Embed Size (px)
Citation preview

mHealth
2
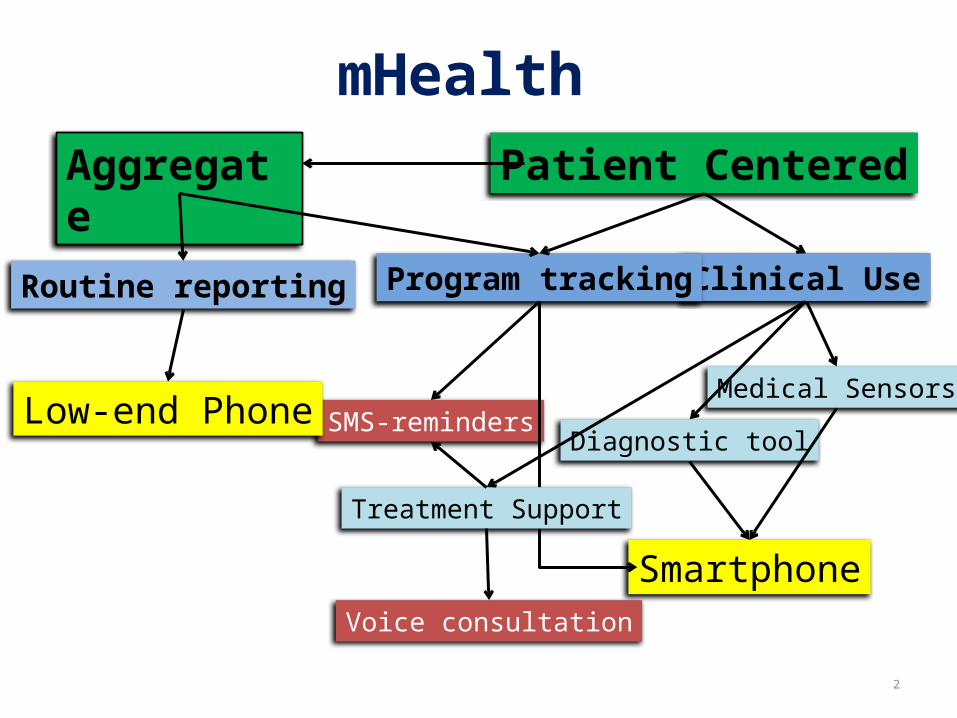
mHealthAggregate
Clinical Use
Patient Centered
Program tracking
Medical Sensors
Diagnostic tool
Smartphone
Routine reporting
SMS-reminders
Treatment Support
Voice consultation
Low-end Phone
Use case Types of mobile application & data bearer
Plaintext SMS Structured SMS SIM-apps “GPRS-apps” (Java J2ME) Mobile Browser – offline/online Voice! Interactive voice response (IVR)
Paper is still a viable option in many contexts!
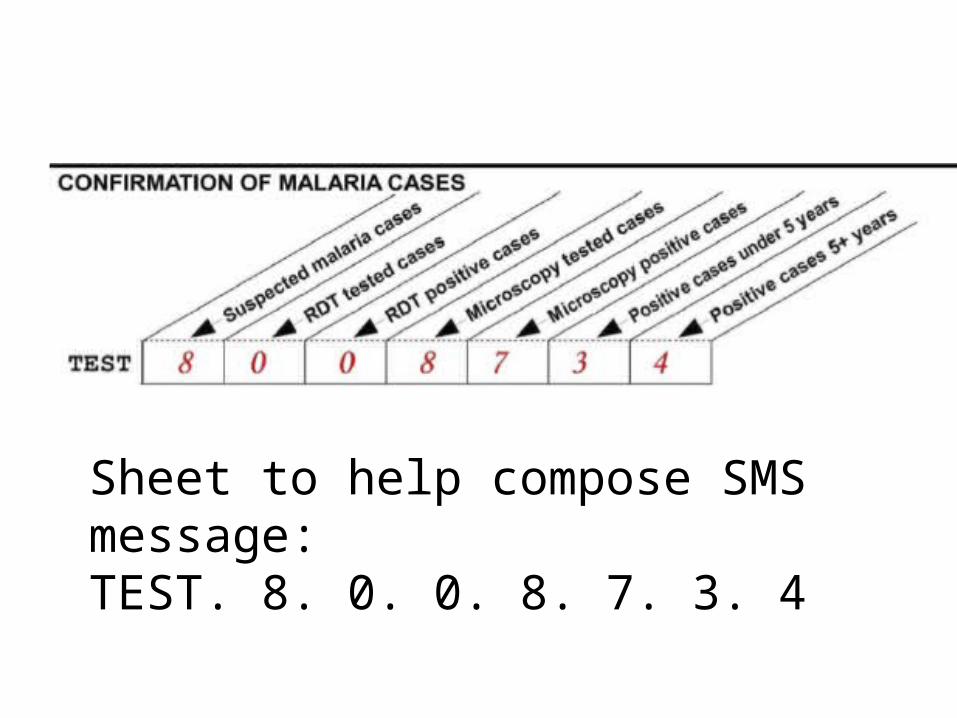
Sheet to help compose SMS message:TEST. 8. 0. 0. 8. 7. 3. 4
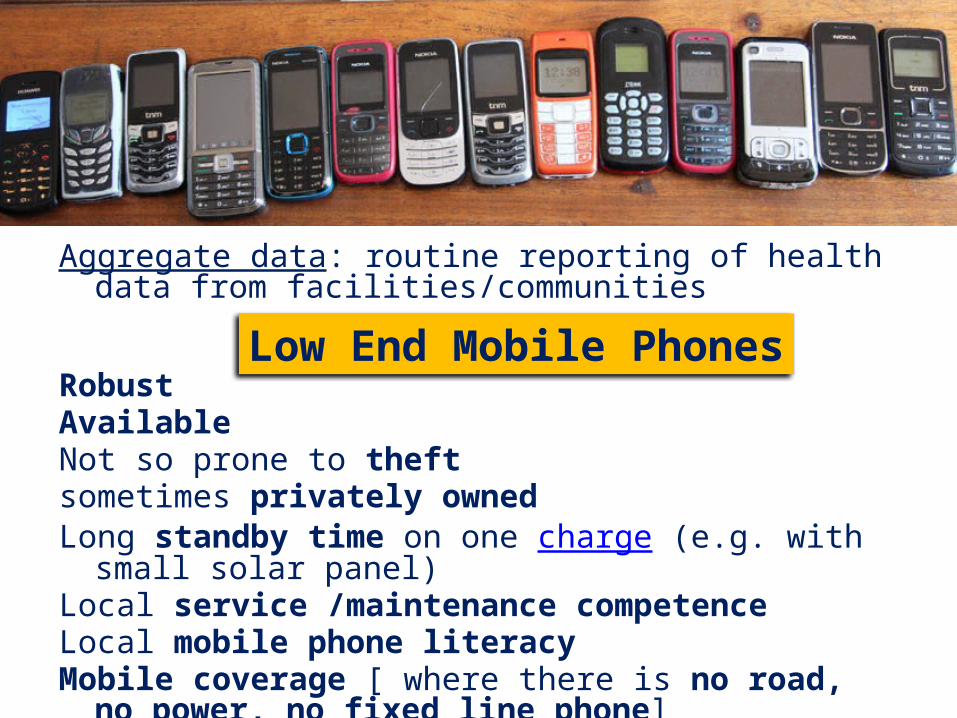
Aggregate data: routine reporting of health data from facilities/communities
RobustAvailableNot so prone to theftsometimes privately owned Long standby time on one charge (e.g. with small solar panel)Local service /maintenance competenceLocal mobile phone literacy Mobile coverage [ where there is no road, no power, no fixed
line phone]
Low End Mobile Phones
mHealth & HMIS goals
Timeliness Assist local decision making based on accurate
data on time
NB: Not all solutions have to be measurable in terms of improved health service quality.
Cost effective HMIS is also important
How can mobiles improve HMIS?Data Quality - Validation rules on phoneOn the spot data capture and transferSave time and reduce mistakes caused by manual collation and transfer
of data
mHealth application areas Routine data (HMIS) Notifiable Diseases (IDSR) Individual “Tracking” => aggregate Stock-outs Individual health monitoring Reminders Etc.
Types of mHealth dataName based/program tracking (ANC, HIV,
TB)or aggregate data (ISDR & routine HMIS)
CHALLENGES Security of identifiable patient data Complexity of work routine (not easy to capture
on a small screen – or any screen) mHealth - Additional burden or Helpful tool?
mHealth; empowering health workers or job surveillance?
Integrate with GIS/GPS – for disease surveillance or can be used for task force surveillance and control
[Example: daily reporting Punjab]Some managers would love to have a camera-drone following their
health workers 24-7!
Missing Feedback in HMISSupervision feedback only when there are errors, mistakes,
shortcomingsSupervision is often irregular and non-supportive and requires
time & resourcesMobile “Feedback” (access to processed data) Progress over time Comparisons to other organization units [vertical/horizontal] HMIS metadata – completness, timeliness % Push or Pull?
What’s in it for the end users?
Save money and time spent on travel [maybe!]More time for service provision [ideally…]Closed User Group (CUG) agreement with
mobile operator = free communication with colleagues!
Processed data ”Feedback”Phone Credit top-up/ reimbursements/bonus
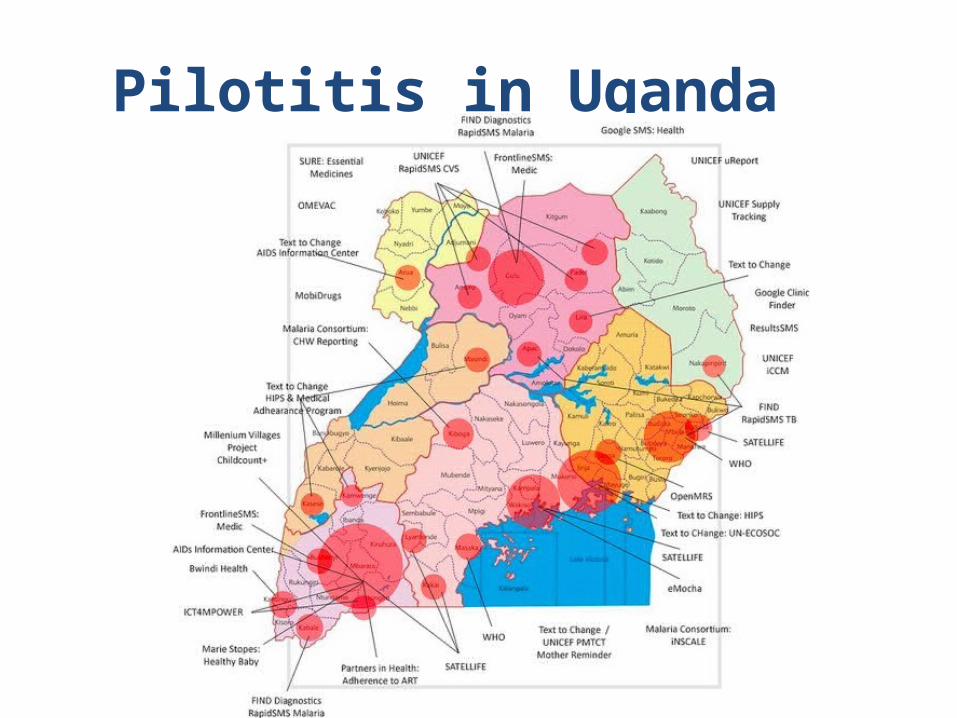
Pilotitis in Uganda

Problems with mHealth PilotsAdditional burden for health workersDonor short attention span - unsustainableWhat works as a pilot does not necessarily scalePilots may focus on technical feasibility while ignoring larger
organizational and political mechanisms (e.g. health worker unions)
Hard to evaluate and-compare across mHelath projects
Partners in mHealth“Ecosystem of actors”: Ministry of Health, NGOs,
researchers, Programme Donors &…
Mobile Operators Network coverage Closed User Group Agreement Social responsibility or New revenue streams?
BUT mHealth Initiative may get stuck with one operator!
Win-Win-Win?





























