Embed Size (px)
Citation preview

Health Care in Crisis:How Special Interests Could Double Health Costs
and How We Can Stop It
By Larry McNeely, U.S. PIRGMichael Russo, U.S. PIRG

2
Acknowledgements
The opinions expressed in this report are those of the authors and do not necessarilyreflect the views of our funders or those who provided editorial review. Any factualerrors are strictly the responsibility of the authors.
© 2009 Florida PIRG Education Fund
With public debate around important issues often dominated by special interests pursuingtheir own narrow agendas, Florida PIRG Education Fund offers an independent voice thatworks on behalf of the public interest. Florida PIRG Education Fund, a 501(c) (3)organization, works to protect consumers and promote good government. We investigateproblems, craft solutions, educate the public, and offer meaningful opportunities for civicparticipation.
Thanks to those who contributed to their ideas, edits, and criticism to this report includingJeff Bernstein, Phineas Baxandall, Steve Blackledge, and Erin Wingo of U.S. PIRG,Deirdre Cummings of MASSPIRG, Laura Etherton of OSPIRG, and especially ourexternal readers, Terry Gardiner of Small Business Majority and Dr. Robert Crittenden ofthe Herndon Alliance. Special thanks are due Elizabeth Ridlington of the Frontier Group.Elizabeth is an author of the California Public Interest Group’s May 2008 reportDiagnosing the High Cost of Health Care and an insightful editor of this report.
The authors owe a special thanks to the New America Foundation’s Sarah Axeen andElizabeth Carpenter. Their report, The Cost of Doing Nothing, provided the projectionsof health costs upon which this report relies.
For additional copies of this report, please visit our website at: www.Florida PIRG.org
About the Authors:
Larry McNeely, as Florida PIRG’s Federal Health Advocate, leads federal-level healthcare advocacy, policy analysis, and communication activities for Florida PIRG and itsstate affiliates.
Mike Russo is the health care advocate for California Public Interest Research Group(CALPIRG). He is the author of Diagnosing the High Cost of Care, a California-specificreport on health care costs and provides health policy expertise for Florida PIRG and itsstate affiliates.

3
TABLE OF CONTENTS
Acknowledgments ..............................................................2
Executive Summary............................................................4
Introduction ........................................................................7
The Cost of Inaction ..........................................................7
Americans’ Health Spending Fails to Deliver Quality......10
Unnecessary Care that Doesn't Improve Outcomes ..........11
Excessive Administrative Expenses..................................13
Unchecked Pharmaceutical Marketing Drives Up Costs .15
Conclusions ......................................................................18

4
Executive Summary
Our health care system is in crisis.Without swift action, that crisis couldthreaten every Florida family’s healthand finances.
Unless the new Congress andAdministration act to reduce health carecosts, the yearly cost of the averageemployer-paid family health policy inFlorida is projected to more than doublefrom $11,046 in 2006 to $22,376 by2016 even after adjusting for inflation. Ifrecent trends continue, wages andhousehold incomes will simply not keepup with these high costs. Nor will thebusiness sector be immune to this crisis.Unchecked, this cost epidemic couldalso severely impact the smallbusinesses that drive job creation in theFlorida’s economy.
Unfortunately, too much of theseastronomic costs are going to enrichspecial interests, not buy the best healthcare. The Congressional Budget Officeestimates that nationally as much as onethird of health care spending is wastedand does not improve outcomes. Thatmeans that, in 2007, one out of everythree dollars that Americans spent onhealth care, or $730 billion, went to theinsurance bureaucracies, drugcompanies, medical devicemanufacturers, and providers withoutimproving a single person’s health. InFlorida, one third of health spendingamounts to $31.72 billion.
This report examines three importantsources of this unproductive spending.We conclude with a package of urgentlyneeded reforms which target thosecauses, improve quality of care, and reinin this unnecessary spending. As part of
comprehensive health reform, thesepolicies will enable America to emergefrom this crisis with a health system thatconsumers and businesses can afford andfamilies can depend on.________________________________Unnecessary Medical CareUndermines Patient Health andIncreases Costs
Research has shown that patients wholive in regions with above-averagehealth care spending are not anyhealthier than people in lower-costregions. In parts of the country wheremore specialists and hospital beds areavailable, doctors send patients tospecialists or to the hospital morefrequently, yet the patient outcomes areno better.
Medicare and private insurancepayment policies compensatedoctors on the basis of how manytests and procedures are ordered,not on the basis of whethereffective treatment is delivered.
Payment for care does notadequately support effectivestrategies that improve patienthealth and reduce the amount ofunnecessary care prescribed suchas primary care, coordinatedcare, patient involvement in caredecisions, and the use ofevidence-based care.
High-performing health systemsthat seek to reduce unnecessarycare, like the Mayo Clinic andUtah’s Intermountain HealthSystem, can reduce costs perpatient by as much as 43%, whileproviding quality care. IfAmerica’s hospitals achievedIntermountain’s level of quality

5
and efficiency, we would spend$299 billion less a year forhospital care. If Florida hospitalsimproved their efficiency by43%, the state would save$13.54 billion.
_________________________________Excessive Administrative ExpensesInflate Insurance and Medical Prices
Many administrative costs withinAmerica’s health care system are theresult of efforts to shift costs from onepayer to another—from the insurancecompany to a hospital, or from aphysician to a patient. This paperworkincreases total costs without improvingoutcomes for patients.
Unnecessarily duplicative andcomplex billing and insurancecertification requirements addbillions in additionaladministrative costs.
The credentialing process bywhich physicians are certified asproviders is unnecessarilyburdensome and wasteful
Insurers and providers spend tensof billions a year nationally oninsurance-related paperwork thatdoes not contribute to the qualityof care.
_________________________________Unchecked Pharmaceutical MarketingDrives Up Costs
Americans spend billions of dollarsannually on prescription drugs that areno better than cheaper alternatives orthat may have dangerous orunrecognized side-effects. Worse, drugcompanies’ marketing campaigns insupport their most expensive drugs cost$11.5 billion in 2005.
Drug advertising generallyencourages the use of newer,
more expensive medications,even if they are no more effectivethan existing ones
Pharmaceutical companiesincreased prescription drugadvertising by 250 percent from1997 to 2007. In response,physicians prescribe andconsumers purchase billions ofdollars of unnecessary and evenrisky medicine each year.
Direct marketing to physicians,which has been shown to rely onmisleading information, booststhe total number of prescriptionsand increases the number ofprescriptions for newer and moreexpensive drugs that are no betterthan old ones.
_________________________________Solutions
Fortunately, the high cost of care can bereduced and wasted spending ispreventable. America can fix thisproblem now. In light of the 2008election, health care reform will be onCongress’ agenda in 2009. If thesereforms are to be economicallysustainable, they must tackleunproductive spending that doesn’timprove health. This report recommendsthe adoption of the following policyinitiatives:
Reduce Ineffective Medical Care WhileImproving Quality
Fund comparativeeffectiveness researchthat studies whichmedical procedures,regimens and drugs workand which do not.
Broadly implement andincentivize coordinatedcare systems such as

6
medical homes.Compensate primary careproviders adequately.
Expand informationprovided to patients andencourage them to sharein decision making abouttheir care
Reform public andprivate payment systemsto provide the rightincentives for high-quality care and reduceunnecessary but costlytests and procedures.
Reduce Expensive AdministrativeBureaucracy
Standardize systems forenrollment, credentialing,billing and insurancepayment.
Limit insurers’administrativeexpenditures to a certainpercentage of premiumdollars.
Reduce Prescription Drug Costs
Strengthen FDAmonitoring of falsestatements in direct-to-consumer advertising andmarketing materials
Undertake a publiclyfunded effort to publicizethe benefits and prices ofdrugs to counter theunreliable informationprovided bypharmaceuticalcompanies.
Limit industry’s gifts tophysicians and requiredrug companies todisclose more informationabout their marketingpractices
Some of these reforms could happenfairly quickly; others will take years. Butit is critical that we start now byaddressing overspending that does notdeliver results. Residents of Floridasimply can not afford any more years ofspiraling health care costs.

7
Introduction
Our health care system is in crisis, andwithout dramatic action soon, itthreatens the health and economic futureof all Floridians.
The crisis can be recognized in theshrinking pool of employers offeringcoverage, in the growing number ofuninsured, in the strain on state budgetscaused by health care costs. But mostAmericans recognize it in their monthly
budgets and their mounting health carebills.
What American families don’t know ishow much worse the cost of health carecould get without health reform. Andthey do not fully realize that the healthcare system they pay for is designedprimarily to generate profits for insurersand drug companies, not to provide themquality care.
The Cost of Inaction
The total premium cost for employer-sponsored family health insurance hasballooned by over 100% in less than tenyears.i While the resulting pain has beenfelt acutely by consumers, business hassuffered too. In the face of high-costpremiums, employers, especially smallbusinesses, face tough choices: shouldergreater costs and potentially harm theircompetitiveness, pass large increases onto employees who aren’t equipped to paythem, or reduce coverage. In manycases, employers are covering less ofemployees’ premiums and requiringincreased deductibles.ii The percentageof employers who offer any coveragehas declined from 66% in 1999 to 63%in 2008.iii
As a result of these dynamics, more andmore Americans are on their own whenstruggling with rising health care costs.It’s no wonder that polls show that thecost of health care is one of Americanfamilies’ biggest worries.iv
High costs also hurt small businessesand the economy that depends on them.After all, two thirds of net new jobs are
created by small businesses each year.v
But employee health care costs for smallbusinesses, which lack the buying powerof larger firms, are 18% higher than forbigger companies.vi The additionaldollars spent on health care are dollarsnot spent on growing their businesses orhiring new staff.
As these pressures on families and smallbusinesses have increased, a consensushas begun to emerge that broad healthreform is necessary, even while thedetails of reform are subject to debate.Some political leaders have stated thatthe new administration and Congressoffer the best opportunity for majorreform in decades.vii Doctors groups andbusiness lobbies have shown anunprecedented willingness to work onthe issue.viii
Perhaps most importantly, the costs ofinaction to the public would be simplyoverwhelming. If Floridians do not winreforms that squeeze out our system’scostly inefficiencies, the full cost ofpremiums will climb to $22,376 forfamily and $7,536 for individual

8
employer-sponsored insurance by 2016.With these projected increases, the costof a family health insurance policy willbe equal to 42.7% of median householdincome.ix
The outlook for consumers gets evenworse when other forms of cost-sharingare examined. The average yearly
deductible is projected to rise from see$1,567 to $4,814 in constant dollars. Co-pays for doctor visits are projected toincrease from $19 to $27.
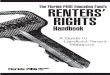
Figure 1 below details the projectedgrowth of premiums, deductibles and co-pays, if no changes are made.
Figure 1: Projected Health Care Costs for 2008 to 2016
The Cost of Inaction:Florida 2006 2016 % IncreaseAverage Yearly Deductible
$1,567 $4,814 207%
Avg. Total Cost of Family Employer-provided Insurance $11,046 $22,376 103%
Avg. Total Cost of IndividualEmployer-provided Insurance $3,936 $7,536 91%
Avg. Employee Contribution toPremium for Family Employer-provided Insurance
$3,600 $8,592 139%
Average Co-pay for Doctor Visits
$19 $27 42%
All costs are in constant 2006 dollars.
It should also be noted that theseprojections do not capture the full impacton health costs. Increased costs may behard to bear for consumers as is, but theycould lead to even greater system costs ifhigher deductibles and co-paysdiscourage patients from seeking neededcare. For example, a patient with a highdeductible might forego care until a
health condition becomes acute. Thenthe patient may be forced to seekexpensive hospital care, driving uppremiums for everyone.
The rising costs that drive premiumgrowth also mean higher prices forhealth care services purchased outright.Thus, a family’s $3,000 deductible in

9
2016 won’t buy the same amount of carethat $3,000 buys today.
Further, projected employeecontributions to insurance will likely be
even greater as employers will have anincentive to shift more of the premiumcost to employees as costs go up.
Myths of High Health Care Costs
High health care costs have been attributed to many different factors, often mistakenly.Some of the most common are addressed below.
Aging population. The argument: As the U.S. population ages, Americans require morehealth care, on average, to maintain their health. In reality: While older patients doindeed require more care, data from the federal government on why costs for Medicaidand Medicare (which serves older Americans) are rising shows that the aging populationis only a small factor in the cost of health care.x
Malpractice insurance. The argument: The cost of malpractice insurance has been risingrapidly, driving up health care costs, as doctors charge more to cover the cost ofinsurance and practice “defensive medicine” to avoid lawsuits. In reality: Malpracticerates have been on the rise, but malpractice suits may not be the cause of substantiallygreater health spending. One study of malpractice awards suggests that claims have beensteady for years and are not a major cause of increases in malpractice insurancepremiums.xi Thus, changes in malpractice insurance costs play a relatively small role inoverall health care costs. The Congressional Budget Office has concluded thatmalpractice reform would not have a measurable impact on national health spending.xii
Consumers pay for too little of their own care. The argument: Consumers pay for sucha small amount of their health care that they demand too much of it, thereby increasingcosts for insurers. In reality: Research is not clear on the impact of requiring consumersto pay for a larger share of their health care. Economic modeling of health care plans withhigh deductibles suggests they may reduce overall health care spending by 4 to 15percent.xiii However, such plans achieve savings in part because patients avoid bothnecessary and unnecessary care in equal measure. Thus, the long-term impacts on healthcare costs are unknown. Also, the finding that cost-sharing can save costs withoutharming patient health is based on a study conducted in the 1970s in which participantswho faced large medical bills likely dropped out of the study before incurring thosecosts.xiv
New drugs and better technology. The argument: Health care costs are rising becausewe are spending more money on research and development of new technologies anddrugs. These higher costs are acceptable because they make us healthier. In reality:Improvements in technology definitely can improve health, but spending on new drugsand technologies is imperfectly correlated to better health. For example, the breast cancerdrug Herceptin offers a powerful treatment for women whose tumors include a particulargenetic mutation. For women without that gene, which physicians can reliably test for,

10
the drug offers nothing. Nonetheless, approximately 12 to 20 percent of Herceptinprescriptions are for women who clearly will not benefit from it.xv
Americans’ Health Spending Fails to Deliver QualityCare
In 2007, health care spending amountedto16.2% of the United States grossdomestic product, or $2.2.trillion.xvi Tounderstand why Americans pay so muchfor health care now and face increasedcosts in the future, we must first confronta basic fact about America’s health caresystem: increased health care spendingdoes not deliver the quality of healthcare that it should.
The United States trails in manyindicators of health and well-being.America ranks 44th in the world inaverage life expectancy and 41st in theworld in infant mortality.xvii The U.S.fares poorly on measures such as babies’birth-weight and is only average in thepercentage of children who receiveimmunizations.xviii Age-adjustedmortality from several chronic diseasesis worse in the U.S. than in Canada,France, Germany, Greece, Japan andBritain because care of those withchronic diseases falls short. Forexample, nationwide, less than half ofdiabetics receive three basic tests fordiabetes that provide an assessment ofhow the disease is being controlled andoffer early warning of possiblecomplications.xix Finally, a recent studyexamined the rate of amenable mortality,or deaths that could have been preventedby quality health care, and found that theUS lagged far behind otherindustrialized nations. If the American
amenable mortality rate was improved tothe average of the top 3 nations, 101,000lives could be saved every year.xx
Why does America’s huge investment inhealth care not yield better results?Researchers at the Congressional budgetoffice estimate that as much as one-thirdof health care spending in the U.S. doesnot improve patient health.xxi In 2007,this estimate means that as much as $733billion of our $2.2 trillion healthspending was wasted. Florida wouldhave wasted up to $31.74 billion out of$95.22 billion total spending. No matterwho pays for this care, it does not helppatients live better or longer, and therebydrives up health care costs withoutproviding any corresponding benefit
Americans are paying for treatment thatdoes not result in better outcomes forpatients. No matter who pays for thiscare, it does not help patients live betteror longer, and thereby drives up healthcare costs without providing anycorresponding benefit. The next threesections of this report examine threemajor categories of unproductivespending: overuse of high-cost,uncoordinated specialty and acute care;excessive administrative costs; andprescription drug marketing thatencourages the use of more drugs, moreexpensive drugs, and drugs with a lessestablished record of safety.

11
Unnecessary Medical Care Undermines Patient Healthand Increases Costs
Americans are subjected to a widevariety of unnecessary medicaltreatments – treatments that cost thehealth care system billions of dollars anddon’t make Americans any healthier. Butwe often fail to get the basics right. Ourhealth care system frequently fails toprovide effective, low-cost treatmentsthat work – triggering higher costs downthe line. Too often, Americans’ healthcare treatment is determined,deliberately or inadvertently, by theavailability of medical resources in acommunity or by the profit motives ofdoctors, hospitals, drug companies,insurers, and other entities in the healthcare system – and not by what is mostlikely to make a patient well._________________________________Variation in Health SpendingReveals Patterns of Overuse,Underuse
When discrepancies in spending andhealth outcomes between differentregions of the country are examined,researchers have found that expensiveforms of care, specifically hospital careand specialty care, are overused, i.e.used when not medically necessary.They also found that the types of carethat are effective and cost-efficient areunderused.xxii
The scale of this problem is quite large.Analyzing Medicare spending, theDartmouth Institute of Medicine hasfound that some regions actually spend250% than others to provide Medicareservices.xxiii The explanation of thisregional variation can be found in whatthat spending goes toward. Patients in
high-spending regions are more likely toreceive less of the care that has beenproven to be valuable and could savecosts over the long term—such astreatment for high blood pressure,medication to reduce the risk of deathfor heart attack patients, and screeningfor colorectal cancer.xxiv Patients inareas of the country with high per capitahealth care spending have moreappointments with physicians, see alarger number of doctors, and spendmore days in the hospital—yet, onaverage, the quality of their care isworse, not better.
It has been observed that patients whofractured a hip, had surgery for coloncancer, or suffered a heart attack inregions with more health care resourcesand expenditures were more likely to diein the five years after the onset of theirproblem than patients in regions whereresources and spending were less.xxv
Patients treated for fractured hips atacademic hospitals in high-spendingregions were 1.9 percent more likely todie than their counterparts in low-spending regions, and colon cancer andheart attack patients were both 5.2percent more likely to die.xxvi (Dataadjusted for differences in patienthealth).xxvii This was true even thoughpatients in high spending regions visitmore doctors and spend more days inhospitals.
In fact, the Dartmouth Institute suggeststhat it is precisely the hospital- andspecialty-focused structure of care inthose high cost regions that leads to thepoorer outcomes. The Dartmouth

12
Institute suggests that this pattern ofunderuse of some care and overuse ofother, more expensive care is driven bywhat they call supply-sensitive care orsupply driven demand. In layman’sterms, this means that the more hospitalbeds, expensive hi-tech procedures ortests, and specialists are available, themore they will be used, regardless ofpatient need.
The source of supply-sensitive care isexplainable. To remain competitive intoday’s market, health systems andprovider groups expand hospitals, opendiagnostic centers, acquire new high-tech medical devices, and bring on newspecialists. In order to recover theexpense of their investment, they havean incentive to encourage usage of thesemore costly care alternatives, andinevitably patients who could be treatedadequately with primary or preventativecare will tend to receive the high costtreatment instead. To address thesecostly patterns of unnecessary care andpoor outcomes, we must first identify theincentives that create those patterns._________________________________Skewed Incentives Lead toUnnecessary Care
The first factor is the payment systemthat Medicare and some private healthinsurance companies use. Under thissystem, known as “fee-for-service”,health care providers receive paymentfor each visit with a patient, each testordered, and each procedure performed.Payment is not based on whether a givenservice is needed or how well the patientis cared for overall. Instead, payment isbased on how much care the patientreceives. Thus, the fee-for-servicepayment structure encourages hospitalsand doctors to deliver higher complexity
and quantity of tests and treatments inorder to maximize revenue.
Second is the problem of uncoordinatedcare. Often, the doctor treating a patientfails to consult with the patient’s otherphysicians. Without coordination, thepatient’s care becomes more fragmented,with no single person in charge of thepatient’s overall well-being. Poorcommunication among providers mayresult in the patient having the same testperformed twice. The patient’s treatmentunder one doctor may work at cross-purposes with another’s. Differentphysicians may even prescribe drugs thatshould not be taken at the same time.Unaware of the overall picture, eachphysician attempts to give the patientonly the care within the doctor’sspecialty. This results in both lesseffective care and wasted resources.
The lack of coordination in the deliveryof health care is exacerbated by the wayprivate and public payers compensateprimary care physicians, who are themost likely source of care coordination.An important component of quality careis time spent in consultation with apatient, which is typically the duty of theprimary care physician. Thereimbursement system, established byMedicare, and followed by manyinsurance companies, places a highervalue on procedures than onconsultation, even if consultation is moreuseful to patient health. Quality primarycare and coordinated care require moreconsultation. As a result, primary carephysicians have a lower reimbursementrate for the time they do spend withpatients than specialists. The imbalancebetween specialist and primary careincome has become so bad that only 7%of medical students are planning careers

13
in general practice or primary careinternal medicine, xxviii further restrictingour system’s ability to provide cost-saving care coordination.
A lack of patient knowledge andinvolvement in their care decisions alsocontributes to wasteful unnecessary care.Currently, physicians generally directcare decisions, with patients playing apassive role. But typically, when patientsare more involved in treatment decisionsand better understand the benefit andrisks of their options, they prefer lessintensive care, thus reducing costs.xxix
Finally, medical care given to patientstoo often lacks adequate basis inscientific evidence. Only half of medicalinterventions are supported by adequateevidence of clinical effectiveness.xxx. Ofthose diseases for which there is anestablished, evidence-based course oftreatment, patients receive therecommended care 54% of the time.xxxi
Even when evidence exists and anestablished course of treatment isavailable, clinical evidence has beenshown to fail to account for differingeffects of the same treatment on differentpopulations such as children or
minorities. In this environment ofuncertainty, providers are more likely toprovide the patient with excessive care,.i.e. more hospital admissions, moretests, more expensive procedures. Ifevidence were available, however, theprovider might use a more limited andless expensive set of treatments toaddress the case.
These sources of unnecessary andineffective medical care are complex.Yet over time, respected health systems,such as the Mayo Clinic and theIntermountain Health system, havetackled them and succeeded. Both theseinstitutions achieved low per patientcosts while providing excellent qualityof care and health outcomes.xxxii
According to the Dartmouth Institute forHealth Policy and Clinical Practice,hospital spending would decrease by43% if the entire nation matchedIntermountain Health’s per patientcosts.xxxiii If those savings had beenachieved in 2007, the United Stateswould have spent 13.5%, or $299 billionless on health care.xxxiv In Florida,achieving a 43% reduction in hospitalspending could save $13.54 billion.
Excessive Administrative Costs Inflate Insurance andMedical Prices
Some administrative spending isessential to the delivery of health care,but a large portion of administrativecosts pay for billing and other insurance-related activities that have little bearingon the quality of health care that apatient receives. Much of this isunnecessarily complicated andduplicative. As Americans struggle toafford care today and face rising
premiums and deductible, we can illafford spending on insurance companybureaucracy that does nothing toimprove health. Billing andcredentialing are two examples of theduplicative red tape in the insuranceindustry.
For doctors to be paid, doctors’ officesneed to send a bill to an insurance

14
company. Then they must record whenreimbursement comes through.Unfortunately, the complexity of billingand insurance requirements can turn thisseemingly simple task into an expensiveprocess. A single insurance companymay offer dozens of insurance plans thatcover different procedures at differentreimbursement levels and requiredifferent co-payments from patients.Complex billing systems do not add tothe quality of care that the patientreceives, but increase costs as physiciansand hospitals require more time andpersonnel to handle all the paperwork.
Insurance companies want to ensure thatdoctors covered by an insurance plan arecapable of providing high-quality care.To this end, insurance companies requirephysicians to submit information ontheir credentials before the insuranceplan will cover their services. With fewexceptions, every insurance plan asks forslightly different information, requiresphysicians to submit their credentials ina different format, and requests updatedinformation every few years. Similarly,hospitals want to ensure that onlyphysicians of skill and good traininghave admission privileges and thusrequire physicians to submit hospital-specific credential-review applications.
The Medical Group ManagementAssociation (MGMA), an organizationthat helps physicians deal with theadministrative complexities of practicingmedicine, surveyed physicians’ grouppractices to learn more aboutcredentialing demands. The surveyfound that, on average, each physicianhad to submit 17 credentialingapplications annually to insurancecompanies, hospitals, and other healthcare facilities, and that completing each
application required nearly 90 minutesof staff time.xxxv
The MGMA estimated that the U.S.spends $2.15 billion every year as everyhospital and health insurance companyverifies the credentials of the physicianswith which they work, even if thosephysicians’ credentials have beenverified by the hospital next door. If thisduplicative credentialing wereeliminated, the U.S. would save $1.95billion annually.xxxvi
_________________________________Insurance Company Red TapeCosts Americans Tens of Billions
A recent study suggests thatadministrative expenses by insurancecompanies contribute to the high cost ofcare. Conducted by Dr. James Kahn, thestudy examined the elements ofadministrative costs for insurers,hospitals, and doctors’ offices inCalifornia.
They analyzed the portion ofadministrative costs dedicated to billingand insurance-related activities ratherthan to oversight and management, sincethe latter can directly improve patientcare. The researchers studied hospitals,public and private insurance carriers, andphysicians’ offices of different sizes andspecialties to determine the amount oftime spent on administrative tasks thatdo not improve care. At insurancecompanies, for example, billing and,insurance-related costs included allclaims payment processing, sales,marketing, finance and underwriting.The costs incurred in reviewing thecredentials of doctors, providingcustomer service, maintaining computersystems, and reviewing cases werecounted partially as billing and

15
insurance-related and partially as qualityof care issues.
They found that billing and insurance-related activities comprise 85 percent ofinternal administrative costs forcommercial insurance plans, equal to 8percent of total health care premiums.
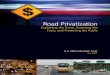
Dr. Kahn and his co-authors concludedthat billing and insurance-related costsrepresent 20 to 22 percent of privatelyinsured spending in hospitals and forphysician care in California (see Figure3).xxxvii
Figure 5. Spending by private insurers in California on share of billing andinsurance-related costs compared to total hospital and physician care paid byprivate insurers in Californiaxxxviii
Medical care66%
Otheradministrative
costs13%
Billing andinsurance-related
costs21%
Using national figures on spending byprivate insurance and total Californiaspending in hospitals and physicians’offices, an analysis by the CaliforniaPublic Interest Research Group foundthat the billing and insurance-relatedfunctions examined in the Kahn studyconsumed between $9 billion to $9.9billion in California.xxxix That is 5.4 to
5.9 percent of total health care spendingin the state.
This study’s data and conclusions arelimited to California. If the national levelof administrative red tape were just halfthat of California, it would account for2.7% of national health spending, or$72.9 billion. 2.7% of Florida’s healthspending would be $2.57 billion.
Unchecked Pharmaceutical Marketing Drives Up Costs
Extensive marketing of prescriptiondrugs raises health care costs and fails toimprove patient health. Pharmaceutical
marketing encourages patients to takedrugs that cost more and may be riskierthan alternative medications. In some

16
cases, it encourages use of drugs thatpatients do not need.
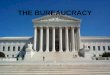
Pharmaceutical companies spent morethan two and a half times as muchmoney marketing drugs to consumers in2007 as they did just ten years earlier.The amount of marketing to physicians
rose more slowly—though stillincreasing more than 40 percent—butthe total cost of promoting drugs tophysicians was nearly twice that ofdirect-to-consumer advertising.xl 2007data did show a slight decrease in thepharmaceutical spending, but, at $11.45billion, it remains a staggering sum.
Table 4. Drug Company Spending (billions of 2007 dollars)xli
1997 2007 IncreaseDirect to consumer ads $1.34 $4.77 256%Promotion to physicians $4.75 $6.68 41%Total $6.09 $11.45 88%
Direct To Consumers DrugAdvertising Leads to Poor CarePhysicians strive to respond to patientrequests and ensure that the patient is incharge of his or her health care.However, doctors often have misgivingsabout writing a prescription requested bypatients, when those requests areprompted by DTC ads.
Consumers are not very well informedby whatever they learn frompharmaceutical marketing. Drug ads—from brief TV commercials to glossymagazine ads to the fine print of thoseads—are not designed to provideconsumers with a completeunderstanding of the relative risks andadvantages of drugs and to thoughtfullyevaluate their options.
Doctors recognize that DTC ads leaveconsumers ill-informed, and as a resultare often uncomfortable writingprescriptions requested by patients. In astudy published in the CanadianMedical Association Journal, Dr.Barbara Mintzes and colleagues foundthat when physicians wrote aprescription in response to a patientrequest, the doctor was reluctant about it
being the right choice in 50 percent ofcases.xlii
____________________________DTC Ads Promote the Use ofNewer, More Expensive, Less-Tested DrugsPharmaceutical companies undertakemulti-million dollar marketingcampaigns with extensive DTCadvertising for new drugs to promoteimmediate and widespread prescribing,and to maximize profits before thecompany’s patent expires. Often, thesenew drugs provide no additional benefitand may even impose greater risks onpatients. Unlike medications that havebeen on the market for years and used bymany patients, new drugs have beentested on only a few hundred or a fewthousand patients, in controlled studiesthat might have been only a few monthslong.xliii As a result, the complete sideeffects of the drug are not known whenmillions of patients begin taking themedication.
In response to ads, patients regularly asktheir doctors for a specific drug or for aprescription to treat a problem theylearned about through ads. Overall, theGovernment Accountability Office, in a

17
study of DTC ads, estimates that“between 2 and 7 percent of consumerswho saw DTC advertising requested andultimately received a prescription for theadvertised drug.”xliv
The end result of how consumersrespond to DTC ads and how physiciansrespond to patient requests is thatpharmaceutical companies earn anadditional $2.20 in sales for every $1spent on DTC ads.xlv From theperspective of a drug manufacturer, DTCads are effective at increasing sales andprofits. However, from a broaderperspective, DTC ads raise health carecosts without improving patient health._________________________________Marketing to Physicians InflatesPricesAs significant as the effects of direct-to-consumer marketing are, studies haveshown that physicians’ prescribinghabits change further in response tovisits from drug companyrepresentatives, ads in medical journals,and other approaches that directly targetdoctors.xlvi
In 2007, pharmaceutical companiesspent 40 percent more money marketingtheir drugs to doctors than toconsumers.xlvii Including the retail valueof free samples provided to doctors, thecost of marketing to physicians is severaltimes greater than the industry’sspending on DTC advertising.xlviii
Overall, drug companies spent $8,000 to$15,000 on marketing for every doctorin the U.S.xlix
Drug companies market their productsby providing free meals to doctors andtheir staff, paying for doctors to attendconferences or continuing medical
education events, paying speaking feesto doctors, placing ads in medicaljournals, and hiring thousands ofmarketing staff to visit physicians’offices to meet with doctors and deliverdrug samples. Professor Dick Wittink atYale has estimated that every dollar thatpharmaceutical companies spent on staffwho visited physicians’ offices earnedthe company $11.60 in additional sales.l
Journal ads increased sales by $12.20 forevery dollar spent.
Dr. Ashley Wazana at McGill Universityin Quebec analyzed the results of 29rigorous studies of how physiciansrespond to the influence ofpharmaceutical advertising and foundnumerous negative effects. Doctors withthe most interaction with drugcompanies wrote fewer prescriptions forgeneric drugs, failed more often toidentify false claims about drugs,requested more drugs with no realadvantage over those already available.li
Despite this powerful influence,information provided by drug companieshas been shown to mislead doctors aboutthe value and risk of various products,detracting from physicians’ ability toselect the best drug for a patient. Anexamination of the statements made bydrug company marketing staff whentalking to doctors revealed that 10percent of statements were wrong andthat every mistake placed the company’sdrug in a more favorable light.lii Asurvey of psychiatrists at the Departmentof Veteran’s Affairs found that “manyassertions made by drug companyrepresentatives are inconsistent withprescribing information approved by theU.S. Food and Drug Administration.”liii

18
Conclusion and Recommendations
The extent and causes of rising healthcosts described above are not new tohealth policy experts. In addition to thisreport, studies from the CongressionalBudget Office, the Institute ofMedicine,liv the Medicare PaymentAdvisory Commission,lv the DartmouthInstitute on Health Policy on ClinicalPractice, and the Commonwealth FundCommission on a High PerformingHealth Systemlvi have all spotlighted theneed for delivery and payment reformhighlighted here. States like New York,New Jersey, and Washington havelimited the amount that insurers canspend on administrative expenses.lvii
State and federal lawmakers areconsidering so-called sunshine laws toend the costly link between drugcompany marketing and prescribingpractices.
To avert dramatically higher costs,health reform legislation must tacklethese problems. If these wastefulpractices are left unaddressed,Americans can expect their premiumsand deductibles to rise dramatically, asdiscussed in the first section of thereport. But the consequences don’t stopthere. Without reform, rising costs inMedicare and Medicaid will squeezepublic sector budgets across thecountry.lviii And Florida’s businesses,already struggling with a tougheconomy, will face ballooning healthcosts if they still offer coverage orsicker, less productive employees if theydo not. There is no one silver bullet thatwill solve the problem of rising costs,but the analyses of misallocated care,administrative expenses, and drug costsabove do suggest a set of policy
solutions, that together can reduce thegrowth in health care costs._________________________________Reduce Ineffective Medical CareWhile Improving Quality
Reform public and privatepayment systems to provideincentives for quality of care,not quantity. Doctors andhospitals should be rewarded forproviding the type of care thatimproves patients’ health—notsimply for providing moremedical care under today’s fee-for service system.
Shift incentives to emphasizecoordinated and primary care.To reduce costly inefficient anduncoordinated care, innovativevehicles for coordination ofmedical care, such as medicalhomes, disease management, andcommunity health teams must beadopted as broadly aspracticable. Payment systemsshould be adjusted to compensateprimary care physiciansadequately.
Educate patients to help themmake the right decisions.Health reform legislation shouldexpand the amount ofinformation provided to patientsto evaluate doctors and hospitalsand promote “shared decision-making,” in which patients aregiven detailed information abouttreatment options andempowered to make decisionsabout their medical care.

19
Study what works and whatdoesn’t. The United Statesspends few resources onevaluating which courses oftreatment provide the bestresults, known as comparativeeffectiveness research. Thisresearch funding should bedramatically increased. Researchshould compare efficacy ofcompeting drugs. But, tomaximize savings, it should alsoprioritize comparison of specificpreventative approaches to morecostly pharmaceutical andsurgical treatments. Any suchresearch must include funding tostudy the disparate effects oftreatment on differentpopulations, including minorities,immigrants and children.
_________________________________Reduce ExpensiveAdministrative Bureaucracy
Develop standardized systemsfor enrollment, credentialing,billing and insurance payment.Financial incentives could beoffered to health care providerswho participate in a standardsystem, or such participationcould be required for any insurerjoining a connector or nationalinsurance subsidy program, orparticipation could be mandatedfor all insurers.
Limit insurers’ administrativeexpenditures to a certainpercentage of premium dollars.This would ensure that premiumpayments are going to healthcare, not administrative waste, bylimiting insurer’s spending that
isn’t related to care. It wouldcreate an incentive for efficientand simplifed interactions withphysicians and hospitals. Anysuch cap must ensure that thecosts of disease managementservices, which can reduce costsfor chronic care, are notrestricted.
_________________________________Reduce ExcessivePharmaceutical Marketing Costs
Increase Federal Monitoring ofAdvertising and Marketing.The Food and DrugAdministration should beef up itsmonitoring and enforcementefforts under existing lawsgoverning pharmaceuticalmarketing. The agency shouldset a goal of stopping falsestatements before advertising ormarketing materials get toproviders and the public.
End Improper MarketingPractices to Doctors. Restrictgifts to physicians and requiredrug companies to disclose moreinformation about theirmarketing to physicians,including gifts, free meals,speaking fees, and paidconsulting arrangements.
Provide Doctors Neutral,Unbiased Information onDrugs. To counter the sometimesmisleading information providedby pharmaceutical companies,independent efforts to provideobjective information on thebenefits and prices of drugsshould receive public fundingand support. Pennsylvaniaalready operates such an“academic detailing” program in

20
which physicians and researchersevaluate drugs and provideimpartial education aboutdifferent prescription drugs.lix
Some of these reforms could happenfairly quickly; others will take years. Butwithout action on health reform, highcosts will increasingly burden families,
businesses, and the economy as a whole.As the new Congress and Administrationtake up health reform, it is critical thatthey do health reform right by reducinghealth care spending that does notdeliver results.

21
A Note on Projections
The projections of health costs contained in the section “Cost of Inaction” were takenwholly from the New America Foundation report, The Cost of Doing Nothing. Thatreports’ authors explain their projections in the following way:
All of the projections in this paper are computed through the use of historicaldata. We assumed that if nothing is done to reform our health care system, thencosts would continue to grow at a similar rate as they have been for the pastdecade. Therefore, to compute our projections, we took 10 years of data anddetermined a compound annual rate of growth over that 10 year period. In caseswhere 10 years of matching data was not available, we took the longest possiblespan-the shortest being 7 years. These compound annual growth rates were thenapplied to the most recent year of data, in most cases, data from 2006 or 2007.By continually applying the annual growth rate, year by year, until 2016, we wereable to estimate how prohibitively expensive our health care system will be if wedo not act soon.
Endnotesi The Henry J. Kaiser Family Foundation. Employee Health Benefits: 2008 Summary of Findings.http://ehbs.kff.org/images/abstract/7791.pdfii The Henry J. Kaiser Family Foundation. Employee Health Benefits: 2008 Summary of Findings.http://ehbs.kff.org/images/abstract/7791.pdfiii The Henry J. Kaiser Family Foundation. Employee Health Benefits: 2008 Summary of Findings.http://ehbs.kff.org/images/abstract/7791.pdfiv Lake, Celinda “Women, Health Care reform, and the 2008 Election.” (Powerpoint presentation for RaisngWomen’s Voices conference.) October 15, 2008.v National Federation of Independent Business: downloaded on December 29, 2009 fromhttp://www.fixedforamerica.com/content/?id=294#businessvi National Federation of Independent Business: downloaded fromhttp://www.fixedforamerica.com/content/?id=294#businessvii Statement from Senator Edward M Kennedy, Massachusetts. November 18, 2008. downloaded fromhttp://kennedy.senate.gov/newsroom/press_release.cfm?id=B1442C22-02BC-458B-AB86-00FB987119A7&type=archiveviii Texeira, Ruy. What the Public Really Wants on Health Care. Center for American Progressix New America Foundation. The Cost of Doing Nothing. November 13, 2008. Downloaded fromhttp://www.newamerica.net/files/NAF_CostofDoingNothing.pdfx Congressional Budget Office, The Long-Term Outlook for Health Care Spending, November 2007.xi Ceci Connolly, “Malpractice Situation Not Dire, Study Finds,” Washington Post, 10 March 2005.xii Congressional Budget Office, Key Issues in Analyzing Major Health Care Proposals, 18 December 2008.xiii RAND, for the California Health Care Foundation, “Consumer Directed” Health Plans: Implications for HealthCare Quality and Cost, June 2005.xiv John Nyman, “Health Plan Switching and Attrition Bias in the RAND Health Insurance Experiment,”Journal of Health Politics, Policy and Law, April 2008, DOI:10.1215/03616878-2007-062.xv Barbara Culliton, “Insurers and ‘Targeted Biologics’ for Cancer: A Conversation with Lee N. Newcomer,”Health Affairs, web exclusive, 27 November 2007.

22
xvi Nolte, Ellen & C. Martin McKee. “Measuring the Health of Nations: Updating an Earlier Analysis,” HeatlhAffairs. 2008.xvii United Health Foundation, America’s Health Rankings: A Call to Action for People & Their Communities:Comparisons to Other Nations, downloaded fromwww.unitedhealthfoundation.org/ahr2007/comparisons.html, 20 March 2008.xviii United Health Foundation, America’s Health Rankings: A Call to Action for People & Their Communities:Comparisons to Other Nations, downloaded fromwww.unitedhealthfoundation.org/ahr2007/comparisons.html, 20 March 2008.xix U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, NationalHealthcare Quality Report 2007, February 2008.xx Nolte, Ellen & C. Martin McKee. “Measuring the Health of Nations: Updating an Earlier Analysis,”Heatlh Affairs. 2008.xxi Statement of Peter R. Orszag, Director, Congressional Budget Office. Opportunities o IncreaseEfficiency in Health Care at the Health Reform Summit of the Committee on Finance,United States Senate.June 16, 2008
xxiii Dartmouth Center for the Evaluative Clinical Sciences, An Agenda for Change: Improving Quality andCurbing Health Care Spending, 18 December 2008
xxv Dartmouth Center for the Evaluative Clinical Sciences, Supply-Sensitive Care: A Dartmouth Atlas ProjectTopic Brief, 15 January 2007.xxvi Dartmouth Medical School, Center for the Evaluative Clinical Sciences, The Dartmouth Atlas of HealthCare 2006: Care of Patients with Severe Chronic Illness, 2006.xxvii Elliott Fisher et al., “Variations in the Longitudinal Efficiency of Academic Medical Centers,” HealthAffairs, web exclusive, 7 October 2004.xxviii Hauer, Karen E., et.al. “Factors Associated With Medical Students' Career Choices Regarding InternalMedicine.” Journal of the American Medical Association. Vol. 300 No. 10, September 10, 2008.xxix Dartmouth Center for the Evaluative Clinical Sciences, Preference-Sensitive Care: A Dartmouth Atlas ProjectTopic Brief, 15 January 2007.xxx Consumers Union. Powerpoint Presentation to the Bipartisan Policy Center. April 2008. Downloadedfrom http://www.bipartisanpolicy.org/ht/d/sp/i/5479/pid/5479xxxi McGlynn, E.A., et al, “The Quality of Health Care Delivered in the United States,” The New EnglandJournal of Medicine, 2003:348(26): 2635-2645; and updated in Asch, S., et al., “Who is at Greatest Risk forReceiving Poor-Quality Health Care? The New England Journal of Medicine, 2006:354(11): 1147-1156.xxxii Dartmouth Medical School, Center for the Evaluative Clinical Sciences, The Dartmouth Atlas of HealthCare 2006: Care of Patients with Severe Chronic Illness, 2008.xxxiii xxxiii Dartmouth Center for the Evaluative Clinical Sciences, An Agenda for Chagne: Improving Quality andCurbing Health Care Spending, 18 December 2008.xxxiv $299 billions is 43% of $696.5 billion, the total national health expenditures on hospital care, accordingto Center for Medicare/Medicaid Serrvices. National Health Expenditures Aggregate Amounts and AverageAnnual Percent Change, by Type of Expenditure: Selected Calendar Years 1960-2007 . downloaded fromhttp://www.cms.hhs.gov/NationalHealthExpendData/Downloads/tables_.pdfxxxv Medical Group Management Association, Group Practice Research Network, Analyzing the Cost ofAdministrative Complexity in Group Practice, September 2004.xxxvi William Jessee, “Keep It Simple, Stupid: Administrative Complexity Raises Costs, Frustrates Patients andHampers Care,” Connexion, Medical Group Management Association, March 2004.xxxvii James Kahn et al., “The Cost of Health Insurance Administration in California: Estimates for Insurers,Physicians, and Hospitals,” Health Affairs, 240: 1629-1639, 2005.xxxviii James Kahn et al., “The Cost of Health Insurance Administration in California: Estimates for Insurers,Physicians, and Hospitals,” Health Affairs, 240: 1629-1639, 2005.

23
xxxix Nationally, private insurance paid for 36 percent of hospital care and 49 percent of physician care in2006, per U.S. Department of Health and Human Services, Centers for Medicare and Medicaid, Office ofthe Actuary, National Health Statistics Group, National Health Expenditures by Type of Service and Source ofFunds: Calendar Years 1960-2006, 7 January 2008. In California in 2004, total spending on hospital andphysician care was $108 billion, per U.S. Department of Health and Human Services, Centers for Medicareand Medicaid, Office of the Actuary, National Health Statistics Group, Health Expenditures by State of Provider:State-Specific Tables, 1980-2004, February 2007. Kahn et al. estimate that 19.7 to 21.8 percent of privateinsurance spending for hospital and physician care is consumed by billing and insurance-related costs.xl Government Accountability Office, Prescription Drugs: Improvements Needed in FDA’s Oversight of Direct-to-Consumer Advertising, November 2006.xli IMS Health Inc., “Total U.S. Promotional Spend by Type 2007.” Top Line Industry Data. 2008. downloadedfromhttp://www.imshealth.com/deployedfiles/imshealth/Global/Content/StaticFile/Top_Line_Data/PromotionalSpendChartWebsite.pdfxlii Barbara Mintzes et al., “How Does Direct-to-Consumer Advertising (DTCA) Affect Prescribing? A Surveyin Primary Care Environments With and Without Legal DTCA,” Canadian Medical Association Journal, 2September 2003, 169(5).xliii The Food and Drug Administration is willing to approve new medicines based on evidence from brief andpoorly designed studies, facilitating the entry of relatively untested drugs into the market. Committee on theAssessment of the U.S. Drug Safety System, Institute of Medicine, The Future of Drug Safety: Promoting andProtecting the Health of the Public (Washington, D.C.: The National Academies Press, 2007).xliv Government Accountability Office, Prescription Drugs: Improvements Needed in FDA’s Oversight of Direct-to-Consumer Advertising, November 2006.xlv Government Accountability Office, Prescription Drugs: Improvements Needed in FDA’s Oversight of Direct-to-Consumer Advertising, November 2006.xlvi Government Accountability Office, Prescription Drugs: Improvements Needed in FDA’s Oversight of Direct-to-Consumer Advertising, November 2006.xlvii IMS Health Inc., “Total U.S. Promotional Spend by Type 2007.” Top Line Industry Data. 2008.downloaded fromhttp://www.imshealth.com/deployedfiles/imshealth/Global/Content/StaticFile/Top_Line_Data/PromotionalSpendChartWebsite.pdfxlviii Government Accountability Office, Prescription Drugs: Improvements Needed in FDA’s Oversight of Direct-to-Consumer Advertising, November 2006.xlix David Blumenthal, “Doctors and Drug Companies,” New England Journal of Medicine 351(18), 28 October2004.l Dick Wittink, Yale School of Management, Analysis of Return on Investment (ROI) of PharmaceuticalPromotion (ARPP): A Second Independent Study, downloaded from www.rxpromoroi.org/arpp/index.html, 27March 2008. $11.60 in additional sales for every dollar spent applies to drugs that earned revenues of $500million or more and that were released from 1998 to 2000.li Ashley Wazana, “Physicians and the Pharmaceutical Industry: Is a Gift Ever Just a Gift?” Journal of theAmerican Medical Association 283(3), 19 January 2000.lii Michael Ziegler et al., “The Accuracy of Drug Information from Pharmaceutical Sales Representatives,”Journal of the American Medical Association 273(16), 26 April 1995, as cited in Michael Millenson, forBlueCross BlueShield Association, Getting Doctors to Say Yes to Drugs: The Cost and Quality Impact of DrugCompany Marketing to Physicians, no date. A more recent report by NJPIRG Law & Policy Center elaborateson the content of misleading information presented by drug companies. Abigail Caplovitz, NJPIRG Law &Policy Center, Turning Medicine Into Snake Oil: How Pharmaceutical Marketers Put Patients at Risk, May 2006.liii Michael Sernyak and Robert Rosenheck, “Experience of VA Psychiatrists with Pharmaceutical Detailing ofAntipsychotic Medications,” Psychiatric Services 58(10), October 2007.liv Institute of Medicine. Knowing What Works in Health Care: A Roadmap for the Nation January 24, 2-008.

24
lv Medicare Payment Advisory Commission. A Report to Congress: Reforming the Delivery System. June 2008.downloaded from http://www.medpac.gov/documents/Jun08_EntireReport.pdflvi Anthony Shih et al. Organizing the U.S. Health Care Delivery System for High Performance. CommonwealthFund Commission on a High-Performing Health System: Volume 98, August 7, 2008.lvii Families USA. Failing Grades: Consumer Protections in the Inidividual Health Insurance Market. June2008, Families USA. Downloaded from http://www.familiesusa.org/assets/pdfs/failing-grades.pdflviii Orxag, Peter, Director, Congressional Budget Office. The Overuse, Underuse, and Misuse of Health Care.Testimony before the U.S. Senate Finance Committee, July 17, 2008. downloaded fromhttp://www.cbo.gov/ftpdocs/93xx/doc9385/MainText.2.1.shtml.lix PACE Program of the Pennsylvania Department of Aging, Independent Drug Information Service, downloadedfrom www.rxfacts.org/home.html, 16 April 2008.