-
The International Journal of Oral & Maxillofacial Implants
1521
Osseointegrated oral implants are a major tool in prosthetic
dentistry. Although most implants are successful, implant failures
occasionally occur. Failing implants are frequently characterized
by loss of sup-porting bone, and these implants must be removed.
The reasons for failure of implants are multiple (occlu-sion,
parafunction, overloading, premature loading, and bacterial
infection).1 Above all, two principal rea-sons for implant failure
are mechanical stress and/or bacterial infection. Implants that
fail after demonstrat-ing osseointegration are considered to be
late failures. The factors contributing to late or delayed implant
fail-ure such as peri-implantitis are not well-known, and many
questions about etiology and treatment remain unanswered.
Peri-implantitis is defined as an irrevers-ible inflammatory
reaction associated with loss of sup-porting bone around an
osseointegrated implant in function.2,3 Two cross-sectional studies
reported that peri-implantitis was identified in approximately
28%
1 Assistant Professor, Division of Fixed Prosthodontics and Oral
Implantology, Department of Oral Rehabilitation, School of
Dentistry, Health Sciences University of Hokkaido, Kanazawa,
Hokkaido, Japan.
2 Professor and Chairman, Division of Fixed Prosthodontics and
Oral Implantology, Department of Oral Rehabilitation, Health
Sciences University of Hokkaido, Kanazawa, Hokkaido, Japan.
3 Assistant Professor, Department of Oral Microbiology, School
of Dentistry, Health Sciences University of Hokkaido, Kanazawa,
Hokkaido, Japan.
4 Professor and Chairman, Department of Oral Microbiology,
School of Dentistry, Health Sciences University of Hokkaido,
Kanazawa, Hokkaido, Japan.
Correspondence to: Dr Naoki Tamura, Division of Fixed
Prosthodontics and Oral Implantology, Department of Oral
Rehabilitation, School of Dentistry, Health Sciences University of
Hokkaido; 1757 Kanazawa Ishikari-Tobetsu Hokkaido, 061-0293, Japan.
Fax: +81-133-23-2892. Email: [email protected] 2013 by
Quintessence Publishing Co Inc.
Analysis of Bacterial Flora Associated with Peri-implantitis
Using Obligate Anaerobic
Culture Technique and 16S rDNA Gene SequenceNaoki Tamura, DDS,
PhD1/Morio Ochi, DDS, PhD2/Hiroshi Miyakawa, PhD3/Futoshi Nakazawa,
PhD4
Purpose: To analyze and characterize the predominant bacterial
flora associated with peri-implantitis by
using culture techniques under obligate anaerobic conditions and
16S rDNA gene sequences. Materials and Methods: Subgingival
bacterial specimens were taken from 30 patients: control (n = 15),
consisting
of patients with only healthy implants; and test (n = 15),
consisting of patients with peri-implantitis. In
both groups, subgingival bacterial specimens were taken from the
deepest sites. An anaerobic glove box
system was used to cultivate bacterial strains. The bacterial
strains were identified by 16S rDNA gene-
based polymerase chain reaction and comparison of the gene
sequences. Results: Peri-implantitis sites
had approximately 10-fold higher mean colony forming units (per
milliliter) than healthy implant sites.
A total of 69 different bacterial species were identified in the
peri-implantitis sites and 53 in the healthy
implant sites. The predominant bacterial species in the
peri-implantitis sites were Eubacterium nodatum, E brachy, E
saphenum, Filifactor alocis, Slackia exigua, Parascardovia
denticolens, Prevotella intermedia, Fusobacterium nucleatum,
Porphyromonas gingivalis, Centipeda periodontii, and Parvimonas
micra. The predominant bacteria in healthy implant sites apart from
Streptococcus were Pseudoramibacter alactolyticus, Veillonella
species, Actinomyces israelii, Actinomyces species,
Propionibacterium acnes, and Parvimonas micra. Conclusion: These
results suggest that the environment in the depths of the sulcus
showing peri-implantitis is well suited for growth of obligate
anaerobic bacteria. The present study
demonstrated that the sulcus around oral implants with
peri-implantitis harbors high levels of asaccharolytic
anaerobic gram-positive rods (AAGPRs) such as E nodatum, E
brachy, E saphenum, Filifactor alocis, Slackia exigua, and
gram-negative anaerobic rods, suggesting that conventional
periodontopathic bacteria are not the only periodontal pathogens
active in peri-implantitis, and that AAGPRs may also play an
important role.
Int J Oral MaxIIlOfac IMplants 2013;28:15211529. doi:
10.11607/jomi.2570
Key words: 16S rDNA, bacterial flora, obligate anaerobe,
peri-implantitis
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
1522 Volume 28, Number 6, 2013
and 56% of subjects and in 12% and 43% of implant sites,
respectively.3 Signs of a failing dental implant are detected both
clinically and radiographically, with the diagnosis made in a
similar way to periodontitis.4
The initially sterile and clean surface of an implant enters the
totally different environment of adult gingival or periodontal
tissues and bacterial flora, offering a new surface in the oral
cavity for adherence and coloniza-tion of bacteria. Biofilm
formation on oral implants can cause inflammation of peri-implant
tissue, endangering the long-term success of osseointegrated
implants.5 It is known that a large diversity of bacterial species
inhabit the peri-implant area. A common finding in previous studies
was that similar bacterial flora was found around oral implants and
natural teeth.6 A high proportion of coccoid cells and facultative
bacterial species and low frequencies of periodontal pathogens
including gram-negative bacteria were detected in healthy implant
sites. Clinical observations have recently revealed that early
colonization patterns differ between implant and tooth surfaces.7
On the other hand, many reports have indicated that the infected
lesions in the sulcus around peri-implantitis sites are
traditionally associated with chronic periodontopathic bacteria.8,9
It has tradition-ally been thought that peri-implantitis is
associated with a group of obligate anaerobic gram-negative rods
(OGNRs), in particular black-pigmented and motile rods, and that
gram-negative anaerobic cocci such as Veillonella also play an
important role.1,6,10 However, these periodontopathic bacteria have
also been ob-served in healthy implant sites.11
It has long been known that there are many uncul-tured,
undescribed, and unknown bacterial species in the human oral
cavity.1214 Some oral bacteria, such as asaccharolytic anaerobic
gram-positive rods (AAGPRs), are fastidious and grow poorly on
artificial culture me-dia; therefore, some of them are still not
well known. Numerous bacterial strains of AAGPRs have been
iso-lated from human oral infectious lesions, several of which have
been documented as etiologic agents of chronic periodontitis15
based on their frequent isola-tion from diseased periodontal
sites.
Previously, new isolates of AAGPRs were classified as members of
the genus Eubacterium, which has histori-cally acted as a
repository for a large number of diverse organisms16 and contains
species and groups that are phylogenetically unrelated.12 Recent
studies have de-scribed many oral AAGPR isolates, some of which
qual-ify as members of the genus Eubacterium but could not be
assigned to any of the established species. In addition, several
novel genera have been proposed for some of the AAGPRs, eg,
Pseudoramibacter, Slackia, Filifactor, and Mogibacterium, and some
species of Eubacterium have been transferred to the novel genera
according to their phylogenetic characteristics. It has
been shown that antibody titers against some species of AAGPRs
in the sera of patients with periodontitis are higher than those of
healthy people, suggesting that these bacteria cause immunologic
reactions in periodontal lesions.1,2,17 Nevertheless, AAGPRs are
not well-known because of the difficulty in cultivat-ing them, the
small size of the colony, and their lack of reactivity in
conventional biochemical tests. Thus, further studies are needed to
better understand the asaccharolytic microorganisms under the
obligate an-aerobic conditions of peri-implantitis.
Recently, the analysis of 16S rDNA gene-based polymerase chain
reaction (PCR) has become a useful approach to assess the
phylogenetic and taxonomic diversity of bacterial isolates.15,16,18
Culturing under obligate anaerobic conditions is also an important
technique to allow the detection of almost every spe-cies in a
given sample, revealing the presence of previ-ously uncultivated
and unclassified strains.
Peri-implant infection by pathogenic bacteria can-not be
understood without a comprehensive knowl-edge of obligate
anaerobes. Therefore, it seems appropriate to compare the bacterial
flora of peri-implantitis with that of healthy implants by using
cul-ture techniques under obligate anaerobic conditions and 16S
rDNA gene-based PCR. The aim of this study was to identify and
characterize the predominant an-aerobic bacterial flora in the
sulcus around progressive peri-implantitis in partially edentulous
patients.
MaTerials and MeThods
Patient and sample CollectionThis study was approved by the
ethics committee of the Health Sciences University of Hokkaido and
the Health Sciences University of Hokkaido Hospital (Kanazawa,
Hokkaido, Japan). The examination was performed with the
understanding and written con-sent of each patient. The patients
were categorized into two groups: the peri-implantitis group and
the healthy implant group. Medical and dental histories were
ob-tained, and full-mouth periodontal and implant exami-nations
were performed. Both groups had one or more dental implants exposed
for more than 6 months to the oral environment. The patients in the
peri-implantitis group had clinical signs of peri-implantitis
around one or more implants. The patients in the healthy implant
group had no clinical signs of peri-implantitis. One im-plant was
selected from each patient. Patients were ex-cluded if they had
severe systemic disease, had taken antibacterial medication, had
used mouth rinses dur-ing the previous 6 weeks, or had received
peri-implant therapy within the previous 6 months that could
inter-fere with the clinical parameters evaluated.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
The International Journal of Oral & Maxillofacial Implants
1523
Peri-implantitis sites were characterized by a prob-ing depth
(PD) of 4 mm, suppuration, bleeding on probing (BOP),19 and visible
three-thread loss of al-veolar bone clearly extending around the
implant as visualized on radiographs.3,20 PD was measured in the
deepest pocket of each quadrant between the gingival margin and the
base of the peri-implant pocket with a pressure sensitive probe
(Click-Probe, KerrHawe).21 BOP was recorded as present or absent.
Radiographic bone loss around implants was evaluated from available
ra-diographs (periapical or orthopantomography) from the
fixture-abutment junction or the shoulder of the implants, or the
cemento-enamel junction (Table 1). Based on these data, the
diagnosis of peri-implantitis was made.
Microbial samplingSample sites were isolated with cotton rolls,
air dried, and supragingival plaque was carefully removed using a
pledget of cotton wool to avoid contamination. Sub-gingival
bacterial specimens were taken with sterile endodontic paper points
(ISO #50), which were gently inserted to the deepest point of each
peri-implant or periodontal lesion and kept in place for 30
seconds. The paper points were then removed and placed in an
anaerobic sterile transport vial containing 1 mL of semisolid
medium (redox potential: 200 to approxi-mately 400 mV, 3.7% brain
heart infusion, 0.2% agar). Samples were transferred as soon as
possible (within 30 minutes) to an anaerobic glove box containing
80% nitrogen, 10% hydrogen, and 10% carbon dioxide.
Microbiological analysisFor in vitro evaluation, the suspension,
dispersion, and dilution of samples and the culture of bacterial
strains in the samples were carried out in the anaerobic glove box.
The inside of the anaerobic glove box was maintained under 300 mV
in redox potential during all experimental procedures. All plates,
media, buffer solutions, and experimental instruments were kept in
the anaerobic glove box for at least 7 days before use. Anaerobic
bacterial isolation was executed by the fol-lowing standard
procedures.
Each sample was suspended in 1 mL of sterilized
phosphate-buffered saline (PBS) and mechanically dis-persed with a
teflon homogenizer and vortex mixer for 30 seconds. Serial 10-fold
dilutions (0.1 mL each, from 102 to 106) were spread onto the
surface of nonse-lective blood medium (BHI blood agar plate; 3.7%
brain heart infusion, 1.5% agar, 5% defibrinated sheep blood, 0.1%
hemin, 0.1% menadione) and incubated in the anaerobic glove box at
37C for 7 days. Bacterial strains found on the nonselective blood
medium were enumerated, and their percentage of the total number of
colony forming units (CFUs) was calculated. When
the number of colonies on a BHI blood agar plate did not exceed
100, all of these colonies were isolated and subcultured for
identification.
Subcultured colonies were incubated anaerobically or aerobically
for 3 days, and for the purposes of this study, obligate anaerobes
were defined as bacteria that grew only in the anaerobic glove box.
In addition, these subcultured isolates were examined by gram
staining.
Primer selection and 16s rdna Gene-Based PCrFour primer sets
were included in individual PCR assays. The following universal
primers were used for amplifi-cation of approximately 1,500 bp 16S
rDNA22,23: forward primer 16S27F (5-AGAGTTTGATCCTGGCTCAG-3),
16S341F (5-CCTACGGGAGGCAGCAG-3), reverse prim-er 16S1492R
(5-TACGGCTACCTTGTTACGACTT-3), and 16S907R
(5-CCGTCAATTCCTTTGAGTTT-3). Each DNA amplification technique by
colony-directed PCR was performed in a total volume of 50 L in 0.2
mL micro-reaction tubes (MicroAmp, PE Biosystems), contain-ing 1PCR
buffer with 23 L deionized water, primers at a concentration of 0.2
mol/L, and 25 L of DNA polymerase (AmpliTaq Gold, PCR Master Mix,
Applied Biosystems).
The amplification program was as follows: pre-heating at 95C for
15 minutes, 35 cycles of denaturing at 94C for 1 minute, annealing
at 52C for 1 minute, extension at 72C for 5 minutes, and a final
exten-sion step for 10 minutes at 72C using a thermocycler (Veriti,
Applied Biosystems). The amplification prod-ucts were subjected to
electrophoresis on 2.0% aga-rose gel and visualized by ethidium
bromide staining.
sequencing of 16s rdna and Phylogenetic analysisThe PCR products
obtained above were sequenced at Takara Bio. Then, 16S rDNA
sequences of bacterial
Table 1 Patient selection Criteria
Peri-implantitis site
healthy implant site
Bleeding on probing +
Suppuration +
Probing pocket depth (PD)* 4 mm < 4 mm
Radiographic bone loss** +
Periodontal maintenance care
Antibacterial agent None None
Time since implant placement > 6 mo > 6 mo
*Probing pocket depth assessed as greatest distance between
gingival margin and base of the peri-implant pocket.**Radiographic
bone loss around implants was evaluated from available radiographs
from the fixture-abutment junction or the shoulder of the implants,
or the cemento-enamel junction.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
1524 Volume 28, Number 6, 2013
strains were compared with 16S rDNA gene sequences from the
GenBank database using the BLAST search program through the website
of the DNA Data Bank of Japan (DDBJ). A 16S rDNA gene sequence
similarity of 98% was used as the cutoff for positive
identification of taxa.24,25
statistical analysisThe Mann-Whitney U test (P < .01: average
total colony-forming units, P < .05: the proportional
distribution of OGNRs and AAGPRs) was used for statistical analyses
of the significant differences between the two groups.
resulTs
Clinical features of patients and sites selected for bac-terial
sampling are summarized in Table 2. A total of 30 partially
edentulous patients involved in this study were selected from
systemically healthy patients referred to the Health Sciences
University of Hokkaido and Health Sciences University of Hokkaido
Hospital. The patients included 12 females and 18 males. Fifteen
patients with peri-implantitis (8 females and 7 males) and 15
pa-tients with healthy implants (4 females and 11 males) were
characterized as shown in Table 2. The implants of the
peri-implantitis patients included three types. One implant was
made of single crystal aluminum oxide, 11 were made of commercially
pure titanium, and three implants were coated with hydroxyapatite.
The healthy implants were made of commercially pure titanium. The
mean age was 56.9 years (range, 46 to 76 years) in the
peri-implantitis group and 63.4 years (range, 46 to 77 years) in
the healthy implant group. The mean PD and CFUs were higher in the
peri-implantitis group than in the healthy implant group. The mean
PD was 6.8 mm (range, 4 to 10 mm) in the peri-implantitis sites and
1.3 mm (range, 1 to 3 mm) in the healthy implant sites. A high
proportion of patients with a diagnosis of peri-implantitis
presented with a generalized loss of supporting bone around the
implants.
Bacterial strains were detected in all colonies cul-tured on the
nonselective blood medium under an-aerobic conditions by serial
10-fold dilutions to a level 1104 per mL. Quantitative bacterial
analysis of peri-implantitis sites showed an average total of 6.34
0.52 colony-forming units (logarithm CFUs/mL).
Table 2 Clinical Features of Patients
Clinical featuresPeri-implantitis
sitehealthy implant
site
Patients 15 15
Age (y) 56.9 (range, 4676)
63.4 (range, 4677)
Sex (F/M) 8/7 4/11
Mean probing depths
6.8 (max, 10 mm; min, 4 mm)
1.3 (max, 3 mm; min, 1 mm)
Mean CFUs/mL* 6.34 0.52** 5.16 0.86
CFUs: colony-forming units; max: maximum; min:
minimum.*Logarithm CFUs/mL**Statistically different from healthy
implant sites, P < .01, Mann-Whitney U test.
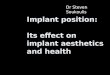
Fig 1 Proportional distribution of bacterial genera at
peri-im-plantitis sites: orange, OGNRs; blue, AAGPRs. Gram staining
characteristics: green, gram-pos-itive cocci; purple, gram-negative
cocci; light blue, gram-positive rods; red, gram-negative rods. The
bacterial flora of peri-implan-titis sites consisted of bacteria of
31 genera.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
The International Journal of Oral & Maxillofacial Implants
1525
In contrast, the average total CFUs in the healthy im-plant
group was 5.16 0.86. Significant differences were seen between the
CFUs of the peri-implantitis and healthy implant groups (P <
.01) (Table 2).
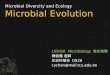
Figures 1 and 2 show the proportional distribu-tion of bacterial
genera in peri-implantitis sites and in healthy implant sites,
respectively. Streptococcus was the main genera present at both
healthy and peri-implantitis sites. The flora observed at
peri-implantitis sites consisted of bacteria of 31 genera, but only
20 genera were detected at healthy implant sites (Figs 1 and 2).
The total proportion of OGNRs and AAGPRs
accounted for about 40% of all CFUs at peri-implantitis sites,
in contrast to about 10% at healthy implant sites. At
peri-implantitis sites, the predominant genera were Streptococcus
(34%), Eubacterium (13%), Prevotella (10%), Actinomyces (6%), and
Fusobacterium (4%). At healthy implant sites, the predominant
genera were Streptococcus (45%), Actinomyces (14%), Veillonella
(14%), and Propionibacterium (8%). The proportion of Streptococcus
at healthy implant sites was larger than at peri-implantitis sites.
At peri-implantitis sites, Eubacterium that were AAGPRs and
Prevotella that were OGNRs were the next most predominant
genera.
Fig 2 Proportional distribution of bacterial genera at healthy
implant sites: orange, OGNRs; blue, AAGPRs. Gram staining
characteristics: green, gram-pos-itive cocci; purple, gram-negative
cocci; light blue, gram-positive rods; red, gram-negative rods. The
bacterial flora of healthy im-plant sites consisted of bacteria of
20 genera.
P < .05
Mea
n pr
opor
tion
of A
AGPR
s (%
)
40
30
20
10
0Peri-implantitis Healthy implants
P < .05
Mea
n pr
opor
tion
of O
GN
Rs
(%)
40
30
20
10
0Peri-implantitis Healthy implants
Fig 3 Mean proportional distribution of AAGPRs. The mean
proportional distribution was statistically significantly higher in
the peri-implantitis group (P < .05, Mann-Whitney U test).
Fig 4 Mean proportional distribution of OGNRs. The mean
pro-portional distribution was statistically significantly higher
in the peri-implantitis group (P < .05, Mann-Whitney U
test).
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
1526 Volume 28, Number 6, 2013
Figures 3 and 4 represent the mean proportional distri-bution of
AAGPRs and OGNRs. AAGPRs were detected in the peri-implantitis
group (18%) and in the healthy implant group (3%). OGNRs were
detected in the peri-implantitis group (20%) and in the healthy
implant group (6%). These data reveal statistically significant
differences between the two groups. The mean pro-
portional distributions were statistically significantly higher
in peri-implantitis (P < .05).
Peri-implantitis sites were colonized by complex bacteria with a
large proportion of OGNRs and AAGPRs. A total of 69 different
bacterial species were identified in the peri-implantitis sites
(Fig 5) and 53 in the healthy implant sites (Fig 6).
Fig 5 Proportional distribution of the 69 different bacterial
spe-cies identified at peri-implanti-tis sites: orange, OGNRs;
blue, AAGPRs.
Fig 6 Proportional distribution of the 53 different bacterial
spe-cies identified at healthy implant sites: orange, OGNRs; blue,
AAGPRs.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
The International Journal of Oral & Maxillofacial Implants
1527
Significant differences in bacterial species were observed
between healthy implant sites and peri-implantitis sites. The
predominant obligate anaero-bic bacterial species at the
peri-implantitis sites were E nodatum (7%), P intermedia (5%), F
nucleatum (3%), Filifactor alocis (3%), E brachy (3%),
Parascardovia denticolens (3%), and Parvimonas micra (3%), while
the predominant obligate anaerobic bacterial species at the healthy
implant sites were Veillonella species (spp) (14%),
Propionibacterium acnes (5%), Pseudoramibacter alactolyticus (3%),
and Parvimonas micra (2%).
disCussion
This study aimed to identify the predominant bacteria and
characterize the anaerobic bacterial flora in the sulcus around
progressive peri-implantitis. Selection of the patients for each
group was based on clinical conditions such as BOP, suppuration,
PD, and radio-graphic criteria (Table 1).
In this study, various designs of implant were repre-sented in
the peri-implantitis group. Previous studies have found no
statistically significant difference in the frequency of
peri-implantitis related to the type of im-plant, except for a
higher frequency of peri-implantitis around implants with rough
surfaces than around those with smooth surfaces. There is limited
and conflicting evidence to suggest that implant surface and design
may be a risk indicator for peri-implantitis. 26 In this study,
differences in implant surface were not taken into account,
although it may be an important area for future research.
In this study, the bacterial flora of peri-implantitis sites was
characterized using anaerobic culture tech-niques and 16S rDNA
gene-based PCR for bacterial identification, and compared with that
of healthy im-plant sites. All bacterial strains were cultivated
un-der obligate anaerobic conditions (redox potential: 400 mV).
Culture methods are known to be useful tools for studying the
bacterial flora of infectious le-sions by detecting which
microorganisms inhabit a given area,15 although the process is
labor intensive and time-consuming. However, sensitive and accurate
molecular techniques are necessary to characterize the bacterial
flora in peri-implantitis in order to deter-mine their association
with clinical symptoms and the prognosis of treatment. In the past,
a checkerboard DNADNA hybridization technique was the most usual
method for identifying bacteria in the field of clinical
dentistry.27 Although this technique can be used to detect
gene-specific bacteria, it cannot ran-domly detect bacteria.
Therefore, culture techniques under obligate anaerobic conditions
and 16S rDNA gene-based PCR are important tools for detecting
oral bacterial species in the human oral cavity, and for
identifying the predominant bacteria that may be im-portant
pathogens for infection.
As a result, the present study has demonstrated sig-nificant
differences between the bacterial flora in the two groups, and has
revealed characteristics of the bacterial flora of peri-implantitis
sites (Figs 5 and 6). In addition, significantly more CFUs were
observed in peri-implantitis sites than in healthy implant sites
(Table 2).
When the flora of the two groups were compared at the genus
level, the present study showed that the pre-dominant genera in the
peri-implantitis sites were Strep-toccocus and Eubacterium, while
genera Streptoccocus, Veillonella, and Actinomyces were predominant
in the healthy implant sites (Figs 1 and 2).
In the literature there has been much speculation surrounding
the relationship between implant failures and peri-implantitis, the
flora of periodontitis, and the flora of peri-implantitis. Failing
oral implants are gener-ally found to harbor bacterial flora
traditionally associ-ated with periodontitis such as P gingivalis,
T forsythia, T denticola, and F nucleatum. Previous studies have
found that the bacterial flora of peri-implantitis and periodontal
infections was similar,1,10 and one study demonstrated that in
several cases of peri-implantitis, culture techniques identified
species that included not only pathogens such as P gingivalis, P
intermedius, and A actinomycetemcomitans, but also Escherichia coli
and S aureus.28
Although Streptococcus was one of the predomi-nant genera
detected in samples from both groups, the species of the genus at
the two sites were completely different. S constellatus and S
sobrinus were frequently isolated from the peri-implantitis sites,
but were not detected at the healthy implant sites (Figs 5 and 6).
In contrast, S parasanguinis, S mutans, and S oralis were detected
only at healthy implant sites (Figs 5 and 6). A long-term study on
colonization of the peri-implant area showed a decrease in the
proportion of faculta-tive anaerobic cocci such as Streptococcus
species and an increase in the percentage of obligate anaerobic
rods, eg, Fusobacterium spp and Prevotella spp.29 These results may
indicate the possibility that some species of genus Streptococcus
have ecological significance in the flora of peri-implantitis
sites.
Veillonella spp were found to be the predominant bac-teria in
healthy implant sites in our study. This finding is consistent with
the observations of the previous study. 7
OGNRs were detected in both groups. Long-term clinical studies
have suggested that the bacterial flora of peri-implantitis sites
was characterized by a high proportion of OGNRs belonging to the
red and orange complex species.17,27,30,31 In this study,
microbiological culture of peri-implantitis sites has detected
bacterial species including P gingivalis, P intermedia, F
nucleatum,
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
1528 Volume 28, Number 6, 2013
Parvimonas micra, and other major pathogenic bacte-ria
characteristic of chronic periodontitis. Other studies have
reported that implants with peri-implantitis har-bor A
actinomycetemcomitans.32,33 However, these find-ings were not
confirmed at peri-implantitis sites in this study. Our results
showed the presence of P gingivalis, but red complex bacteria (T
forsythia, T denticola), A actinomycetemcomitans, S aureus, and
Candida spp were not detected. These bacteria may be cultivable but
undetectable for a mean CFU threshold level of 1104 per mL;
however, these bacteria must certainly be pres-ent at lower levels
than other red, orange, green, purple, and yellow complexes.
On the other hand, gram-positive bacilli accounted for 35% of
the total proportional distribution at peri-implantitis sites and
27% at healthy implant sites. In addition, AAGPRs were detected in
the peri-implan-titis group (18%) but were almost undetectable in
the healthy implant group (3%), confirming that the constitution of
the bacterial flora differed markedly between the two groups (Figs
3 and 4). A previous study reported that many AAGPRs are
significantly as-sociated with periodontitis, periapical
infections, and oral abscesses, but are rarely found under healthy
oral conditions.13 In the present study, an overwhelming number of
AAGPRs (colored green in Fig 3) and OGNRs (colored green in Fig 4)
were detected in peri-implantitis sites. These bacteria were
obligate anaerobes and were detected only in limited numbers at
healthy implant sites. The proportion of AAGPRs was almost the same
as the proportion of OGNRs at peri-implantitis sites. However,
AAGPRs were outnumbered more than two to one at healthy implant
sites. The ratio of AAGPRs to OGNRs and total isolates increased
significantly at peri-implantitis sites. Uematsu and Hoshino
reported that AAGPRs, such as Eubacterium, Mogibacterium, Slackia,
and others, often predominated in periodonti-tis sites.14 Thus, it
appears that AAGPR growth and bio-film formation may be influenced
by periodontopathic bacteria.
E nodatum, E saphenum, E minutum, and Filifactor alocis, which
are species of AAGPRs and were detected in this study, have been
known to produce the short-chain fatty acid butyrate as one of the
end products.14,15,18,34,35
OGNRs such as Fusobacterium spp and Prevotella spp are also
known to produce butyrate.3638 Butyrate has been reported to
inhibit cell growth of human gingival fibroblasts39 and human
endothelial cell proliferation in vitro,40,41 and to induce
apoptosis in T and B cells.37,42,43 Therefore, butyrate may have an
important role in the local tissue destructive process in the
pathogenesis of peri-implantitis. The presence of AAGPRs in this
study suggests that AAGPRs may possibly act in periodontitis to
cause tissue destruction at the base of the advanced progressive
peri-implantitis sulcus. This suggests that
bacterial flora at peri-implantitis sites reveals that AAGPRs
are also predominant in addition to specific bacteria linked with
peri-implantitis.
Previously, it was reported that uncultivated bac-terial species
were identified in peri-implantitis sites by 16S rRNA gene clone
library analysis.44 Since these species might not be detected in
the present study with culture techniques, further studies are
necessary for considering the role of uncultivated or viable
non-culturable bacterial species.
ConClusions
The present study indicates that an obligate anaerobic
environment exists at the base of the peri-implantitis sulcus, and
is suited for growth of AAGPRs and OGNRs. Although further work is
necessary to elucidate the bacterial flora in peri-implantitis, the
fact that the sul-cus around oral implants with peri-implantitis
showed high levels of AAGPRs and OGNRs suggests that con-ventional
periodontopathic bacteria are not the only periodontal pathogens
active in peri-implantitis, and that AAGPRs may possibly play an
important role.
aCKnowledGMenTs
The Health Sciences University of Hokkaido and the Health
Sci-ences University of Hokkaido Hospital supported this work. The
authors reported no conflicts of interest related to this
study.
reFerenCes
1. Pye AD, Lockhart DE, Dawson MP, Murray CA, Smith AJ. A review
of dental implants and infection. J Hosp Infect 2009;72:104110.
2. Albrektsson T, Isidor E. Consensus report of session IV. In:
Lang NP, Karring T (eds). Proceedings of the First European
Workshop on Periodontology. London: Quintessence, 1994:365369.
3. Lindhe J, Meyle J. Peri-implant diseases: Consensus report of
the Sixth European Workshop on Periodontology. J Clin Periodontol
2008;35:282285.
4. Brgger U, Hugel-Pisoni C, Brgin WB, Buser D, Lang NP.
Correlations between radiographic, clinical, and mobility
parameters after load-ing of oral implants with fixed partial
dentures. A 2-year longitudinal study. Clin Oral Implants Res
1996;7:230239.
5. Marinello CP, Berglundh T, Ericsson I, Klinge B, Glantz PO,
Lindhe J. Resolution of ligature-induced peri-implantitis lesions
in the dog. J Clin Periodontol 1995;22:475479.
6. Leonhardt , Renvert S, Dahln G. Microbial findings at failing
implants. Clin Oral Implants Res 1999;10:339345.
7. Frst MM, Salvi GE, Lang NP, Persson GR. Bacterial
colonization immediately after installation on oral titanium
implants. Clin Oral Implants Res 2007;18:501508.
8. Mombelli A, van Oosten MAC, Schrch E Jr, Lang NP. The
microbiota associated with successful or failing osseointegrated
titanium implants. Oral Microbiol Immunol 1987;2:145151.
9. Slots J, Rams TE. New views on periodontal microbiota in
special patient categories. J Clin Periodontol 1991;18:411420.
10. Shibli JA, Melo L, Ferrari DS, Figueiredo LC, Faveri M,
Feres M. Com-position of supra and subgingival biofilm of subjects
with healthy and diseased implants. Clin Oral Implants Res
2008;19:975982.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.
-
Tamura et al
The International Journal of Oral & Maxillofacial Implants
1529
11. Leonhardt , Grndahl K, Bergstrm C, Lekholm U. Long-term
follow-up of osseointegrated titanium implants using clinical,
ra-diographic, and microbiological parameters. Clin Oral Implants
Res 2002;13:127132.
12. Nakazawa F, Hoshino E. Genetic relationships among
Eubacterium species. Int J Syst Bacteriol 1994;44:787790.
13. Wade WG, The role of Eubacterium species in periodontal
disease and other oral infections. Microb Ecol Health
1997;9:367370.
14. Uematsu H, Hoshino E. Predominant obligate anaerobes in
human periodontal pockets. J Periodont Res 1992;27:1519.
15. Poco SE, Nakazawa F, Sato M, Hoshino E. Eubacterium minutum
sp. nov., isolated from human periodontal pockets. Int J Syst
Bacteriol 1996;46:3134.
16. Nakazawa F, Hoshino E. Immunological specificity of oral
Eubacterium species. J Gen Microbiol 1993;139:26352640.
17. Socransky SS, Haffajee AD. Dental biofilms: Difficult
therapeutic targets. Periodontol 2000 2002;28:1255.
18. Cheeseman SL, Hiom SJ, Weightman AJ, Wade WG. Phylogeny of
oral asaccharolytic Eubacterium species determined by 16S ribosomal
DNA sequence comparison and proposal of Eubacterium infirmum sp.
nov. and Eubacterium tardum sp. nov. Int J Syst Bacteriol 1996;46:
957959.
19. Lang NP, Nyman S, Senn C, Joss A. Bleeding on probing as it
relates to probing pressure and gingival health. J Clin Periodontol
1991;18:257261.
20. Lisa JA, Mayfield H. Peri-implant diseases: Diagnosis and
risk indica-tors. J Clin Periodontol 2008;35:292304.
21. Mombelli A, Graf H. Depth-force pattern in periodontal
probing. J Clin Periodontol 1986;13:126130.
22. Huys G, Vanhoutte T, Joossens M, et al. Coamplification of
eukaryotic DNA with 16S rRNA gene-based PCR primers: Possible
consequenc-es for population fingerprinting of complex microbial
communities. Curr Microbiol 2008;56:553557.
23. Washio J, Sato T, Koseki T, Takahashi N. Hydrogen
sulfide-producing bacteria in tongue biofilm and their relationship
with oral malodor. J Med Microbiol 2005;54:889895.
24. Fox GE, Wisotzkey JD, Jurshuk P Jr. How close is close: 16S
rRNA sequence identity may not be sufficient to guarantee species
identity. Int J Syst Bacteriol 1992;42:166170.
25. Stackebrant E, Goebel BM. Taxonomic note: A place for
DNA-DNA reassociation and 16S rRNA sequence analysis in the present
species definition in bacteriology. Int J Syst Bacteriol
1994;44:846849.
26. Heitz-Mayfield LJA. Peri-implant diseases, diagnosis and
risk indica-tors. J Clin Periodontol 2008;35(suppl 8):292304.
27. Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr.
Microbial complexes in subgingival plaque. J Clin Periodontol
1998;25:134144.
28. Leonhardt , Dahlen G, Renvert S. Five-year clinical,
microbiological, and radiological outcome following treatment of
peri-implantitis in man. J Periodontol 2003;74:14151422.
29. Mombelli A, Mericske-Stern R. Microbiological features of
stable osseointegrated implants used as abutments for overdentures.
Clin Oral Implants Res 1990;1:17.
30. Bower RC, Radny NR, Wall CD, Henry PJ. Clinical and
microscopic findings in edentulous patients 3 years after
incorporation of osseointegrated implant-supported bridgework. J
Clin Periodontol 1989;16:580587.
31. Botero JE, Gonzalez AM, Mercado RA, Olave G, Contreras A.
Subgin-gival microbiota in peri-implant mucosa lesions and adjacent
teeth in partially edentulous patients. J Periodontol
2005;76:14901495.
32. Van Winkelhoff AJ, Wolf JW. Actinobacillus
actinomycetemcomitans associated peri-implantitis in an edentulous
patient. A case report. J Clin Periodontol 2000;27:531535.
33. Hultin M, Gustafsson A, Hallstrom H, Johansson LA, Ekfeldt
A, Klinge B. Microbiological findings and host response in patients
with peri-implantitis. Clin Oral Implants Res 2002;13:349358.
34. Cato EP, Moore LVH, Moore WEC. Fusobacterium alocis sp. nov.
and Fusobacterium sulci sp. nov. from the human gingival sulcus.
Int J Syst Bacteriol 1985;35:475477.
35. Jalava J, Eerola E. Phylogenetic analysis of Fusobacterium
alocis and Fusobacterium sulci baced on 16S rRNA gene sequences:
Proposal of Filifactor alocis (Cato, Moore and Moore) comb. nov.
and Eubacte-rium sulci (Cato, Moore and Moore) comb. nov. Int J
Syst Bacteriol 1999;49:13751379.
36. Bartold PM, Cully NJ, Zilm PS, Rogers AH. Identification of
compo-nents in Fusobacterim nucleatum chemostat-culture
supernatants that are potent inhibitors of human gingival
fibroblast proliferation. J Periodont Res 1991;26:314322.
37. Kurita OT, Ochiai K, Fukushima K. Volatile fatty acid,
metabolic by product of periodontopathic bacteria, induces
apoptosis in WEHI 231 and RAJI B lymphoma cells and splenic B
cells. Infect Immun 1998;66:25872594.
38. Takahashi N, Sato T, Yamada T. Metabolic pathways for
cytotoxic end product formation from glutamate and
aspartate-containing pep-tides by Porphyromonas gingivalis. J
Bacteriol 2000;182:47044710.
39. Jeng JH, Chan CP, Ho YS, Lan WH, Hsieh CC, Chang MC. Effects
of butyrate and propionate on the adhesion, growth, cell cycle
kinet-ics, and protein synthesis of cultured human gingival
fibroblasts. J Periodontol 1999;70:14351442.
40. Tse CS, Williams DM. Inhibition of human endothelial cell
prolifera-tion in vitro in response to n-butyrate and propionate. J
Periodont Res 1992;27:506510.
41. Pllnen MT, Overman DO, Salonen JI. Bacterial metabolites
sodium butyrate and propionate inhibit epithelial cell growth in
vitro. J Periodont Res 1997;32:326334.
42. Kurita OT, Fukushima K, Ochiai K. Butyric acid-induced
apoptosis of murine thymocytes, splenic T cells, and human Jurkat T
cells. Infect Immun 1997;65:3541.
43. Kurita OT, Fukushima K, Ochiai K. Lipopolysaccharide
stimulates butyric acid-induced apoptosis in human peripheral blood
mono-nuclear cells. Infect Immun 1999;67:2229.
44. Koyanagi T, Sakamoto M, Takeuchi Y, Ohkuma M, Izumi Y.
Analysis of microbiota associated with peri-implantitis using 16S
rRNA gene clone library. J Oral Microbiol 2010;2:51045110.
2013 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS
DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART MAY BE
REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION
FROM THE PUBLISHER.