Liaison
Staging Air OpsBranch
SchoolDivision
NeighborhoodDivision
Evacuation Branch
Access ControlGroup
Command Post
Media Area
Staging Area
Processing Area
SchoolRelocation Site
CitizenAssembly Area
Site SecurityGroup
Security Branch
Patrol Contact/Search Cell
TNT Contact/Search Cell
Interior RescueCell
ContainmentTeam
Contact/SearchGroup
HNT Group
EOD Group
Tactical Branch
SuppressionGroup
VentilationGroup
ExposureGroup
HAZMATGroup
Fire Branch
Patient RemovalGroup
Triage Group
TreatmentGroup
Medical CommsGroup
AmbulanceAssembly Area
Landing Zone
TransportGroup
Medical Branch
Unified Operations SectionLaw Enforcement/Fire
InvestigationUnit
Status UnitSITSTATRESTAT
CivilianLocator Unit
DocumentationUnit
TechnicalSpecialists
Intel/Plans Section
Comms Unit
Medical Unit
Food Unit
Services Branch
Ground SupportUnit
Facilities Unit
Supply Unit
Support Branch
Logistics Section
Time Unit
Cost Unit
ProcurementUnit
Finance Section
Unified CommandLaw Enforcement/Fire
63
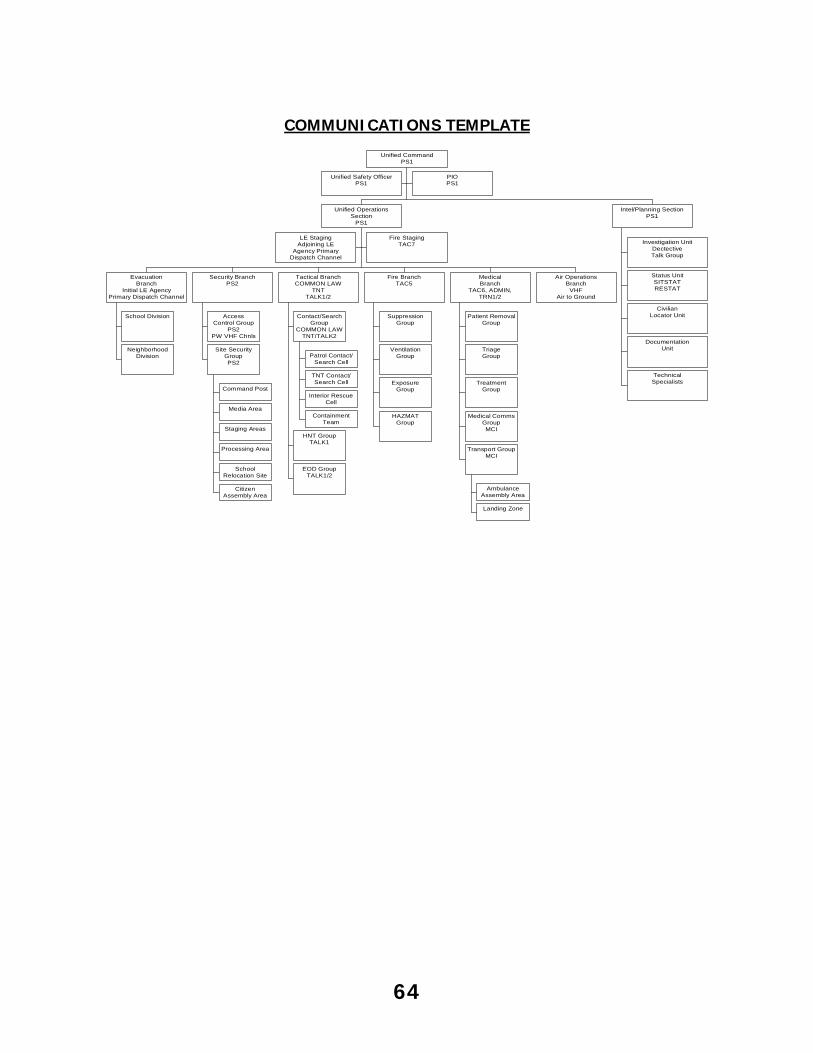
COMMUNICATIONS TEMPLATE
Unified Safety OfficerPS1
PIOPS1
LE StagingAdjoining LE
Agency PrimaryDispatch Channel
Fire StagingTAC7
School Division
NeighborhoodDivision
EvacuationBranch
Initial LE AgencyPrimary Dispatch Channel
AccessControl Group
PS2PW VHF Chnls
Command Post
Media Area
Staging Areas
Processing Area
SchoolRelocation Site
CitizenAssembly Area
Site SecurityGroupPS2
Security BranchPS2
Patrol Contact/Search Cell
TNT Contact/Search Cell
Interior RescueCell
ContainmentTeam
Contact/SearchGroup
COMMON LAWTNT/TALK2
HNT GroupTALK1
EOD GroupTALK1/2
Tactical BranchCOMMON LAW
TNTTALK1/2
SuppressionGroup
VentilationGroup
ExposureGroup
HAZMATGroup
Fire BranchTAC5
Patient RemovalGroup
TriageGroup
TreatmentGroup
Medical CommsGroupMCI
AmbulanceAssembly Area
Landing Zone
Transport GroupMCI
MedicalBranch
TAC6, ADMIN,TRN1/2
Air OperationsBranch
VHFAir to Ground
Unified OperationsSection
PS1
Investigation UnitDectectiveTalk Group
Status UnitSITSTATRESTAT
CivilianLocator Unit
DocumentationUnit
TechnicalSpecialists
Intel/Planning SectionPS1
Unified CommandPS1
64
SCOGGINS DAM FAILURE/TUALATIN RIVER FLOOD A failure of Scoggins Dam will result in flooding of the Tualatin River, its tributaries and portions of the Cities of Gaston, Forest Grove, Cornelius, Hillsboro, King City, Tigard, and Tualatin along with portions of un-incorporated Washington County. Many major roadways will become impassable, isolating portions of the County.
The Scoggins Dam Reservoir Supervisor is responsible for notifying WCCCA in case of a potential or actual failure of the dam. This notification will be made on the dispatch frequency or by telephone.
The notification will include any or all of the following: - “Dilley is at flood stage”: This notification means that the river gauge at Dilley
has reached a flood stage of 16’5”. - “Reservoir is at capacity”: This means that the reservoir is full. Further in-flow
will be released.
Emergency events occur with varying, unpredictable degrees of severity. The event could be slow and developing (extended rainfall), or a sudden event such as an earthquake or structural failure of the dam.
If an emergency event is declared at the Dam, WCCCA will make a response level notification of I, II, or III. Based on the type of incident normal progression through level I, II, and III may not occur.
Response Level I (get ready) is the least serious level and means that involved agencies should prepare for emergency response activities. Nothing significant is to be done except to stay aware of the event that is unfolding and the completion of plan review and preparation. Nothing serious is occurring at the reservoirs or dam, but the potential is there. If Response Level I is declared the following activities shall take place:
- Metro West Ambulance Management is notified. - Washington County EMS Office is notified.
Response Level II (get set) is the next level and means that conditions have deteriorated and that more serious planning and preparation activities need to be completed. Evacuation is considered at this level but not ordered. Emergency responders should move equipment out of flood prone areas. If Response Level II is declared, the following activities shall take place:
- Response Level I activities if not already completed. - Staff available units. - Respond one ambulance to Gaston for standby. Contact Gaston RFPD for
staging location. - Respond one ambulance to the Midway Fire Station for standby.
65
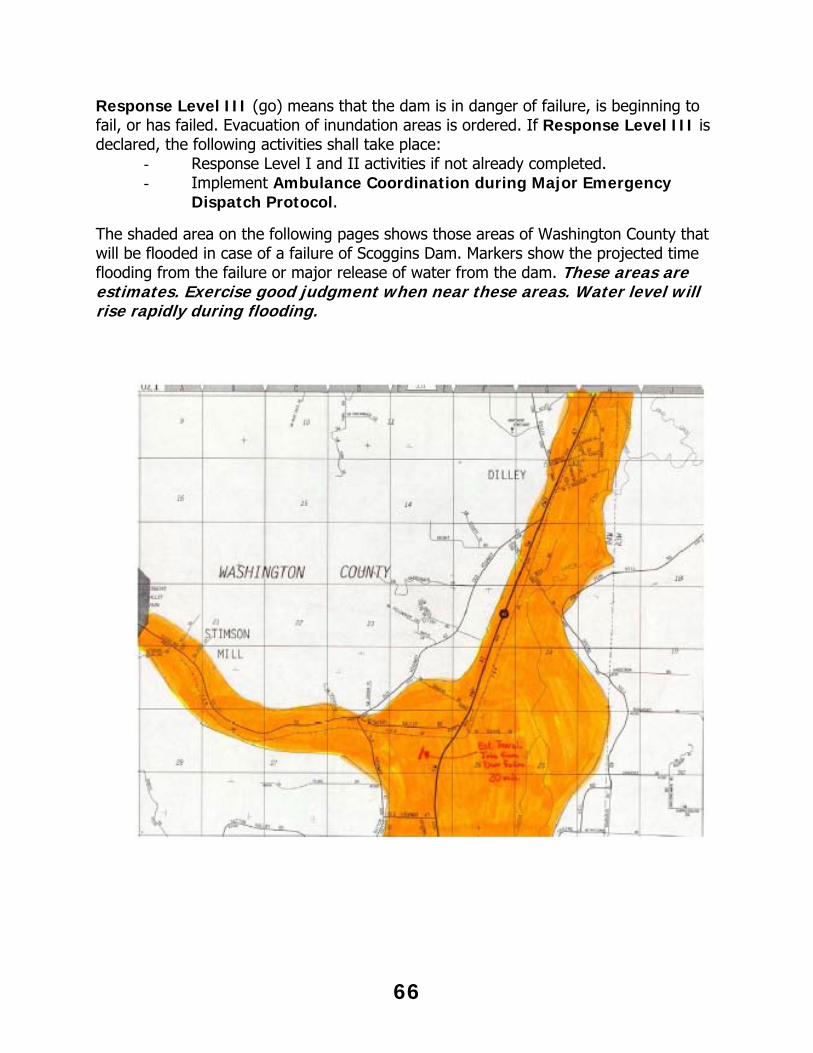
Response Level III (go) means that the dam is in danger of failure, is beginning to fail, or has failed. Evacuation of inundation areas is ordered. If Response Level III is declared, the following activities shall take place:
- Response Level I and II activities if not already completed. - Implement Ambulance Coordination during Major Emergency
Dispatch Protocol.
The shaded area on the following pages shows those areas of Washington County that will be flooded in case of a failure of Scoggins Dam. Markers show the projected time flooding from the failure or major release of water from the dam. These areas are estimates. Exercise good judgment when near these areas. Water level will rise rapidly during flooding.
66
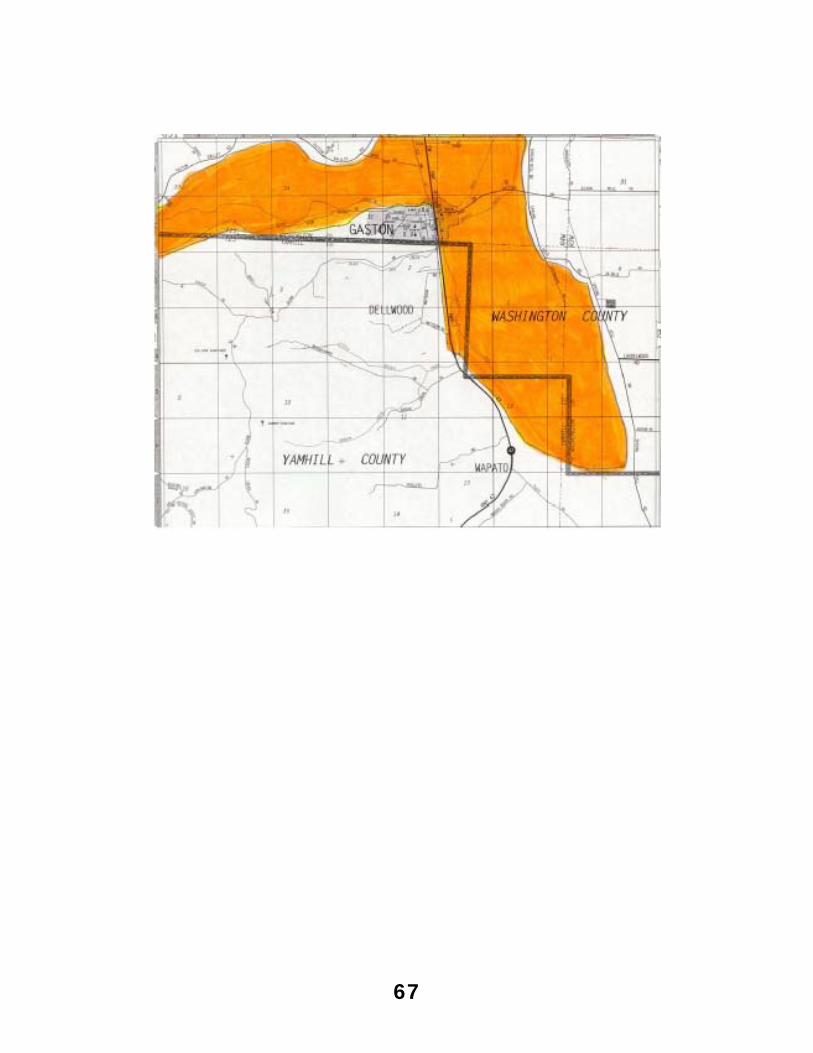
67
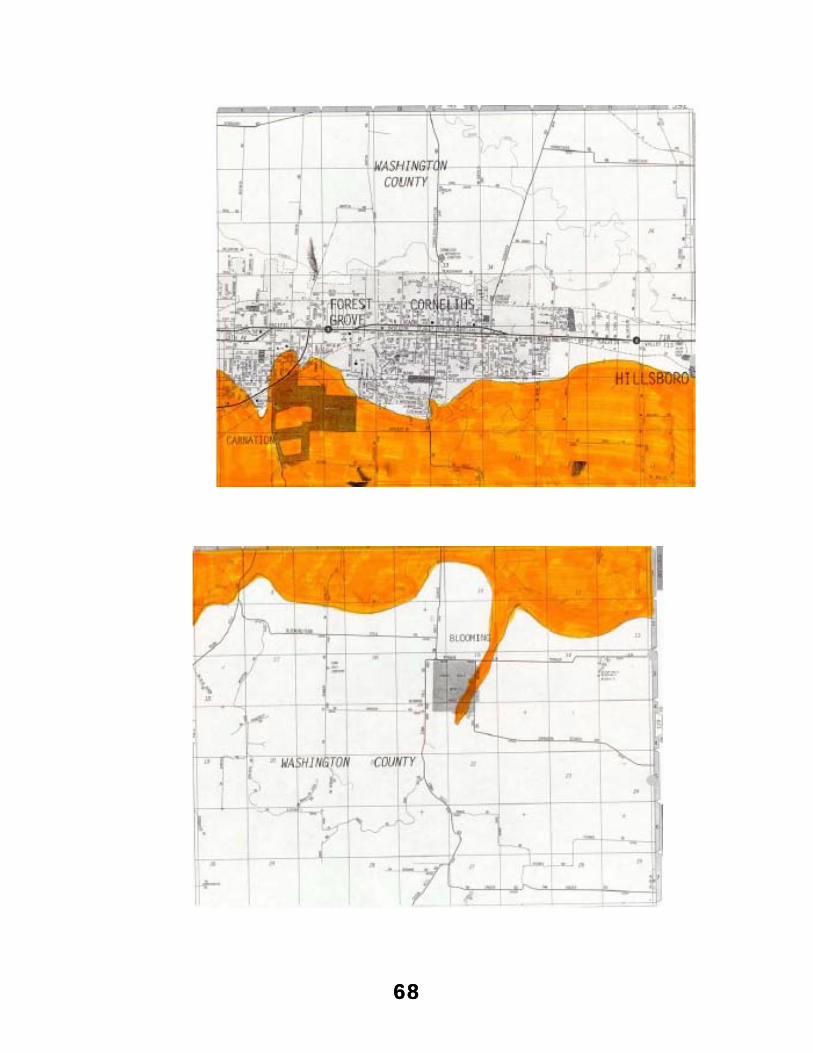
68
68
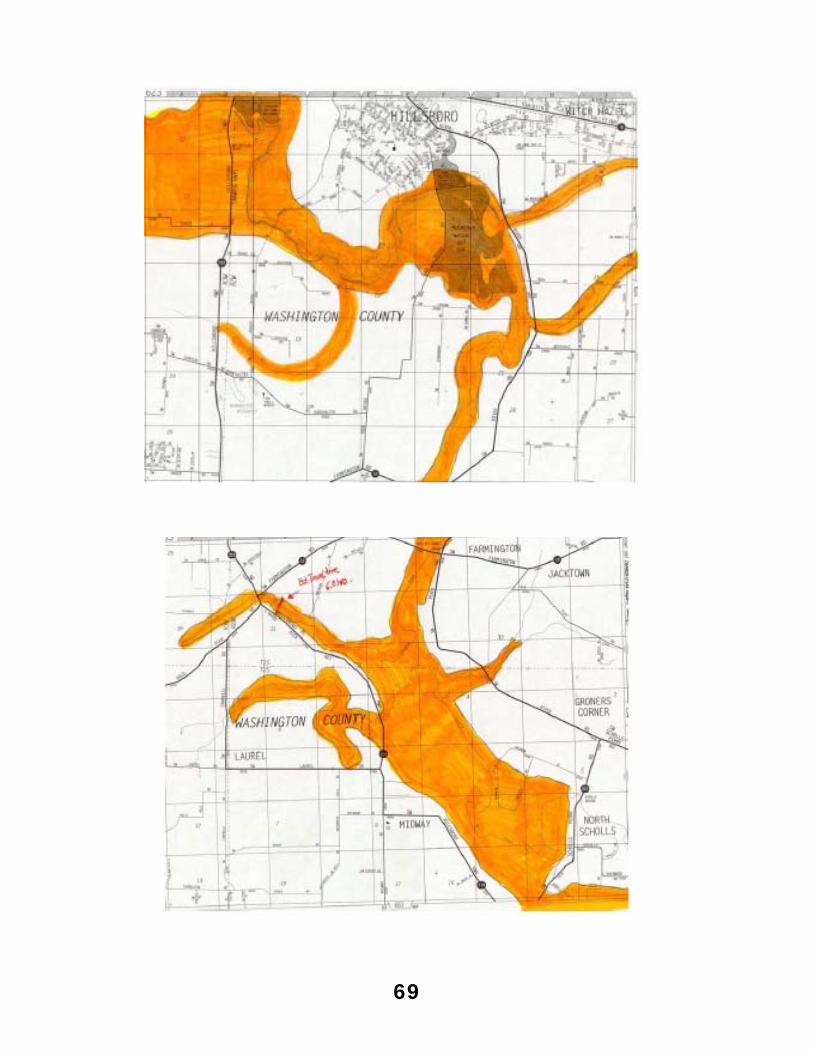
69
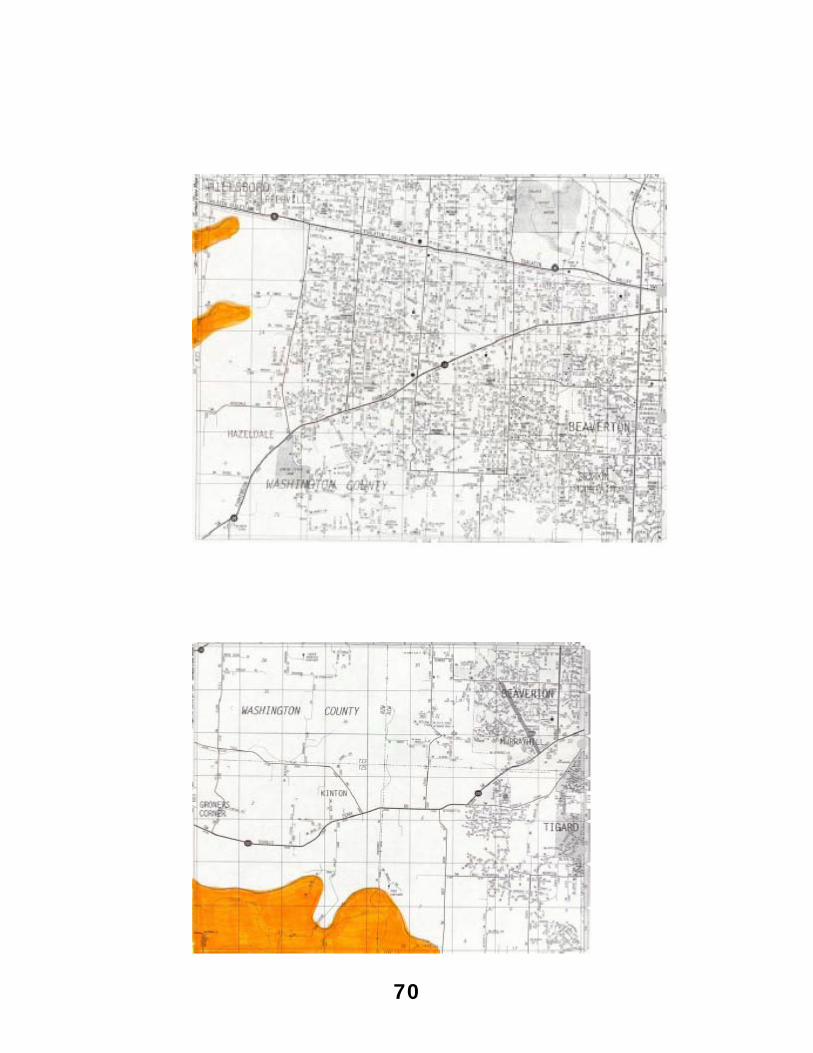
70
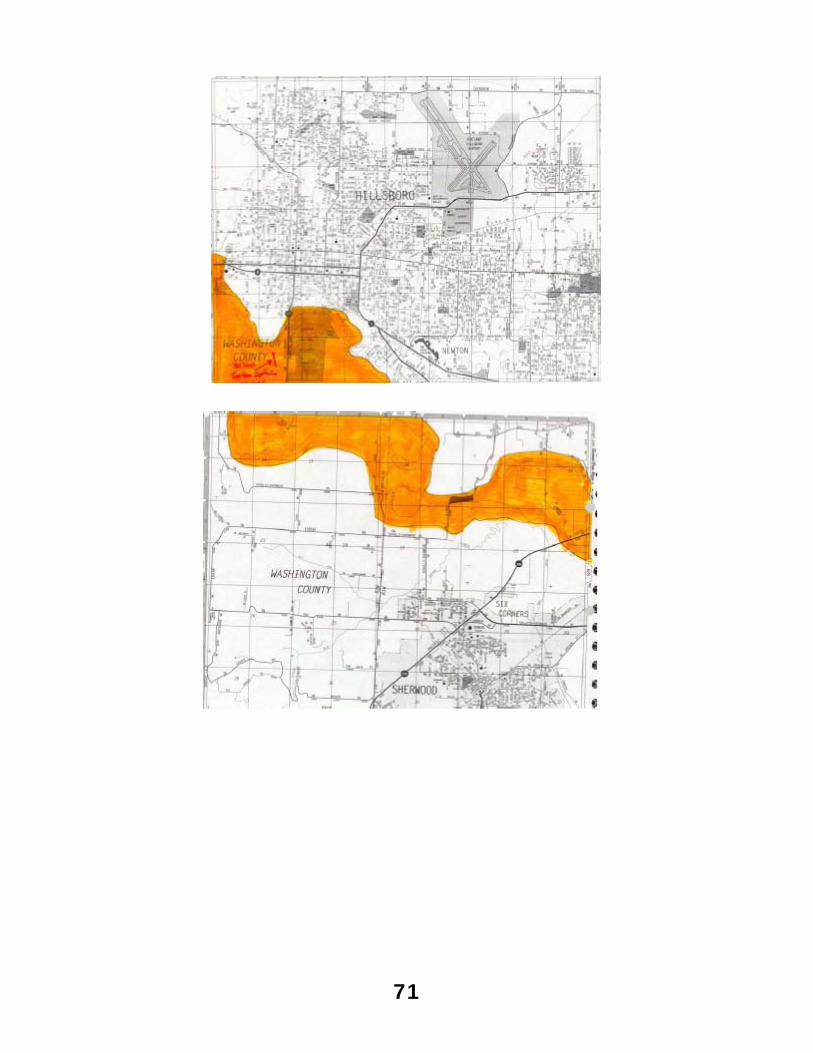
71
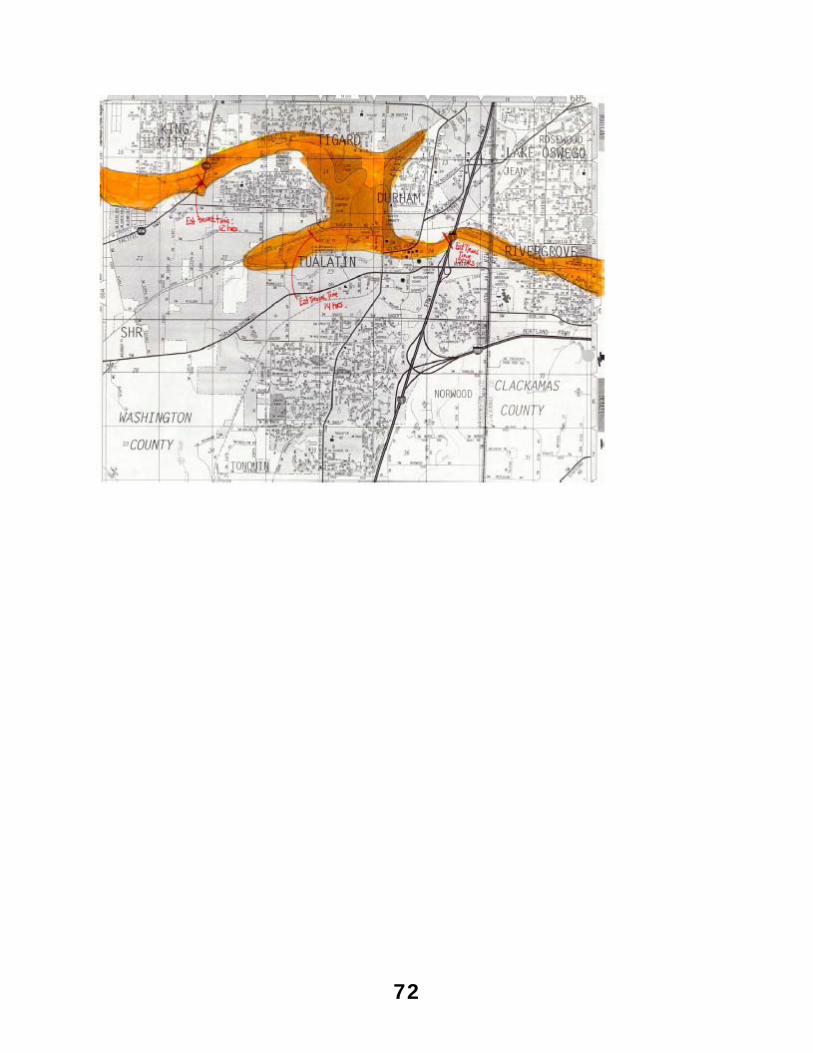
72
73
COMMUNICATIONS CENTER PROTOCOL RECEIPT FORM
I have received a copy of the Communications Center Protocols. I have reviewed these protocols and have had an opportunity to discuss any questions with the Washington County EMS Office. _____________________________________________ Signature _____________________________________________ Printed Name _____________________________________________ Date _____________________________________________ Agency
This form must be returned to the Washington County EMS Office before February 01, 2007 or within 30 days of employment as a
dispatcher with a Washington County licensed ambulance or wheelchair car provider.





























