Embed Size (px)
Citation preview

Development Impact Evaluation Initiative
Innovating in Design: Evidence for Impact in Health
Cape Town, South Africa December 10-14, 2012
Evidence for Impact in Health Scaling up innovative interventions in development/small changes, big results: design features for high impact
Michael Kremer (Harvard University)
1
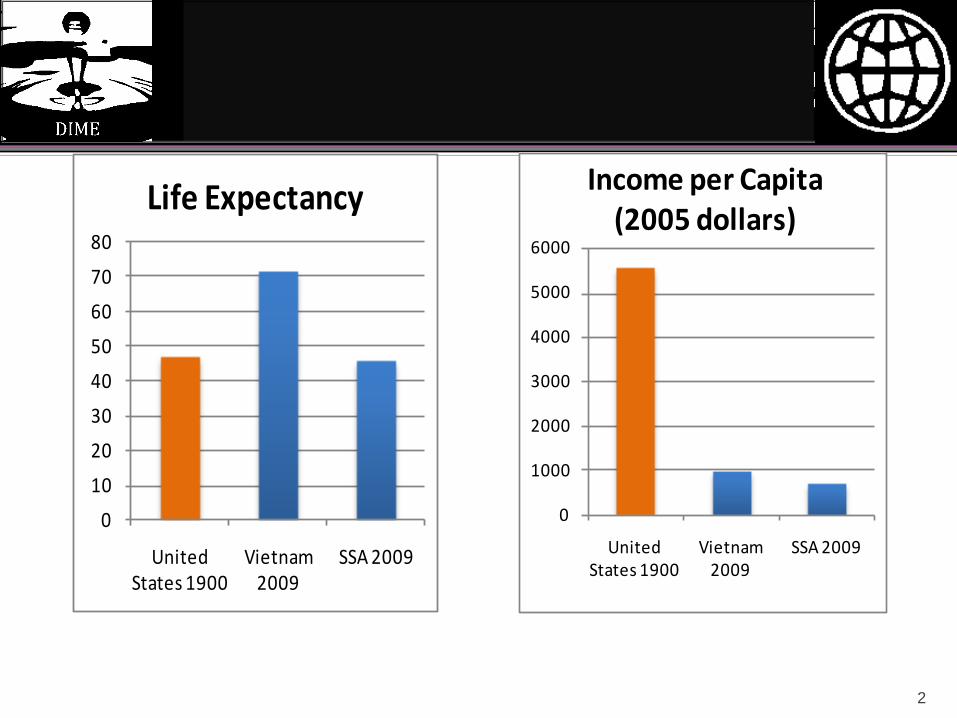
0
1000
2000
3000
4000
5000
6000
United States 1900
Vietnam 2009
SSA 2009
Income per Capita (2005 dollars)
0
10
20
30
40
50
60
70
80
United States 1900
Vietnam 2009
SSA 2009
Life Expectancy
2
Overview
1. Impact of Health Investments
2. Consumer Behavior
A. Prevention
B. Treatment
3. Health Care Provision
3
Development impact of health investment: NTD example
Helminths widespread, treatment inexpensive and safe, diagnosis expensive
WHO recommends mass school-based treatment Prospective trial of Kenyan NGO program School absence falls by ¼ Epidemiological effects Neighboring schools, younger children Long run effects on work hours, earnings 60% rate of return Increased tax revenue > program cost
Response
Strong interest from PS of Ministry of Education, World Bank Inter-ministry committee Deworm the World Initiative at WEF Generates high-level political support Funds technical assistance
Inclusion in MoE plan, rollled out to 3.5 million children in 2009
Scandal in education ministry, donor support put on hold Identification of new donor for 5 year program reaching
more than 5 million children per year Programs in Bihar, Delhi, Rajasthan…

Public Goods: Spring Protection and Road Safety
$1K capital cost, negligible marginal cost
Randomized trial suggests 25% reduction in diarrhea, but substantial recontamination
Estimate willingness to walk, effects of different pricing and propery righs systems, prioritization among springs
Stickers in matatus encouraging consumers to speak up
(Kremer et al 2007) 6 1. Consumer Behavior 2. Health care provision
Determinants of Health
Consumer Behavior Prices Financial incentives (negative prices) Information
Quality of Provision Incentives Community monitoring and accountability
1. Consumer Behavior 2. Health care provision
Example: Deworming in Kenya
8
Price response (Kremer and Miguel 2007)
o 75% take-up when free, 18% with small user fee o No difference in take-up with family size despite per family fee structure o Sicker students not more likely to pay for drugs
1. Consumer Behavior 2. Health care provision
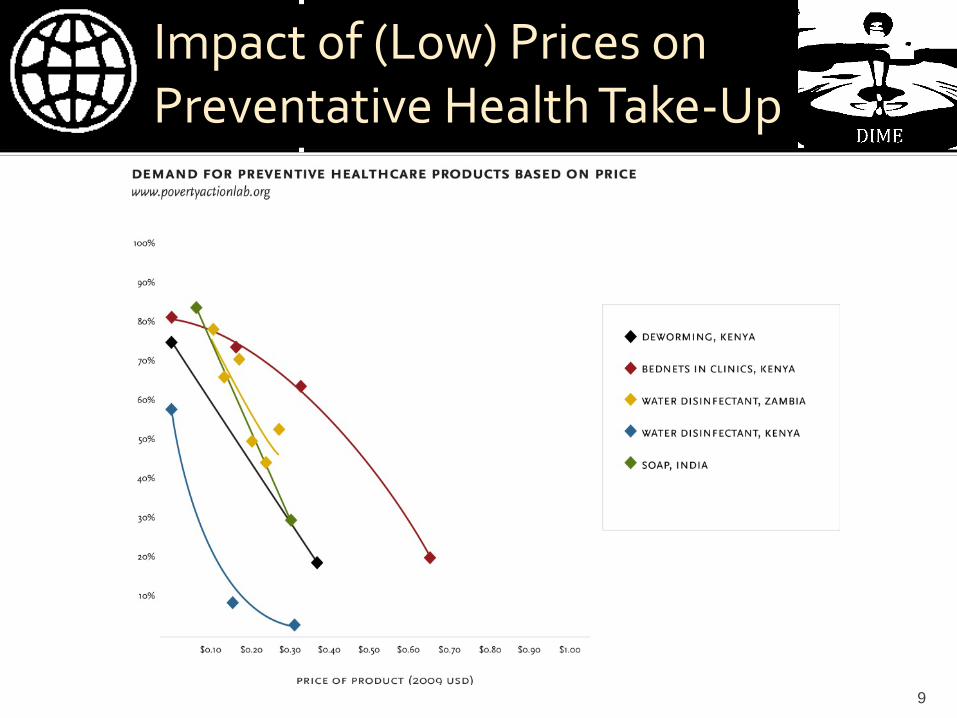
Impact of (Low) Prices on Preventative Health Take-Up
9
Does Paying Makes People More Likely to Use Health Goods?
Widely believed by practitioners
Could arise due to sunk cost fallacy
No evidence Bednets in Kenya & Uganda (Cohen &
Dupas 2010; Hoffman et al 2009)
Water purification in Zambia (Ashraf et al
2010)
10 1. Consumer Behavior 2. Health care provision
Financial Incentives (Negative Prices)
Large negative prices in conditional cash transfer
programs increase uptake of preventative health Health & education: Mexico (Gertler 2004; Schultz
2004) Health: Tanzania (Evans et al. 2012)
Small incentives also have remarkable impact HIV test results in Malawi (Thornton 2008) Vaccination in India Cash transfer in Malawi: Transfer amount does not
affect outcomes (Baird et al 2011)
11 1. Consumer Behavior 2. Health care provision
Implications
Implications for understanding consumer behavior Present-bias can explain several puzzles ▪ Prevention vs. Treatment ▪ Sensitivity to prices around zero
Implications for policy Partial cost sharing is typical compromise, but may be
worst of all worlds Zero prices, small subsidies Prioritization: cost effective prevention approaches for
communicable disease
Information
Often, little impact of health education Intensive school health education intervention had no impact on
worm prevention behaviors in Kenya (Kremer & Miguel 2007)
But in some cases, dramatic impacts Information on HIV prevalence by age in Kenya (Dupas 2011)
Rational learning model vs. limited attention model Fade out of education campaign effect Greater responsiveness to coarse information in Bangladesh (Bennear
et al 2011)
People tested negative for malaria still buy malaria meds in Kenya (Dupas et al 2012)
13 1. Consumer Behavior 2. Health care provision
Acute Treatment
Substantial expenditure on health treatment of doubtful utility (Das and Hammer, 2005; Banerjee et al., 2004)
Consumers bear substantial health risk (Gertler & Gruber 2002)
Low take-up of voluntary health insurance in Nicaragua (Thornton et al 2010)
Limited and mixed evidence on effect of price of clinic visits on take-up, health Exogenous increase in fees at clinics in Indonesia (Dow et al 2003)
Subsidized anti-malaria in Kenya (Cohen and Dupas 2011)
Mexican Seguro Popular health insurance program had no effect on healthcare utilization in short term (King et al 2009)
14 1. Consumer Behavior 2. Health care provision
Applying the Lessons: Program Design and Testing
Water infrastructure often expensive, recontamination frequent
Chlorination safe, effective, low-cost, but single-digit take-up under social marketing
Design for free distribution, convenience, habit formation, norm formation
15 1. Consumer Behavior 2. Health care provision
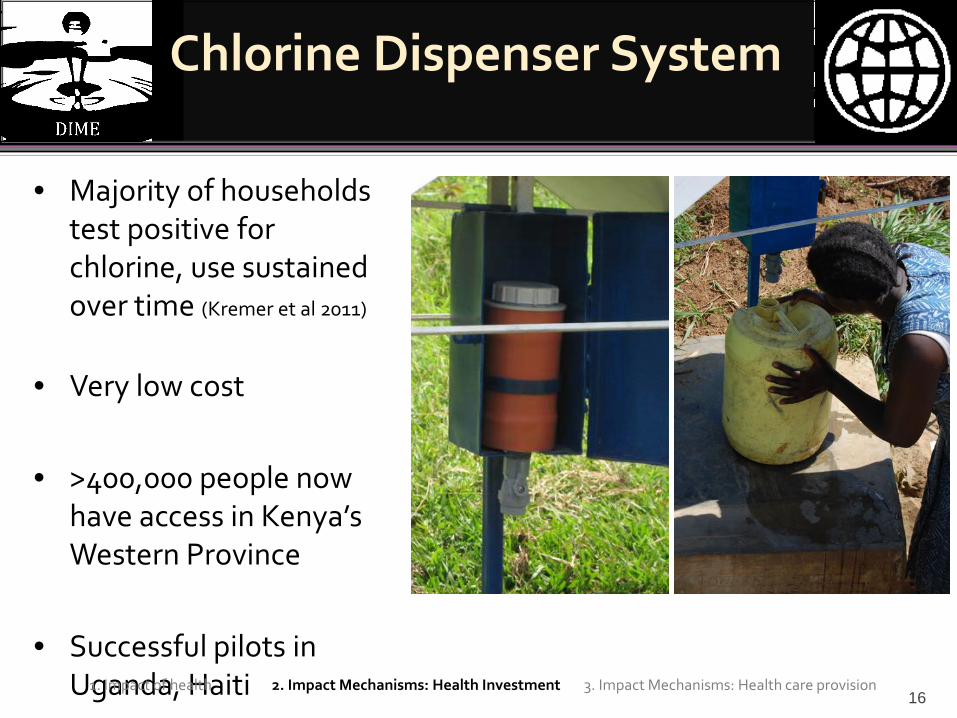
Chlorine Dispenser System
16
• Majority of households
test positive for chlorine, use sustained over time (Kremer et al 2011)
• Very low cost
• >400,000 people now have access in Kenya’s Western Province
• Successful pilots in Uganda, Haiti
1. Impact of health 2. Impact Mechanisms: Health Investment 3. Impact Mechanisms: Health care provision
Overview
1. Consumer Behavior
2. Health care provision
17
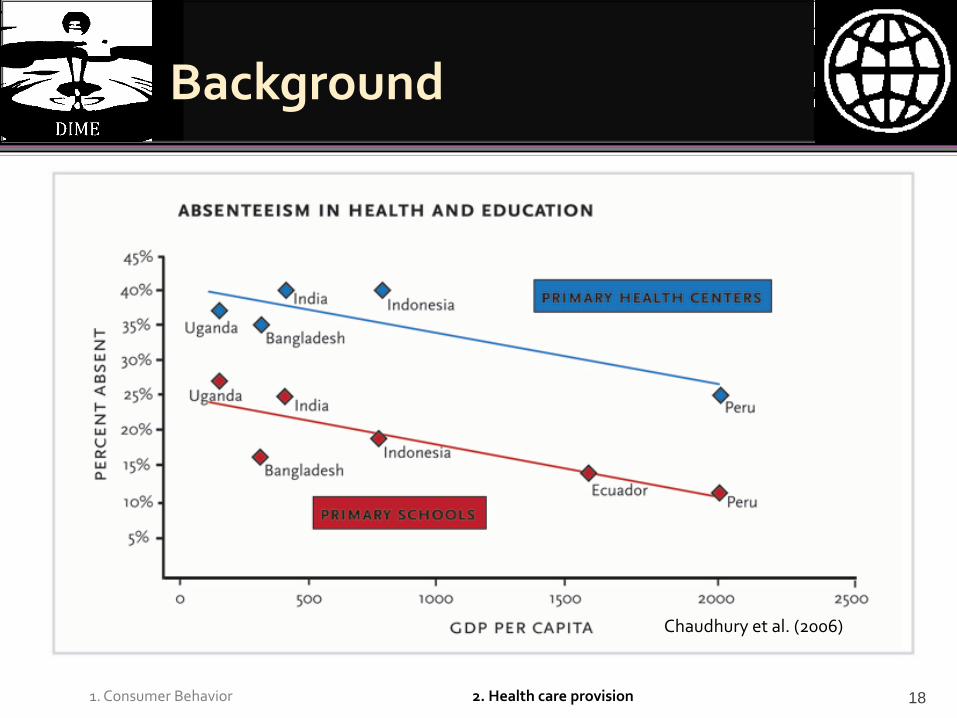
Background
18
Chaudhury et al. (2006)
1. Consumer Behavior 2. Health care provision
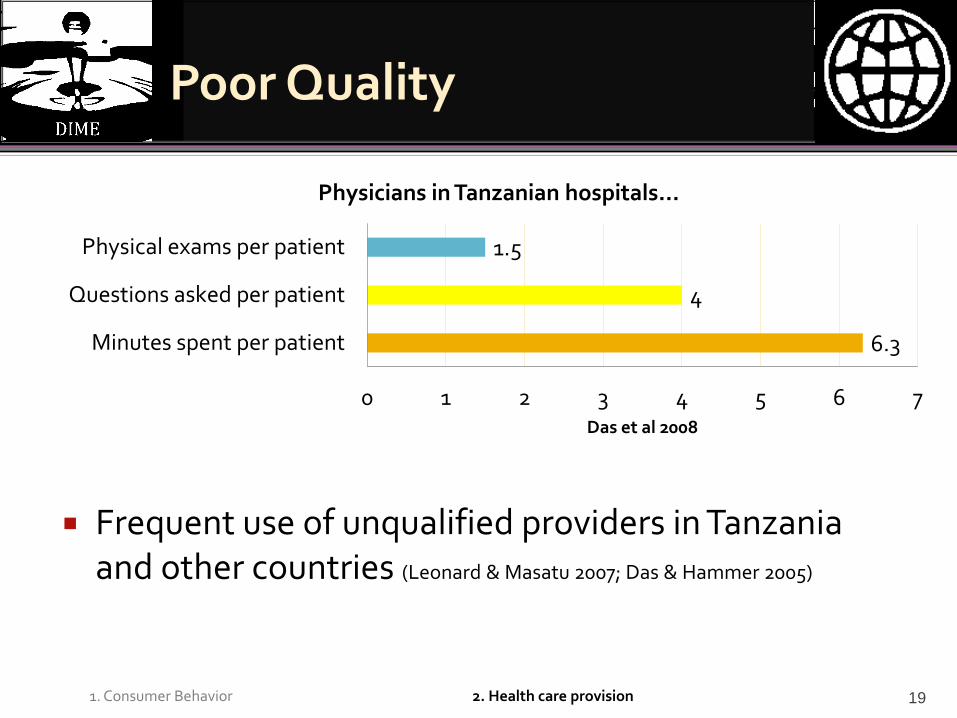
Poor Quality
Frequent use of unqualified providers in Tanzania and other countries (Leonard & Masatu 2007; Das & Hammer 2005)
19
6.3
4
1.5
0 1 2 3 4 5 6 7
Minutes spent per patient
Questions asked per patient
Physical exams per patient
Das et al 2008
Physicians in Tanzanian hospitals…
1. Consumer Behavior 2. Health care provision
Approaches to Addressing Government Failure in Service Delivery
Management reforms (e.g. supply chain management
Provider Incentives
Community mobilization for accountability
Paying for results
Contracting for health
20 1. Consumer Behavior 2. Health care provision
Provider Incentives
Pay for performance program in Rwanda: Significant increase in quality prenatal care but no impact on number of visits, immunization rates (Basinga et al 2010)
Non-financial rewards motivate public
health workers in Zambia (Ashraf et al 2012)
Monitoring program linked pay to nurse attendance in India (Banerjee et al 2008)
Initial attendance boost; disappears after 6 months (program undermined)
21 1. Consumer Behavior 2. Health care provision
Community Mobilization and Accountability
Community monitoring of health services in Uganda (Björkman & Svensson 2009) Provider absence 14% lower in treatment
facilities Vaccination rates increased 46% 46% more children received vitamin A
supplements Health improvements
Contrasting results elsewhere and weakness of pre-existing Ugandan efforts suggests implementation critical 22
Paying for Results?
Block grants to communities tied to results (Olken et al 2011)
Regular weight checks for children and iron tablets for pregnant women increased Malnutrition fell by 2.2
percentage points
23 1. Consumer Behavior 2. Health care provision
Contracting for Health in Cambodia
Management of healthcare contracted out to NGOs in some districts (Bhushan et al 2006)
Targeted health outcomes increased one standard deviation 42% increase in vitamin A and 36% increase in
prenatal care coverage Decreased absence rates among providers
• No change in non-targeted health outcomes • Increased government spending in contract districts offset by
decrease in private health spending
24 1. Consumer Behavior 2. Health care provision
Factors in Project Design
Consumer Prices and subsidies Design for convenience, habit formation
Provider Management Incentives Governance